Download - Cerebral angiography technique

CEREBRAL
ANGIOGRAPHY(DSA)-
TECHNIQUE AND
NORMAL ANATOMY
Dr prashant shringi
Senior resident neurology

NORMAL ANATOMY
• ARTERIAL SUPPLY
• 2 Internal Carotid Artery
• 2 Vertebral Arteries


CIRCLE OF WILLIS
• Grand Vascular Station of the Brain
• Classical –18% to 20%
• Majority circles shows anomaly-52%
• Most frequent anomaly is hypoplasia of ACA-24%
• Accesory vessels in the form of duplication/triplicationsof
ACOM (2 M.C.) -12%
Fetal posterior cerebral artery-10%

CIRCLE OF WILLIS

COMPONENTS:
• Internal carotid arteries
• Horizontal segments of Anterior cerebrals(A1)
• Anterior communicating artery
• Proximal segments of posterior cerebrals(P1)
• Posterior communicating arteries
• Basilar artery

Branches of ACA
• A1- medial lenticulostriate artery
• ACoA- Perforating branches
• A2- Recurrent artery of Heubner (RAH)
• Orbitofrontal artery
• Frontopolar artery
• A3- Pericallosal and Callosomarginal a.
• A4 & A5- Cortical branches

ACA
MIDDLE CEREBRAL ARTERY
• Larger terminal branch of ICA
• Run laterally in stem of lateral sulcus
• Curves on superolateral surface
• Runs backwards in depth of posterior ramus of lateral
sulcus

• M1 segment =horizontal segment from origin to its
bifurcation (it is in sylvian fissure)
• M2 segment =lacunar segment -in the insula loops over
insula—laterally to exit from sylvian fissure
• M3 segment = opercular branch-from sylvian fissure &
ramify over cerebral cortex
• Anomalies of MCA are uncommon


POSTERIOR CEREBRAL ARTERY
P1-Peduncular/Precommunicating
P2-Ambient segment
P3-Quadrigeminal segment
P4-Cortical branches
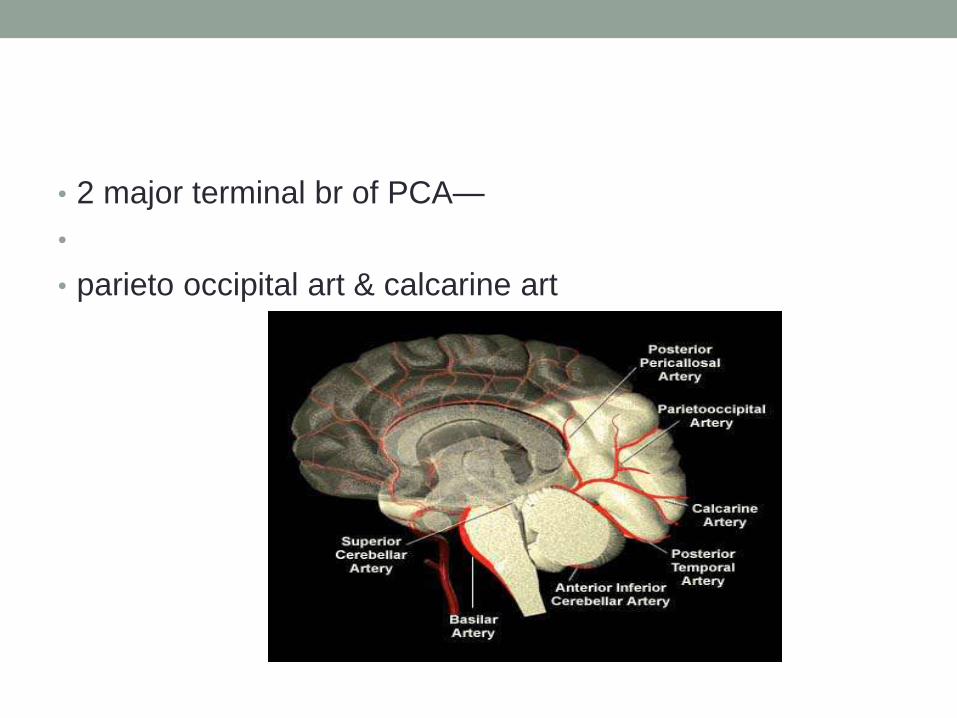
• 2 major terminal br of PCA—
•
• parieto occipital art & calcarine art

POSTERIOR FOSSA
• Vertebral artery
• Basilar artrery
• Vertebral arteries
• Originate from the subclavian arteries
• Left VA is dominant in 60% cases

Branches of vertebral artery
• Extracranial -numerous branches to the meninges,spinalcord & muscles
• -Posterior meningeal artery
• Intracranial-
-Anterior spinal artery
• -Posterior inferior cerebellar Art.
• Anterior medullary
• Lateral medullary
• Tonsillomedullary
• Telovelotonsillar
• Cortical branches

BASILAR ARTERY
•Right and left VA unite to form basilar artery
• Courses infront of pons (Prepontine cistern)terminates in the interpeduncular cistern
• 3cm in length,1.5 to 4mm in width

Branches of basilar artery
•Anterior inferior cerebellar artery (AICA)
• Superior cerebellar artery
•Pontine artery
• Labyrinthine artery

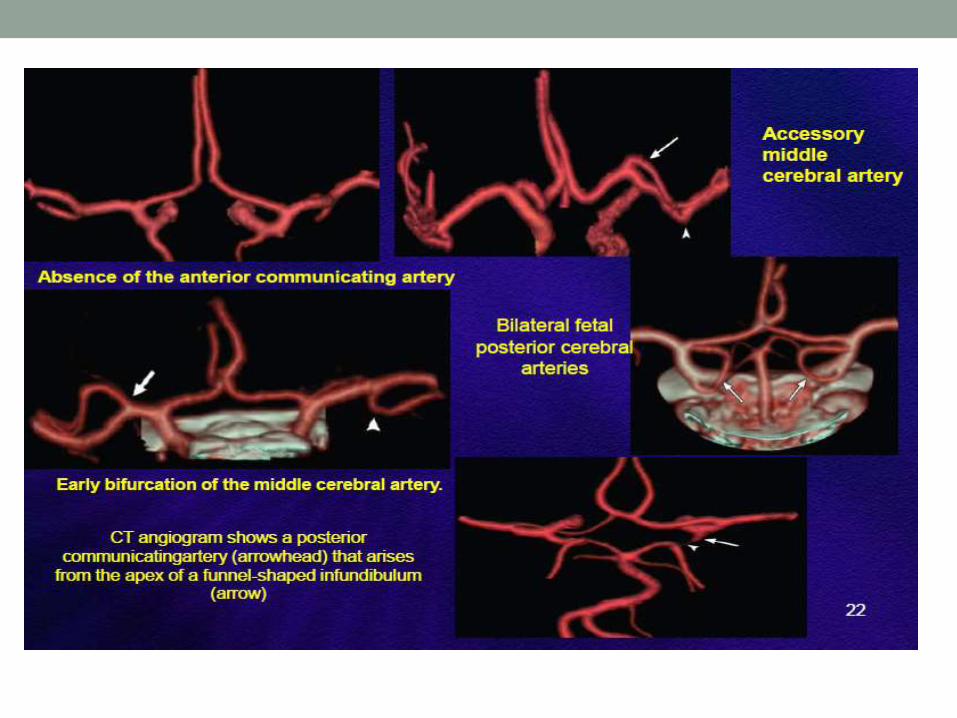
Normal VARIANTS
• Fenestrations and duplications
•Variants of the circle of Willis
• Persistent carotid-basilar anastomoses
• Anomalies identified in the skull base

Normal Variants of the Circle of Willis


CEREBRAL ANGIOGRAPHY
•Angiography –
• Radiological study of blood vessel in the bodyafter the introduction of iodinated contrastmedia.

Imaging Techniques
• Vascular structures of brain can be imaged by 4
means:
• 1. DSA: gold standard
• Invasive and risk of nephrotoxic contrast,ionising
radiation
• 2. Vascular ultrasound: least invasive, can be
done bedside, cost effective.
• Best choice for imaging vessels close to skin
surface.

•Drawback: limited anatomic coverage, deep vessels cant be imaged, operator dependent, requires skill.

• 3 CT angio: main drawbacks are contrast use andradiation exposure,
• calcifications are overestimated.
• Preferred for aorta and coronaries
• 4 MRA : non invasive, no radiation exposure.
• Preferred for carotids and intracranial vessels as MRIbrain can also be obtained
• widely used in neurological disorders
•ANGIO?
• ‘ANGIO means blood vessel’
• SUBTRACTION?
• It is simply a technique by which bonestructures images are subtracted or canceledout from a film of bones plus opacified vessels,“leaving an unobscured image of the vessels”

DSA
•Acquisition of digital fluoroscopic imagescombined with injection of contrast materialand real time subtraction of pre- and postcontrast images to perform angiography isreferred to as digital subtraction angiography

HISTORY
Portuguese neurologist Egas Moniz,( NobelPrize winner 1949), in 1927 developed thetechnique of contrast x-ray cerebral angiographyto diagnose diseases,
such as tumors and arteriovenousmalformations.

• Idea of subtraction images was first proposedby the Dutch radiologist Ziedses des Plantes inthe 1935, when he was able to producesubtracted images using plain films.

HISTORICAL DEVELOPMENT
•CONVENTIONAL SUBTRACTION TECHNIQUE:
•Photographic method used to eliminateunwanted images.
•No addition of information; only purpose tomake diagnostically important information

•Developed in 1970s, University of Wisconsin,University of Arizona, University of Kiel.
•USA
•Commercial systems introduced in 1980.

• 3 conditions:
• SCOUT FILM
•ANGIOGRAM FILM-CONTRAST
•NO MOTION OF HEAD

PRINCIPAL
• Principles of subtraction are based on thefollowing:
• Scout film shows the structural details of theskull and the adjacent soft tissue.
•Angiogram film shows exactly the sameanatomic details, if the patient does not move,plus the opacified blood vessels.

• If all the information in the scout film could besubtracted from the angiogram film, only theopacified vessel pattern would remain visible.

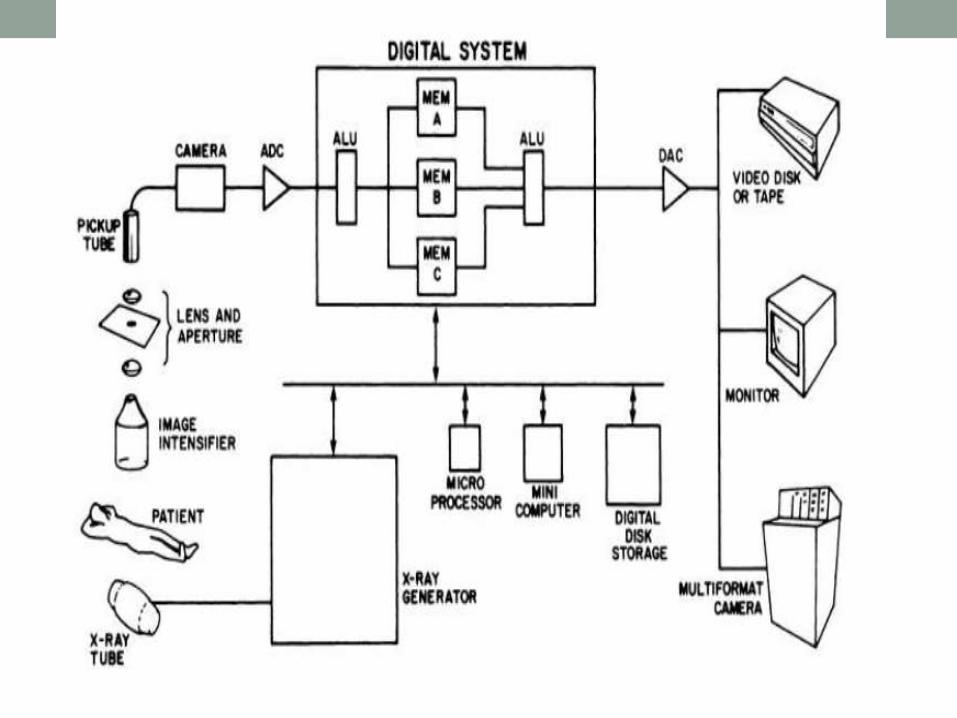
DIGITAL IMAGE PROCESSOR

WHY DSA?
• Digital subtraction angiography (DSA) was developedto improve vessel contrast.
• Technique that uses a computer to subtract twoimages, obtained before and after contrast media isinjected into the vessels of interest.
• Anatomical structures that are the same in the twoimages can be removed and the resulting imageshows the vessels only

•Modern DSA systems are based on digitalfluoroscopy/fluorography systems, which areequipped with special software and displayfacilities

• Image before the contrast agent isadministered is called the mask image.
•
•Once the contrast is administered, a sequenceof images are taken by a television camera inanalog form, which is then digitised bycomputer

• DSA processor has two separate imagememories, one for the mask and the other forthe images with contrast medium.
• These two image memories are subtractedfrom one another arithmetically, and the resultgoes to an image processing and display unit.

Indications
•Diagnostic:
•Non traumatic Subarachnoid Hemorrhage(SAH)
• Arterial dissection
• laceration
•Aneurysm

Indications
•Pseudoaneurysm
• Thrombosis (Extracranial & Intracranial)
•Arterio-venous malformation (AVM).
•Arterio-venous fistula (AVF).
• Tumor vascularity

•Therapeutic:
• Embolisation
• Stenting
• Thrombolysis
• Thrombectomy

Contra indications
•No absolute contraindication.
• Poor renal reserve.
• Deranged coagulogram.
• Allergic to contrast media

Contrast Media
• Blood vessels are not normally seen in an x-ray
image, because of low tissue contrast.
• To increase image contrast, contrast agents,
which are dense fluids with elements of high
atomic numbers, such as iodine, are injected into
a blood vessel during angiography. Because of its
higher density and high atomic number, iodine
absorbs photons more than blood and tissue.

Creates detailed images of the blood vessels inreal time.
• First contrast media used for intravascularinjection were called high-osmolar contrastmedia (HOCM).

• High osmolarity caused adverse effects such as
pain, endothelial damage, thrombosis, and
increased pressure in the pulmonary circulation.
• Low-osmolar contrast media (LOCM) were first
developed in the 1970's reduce side effects.
• Major risks of modern iodine contrast media is an
allergic reaction to iodine

•Non ionic Iso-osmolar contrast media.
•30-40% dilution with normal saline.
•50 ml of diluted contrast media is enough to doa standard cerebral angiogram with total 8projections.
•Approx. 5-8 ml diluted contrast / injection.

Materials used
• Catheters
• Arterial sheath
• Medicut
• Guidewires
• Contrast
• Connector/100
cm.tubing
• Surgical blade
• Saline
• Disposable syringes
• Local anesthesia
• Heparin
• Surgical gloves
• Elastoplast

Picard Pigtail
Sim -1

•

Guide Wires Medicut

PREPARATION
• Nil orally 4-6 hrs.
• On trolley
• In hospital gown
• Groin shave
• Records
• Should be well
hydrated.
• Should void before
procedure.
• Peripheral pulses
marked.
• I.V line in place.
• Informed consent

PROCEDURE
•Gaining arterial access.
• Selective arterial catheterization.
• Image acquisition.
•Closure of arterial access.
•Post processing
•Hard copy

• Patients may be sedated to reduce anxiety.
• Monitor of vitals
• Local anesthetic is usually used in the areawhere the catheter is to be inserted,
•Most common femoral artery

PROCEDURE
• Small incision given, medicut is inserted into the artery,
• Fluoroscopy is used to guide the needle to the proper
position .
• Needle is then removed after placing guide wire in the
artery and vascular sheath is inserted over the guide wire
.
• Catheter is then inserted along the guide wire through the
sheath

• When the catheter is in the correct position, the wire is
pulled out and dye is injected through the catheter.
• Images are acquired during contrast injection.
• Injections can be made directly into the artery of interest
(selective arteriography)

COMPLICATIONS
• 0.16% major complication rate.
• Local complications: hematoma, vessel laceration,
dissection, pseudoaneurysm ,AVfistula.
• Systemic complications: contrast reactions, fever,
sepsis, dehydration, death.
• CNS complication: aggravation of preexisting
complaints, neurological deficit.

POSTPROCEDURAL CARE
• After the catheter is removed compression is applied to
the puncture site
• Bed rest for a minimum of 4 hours
• During rest patient is monitored and vital sign like
peripheral pulse like distal to Puncture are regularly
• Extremity is also checked for warmth, color, numbness to
ensure circulation has not been disrupted.

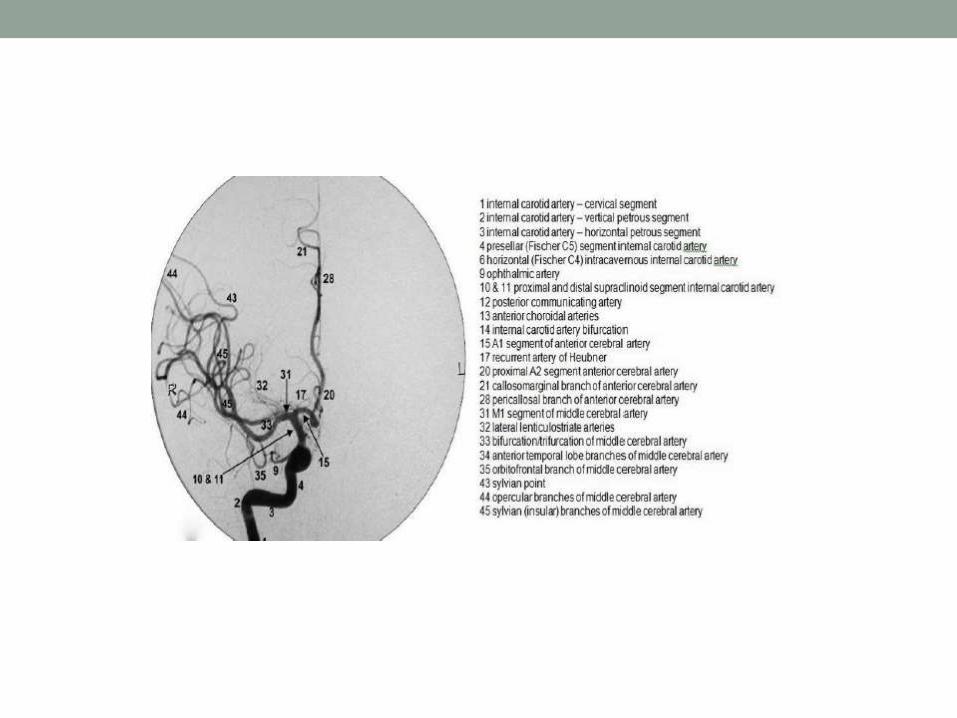
Cerebro-vascular anatomy as
appreciated in DSA




Diagnostic usage
• Acom aneurysm:

ACA Aneurysm

MCA Aneurysm

Pcom Aneurysm

AV Malformation

Tumour vascularity

Digital subtraction angiography based
advances
•Better visualization and less radiation exposureare key tenets in the development of digitalsubtraction angiography
•Complexity of disease types increases andmore technically challenging, cutting-edgeprocedures are performed

• Digital subtraction angiography systems with flat
panel : ADVANTAGES-
• High spatial resolution, wide dynamic range,square field of view, and real-time imagingcapabilities with no geometric distortion—all ofwhich may be used for improve image quality,reduced patient exposure to radiation

• Hatakeyama et al have shown that two-dimensional (2D)
and three-dimensional (3D)digital subtraction angiography
using the flat panel detector system of the direct
conversion type, with low radiation dose, is superior in
image quality for visualizing small intracranial vessels with
significantly decreased radiation exposure compared with
digital subtraction angiography with the conventional
image intensifier television system
• Hatakeyama Y, Kakeda S, Korogi Y, et al. Intracranial 2D and 3DDSA with flat panel detector of the
direct conversion type: initial experience. Eur Radiol 2006;16:2594 –2602.


Digital subtraction techniques
• Mask subtraction
• Dual energy subtraction
• Time interval differencing
• Temporal filtering

•Allura Xper FD20/10 biplane flat detectorsystem with integrated 3D for intricateneurovascular procedures.
• 3D- reconstructions
• Xper CT
• SPECTRA BEAM
• 3D Roadmapping
• multi-modality information integration


•Redefines image clarity and capturesinformation at a resolution four times greaterthan conventional X-ray systems.

Xper CT
• With XperCT clinicians can access CT-like imaging right
on the angio system so can assess soft tissue, bone
structure and other body structures before, during or after
an interventional procedure.
• XperCT reconstruction is created from rotational
acquisition performed on the Allura Xper system.
• This reconstruction can be overlaid with the 3D vascular
image.

• 3D soft tissue imaging supports diagnosis
planning, interventions and treatment follow-up
• XperCT can be combined with Allura 3D-RA
images to visualize soft tissue and vascular
anatomy on one image.

Spectra Beam
• Basically a selectable copper beam filtration
• Combination of Spectra Beam with the MRC-
tube allows increased X-ray output with better
filtration of soft radiation.
• Reduces patient X-ray dose for cardiac and
vascular applications, while maintaining the same
image quality.

Disadvantage of DSA
• Limited spatial resolution
•Artifacts
• Small visual field
•Not a good technique for neoplasm

Conclusion
•Despite recent advances in CT angiography andMR angiography, DSA remains the standardimaging technique for evaluation of thecerebral vasculature .
•3D reconstruction of the dataset acquiredduring rotational DSA represents the latestdevelopment in the neurovascular imaging .

• 3D-DSA has taken a prominent role intreatment planning by enabling betterappreciation of the morphology of complexvascular lesions before endovascular or surgicalmanagement.
• Superior in the performance of sophisticatedtasks such as aneurysm volume measurement

•On the other hand, inability of 3D-DSA tosimultaneously image osseous and vascularstructures is noted as a weakness of thistechnique compared with CT angiography .

Refrences-
• The Principle of Digital Subtraction Angiography and Radiological Protection;K. OKAMOTO, . IT, K. SAKAI, S. YOSHIMURA ; InterventionalNeuroradiology 6 (Suppl1): 25-31, 2000
• Advances in Interventional Neuroimaging; Vallabh Janardhan and Adnan I.Qureshi; Vol. 4, 414–419, July 2007 c The American Society for ExperimentalNeuroTherapeutics,
• Intracranial Vascular Stenosis and Occlusive Disease: Evaluation with CTAngiography, MR Angiography, and Digital Subtraction Angiography; Bash etal; AJNR Am J Neuroradiol 26:1012–1021, May 2005
• Uptodate.com
• Digital substraction Angiography ;John hopkins Medical university
• Gray’s text book of anatomy
• Teachme anatomy .com

• THANK YOU







