Download - Antagonist or agonist
Antagonist ……..is the answer
Dr Santosh Gupta MS,FRM
Consultant Reproductive Medicine Manipal Ankur Reproductive Services
Evolving human wisdom
Use of antagonist is also evolving in the hands of doctors worldwide
IVF : Miracle of millennium
From 1978 till today…………….
• Natural cycle IVF
• 1980s learned the ART of LH surge control by GnRH agonist
• IVF became a global phenomenon “ BUT” a chapter of IVF related complications opened

Emergence of new Super HERO “ ANTAGONIST”

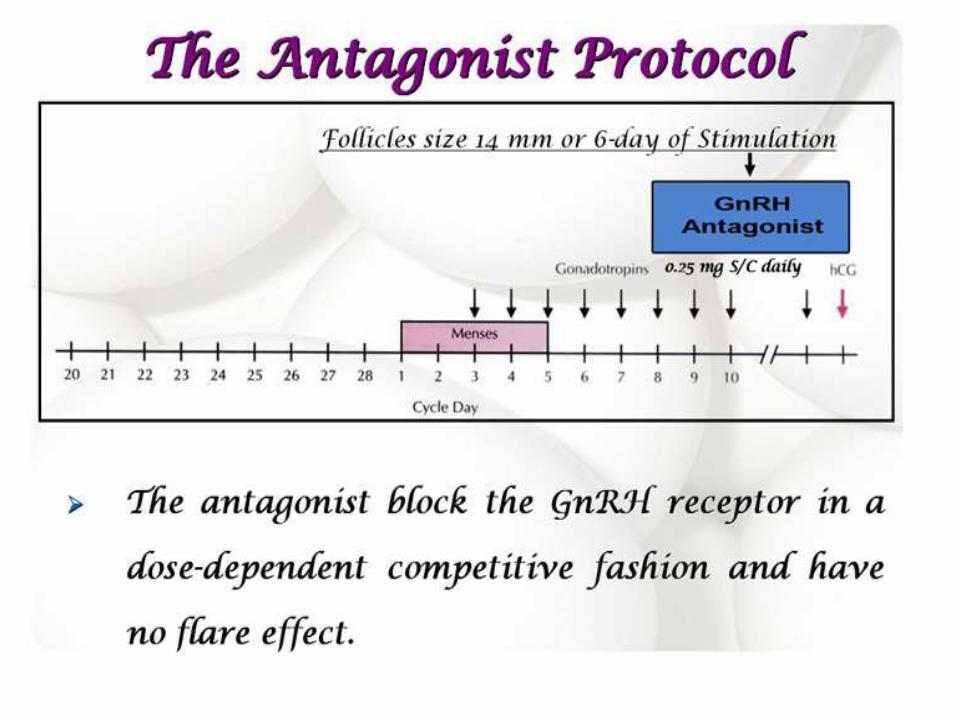
Mechanism of action

Commercially available
• Cetrorelix
• ganirelix
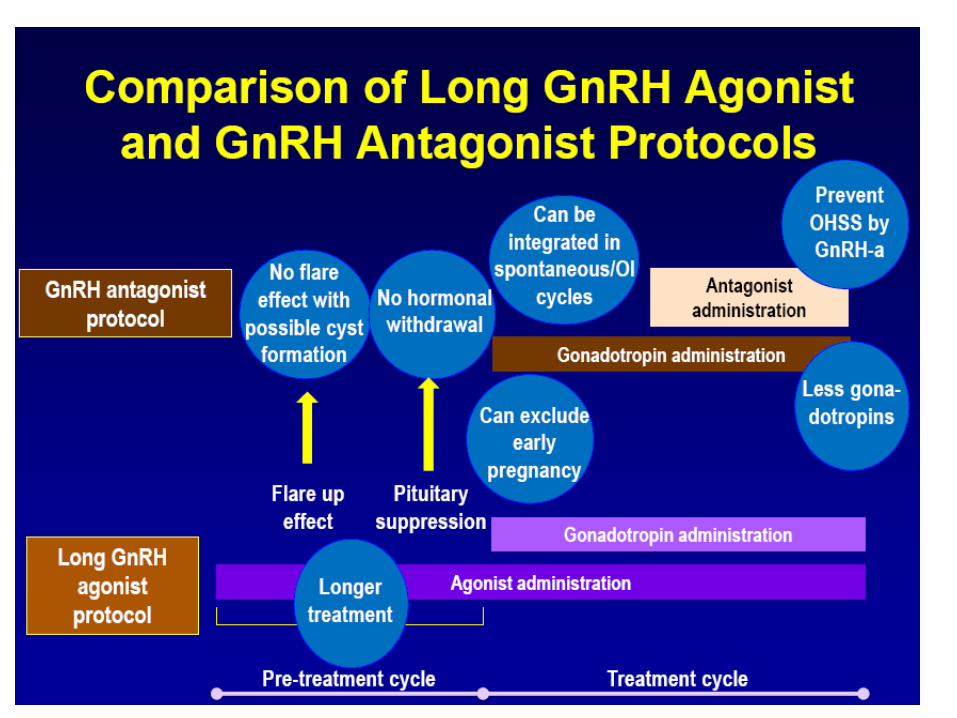
Advantages of GnRH antagonist
• Shorter duration of treatment
• Less injections
• Less consumption of Gonadotropins
• No flare up /no cyst formation
• No pituatory desensitization “more physiological”
• Lesser incidence of OHSS
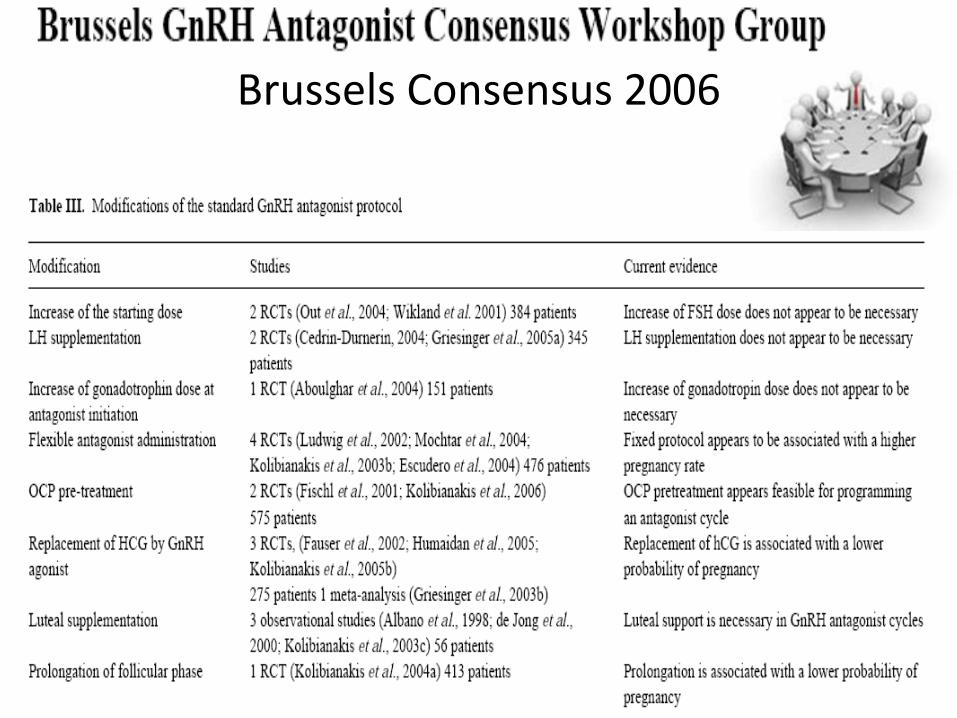
Brussels Consensus 2006
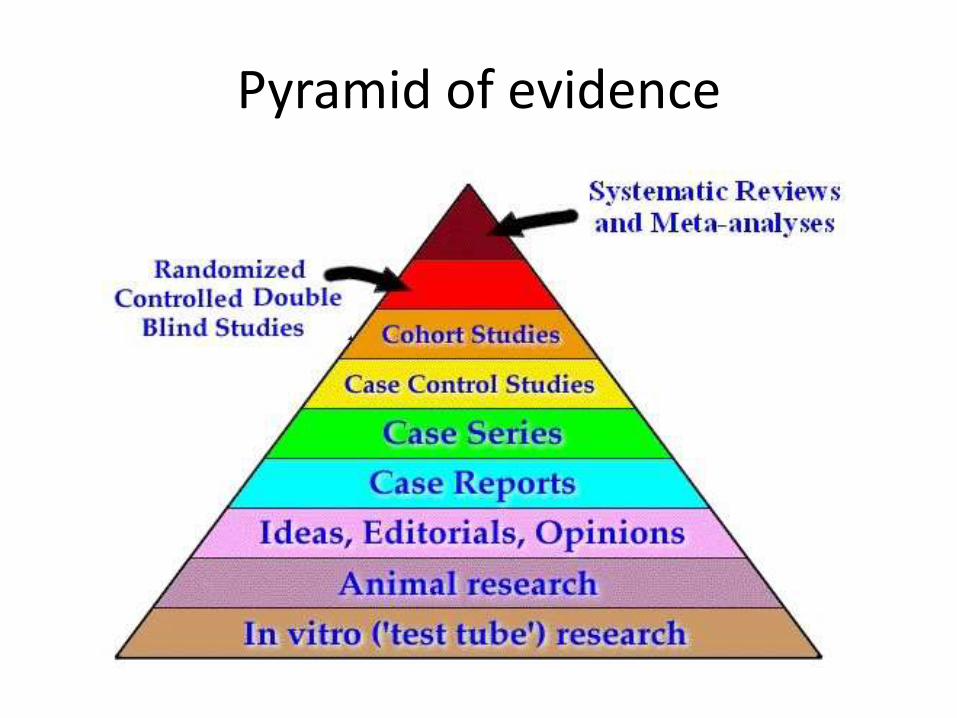
Pyramid of evidence

Efficacy………
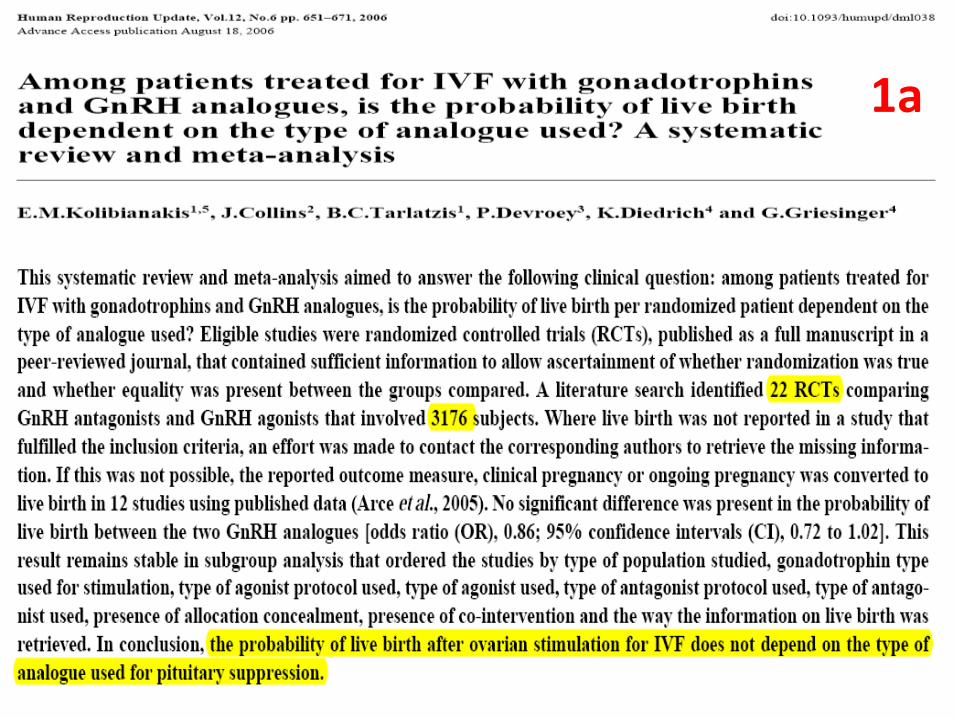
1a
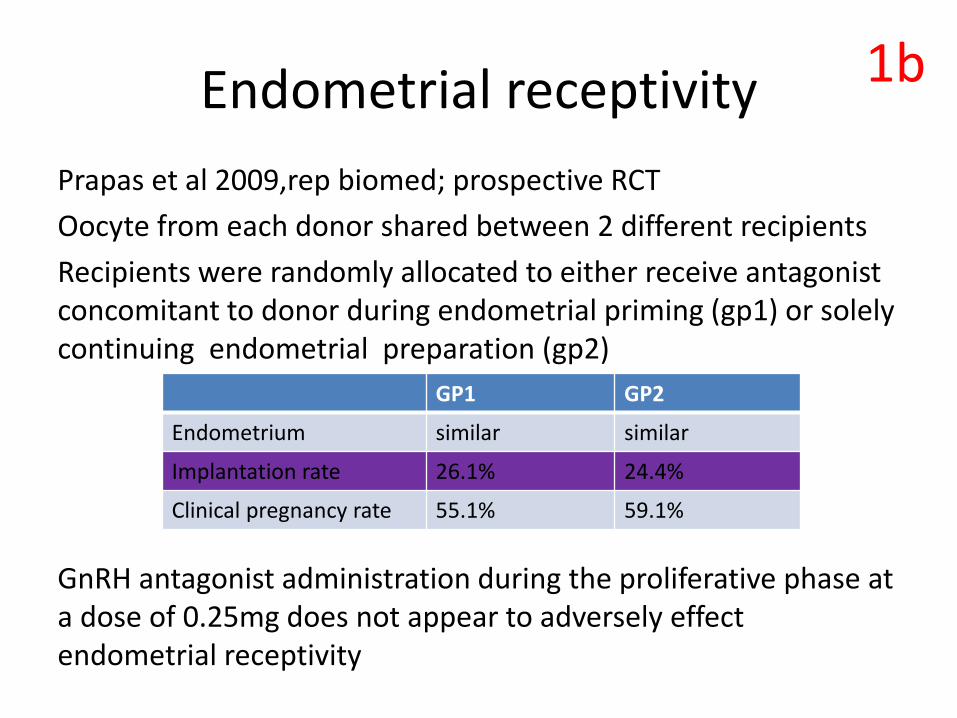
Endometrial receptivity
Prapas et al 2009,rep biomed; prospective RCT
Oocyte from each donor shared between 2 different recipients
Recipients were randomly allocated to either receive antagonist concomitant to donor during endometrial priming (gp1) or solely continuing endometrial preparation (gp2)
GnRH antagonist administration during the proliferative phase at a dose of 0.25mg does not appear to adversely effect endometrial receptivity
GP1 GP2
Endometrium similar similar
Implantation rate 26.1% 24.4%
Clinical pregnancy rate 55.1% 59.1%
1b

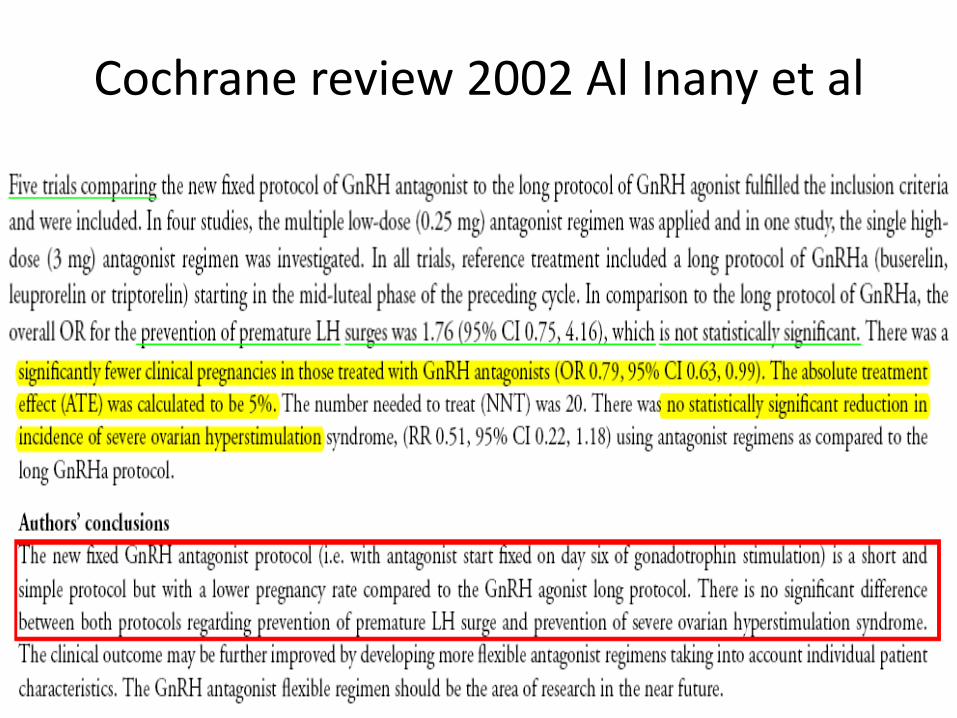
Cochrane review 2002 Al Inany et al
Antagonist versus agonist
Inexperience of the centre
Use of antagonist in higher age group
Use of antagonist in “unfavourable prognosis a priori”
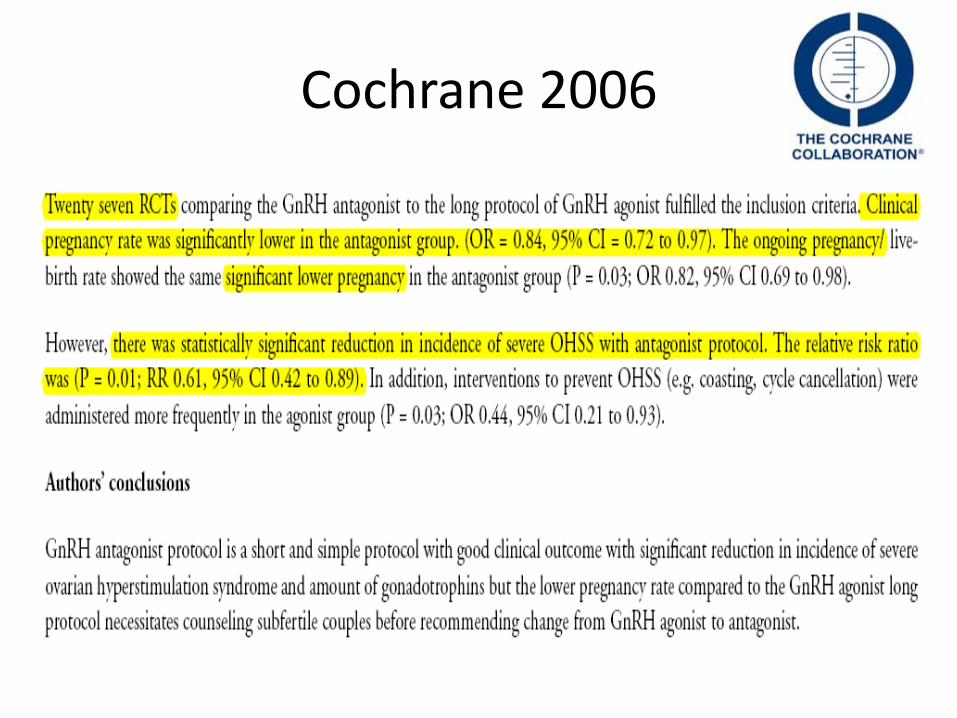
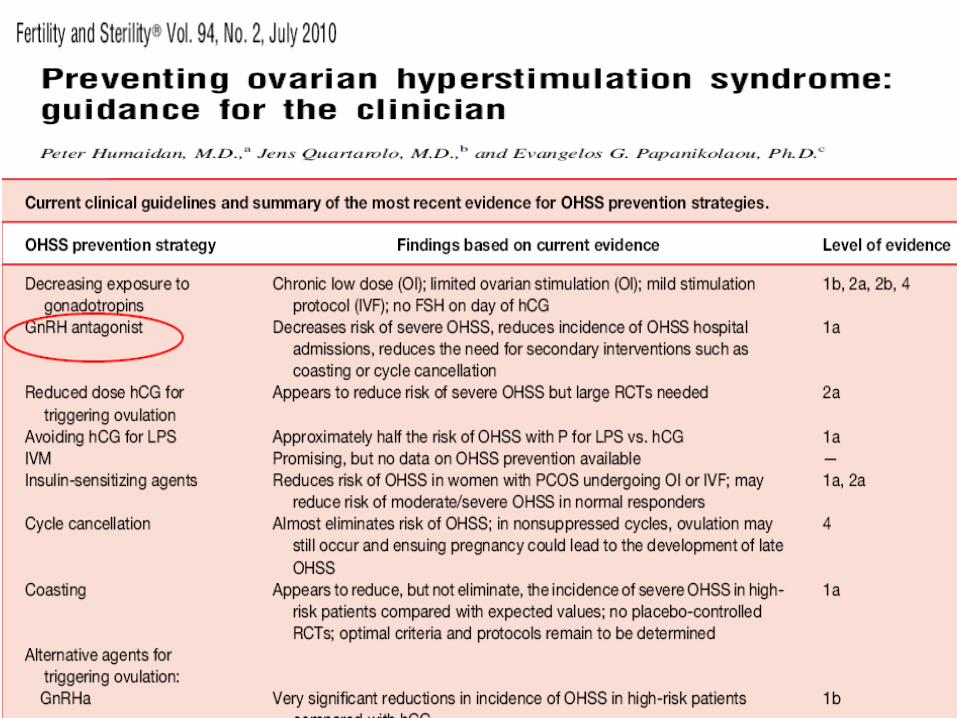
Cochrane 2006
Cochrane review and meta-analysis 2011
45 RCTs
7511 randomized women
Conclusion
The GnRH antagonist protocol is short and simple protocol
with a comparable live birth rate to long agonist protocol.It
is associated with a highly significant reduction in the
incidence of OHSS compared to the agonist protocol
therefore justifies a move away from the standard GnRH
agonist long protocol to a GnRH antagonist protocol
1A
Burden of treatment……OHSS
3 OHSS related death in 100000 ART cycles
“In 2003-2005, 4 deaths (of the 12) were due to OHSS”.
3 levels of safety
• Less incidence of OHSS(1a)
• Gives freedom to use GnRH agonist as a
trigger to replace hCG
• Use of antagonist in luteal phase
Preferred protocol in PCOS……….
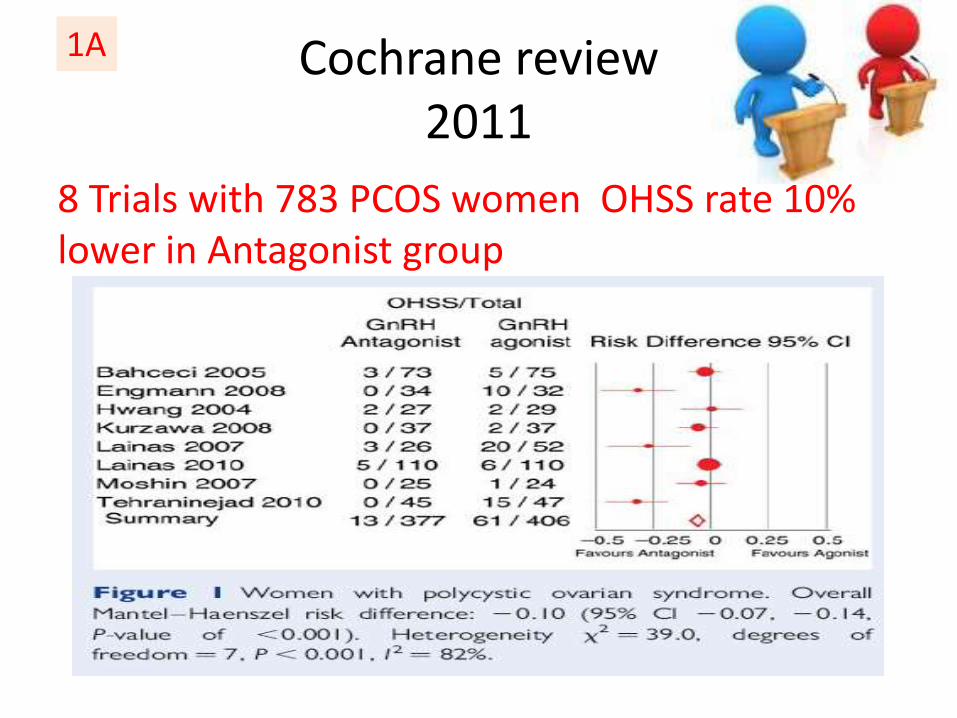
Cochrane review2011
8 Trials with 783 PCOS women OHSS rate 10% lower in Antagonist group
1A

11

Poor Response…….

Friendly IVF
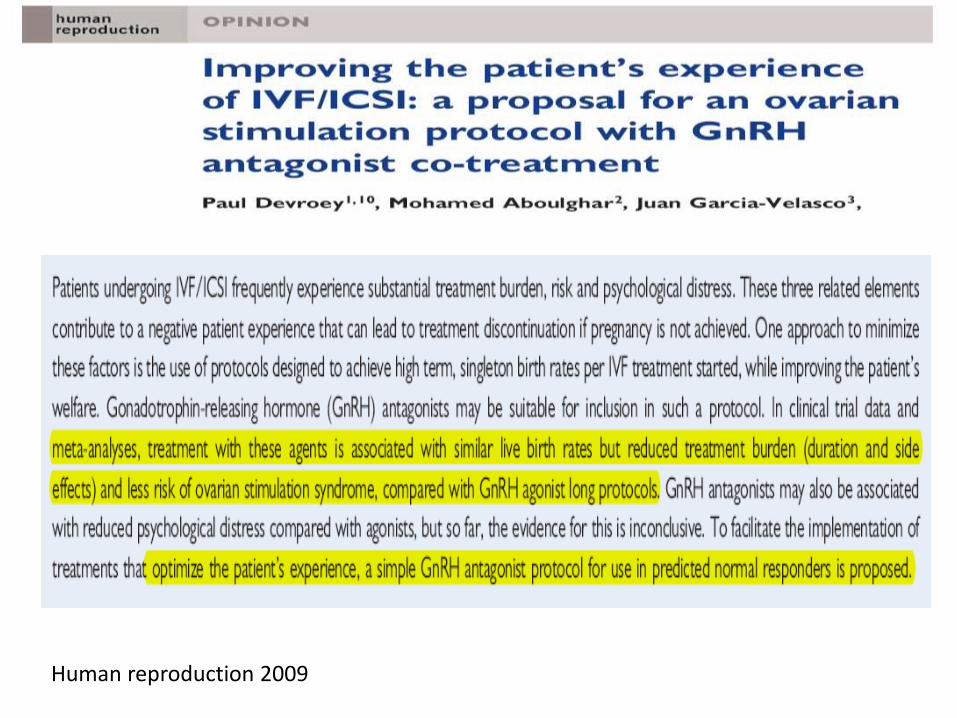
Human reproduction 2009
Reducing treatment stress
De Clark et al 2006 ,human reproduction
In a study involving 391 women who were undergoing IVF with the conventional long agonist protocol reported statiscally significantly more symptoms of depression during the week before stimulation than control patients who did not experience downregulation.

Newer challenges…mild IVF
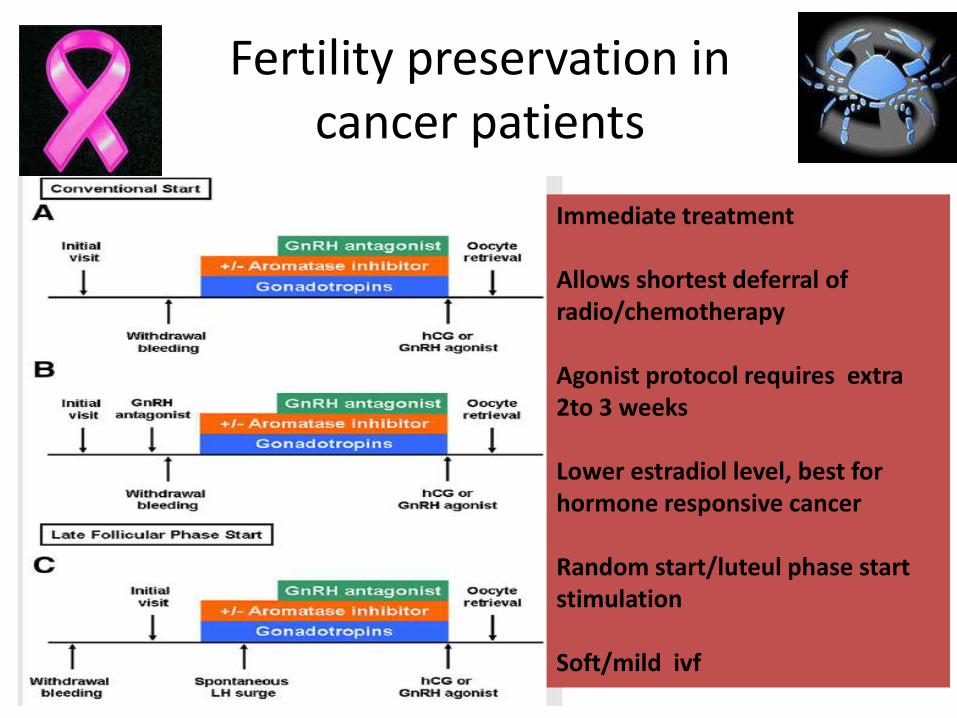
Fertility preservation in cancer patients
Immediate treatment
Allows shortest deferral of radio/chemotherapy
Agonist protocol requires extra 2to 3 weeks
Lower estradiol level, best for hormone responsive cancer
Random start/luteul phase start stimulation
Soft/mild ivf
Crystal ball where we are heading ……….????
IN
Antagonist protocol
OHSS free clinic
OUT
Long agonist protocol
Severe OHSS
OHSS related death

Its antagonist only………..







