
CMV:AnUpdate
JayA.Fishman,M.D.Professor ofMedicine,HarvardMedicalSchool
Director,TransplantInfectiousDiseaseandCompromised HostProgram,MassachusettsGeneralHospital
AssociateDirector,MGHTransplantCenter,Boston,MA,USA

Virusesmaybedangerous....

Cytomegalovirus
• Betaherpesvirinae subfamilyoftheHerpesviridae• Thestructure:
– Nucleuscontainingtheviralgenome(lineardouble-strandedDNA)– Icosahedral proteincapsid– >200geneswithsignificantvariation– Thetegumentproteinmatrix(e.g.,pp65):
• Proteinswithstructuralroles• Proteinswhichmodulatestheimmunehostcellresponse
– Anouterenvelopederivedfromthehostcellnuclearmembrane.• GlycoproteingB - involved incellattachmentandpenetration• GlycoproteingH- involved inthefusionoftheviralenvelopewiththehostcellmembrane
Pérez-Sola,M.J.etal.EIMC2008;26(1):38-47
CroughTetal.ClinMicrobRev,Jan2009,76-98

PathogenicConsiderations
• Longerreplicationcyclethanotherherpesviruses• Reactivation ofviralreplicationisrelatedtohostimmunityand
inflammation• “CMVInfection”isnotuniform
– ManygeneticvariantstrainsofCMVwithmultipletargetcells:Monocytes,macrophages,endothelialcells,epithelialcells,parenchymalcells,immaturedendriticcells,lymphocytes,CD34+cells
– “Latency”inmultiplecelltypes– Biologicaleffectsvarybyviralstrain:
• Cellulartropism,penetrationandtransfertothecellnucleus
• Viralgeneexpressioniscelltype-specific• Replicationandspreadtoothercells(virulence)• Immuneresponsestoinfectionbycelltype

DisseminatedCMV
Liver
LungKidney
Colon

RiskfactorsforCMVdiseaseinsolid-organtransplantpatients
§ Primaryinfection(D+/R−)§ Transplantedorgans,cells§ Bloodproducts
§ FactorsfavoringCMVreactivation§ Inflammation/Fever (cytokines)§ Surgery/Trauma§ Intraoperative hypothermia§ Sepsisorseverebacterial
infections§ T-celldepletion§ Co-infectionswithotherviruses
§ Herpesvirus6or7(HHV6or7)
Factorsfavoringprogressiontoinvasivedisease• Immunosuppression
• T-celldepletion• Mycophenolate,azathioprine• Methylprednisoloneboluses• Alemtuzumab• Highviralload
• Immunomodulation• Herpesvirus6(HHV6)orHHV7
• Geneticfactors• MutationsinTLR2andTLR4genes• Deficiencyofmannose-binding lectin orgenotypeassociatedwithlowproduction ofMBL
ModifiedfromGESITRA-SEIMC/REIPIrecommendationsforthemanagementofCMVinfectioninsolid-organ transplantpatients,Enferm InfeccMicrobiol Clin.2011

CMVreplicationandrelease
PathwaysforCMVreactivation
ReinkePetal.TransplantInfectDis 1999;1:157-64.
TNF-α
NF-κBStress
catechols
Pro-inflammatoryprostaglandins
cAMP
EICMV
Anti-T-cellantibodies
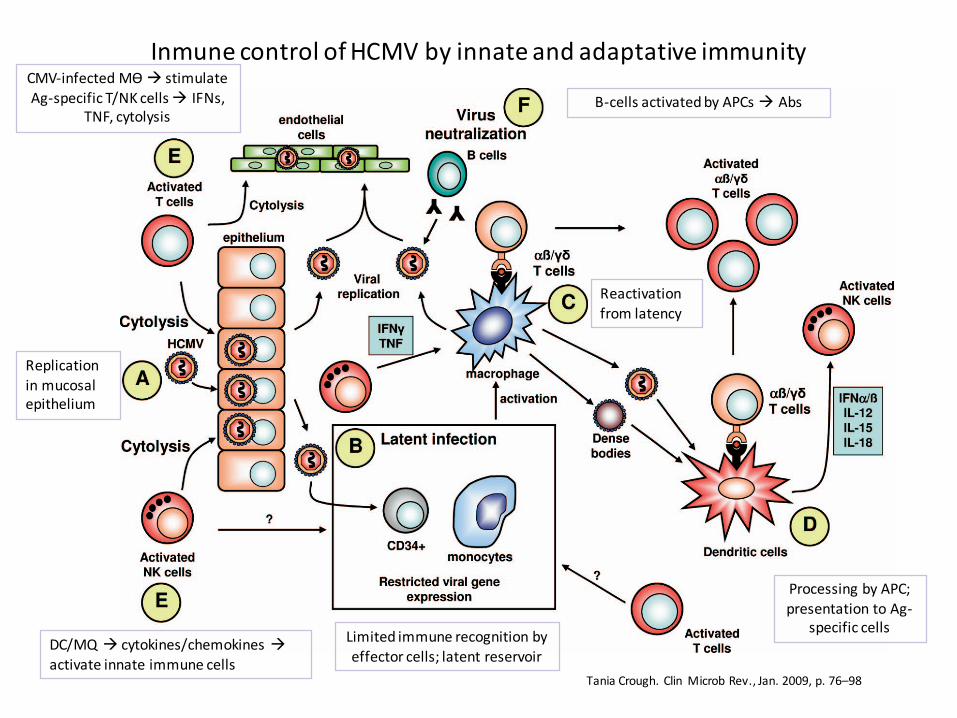
InmunecontrolofHCMVbyinnateandadaptativeimmunity
TaniaCrough.ClinMicrobRev.,Jan.2009,p.76–98
Replicationinmucosalepithelium
Limitedimmunerecognitionbyeffectorcells;latentreservoir
Reactivationfromlatency
ProcessingbyAPC;presentationtoAg-
specificcellsDC/MQà cytokines/chemokinesàactivateinnateimmunecells
B-cellsactivatedbyAPCsà AbsCMV-infectedMѲ à stimulateAg-specificT/NKcellsà IFNs,
TNF,cytolysis

1. CMVinhibitsdifferentiationofmyeloidantigen-presentingcellsfrommonocyticprecursors(transientblockinthecytokine-induceddifferentiationofmonocytesintofunctionallyactiveCD1a-positivedendritic cells)
2. CMValterstheimmunostimulatory propertiesofdifferent subsetsofmonocytesandDC,rendering themlesscapableofdeveloping intoprofessionalAPCs.
3. VirallyencodedIL-10(cmvIL-10)blunts theantiviralpropertiesofAPCs.4. HCMVhampersantigen-presentingcelltraffickingandphagocytic capacity.
– DecreasedAPCmigrationtositesofinflammationandtodraining lymphnodesinresponsetochemotactic stimuli(RANTES,MIP-1,andMIP-3)
• HCMV-infectedPlasmacytoid DCshavereducedsecretionofcytokinesincluding IFN-γ,reducedallostimulation,decreasedCD4andCD8T-cells
5. Transitorybutsubstantialimmunosuppressionthatinhibits theimmuneresponseagainstthevirusandunrelatedpathogens,mainlyinsubjectswithprimaryinfection
• Reactivationofotherviralinfectionsduring acuteHCMVinfection• Enhancespre-existingimmunosuppression insolid-organ transplantand
alloSCT recipients, increasingtheirriskforinvasivebacterialandfungalinfections
CMVaffectsmanyfunctionsofantigen-presentingcells

CMVRetinitis:LungTransplantRecipient

CMVcecalulcerationinpatientwithnegativeantigenemiaandPCRassaysforCMV

DirectEffects:InvasiveInfectionbyCMVInvasiveColitisAfterLiverTransplant

EffectsofViralInfectioninTransplantation
• “DIRECTEFFECTS”-- CAUSATIONOFINFECTIOUSDISEASESYNDROMES– Feverandneutropenia,hepatitis– Colitis,Retinitis,Nephritis,Pancreatitis
• “INDIRECT”orIMMUNOMODULATORYEFFECTS– SystemicImmuneSuppressionà OI’s– GraftRejection,GVHD– AbrogationOfTolerance
• Oncogenesis/CellularProliferation– HepatitisB:hepatocellular carcinoma– EpsteinBarrVirus:B-celllymphoma(PTLD)– HepatitisC:splenic lymphoma(villouslymphocytes)– Papillomavirus:Squamous cell&anogenital cancer– HHV8(KSHV):Kaposi’ssarcoma,effusionlymphoma– Acceleratedatherogenesis,BK-uretericobstruction

CMVSyndromeFever
WeaknessMyalgiaArthralgia
Myelosuppression
EndOrganDiseaseNephritisHepatitisCarditisColitis
PneumonitisRetinitis
Encephalitis
CMVdisease
LatentCMVinfection
ActiveCMVinfection(viremiaandintissue)
ALG,Fever,TNFα,Sepsis,Suppression
AtherosclerosisBronchiolitisobliterans
Vanishingbileductsyndrome
Opportunisticinfection
Systemicimmunesuppression
Acute Chronic Acute
Cellulareffects:antigenandcytokine
expression
EBV-associatedPTLD
Allograftinjury1
Allograftrejection1
FishmanJA&RubinRHNEngl JMed.1998;338:1741

HCMVProtein Function
FCReceptorhomologueTRL11/IRL11,UL118/119
Blocksantibody-dependent cytotoxicity;binding nonspecificantibodycoatingagainstCD8andNKcells
Pp65matrix Phosphorylates IE-1proteintoinhibitMHCclassI-restrictedantigenpresentation
US3,US6,US10,US11 BlockgenerationandexportofMHCclassIpeptidesUS3,US6,US10,US11 ReducedexpressionofMHCclassIpeptidesUS2 ReducedantigenpresentationinMHCclassIIpathwayMHC-Ihomologue UL40,UL122miRNA,UL142,UL141
BlocksNKcellactivation(also:UL16,pp65)
UL18 MHCclass1homologue; reducedimmunesurveillanceUL20 T-cellreceptorhomologue; reducedantigenpresentationIE86 Inactivatesp53;increasesmoothmuscleproliferationUL33,UL33,UL78,US27,
US28Transmembraneproteinschemokinereceptors;reduced
interferonandchemokineeffects;reducedinflammation, increasedviraldissemination
IL-10homologue UL111a;IL8CXC-1UL146,UL147
Immunosuppression; reducedMHCclassI/IIexpressionandlymphocyteproliferation; increasedneutrophilchemotaxis;reduceddendritic cellandmonocytechemotaxisandfunction
UL144 TNFreceptorhomologueUL36,UL37 Anti-apoptosis forinfectedcells

CMVinterfaceswithinnateandadaptiveimmunesystems
CroughandKhanna,ClinMicrobiol Rev2009
Areasofinvestigation:
- Migrationandchemotaxis
- Cellulardifferentiation- Cellsurvivaland
apoptosis- Determinantsof
reactivationandlatency
- Pathogenrecognition- Globaltranscriptional
andfunctionalchanges

CMV“IndirectEffects”:PossibleMechanisms• UpregulationofMHCclassIIantigensandhomologybetweenCMVIEantigen
andMHCclass-I(HLA-DRβ)1-2
• BlockofCD8+(MHCclassI)recognition• BlocksCMVantigenprocessinganddisplay(immediateearlyAgmodification,
poorCTLresponse)• IncreasedICAM-1,VCAM,cellularmyc&fos(adhesion)• InversionofCD4/CD8ratio3-4
• Increasedcytokines:IL-1β,TNFα,IFNγ,IL-10,IL-4,IL-8,IL-2/IL-2R,C-X-Cchemokines,andIL-85-6
• IncreasedcytotoxicIgM7
• Stimulationofalloimmuneresponsebyviralproteins1-2
• IncreasedPDGF,TGFβ;autoantibodies• IncreasedgranzymeBCD8+T-cells,γδ-T-cells
ICAM-1=Intercellularadhesionmolecule-1PDGF=Platelet-derivedgrowthfactorVCAM=Vascularcelladhesionmolecule
1.Fujinami RS,etal.JVirol. 1988;62:100-105.2.BeckS.Nature. 1988;331:269-272.3.SchooleyRT,etal.NEnglJMed.1983;308:307-313.4.Fishman JA,etal.DiagnImmunol.1983;1:261-265.5.KernF,etal.JAmSocNephrol.1996;7:2476-2482.6.TongCY,etal.JMedVirol.2001;64:29-34.7.BaldwinWM3rd,etal.BrMed(ClinResEd).1983;287:1332-1334.

Mechanisms– ShortVersion– ⇑ Adhesionmolecules(VCAM,ICAM,LFA-1,VLA-4)
– ⇑ Pro-inflammatorycytokines– ⇑ HLA-DRandMHCClassImimic– ⇑ Anti-endothelialAbs?– ⇓ Antigenpresentation(dendriticcellmaturation)
– ⇓ Leukocytemobilization

OpportunisticInfectionsPromotedbyCMVInfectioninTransplantPatients
• Pneumocystiscarinii• Fungalinfections(esp.intra-abdominaltransplants):• Candidemia andintra-abdominal infection inOLTx;patientswithinitialpoorgraftfunction
• Aspergillusspp.RoleofCMVinpromotingfulminant HCVhepatitisratherthandirecteffect
• Bacteremia:Listeria monocytogenes• Epstein-Barrvirusinfection(RCWalkeretal,CID,1995,20:1346-55),HHV6,HHV8/KSHV?
• HCV:riskforcirrhosis,retransplantation,mortality

IndirectEffectsofCMV:Organ-specific• Renal:Decreasedearlygraftfunctionandsomechronicdysfunction(increased
byHHV6andHHV7)– AcutebutpossiblynotchronicallograftrejectionisreducedbyCMV
prophylaxis
• Liver:CMVassociatedwithcirrhosis,graftfailure,needforretransplantation&death– MoreaggressiveHCVrecurrenceandfibrosisafterOLTx (partially
attributedtoHHV6)– CMVdiseaseispreventable
• Heart:cardiacallograftvasculopathy– Reducedbyganciclovir +/- CMVIg
• Lungs:CMVandD+/R- associatedwithBronchiolitisObliteransSyndrome,infection,death– Reducedbyivganciclovir +/- CMVIg
• Pancreas:Notstudied(noCMVyetinislets)

CMVandHSCTOpportunisticInfections
MarretalBlood2002 Nichols etalJID2002

Therapeutics- Terminology• Whatareyoumeasuring?
– Antigenemia– measuringCMVspecificantigeninPBMCs,forexamplepp65assay
– Viremia– culture-basedonly(requiresreplicatingvirus)– DNAemia – measuringCMVDNAbyQNAT (wholebloodor
plasma)QNATcalibratedtotheWHOstandardispreferredfordiagnosis,decisionsregardingpreemptiveantiviraltreatment,andmonitoringresponsetotherapy.
– TissueorBAL– mustbenormalizedtohousekeepinggene,urea,unitvolume,unitmass.
– Viralassaysandcultureofblood,urine,ororalsecretionsarediscouragedinadultsfordiagnosisofactiveinfectionordisease.
• Serology– PositiveIgGisamarkerofpreviousexposure(positive
serologydoesnotdefine“activeinfection”)

Recommendations:Diagnostics• EitherplasmaorwholebloodisanacceptablespecimenforQNAT.Specimentypeorassayshouldnotbechangedwhenmonitoringpatients.
• DespitereportinginIU/ml,viralloadvaluescannotbedirectlycomparedacrosscentersand/orlaboratoriesunlessidenticaltestingreagentsandprocedurescanbeassured.
• Changesinviralloadexceeding0.5log10IU/ml(3-fold)areconsideredtorepresentclinicallysignificantdifferencesinDNAemia

Terminology2
• Surveillance – patientisatrisk,butnoevidenceofanevent(infection)orbiomarker(NAT)
• Monitoring – Patienthaseventorbiomarker(previouslyknownpositiveassay)
• Hybridapproach– universalprophylaxisfollowedbypreemptivetherapy(surveillanceafterprophylaxis)
DoweknowhowtoPreventCMVInfection?
Universalvs.Pre-emptivetherapy

Prophylaxisvs PreemptiveTherapy
• ProphylaxismaybepreferredinD+/R-,withD+orR+&antilymphocyte therapy,potentimmunosuppression including desensitization (plasmapheresis orimmunoadsorption) andABOincompatibleprotocols,orwithrituximab,bortezomib,eculizumab.Rolewithbelatacept hasnotbeenstudied.
• Treatmentofacuterejectionwithantilymphocyte antibodies inat-riskrecipientsshould resultinreinitiation ofprophylaxisorpreemptivetherapyfor1to3months
• CMVDNAemia iscommonaftercessationofprophylaxis,notablyinhighriskpatients
Prophylaxis PreEmptiveTherapy
EarlyCMVDNAemia Rare CommonPreventionofCMVdisease Goodefficacy Goodefficacy*
(*less optimalinhighriskpopulations)
LateCMV(infection/disease) Common RareResistance Uncommon UncommonEaseofimplementation Relativelyeasy MoredifficultOtherherpesviruses PreventsHSV,VZV DoesnotpreventOtherOpportunisticinfections Mayprevent UnknownCost Drugcosts Monitoringcosts
Safety Drugsideeffects Lessdrugtoxicity
Preventionofrejection Mayprevent Unknown
Graftsurvival Mayimprove Mayimprove

Time(days)
DoublingTime=ln2/a
y=y0eax
AverageDT=1-2days
Log 1
0ViralLoa
d
detectionthreshold
Preemptive inD+/R-
LisboaLF,etal.Abstractpresentedat:AmericanTransplantCongress;May30-June 3,2009;Boston,Massachusetts.Abstract388. DT=Doublingtime

CMVdiseaseinD+/R- renalrecipients:Meta-analysis(allagents)
• UniversalandPre-emptiveprophylaxissignificantlyreducetheriskofCMVdisease
-81%
-64%
-100%
-80%
-60%
-40%
-20%
0%Universal Pre-emptive
CM
V di
seas
e ris
k re
duct
ion
(%)
p=ns
Kalil AC et al. Ann Intern Med 2005; 143: 870

Anti-CMVProphylaxisIsAssociatedWithIncreasedRenalGraftSurvivalat4Years(P=0.0425)
1009080706050
0
Oralganciclovirprophylaxis
IVpreemptivetherapy
Freedo
mfrom
graftlo
ss;
uncensored
ford
eath(%
)
1 2 3 4Timeaftertransplantation(years)
KliemV,etal.AmJTransplant. 2008;8:975-983. (B)Khoury JA,etal.AmJTransplant.2006;6:2134-2143. (VGCV)(B)ReischigT,etal.AmJTransplant. 2008;8:69-77. (VACV)(B)
Pvalue(Logranktest)=0.0425
ProphylaxisreducedCMVinfectionby65%(P<0.0001)

Effectofanti-CMVprophylaxisonconcomitantinfections
0.31
0.65
0.27
0.0
0.2
0.4
0.6
0.8
1.0
Placebo/notreatment
Herp. Simplex,Varic. Zoster
Bacterialinfections
Protozoalinfections
Rela
tive
risk
-73% -69%-35%
Hodson EM et al. Lancet 2005; 365: 2105
FungalInfections
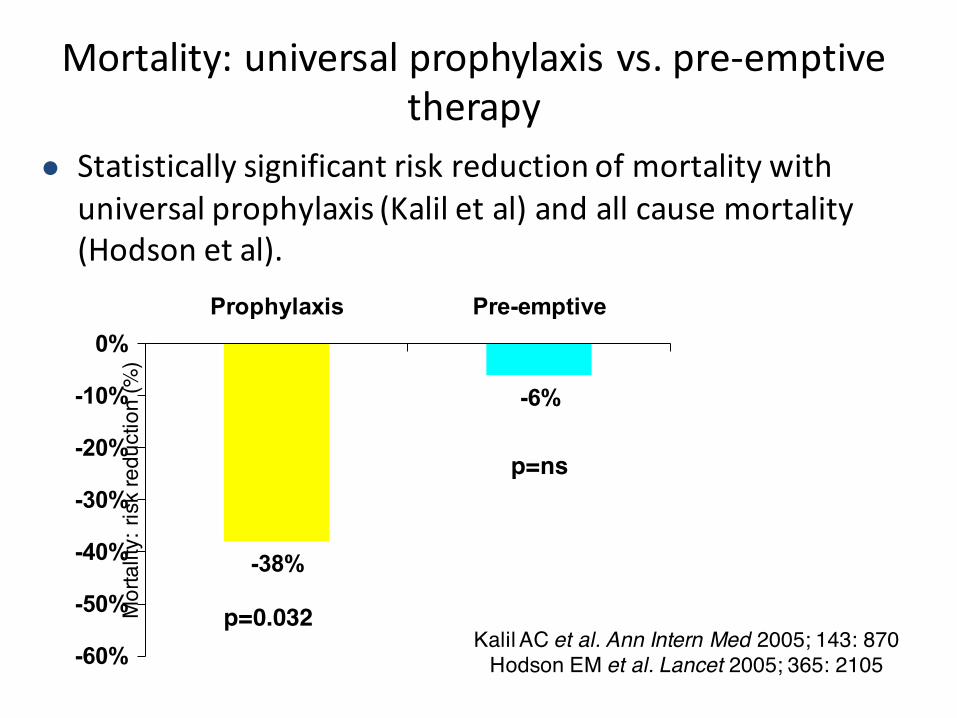
l Statisticallysignificantriskreductionofmortalitywithuniversalprophylaxis(Kaliletal)andallcausemortality(Hodsonetal).
Mortality:universalprophylaxisvs.pre-emptivetherapy
-38%
-6%
-60%
-50%
-40%
-30%
-20%
-10%
0%Prophylaxis Pre-emptive
Mor
talit
y: ri
sk re
duct
ion
(%)
Kalil AC et al. Ann Intern Med 2005; 143: 870Hodson EM et al. Lancet 2005; 365: 2105
p=0.032
p=ns

àD+/R+recipientsonpreemptivetherapyhadhighestrateofCMVdisease(19.2%vs.4.4%,P0.003).àNochgGFR,rejection,graftloss(5yrf/u)
11%
39%

D+R−onPre-emptiveTherapy:DirecteffectsofCMVandanti-CMVtreatment
Prophylactic(n=32)
Preemptive(n=80)
PValue
CMVinfection 11(34%) 40(60%) 0.02CMVdisease 5(16%) 21(26%) 0.3Late-onsetinfection 9(28%) 6(8%) 0.003Peakviralload(mean,log10copies/mL)
4.2±1.1 5.0±1.0 0.06
Anti-CMVdrugresistance 1(3%) 13(16%) 0.05RecurrentCMV 3(9%) 18(23%) 0.1
Couzietal,High IncidenceofAnticytomegalovirusDrugResistanceAmongD+R−KidneyTransplantRecipientsReceivingPreemptiveTherapy,AJT,2011

Prophylaxis,Pre-emptiveTherapy,andHybridCare
1 32 765Transplant Months
Pre-emptivemonitoringperiod(onceweeklyfor12-16weeks);ifCMVdetected(viralloadorpp65Ag),treatuntilcleared
indicatesCMVsurveillancebyviralload(orpp65Ag)
AmericanSocietyofTransplantation.AmJTransplant2004;4:51–8
Prophylaxisperiod(commonly90–100days)
HYBRID:Prophylaxis+Monitoring

Long-TermOutcomesofPreemptiveValganciclovirComparedwithValacyclovirProphylaxisforPreventionofCMVinRenal
Transplantation
JournaloftheAmericanSocietyofNephrologybyAmericanSocietyofNephrologyReproducedwithpermissionofAMERICANSOCIETYOFNEPHROLOGYintheformatRepublishincontinuingeducationmaterialsviaCopyrightClearanceCenter. 35

Cooking upahybridstrategybyDavide Abate

Hybrid Approaches Vary
• Inpre-emptivetherapy:• Surveillanceonceweeklyfor3- 4months• NAT-DNAemia atpositivethresholdà treatmentdose+/- reductionin
immunuosuppression forminimumof2weeksoftreatment.• Afterresolution,discontinueantiviralandcontinueweeklysurveillance.• SpecificthresholdsfordefiningoptimalPEThavenotyetbeendefined
• Useofsurveillanceafterprophylaxismaybeconsideredinpatientsconsideredatincreasedriskforpost-prophylaxisCMVdisease(e.g.,weeklyfor~8-12weeks).
• Specialgroups:• D+/R- patientsafterliver,heart,andpancreas3-6monthsdependingonthedegreeof
immunosuppression, includingantilymphocyte antibodiesforinduction.• D+/R- lungtransplantrecipients:6-12months.R+lungtransplantrecipients6months
prophylaxiswhileD+/R+areathigherriskfordevelopingCMVdisease.
• Limitedreportsdonotsupporttheroutineuseofsecondaryprophylaxis.

• ProspectivecohortstudyofconsecutiveCMV+SOTpatientsundergoingkidney,liver,liver–kidney)andhearttransplantation
• Lowrisk,R+,noanti-lymphocytedepletiontherapy• Testedevery2weeks(first100days)&every4weeks(day100-
180),~10-11testseach• Aviralloadof3983IU/ml*(2600copies/ml)wasestablishedas
theoptimalcut-off;99.6%NPV,sensitivity90%,specificity89%• AmajorityofpatientswillnotdevelopCMVdiseasewithout
specificantiviraltherapy(18of393incohort;15beforeday100)
• Limitations:can’tapplyifhigherrisk,ATGuse,differentISregimen 39

SpecialCases• Transplantrecipientsonmammaliantargetofrapamycin
(mTOR)inhibitorssuchassirolimus andeverolimusmayhavelowerratesofCMV;whetherthisshouldaltertheirpreventionstrategyisunknown.Effectisdose-dependent.
• TherearelimiteddatatosupporttheuseofCMVimmunoglobulin(CMVIg)forprophylaxiswhenappropriateantivirals aregiven.

Molecularmechanismsofanti-CMVeffectsofmTORinhibitors
• CMVeventsaftersolidorgantransplantationoccurredsignificantlymoreoftenunderCNIs(RR=2.27)thanwithrapamycin.
• mTOR-I+CNIvs.CNIalonein15trialsofkidney,heart,andlivertransplantationàhigherCMVincidencewhenpatientsreceivedanmTOR-Ifreeimmunosuppression(RR=2.45).

AllCMVIgG+@transplant;switched@6mos
prednisolone/MMFprednisolone/everolimus
prednisolone/CyA

mTOR Effectisdosedependent
AJT,11:2453–2462,November2011

CookingTreatmentRecommendations
TherapeuticMastersforCMV

Agent Route Target Toxicity Availability
Ganciclovir(GCV)
IV>>PO UL54,DNApolymerase
Marrow Yes
Valganciclovir(VGCV)
PO UL54,DNApolymerase
Marrow Yes
Foscarnet IV UL54,DNApolymerase
Renal,metabolic
Yes
Cidofovir(CDV)
IV UL54,DNApolymerase
Renal Yes
Brincidofovir(CMX001)
PO UL54,DNApolymerase
Less renalthanCDV
NotforCMV
Letermovir(AIC246)
PO/IV UL56, DNApackaging
Limited Experimental
Maribavir(MBV)
PO UL97, egress Limited Experimental
Anti-CMVAgents
NEWAGENTSWILLNOTCOVERHSV-VZVASWELLAS
VALGANCICLOVIR.

Therapy• WiththeuseofhighlysensitiveQNAT(LLOQ<200IU/ml),considerdiscontinuingtherapyafteroneresultislessthantheLLOQ.Confirmatorytestingshouldbedoneoneweekafterdiscontinuingtherapy.
• Iftheassayisnothighlysensitivethen2consecutiveundetectable(negative)resultsareneededtodiscontinuetherapy
• Drugresistanceshouldbesuspectedinpatientswithclinicaltreatmentfailuredespitegreaterthantwoweeksofantiviraltreatment

UL97Mutations
FoldchangeinganciclovirEC50a
Genotypefrequency
5-15x 2-5x <2x
Mostcommon M460V/I,H520Q,A594V,L595S,C603W
C592G
Lesscommonatcodons460,590-
607
M460T,A594G,595delb,L595F/W,E596Y,597del2b,
599del,K599T,600del,601del,601del2,C603R,C607Y,del(≥3)c
A591V,A594E/T,E596G,C603S,596delb,600del2,C607F
E596D,N597D,K599E/R,L600I,T601M,D605Ed
Atypicalloci F342Se,K355Me,V356Ge,V466Ge,C480Re,C518Y,P521Le
L405P,I610T,A613V M615V,Y617H,A619V,L634Q,E655K,A674T
(a)Moderateresistance(5-15x),low-graderesistance(2-5x),orinsignificantresistance(<2x)
(b)=inframedeletionofcodon
(c)Inframedeletionof≥3codons inthe590-607rangecanbeassumedtoconfermoderateganciclovirresistance(8- to15-fold).Deletionoflessthan3codonsmayconfervaryingdegreesofganciclovirresistance(4- to10-fold).
(d)D605E isabaselinesequencepolymorphismcommonineastAsia,unrelatedtodrugresistance
(e)Maribavircross-resistancedocumented,allexceptF342Saremarkedlygrowth-inhibited

AlgorithmforSuspectedCMVResistance
Kotton CN et al. UpdatedInternational Consensus Guidelines ontheManagementofCytomegalovirusinSolid-OrganTransplantation.Transplantation. 2013;96(4):333-360.
Genomesequence ofUL54andUL97
Caveats• Notallgenesaresequenced• Notallmutationsareknown• Notallmutationsareequal• Somemutationsassociatedwithdecreasedviralfitness• Polyclonalinfectionsarecommon
Kotton 2013

CMVUL54DNAPolymeraseMutations
Exo andregionVmutationsconferGCV-CDVcross-resistanceFOS-Rmutationsmayconferlow-gradeGCV±CDVcross-resistance
CrossResistance
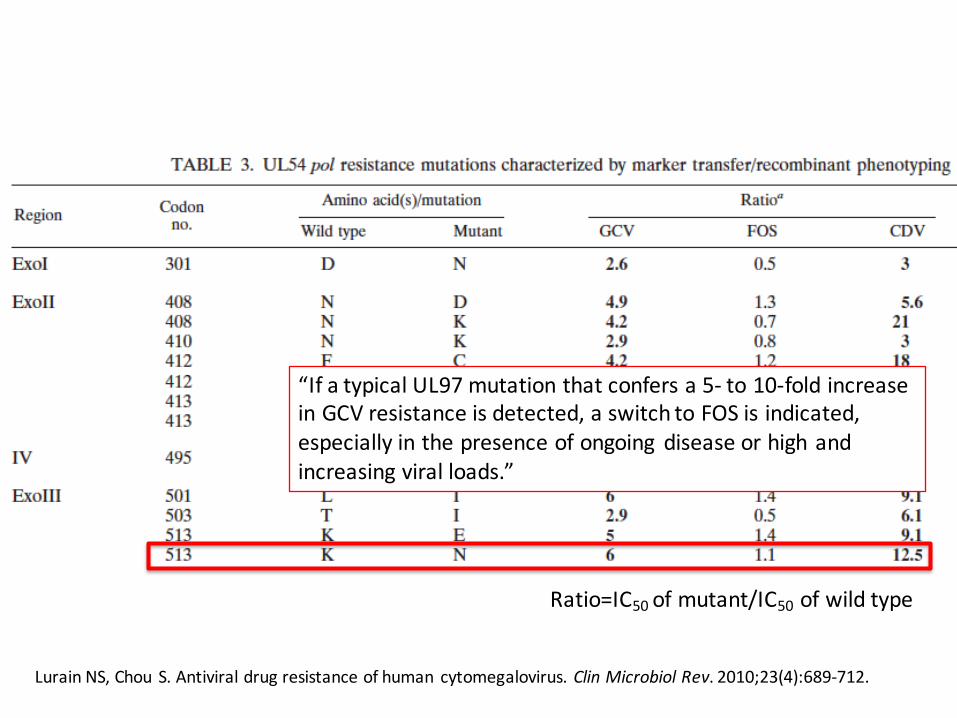
Lurain NS,Chou S.Antiviraldrugresistanceofhuman cytomegalovirus.Clin Microbiol Rev.2010;23(4):689-712.
Ratio=IC50 ofmutant/IC50 ofwildtype
“IfatypicalUL97mutationthatconfersa5- to10-foldincreaseinGCVresistanceisdetected,aswitchtoFOSisindicated,especiallyinthepresenceofongoing diseaseorhighandincreasingviralloads.”

Immunology• Serostatus isusefulbutreflectshighlyvariablepopulations
intermsofpredictionofriskforCMVinfection.• IgG hypogammaglobulinemia isassociatedwithanincreased
riskofCMVdiseaseaftertransplantation.Measurementoftotalimmunoglobulins issuggestedinsituationswhereCMVisdifficulttocontrol.
• CMV-specificcellularimmunemonitoringhasbeenshowntopredictCMVinfectioninthepre-transplantandpost-transplantsettingsinprospectiveobservational,multi-centerstudies.InterventionalstudiestodeterminepreciseclinicalutilityofCMIareongoing.
• CMVvaccinesareinpreclinical,phaseIandphaseIItrials.TheprimarygoalofaCMVvaccineshouldbetopreventormodulateCMVreplicationand/orCMVdisease.
• T-celltherapiesshouldbefurtherevaluatedforresistant/refractoryCMV.

PredictiveMarkers?• Serostatus basedriskstratification(i.e.D+ /R−,D+ /R+,D−/R+,andD−/R−)hidesasubstantialheterogeneityoftheindividualrisksforCMVreplicationandprogressiontoCMVdisease.• TheriskofCMVdiseaseamongD+ /R−patientsinthefirstyearposttransplant rangefrom6.4to58.3%whentheorganrecipientswereregroupedaccordingtoCMV-specificcell-mediatedimmunitytestingresultsattheendofantiviralprophylaxis.• Testsandmarkerscapableofindividualizing theriskofCMVreplicationmaysignificantlyimproveCMVpreventative strategies.

Cell-mediatedimmunitytopredictcytomegalovirusdiseaseinhigh-risksolidorgantransplantrecipients:LateonsetCMV.
• UtilityoftestingCD8+T-cellresponseagainstCMVasapredictoroflate-onsetCMVdiseaseafterastandardcourseofantiviralprophylaxis.108evaluablepatients(D+/R+n=39;D-/R+n=34;D+/R- n=35)ofwhom18(16.7%)developedsymptomaticCMVdisease.
• TestingusingtheQuantiFERON-CMVassayatbaseline,1,2and3monthsposttransplant (21-peptidepool).
• CMIwasdetectablein38/108(35.2%)patients(cutoff0.1IU/mLinterferon-gamma).
• CMVdiseaseoccurredin2/38(5.3%)patientswithadetectableinterferon-gammaresponseversus16/70(22.9%)patientswithanegativeresponse;p=0.038.
• InthesubgroupofD+/R- patients,CMVdiseaseoccurredin1/10(10.0%)patientswithadetectableinterferon-gammaresponse(cutoff0.1IU/mL)versus10/25(40.0%)patientswithanegativeCMI,p=0.12.
• MonitoringofCMImaybeusefulforpredictinglate-onsetCMVdisease KumarDetal.AmJTransplant.2009May;9(5):1214-22.

IFN-γ andCMVDisease
P=0.02
DetectableIFN-γ CD8+response
NoDetectableIFN-γ CD8+response
KumarD,etal.AmJTransplant. 2009;9:1214-1222.(B)
0 10 20 30 40 50 60 70 80 90 10050
60
70
80
90
100
Timeafterstoppingprophylaxis(days)
Free
domfrom
CMVdisease(%
)

Chemokines andImmuneControlofCytomegalovirusinOrganTransplantRecipients.
• CMVviremic organtransplantrecipients,chemokineexpression—specificallythechemokineCCL8(AUC0.84995%CI0.721–0.978;p = 0.003)andtheinterferon-γ inducedchemokineCXCL10(AUC0.841,95%CI0.707–0.974;p = 0.004)—wereassociatedwithcontrolofviralreplication.
• HomozygousTTpolymorphismintheCCL8promoter(SNPrs3138035)ofD+/R- transplantrecipientsconferredanincreasedriskofviralreplicationafterdiscontinuationofantiviralprophylaxis(hazardratio3.6;95%CI2.077–51.88).
• TheprimarycelltypeproducingCCL8inresponsetoCMVpeptidestimulationwasthemonocyte fractionwhereCCL8productionisassociatedwithspontaneousviralclearanceinpatientswithCMVviremia. Thereisdose-dependentreductioninCCL8productionwithimmunosuppression.Lisboa,L.F.etal.(2015),AmericanJournalofTransplantation.doi: 10.1111/ajt.13207

Virus-SpecificTcellAdoptiveTransfer
Ridell etalScience1992

Leen etalBlood2013Papadopoulou etal.Sci TransMed2014
• PBMCsfromHLAhomozygous,seropositivedonors• Generatedtrivalent(CMV,EBV,AdV)CD8Tcells• CreatingabankofreadytousevirusspecificCTLs
• Identified50patientswithrefractoryviralinfectionsafterSCT
• MatchedHLAofvirusspecificTcellswithpatients• AdoptivetransferofvirusspecificTcellsweekly• Subsequently havedevelopedpentavalent Tcells(CMV,
EBV,HHV6,AdV,BKV)

Valganciclovir
Valganciclovir ->Ganciclovir
HighdoseGanciclovir+Foscarnet
HighdoseFoscarnet
CMVTcells
UL54K513N
UL54A834P
CMVdiseaseafterSCT

MajorChanges• Biology:MechanismofCMVeffectonmacrophagefunctionappearstobeviainhibitionofinflammatorypathways.
• QNAT:increasedsensitivityà positiveinGIdiseaseandsinglenegativeassaymaybesufficientforstoppingtherapy
• Prophylaxisroutinein:– AllD+R-– D+orR+heartandlungs.
• Multiplenewdrugsà soon?• UseofCMV-specificT-celltherapymightaddressresistance.







