Download - 5 Immunol of Mammary gland

Session 5
Mucosal Immunology of the Mammary Gland
Stephanie Dorosko, PhD
Department of Microbiology & ImmunologyDartmouth Medical School
1 Medical Center Drive Lebanon, NH 03756 USA

Topics
• Anatomy and physiology review• Immune cells in breast milk• Non-cellular immune components in
breast milk• Breast milk transmission: statistics,
potential mechanisms, timing, sIgA, ART

Lawrence, RA.Breastfeeding: A Guide for the Medical Profession. Boston: Mosby, 1999, p.61

Lawrence, R.A. Breastfeeding: A Guide for the Medical Profession. Boston: Mosby, 1999, p. 62.

p.46
Lawrence, R.A. Breastfeeding: A Guide for the Medical Profession. Boston: Mosby, 1999, p.46

Lawrence, R.A. Breastfeeding: A Guide for the Medical Profession. Boston: Mosby, 1999, p.74

Mammary Alveoli – Cross Section
Schackleton et al, Nature 2006, 439:84-88

Lymphocytes in breast milk: functionsnot well understood

Macrophages: phagocytosis, storageand transport of IgA, excrete factorsto enhance maturation of intestinal
epithelium
Neutrophils: mammary tissue defenseagainst microorganisms

IgA: enteromammary link
Brandtzaeg, P.Nutrition Reviews 1998,56:S5-18

Other immune factors
• Lysozyme:enzyme secreted by neutrophils andsome macrophages. Bacteriostatic againstEnterobacteriaceae and gram-positive bacteria,digests part of cell wall proteoglycan
• Lactoferrin: iron-binding protein, deprivesmany types of bacteria and yeast of iron(bacteriostatic)
• Glycolipids, glycoproteins, freeoligosaccharides: inhibit bacterial and viraladhesion to intestinal epithelium
• Cell signalling factors: interleukins, cytokines

Breast milk transmission ofHIV-1

Current AIDS Statistics on Children <15 years of age Worldwide: 2005
• Living with HIV/AIDS 2.3 million
• Newly infected 700,000
• Died from AIDS 570,000
• More than 90% infected by MTCTUNAIDS, AIDS Epidemic Update: 2005. www.UNAIDS.org

HIV in Tanzania
• 7% of mainland adult population• 11% prevalence in cities and towns• 13% in women aged 30-34 years
• Antenatal clinics:– 5% Kagera– 15% Mbeya (compared to >20% in 1994)
• Lower prevalence than many of its neighboringcountries
Timing and Rate of MTCT
• 58% HIV+ before 4 weeks
• 42% HIV+ after 2 months (breastfeeding)
Coutsoudis et al, J Infect Dis 2004, 189:2154-66

MTCT of HIV-1 throughBreast Milk
• Mechanism of HIV transmission via this route isnot fully understood
• Previous studies have found several risk factorsassociated with MTCT through BF
Clinical mastitis (Embree, 2000; John, 2001)
Breast milk HIV-1 RNA viral load (Pillay, 2000;Rousseau 2003)
Breast milk sodium level (Semba, 1999)
Breast milk cell-associated DNA (Rousseau, 2004;Koulinska, 2006)
Low maternal CD4+ T-cell count; high plasma HIV-RNA levels (Rousseau, 2004))

Definition of Mastitis
• Inflammatory response of themammary tissue in response topathogenic bacteria which haveentered the gland through thelactiferous ducts

From“Physiology of lactation,” Chap.3, from Lawrence RAand Lawrence RM, Breastfeeding: A Guide for the Medical
Profession, 5th ed. Boston: Mosby, 1999.

Clinical Mastitis andRisk of MTCT
• OR = 2.7 (95% CI, 1.1-6.7)– (Embree et al, AIDS, 2000)
• RR = 3.9 (95% CI, 1.2-12.7)– (John et al, JID, 2001)

Subclinical Mastitis andRisk of MTCT:
Sodium level
Risk of MTCTOR (95% CI), P
ElevatedSodium (Na+) level
2.31 (1.23-4.26),<0.01
2.95 (1.63-5.30),<0.0004
Breast milk Na+ > 12mmol/L
@ 12 months
2.38 (1.26-4.42),<0.0008
2.77 (1.52-5.04),<0.0009
Breast milk Na+ > 12mmol/L
@ 6 weeks
MultivariateUnivariate
Semba et al, JID, 1999

SubclinicalMastitis
Sodium Level &
Viral RNA
Semba et al. JID, 1999

Detectable Viral RNA and Riskof MTCT
2.97 (1.25-7.04), <0.0112 monthsSemba et al, JID, 1999
2.82 (1.22-6.51)1wk – 15 monthsPillay et al, JAIDS, 2000
2.97 (1.23-7.18),<0.0166 weeksSemba et al, JID, 1999
Risk of MTCTOR (95% CI), P
Postpartum Period

Rousseau et al, J Infect Dis 2003, 187:741-7
Breast milk HIV-1 RNA in transmitters versus non-transmitters

Significance of cell-associated virus inbreast milk
• Proportion of breast milk HIV-infected cells: totalcells association with breast milk RNA (Rousseau, J Infect Dis2004, 190:1880-8)
• Each log10 increase in infected cells/mL associatedwith 3-fold increase in transmission
• Each 10-fold increase in breast milk HIV RNA orDNA (cell associated virus) associated with 3-foldincrease in breast milk transmission (Koulinska J AIDS 2006,41:93-9)
• Breast milk cell-associated virus predictivethroughout lactation; HIV RNA predictive oftransmission only after 9 months

Mechanisms of HIV-1 intestinal transmission invitro
Hocini and Bomsel, J Infect Dis 1999, 179:S448-53

Possible anti-HIV immunefactors in milk
• CD 8+ T-lymphocytes• HIV-specific secretory IgA• Lactobaccillus• Lactoferrin• Alpha-defensins• SLPI• Vitamin A
CD8+ T-lymphocytes
• Breast milk CD8+ T- lymphocytes withresponse to HIV-1 gag (Sabbaj et al, J Virol 2002, 76:7365-73)
• Recognition of and responses to HIV-1 antigensgag and env greater in magnitude from breastmilk CD8+ lymphocytes than from pairedperipheral blood CD8+ cells (P< 0.05) (Lohman et al, JInfect Dis 2003, 188:1666-74)
• Percentages of CD8+ cells were similar in bothbreast milk and blood
• Selective transport to breast milk?

HIV-specific sIgA
• HIV-specific sIgA, IgG and IgM have beenfound in colostrum and breast milk (Becquart, Bomsel)
• Colostral sIgA has most efficient ability toneutralize/bind HIV (Bomsel)
• No difference in quantity of HIV-specific sIgAor neutralizing activity in transmitters versusnon-transmitters (Becquart)
• However, Becquart’s study did not measureviral RNA or DNA in breast milk

Lactobaccillus ssp.
• Naturally occuring bacteria found ingastrointestinal tract of breastfeedinginfants
• New data showing their presence inbreast milk (Rodriguez)
• Anti-HIV activity found in vitro (Connor,
unpublished) exploring which of their productsare responsible
Lactoferrin
• Few studies specifically on lactoferrin’seffect on HIV-1 replication in breast milk
• Lactoferrin demonstrated inhibition ofHIV-1 replication at level of viralfusion/entry in vitro (Moriuchi and Moriuchi, 2001)
Alpha-defensins
• Peptides produced by immune cells• Anti-HIV activity among HIV+ long-term
nonprogressors• In breast milk, increased concentrations
associated with increased HIV RNA (predictorof transmission) (Kuhn et al, J AIDS 2005, 39:138-42)
• However, increased concentration associatedwith decreased risk of transmission duringdelivery and from breastfeeding
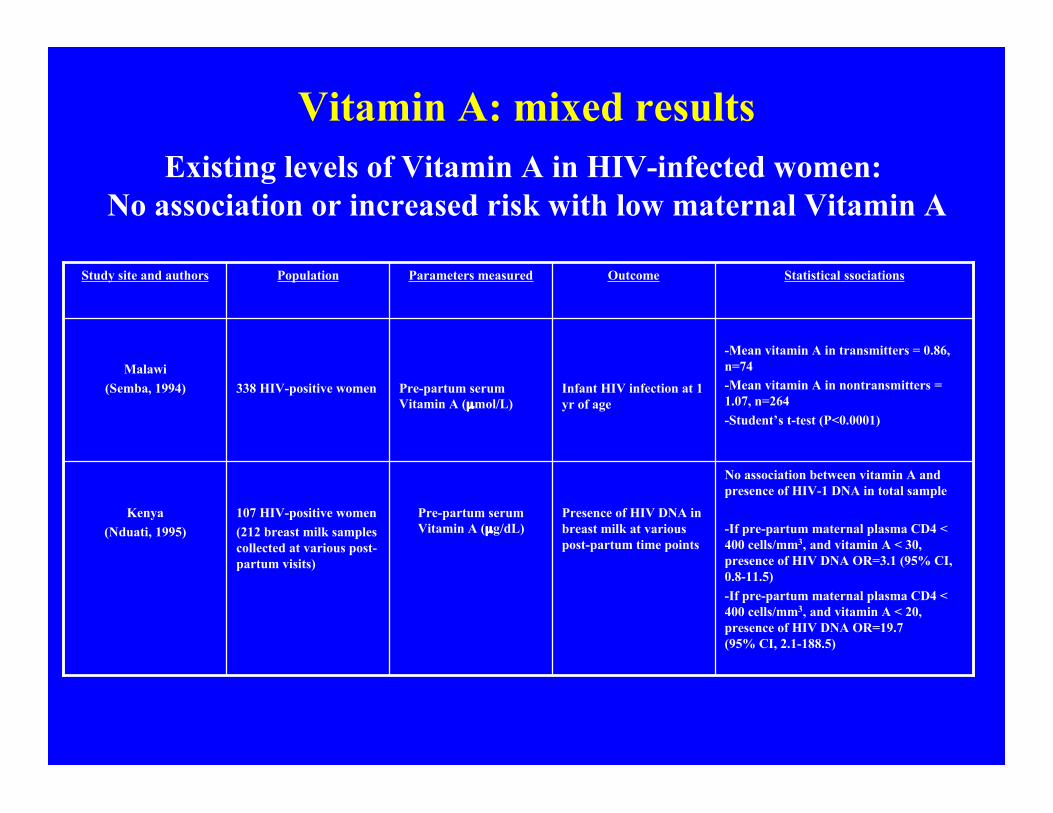
Vitamin A: mixed results
No association between vitamin A andpresence of HIV-1 DNA in total sample
-If pre-partum maternal plasma CD4 <400 cells/mm3, and vitamin A < 30,presence of HIV DNA OR=3.1 (95% CI,0.8-11.5)-If pre-partum maternal plasma CD4 <400 cells/mm3, and vitamin A < 20,presence of HIV DNA OR=19.7(95% CI, 2.1-188.5)
Presence of HIV DNA inbreast milk at variouspost-partum time points
Pre-partum serumVitamin A (µg/dL)
107 HIV-positive women(212 breast milk samplescollected at various post-partum visits)
Kenya(Nduati, 1995)
-Mean vitamin A in transmitters = 0.86,n=74-Mean vitamin A in nontransmitters =1.07, n=264-Student’s t-test (P<0.0001)
Infant HIV infection at 1yr of age
Pre-partum serumVitamin A (µmol/L)
338 HIV-positive womenMalawi
(Semba, 1994)
Statistical ssociationsOutcomeParameters measuredPopulationStudy site and authors
Existing levels of Vitamin A in HIV-infected women: No association or increased risk with low maternal Vitamin A

Vitamin A Intervention Studies:No difference or increased transmission
Overall MTCT RR withvitamin A vs. placebo = 1.38(95% CI 1.09-1.76, P= 0.009)-MTCT via breastfeeding RRwith vitamin A vs. placebo =1.33 (95% CI 0.95-1.86, P =0.10)
Infant HIV infectionincluding BF period -Infant HIV infection onlythrough BF
5000 IU preformed vitaminA and 30 mg beta caroteneor;- Vitamins B1, B2, B6,niacin, B12, C, E and folicacid, or;-Both, or;-Placebo(from 2nd trimester throughlactation)
1078 HIV- positive womenTanzania(Fawzi,2002, AIDS)
No difference in overall MTCTat 6wks, 12, and 24 mosbetween vitamin A and controlgroup-Vitamin A group had lessMTCT between 6wks and 24mos (P= 0.04)
Infant HIV infection at6wks, 12 and 24 mos of age
3 mg retinol, 30 mg iron,400 µg folate, or;- 30 mg iron, 400 µg folate(daily until delivery)-All women received 30 mgretinol at 6 wks postpartum
697 HIV-positive pregnantwomen at 18-28 wksgestation
Malawi(Kumwenda, 2002, CID)
No difference in risk of infantHIV infection betweenintervention and placebogroups
Infant HIV infection at 3months of age
5000 IU retinyl palmitateand 30 mg beta-carotenedaily during 3rd trimester,and 200,000 IU retinylpalmitate at delivery; or-Placebo
728 HIV-positive womenSouth Africa
(Coutsoudis, 1999)
Statistical ssociationsOutcomeInterventionPopulationStudy site and authors

Impact of Exclusive Breastfeedingversus Mixed Feeding
Illif et al, AIDS 2005, 19:699-708

Antiretroviral Therapy andMTCT
Shapiro et al, JID 2005, 192:720-7

Antiretroviral Therapy andMTCT
Shapiro et al, JID 2005, 192:713-9

Resistance w/ single dosenevrapine
• The majority of women (~65%) exposedto single-dose NVP have detectableNNRTI-associated resistance mutations6-36 weeks post-partum (Johnson et al. JID 192: 16-23,2005)
Resistance w/ single dosenevrapine
• Using sensitive PCR-based techniques,NVP-resistance mutations can persistup to 12-14 months after treatment inboth mothers and infants (Flys et al. JID 192: 24-29,2005)

Resistance w/ single dosenevrapine
• Women with detectable NNRTI-resistancemutations early in the postpartum periodhave inferior virologic response tosubsequent NNRTI-based treatments(Jourdain et al. NEJM 351:229-40, 2004)

Resistance w/ single dosenevrapine
• The frequency of NNRTI-associatedresistance mutations is significantlyhigher in women infected with HIV-1subtype C (62%) than HIV-1 subtypeA (19%) or D (36%) (Eshleman et al.JID 192: 30-36,2005)
Current Tanzanian policy• Single dose nevirapine 200 mg orally to mother at onset
of labor
• And single dose nevirapine 2 mg/kg to infant within 72hours of delivery
• Linking pregnant women to triple ART who have:– CD4+ count < 200 cells/mm3;or– WHO Stage 3 symptoms and CD4+ cell count ≤350; or– WHO Stage 4 regardless of CD4 + cell count
United Republic of Tanzania Ministry of Health, National Guidelines for the Clinical Management ofHIV and AIDS, 2005

Many questions• Final word on cell-free vs. cell-associated virus as
major contributor to transmission (perhaps both)• Source of viral RNA and proviral DNA – all from
plasma?• Role of infant intestinal inflammation (subclinical) in
increased transmission during mixed feeding• Role of infant’s immune system• Proportions of milk anti-viral factors: viral load in
breast milk?• Nevirapine- resistant virus from treatment at delivery
transmitted to infant through breastfeeding?• Effect of HAART for mothers throughout lactation on
breastfeeding transmission

Asanteni Sana
Thank you
Do you have questions?







