
1
Chest Pain: Primary PCI
Integrated Care Pathway
PATIENT DETAILS (Addressograph) NEXT OF KIN Name: ………………………………… Address: ………………………………. …………………………………………..
Post Code: …………………………….
DOB: ………………………………….. Age …………………………………..… Hospital No: ……………………………
Name……………………………………. Relationship …………………………… Address …………………………………
…………………………………………… Phone No: ………………………….….
Mobile No: …………………………….. Other contact No………………………..
GP Address
Date/ time of admission
Ethnic origin White Black Asian
Oriental Other
Consultant
Allergies/Warnings
Admitting nurse
This pathway is intended for guidance only. It is in no way intended to be prescriptive. Clinical decisions remain at the discretion of the clinician. Where a clinical decision would result in a variation from treatment and care set out in the pathway, please
document that variation and the reason for it.
Pages are colour coded – see key below
Protocols Doctors Nurses Multi disciplinary
Next review Dec 2012

2
3
Clinical assessment for procedure
Date/time………………………………………………. Bleep no…………………..
Name of Doctor……………………………………………..…..
History of presenting complaint Pain time......................... Call time.......................... Hospital arrival................ Cath lab arrival…………..
Please circle Anterior/ Inferior/ Posterior/ Lateral/ LBBB Thrombolysis given (if PHT) Time…………. Consent signed Y/N
Drugs given (including medications given by WAST)
Aspirin 300mg Yes / No Given by: Time: Clopidogrel 600mg Yes / No Given by: Time: Ticagrelor 180mg Yes / No Given by: Time: Prasugrel 60mg Yes / No Given by: Time:
Other (state drug, dose, administered by and time)
Allergies
Cath lab nurse assessment for procedure
4
Procedure/ PPCI (Consultant to Complete)
Grafts (if applicable)
Procedure Angiogram / Angioplasty Start time............ Finish time.................... Stent type: DES / BMS / No stent used Reperfusion time (balloon/ Export)........... Access site: Radial R / L Femoral R/ L Contrast volume mls.......... Comments Medications given (see next page) Procedure complication Management plan: Is patient fit for repatriation to local hospital within 24 hours? Yes / No Signed.................................. Print.................................. Date..................
5
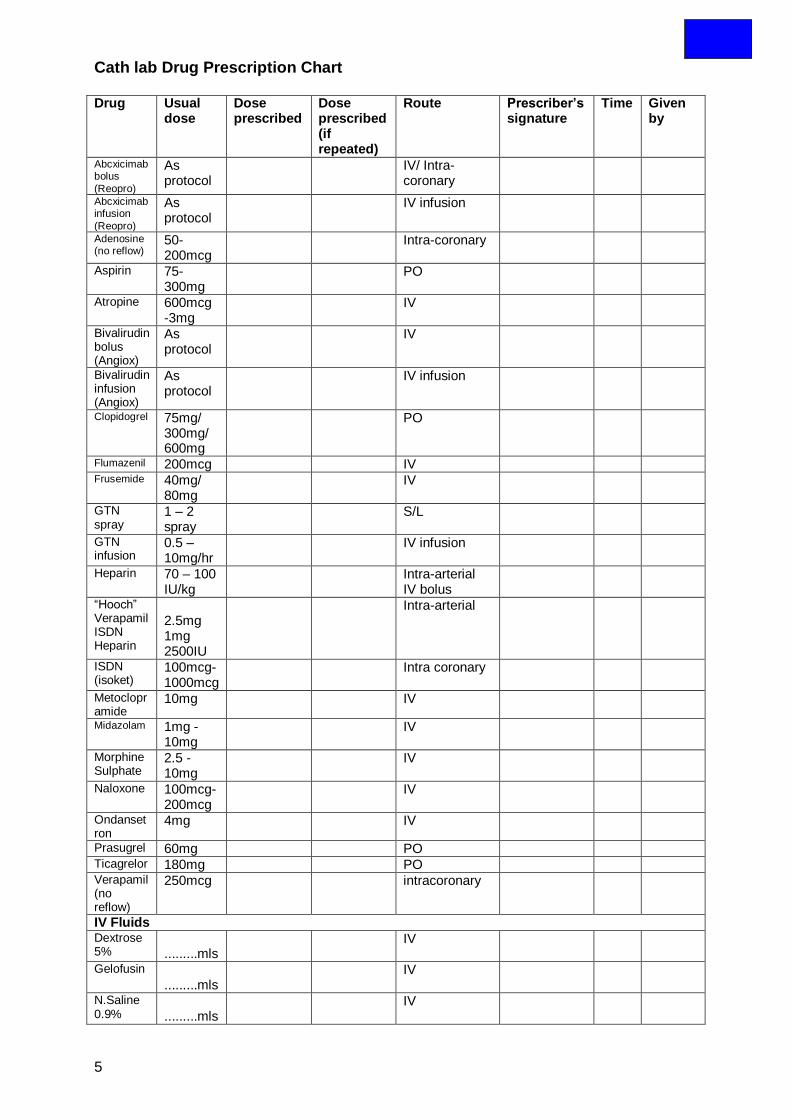
Cath lab Drug Prescription Chart Drug Usual
dose Dose prescribed
Dose prescribed (if repeated)
Route Prescriber’s signature
Time Given by
Abcxicimab bolus
(Reopro)
As protocol
IV/ Intra-coronary
Abcxicimab infusion
(Reopro)
As protocol
IV infusion
Adenosine (no reflow)
50-200mcg
Intra-coronary
Aspirin 75-300mg
PO
Atropine 600mcg -3mg
IV
Bivalirudin bolus (Angiox)
As protocol
IV
Bivalirudin infusion (Angiox)
As protocol
IV infusion
Clopidogrel 75mg/ 300mg/ 600mg
PO
Flumazenil 200mcg IV Frusemide 40mg/
80mg IV
GTN spray
1 – 2 spray
S/L
GTN infusion
0.5 – 10mg/hr
IV infusion
Heparin 70 – 100 IU/kg
Intra-arterial IV bolus
“Hooch” Verapamil ISDN Heparin
2.5mg 1mg 2500IU
Intra-arterial
ISDN (isoket)
100mcg-1000mcg
Intra coronary
Metoclopramide
10mg IV
Midazolam 1mg -10mg
IV
Morphine Sulphate
2.5 -10mg
IV
Naloxone 100mcg-200mcg
IV
Ondansetron
4mg IV
Prasugrel 60mg PO Ticagrelor 180mg PO Verapamil (no reflow)
250mcg intracoronary
IV Fluids Dextrose 5%
.........mls
IV
Gelofusin .........mls
IV
N.Saline 0.9%
.........mls
IV

6
Clinical assessment post procedure/ PPCI – cath lab
AVPU – alert, voice, pain, unresponsive
7
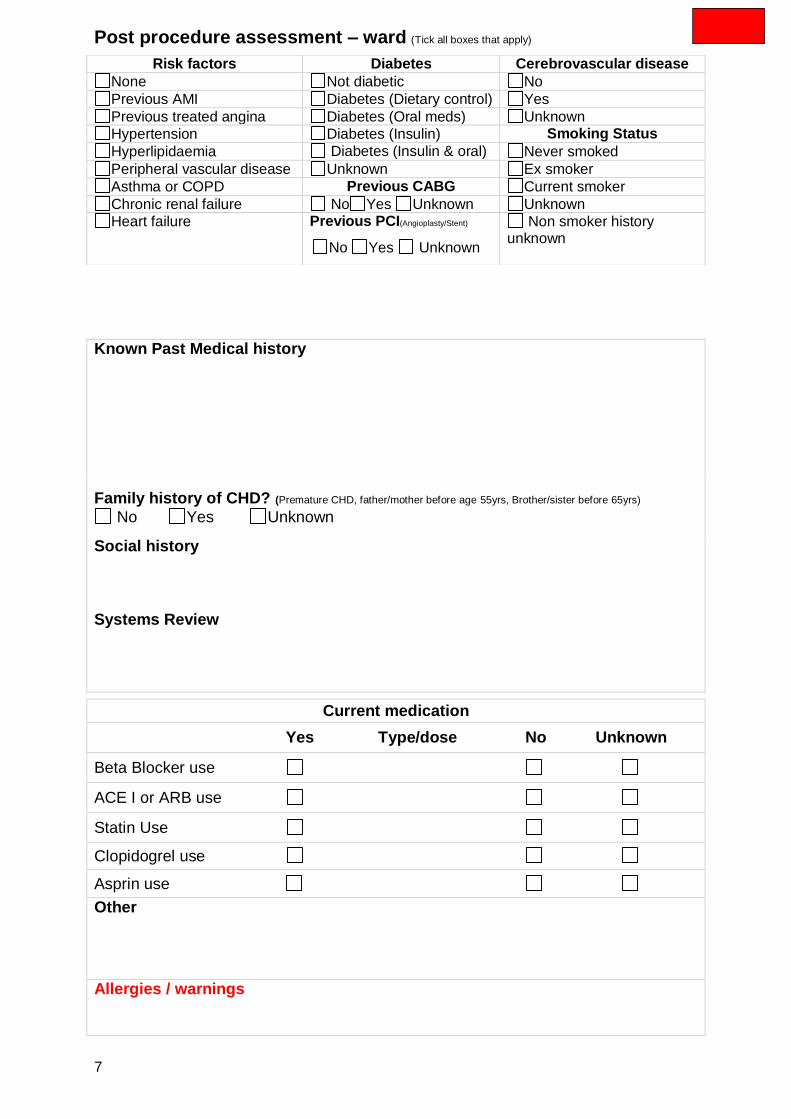
Post procedure assessment – ward (Tick all boxes that apply)
Known Past Medical history
Family history of CHD? (Premature CHD, father/mother before age 55yrs, Brother/sister before 65yrs)
No Yes Unknown
Social history Systems Review
Current medication
Yes Type/dose No Unknown
Beta Blocker use
ACE I or ARB use
Statin Use
Clopidogrel use
Asprin use
Other
Allergies / warnings
Risk factors Diabetes Cerebrovascular disease
None Not diabetic No
Previous AMI Diabetes (Dietary control) Yes
Previous treated angina Diabetes (Oral meds) Unknown
Hypertension Diabetes (Insulin) Smoking Status
Hyperlipidaemia Diabetes (Insulin & oral) Never smoked
Peripheral vascular disease Unknown Ex smoker
Asthma or COPD Previous CABG Current smoker
Chronic renal failure No Yes Unknown Unknown
Heart failure Previous PCI(Angioplasty/Stent)
No Yes Unknown
Non smoker history unknown
8
Clinical examination
Height............ Weight............... CARDIOVASCULAR BP / Pulse Heart sounds I II I JVP Bruits present Yes / No Site................ RESPIRATORY SaO2: RA.......... O2....................L/min GASTROINTESTINAL OTHER RELEVANT CLINICAL FINDINGS
Investigations requested
FBC ARTERIAL GASES TROPONIN T@ 0hrs
12 hrs
ESR BLOOD CULTURE CK
U&E URINE MICRO,C&S AMYLASE
LFT/Ca CRP LIPIDS
COAG TFT GLUCOSE
X-RAYS - CHEST
ABDO
SKELETAL
ECG ECHO OTHER

9
Date Date Date Date Date
Hb Na T. Prot Ca Coag Screen
WCC K+ Albumin Corr. Ca
Neu Chlor Bilirubin Gluco T. Chol
Plt Bic Alk Ph AST LDL
MCV Urea ALT Amylase HDL
ESR Creat GGT CRP Trig
1st Trop T 2nd Trop T
Echo findings: LV systolic impairment (please circle): Mild Moderate Severe EF% Valvular pathology (please specify): Aortic Mitral Tricuspid Pulmonary
Other test results
Blood glucose >11 mmols - Sliding Scale insulin Whenever blood glucose >11mmols/L on admission commence sliding scale.
Add 50 units of Actrapid Insulin to 50 mls Normal saline in a 50-ml syringe, infuse intravenously via a syringe driver. Measure blood glucose 1-2 hourly depending on the patients’ diabetic stability.
The infusion continues for at least 24hours, titrate dose according to regimen below.
Stop Metformin. Refer to diabetic specialist nurse
Blood glucose Infusion rate Blood glucose Infusion rate
0 - 2 mmol/l 0.5mls/hr 10 - 15mmol/l 4.0mls/hr
2 - 4 mmol/l 1.0mls/hr 15 – 20mmol/l 6.0mls/hr
4 - 10 mmol/l 2.0mls/hr >20mmol/l Contact doctor
10
11
Day 0. First 24 hours Post Admission: Medical review
Management Circle Initial Pain free Y / N / NA Check observations stable Y / N / NA Access site reviewed Y / N / NA Patient and next of kin aware of diagnosis and treatment plan Y / N Order day 1 bloods Y / N
Prescribe Circle Initial
Morphine IV prn, anti-emetic IV prn, GTN SL prn Y / N / NA
Standard secondary prevention medications in place (tick) Aspirin Clopidogrel/ Ticagrelor/ Prasugrel ACE Beta blocker Statin if not state why
Comments and variances

12
Day 0 – first 24 hours Post admission: Nursing Review
If no further comments needed. Please or N/A and initial am pm Night
Patient pain free / no discomfort in chest/ back/ neck/ arms/ jaw
Connected to cardiac monitor and record rhythm on observation chart. Continue cardiac monitoring for up to 24 hours if uncomplicated
12 lead ECG’s: On admission to CCU and if pain experienced
Perform cardiovascular, including temp, respirations and saturations and peripheral vascular observations every 30 minutes for 4 hours.
Check for ooze or haematoma at femoral / radial site
Bed rest: at max 300 until 2 hours after sheath removal
ACT check before sheath removal
Arterial sheaths removed when ACT < 150 Venous sheaths removed 1 hour post PCI TR band gradually release air from 3 hours post PCI until no pressure then remove
Sit up to 450 ( 2 hours post arterial sheath removal/ 1 hour after venous sheath removal/ immediately if radial approach)
Bed rest for 12 hours and fully assisted with hygiene needs
Fluid balance charted
MRSA screen performed
Cannula flushed and site checked
Refer patient to cardiac rehab team
Discussion with patient re: current condition and treatment plan
If eligible for repatriation contact bed manager of relevant hospital and inform them of possible repatriation
Check admission blood results. Monitor blood glucose
Ensure patient and relatives informed of diagnosis and treatment plan
Additional notes and variances

13
CCU Nursing staff to complete following pages
PATIENTS ADMISSION DETAILS
Marital status Single Married Widowed Divorced Other
Lives with: Type of accommodation:
Social circumstances:
Occupation:
Religion:
Presenting symptoms / patient condition on arrival:
Patient Wishes. Are there any issues that may influence decision making?
Advanced Decision □ Court Appointed Deputy □ Power of Attorney □ None □
Patient Signature…………………………...Date………….
These may not be relevant in all situations but collecting information on the existence of any of these may be useful i f a decision
needs to be made at a later stage and the individual lacks capacity to make the decision at the time. It is in keeping with the principles of the MCA to support individuals to make decisions at the time, in advance of incapacity, or by nominating a proxy decision-maker. Agreement to sharing information (please tick as appropriate) I agree that relevant health and social care professionals and service providers may be consulted, and that assessment information is shared with them, in order to understand and respond to my needs. I wish to restrict sharing of information (details below) Person unable to give consent (details below) Details re consent issues:
Signature of assessed person………………………………………………..Date………………..
Name…………………………………Signature………………………………Date………………..

14
Day 0 – first 24 hours post admission. Nursing notes
Additional notes and variances
Date/ Time

15
Day 1 : Medical review
Medications
Standard secondary prevention medications in place (tick) Aspirin Clopidogrel/ Ticagrelor/ Prasugrel ACE Beta blocker Statin if not state why Patients with symptoms and/ or signs of heart failure and left ventricular dysfunction consider eplerenone
Management Circle Initial
Order day 1 bloods Y / N
Glycaemic control Y / N
Organise echo Y / N
Give all patients copy of ECG Y / N
Comments and variances

16
Day 1: Nursing Review
If no further comments needed. Please or N/A and initial am pm night
Patient pain free / no discomfort in chest/ back/ neck/ arms/ jaw
Connected to cardiac monitor and record rhythm on observation chart. Continue cardiac monitoring for up to 24 hours if uncomplicated
12 lead ECG’s: routine and if pain experienced
BP, pulse, respiration, saturations, temp within normal limits for patient?
Document fluid balance and record bowel movements
Assess access site clean and dry and peripheral vascular observations satisfactory
Report any changes to medical staff
Gently mobilise if no pain. May sit out of bed
Assist with hygiene needs
Venous cannula flushed and site checked
MRSA results checked
Repatriate eligible patients to relevant CCU
Inform patient and relatives of progress and any changes to treatment plan
If discharge planning for today or tomorrow see appendix 1
Additional notes and variances

17
Day 2: Medical Review
Management Circle Initial
Discontinue cardiac monitoring as appropriate Y / N
If discharge planning for today complete appendix 1 Y / N
Cholesterol checked recently or during admission. If familial hypercholesterolaemia suspected refer to lipid clinic
Y / N
Additional notes and variances

18
Day 2: Nursing Review
If no further comments needed. Please or N/A and initial am pm night
Patient pain free / no discomfort in chest/ back/ neck/ arms/ jaw
12 lead ECG’s: routine and if pain experienced
BP, pulse, respiration, saturations, temp within normal limits for patient?
Fluid balance maintained and record bowel movements
Report any changes to medical staff
Sit out and freely mobilise around the bed
May wash in bathroom or shower if pain free
Inform patient and relatives of progress and any changes to treatment plan
If discharge planning for today or tomorrow see appendix 1
Additional notes and variances
Cardiac Rehabilitation review Date:
Rehab location:
Smoking cessation discussed Y / N Referral to smoking cessation Y / N
Healthy eating Y / N Medication management Y / N
Alcohol intake Y / N Chest pain management Y / N
Physical activity Y / N Driving Y / N
Surgical advice Y / N Returning to work Y / N
Stair assessment completed Y / N Post PCI advice Y / N
Clopidogrel card given Y / N Sexual activity advice Y / N
Stress and relaxation Y / N
Comments and variances
19
Day 3: Medical Review
Management Circle Initial
Complete discharge planning – appendix 1 Y / N
Additional notes and variances

20
Day 3: Nursing Review
If no further comments needed. Please or N/A and initial am pm Night
Patient pain free / no discomfort in chest/ back/ neck/ arms/ jaw
12 lead ECG’s: routine and if pain experienced
BP, pulse, respiration, saturations, temp within normal limits for patient?
Mobilise to bathroom and around ward
Wash in bathroom
Record bowel movements
Inform patient and relatives of progress and any changes to treatment plan
Additional notes and variances

21
Reperfusion and ECG
ECG determining treatment (one option)
ST Segment elevation LBBB
Place first 12 lead ECG performed
Ambulance In hospital Other healthcare facility
Who made the initial decision to attempt reperfusion?
No reperfusion attempted Specialist nurse A&E Clinician Member of on-call medical team Member of on-call cardiology team GP Paramedic Unknown
Reason pre-hospital thrombolytic (reperfusion treatment) treatment not given
Too late Risk of haemorrhage Uncontrolled hypertension Administrative failure Elective decision Patient refused treatment Ineligible ECG Other please specify……………………… Unknown
Date and Time of First Arrest
_ _ / _ _ / _ _ _ _ _ _ : _ _
Where did it occur? No arrest Before ambulance arrived After ambulance arrived A&E department CCU Medical ward Elsewhere in hospital Catheter lab
Method of admission?
Called GP/other health professional who saw patient then called emergency service
Called GP who called emergency services then saw patient
Called 999 Called NHS Direct Made own way to hospital (did not call
anyone) Called local helpline Called GP told to make own way to hospital Patient already in hospital Transferred from local A&E for PPCI Other please specify………………………… Unknown
Ambulance job number…………………….
Thrombolytic drug used (if applicable)
Tenecteplase (TNK) Alteplase (TPA)
Successful re-perfusion post lysis
yes no Was there a justified delay before reperfusion?
No Initial ECG ineligible Sustained hypertension Concern re recent cerebrovascular
event or surgery Delay obtaining consent Cardiac Arrest Obtaining consent for therapeutic trial Hospital administration failure Ambulance procedural delay Consideration of primary PCI Ambulance administrative delay Ambulance 12 lead ECG not diagnostic of
STEMI Delay in activating cath lab team Cath lab access delayed Pre-PCI complication Equipment failure Other*
Please specify______________________________ ____________________________________
What was cardiac rhythm?
Asystole VF/pulseless VT PEA Not known
Outcome
No return of circulation Return of circulation, died in hospital Discharged with neurological deficit Discharged, with NO neurological deficit Resuscitation not attempted Not Known Transferred to another hospital

22
Multidisciplinary continuation Sheet Date/ Name/ Signature
23
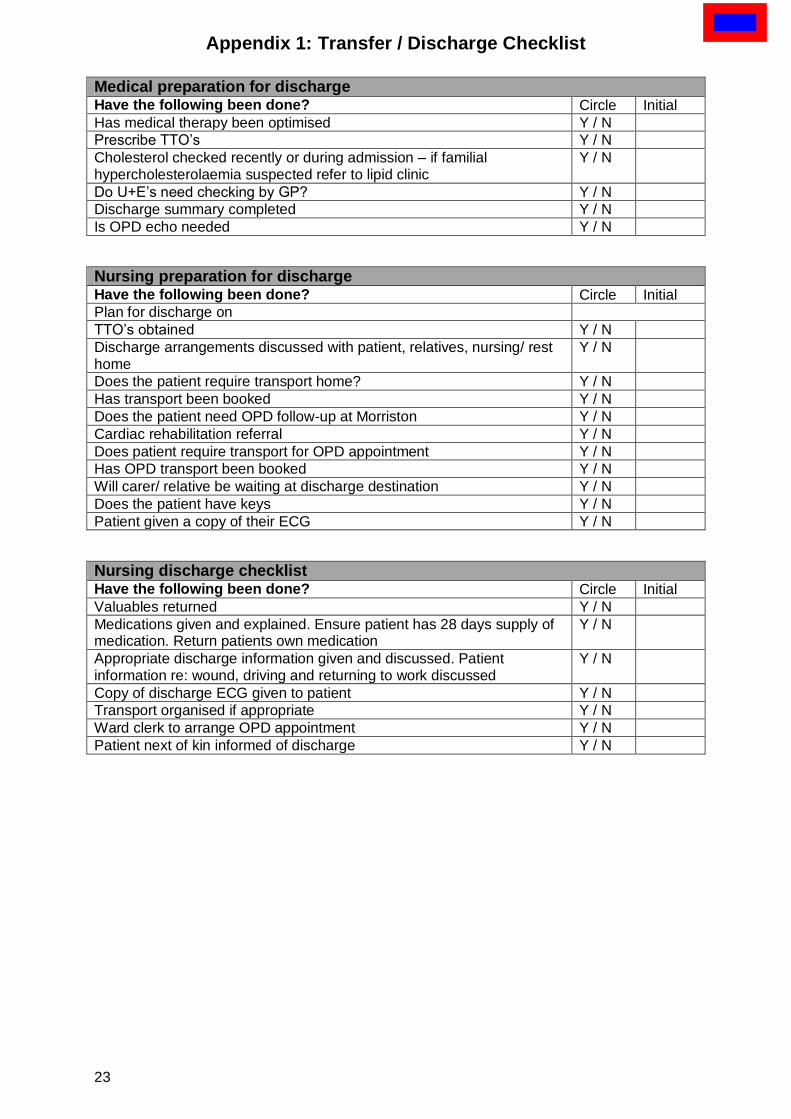
Appendix 1: Transfer / Discharge Checklist
Medical preparation for discharge
Have the following been done? Circle Initial
Has medical therapy been optimised Y / N
Prescribe TTO’s Y / N
Cholesterol checked recently or during admission – if familial hypercholesterolaemia suspected refer to lipid clinic
Y / N
Do U+E’s need checking by GP? Y / N
Discharge summary completed Y / N
Is OPD echo needed Y / N
Nursing preparation for discharge
Have the following been done? Circle Initial
Plan for discharge on
TTO’s obtained Y / N
Discharge arrangements discussed with patient, relatives, nursing/ rest home
Y / N
Does the patient require transport home? Y / N
Has transport been booked Y / N
Does the patient need OPD follow-up at Morriston Y / N
Cardiac rehabilitation referral Y / N
Does patient require transport for OPD appointment Y / N
Has OPD transport been booked Y / N
Will carer/ relative be waiting at discharge destination Y / N
Does the patient have keys Y / N
Patient given a copy of their ECG Y / N
Nursing discharge checklist Have the following been done? Circle Initial
Valuables returned Y / N
Medications given and explained. Ensure patient has 28 days supply of medication. Return patients own medication
Y / N
Appropriate discharge information given and discussed. Patient information re: wound, driving and returning to work discussed
Y / N
Copy of discharge ECG given to patient Y / N
Transport organised if appropriate Y / N
Ward clerk to arrange OPD appointment Y / N
Patient next of kin informed of discharge Y / N







