
1
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
WHAT HAVE LARGE TRIALS TAUGHT US ABOUT TREATING OSA?
Clete A. Kushida, M.D., Ph.D.Professor, Stanford University Medical Center
Medical Director, Stanford Sleep Medicine CenterDirector, Stanford Center for Human Sleep Research
Conflict of Interest DisclosuresClete A. Kushida, M.D., Ph.D., Professor, Stanford University
What Have Large Trials Taught Us About Treating OSA?
Type of Potential Conflict Details of Potential Conflict
Grant/Research Support ResMed, Pacific Medico
Consultant Philips-Respironics
Speakers’ Bureaus
Financial support
Other
Kaplan-Meier Survival Curves Across Sleep Apnea Severity
Marin JM, Lancet, 2005

2
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
Grote L, Hedner J, Peter JH. Mean blood pressure, pulse pressure and grade of hypertension in untreated hypertensive patients with sleep-related breathing disorder. J Hypertens 2001; 19:683–690.
OSA and HTN Severity CPAP and HTN
Sanner BM, Tepel M, Markmann A, et al. Effect of continuous positive airway pressure therapy on 24-hour blood pressure in patients with obstructive sleep apnea syndrome. Am J Hypertens 2002; 15:251–257.
A prospective study with automated ambulatory 24-hour BP monitoring reported a lower mean arterial BP at a 9 month follow-up period than at baseline in 40 of 52 patients with OSA started on CPAP therapy
CPAP and HTN (cont.)
Pepperell JC, et al. Ambulatory blood pressure after therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: a randomised parallel trial. Lancet 2002; 359:204–210.
CPAP and HTN (cont.)
Barbé F. Effect of Continuous Positive Airway Pressure on the Incidence of Hypertension and Cardiovascular Events in Nonsleepy Patients With Obstructive Sleep Apnea: A Randomized Controlled Trial. JAMA, 2012 May 23;307(20):2161-8
Cumulative incidence of hypertension or cardiovascular events for the intervention groups during follow-up, with/without CPAP group stratified according to adherence (<4 vs ≥4 h/night) and the P values for their incidence density ratios in reference to the control group.

3
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
Gotsopoulos H, Kelly JJ, Cistulli PA. Oral appliance therapy reduces blood pressure in obstructive sleep apnea: a randomized, controlled trial. Sleep 2004; 27:934–941.
OA and HTN
Reduction in daytime SBP and DBP and 24-hour DBP after treatment of OSA in 61 patients with a mandibular advancement splint for 4 weeks. MAS reduction in mean 24-hr DBP (1.8 ± 0.5 mmHg) vs. control (P = .001) but not in 24-hour SBP. Awake BP variables reduced with MAS, mean of 3.3 ± 1.1 mmHg SBP (P = .003) and 3.4 ± 0.9 mmHg DBP (P < .0001).
OA vs. CPAP and HTN
Mean differences from baseline in BP variables; CPAP (closed symbols) and MAD (open symbols) for 24-hr wake and sleep periods.
Top = all completers, n = 108; Bottom = HTN completers, n = 45
Phillips CL, Grunstein RR, Darendeliler MA, Mihailidou AS, Srinivasan VK, Yee BJ, Marks GB, Cistulli PA. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med. 2013;187(8):879-87.
Shibata N, Nishimura T, Hasegawa K, et al. Influence of sleep respiratory disturbance on nocturnal blood pressure.Acta Otolaryngol Suppl 2003; 550:32–35.
• A study found an improvement in blood pressure in proportion to the oxygen desaturation time in 31 patients with OSA after surgery.
• After surgery, an improvement in AHI of > 50% was noted in 19/31 patients (61.3%). Improvements in DT and change in BP were > 50% in 21/31 (67.7%) and 14/ 31 (45.2%) patients, respectively.
Surgery and HTN Contrasting Results
Barbe F, Mayoralas LR, Duran J, et al. Treatment with continuous positive airway pressure is not effective in patients with sleep apnea but no daytime sleepiness. A randomized, controlled trial. Ann Intern Med 2001; 134:1015–1023.
A multicenter, randomized, sham CPAP-controlled, parallel-group study of 55 SDB patients with an AHI ≥ 30, ESS ≤ 10, and normal average BP.
No significant effect of CPAP therapy on BP, when used for six weeks, was found.

4
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
• lack of a consistent definition for abnormal breathing events or non-standardized AHI cutoff across studies
• lack of proper randomization or inadequate blinding
• short or inadequate follow-up• Mixing of hypertensive/normotensive subjects
Contrasting Results (cont.)
Several factors may contribute to the contrasting results seen in some of these studies evaluating the effect of OSA treatment on BP:
OSA
C
C
?
?
NCF in OSA PatientsAuthor(Year)
Study Type
nOSA
SeverityConclusions
Barbé(2001)
RCT 29/25 severe no difference in Active vs. Sham CPAP groups for 8 A/P, L/M, and E/F tests
Bédard(1991)
CC 20/10mod-
severedecrease* in 7/9 A/P and 2/4 E/F tests; decrease* in 5/6 L/M tests (only severecases)
Cheshire(1992)
CS 29mod-
severecorrelation* between AHI and 1/2 EF tests and IQ decrease; no correlation in 3 A/P or1 L/M tests
Findley(1986)
CS 26 severedecrease* in 4/8 A/P, L/M, and E/F tests for hypoxemic vs. non-hypoxemic OSAsubjects
Greenberg(1987)
CC 14/14 severe decrease* in 7/14 A/P and E/F tests vs. controls
Ingram(1994)
CC 16/43mild-
severeno difference in OSA vs. controls subjects ≥ 54 yrs for 1 A/P test
Kim(1997)
CH 199/642mild-
severenegative association* between log AHI and psychomotor efficiency in 8 A/P, L/M, orE/F tests
Naëgelé(1995)
CC 17/17 severe decrease* in 1/4 A/P tests, 8/10 L/M tests, and 3/9 E/F tests vs. controls
Presty(1991)
CS 119mild-
severedecrease* in A/P and L/M tests for those OSA patients with severe hypoxia
Redline(1997)
CC 32/20mild-mod
decrease* in 1/4 A/P tests and 1/5 E/F tests; no difference in 3 L/M tests vs. controls
Telakivi(1993)
CS 31mild-
severeno correlation between hypoxia or sleepiness and 7 A/P, L/M, and E/F tests
Verstraeten(1996)
CC 26/22mild-
severeno differences in OSAS vs. insomnia subjects for 6 A/P, L/M, or E/F tests
*Significance Level: p < 0.05; Study Type: RCT = randomized control trial; CC = case-control, CH = cohort; CS = case series; n: cases/controls(if applicable); OSA Severity by average Apnea-Hypopnea Index (AHI), with mild = 5 - 15 events/hr, moderate = 15 - 30 events/hr, and severe> 30 events/hr; Test Type: A/P = tests of attention and psychomotor function, L/M = tests of learning and memory, E/F = tests of executive andfrontal-lobe function

5
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
APPLES
APPLES was a randomized, blinded, sham-controlled, multicenter trial of CPAP therapy, with these specific aims:
• To assess the long-term effectiveness of CPAP therapy on neurocognitive function, mood, sleepiness and quality of life
• To identify specific deficits in neurocognitive function associated with OSA
• To determine which deficits in neurocognitive function in OSA subjects are reversible and most sensitive to the effects of CPAP
• To develop multivariate composite indices to assess the clinical effectiveness of CPAP
• To use functional magnetic resonance imaging (fMRI) on a subset of OSA subjects
NHLBI-AppointedData and Safety
Monitoring Board (DSMB)
Data Coordinating Center
Co-Director, Operations (DO)Co-Director, Biostatistics (DB)
Co-Director, Data Management (DM)Clinical Trialist (CT)
APPLES Coordinator (AC)Quality Assurance/Control Supervisor (QS)
Database Administrator/Data Manager (DD)System Administrator (SA)Chief Neuropsychologist (N)
PSG Scorers (PS)
Clinical Coordinating Center
Principal Investigator (PI)Senior Advisor (SA)
Administrative Director (AD)Procurement Officer (PrO)
NHLBI Program Officer
Clinical Centers (5)
Clinical Center Director (D)Physician-Observer (PO)
Clinical Center Coordinator (C)Data Aide (DA)
PSG Technologists (PSGT)Psychometricians (PM)
Committees
TrainingQuality Assurance/Control
Publication and Presentation
Additional Protocol Review
Consultant Teams
MethodologySleep-Disordered Breathing
EEG/Neurocognitive FunctionMood and Sleepiness
AssessmentQuality of Life Assessment
Secondary Analysis-NC Team
Steering Committee
NHLBI Director
Study Organization
Stanford University, University of Arizona, St. Mary’s Medical Center, St. Luke’s Hospital, Brigham and Women’s Hospital
Inclusion Criteria• OSA as defined by the AASM Task Force OSA diagnostic criteria and a
respiratory disturbance index (RDI) ≥ 10 by polysomnography.
• Male or female gender
• Age ≥ 18 years
Key Exclusion Criteria• Prior treatment for OSA with CPAP or surgery.
• Any individual in the household currently on CPAP or on CPAP in the past.
• An oxygen saturation < 75 percent for > 10 percent of the diagnostic sleep study.
• A near-miss or prior automobile accident due to sleepiness within the past 12 months.
• Conditions, disorders, medications, or substances that could potentially affect neurocognitive function and/or alertness.
• A score ≤ 26 on the Mini Mental State Examination.
Inclusion / Exclusion Criteria
Secondary Outcomes Primary
Outcomes Neurocognitive Function
Daytime Sleepiness Mood Quality
of Life Demographic-
Physical
PN, BSRT, SWMT
SDC, SDCDR, PC, PASAT,
SAT, PVT, VSC, WASI, fMRI
MWT, ESS, SSS, FS
MINI, BDI-I,
POMS, HAM-D
SAQLI, QWB-
SA
age, sex, body mass index, hip,
waist, neck circumference,
pulse, blood pressure
Outcome Measures
PN = Pathfinder Number MWT = Maintenance of Wakefulness TestBSRT = Buschke Selective Reminding Test ESS = Epworth Sleepiness ScaleSWMT = Sustained Working Memory Test SSS = Stanford Sleepiness ScaleSDC = Symbol Digit Coding FS = Fatigue ScaleSDCDR = Symbol Digit Coding Delayed Recall MINI = Mini International Neuropsychiatric InterviewPC = Pathfinder Combined BDI-I = Beck Depression Inventory-IPASAT = Paced Auditory Serial Addition Task POMS = Profile of Mood StatesSAT = Shifting Attention Test HAM-D = Hamilton Rating Scale for DepressionPVT = Psychomotor Vigilance Task SAQLI = Calgary Sleep Apnea Quality of Life IndexVSC = Visual Sequence Comparison QWB-SA = Quality of Well-Being Scale, Self-AdministeredWASI = Wechsler Abbreviated Scale of IntelligencefMRI = Functional Magnetic Resonance Imaging

6
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
• One trial of a 2.5-minute task
• Test of attention, requiring the subject to scan a visual field to locate and connect numbers in sequence
• Measures number sequencing skills, ability to systematically apply an organizing principle, immediate memory, motor coordination, and visual scanning (A/P)
Variables:
PFNRTC, PFNACC, PFNPUT, PFNTOTL, PFNCOOR
CogScreen – PN(Trails A Computer Analogue)
• One trial of a 15-minute task
• Selective reminding test – after 1st trial, only the words not recalled are provided
• A word recalled on 1 trial, but not the next is said to represent “short-term retrieval” (L/M)
• A word remembered on 2 consecutive trials is said to have entered “long-term storage” (L/M)
Variables:
STR, LTR, RLTR, CLTR, LTS, SumRecall, DR TotalRecall
BSRT
• Three 11-minute blocks with 4-minute trials of a 1-back and 2-back working memory task
• Subject compares the spatial position of a stimulus with the position of the stimulus that occurred on a previous trial (E/F)
• Behavioral and EEG data are collected during performance, these measures are combined to yield a composite score indicating degree of change from baseline
Variables:
Activation, Alertness, Behavioral, and Overall Indices x 3
SWMT
456 Completed On-Treatment468 Completed On-Study
417 Completed On-Treatment432 Completed On-Study
427 Completed On-Treatment443 Completed On-Study
372 Completed On-Treatment403 Completed On-Study
102 Dropped for Any Reason9 Disqualified for Any Reason2 Died
126 Dropped for Any Reason11 Disqualified for Any Reason
2 Died
1098 Randomized & Analyzed
1516 Enrolled (CE, TS)
1224 DX PSG Visit
1105 Randomized (CT)
2 Excluded2 AHI <10 post-QC
5 Excluded4 Received both arms1 AHI <10 post-QC
112 Excluded for Any Reason7 Withdrawn for Any Reason
156 Excluded for Any Reason136 Withdrawn for Any Reason
558 Active CPAP 547 Sham CPAP
556 Active CPAP 542 Sham CPAP
2M-CPAP Visit 2M-CPAP Visit
6M-CPAP Visit 6M-CPAP Visit

7
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
Active CPAPMean (SD) or Count (%)
Sham CPAPMean (SD) or Count (%)
Randomization FactorsSex
Male (%) 363 (65.3) 356 (65.7)Female (%) 193 (34.7) 186 (34.3)
RaceWhite (%) 424 (76.3) 411 (75.8)Not White (%) 132 (23.7) 131 (24.2)
OSA SeverityMild OSA (%) 78 (14.0) 71 (13.1)Moderate OSA (%) 174 (31.3) 170 (31.4)Severe OSA (%) 304 (54.7) 301 (55.5)
DemographicsAge (y) 52.2 (12.2)* 50.8 (12.2)*Married (%) 325 (58.5) 309 (57.0)BMI (kg/m2) 32.4 (7.3) 32.1 (7.0)Highest Grade Level (y) 15.50 (2.6) 15.50 (2.6)WASI Full-4 IQ 112.1 (12.7) 112.0 (13.3)WASI Verbal IQ 110.0 (12.8) 110.0 (13.9)WASI Performance IQ 111.6 (13.5) 111.4 (13.0)
Baseline DataActive CPAPMean (SD)
Sham CPAPMean (SD)
Sleep StudyTotal Sleep Time (min) 375.4 (66.6) 378.3 (63.8)Sleep Efficiency (%) 78.2 (13.3) 78.4 (12.2)Sleep Latency (min) 18.8 (22.4) 19.0 (21.4)REM Latency (min) 137.0 (83.6) 137.6 (82.9)Stage 1 (% of TST) 18.8 (14.3) 18.9 (14.6)Stage 2 (% of TST) 60.7 (13.3) 60.3 (13.8)Stage 3 (% of TST) 2.4 (4.6) 2.6 (5.0)Stage 4 (% of TST) 0.5 (2.0) 0.6 (2.0)Stage REM (% of TST) 17.4 (7.2) 17.6 (6.9)
Apnea Hypopnea Index 39.7 (24.9) 40.6 (25.6)
Minimum O2SAT - Sleep (%) 81.0 (7.6) 80.8 (8.5)O2SAT<85% (% of TST) 2.2 (6.1) 2.3 (6.3)
Baseline Data
Active n = 556Sham n = 542p = 0.5122
Active n = 454Sham n = 420p < 0.0001*
Active n = 442Sham n = 398p < 0.0001*
AHI Means
DX 2M 6M
Per-Protocol GEE of PFN

8
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
Covariates
• Gender
• Race (white vs. non-white)
• OSA severity (mild, moderate, severe)
• %TST O2<85
• Age <60 years
• WASI verbal IQ and performance IQ
Visits/OSA SeverityActive CPAP:
Mean Estimate(95% CI LB-UB)
Sham CPAP:Mean Estimate(95% CI LB-UB)
P Value
2M(Active n = 437; Sham n = 394)
0.035(-0.019 – 0.090)
-0.074(-0.133 – -0.015)
0.0074*
6M(Active n = 426; Sham n = 374)
0.072(0.012 – 0.132)
0.018(-0.046 – 0.082)
0.2254
COVARIATE-Adjusted
2M(n = 828)
Mild OSA-0.017
(-0.152 – 0.119)0.011
(-0.135 – 0.157)0.7834
Moderate OSA0.016
(-0.087 – 0.120)-0.032
(-0.128 – 0.064)0.4950
Severe OSA0.054
(-0.017 – 0.125)-0.112
(-0.197 – -0.028)0.0031*
6M(n = 796)
Mild OSA0.023
(-0.132 – 0.177)-0.046
(-0.216 – 0.123)0.5515
Moderate OSA0.017
(-0.086 – 0.121)0.008
(-0.108 – 0.125)0.9101
Severe OSA0.113
(0.031 – 0.195)0.039
(-0.046 – 0.124)0.2176
GLMM: SWMT Overall Mid-Day Index
Sham CPAP = 3.4 Hours
Active CPAP = 4.2 Hours
Mean Hours of Nightly CPAP
P < 0.001*
Active CPAP Sham CPAP76,770 days 69,807 days
Adherence
Baseline features associated with better adherence:
• Increased age
• Higher IQ
• White ethnicity
• Being married
• Poorer sleep quality (e.g., decreased sleep efficiency, longer sleep latency, longer REM latency)

9
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
Variable Category
Number of
VariablesVariables
Demographics 11 Age, BMI, Married, WASI Full-4 IQ, WASI Verbal IQ, WASI Performance IQ,Highest Grade Level, MMSE Total Score, Ethnicity, Study Arm, Site
Health Variables
33
Caffeine Servings/Wk, Alcohol Servings/Wk, Current Smoker, CV History, AM Headaches, Dry Mouth/ Throat, Bruxism, Nasal Congestion, Hypertension,
Asthma, COPD, GERD, Chronic Pain Syndrome, Thyroid Disease, Diabetes, Eczema, Anemia, 5 Year
Weight Gain >20 Lbs, Allergic Rhinitis, Depression, Anxiety, Rhinoplasty, Cancer, Smoker, Claustrophobia, Neck Circumference, Nose Exam, Oral/Throat Exam,
Coughing/Wheezing, Shortness of Breath, Pain in Joints/Muscles/Back, Leg Cramps/Jerks, Need to Go to Bathroom
Sleep Variables
38
AHI TST, AHI NREM, AHI REM, O2 Sat<85%TST, Avg SpO2 NREM, Avg SpO2REM, Min SpO2, Hrs Sleep/Night, Snore Duration, TIB, TST, Sleep Efficiency, SO after LO, %TSTS3, %TSTS4, %REM, Arousal Index, PLM Index, OA Index, CA
Index, MA Index, Hypopnea Index, Avg SpO2 Wake, Desaturation Index, Number of Awakenings, Naps/Wk, Difficulty
Rising, EDS, Trouble Falling Asleep, Difficulty Falling Back to Sleep at Night, Difficulty Falling Back to Sleep in AM, Pain Affects Sleep, Worry About Sleep,
Unrested During Day, Not Enough Sleep, Noisy Surroundings, MEQ Total Score, MEQ Category
Neurocognitive 3 PVT Median RT, PVT Mean Slowest 10% of RTs, PASAT Total Correct
Mood 9 HAM-D Total Score, POMS TMD, POMS Factor F, POMS Factor T, POMS Factor D, POMS Factor A, POMS Factor C, POMS Factor V, BDI Total Score
Sleepiness 3 MWT Mean Sleep Latency, ESS Total Score, SSS Mean Score
Quality of Life 5 SAQLI Total Score, SAQLI Domain A Mean, SAQLI Domain B Mean, SAQLI Domain C Mean, SAQLI Domain D Mean
Possible Confounders
CPAP Adherence-Adjusted Primary Neurocognitive Outcomes
CPAP Study Arm
NC Mean Estimate (95% CI LB - UB)
Lower 3 Quartiles for %TSTO2 <85
NC Mean Estimate (95% CI LB - UB) Upper Quartile for
%TSTO2 <85
P Value
CogScreen Pathfinder Number Total Time
DXActive CPAP 24.05 (23.46 – 24.64) 26.80 (25.59 – 28.02) <0.0001*Sham CPAP 24.49 (23.83 – 25.15) 24.36 (23.36 – 25.36) 0.9572
2MActive CPAP 24.77 (23.99 – 25.54) 26.78 (25.36 – 28.20) 0.0043*Sham CPAP 24.41 (23.70 – 25.12) 23.70 (22.67 – 24.74) 0.5405
6MActive CPAP 24.19 (23.52 – 24.87) 27.40 (25.85 – 28.95) <0.0001*Sham CPAP 24.40 (23.67 – 25.13) 24.35 (23.01 – 25.69) 0.8879
BSRT Sum Recall
DXActive CPAP 49.93 (49.05 – 50.81) 49.07 (47.52 – 50.62) 0.3357Sham CPAP 50.12 (49.23 – 51.02) 49.09 (47.60 – 50.58) 0.2545
2MActive CPAP 52.87 (52.00 – 53.75) 50.68 (48.92 – 52.43) 0.0208*Sham CPAP 52.10 (51.07 – 53.13) 51.52 (49.90 – 53.14) 0.5561
6MActive CPAP 54.47 (53.56 – 55.38) 52.95 (51.20 – 54.69) 0.1108Sham CPAP 54.31 (53.30 – 55.32) 54.18 (52.63 – 55.73) 0.8928
SWMT Overall Mid-day
2MActive CPAP 0.003 (-0.061 – 0.066) 0.132 (0.023 – 0.242) 0.0448*
Sham CPAP-0.079 (-0.146 – -
0.013)-0.057 (-0.173 –
0.059)0.7411
6MActive CPAP 0.070 (0.001 – 0.139) 0.079 (-0.040– 0.198) 0.9010
Sham CPAP0.005 (-0.069 – 0.078) 0.058 (-0.070 –
0.187)0.4785
Primary NC by O2 Quartiles Secondary NC Variables
SWMT – Mid-day Behavioral Index
Active CPAP Mean Estimate (95% CI LB-UB)
Sham CPAP Mean Estimate (95% CI LB-UB)
P Value
2M (n = 843)
Mild OSA 0.180 (0.006 – 0.355) 0.104 (-0.074 – 0.283) 0.5419Moderate OSA 0.137 (0.035 – 0.238) 0.126 (0.007 – 0.245) 0.8900
Severe OSA 0.205 (0.117 – 0.294) -0.011 (-0.128 – 0.106) 0.0031*
6M (n = 815)Mild OSA 0.143 (-0.072 – 0.357) 0.116 (-0.123 – 0.356) 0.8703
Moderate OSA 0.194 (0.062 – 0.325) 0.314 (0.191 – 0.437) 0.1838Severe OSA 0.321 (0.212 – 0.430) 0.173 (0.052 – 0.295) 0.0739
SWMT – Mid-day Activation Index
2M (n = 815)Mild OSA -0.050 (-0.268 – 0.169) 0.317 (0.031 – 0.603) 0.0450*
Moderate OSA 0.262 (0.084 – 0.440) 0.170 (0.006 – 0.334) 0.4512Severe OSA -0.003 (-0.109 – 0.103) 0.033 (-0.093 – 0.159) 0.6672
6M (n = 787)Mild OSA 0.157 (-0.089 – 0.403) 0.118 (-0.117 – 0.353) 0.8197
Moderate OSA 0.016 (-0.131 – 0.162) 0.014 (-0.188 – 0.216) 0.9890 Severe OSA 0.058 (-0.068 – 0.185) 0.123 (-0.016 – 0.262) 0.5029
10
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
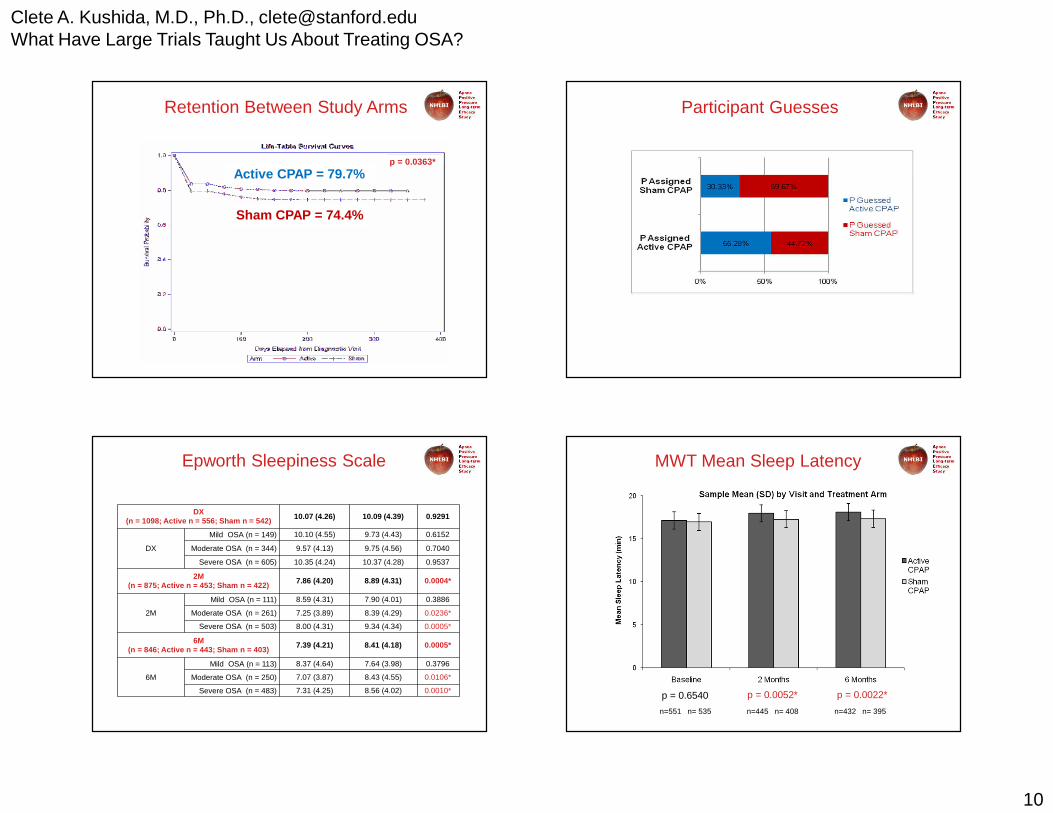
Active CPAP = 79.7%
Sham CPAP = 74.4%
p = 0.0363*
Retention Between Study Arms Participant Guesses
Epworth Sleepiness Scale
DX (n = 1098; Active n = 556; Sham n = 542) 10.07 (4.26) 10.09 (4.39) 0.9291
DX
Mild OSA (n = 149) 10.10 (4.55) 9.73 (4.43) 0.6152
Moderate OSA (n = 344) 9.57 (4.13) 9.75 (4.56) 0.7040
Severe OSA (n = 605) 10.35 (4.24) 10.37 (4.28) 0.9537
2M (n = 875; Active n = 453; Sham n = 422)
7.86 (4.20) 8.89 (4.31) 0.0004*
2M
Mild OSA (n = 111) 8.59 (4.31) 7.90 (4.01) 0.3886
Moderate OSA (n = 261) 7.25 (3.89) 8.39 (4.29) 0.0236*
Severe OSA (n = 503) 8.00 (4.31) 9.34 (4.34) 0.0005*
6M(n = 846; Active n = 443; Sham n = 403)
7.39 (4.21) 8.41 (4.18) 0.0005*
6M
Mild OSA (n = 113) 8.37 (4.64) 7.64 (3.98) 0.3796
Moderate OSA (n = 250) 7.07 (3.87) 8.43 (4.55) 0.0106*
Severe OSA (n = 483) 7.31 (4.25) 8.56 (4.02) 0.0010*
MWT Mean Sleep Latency
p = 0.0052* p = 0.0022*p = 0.6540
n=551 n= 535 n=445 n= 408 n=432 n= 395

11
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
MWT-MSL ≤ 14.5Active CPAP P Value Sham CPAP P Value
CogScreen Pathfinder Number – Total Time
2MSpearman Correlation Coefficient (∆ MWT-MSL vs. ∆ PFN-TOTL)
0.0322n = 101
0.74940.1197n = 85
0.2754
6MSpearman Correlation Coefficient (∆ MWT-MSL vs. ∆ PFN-TOTL)
-0.1629n = 101
0.10350.1239n = 83
0.2643
BSRT – Sum Recall
2MSpearman Correlation Coefficient
(∆ MWT-MSL vs. ∆ BSRT-SR)
-0.0894n = 101
0.37400.0109n = 85
0.9214
6MSpearman Correlation Coefficient
(∆ MWT-MSL vs. ∆ BSRT-SR)
-0.1356n = 101
0.17640.1108n = 82
0.3216
SWMT – Mid-day Overall Index
2MSpearman Correlation Coefficient (∆ MWT-MSL vs. ∆ SWMT-OMD)
0.2084n = 98
0.0395*0.0774n = 80
0.4948
6MSpearman Correlation Coefficient (∆ MWT-MSL vs. ∆ SWMT-OMD)
0.1598n = 95
0.12190.1015n = 78
0.3766
For Participants with MWT-MSL ≤14.5, Correlation between Change in MWT-MSL vs. Change in Primary Neurocognitive Outcome by Visit and Study Arm
?• The detection of CPAP effects for only the primary E/F
variable suggests this test is a more sensitive measure for subtle neurocognitive changes, combining a cognitive task with simultaneous EEG measures of brain function.
• Lower levels of oxygen saturation and increased sleepiness had an association with this primary E/F variable.
• However, these effects were only detected at 2 months and were minor compared to effects of caffeine and diphenhydramine for this measure in other studies.
Individual Variability and Cognitive Reserve
• Individual variability: Deficits in NCF may vary significantly among individuals independent of sleep history and may involve a trait-like differential yet stable vulnerability to impairment from sleep loss, of which the neurobiological correlates are presently unidentified.1
• The concept of cognitive (or brain) reserve may be important; the neural effect of sleep loss may be mediated through cognitive reserve, so that individuals with more reserve are able to withstand a greater insult before performance is detrimentally affected.2
1Van Dongen HPA et al. Systematic interindividual differences in neurobehavioral impairment from sleep loss: Evidence of trait-likedifferential vulnerability. Sleep. 2004; 27(3):423-33. 2Van Dongen HP. Brain activation patterns and individual differences in working memory impairment during sleep deprivation. Sleep. 2005 Apr 1;28(4):386-8.
Limitations
Could these factors collectively result in less susceptibility to the neurocognitive effects of OSA and a subsequent reduced response to treatment?

12
Clete A. Kushida, M.D., Ph.D., [email protected] Have Large Trials Taught Us About Treating OSA?
Key Issues and Future Research
• OSA is a multifaceted disorder with many comorbidities and outcomes; we believe that the mixed results from prior studies and the limited effect of CPAP on E/F measures of neurocognition in this study suggest the existence of a complex OSA-neurocognitive relationship.
• Clinicians should consider disease severity, sleepiness, and individual differences (variability and cognitive reserve) including treatment adherence in managing their OSA patients with CPAP.
• We need more large-scale studies (e.g., APPLES, CATNAP)
• Sleep-neurocognitive expert teams need to further evaluate these and other test batteries (e.g., CANTAB, Mindstreams, CNS Vital Signs [CNSVS]) to select the most relevant tests and variables for each major sleep area of study
ComparativeOutcomesManagement withElectronic DataTechnology
ACKNOWLEDGEMENTS
APPLES was funded by contract 5UO1-HL-068060 from the National Heart, Lung and Blood Institute. The APPLES pilot studies were supported by grants from the American Academy of Sleep Medicine and the Sleep Medicine Education and Research
Foundation to Stanford University and by the National Institute of Neurological Disorders and Stroke (N44-NS-002394) to SAM Technology. APPLES investigators gratefully recognize the vital input and support of Dr. Sylvan Green who died before the results of
this trial were analyzed, but was instrumental in its design and conduct.
ADMINISTRATIVE COREClete A. Kushida, MD, PhD; Deborah A. Nichols, MS; Eileen B. Leary, BA, RPSGT; Pamela R. Hyde, MA; Tyson H. Holmes, PhD;
Daniel A. Bloch, PhD; William C. Dement, MD, PhD
DATA COORDINATING CENTER Daniel A. Bloch, PhD; Tyson H. Holmes, PhD; Deborah A. Nichols, MS; Rik Jadrnicek, Microflow, Ric Miller, Microflow, Usman Aijaz,
MS; Aamir Farooq, PhD; Darryl Thomander, PhD; Chia-Yu Cardell, RPSGT; Emily Kees, Michael E. Sorel, MPH; Oscar Carrillo, RPSGT; Tami Crabtree, MS; Booil Jo, PhD; Ray Balise, PhD; Tracy Kuo, PhD
CLINICAL COORDINATING CENTERClete A. Kushida, MD, PhD, William C. Dement, MD, PhD, Pamela R. Hyde, MA, Rhonda M. Wong, BA, Pete Silva, Max Hirshkowitz,
PhD, Alan Gevins, DSc, Gary Kay, PhD, Linda K. McEvoy, PhD, Cynthia S. Chan, BS, Sylvan Green, MD
CLINICAL CENTERS
Stanford UniversityChristian Guilleminault, MD; Eileen B. Leary, BA, RPSGT; David Claman, MD; Stephen Brooks, MD; Julianne Blythe, PA-C, RPSGT; Jennifer Blair, BA; Pam Simi, Ronelle Broussard, BA; Emily Greenberg, MPH; Bethany Franklin, MS; Amirah Khouzam, MA; Sanjana
Behari Black, BS, RPSGT; Viola Arias, RPSGT; Romelyn Delos Santos, BS; Tara Tanaka, PhD
University of ArizonaStuart F. Quan, MD; James L. Goodwin, PhD; Wei Shen, MD; Phillip Eichling, MD; Rohit Budhiraja, MD; Charles Wynstra, MBA; Cathy Ward, Colleen Dunn, BS; Terry Smith, BS; Dane Holderman, Michael Robinson, BS; Osmara Molina, BS; Aaron Ostrovsky,
Jesus Wences, Sean Priefert, Julia Rogers, BS; Megan Ruiter, BS; Leslie Crosby, BS, RN
St. Mary Medical CenterRichard D. Simon Jr., MD; Kevin Hurlburt, RPSGT; Michael Bernstein, MD; Timothy Davidson, MD; Jeannine Orock-Takele, RPSGT;
Shelly Rubin, MA; Phillip Smith, RPSGT; Erica Roth, RPSGT; Julie Flaa, RPSGT; Jennifer Blair, BA; Jennifer Schwartz, BA; Anna Simon, BA; Amber Randall, BA







