Download - Carlos Henrique Barrios

Clinical Research as an Alternative
Porto Alegre, November 2016
The Cancer Epidemic
Carlos H. Barrios, M.D.
Hospital do Câncer Mãe de Deus
PUCRS School of Medicine
Latin American Cooperative Group, LACOG
Porto Alegre, Brazil

POTENTIAL CONFLICTS OF INTEREST
• Clinical Research: Pfizer, Novartis, Amgen, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Roche/Genentech, Lilly, Sanofi, Taiho Pharmaceutical, Mylan, Merrimack, Merck, Abbvie, Astellas Pharma, Biomarin, Bristol-Myers Squibb, Daiichi Sankyo, Abraxis BioScience, AB Science, Asana Biosciences, Medivation, Daiichi Sankyo, Exelixis, ImClone Systems, LEO Pharma, Millennium
• Academic Research Projects: CPO, PUCRS, LACOG, GBECAM, INCA-Brazil.
• Advisory Boards and Consulting: Boehringer-Ingelheim, GSK, Novartis, Pfizer, Roche/Genentech, Eisai, Bioepis.
• No financial conflicts to declare.

Realidade Epidemiológica
Aumento da incidência de câncer internacionalmente
EnvelhecimentoAumento da PopulaçãoIncorporação de Fatores de Risco
Mais da metade dos casos de câncer são esperados em países em desenvolvimento
Incidência de câncer deve duplicar em 2020
Em 2030 a incidência por câncer deve aumentar em 78% (África do Sul, China, Índia) e em 98% em regiões menos desenvolvidas
Mortalidade por Câncer deve superar CV em 2030 (OMS) (já está acontecendo nos US)
World Health Organization, The global burden of disease: 2004 update.The Lancet Oncology, Early Online Publication, 1 June 2012, doi:10.1016/S1470-2045
Câncer: Um Desafio Global
Novos Casos2000 - 10,000,0002010 - 15,000,0002030 - 27,000,000
Mortes2000 - 6,200,0002010 - 10,000,0002030 - 17,000,000

• Cancer poses a major threat to public health worldwide, and incidence rates have increased in most countries since 1990.
• In 2013, there were 14.9 million new cancer cases and 8.2 million cancer deaths.
• The trend is a particular threat to developing nations with health systems that are ill-equipped to deal with complex and expensive cancer treatments.
JAMA Oncol. doi:10.1001/jamaoncol.2015.0735Published online May 28, 2015.

Goss P, et al. Lancet Oncology, 2103
Educação da PopulaçãoAcesso ao Sistema de SaúdeAcesso à novas Tecnologias:
Métodos diagnósticos modernosDrogas mais eficazes
Discrepâncias Internacionais

INCIDÊNCIA DE CASOS DE CÂNCER POR 100.000 HABITANTES, BRASIL 2012-2014
POR ESTADO
FONTE: INCA, ESTIMATIVAS 2012 E 2014.
POR REGIÃO
O RIO GRANDE DO SUL É O ESTADO COM MAIOR INCIDÊNCIA
DE NOVOS CASOS DE CÂNCER NOS ÚLTIMOS ANOS.

FONTE: OMS – OPAS, 2012
INCA, 2014
COMISSIÓN HONORÁRIA DE LUCHA CONTRA EL CÁNCER (URUGUAY), 2011.
SEGUNDO A OMS, A ESTIMATIVA DE INCIDÊNCIA DE CÂNCER NO MUNDO É MAIOR EM REGIÕES DESENVOLVIDAS (NORTE
AMÉRICA E EUROPA). NO CONTINENTE SUL AMERICANO O URUGUAI É O PAÍS COM MAIOR INCIDÊNCIA.
TX - INC.
243,22
TX - INC.
306,37
TX - INC.
456,20
TX - INC.
187,13
TX - INC.
330,17
TX - INC.
374,41
TX - INC.
471,66
TX - INC.
208,77
COMPARANDO O RS E POA NO ÂMBITO GLOBAL, O CENÁRIO É EQUIVALENTE AO DE
PAÍSES COM AS MAIORES TAXAS DE INCIDÊNCIA (APRESENTANDO TAXAS MAIORES QUE
AS DO URUGUAI.
ESTIMATIVA DA INCIDÊNCIA DE CASOS DE CÂNCER PARA CADA 100.000 HABITANTES NO MUNDO (OMS, 2012)

PRINCIPAIS CAUSAS DE MORTE EM PORTO ALEGRE (FONTE: SECRETARIA MUNICIPAL DE SAÚDE DE PORTO ALEGRE, 2014.)
Nº MORTES POR CAUSA DE NEOPLASIAS – ULTIMOS 7 ANOS
PRINCIPAIS CAUSAS DE MORTENº MORTES POR DOENÇAS CARDIOVASCULARES – ULTIMOS 7 ANOS
NOS ULTIMOS 7 ANOS EM PORTO ALEGRE, AS MORTES POR DOENÇAS CARDIOVASCULARES APRESENTARAM
QUEDA DE 4,11%, ENQUANTO AS MORTES POR NEOPLASIAS CRESCERAM EM 12,64%.
26.4%
22.9%

Cancer “Globalization”
Cancer is a global challenge that
will (only) be met by global
participation
'The Scream' by Edvard Munch 1893, National Gallery Oslo, Norway

• Consider strategies to address discrepancies
• 15-25% of tumors are related to smoking
• Screening for Breast Cancer, CRC, Prostate?,
Lung?...
• Screening and vaccination for Cervical Cancer
• Addressing the Obesity epidemic
• Vaccination against Hepatitis B
• Vaccination against HPV
• Clinical Research
• Other…
Danaei G et al. Lancet 366: 1784–1793, 2005
Katz IT, et al. N Engl J Med 354: 1110–1112, 2006
Cavalli F. Nature Clin Practice Oncol, 3:582, 2006
Addressing Cancer Globalization…

Descobrir novos tratamentos capazes de superar aqueles já existentes, além de imprimir inovação a medicamentos já consolidados só é possível através de uma investigação minuciosa: a pesquisa clínica.

Pesquisa Clínica
• Desenvolvimento de novas formas para prevenir, diagnosticar e tratar o câncer.
• Através de estudos clínicos podemos comprovar se novos tratamentos são seguros e/ou mais eficazes que os tratamentos atuais.
Pesquisa Clínica
Tratar
Diagnosticar
Manejo de Sintomas Doença
Prevenir
Manejo Eventos
Adversos

CANCER TRIALS (CLINICALTRIALS.GOV)
• ClinicalTrials.gov currently lists 223.743 studies with locations in 190 countries.
• 56.232 studies in Cancer.
Source: www.ClinicalTrials.gov Accessed August 28nd, 2016

CANCER TRIALS (CLINICALTRIALS.GOV)
• ClinicalTrials.gov currently lists 56.232 studies in Cancer.
Source: www.ClinicalTrials.gov Accessed August 28nd, 2016
4,5%
53,7%

Clinical Cancer Research in South America - 2016
World 56.232
South America 1.378 (2.4%)
Argentina 572Brazil 977 (1.7%)Chile 285Colombia 207Ecuador 24Peru 278Uruguay 25Venezuela 44
Source: www.ClinicalTrials.gov Accessed August 28nd, 2016
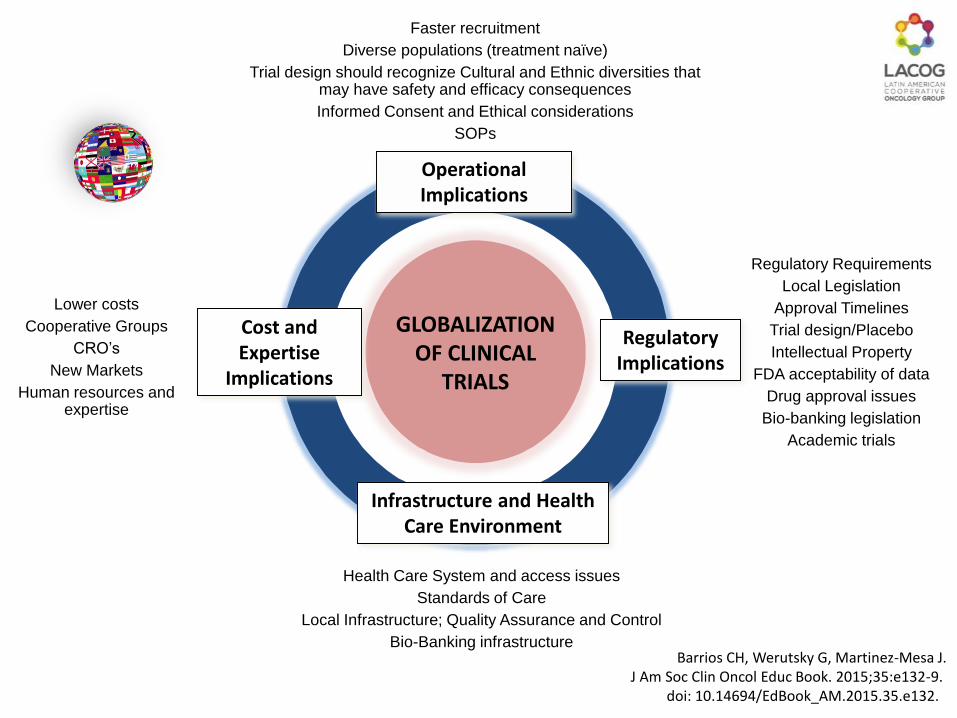
Regulatory Requirements
Local Legislation
Approval Timelines
Trial design/Placebo
Intellectual Property
FDA acceptability of data
Drug approval issues
Bio-banking legislation
Academic trials
Health Care System and access issues
Standards of Care
Local Infrastructure; Quality Assurance and Control
Bio-Banking infrastructure
Faster recruitment
Diverse populations (treatment naïve)
Trial design should recognize Cultural and Ethnic diversities that may have safety and efficacy consequences
Informed Consent and Ethical considerations
SOPs
Lower costs
Cooperative Groups
CRO’s
New Markets
Human resources and expertise
GLOBALIZATION OF CLINICAL
TRIALS
Infrastructure and Health Care Environment
Cost and Expertise
Implications
Operational Implications
Regulatory Implications
Barrios CH, Werutsky G, Martinez-Mesa J.J Am Soc Clin Oncol Educ Book. 2015;35:e132-9.
doi: 10.14694/EdBook_AM.2015.35.e132.

Clinical Cancer Research• Essential to improve therapeutic
results• “Virtuous Circle” of clinical
research: all involved do benefit• Offers “state of the art” therapy• Qualified investigators and large
number of patients (LA)• Should be a strategic priority• Need to recognize and address
bureaucratic and all other barriers that stall development

Brasil e a Pesquisa Clínica em Oncologia
• Oferece o melhor tratamento disponível “state of the art” (mesmo para o grupo controle).
• Particularmente significativo para o Brasil onde o melhor tratamento disponível NÃO esta disponível para a maior parte da população (SUS) e participação em pesquisa oferece NO MÍNIMO o tratamento convencional ideal/ótimo.

Breast Cancer: Number of Cases/year 57.120
Cases in the public system-SUS (73.7%) 42.097
Stages I/II/III (94%) 39.571
HER2 positive patients (20%) 7.914
Number of deaths avoided by Trastuzumab/y (8.8%) 696
Deaths in HER2 positive women (2005-2012)* 4872
Estimated number of deaths in early HER2 positive patients due to lack of access to adjuvant Trastuzumab in the public system in
Brazil 2005-2012.
INCA. Câncer de mama. http://www2.inca.gov.br/wps/wcm/connect/tiposdecancer/site/home/mama, Jan 2014.
IBGE. Pesquisa Nacional por Amostra de Domicílios, 2008 [acesso March 2,
2014].http://www.ibge.gov.br/home/estatistica/populacao/panorama_saude_brasil_2003_2008/PNAD_2008_saude.pdfN)
Simon, SD, et al. Projeto Amazona I, GBECAM
Perez E, ate al. J Clin Oncol 32:374, 2014.
* Presumes constant incidence and mortality 2005-2012
Barrios C, et al. JCO, Brazilian Edition, 2015.

Why do Clinical Trials in Latin America?
• The ability to conduct research is essential to the development of a high quality, sustainable, health system
• Motivations of each stakeholder may differ• Government, Institutions, Pharma, Patients,
Physicians, others
• Everyone has something to gain

In their paper “Clinical Trials Infrastructure as a Quality Improvement Intervention in Low and Middle Income Countries”, Denburg and colleagues address an important and very pragmatic issue with potential transforming impact in health care systems in low and middle-income countries (LMICs). They hypothesize of a clinical trials infrastructure effect that could impact patient care unrelated and outside the constraints of direct clinical research participation.
This infrastructure is broadly defined by the authors as being the organizational culture, systems and expertise that develop as a product of participation in cooperative clinical trials. This would lead to quality improvements within a specific institution that could also be extended to the overall health care system resulting in better outcomes potentially benefiting other patients independent of their individual participation in trials. They further hypothesize, escalating the impact of the notion, that creating this infrastructure may represent a pillar of health care system development.

Why do Clinical Trials in Latin America?
• The questions (hypotheses) that need to be addressed to improve care in low resource settings frequently differ from those that are given highest priority in high resource settings
• More than half of all cancer is in developing countries – this represents a valuable, but largely untapped source of potentially unique knowledge of value to all

Saturation of Clinical Trial Sites
RegionNumber of Trial Sites
(per 1M Population)
US 82
Western Europe 11
Central / Eastern Europe 8
Latin America 2
Asia Pacific < 1
Source: Raps Focus, 2009, Latin American CTAs

Studies Conducted (1996-2016)
Last Update: Jun, 2016
.
71
57
14 1412
8 9
59N=244

Patients Screened/Enrolled
0
500
1000
1500
2000
2500
Screened Enrolled
2420
1553
Last Update: Jul, 2016.



Clinical Research as an Alternative
Porto Alegre, November 2016
The Cancer Epidemic
Carlos H. Barrios, M.D.
Hospital do Câncer Mãe de Deus
PUCRS School of Medicine
Latin American Cooperative Group, LACOG
Porto Alegre, Brazil

Why do Clinical Trials in Latin America?
• With Clinical Trials we offer State of the Art medical management to patients that may not have any access or the basic resources to receive even the most basic care.

In their paper “Clinical Trials Infrastructure as a Quality Improvement Intervention in Low and Middle Income Countries”, Denburg and colleagues address an important and very pragmatic issue with potential transforming impact in health care systems in low and middle-income countries (LMICs). They hypothesize of a clinical trials infrastructure effect that could impact patient care unrelated and outside the constraints of direct clinical research participation.
This infrastructure is broadly defined by the authors as being the organizational culture, systems and expertise that develop as a product of participation in cooperative clinical trials. This would lead to quality improvements within a specific institution that could also be extended to the overall health care system resulting in better outcomes potentially benefiting other patients independent of their individual participation in trials. They further hypothesize, escalating the impact of the notion, that creating this infrastructure may represent a pillar of health care system development.

Clinical Cancer Research• Essential to improve therapeutic
results• “Virtuous Circle” of clinical
research: all involved do benefit• Offers “state of the art” therapy• Qualified investigators and large
number of patients (LA)• Should be a strategic priority• Need to recognize and address
bureaucratic and all other barriers that stall development

• Consider strategies to address discrepancies
• 15-25% of tumors are related to smoking
• Screening for Breast Cancer, CRC, Prostate?,
Lung?...
• Screening and vaccination for Cervical Cancer
• Addressing the Obesity epidemic
• Vaccination against Hepatitis B
• Vaccination against HPV
• Clinical Research
• Other… Danaei G et al. Lancet 366: 1784–1793, 2005
Katz IT, et al. N Engl J Med 354: 1110–1112, 2006
Cavalli F. Nature Clin Practice Oncol, 3:582, 2006
Addressing Cancer Globalization…

CANCER TRIALS (CLINICALTRIALS.GOV)
• ClinicalTrials.gov currently lists 223.743 studies with locations in 190 countries.
• 56.232 studies in Cancer.
Source: www.ClinicalTrials.gov Accessed August 28nd, 2016

CANCER TRIALS (CLINICALTRIALS.GOV)
• ClinicalTrials.gov currently lists 56.232 studies in Cancer.
Source: www.ClinicalTrials.gov Accessed August 28nd, 2016
4,5%
53,7%

Clinical Cancer Research in South America - 2016
World 56.232
South America 1.378 (2.4%)
Argentina 572Brazil 977 (1.7%)Chile 285Colombia 207Ecuador 24Peru 278Uruguay 25Venezuela 44
Source: www.ClinicalTrials.gov Accessed August 28nd, 2016

2698
1575
1069
966903
670
664
619
544
530
424
364
328306
261244
219 194141140133127
Breast
Prostate
Skin
Colorrectal
Lung
Stomach
Uterus
Thyroid
Cervix
Head and Neck
LNH
Sarcoma
Melanoma
Larynx
Esophagus
Kidney
Brain
Pancreas
Mieloma
Luekemia
LH
Hepatic
New Cases of Cancer
LACOG Members Institutions
Number of new cases per month = 13.119

Challenges and Perspectives
Porto Alegre, November 2016
Breast Cancer in Latin America
Carlos H. Barrios, M.D.
Hospital do Câncer Mãe de Deus
PUCRS School of Medicine
Latin American Cooperative Group, LACOG
Porto Alegre, Brazil

• LA-Caribbean region
• A complex region of 600 million people, 33 countries and 14 territories
• 320mi (54%) have no health-care coverage
• Factors behind exclusion from health care:
• Language barriers, unemployment, underemployment, geographic isolation, low education levels and health illiteracy
• For the poorest populations:
• Even in the context of free health care, limited access by the inability to pay medication costs, lack of affordable transportation, inconvenient clinic operation and long waiting times
Goss P, et al. Lancet Oncol, 2013, 14:391
Latin American Facts

Lee B, Liedke P, Barrios CH, et al. Lancet Oncol, 2012; 13:e95.
Latin American Facts

Lee B, Liedke P, Barrios CH, et al. Lancet Oncol, 2012; 13:e95.
Latin American Facts

• Region will be overwhelmed by cancer over the next 2 decades resulting in:
• Significant human suffering
• A sharp rise in costs
• Cancers are diseases of ageing people
• By 2020 in LA >100 million people > 60 years
• By 2030: 1∙7 million new diagnoses and 1 million deaths/y
Goss P, et al. Lancet Oncol, 2013, 14:391
Statement of the Problem: Cancer Control in LA and the Caribbean

Statement of the Problem: Cancer Control in LA and the Caribbean
Projection of Cancer Incidence Burden 2012-2030
Bray F, Piñeros M. Cancer patterns, trends and projections in Latin America and the Caribbean: a global context. Salud Publica Mex 2016;58:104-117.International Agency for Research on Cancer. WHO Cancer Mortality Database [accessed on November 17, 2015].
Available at: http://wwwdepiarc fr/WHOdb/WHOdb htm 2014.
Public 75%
Public 40%
6.2% LMIC
Goss P, et al. Lancet Oncol, 2013, 14:391
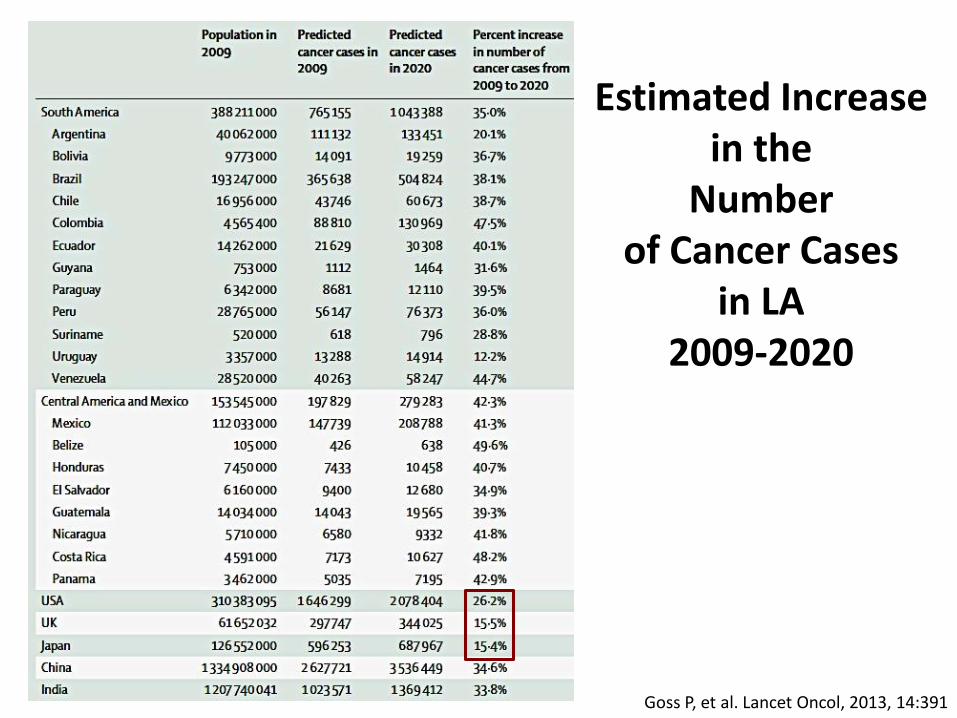
Estimated Increase in the
Number of Cancer Cases
in LA 2009-2020
• Cancer in LA
•Less frequent than US (163 vs. 300/100.000)
•But overall mortality/incidence ratio is 60% higher (0.59 in LA vs. 0.35 in US)
•Largely (but not only) because of more advanced disease at diagnosis
Statement of the Problem: Cancer Control in LA and the Caribbean
Goss P, et al. Lancet Oncol, 2013, 14:391

PRINCIPAIS CAUSAS DE MORTE EM PORTO ALEGRE (FONTE: SECRETARIA MUNICIPAL DE SAÚDE DE PORTO ALEGRE, 2014.)
Nº MORTES POR CAUSA DE NEOPLASIAS – ULTIMOS 7 ANOS
PRINCIPAIS CAUSAS DE MORTENº MORTES POR DOENÇAS CARDIOVASCULARES – ULTIMOS 7 ANOS
NOS ULTIMOS 7 ANOS EM PORTO ALEGRE, AS MORTES POR DOENÇAS CARDIOVASCULARES APRESENTARAM
QUEDA DE 4,11%, ENQUANTO AS MORTES POR NEOPLASIAS CRESCERAM EM 12,64%.
26.4%
22.9%

Breast Cancer in Latin America
• Breast cancer is the most common cancer and kills more women than any other tumor type.
• In 2012 more than 114,900 women were diagnosed and 37,000 women died from Breast Cancer.
• If current trends continue, by 2030, the number new diagnosis will increase 46% and the mortality will reach 78.000 cases a year.
• Breast Cancer cases are projected to increase to over 595,900 and breast cancer deaths to over 142,100 by 2030 in the Americas.
PAHO, Fact Sheet Breast Cancer, 2014.GLOBOCAN 2012. Available from: http://globocan.iarc.fr.
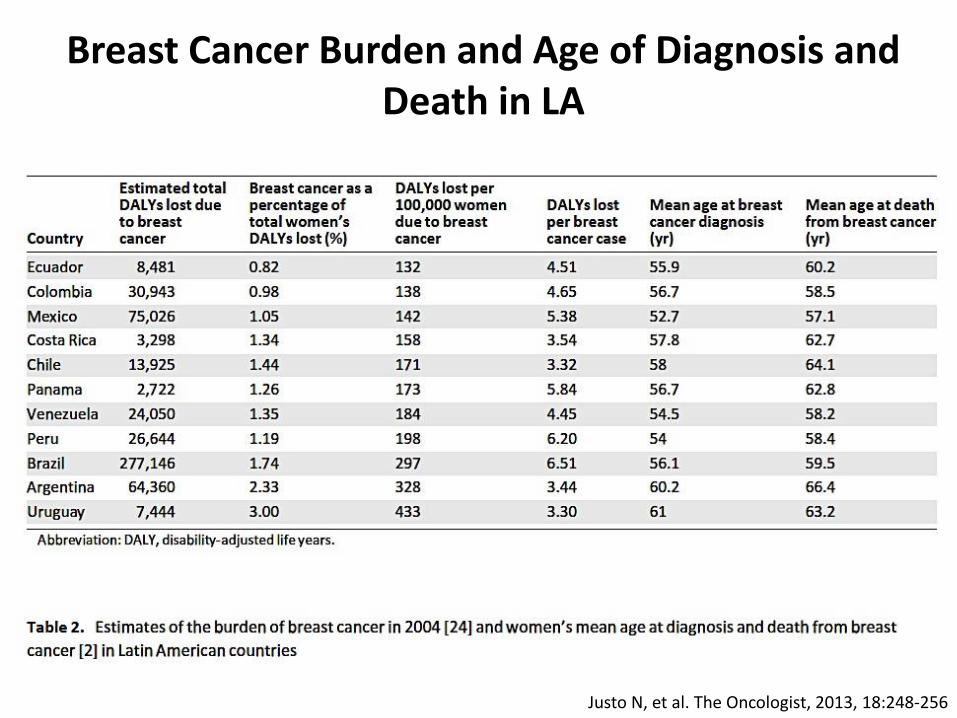
Justo N, et al. The Oncologist, 2013, 18:248-256
Breast Cancer Burden and Age of Diagnosis and Death in LA

Delays in Diagnosis of Breast Cancer in Latin America
• Studies from Brazil and Mexico, showed that the average delay between presentation to a doctor and diagnosis of BC was around 6-7 months.
• In Peru the delay has been estimated in 4-5 months.
• Delays in diagnosis of longer than 12 weeks are considered to affect stage and consequently outcomes and survival
Amadou A, et al. Salud Publica Mex 2014;56:547-554

Mammography Screening in Latin America
A Review of Breast Cancer and Outcomes in Latin America, PAHO

Justo N, et al. The Oncologist, 2013, 18:248-256
Breast Cancer Stage at Diagnosis in LAThe reduced survival is partly due to the fact that around 30%-40% of patients are diagnosed in stages III and IV

Outcomes of Breast Cancer in Latin America
A Review of Breast Cancer and Outcomes in Latin America, PAHO, 2010.
• BC prognosis has improved significantly over the last 50 years.• 5 year survival rates are now over 85% in countries with best outcomes. • In LA, data on survival is scarce and fragmented
• Available information shows a wide disparity across and within countries. • Only in a few countries 5-year survival surpasses 70%

Bray F, Piñeros M. Cancer patterns, trends and projections in Latin America and the Caribbean: a global context. Salud Publica Mex 2016;58:104-117.International Agency for Research on Cancer. WHO Cancer Mortality Database [accessed on November 17, 2015].
Available at: http://wwwdepiarc fr/WHOdb/WHOdb htm 2014.
INCIDENCE MORTALITY
Despite the scarcity of cancer registries, we estimate that in most countries, breast cancer incidence and mortality are increasing.
Trends in BC Incidence and Mortality
ASR per 100.000

Breast Cancer in Latin America: Mortality
A Review of Breast Cancer and Outcomes in Latin America, PAHO
• If current trends continue, by 2030, the number new diagnosis will increase 46%. • Breast Cancer cases are projected to increase to over 595,900 and breast cancer
deaths to over 142,100 by 2030 in the Americas.

The Lancet. Published Online November 26, 2014http://dx.doi.org/10.1016/S0140-6736(14)62038-9
Central analysis of population-based registry data
Individual tumour records from 279 population-based cancer registries67 countries for 25.7 million adults (age 15–99 years) and 75 000 children (age 0–14 years) diagnosed with cancer during 1995–2009
Stomach, Colon, Rectum, Liver, Lung, Breast, Cervix, Ovary, and Prostate in adults, and Adult and childhood Leukemia.

Caveat:Only 6% of the Latin American population is covered by PBCRs compared with 96% of the US population and 32% the EU population. The Lancet. Published Online November 26, 2014
http://dx.doi.org/10.1016/S0140-6736(14)62038-9
1995-1999
2000-2004
2005-2009
78.2% (73.5-82.8)
86.9% (84.3-89.5)
87.4% (84.8-90.0)
Breast Cancer in LA – 5 year survival

Breast cancer deaths registered in the MortalityData System (SIM/WHO) and census data on the resident population collected by the Brazilian Institute ofGeography and Statistics (IBGE/WHO)

Breast Cancer Mortality to Incidence Ratios
Goss P, et al. Lancet Oncol, 2013, 14:391Lee B, Liedke P, Barrios CH, et al. Lancet Oncol, 2012; 13:e95

All Cancer Mortality to Incidence Ratios
Curado MP, et al. Annals of Global Health 2014;80:370-377.
The ratio between mortality and incidence in LatinAmerica is 0.59, higher than the European Union (0.43)and the United States (0.35), which reflects better support ofcancer treatment in developed countries.

New Technologies/Drugs Uptake in Latin America
• In Latin America, uptake of new treatments is slow, almost marginal in some countries.
• This is related with the health care systems’ coverage limitations.
A Review of Breast Cancer and Outcomes in Latin America, PAHO

BREAKDOWN OF SALES OFNEW MEDICINES (2009-2013)
3%9%
10%
55%
23%
Source: IMS Health MIDAS, April 2014.EFPIA, European Federation of Pharmaceutical Industries and Associations, 2014.
88%

Breast Cancer in Latin America
• The economic burden of Breast Cancer is significant, and it can be clearly observed that countries allocate insufficient resources to tackle the disease.
• Women go undiagnosed, uncared for or treated with suboptimal therapies; which results in high morbidity and the associated societal costs.
• Vast inequities exist in access to BC health care in the region and within countries which translates in unequal results in BC outcome.
A Review of Breast Cancer and Outcomes in Latin America, PAHO

Women Children Men Total
First Class
Women (servants)
Died: 4 (0)
Survived: 113 (24)
% Survived: 97% (100%)
First Class
Children
Died: 1
Survived: 6
% Survived: 86%
First Class
Men (servants)
Died: 104 (10)
Survived: 55 (2)
% Survived 34% (17%)
First Class
Total
Died: 119
Survived: 200
% Survived: 63%
Second Class
Women (servants)
Died: 13 (0)
Survived: 78 (1)
% Survived: 86%
Second Class
Children
Died: 0
Survived: 25
% Survived: 100%
Second Class
Men (servants)
Died: 135 (4)
Survived: 13
% Survived: 8% (0%)
Second Class
Total
Died: 152
Survived: 117
% Survived: 43%
Third Class - Steerage
Women
Died: 91
Survived: 88
% Survived: 49%
Third Class - Steerage
Children
Died: 55
Survived: 25
% Survived: 31%
Third Class - Steerage
Men
Died: 381
Survived: 59
% Survived: 13%
Third Class - Steerage
Total
Died: 527
Survived: 172
% Survived: 25%
www.encyclopedia-titanica.orgwww.ithaca.edu/staff/jhenderson/titanic.html

Public 75%
Public 40%
Health Expenditure by Country: (% of GDP by
Private and Public Sectors)
6.2% LMIC
Goss P, et al. Lancet Oncol, 2013, 14:391

Low and Middle Income Countries Spend
Less in Cancer ControlMedical Cancer Control spending per new cancer diagnosis
Numbers represent economic burden per cancer patient in US$ (and as a
percentage of GDP/Capita)
Adapted from: 1. Economist Inteligence Unit. Breakaway: The global burden of cancer— challenges and opportunities [Internet]. 2009. Available de: http://www.livestrong.org/pdfs/GlobalEconomicImpact2. United Nations. Per capita GNI at current prices [Internet]. 2012. Available de: http://data.un.org/Data.aspx?d=SNAAMA&f=grID%3A101%3BcurrID%3AUSD%3BpcFlag%3A13. United Nations. World Population Prospects, the 2010 Revision [Internet]. 2011. Available de: http://esa.un.org/wpp/index.htm4. Lopes G, et al. Nature Rev Clin Oncol 2013.
Central America
and Mexico
$7.39

Public 75%
Public 40%
6.2% LMIC
Goss P, et al. Lancet Oncol, 2013, 14:391
Cost per-patient:
New Cancer Case
in LA 2009

• Cancer represents a significant challenge for
all LA and Caribbean countries.
• The evolving epidemiological transition will
inevitably result in overwhelming human and
financial consequences over the next few
years.
Conclusions
Conclusions
• Breast Cancer represents (and will definitely
remain) a significant burden for the region.
• Significant heterogeneity among and within
countries as well as important gaps in
prevention, screening and treatment are
identified in the LA-Caribbean region.
• Outcomes remain insufficient and require the
active engagement of society and medical
professionals.

Challenges and Perspectives
Porto Alegre, November 2016
Breast Cancer in Latin America
Carlos H. Barrios, M.D.
Hospital do Câncer Mãe de Deus
PUCRS School of Medicine
Latin American Cooperative Group, LACOG
Porto Alegre, Brazil

Source: IMS Health MIDAS, December 2014.Global Oncology Trends Report, 2015.
IMS Institute for Healthcare Informatics.
45 NEW MOLECULAR ENTITIES LAUNCHED 2010-2014 BY INDICATION

Pesquisa Clínica
Pesquisa Clínica
Tratar
Diagnosticar
Manejo de Sintomas Doença
Prevenir
Manejo Eventos
Adversos
• Estudo Clínico
• Experimento Científico: Controlado







