
Advances in Therapies Leading to HIV Eradication
Francesco R Simonetti, MD
Cellular and Molecular Medicine PhD ProgramJohns Hopkins University, Baltimore, MD
Advances in Therapies Leading to HIV Eradication
Francesco R Simonetti, MD
Cellular and Molecular Medicine PhD ProgramJohns Hopkins University, Baltimore, MD
FR Simonetti has no financial relationships with commercial entities to disclose
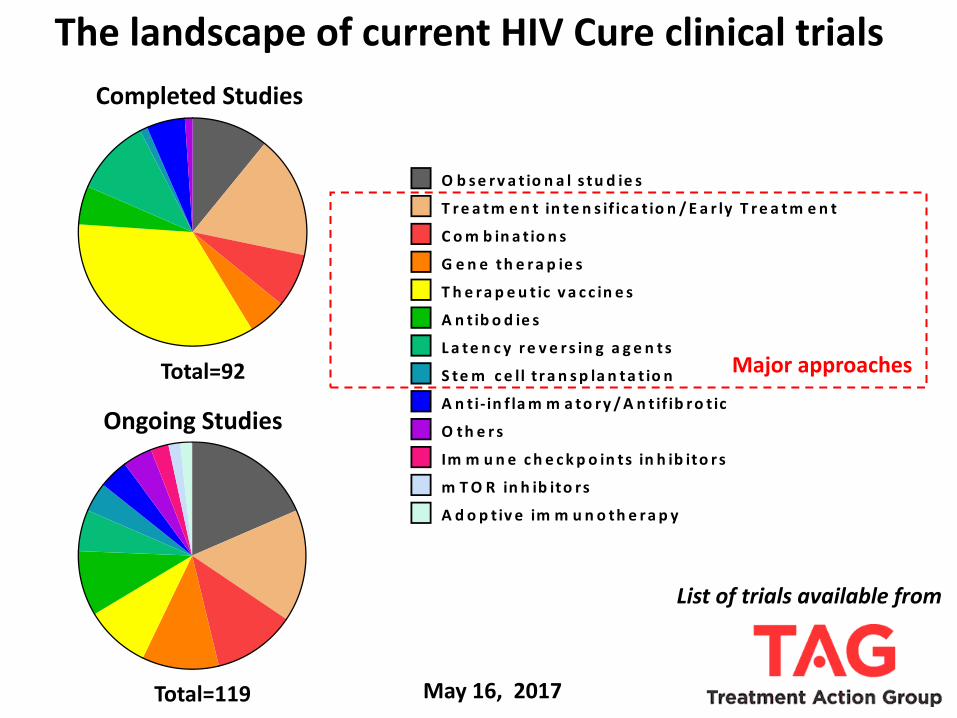
List of trials available from
o n g o in g
T o ta l= 1 1 9
O b s e r v a t io n a l s t u d ie s
T r e a t m e n t in te n s if ic a t io n / E a r ly T r e a t m e n t
C o m b in a t io n s
G e n e t h e r a p ie s
T h e r a p e u t ic v a c c in e s
A n t ib o d ie s
L a t e n c y r e v e r s in g a g e n t s
S te m c e ll t r a n s p la n t a t io n
A n t i- in f la m m a to r y / A n t if ib r o t ic
O t h e r s
Im m u n e c h e c k p o in ts in h ib ito r s
m T O R in h ib ito rs
A d o p t iv e im m u n o th e r a p y
c o m p le te d
T o ta l= 9 2o n g o in g
T o ta l= 1 1 9
O b s e r v a t io n a l s t u d ie s
T r e a t m e n t in te n s if ic a t io n / E a r ly T r e a t m e n t
C o m b in a t io n s
G e n e t h e r a p ie s
T h e r a p e u t ic v a c c in e s
A n t ib o d ie s
L a t e n c y r e v e r s in g a g e n t s
S te m c e ll t r a n s p la n t a t io n
A n t i- in f la m m a to r y / A n t if ib r o t ic
O t h e r s
Im m u n e c h e c k p o in ts in h ib ito r s
m T O R in h ib ito rs
A d o p t iv e im m u n o th e r a p y
c o m p le te d
T o ta l= 9 2
Completed Studies
Ongoing Studies
Total=119
Total=92
The landscape of current HIV Cure clinical trials
May 16, 2017
Major approaches
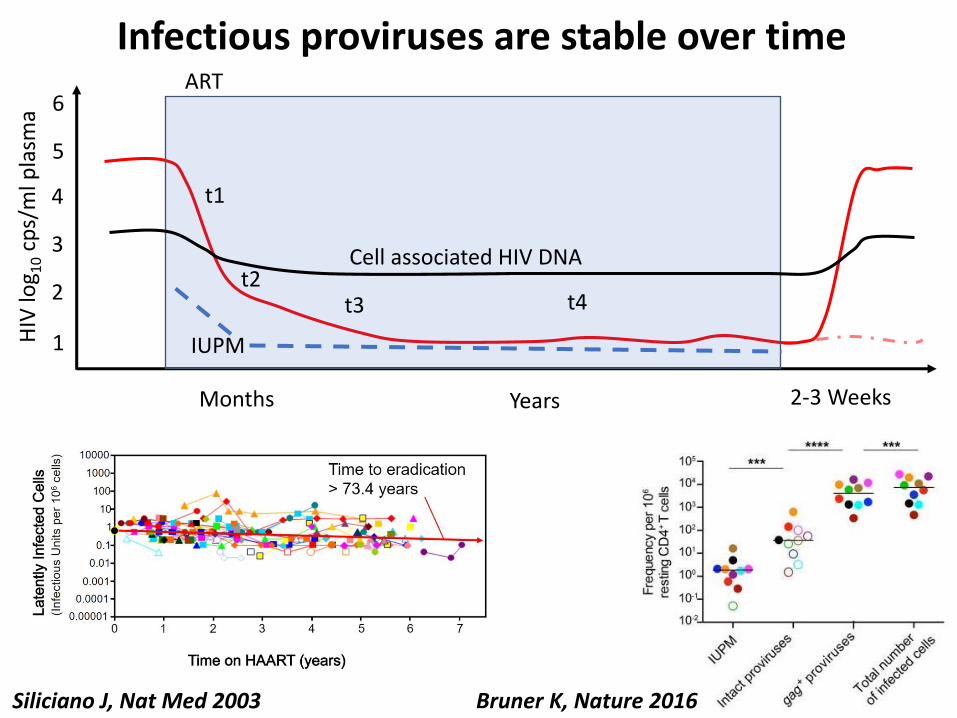
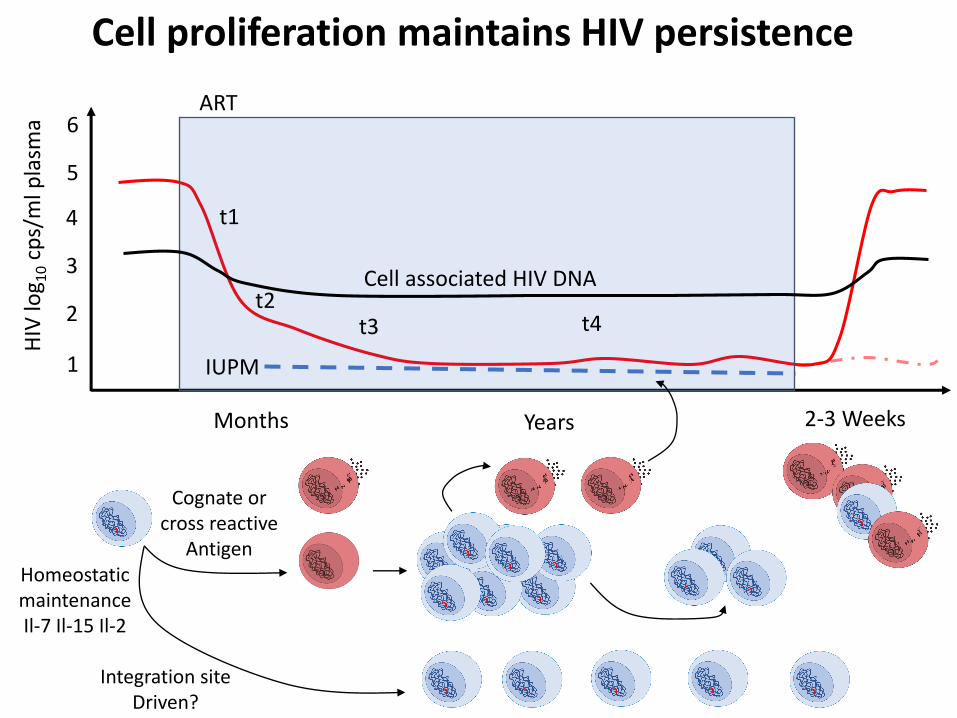
Infectious proviruses are stable over timeART
HIV
log 1
0cp
s/m
l pla
sma
Months Years 2-3 Weeks
t1
t2t3 t4
1
3
2
4
6
5
Cell associated HIV DNA
IUPM
Siliciano J, Nat Med 2003 Bruner K, Nature 2016

What maintains the HIV reservoir?
Mechanism Therapeutic approach
Cryptic ongoing replication • ART intensification• drug delivery• nanoparticles
Latency • Shock and Kill• Gene therapy• Lock HIV transcription
Proliferation of infected cells • Early treatment• Accelerate decay• Block clonal expansion
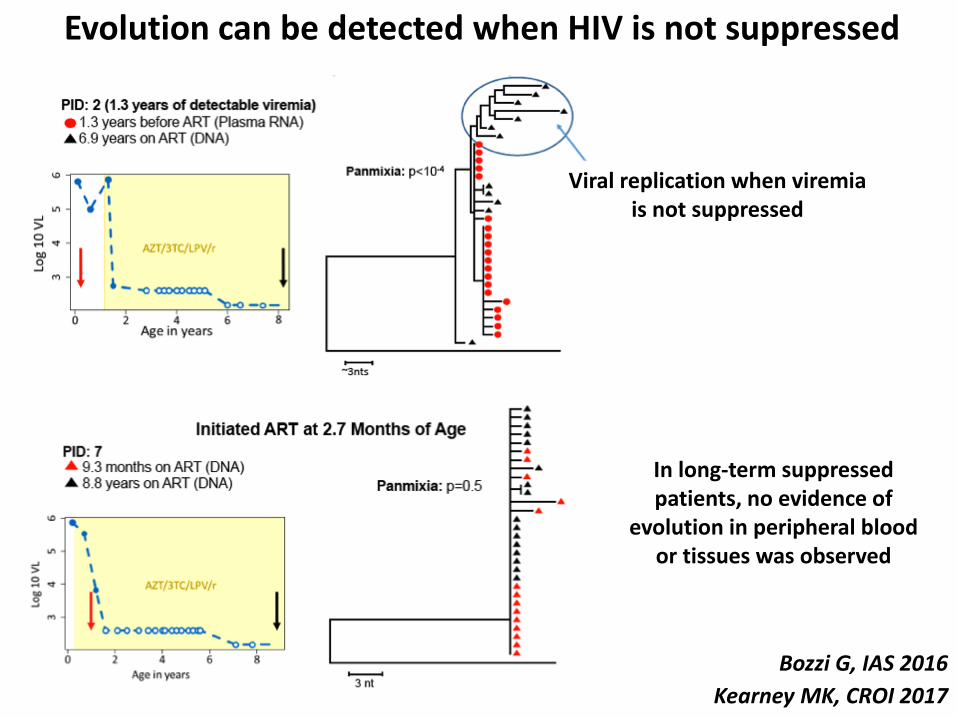
Evolution can be detected when HIV is not suppressed
Kearney MK, CROI 2017
Bozzi G, IAS 2016
In long-term suppressed patients, no evidence of
evolution in peripheral blood or tissues was observed
Viral replication when viremia is not suppressed
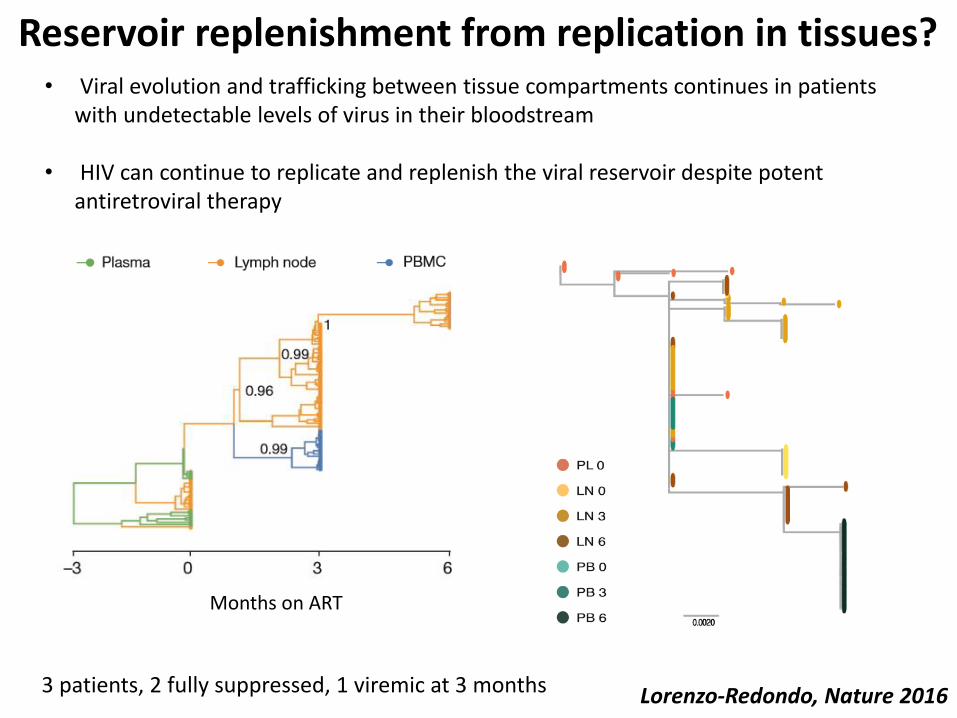
Reservoir replenishment from replication in tissues?
Lorenzo-Redondo, Nature 2016
• Viral evolution and trafficking between tissue compartments continues in patients with undetectable levels of virus in their bloodstream
• HIV can continue to replicate and replenish the viral reservoir despite potent antiretroviral therapy
Months on ART
3 patients, 2 fully suppressed, 1 viremic at 3 months

Rosenbloom D, BioRxiv 2017
Reservoir decay post ART initiation leads to a false evolutionary signal

What maintains the HIV reservoir?
Mechanism Therapeutic approach
Cryptic ongoing replication • ART intensification• drug delivery• nanoparticles
Latency • Shock and Kill• Gene therapy• Lock HIV transcription
Proliferation of infected cells • Early treatment• Accelerate decay• Block clonal expansion

Shock and Kill
Death by viral CPE
Death by CTL
Activation induced cell death
LRA
Limitations of current Shock and Kill strategies• Only a small fraction of proviruses is
reactivated (position effect of integration)
• Defective and intact proviruses might have a different susceptibility to latency reversal
• CTL escape mutations are common in treated chronic infection
Shock and kill strategies need to be coupled with other interventions (bNABs, DARTs, Therapeutic vaccines) to enhance reservoir clearance

What maintains the HIV reservoir?
Mechanism Therapeutic approach
Cryptic ongoing replication • ART intensification• drug delivery• nanoparticles
Latency • Shock and Kill• Gene therapy• Lock HIV transcription
Proliferation of infected cells • Early treatment• Accelerate decay• Block clonal expansion
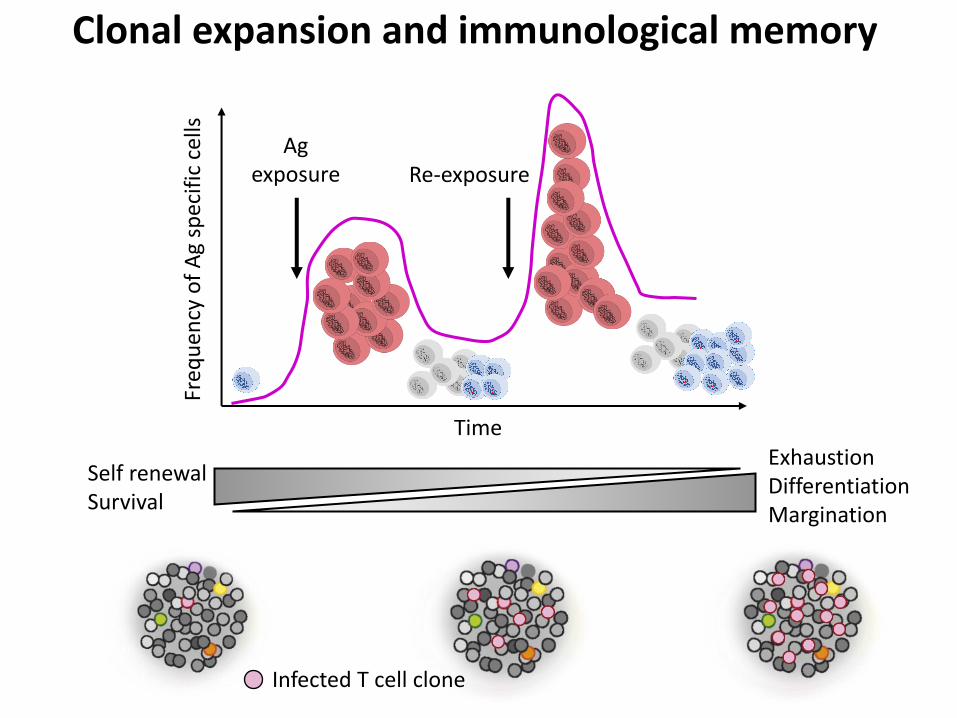
Clonal expansion and immunological memory
ExhaustionDifferentiationMargination
Self renewalSurvival
Freq
uen
cy o
f A
g sp
ecif
ic c
ells
Time
Ag exposure Re-exposure
Infected T cell clone
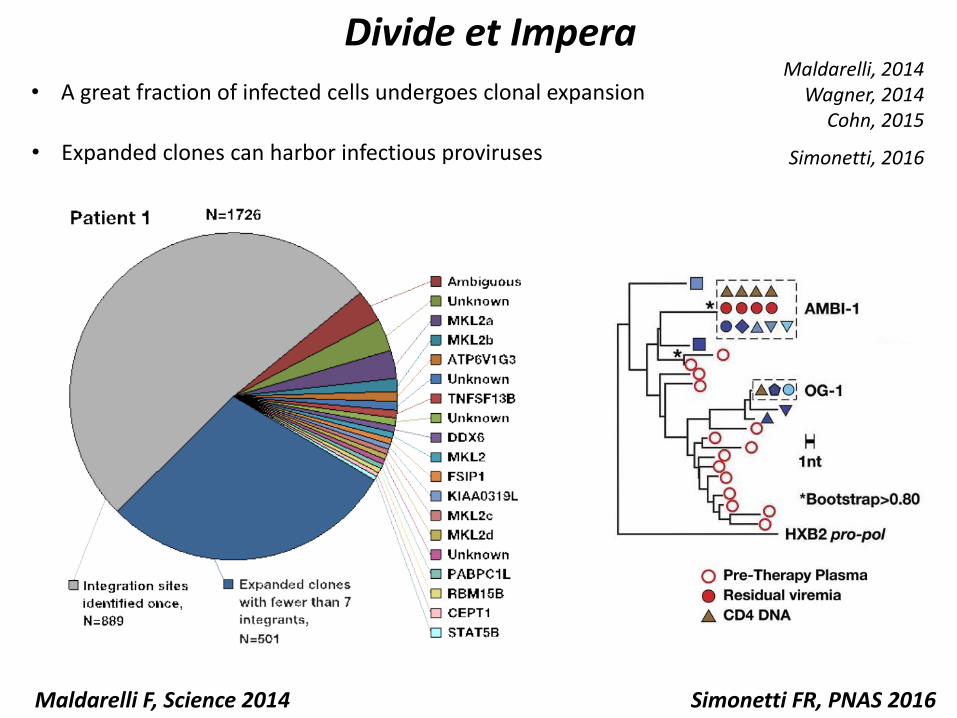
Divide et Impera
• A great fraction of infected cells undergoes clonal expansion
• Expanded clones can harbor infectious proviruses
Maldarelli, 2014Wagner, 2014
Cohn, 2015
Simonetti, 2016
Simonetti FR, PNAS 2016Maldarelli F, Science 2014
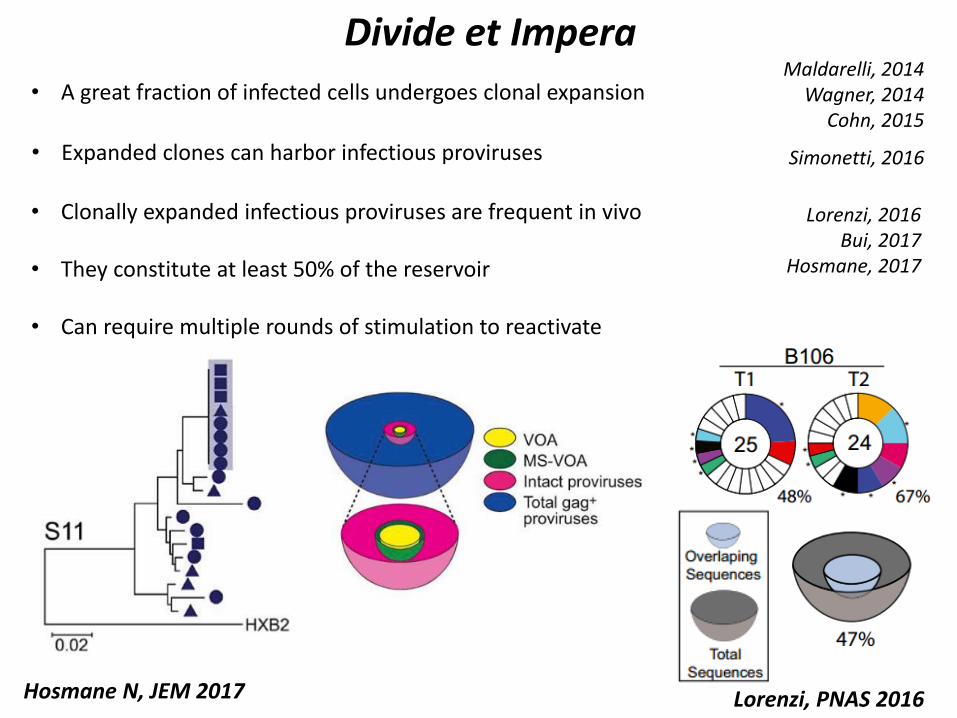
Divide et Impera
• A great fraction of infected cells undergoes clonal expansion
• Expanded clones can harbor infectious proviruses
• Clonally expanded infectious proviruses are frequent in vivo
• They constitute at least 50% of the reservoir
• Can require multiple rounds of stimulation to reactivate
Maldarelli, 2014Wagner, 2014
Cohn, 2015
Simonetti, 2016
Lorenzi, 2016Bui, 2017
Hosmane, 2017
Hosmane N, JEM 2017 Lorenzi, PNAS 2016
ART
Months Years 2-3 Weeks
t1
t2t3 t4
1
3
2
4
6
5
Cell associated HIV DNA
Cognate or cross reactive
AntigenHomeostatic maintenanceIl-7 Il-15 Il-2
Integration siteDriven?
IUPM
Cell proliferation maintains HIV persistenceH
IV lo
g 10
cps/
ml p
lasm
a
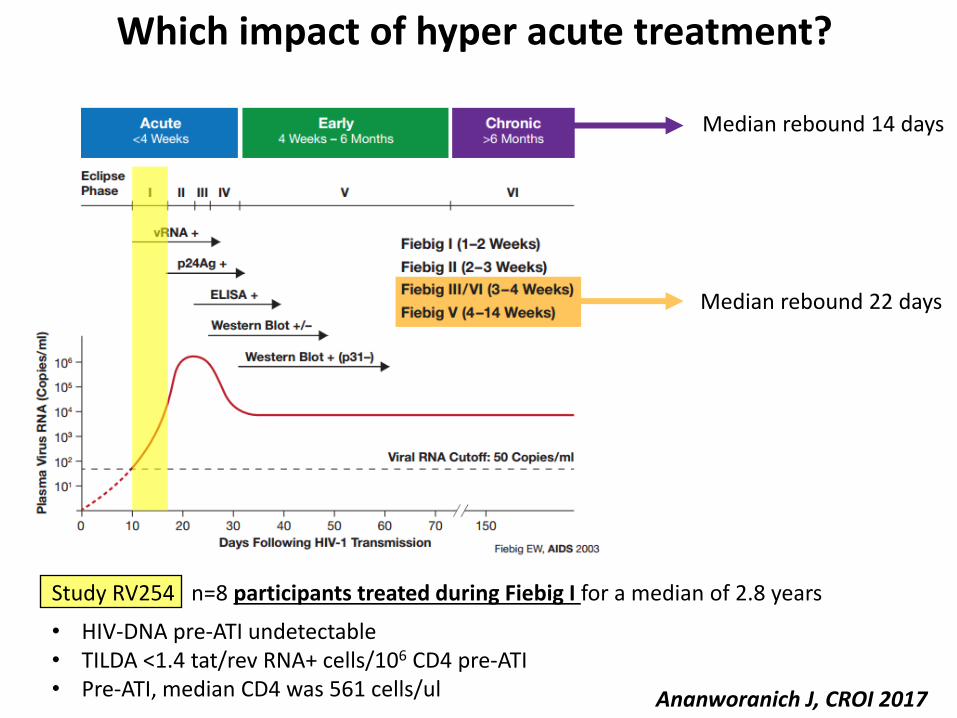
Which impact of hyper acute treatment?
Ananworanich J, CROI 2017
Median rebound 14 days
Median rebound 22 days
• HIV-DNA pre-ATI undetectable• TILDA <1.4 tat/rev RNA+ cells/106 CD4 pre-ATI• Pre-ATI, median CD4 was 561 cells/ul
Study RV254 n=8 participants treated during Fiebig I for a median of 2.8 years
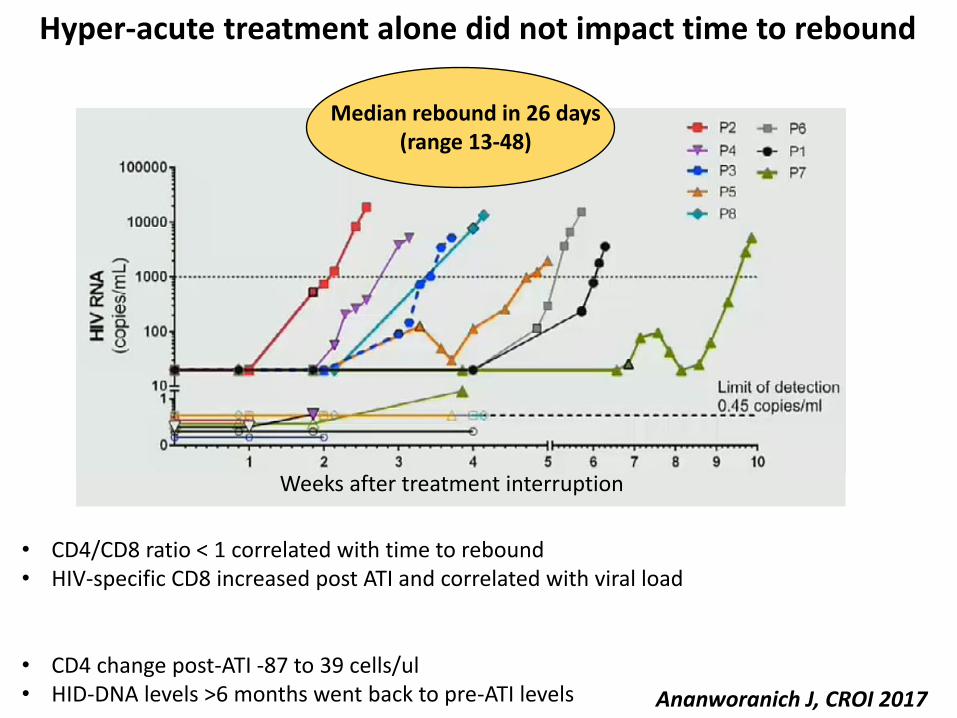
Hyper-acute treatment alone did not impact time to rebound
Ananworanich J, CROI 2017
Weeks after treatment interruption
• CD4 change post-ATI -87 to 39 cells/ul• HID-DNA levels >6 months went back to pre-ATI levels
• CD4/CD8 ratio < 1 correlated with time to rebound• HIV-specific CD8 increased post ATI and correlated with viral load
Median rebound in 26 days (range 13-48)

Early treatment does not prevent HIV clonal expansion
Hughes S, CROI 2017
Additional patients in Fiebig I/II are under investigation
5 out of 8 subjects had detectable clones pre-ART
6 out of 6 subjects had detectable clones post-ART

Viral control induced by HIVcons vaccine in early treated individuals
Mothe et al, BCN02 trial, CROI 2017
Viral control can be achieved by redirecting CTL against conserved HIV regions in the context of retained T-cell function and a reservoir with reduced size and diversity
ChAd+MVA+Romidepsin induced CD8-mediated responses to otherwise subdominant conserved epitopes.
Post treatment control in 40% of the participants
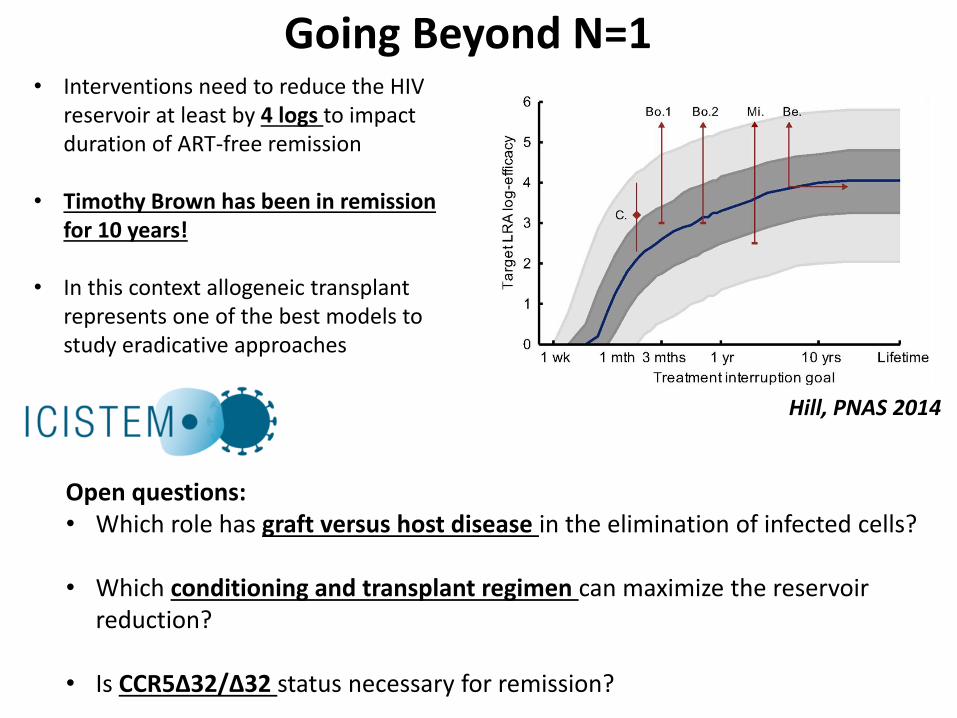
Going Beyond N=1
Hill, PNAS 2014
• Interventions need to reduce the HIV reservoir at least by 4 logs to impact duration of ART-free remission
• Timothy Brown has been in remission for 10 years!
• In this context allogeneic transplant represents one of the best models to study eradicative approaches
Open questions:• Which role has graft versus host disease in the elimination of infected cells?
• Which conditioning and transplant regimen can maximize the reservoir reduction?
• Is CCR5∆32/∆32 status necessary for remission?

Donor Conditioning regimen
Transplant Chimera GVHD HIV DNAcp/106
PBMC
HIV RNA in plasmacp/ml
qVOAIUPM
HIV DNA in ileum biopsy
WT/WT Myoablative Cord blood +HLA mismatched
incomplete NO 25 5 0.034 -
∆32/∆32 Reduced intensity
HLA-matchedunrelated
full YES <LOD <LOD <LOD positive
WT/WT Reduced intensity
HLA-matched sibling
full YES <LOD <LOD <LOD <LOD
Wensing, ECCMID 2017
The “graft versus HIV reservoir effect” may contribute to the clearance of the reservoir
Reservoir reduction is independent of donor CCR5 genotype
Long-term follow up post SCT in three patients
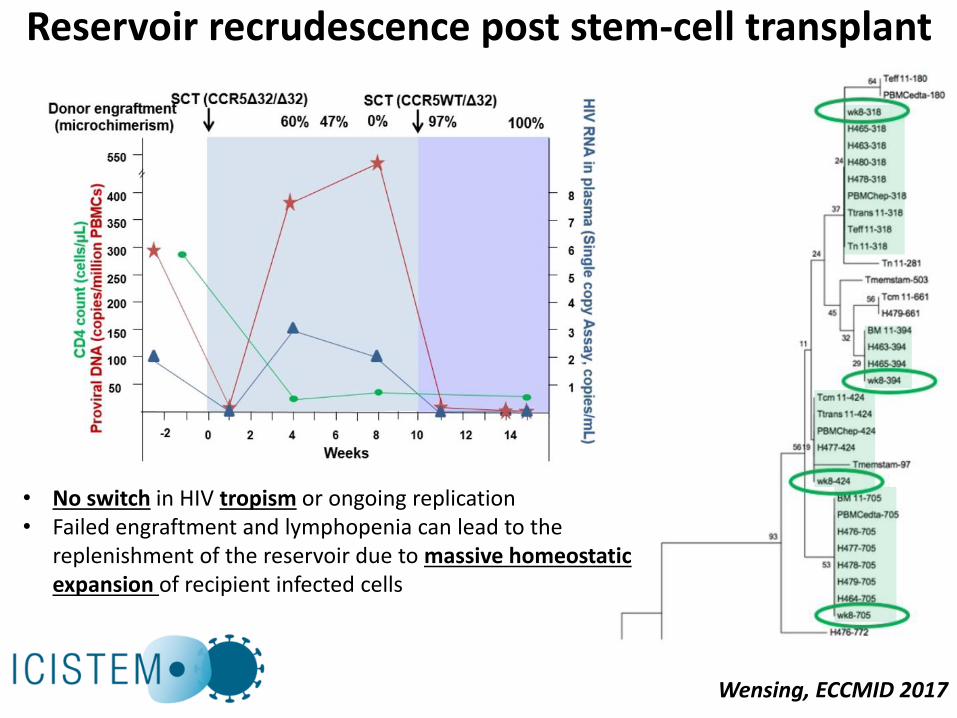
Reservoir recrudescence post stem-cell transplant
Wensing, ECCMID 2017
• No switch in HIV tropism or ongoing replication• Failed engraftment and lymphopenia can lead to the
replenishment of the reservoir due to massive homeostatic expansion of recipient infected cells
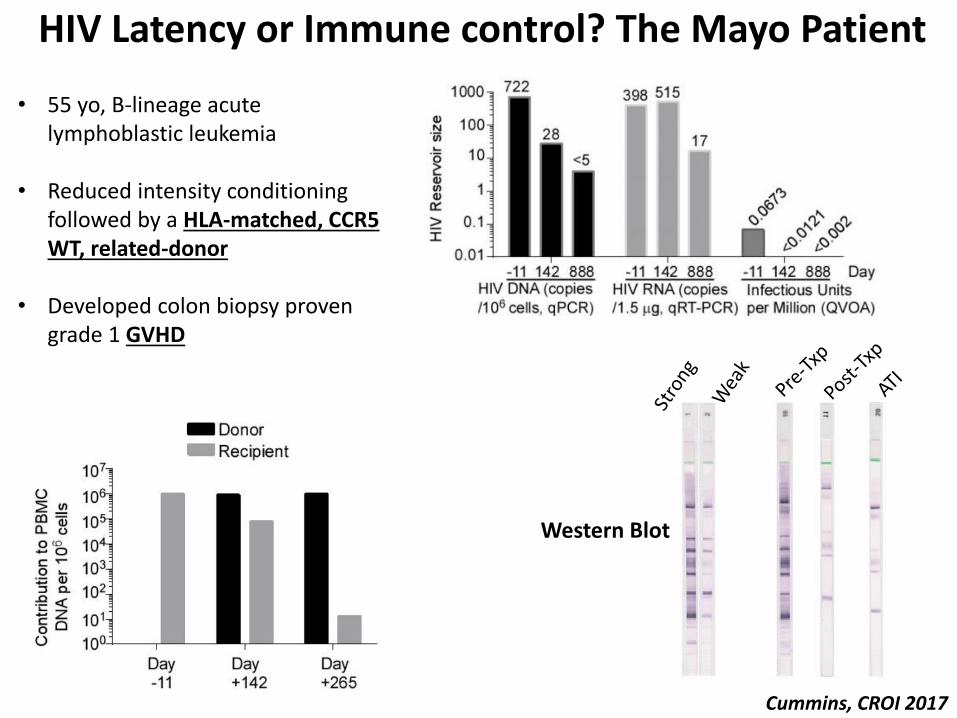
HIV Latency or Immune control? The Mayo Patient
Cummins, CROI 2017
• 55 yo, B-lineage acute lymphoblastic leukemia
• Reduced intensity conditioning followed by a HLA-matched, CCR5 WT, related-donor
• Developed colon biopsy proven grade 1 GVHD
Western Blot
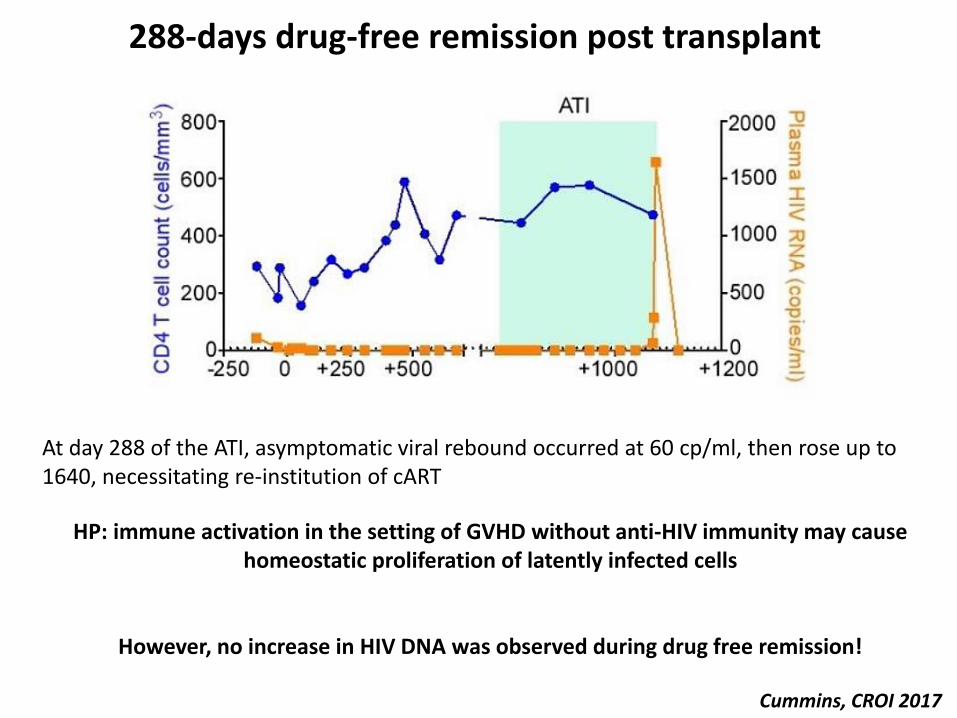
288-days drug-free remission post transplant
Cummins, CROI 2017
HP: immune activation in the setting of GVHD without anti-HIV immunity may cause homeostatic proliferation of latently infected cells
However, no increase in HIV DNA was observed during drug free remission!
At day 288 of the ATI, asymptomatic viral rebound occurred at 60 cp/ml, then rose up to 1640, necessitating re-institution of cART
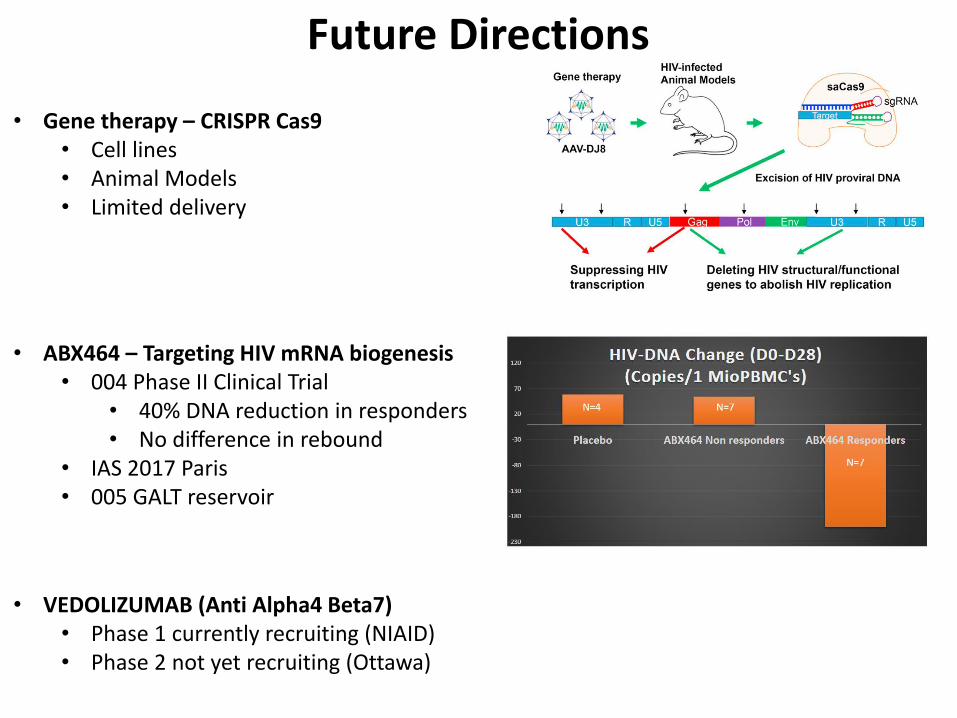
Future Directions
• Gene therapy – CRISPR Cas9• Cell lines• Animal Models• Limited delivery
• ABX464 – Targeting HIV mRNA biogenesis • 004 Phase II Clinical Trial
• 40% DNA reduction in responders• No difference in rebound
• IAS 2017 Paris• 005 GALT reservoir
• VEDOLIZUMAB (Anti Alpha4 Beta7)• Phase 1 currently recruiting (NIAID)• Phase 2 not yet recruiting (Ottawa)

Conclusions
• Clonal Expansion is a major mechanism of persistence and a barrier for HIV cure
• Early treatment alone is not sufficient to increase the chance of post-treatment control
• Bone marrow transplant can help us understand latency, reservoir stability and eradicative potential
• New strategies are in development, both in pre- and clinical phases
1990s 2006
2017 20XX
Acknowledgments
University of Pittsburgh
John W MellorsMichele Sobolewski
Melissa TosianoDianne Koons
Lou Halvas
HIV Dynamics and Replication ProgramFrank Maldarelli
John M CoffinElizabeth M Anderson
Stephen Hughes
University of MilanClaudia BalottaPaolo Cattaneo
Alessia Lai Giorgio Bozzi
Annalisa BergnaFrancesca Binda
Johns Hopkins UniversityRobert F SilicianoJanet D Siliciano
Ya-Chi HoCMM Program
“Since I had the vaccine, I haven’t had to take any pills or meds for six months.”
“It is not a complete cure, everything is fine, I am thrilled, but I am always expecting the worst.”
Thanks to study participants
BCN-02 trial volunteer







