
BENIGN TUMORS OF
BONE Dr. Abdulla Bin-shehna
BENIGN TUMARS OF BONE
1-cystic lesions
2-fibrous lesions
3-cartilaginous lesions
4-benign (occasionally aggressive) bone tumors
5-bone forming tumors
6-miscellaneous bone tumors

Benign bone tumors
Cystic lesions
1- unicameral bone cyst
2- aneurysmal bone cyst
3- ganglion cyst of bone
4- epidermoid cyst

Benign bone tumors Fibrous lesions 1- fibrous cortical defect 2- nonossifying fibroma 3- cortical desmoid 4- benign fibrous histiocytoma 5- fibrous dysplasia 6- osteofibrous dysplasia 7- desmoplastic fibroma 8- giant cell reaction [ giant cell reparative
granuloma]

Benign bone tumor
Cartilaginous tumors
1-osteochondroma
2- multiple osteochondromatosis
3- chondroma
4- multiple enchondromatosis [Ollier disease]

Benign bone tumors
Benign [occasionally aggressive] tumors
1- giant cell tumor
2- chondroblastoma
3- chondromyxoid fibroma
4- langerhans cell histocytoma
Benign bone tumors
Bone forming tumors
- Ostioid osteoma
Benign bone tumors
Miscellaneous benign tumors
1- neural tumors
2- vascular tumors
3- fatty tumors
Unicameral [simple bone]cyst Occurs in childhood, rare in adults, more in males Most in prox. Humerus or prox. Femur Two forms: - active - inactive In their fluid has been reported PGE2 Malignant transformation has been reported asymtomatic unless fracture is present Obliteration after healing of fracture X.Ray : lytic lesion Treatment: -curettage with or without bone graft. -aspiration followed by instillation of . .
Methylprednisolone - F.I.N

Unicameral bone cyst

Technique of aspiration instillation

Pathological fracture :healing :remodling

Bone cyst after injection – fluid level


Treatment by intramedullary flexible nails

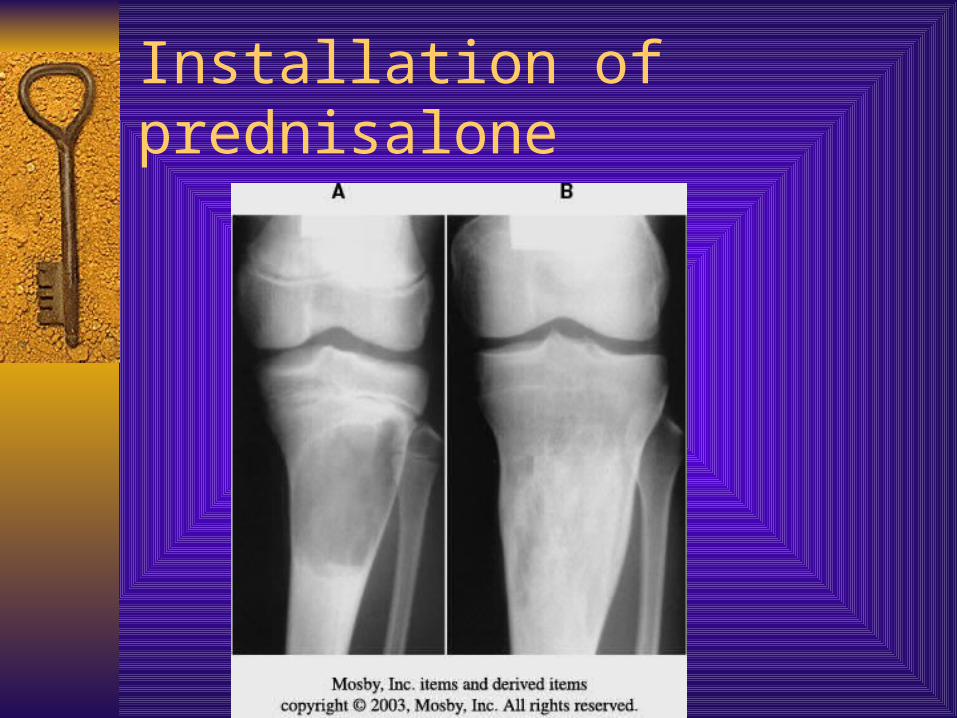
Installation of prednisalone
Aneurysmal bone cyst Occurs in any age, common in young adults Located centrally X.Ray: lytic lesion have a honeycamb shape C.T: location & size – M.R.I: fluid levels Biopsy: to diff. Between G.C.T or Osteosarcoma Grow rapidly Treatment: curettage & bone grafting Recurrence approx. 25% Vertebral lesions treated surgically



Aneurysmal B.C of prox. Ulna, excision and large bone grafting

Aneurysmal bone cyst of phalange
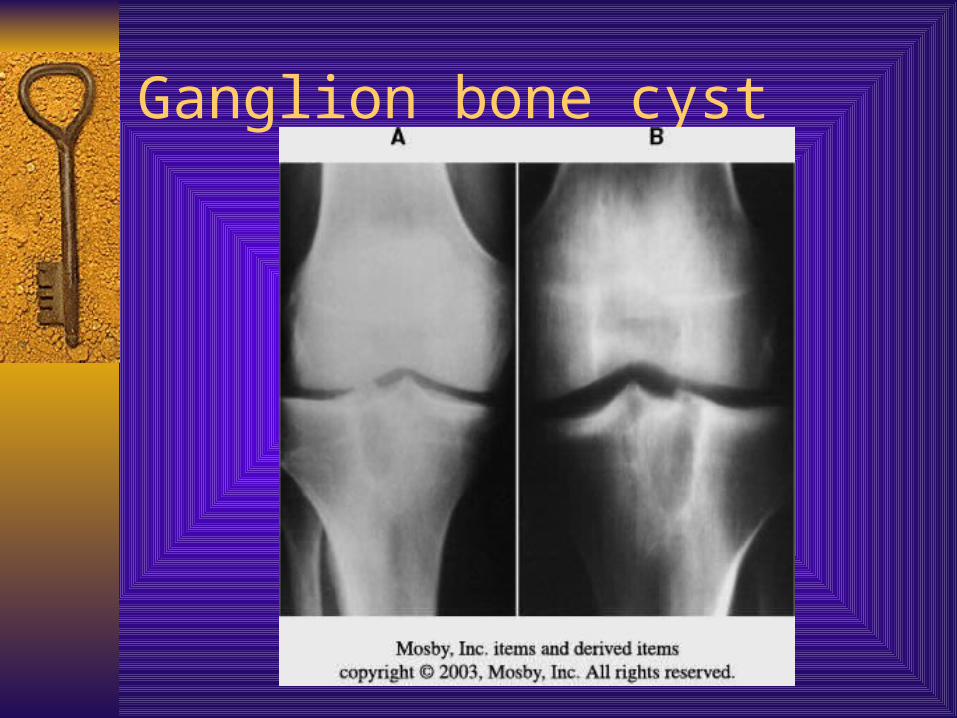
Ganglion cyst of bone
X.Ray: well-demarked lytic defect with thin rim of sclerotic bone
Treatment: curettage
Ganglion bone cyst

Epidermoid cyst
Filled with keratinous material & lined with squamous epithelium

Epidermoid cyst
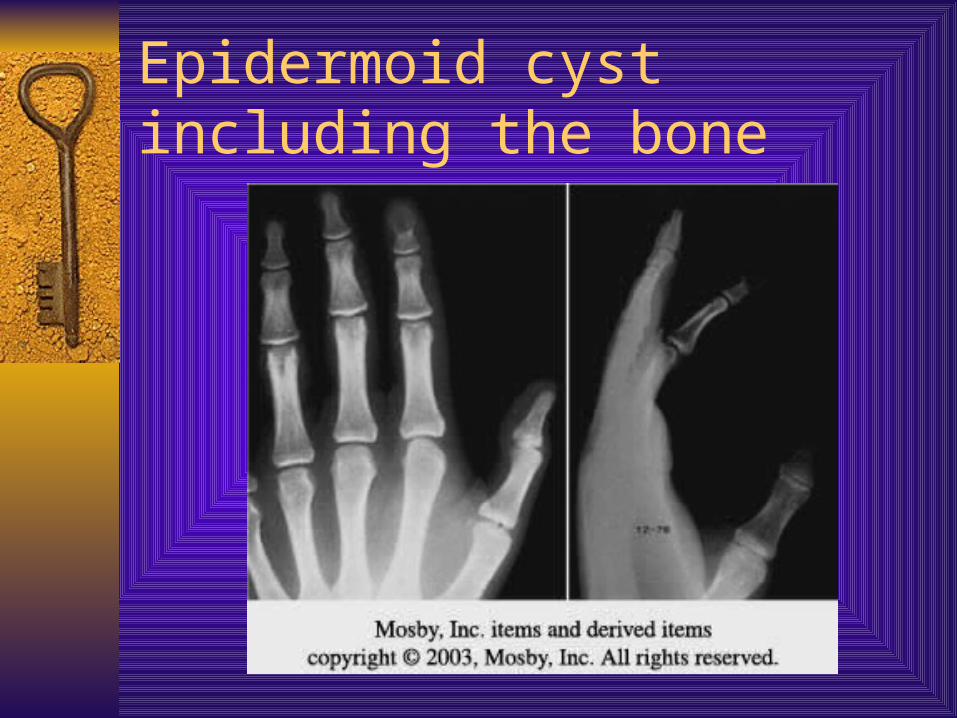
Epidermoid cyst including the bone
Fibrous lesions Fibrous cortical defect [non – ossifying fibroma] - developmental abnormalities - the common benign in children , more in males - generally occurs in the metaphysial region of long bones
[ femur, tibia] - multiple F.C.D occurs approx. in 50% of cases - x.ray: circular or oval with low radio lucent & margins
well - defined thin rim of sclerosis - def. Diagnosis : G.C.T , fibrous dysplasia , xantogranuloma - treatment: F.C.D not necessary –N.O.F curettage & bone
grafting

F.C.D

Non-ossifying fibroma ???!

Fibrous lesions
Cortical desmoid [ periosteal desmoid] - assymptomatic irregularity in
posteriomedial aspect of distal femoral metaph.
- large lesions give symptoms: soft tissue swelling- pain
- x.ray: oblique view 20-40 deg. Externally & lesion appears as erosion of cortex with sclerotic base
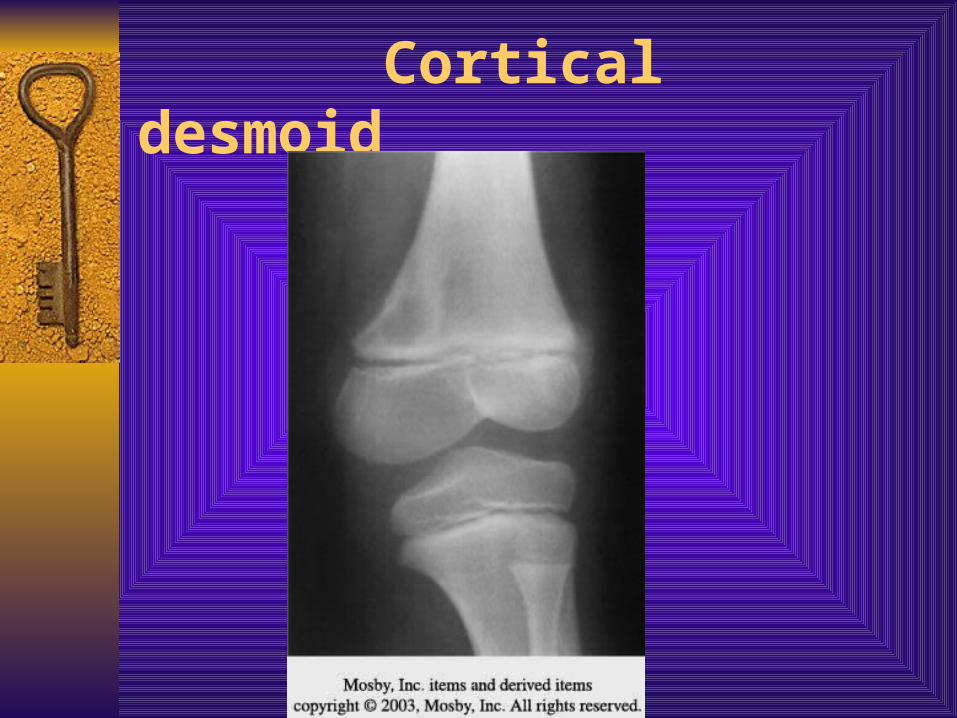
Cortical desmoid

Fibrous lesions
Benign fibrous histocytoma - occurs most in soft tissues & less common in bones - similar to that of nonossifying fibroma histologically - more aggressive in its biological behavior & reotegen.
Characteristics - occurs in any part of long bones or in pelvis - occurs in older patients - x.ray: well – defined lytic lesion with little periosteal
reaction - treatment: aggressive curettage or wide exision

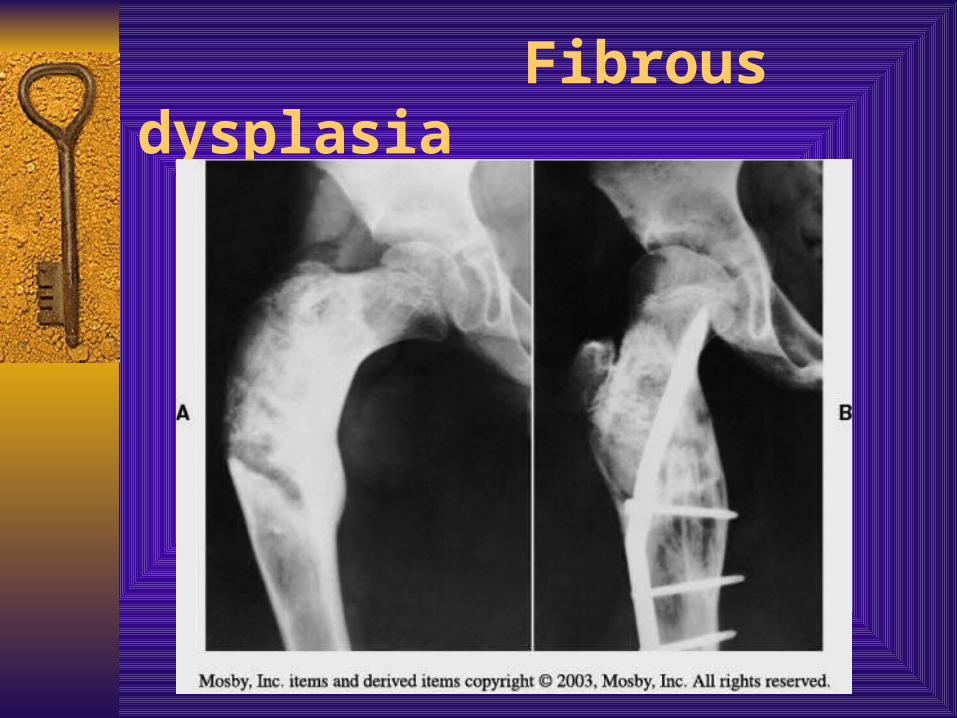
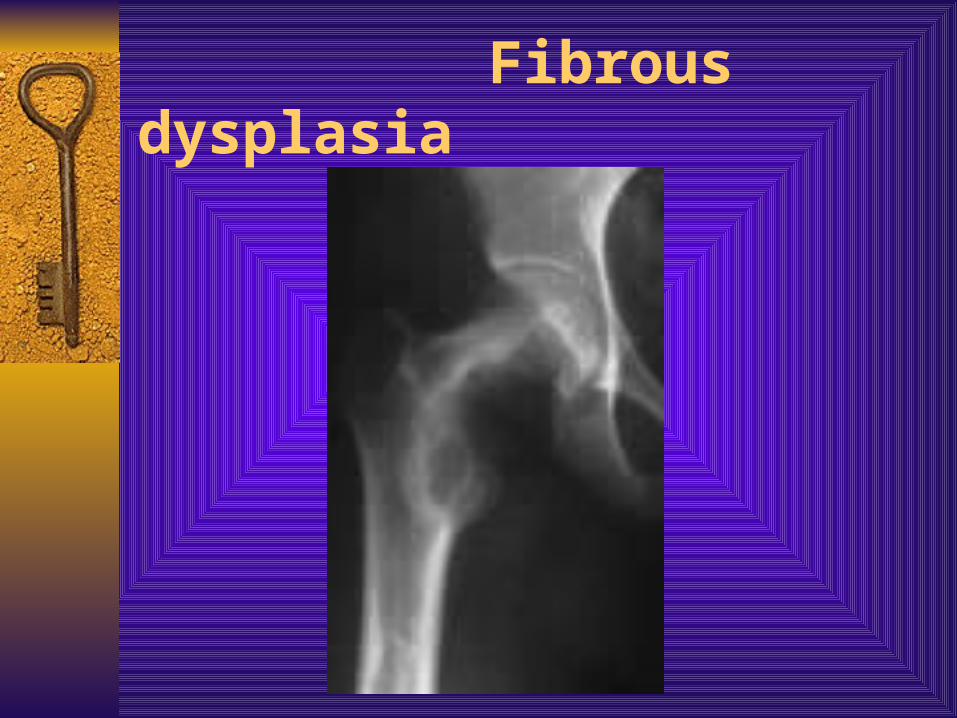
Fibrous lesions fibrous dysplasia - developmental anomaly of bone formation - the hallmark is replacement of normal bone and marrow by fibrous
tissue and small woven bone - occurs in any part of bone - associated abnormalities : sexual precocity- thyroid disease-
abnormal skin pegmentation - large lesion gives: pain, pathological fracture - x.ray: fine & granular area [ ground glass ] - classic sign: shepherd’s crook deformity in prox. Femur - biopsy is necessary - malignant reported - treatment: curettage & bone grafting
Fibrous dysplasia

Fibrous dysplasia
Fibrous dysplasia

Fibrous lesions Osteofibrous dysplasia [ossifying fibroma of long
bones- Campanacci disease - rare lesion, affecting tibia& fibula [usually
diaphysial] - most patients in the first decade- more in boys - clinically: path. Fracture, tibia is enlarged& bowed
anterolaterally x.ray: intra cortical osteolysis with expansion of cortex - treatment: paht. Fractures by cast immobilizing &
curettage + subperiosteal resection in 15 y - deformity corrected by osteotomy
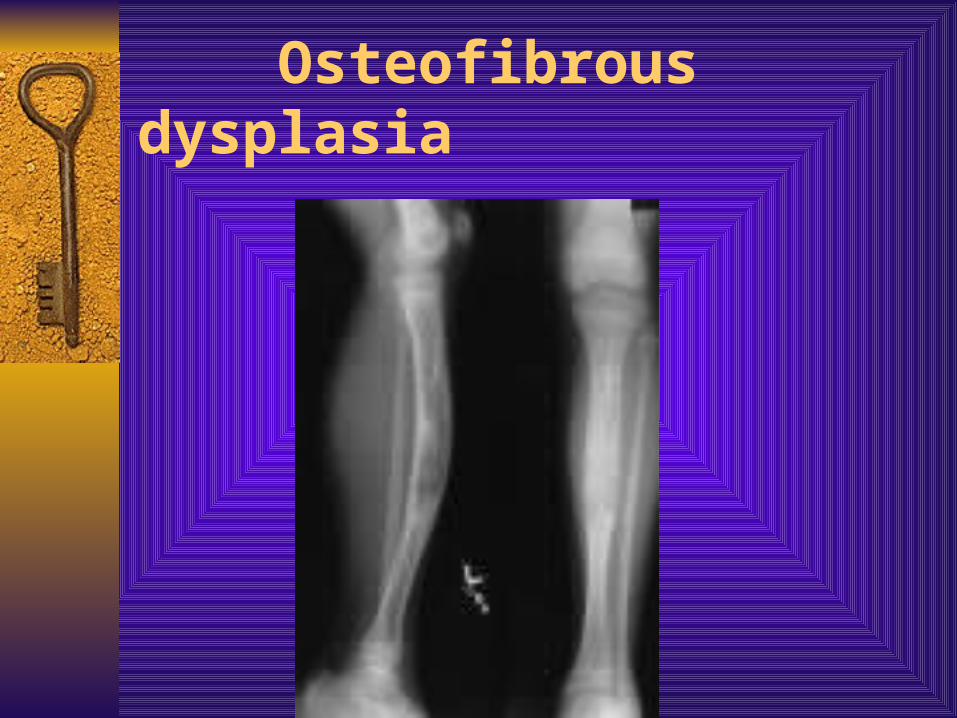
Osteofibrous dysplasia

Osteochondroma- cartilage capped exostosis-the most common of benign tumors; more in males-originate within the periosteum as small nodules-their growth usually stopped when skeletal maturity is
reacted-clinically: mass or pain-x-ray: 2 types; stalked & broad based . Calcification
within the cap -the cap usually thin and thicker should be studied
(secondary chondrosarcoma)-treatment: surgery in large lesions or produce
symptoms or roentgenographic features suggest malignancy
-Recurrence is rare-spontaneous disappearance has been reported

osteochndroma

Osteochondroma of radius
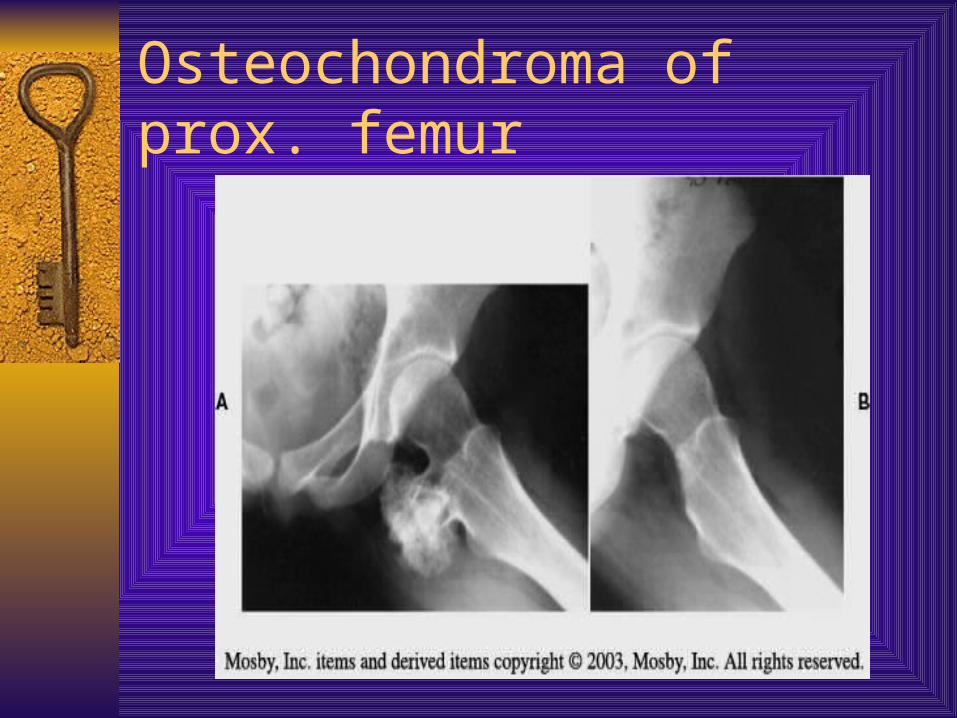
Osteochondroma of prox. femur

Intaarticullar osteochondroma of femur

Osteochondroma of hand

Cartilaginous tumors
Multiple osteochondromatosis
-The most striking feature is the presence of many exostosis
-caused by anomaly of skeletal development
-most regions involved are about the knees , ankles and scapula
-surgery indicated to remove painful mass, improve joint motion and correct deformity

osteochndromatosis

Cartilaginous tumors Multiple enchondromatosis (OLLIER disease)-rare disease in witch many cartilaginous tumors
appear in both large and small tubular bones and in flat bones
-failure of normal endochondral ossification -located in epiphysis and metaphysisDeformities and shorting resulting from the tumors
including bowing of long bones-associated with hemangiomas disease is known as
MAFFUCCI disease-50% malignant transformation-treatment: more obvious deformities can be corrected
by osteotomy
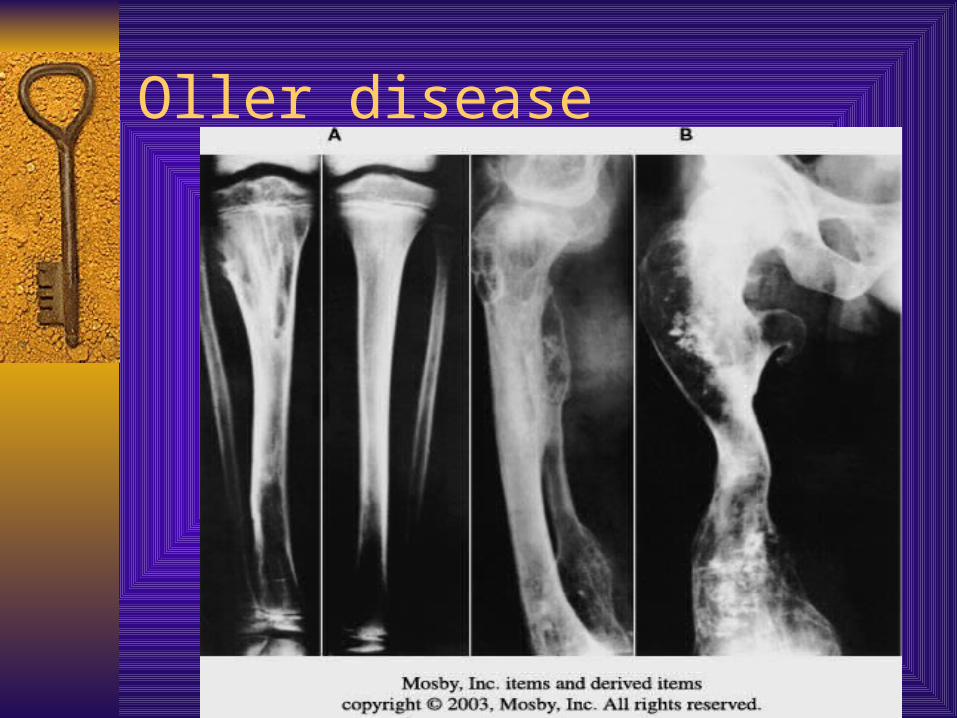
Oller disease

Cartilaginous tumors Chondroma (including enchondroma and
periosteal chondroma)-chondromas are less common than osteochondromas -occur third & forth decades located centrally in
small bones of hands and feet-some times referred to as cart. Hamartoma-asymptomatic and seen incidently or after path.
Fracture-x-ray: low radiolucent appears as well
circumscribed with small foci of calcification-signs of transformation to malignant tumor is; age >
30 , pain , increasing mass, cortical lysis-treatment: curettage and bone grfting , periosteal
chondroma should be excised en bloc
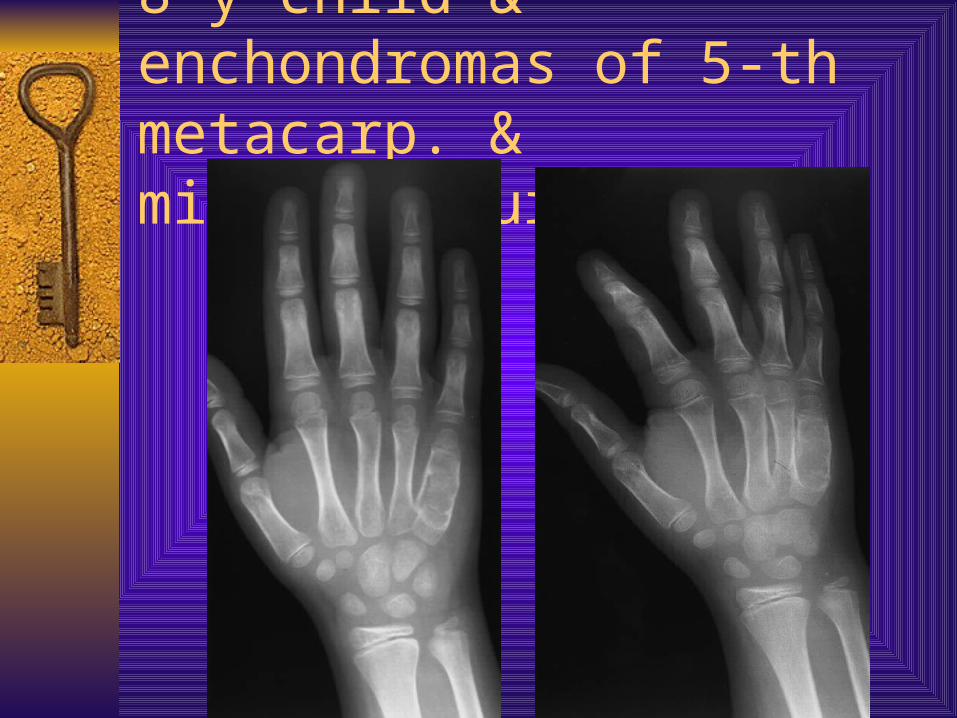
8-y child & enchondromas of 5-th metacarp. & microfracture
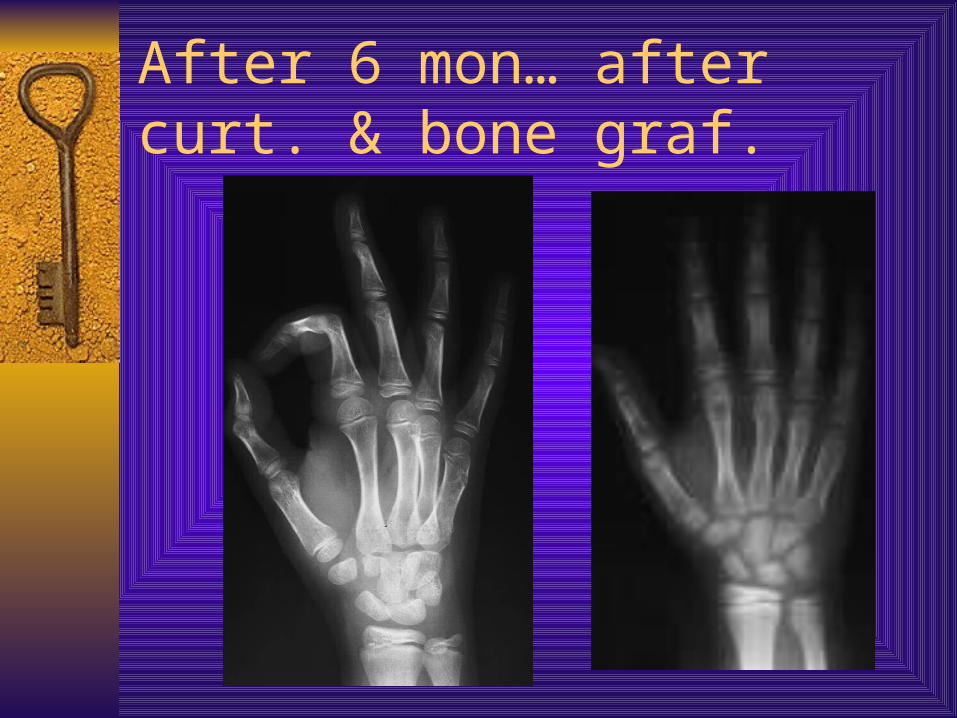
After 6 mon… after curt. & bone graf.
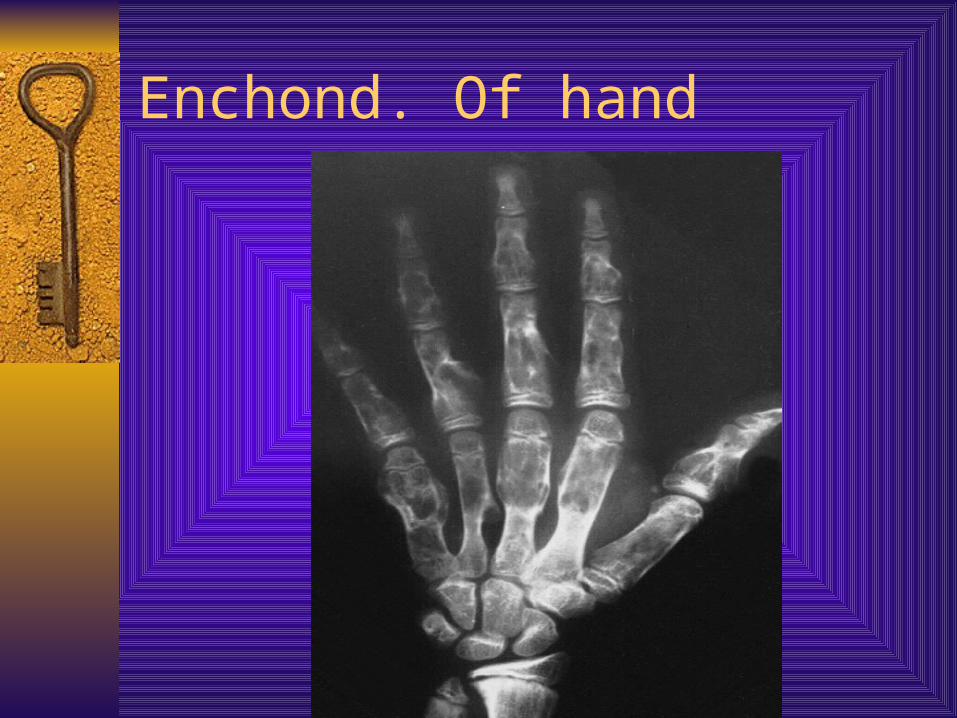
Enchond. Of hand



Enchond. Of femur,& after curettage
Gaint cell tumor-occur in mature long bones(dis. femur & prox. Tibia),
in age 20-40 and rarely in adolescent-located in epiphysis abut subchondral bone-pulmonary metastases occur in 3% of pat.-pul. Metas. May have spontaneous regression or lead
to death-path. Fractures occur in 10-30%-x-ray: purely lytic lesion and expands through cortex .
Malignant expands to soft tissues-MRI; determine the extent of the lesion-treatment: extended curettage with phenol or argon
beam arthroplasty or aethrodesis may be indicated=radiation may be used for inoperable lesions(spine ,
pelvis)


GCT of medial condyle

After curettage and bone cement

GCT excision and arthrodesis


GCT of 5-th. Metatarsal bone
Benign(occasionally aggressive) bone tumors
Chondroblastoma-rare, typically occur in patients ages, 10-20y, more in
males. Most common sites; dis. Femur & prox. Tibia-clinically ; pat. C\O progressive pain that may mimic a
chronic synovitis-x-ray; well-circumscribed lytic lesion centered in
epiphysis of long bones surrounding rim bone. May be located in apophysis such as greater trochanter
-it is usually present as stage 2 , less aggressive than GST
- treatment: extended curettage & bone grafting or cement
- -recurrence treated as primary- -pulmonary metas. Occur approx. in 1%.

Chondroblastoma associated with aneurysmal bone cyst

Chondroblastoma of g.trochanter curettage & prevented fixation

Chondroblastoma in intracondyl notch
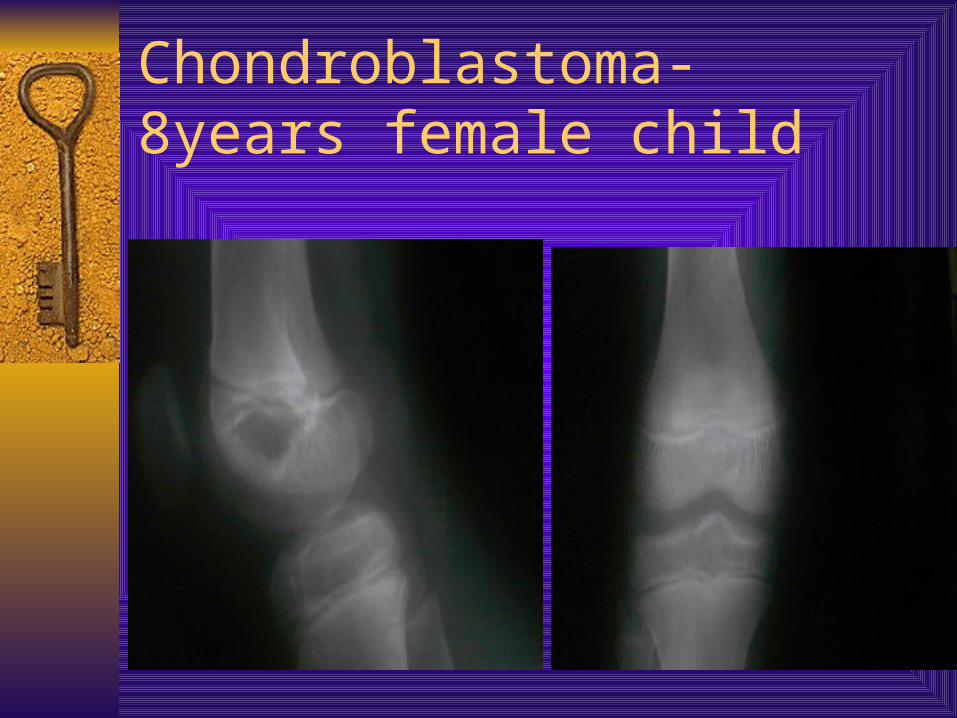
Chondroblastoma- 8years female child

Benign (occasionally aggressive) bone tumors Chondromyxoid fibroma-occur in any age most in (10-30y)-any bone involved but the prox. Tibia is the most
common-clinically: patients c\o pain if the lesion located in
hands or feet, or painless mass-x-ray; well-circumscribed lytic lesion with rim of
sclerosis.,.-may have bubbly appearance-treatment: wide resection or extended curettage-malignancy is rare.. Diagnosed rontegengraphiclly.

Osteoblastoma-is a rare bone forming tumor-occur in age 10-30y more in males. In metaphysis or diaph.-50% of lesions occur in spine-clinically: pain most common symptom, similar as osteod
osteoma(worse at night and relieved by NAID)-in the spine; painful scoliosis and symptoms of root compression-x-ray; the classic appearance is calcified central lesion
surrounding halo and reactive sclerosis-it have low-grade aggressiveness-treatment; extended curettage of wide resection ; sometimes
radiation in spinal lesions.

Langerhans cell histiocytosis-it is group of diseases with similar pathologic features;(eosinophilic
granuloma, Christian disease and Letterer-Siwe) Eosinophilic granuloma-pat. Ages 5-20y-clinical picture as osteomyelitis-occur in any bone ,but common in vertebral bodies-x-ray; vertebra plana and the lesion purely lytic may have hole within
hole-lesions in long bones similar as Ewing sarcoma-treatment; most conservatively(including steroid injection) ;
curettage with bone grafting ; radiation ; and surgical decompression and fusion in spine for rapidly progressive neurologic signs.

Eso. Granuloma,& path. Frac. Healed after pin fixation

Langerhans cell histiocytosis- 20y. Male patient

Bone-forming tumors Osteoid osteoma-occur in first three decades, often in young females-any bone can be involved, 50% the femur or tibia-no malignant changes-pain worse at night and relieved by aspirin-when the lesion near a joint, swelling, stiffness and
contracture may occur or scoliosis-x-ray: cortical sclerosis and multicentric fuci . CT, to detect
nidusTreatment: block resection of the nidus CT-guided percutaneous resection-spontaneous disappearance may occur

Os. Osteoma ,& after resection

CT-guide resection
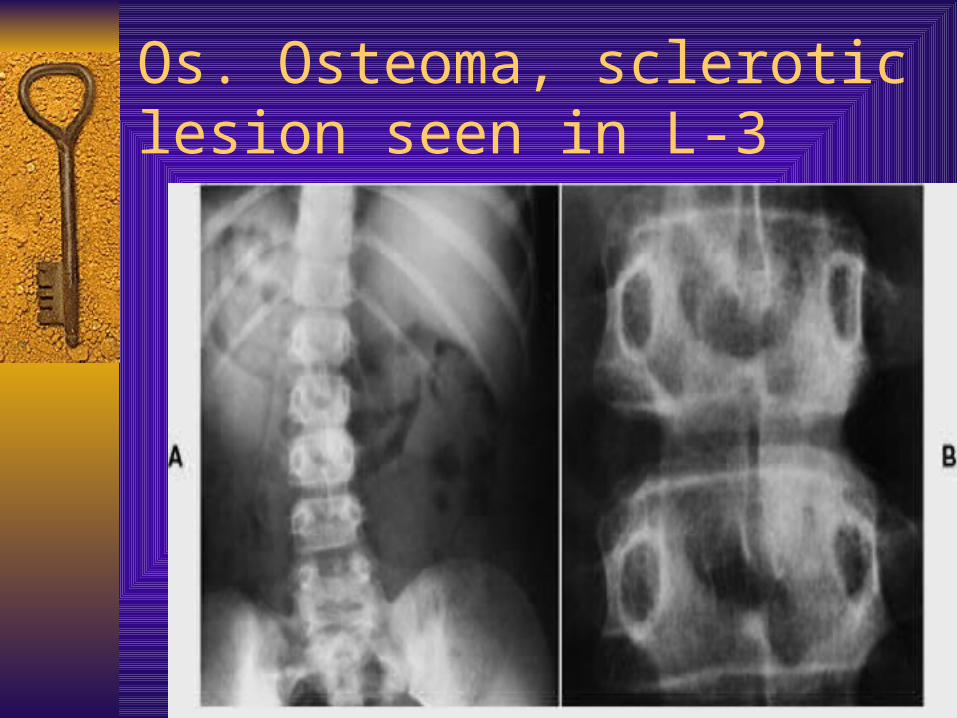
Os. Osteoma, sclerotic lesion seen in L-3


Miscellaneous benign tumors of bone Vascular tumors: hemangioma-is the most common benign vascular tumor-most involve the vertebral body or skull-x-ray: show multiple lytic lesions-treatment: vertebral involvement requair surgery when
neurological function compromised – curettage and bone grafting
radiotherapy Massive osteolysis- disappearing bone disease Cystic angiomatosis Epithelioid hemangioma
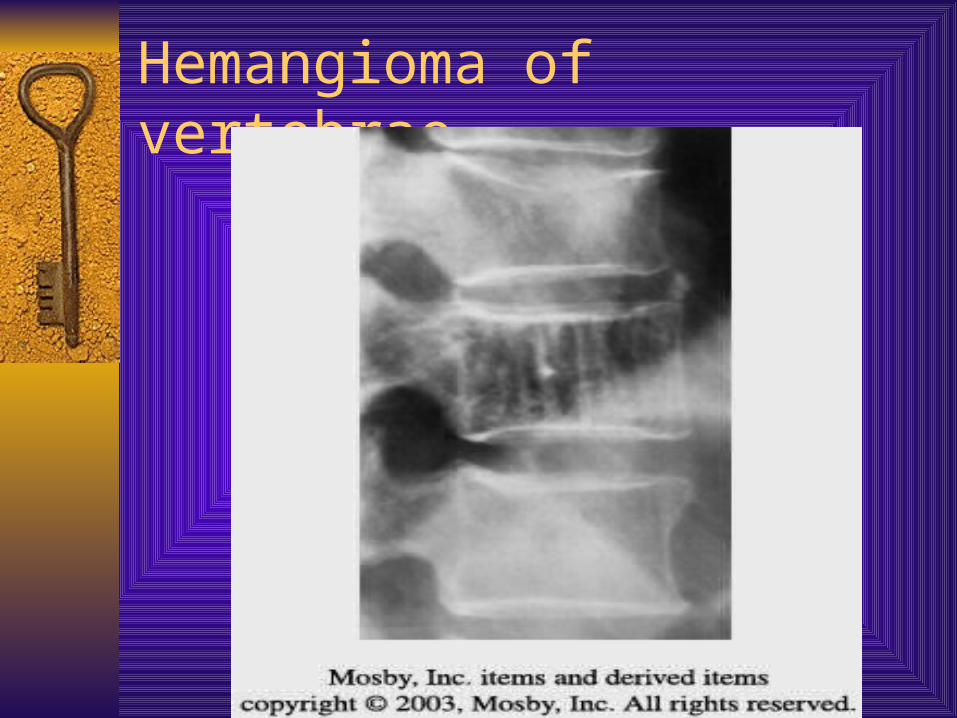
Hemangioma of vertebrae
Neural tumors
Neurofibromatosis
-rare lytic lesion
-develop in bone especially in Von-Recklinghausen disease

THANK YOU

MoKazem.com
من • تقديمها و إعدادها تم محاضرات سلسلة من هي المحاضرة هذه , دمشق مشفى في العظمية الجراحة شعبة في المقيمين األطباء قبل
. . ميرعلي بشار د إشراف تحت• . المحاضرة هذه في الواردة األخطاء عن مسؤول غير الموقع
•This lecture is one of a series of lectures were prepared and presented by residents in the department of orthopedics in Damascus hospital, under the supervision of Dr. Bashar Mirali.
•This site is not responsible of any mistake may exist in this lecture.
كاظم. مؤيد Dr. Muayad Kadhimد







