
THE DOWNFALL TEAM PRESENTS…
Multi-Disciplinary Team Peggy Benenati Risk Management Beverly Campbell Nursing Kim Cerri Quality Roberta Farley Physical Therapy Kelli Farnell Pharmacy Ryan Nadeau Nursing Joan Osborne Education
BE ON THE BALL…PREVENT A FALL!
BHIP Fall Stats FY12: 137 Inpatient falls Rate: 3.2 per 1000 patient days 46th percentile
PROBLEM SELECTION AND GOAL
PROBLEM STATEMENT
Hospital Risks
Cost $16,000 per fall 6.27 more days
Falls Increase Risk!
Patient Risks
Sources: The No Fall Zone, Hospital & Health Networks, 6-1-2013; CDC , www.cdc.gov

SIX SIGMA
ROOT CAUSE ANALYSIS AND PROJECT TOOLS
DMAIC Define, Measure, Analyze, Improve, Control
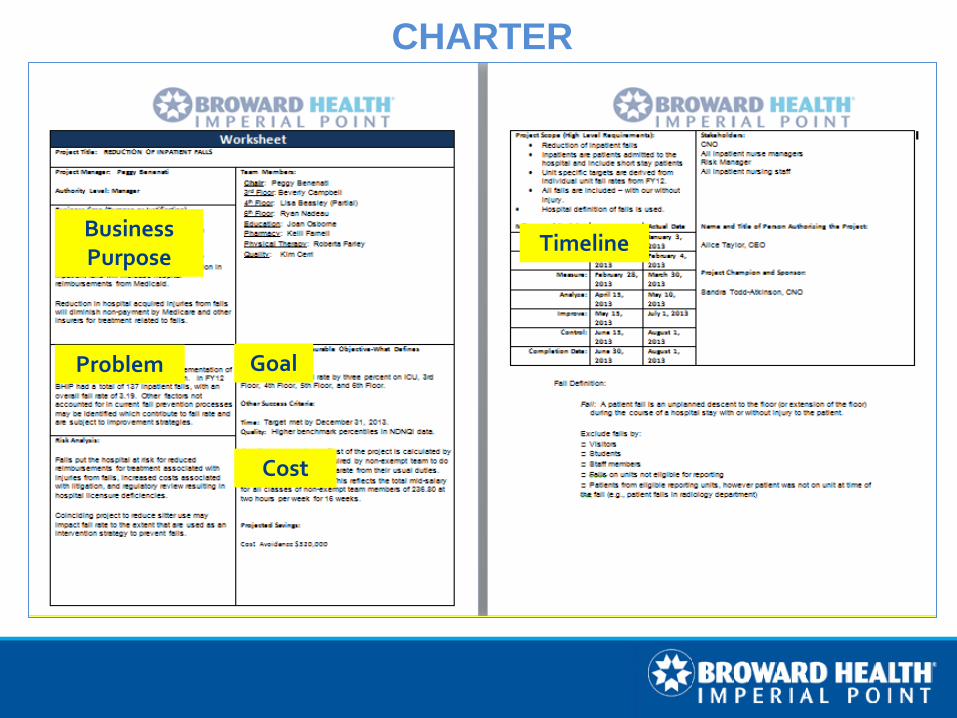
CHARTER
Problem Goal
Business Purpose
Cost
Timeline

Stakeholders CNO Nurse Managers
Communication Plan Project Status Fall reduction is important!
CEO Approval
PROJECT LAUNCH
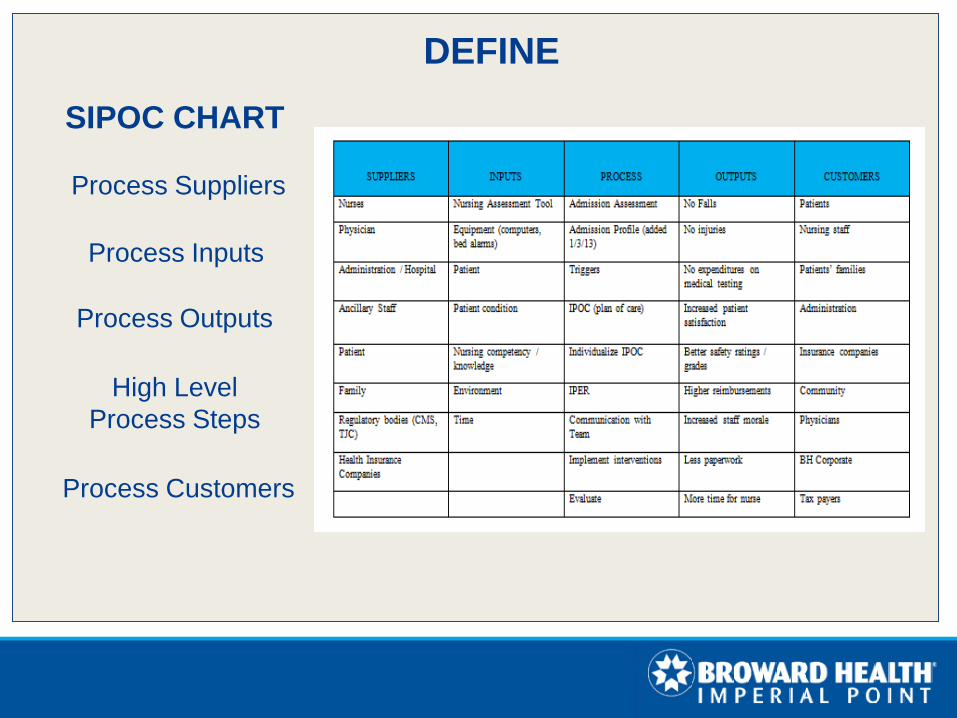
Process Inputs
Process Suppliers
SIPOC CHART
DEFINE
Process Outputs
High Level Process Steps
Process Customers

PROCESS MAP
MEASURE
DATA PROCESS PROBLEM
DOES THE EXISTING DATA REPRESENT THE PROBLEM?

MEASURE SURVEY
• Random Sample • 45 Nurses • Inpatient Units • All Shifts • Likert Scale • Multiple Choice • Narrative Comments
MEASURE
Incident report fall data reviewed and compiled
Survey data reviewed
and compiled
DATA PROCESS PROBLEM

ANALYZE
Descriptive Statistics • 50% of falls occurred during
bathroom or toileting activities • 20% of patients who fell were
not identified at risk
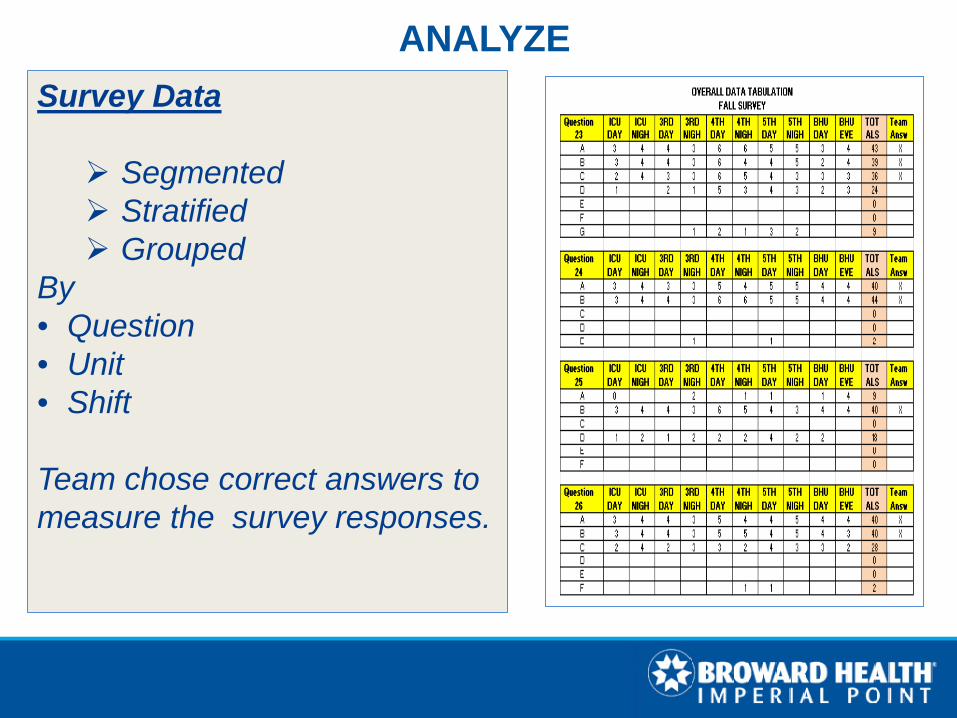
ANALYZE Survey Data Segmented Stratified Grouped
By • Question • Unit • Shift
Team chose correct answers to measure the survey responses.
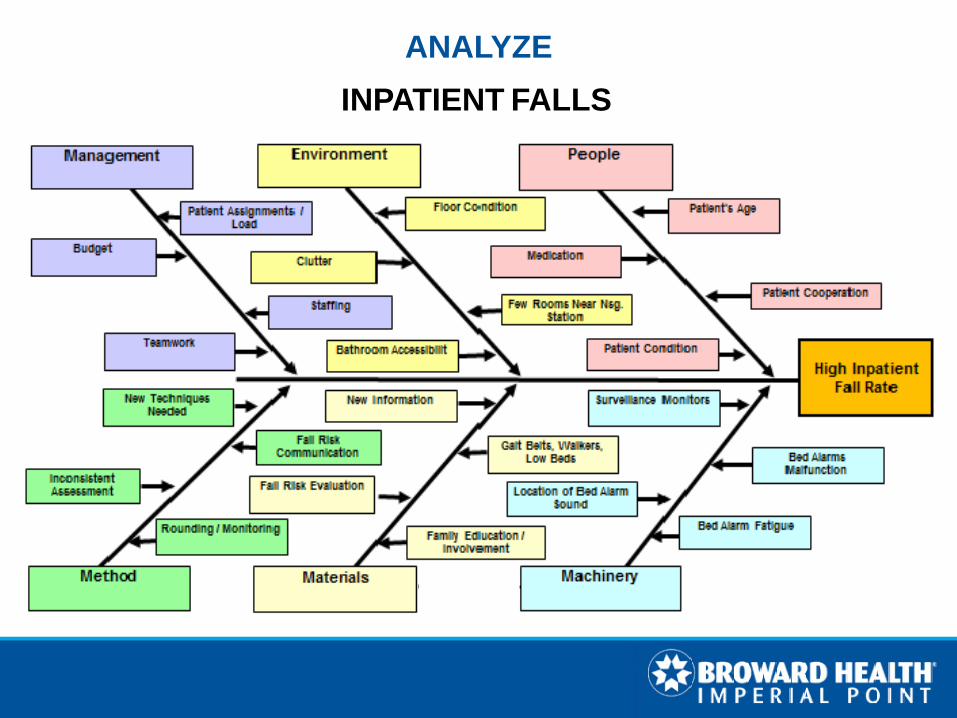
INPATIENT FALLS
ANALYZE
ANALYZE Contributing Factors
Incorrect fall risk assessment Lack of identification of patients at risk for falls Inconsistent use of nursing judgment to initiate the fall
prevention protocol Insufficient communication about patients’ fall risk Lack of patient and family participation in the fall prevention
protocol Inconsistent supervision of patients during bathroom and
toileting activities Variable bed alarm functionality
ANALYZE PRIMARY ROOT CAUSE!
Nurses and patients do not fully understand underlying fall risk factors …. …Resulting in critical barriers to appropriate fall risk identification and effective fall prevention.
IMPROVE AND CONTROL
Strategies to improve and sustain process changes Ensure changes are implemented and adopted as routine

IMPROVE
Multifaceted Approach Systematically address each initial root cause Fix the primary root cause! Twofold Intent Enhance nurses’ understanding of fall risk for better identification Enhance patients’ and families’ understanding of fall risk for better
compliance
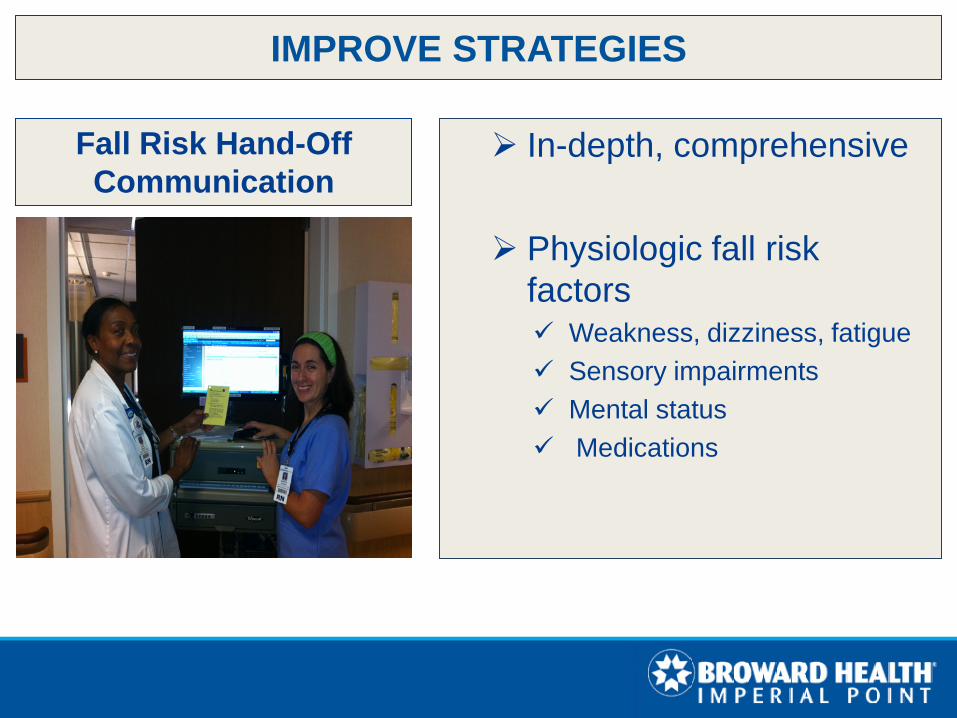
IMPROVE STRATEGIES
In-depth, comprehensive Physiologic fall risk
factors Weakness, dizziness, fatigue Sensory impairments Mental status Medications
Fall Risk Hand-Off Communication

IMPROVE STRATEGIES
INTRODUCING….
THE ABC’S OF INJURY RISK!
AGE
BONES COAGULATION
SURGERY

IMPROVE STRATEGIES Unit Safety Huddles
High Fall Risk Patients Discussed
Comprehensive Post-Fall Evaluation Tool What did the patient / family say? What were the risk factors? What caused or contributed? Was the patient appropriately assessed? Were appropriate interventions in place? What could have been done to prevent the fall?
On the spot analysis and learning!
IMPROVE STRATEGIES

Fall Prevention Critical Concepts Simple statements about proper assessment and use of the
fall prevention process Example: “A secondary diagnosis is any diagnosis in addition
to the admitting diagnosis.”
IMPROVE STRATEGIES
Aligned with shift-hand off communication Enhance patient participation in fall prevention Fall risk is part of the patient’s medical condition
Scripted Teach Back
IMPROVE STRATEGIES

Scripted Rounding Language
Affirmative statement of intent
Encourage patients to use the bathroom
Example: “I am here to take you to the bathroom.”
IMPROVE STRATEGIES
IMPROVE STRATEGIES
RED RULES
Supervision during toileting activities
Bed alarm activated

Improve Bed Alarm Functionality Connect bed alarms to
Cisco Phones Annual Performance
Maintenance for Bed Alarms Wire bed alarms to ring at nursing stations Environmental Services resets bed alarms after making up
beds
IMPROVE STRATEGIES

Fall Risk Shift Hand-Off
1. Is your patient at risk for fall?
2. What is the Morse Fall Scale score?
3. Has your patient fallen during this hospital stay?
• When did the fall occur and what were the circumstances?
• What were the injuries, if any? • How was POC modified?
4. What physiologic factors contribute to the risk?
• Primary and Secondary Diagnoses that cause weakness, dizziness, fatigue, excessive bed rest.
• Four or more medications associated with falls (CIWA protocol, cardiovascular meds, hypoglycemic agents, psychotropics, muscle relaxants, neuroleptics, opioids, sedatives, sleeping aids, antihistamines).
• What are the medication interactions?
• Does the patient have any symptoms or side effects from medications that would increase risk for falls?
• Mental Status (e.g.: confused, disoriented, combative, doesn’t follow directions, lethargic, somnolent).
• Last time patient was toileted?
• Sensory impairments - (vision, hearing, touch (e.g.: diabetic neuropathy).
• Activity level the prior shift - (stayed in bed, up and out of bed, restless).
5. Is your patient at high risk for injury and why?
• Consider ABCS - Age, Bones, Coagulation, Surgery. • Age—Increased age- higher risk. • Bones- Osteoporosis or other conditions that increase
risk of fracture. • Coagulation- Anticoagulation therapy that increases
risk of bleeding- Coumadin, Pradaxa (this does not include VTE prophylaxis with Lovenox).
• Surgery - Recent surgery that increases risk of injury – hip, knee, abdominal surgery.
6. Recommendations to prevent fall and injury from fall.
IMPLEMENTATION HAND-OFF COMMUNICATION

Hand-off Communication and Teach Back
Team members modeled
hand-off and teach back
Unit fall champions Online education
IMPLEMENTATION

Critical Concepts
Safety Huddles
Rounding
Annual competencies
Unit specific implementation
Rounding initiative and live education
IMPLEMENTATION

Monitor and Sustain Improvements
Falls Committee established as subcommittee of the Nursing Quality and Patient Safety Council
Committee review of data and recommendations for improvement.
Second look in June 2014 – Added laboratory initiative for early morning lab draws.
CONTROL

40 % REDUCTION
Reduced Fall Rate from 3.2 to 1.97 10th Percentile!
SIGNIGICANT COST AVOIDANCE

Consistent communication among the team raises fall risk awareness for better prevention!
Critical thinking is required for accurate fall risk assessment!
LESSONS LEARNED
Communicating reasons for fall risk enhances patient and family participation!
PI project done with intensity and focus is far more effective than PI projected done with urgency!
Successful PI project needs accountability for outcomes among the stakeholders!
What you say to encourage patients to use the bathroom really makes a difference!
The process improvement process is just as important as improving the process!

OUR JOURNEY CONTINUES…







