
Clinical Documentation Excellence: Transforming CDI to Meet Modern Challenges
Leigh Williams, MHIIM, RHIA, CPC, CPHIMS Administrator, Business Systems, UVA Health System
Today’s Agenda
• Data-Driven Documentation Maturity Model
• Clinical Documentation Excellence (CDE)
• Program Metrics and Outcomes
• Surgical Services
• Ambulatory Services
• Counterpoints
• 2015 Strategic Initiatives
• Discussion

The University of Mississippi Medical Center
• Academic medical center
• 6 hospitals including women’s, children’s, critical access, and community
• 500 physicians
• 125 specialties
• 100+ clinics
• 5 health sciences schools
CLINICAL DOCUMENTATION EXCELLENCE (CDE)

CDE Program Mission
• To guide our physicians to understanding and creating quality clinical documentation in the pay for performance era.
Data-Driven No Data Actionable Knowledge
Engagement None Engaged
CDE Program Driving Principles
Engage physicians in initiatives to improve pay-for-performance and revenue cycle metrics
Create solutions that support physicians in real-time within existing work flows
Improve inpatient and outpatient documentation accuracy, completeness, and timeliness
Drive improvement in quality outcomes measures and cash collections
CDE Program Goals
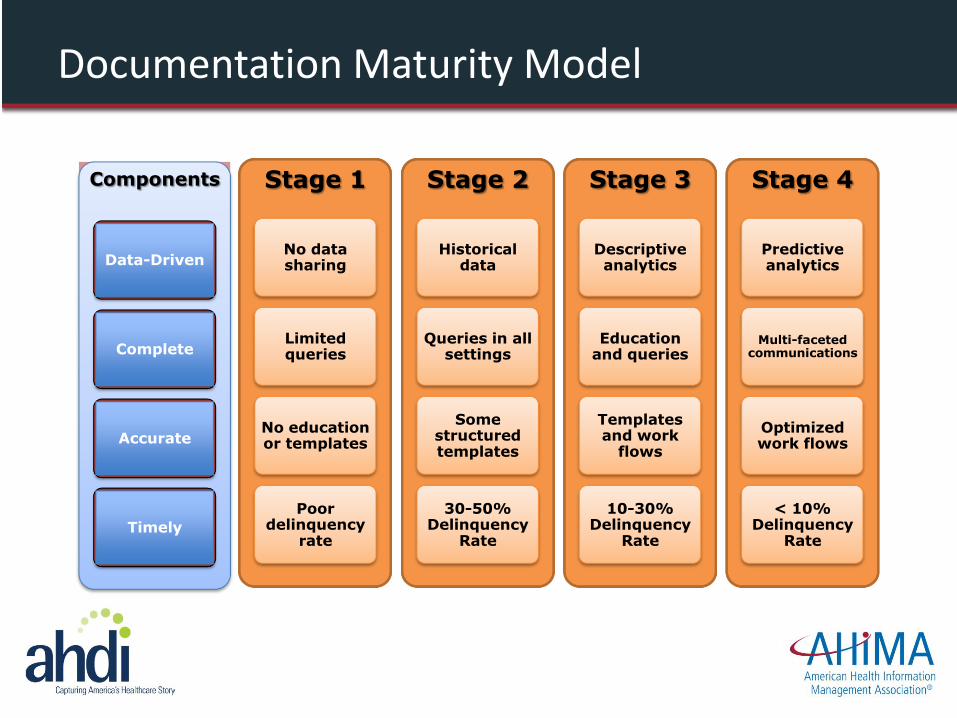
Stage 1
No data sharing
Limited queries
No education or templates
Poor delinquency
rate
Stage 2
Historical data
Queries in all settings
Some structured templates
30-50% Delinquency
Rate
Stage 3
Descriptive analytics
Education and queries
Templates and work
flows
10-30% Delinquency
Rate
Stage 4
Predictive analytics
Multi-faceted communications
Optimized work flows
< 10% Delinquency
Rate
Components
Data-Driven
Complete
Accurate
Timely
Documentation Maturity Model
Program Considerations
• Institute-wide: DRG and CPT based reimbursement
• ICD-10
• Meaningful Use and overall EHR adoption
• Hospital Value-Based Purchasing (VBP) Program
• Hospital Readmissions Reduction Program
• Hospital Acquired Conditions (HAC) Reduction Program
• Department-specific pain points
• Sustainable over years (not focused on one program)
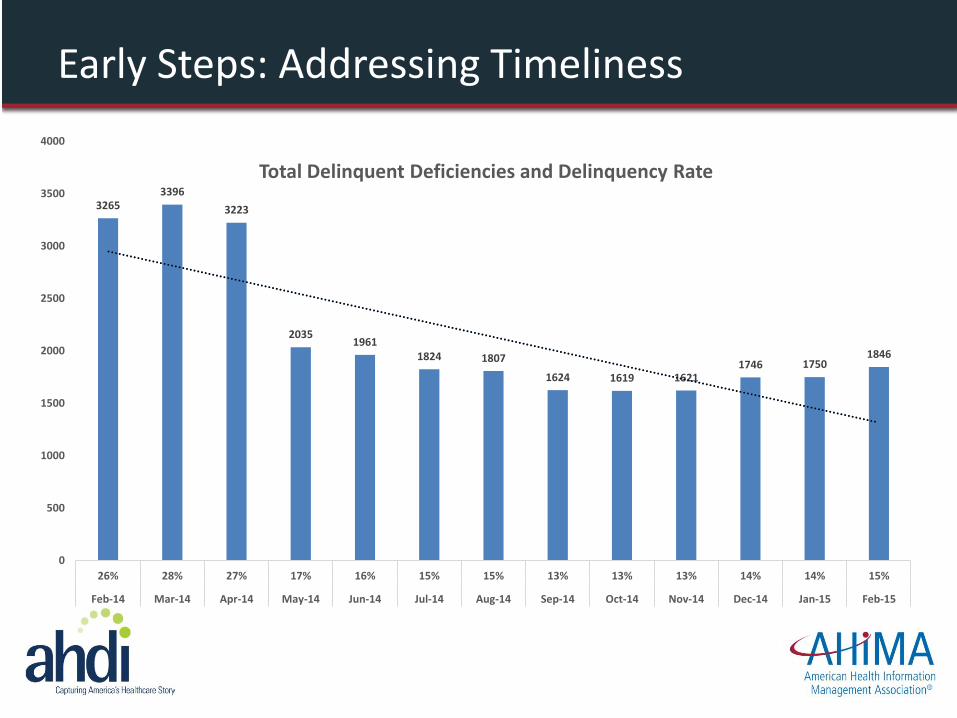
3265 3396
3223
2035 1961
1824 1807
1624 1619 1621 1746 1750
1846
0
500
1000
1500
2000
2500
3000
3500
4000
26% 28% 27% 17% 16% 15% 15% 13% 13% 13% 14% 14% 15%
Feb-14 Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15
Total Delinquent Deficiencies and Delinquency Rate
Early Steps: Addressing Timeliness

$0
$1,000,000
$2,000,000
$3,000,000
$4,000,000
$5,000,000
$6,000,000
$7,000,000
$8,000,000
$9,000,000
Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
Cash on Hold Due to Physician Deficiencies
Talking Impact on the Organization
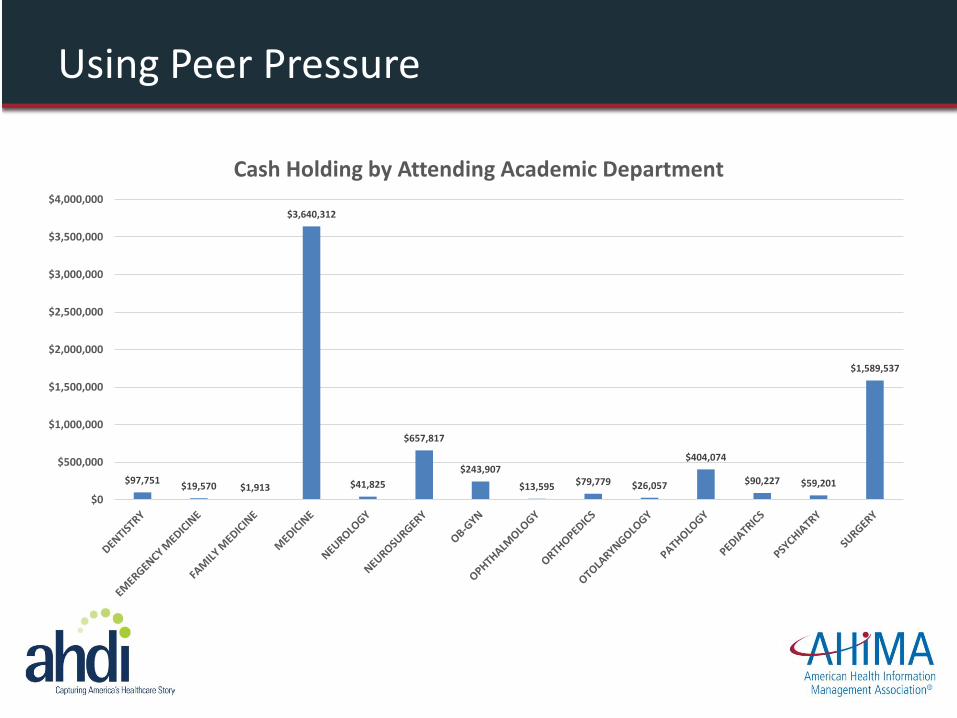
$97,751 $19,570 $1,913
$3,640,312
$41,825
$657,817
$243,907
$13,595 $79,779 $26,057
$404,074
$90,227 $59,201
$1,589,537
$0
$500,000
$1,000,000
$1,500,000
$2,000,000
$2,500,000
$3,000,000
$3,500,000
$4,000,000
Cash Holding by Attending Academic Department
Using Peer Pressure

Beginning the Program: Early Adopters
Neurosurgery
• Team includes department chairman, residency program director, CDI specialist, pro fee coder, and project manager
• Initiated November 2013
• Meets monthly
• Actively supports rounding with physicians and educational sessions
Orthopedics
• Team includes department chairman, residency program director, chief resident, surgeons, CDI specialist, pro fee coder, and project manager
• Initiated October 2013
• Meets monthly
• Actively supports rounding with physicians, educational sessions, grand rounds monthly education, intern program on business basics
Neurosurgery CDE
• Focus on inpatient documentation
• Deficiencies and delinquency rate
• Timely query responses
• Case Mix Index
• Unspecified diagnoses
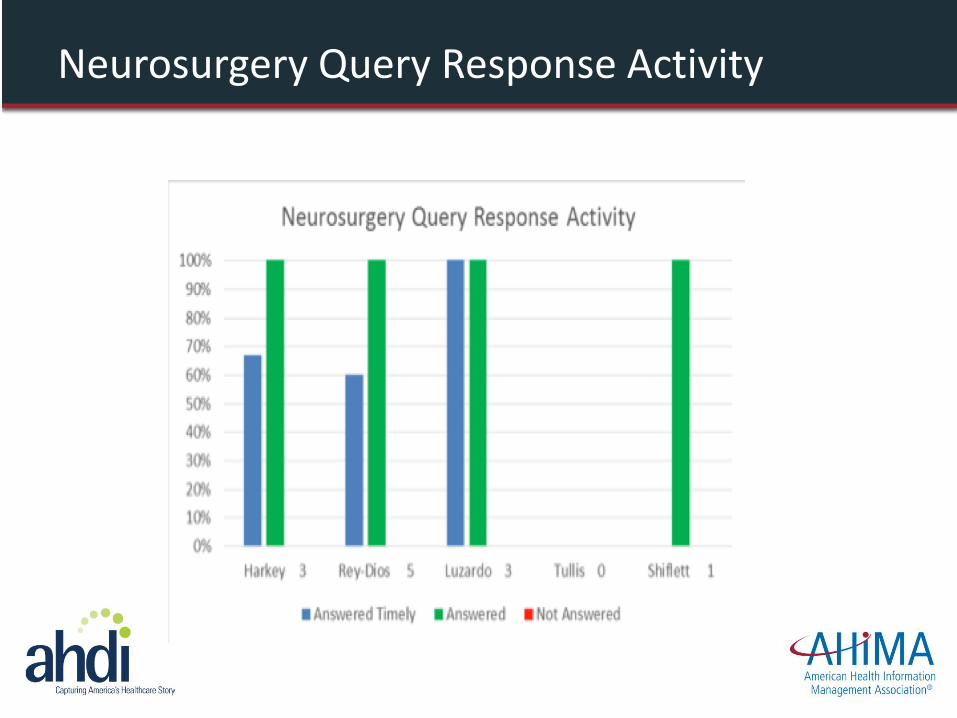
Neurosurgery Query Response Activity
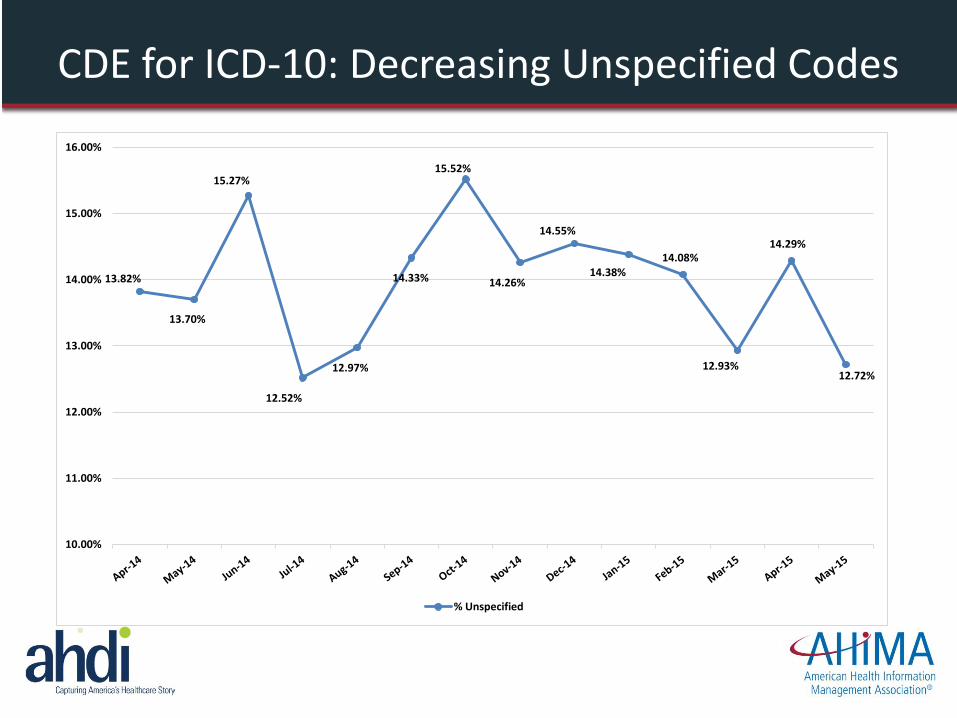
13.82%
13.70%
15.27%
12.52%
12.97%
14.33%
15.52%
14.26%
14.55%
14.38% 14.08%
12.93%
14.29%
12.72%
10.00%
11.00%
12.00%
13.00%
14.00%
15.00%
16.00%
% Unspecified
CDE for ICD-10: Decreasing Unspecified Codes
2.00
2.25
2.50
2.75
3.00
3.25
3.50
3.75
4.00 Ja
n-1
3
Feb
-13
Mar
-13
Ap
r-1
3
May
-13
Jun
-13
Jul-
13
Au
g-1
3
Sep
-13
Oct
-13
No
v-1
3
Dec
-13
Jan
-14
Feb
-14
Mar
-14
Ap
r-1
4
May
-14
Jun
-14
Jul-
14
Au
g-1
4
Sep
-14
Oct
-14
No
v-1
4
Dec
-14
Jan
-15
Feb
-15
Mar
-15
Ap
r-1
5
May
-15
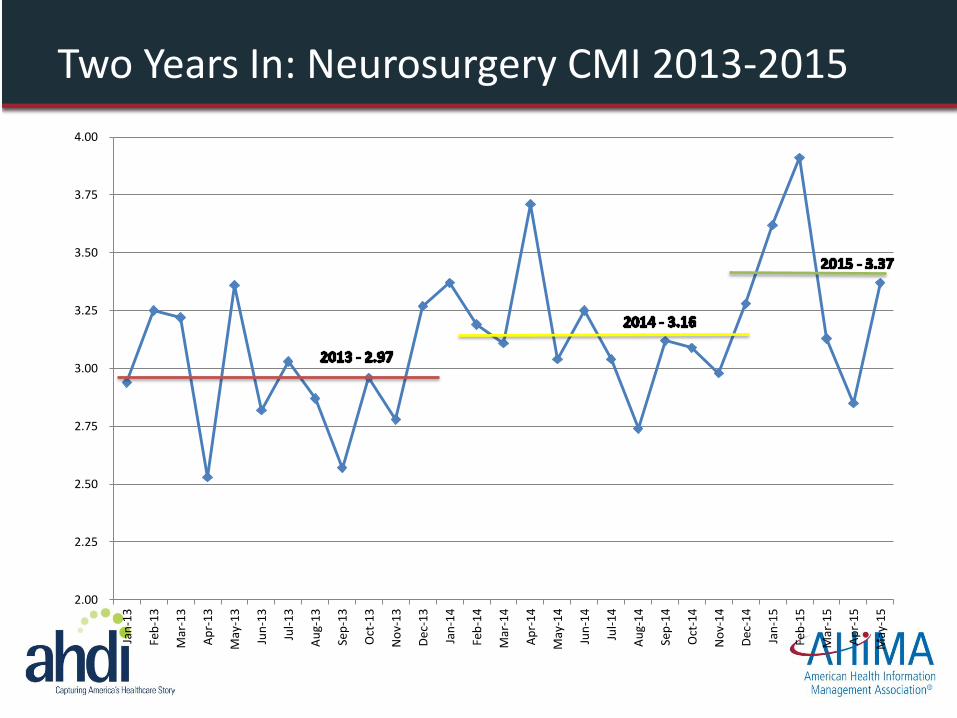
Two Years In: Neurosurgery CMI 2013-2015
Orthopedics CDE
• Full-blown program with inpatient and outpatient scope
• Deficiencies and delinquency rate
• Timely query responses
• Case Mix Index
• Unspecified diagnoses
• Physician business savvy / competency
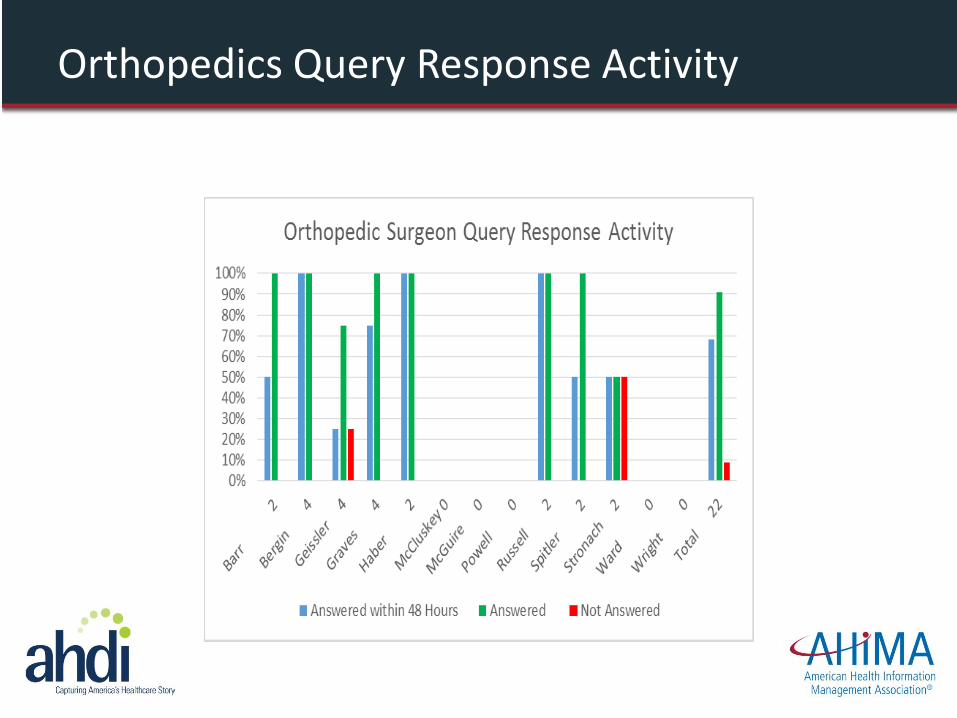
Orthopedics Query Response Activity
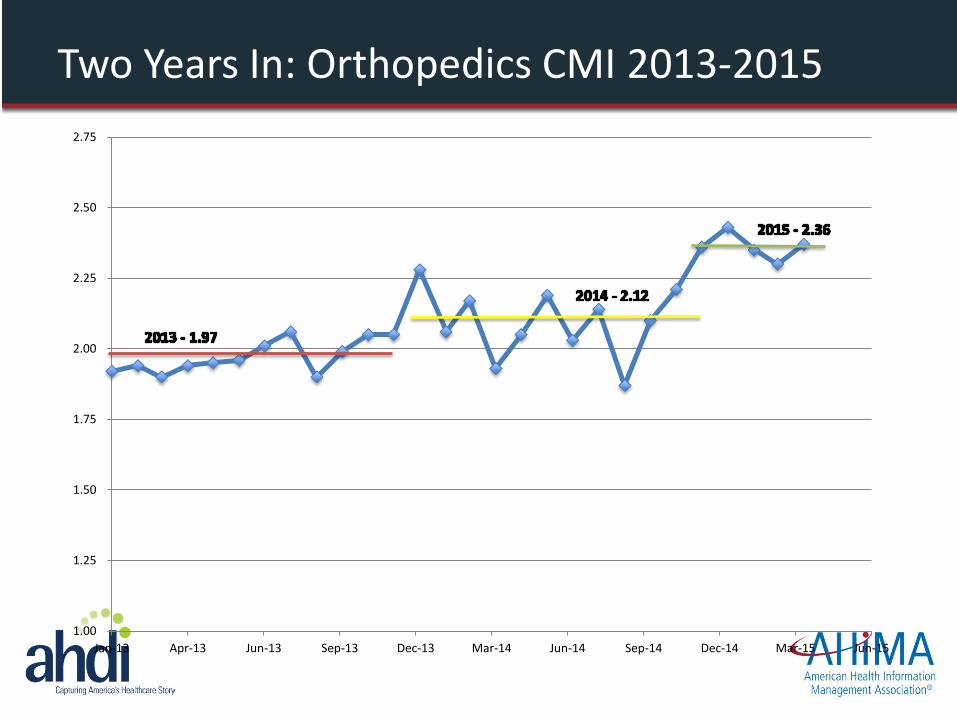
1.00
1.25
1.50
1.75
2.00
2.25
2.50
2.75
Jan-13 Apr-13 Jun-13 Sep-13 Dec-13 Mar-14 Jun-14 Sep-14 Dec-14 Mar-15 Jun-15
Two Years In: Orthopedics CMI 2013-2015
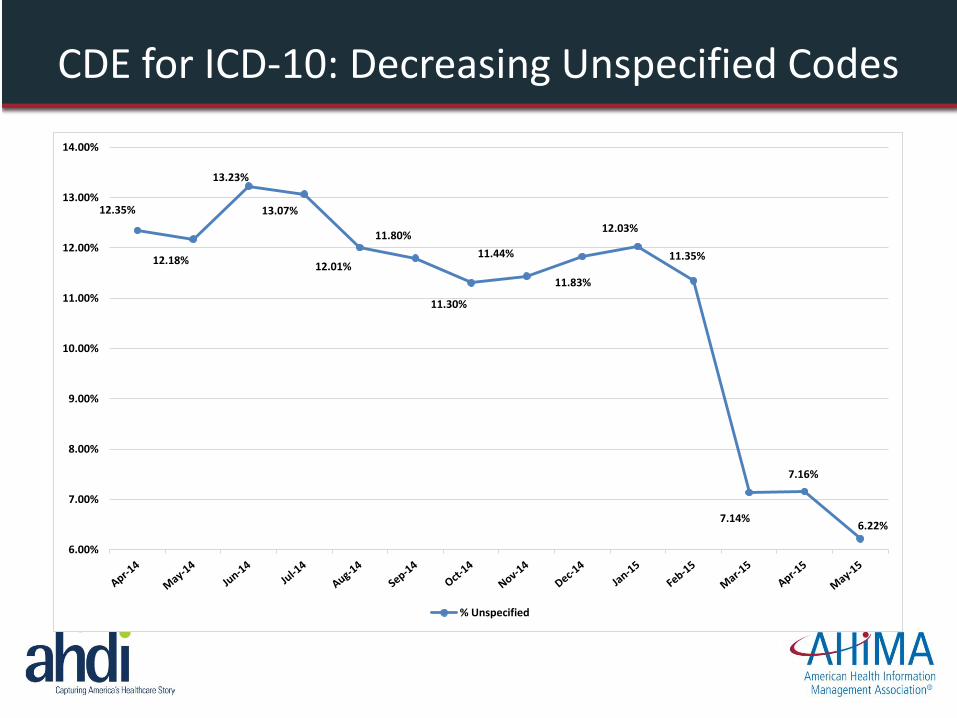
12.35%
12.18%
13.23%
13.07%
12.01%
11.80%
11.30%
11.44%
11.83%
12.03%
11.35%
7.14%
7.16%
6.22%
6.00%
7.00%
8.00%
9.00%
10.00%
11.00%
12.00%
13.00%
14.00%
% Unspecified
CDE for ICD-10: Decreasing Unspecified Codes
Family Medicine CDE
• Patient care focused: Primary care physician role, including when they’re in the hospital
• Open ambulatory encounter count
• Discharge summary deficiencies to drive timely Continuity of Care Documents
• Query response rate
• Unspecified diagnoses
Addressing Timeliness
• Open Encounters and Inpatient Deficiencies
• None more than 10 days
• 1 or 2 deficient discharge summaries, not yet delinquent
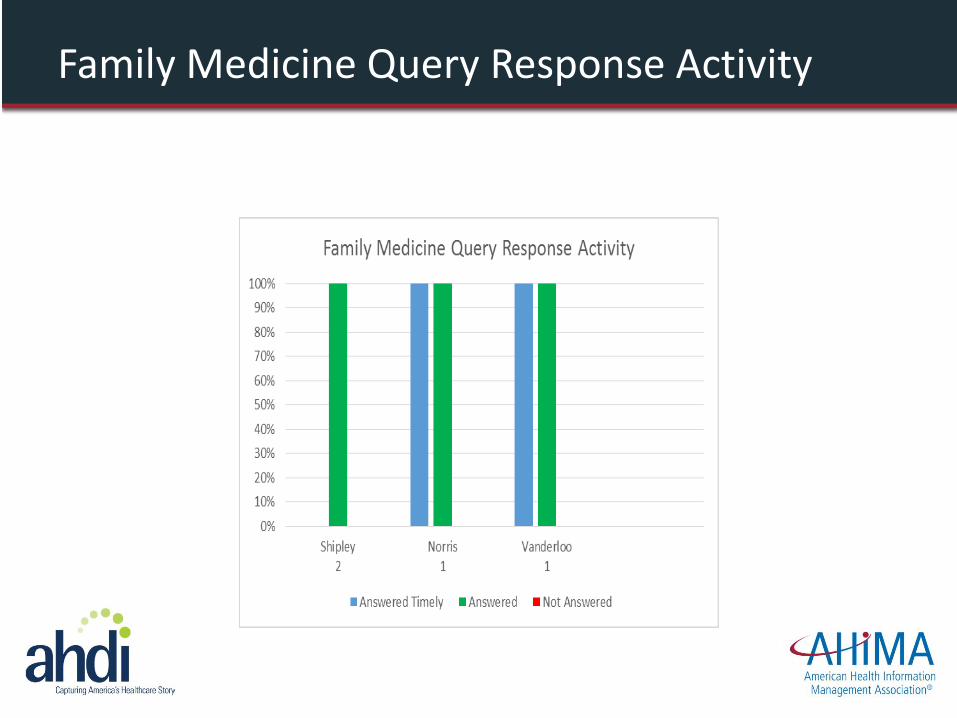
Family Medicine Query Response Activity
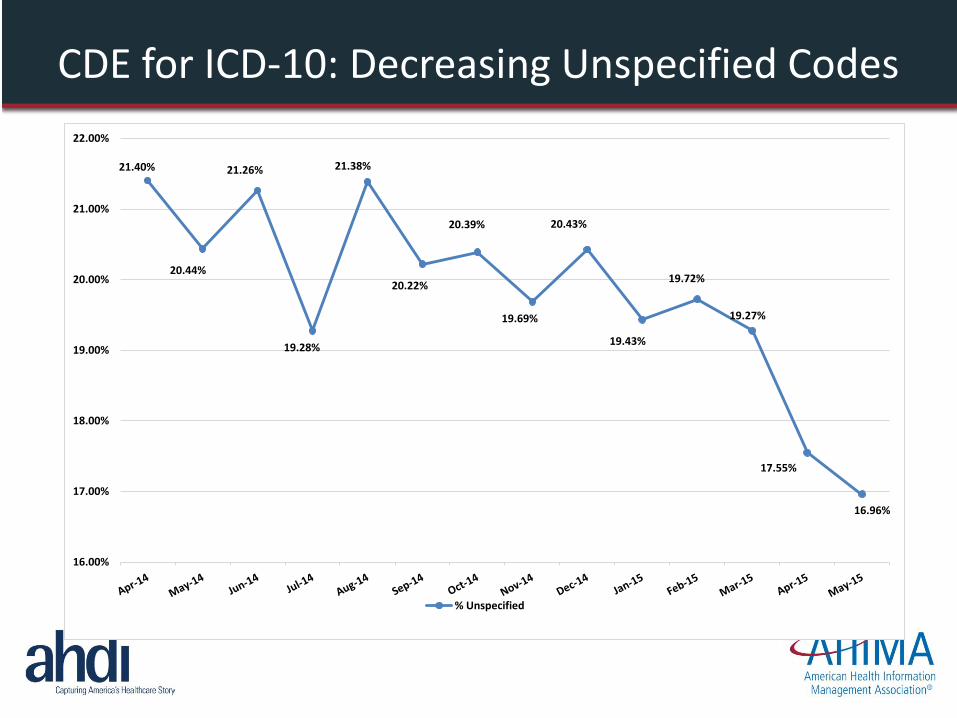
21.40%
20.44%
21.26%
19.28%
21.38%
20.22%
20.39%
19.69%
20.43%
19.43%
19.72%
19.27%
17.55%
16.96%
16.00%
17.00%
18.00%
19.00%
20.00%
21.00%
22.00%
% Unspecified
CDE for ICD-10: Decreasing Unspecified Codes
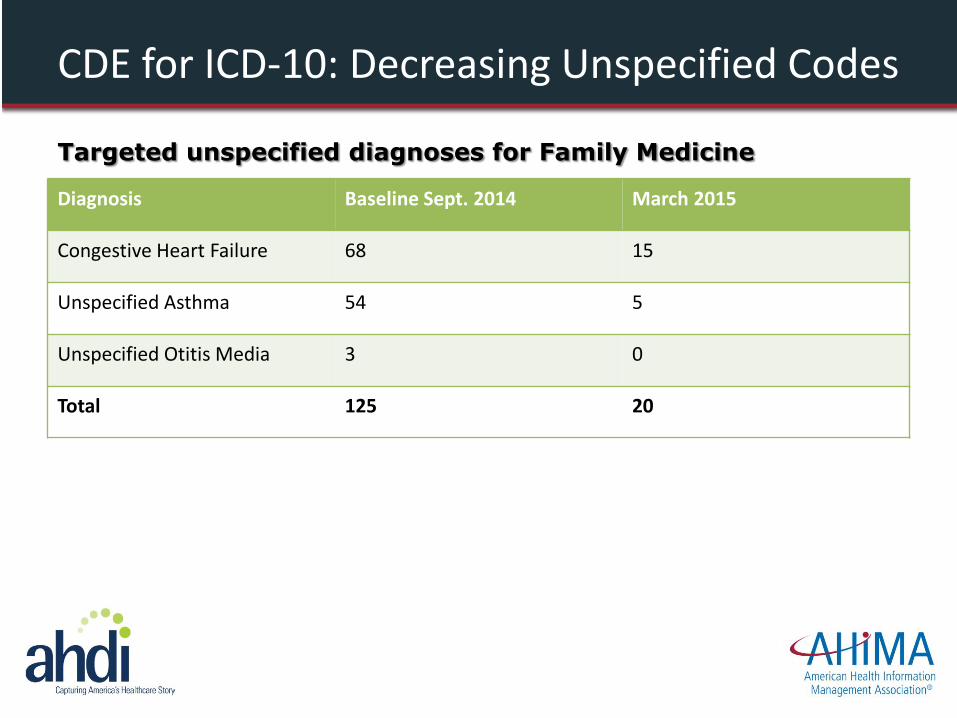
CDE for ICD-10: Decreasing Unspecified Codes
Diagnosis Baseline Sept. 2014 March 2015
Congestive Heart Failure 68 15
Unspecified Asthma 54 5
Unspecified Otitis Media 3 0
Total 125 20
Targeted unspecified diagnoses for Family Medicine
1.00
1.25
1.50
1.75
2.00
2.25
Jan-13 Apr-13 Jul-13 Oct-13 Feb-14 May-14 Aug-14 Dec-14 Mar-15 Jun-15
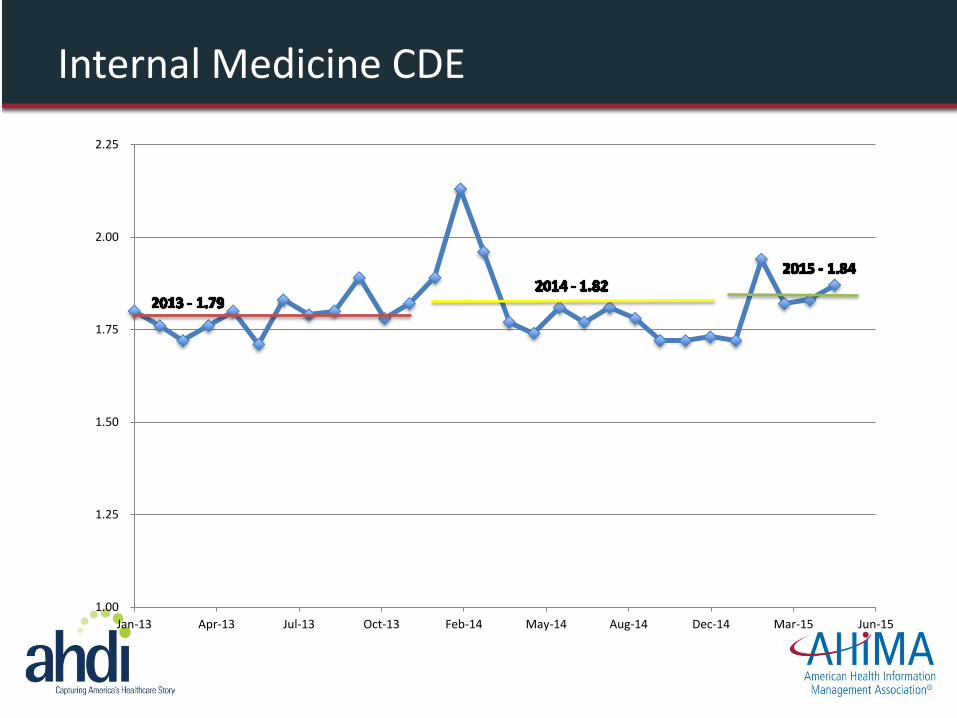
Internal Medicine CDE
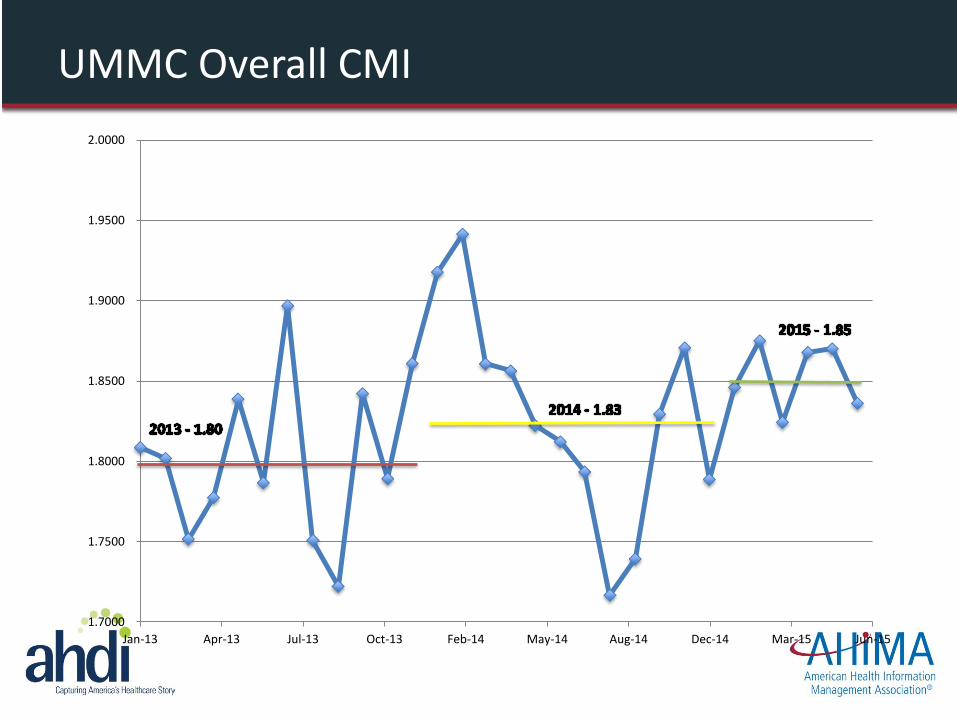
UMMC Overall CMI
1.7000
1.7500
1.8000
1.8500
1.9000
1.9500
2.0000
Jan-13 Apr-13 Jul-13 Oct-13 Feb-14 May-14 Aug-14 Dec-14 Mar-15 Jun-15
CDE in 2016 and Beyond: Future Focus
• Clinical intelligence
• Real-time feedback through EHR dashboards
• Concurrent coding
• Computer assisted physician documentation
• Computer assisted coding
• ICD-10 – diagnosis and problem list support tools
• Structured template development and adoption
Leigh Williams, MHIIM, RHIA, CPC, CPHIMS
Formerly Director, Revenue Cycle / Health Information
Management, The University of Mississippi Medical Center
Currently Administrator, Business Systems,
The University of Virginia Health System
@leightw
Discussion







