
Adrian Towse ISPOR 20th Annual International Meeting Philadelphia • 19th May 2015
Early Access to Medicines: What is in it for Payers?

Modelling the value of early access to medicines
19/05/2015 2
Agenda
1. The Challenge for Payers
2. What matters to regulators and payers?
3. How early and how adaptive?
4. Illustrative case study adapting Baird et al. 2013: Gilenya for relapsing multiple sclerosis
5. Implications
Acknowledgements:
• This modelling is part of a research project funded by Pfizer. The Office of Health Economics is grateful for its support.
• Thank you to my colleagues Mikel Berdud, Amanda Cole and Jorge Mestre-Ferrandiz

Modelling the value of early access to medicines
19/05/2015 3
The challenge
• Many HTA agencies / P&T Committees acting on behalf of payers and reimbursement bodies have major concerns about funding new medicines on the basis of early data
• Without payer “buy in” and hence drug listing and reimbursement, companies do not have a viable commercial model for early access and patients do not get earlier access to medicines

Modelling the value of early access to medicines
19/05/2015 4
What are payer / P&T / HTA body concerns?
• Struggling to pay for fully licensed medicines with a “full” evidence base
• Lowering evidence standards sends the wrong signals
• Increased uncertainty about outcomes has a cost – option value of delay
• Monitoring outcomes (to ensure the drug does deliver) as a form of CED is difficult
• Likelihood of problems at re-review – need to agree an MEA?
Modelling the value of early access to medicines
19/05/2015 5
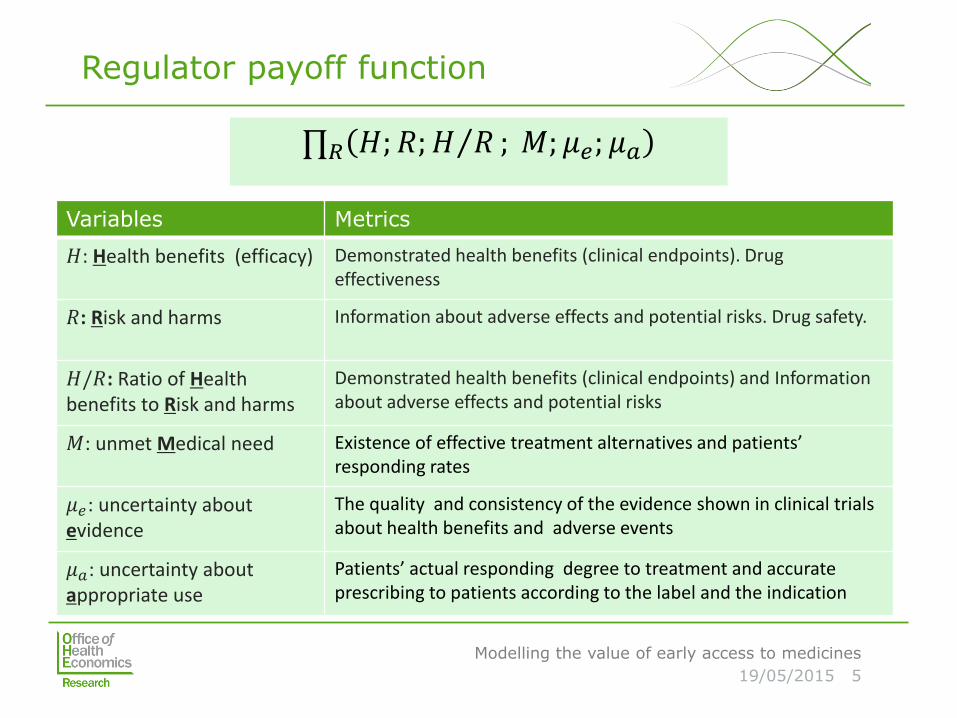
Variables Metrics
𝐻: Health benefits (efficacy) Demonstrated health benefits (clinical endpoints). Drug effectiveness
𝑅: Risk and harms Information about adverse effects and potential risks. Drug safety.
𝐻/𝑅: Ratio of Health benefits to Risk and harms
Demonstrated health benefits (clinical endpoints) and Information about adverse effects and potential risks
𝑀: unmet Medical need Existence of effective treatment alternatives and patients’ responding rates
𝜇𝑒: uncertainty about evidence
The quality and consistency of the evidence shown in clinical trials about health benefits and adverse events
𝜇𝑎: uncertainty about appropriate use
Patients’ actual responding degree to treatment and accurate prescribing to patients according to the label and the indication
∏𝑅 𝐻; 𝑅;𝐻 𝑅 ; 𝑀; 𝜇𝑒; 𝜇𝑎
Regulator payoff function
Modelling the value of early access to medicines
19/05/2015 6
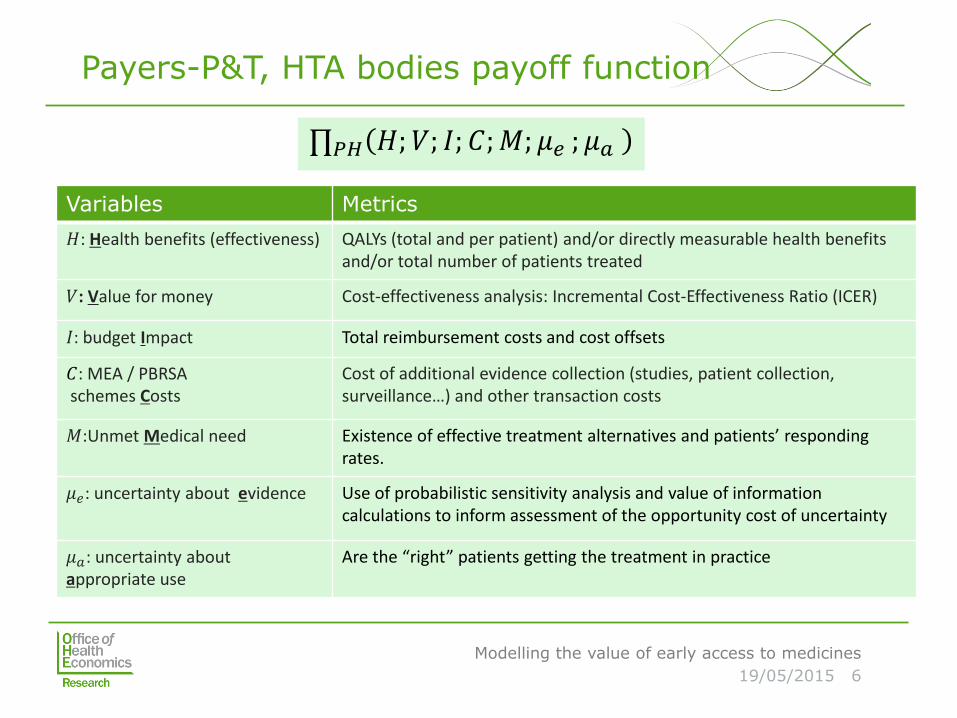
Variables Metrics
𝐻: Health benefits (effectiveness) QALYs (total and per patient) and/or directly measurable health benefits and/or total number of patients treated
𝑉: Value for money Cost-effectiveness analysis: Incremental Cost-Effectiveness Ratio (ICER)
𝐼: budget Impact Total reimbursement costs and cost offsets
𝐶: MEA / PBRSA schemes Costs
Cost of additional evidence collection (studies, patient collection, surveillance…) and other transaction costs
𝑀:Unmet Medical need Existence of effective treatment alternatives and patients’ responding rates.
𝜇𝑒: uncertainty about evidence Use of probabilistic sensitivity analysis and value of information calculations to inform assessment of the opportunity cost of uncertainty
𝜇𝑎: uncertainty about appropriate use
Are the “right” patients getting the treatment in practice
∏𝑃𝐻 𝐻;𝑉; 𝐼; 𝐶;𝑀; 𝜇𝑒 ; 𝜇𝑎
Payers-P&T, HTA bodies payoff function

Modelling the value of early access to medicines
19/05/2015 7
Building on Baird et al. 2013
Modelling the value of early access to medicines
19/05/2015 8
How early and how adaptive?
• Range of regulatory responses to expedite the development/licensing of promising new medicines that address unmet medical need in the treatment of serious or life-threatening conditions
• “Early access” schemes: expedited licensing decision, or facilitating access pre-license
[Incremental approach]
• Adaptive licensing: Recognises iterative development of evidence base; initial licence for narrow population base, re-visited periodically and expanded/restricted in light of new safety and efficacy data
[Transformational approach]

Modelling the value of early access to medicines
19/05/2015 9
The Baird et al. 2013 Checklist
Continuous Learning
Prospectively planned pre- and post-authorization trial(s) [Yes: 1, No: 0]
Clinical confirmation of efficacy based on surrogate endpoints [Yes: 1, No: 0]
Confirmation at traditional significance level of efficacy based on relaxed significance [Yes: 1, No: 0]
Collection of real world performance data such as Registries /observational Studies. [Yes: 1, No: 0] Expanded access program [Yes: 1, No: 0]
Licensing
Periodic benefit/risk reassessments [Yes: 1, No: 0]
Preplanned serial authorizations [Yes: 1, No: 0]
Access
Restricted to on-label population [Yes: 1, No: 0]
Staged expansion of patient populations [Yes: 1, No: 0]
Controlled prescriber or facility access [Yes: 1, No: 0]
Communication and Controls
Established educational support for patients and prescribers [Yes: 1, No: 0] Timely communication of new and emerging product information to patients and prescribers [Yes: 1, No: 0]
Off label use monitored/controlled [Yes: 1, No: 0]
Monitoring of patient adherence [Yes: 1, No: 0]
Enhanced safety monitoring imposed [Yes: 1, No: 0]

Modelling the value of early access to medicines
19/05/2015 10
Case study: Gilenya for Multiple Sclerosis
The starting point in modelling: Gilenya for MS
• Baseline cases (Baird et al. 2013):
• Scenario 1: actual
• Scenario 2: hypothetical adaptive
• Modelled scenarios:
• Temporary Authorisation for Use (Autorisation Temporaire d’Utilisation; ATU), France
• Breakthrough Therapy Designation (BDT), US
• Two data sources are used: Baird et al. (2013) and NICE appraisal on fingolimod (Gilenya)1
• Pilot simulations for modelled scenarios and descriptive comparisons with the baseline cases
1NICE, 2012. Fingolimod for the treatment
of highly active relapsing–remitting multiple
sclerosis. National Institute of Health and
Care Excellence.

Modelling the value of early access to medicines
19/05/2015 11
Scenario # 1 : actual Baird et al. (2013)
•Years to licensing: 8
•Patients: 51,430 (peak)
•Years to peak: 7
•Posmarketing:
• Commitment for observational study
• Risk Evaluation and Mitigation Strategy (REMS)
• Safety monitoring: 1.5 years
Scenario # 2: hypothetical adaptive licensing Baird et al. (2013)
•Staged adaptive
•Years to initial authorisation: 5.5
•Years to full authorisation: 8
•Criteria for AL:
Patients with moderate to severe MS
•Patients in initial authorisation: 28705
•Patients added post-MA: 22725
•Collection of safety and efficacy data required between initial and full authorisation
•Likely withdrawal if conditions are not meet

Modelling the value of early access to medicines
19/05/2015 12
Scenario # 3: Authorisation Temporaire d’Utilisation (ATU), France.
•Temporary authorisation of use (ATU): year 5
•Full Market Authorisation (MA): year 8
•Criteria for ATU:
i-Serious or rare pathologies
ii-Absence of a therapeutic
alternative
iii-Positive Benefit-Risk ratio
•ATU patients: 17,798
•Patients added post-MA: 33,632
•ATU duration: 1 year
•Renewal: conditional to safety-efficacy data gathered during the year of ATU
•Likely withdrawal if conditions are not meet
Scenario # 4: Breakthrough Therapy Designation (BTD), US.
•Years to licensing: 5 years
•Criteria:
i-Serious condition and
unmet medical need
ii-Evidence of efficacy in at
least one clinically significant
endpoint over available
therapies
•Patients: 51,430
•Postmarketing:
Data on actual use of the medicinal product
No Postmarketing confirmatory trials
•Likely withdrawal if data on benefit-risk are not supportive

Modelling the value of early access to medicines
19/05/2015 13
Patient years evolution across time and scenarios
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
900,000
Years of treatmentATU
Years of treatmentBTD
Years of treatmentscenario # 1 (Baird etal. 2014)
Years of treatmentscenario # 2 (Baird etal. 2014)
Year

Modelling the value of early access to medicines
19/05/2015 14
Total QALY gain along the timeline by scenario
0
5000
10000
15000
20000
25000
30000
35000
40000
0 1 2 3 4 5 6 7 8 9
10
11
12
13
14
15
16
17
18
19
20
Total QALY gain ATU
Total QALY gain BTD
Total QALY gain baselinecase Baird et al. 2014
Total QALY gain AL Baird etal. 2014
Year

Modelling the value of early access to medicines
19/05/2015 15
Implications
• If the expected incremental outcome is positive and expected to provide value for money such that no further evidence collection is justified and the budget impact is not significant then early access is, prima facie, unambiguously better for payers
• If more evidence is required and it is not possible for payers to require this under an early access scheme, then it still makes sense for payers to approve, but with regret
• If more evidence is required and it is possible for payers to require this (or it is being made available to regulators) under an early access scheme, then payers need to put in place schemes (co-ordinated with regulators to reduce costs) to tackle 𝜇𝑒 and 𝜇𝑎. An adaptive pathway is optimal.

Modelling the value of early access to medicines
19/05/2015 16
About OHE
To enquire about additional information and analyses, please contact Professor Adrian Towse at [email protected].
To keep up with the latest news and research, subscribe to our blog, OHE News.
Follow us on Twitter @OHENews, LinkedIn and SlideShare.
The Office of Health Economics is a research and consulting organisation that has been providing specialised research, analysis and expertise on a range of health care and life sciences issues and topics for over 50 years.
OHE’s publications may be downloaded free of charge for registered users of its website.
Office of Health Economics Southside, 7th Floor 105 Victoria Street London SW1E 6QT United Kingdom
+44 20 7747 8850 www.ohe.org
©2014 OHE







