
ARTHRITIS- Current Medical and Surgical Management
•
Dr Jacqueline Andrews
Consultant Rheumatologist
Mr George Whitwell and Mr Campbell Maceachern
Consultant Orthopaedic Surgeons
Leeds Teaching Hospitals NHS Trust
May 9th 2016

What is Arthritis?
• arth - joint
• itis – inflammation
• Arthritis – inflammation of the joint(s).
Types of arthritis- more than 100!
• Non-inflammatory - mainly managed in Primary Care and by Orthopaedic Surgeons
• Inflammatory - mainly managed by Rheumatologists
• Infectious - uncommon
• Haemorrhagic - very uncommon

INFLAMMATORY ARTHRITIS
• Rheumatoid Arthritis (RA)
• Juvenile Idiopathic Arthritis (JIA)
• Spondyloarthropathies (SpA)
• Crystal deposition disease
Ankylosing SpondylitisPsoriatic ArthritisEnteropathic Arthritis- IBDReactive Arthritis
GoutCPPD disease (Pseudogout)

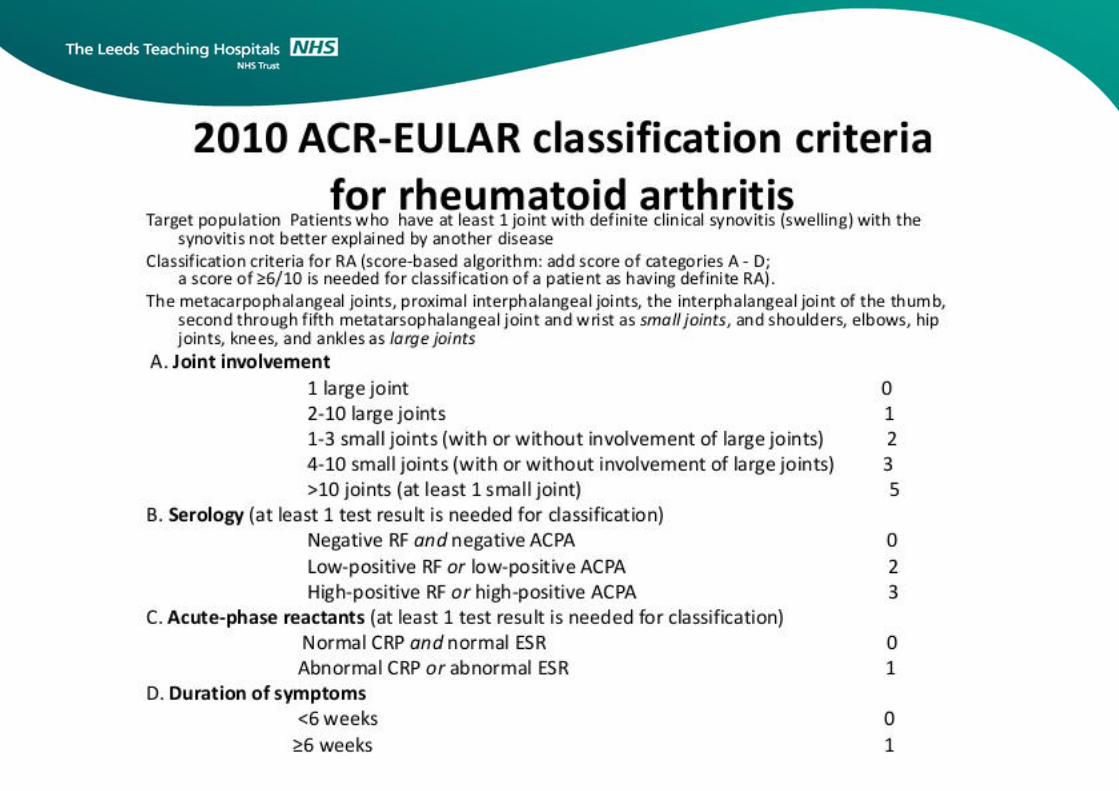
RHEUMATOID ARTHRITIS
• 1% of population
• Females > Males
• Most common during child-bearing years
• Tiredness, weight loss,
• Pain and swelling of joints
• Early morning stiffness

5

1. Stop the Inflammation- prevent damage:
• Traditional disease modifying agents
– Methotrexate, Sulphasalazine, Hydroxycholorquine, Leflunomide
• Biologics- target individual molecules involved in inflammation pathways
– Anti “tumour necrosis factor” (TNF) drugs: adalimumab, certolizumab, etanercept, infliximab.
– Other biologics target different proteins: abatacept, rituximab, tocilizumab
2. Rehabilitation and prevent co-morbidities:
Occupational therapy, Physiotherapy, Podiatry, Psychology
Annual review- cardiovascular risk, bone health, immunisation check etc
3. Reconstruct –surgery increasingly uncommon
RA - TREATMENT

SPONDYLOARTHROPATHIES (SpA)
1. Ankylosing Spondylitis
2. Psoriatic
3. Enteropathic (IBD)
4. Reactive Arthritis

Diagnostic Testing
Share common features:
• Joint, back and eye inflammation, rashes, digestive disorders
• Associated with the HLA B27 gene
• no diagnostic laboratory testing
• But some typical X-Ray appearances – eg “pencil in cup” appearance

Ankylosing Spondylitis (AS)
• Causes inflammation and eventually fusion of the spine and the spinal joints.
• Involvement of peripheral joints and eye also common.
• Causes pain, stiffness and decreased spinal mobility
• Incidence ranges from 0.1 to 1 percent of population
– Men are affected 3 X more than women
– Commonly develops age 15 to 40

Management of AS
Education
Exercise
Physiotherapy
Rehabilitation
NSAIDs
Peripheral
disease
Spinal
disease
Sulfasalazine
TNF blockers
A
n
a
l
g
e
s
i
c
s
Local corticosteroids
S
u
r
g
e
r
y
Zochling J, et al. Ann Rheum Dis.

Psoriatic Arthritis
Likely in up to 25-34% of patients with psoriasis
Incidence in population around 1%
Males =Females
Peak age of onset between 30-55 years
“enthesitis” (inflammation at site of tendon insertion)
“tenosynovitis” (inflammation of tendon and its enveloping sheath)
“dactylitis “ (“sausage digit”)
Treatment:
- Methotrexate very effective for skin and joints
- Biologics increasingly used in severe disease
- New oral treatment - Apremilast

CRYSTAL DEPOSITION DISEASES
GOUT
• Disorder of purine metabolism
• Leads to deposits of urate crystals in joint and surrounding tissues “tophi”
• 2 Types: – Primary (95%): inherited disorder with overproduction or under excretion of
urate
– Secondary (5%): due to underlying medical condition (blood or kidney disorder)
• 20 times more common in men than women
• Foot, ankles, hands, wrists and elbows most commonly affected

GOUT- treatment
Acute Attacks:- treat quickly!
• Indomethacin and other anti-inflammatories (NSAIDS)
• Colchicine
• Steroids- tablets, injections
Chronic disorder:
• Adjust diet (low purine)
• Drugs- Allopurinol, Colchicine

PSEUDOGOUT- aka CPPD disease
• Caused by inflammation due to deposits of calcium pyrophosphate dihydrate (CPPD) crystal- mimics gout
• More common in later life and if suffer from Osteoarthritis
• Most often affects the knee and the wrists
• X-rays show calcium deposits in cartilage andsurrounding tissues
• Treatment- similar to gout

Rheumatology at Leeds Teaching Hospitals NHS Trust
• EULAR (European Rheumatology Society) Centre of Excellence in Rheumatology since 2005
• Chapel Allerton Hospital facilities
– Ward C2 - 20 bed ward shared with Dermatology
– Day Care Unit C5 - 5,00 patient visits per year-new extended hours
– Outpatient Suite - 35,000 patient visits per year
– Others - Physiotherapy (hydrotherapy), Occupational Therapy
Podiatry, Research Facilities
• St James’s University Hospital:
– Inpatient beds
– Outpatient Clinics
• Wharfedale Hospital:
– Outpatient Clinics
• 24 hour 7 day on-call medical service

Rheumatology Research at Leeds
• The Leeds Musculoskeletal Biomedical Research Unit (LMBRU) is an NIHR funded centre of excellence for musculoskeletal research, established in 2008
• A partnership collaboration between the Leeds Teaching Hospital Trust and the University of Leeds which has led to:
– developing and trialling new treatments (especially Biologic agents) for Inflammatory Arthritis
– blood tests to aid the early diagnosis of Rheumatoid Arthritis
– new imaging methods to diagnose arthritic conditions earlier and more accurately
• Research –it’s important- how you can get involved!
– LMBRU Patient and Public Involvement Group
– Established 2009 > 120 active members
– THANK YOU

Hip and Knee
Osteoarthritis
Mr Campbell Maceachern
Mr George Whitwell
Consultant Orthopaedic Surgeons
Chapel Allerton hospital Leeds

Chapel Allerton Orthopaedic Centre
• Opened 12 Years ago
• 9 joint replacement surgeons
• 4 Specialist Orthopaedic Theatres
• 1400 hip and knee joint replacements per year
• Dedicated outpatient suite with pre-assessment clinics
• Dedicated multidisciplinary teams

NON - INFLAMMATORY ARTHRITIS
OSTEOARTHRITIS
Osteoarthritis, is also known as osteoarthrosis or degenerative joint disease
Progressive disorder of the joints caused by gradual loss of cartilage resulting in pain and
reduced function.


Types of Osteoarthritis
• Primary / Idiopathic (most common)
• Secondary
– Trauma
– Infection, Rheumatoid, Gout
– Vascular
– Neuropathy
– Haemophilia
– Metabolic
What Causes Primary Osteoarthritis
• Ageing?– Undeniably related– Why do some 90 year olds not have it?
• Overuse– Related to job – manual labourers– Obesity– (Secondary – due to recurrent microtrauma)
• Genetic– Increasing evidence of genetic component– Tends to run in families

• Pain – Worse on movement and at end of day
• Stiffness – Stiff after rest, but improves with movement
• A grating or grinding sensation
• Swelling – The swelling may be hard (bone spurs) or soft (extra fluid)
• Reduced Function
– Feeling of instability
– Reduced range of movement
– Less Strength
Symptoms of Osteoarthritis

• Very common
• 8.5 million people in UK symptomatic
• True incidence far higher (>80% in over 70s)
• Women > Men
• Increasing with ageing population
How Common is it?
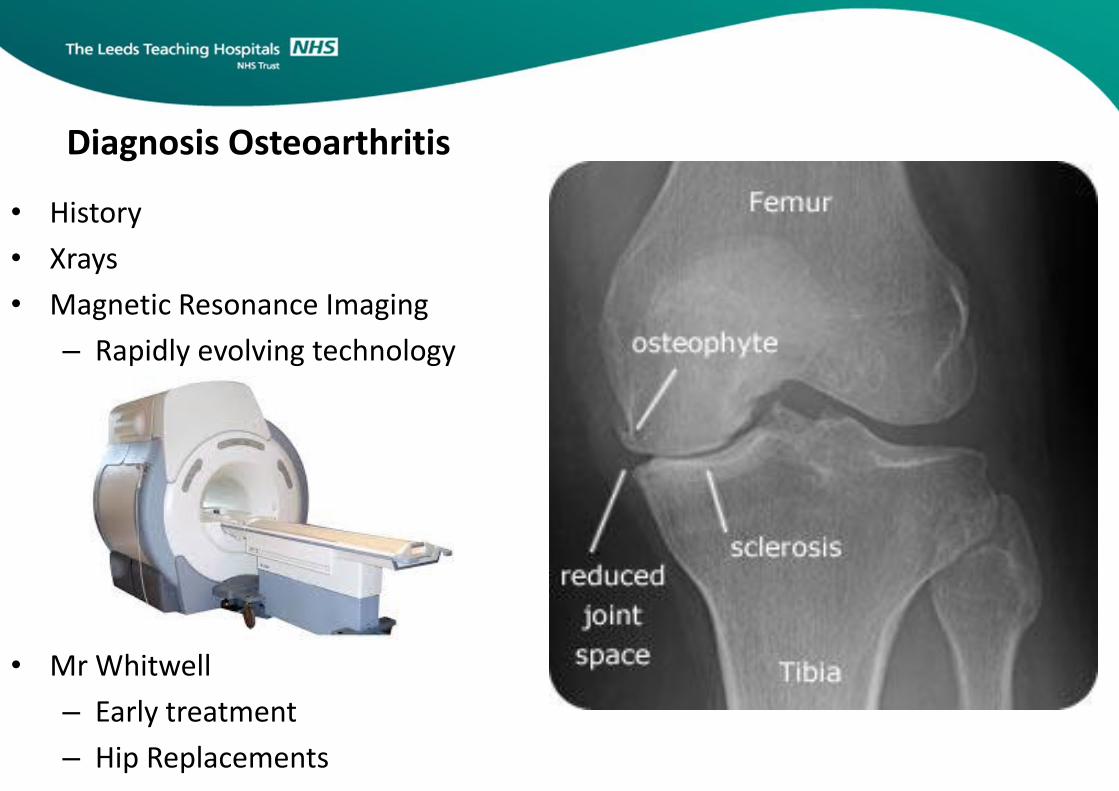
• History
• Xrays
• Magnetic Resonance Imaging
– Rapidly evolving technology
Diagnosis Osteoarthritis
• Mr Whitwell
– Early treatment
– Hip Replacements

Conservative Treatment
Physiotherapy and exercise regimes
• Increase muscle strength and tone
• Increase joint movement
• Improve stability
• Postural advice
• Improve general fitness

Conservative treatment
Weight loss -
- Activity modification
May 9th 2016

Medical treatment

Medical Treatment
• Injections
– Steroids
– Hyaluronic acid ?

Arthroscopy
May 9th 2016

Arthroscopy
May 9th 2016

Knee Arthroscopy
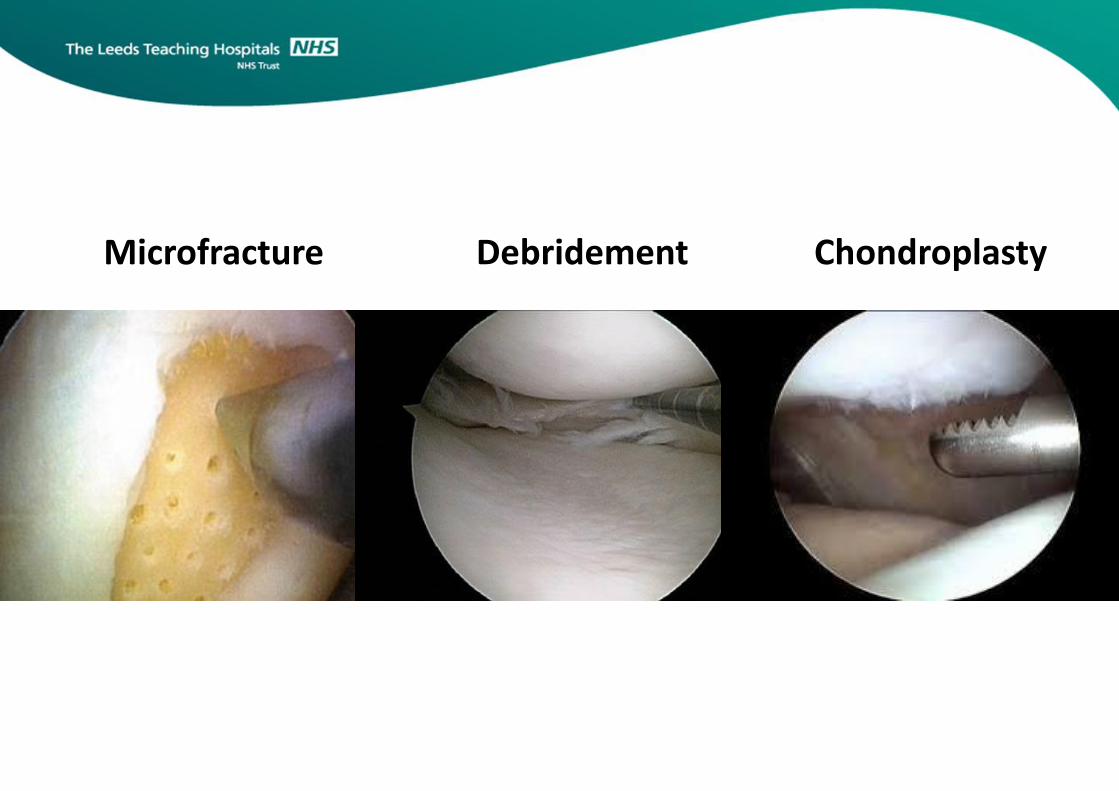
Microfracture Debridement Chondroplasty
Hip replacements
• First performed 1960’s
• 60,000 performed annually in UK
• Over 90% last patients lifetime
• “Operation of the century”
• All UK operations are now entered on NJR

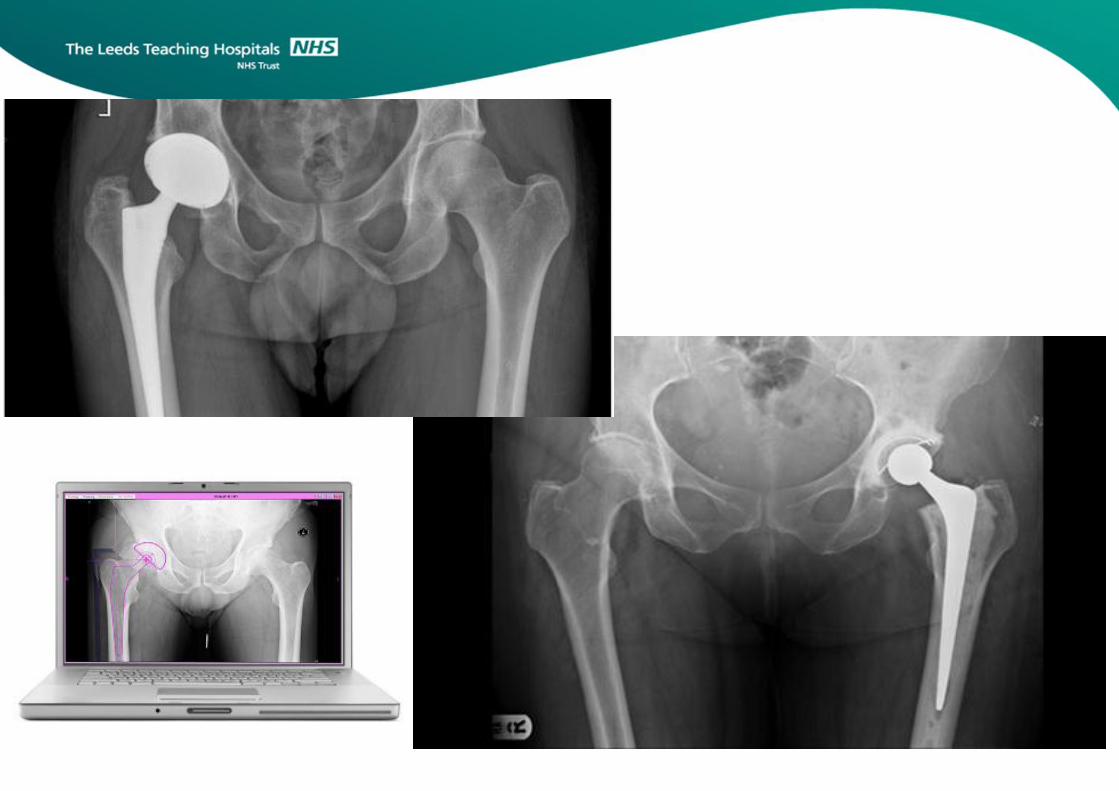
Hip replacements
• Spinal anesthetic
• Average hospital stay 3.5 days
• Patients walking around day of surgery
• Complication rates < 1%

Hip Replacements
May 9th 2016

Hip replacement
May 9th 2016

Hip Replacements
May 9th 2016

Hip Replacements

Surgical Treatment of Knee Arthritis
– When non-surgical and minimally invasive techniques fail to relieve symptoms
– Consider Joint Replacement
• Partial Knee Replacement
• Total Knee Replacement
– Pain is severe
– Function and quality of life is significantly impaired

Consider previous Xray
demonstrating Arthritis
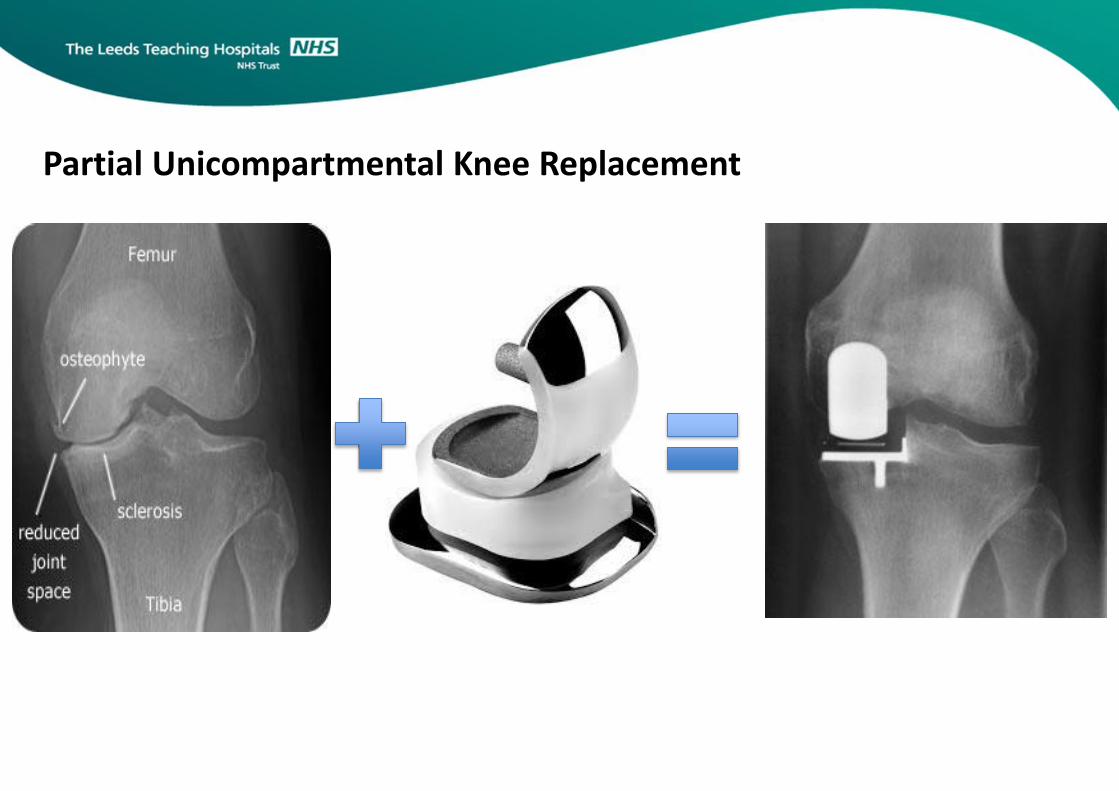
Partial Unicompartmental Knee Replacement

Partial Knee Replacement
• Benefits
• Feels like native knee
• Very good function
• Faster recovery
• “Forgotten Surgery”
• Drawbacks
• Remainder of knee remains susceptible to arthritis
• 2.5% of all patients will require revision to full knee replacement 7-10 years later

Total Knee Replacement

Total Knee Replacement
• Benefits
• Very good at reducing pain and improving daily function
• Pain significantly reduced in 90% of patients
• Drawbacks
• Often doesn’t feel like native knee
• Kneeling can be difficult in 50% of patients
• Mechanical joints can wear out
– May need a revision procedure

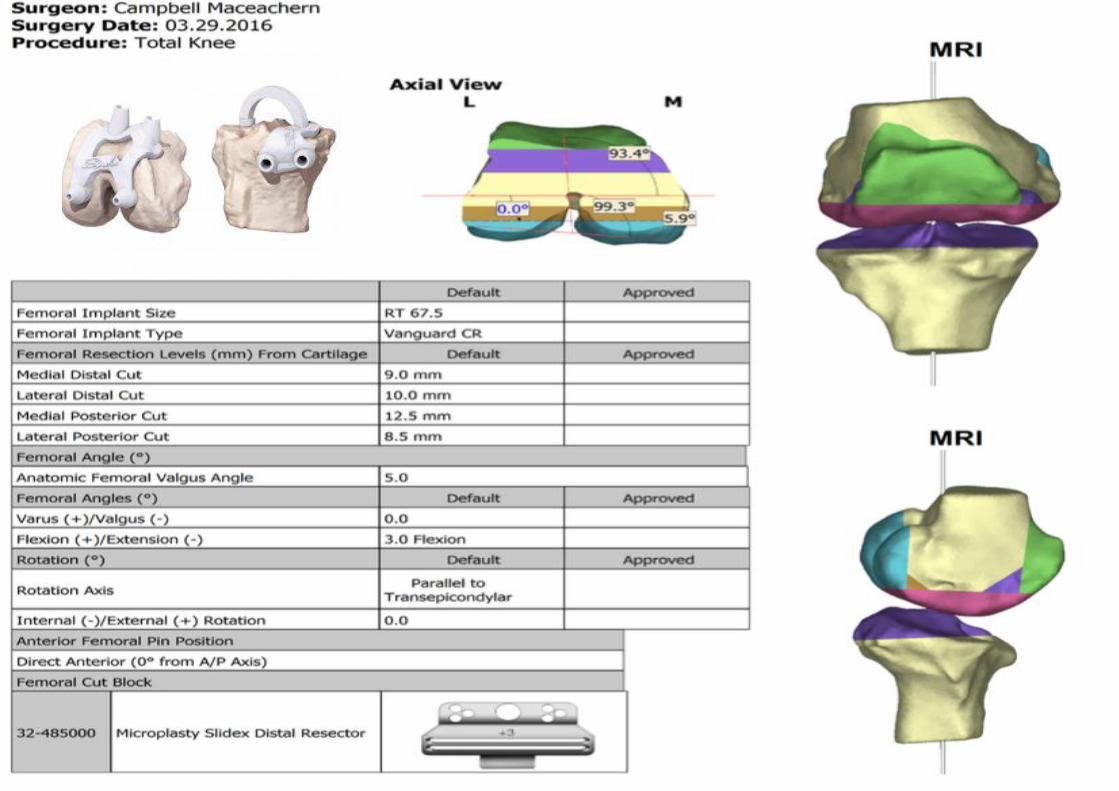
Total Knee Replacement - Advancements
• Templating
• Import x-rays computer interface
• Allows accurate measurements
– Ensure precise fitting implants
• Custom Patient-Specific Technology
• Using MRI or CT
• Very precise custom jigs are 3D printed
• Used during the operation for precise implant placement
• Very useful for grossly abnormal anatomy
Knee MRI






![Original Article[7] ThefreeDictionary.com Arthritis in turn citing. [8] Wollenhaupt J, Zeidler H. "Undifferentiated Arthritis and Reactive Arthritis". Current Opinion in Rheumatology](https://cdn.vdocuments.us/doc/165x107/613ca4354c23507cb63583bf/original-article-7-thefreedictionarycom-arthritis-in-turn-citing-8-wollenhaupt.jpg)

