
1
Chapter Ⅴ.The Thyroid
PS Wang/ 2004.05

2
W.F.Ganong:Review of Medical Physiology 2003 20th Ed. Fig.18-1 #147

3W.F. Ganong: Review of Medical Physiology 2003 20th Ed. Fig.18-2 #148

4
• The thyroid gland is the only tissue of the body which is able to accumulate iodine in great quantities and combine it into a hormone.
• The basic unit of the thyroid gland is the thyroid follicle which consists of a hollow sphere made up of a single layer of epithelial cells which enclose a colloid-filled space.
PS Wang/2004.0
5

5M. E. Hadley: Endocrinology 2nd ed. 1988 fig.13.4 #2019

6
• T3 or T4 may be secreted directly into the criculation or stored in the follicle after combination with a protein to form thyroglobulin (a kind of glycoprotein with MW = 680,000)
• When needed, the thyroglobulin is hydrolyzed by a protease enzyme present in the follicular cells thereby freeing thyroxine into the blood stream
PS Wang/2004.0
5

7Guyton & Hall : Textbook of Medical Physiology 10th ed.2000 fig.76-2 #364

8
Function of Thyroid Cells
1. Thyroid cells collect and transport the iodine and synthesize the thyroglobulin, then secrete it into the colloid.
2. Remove the thyroid hormones from thyroglobulin and secrete them into the circulation.
PS Wang/2004.0
5

9
The steps in thyroid hormone biosynthesis are as follows:1. I- trapping2. I- oxidized to I2
3. Iodination of tyrosine to mono-iodotyrosine (MIT)
4. Further iodination of MIT to di-iodotyrosine (DIT)
5. Condensation of 2 molecules of DIT to form thyroxin
6. (Possible) condensation of 1 molecule of MIT and 1 molecule of DIT to form tri-iodothyronine (T3 or TRIT). A summary of these reactions is given in Figure 7-2.
PS Wang/2004.0
5

10
#144

11W.F. Ganong: Review of Medical Physiology 2003 20th Ed. #153 p329
12
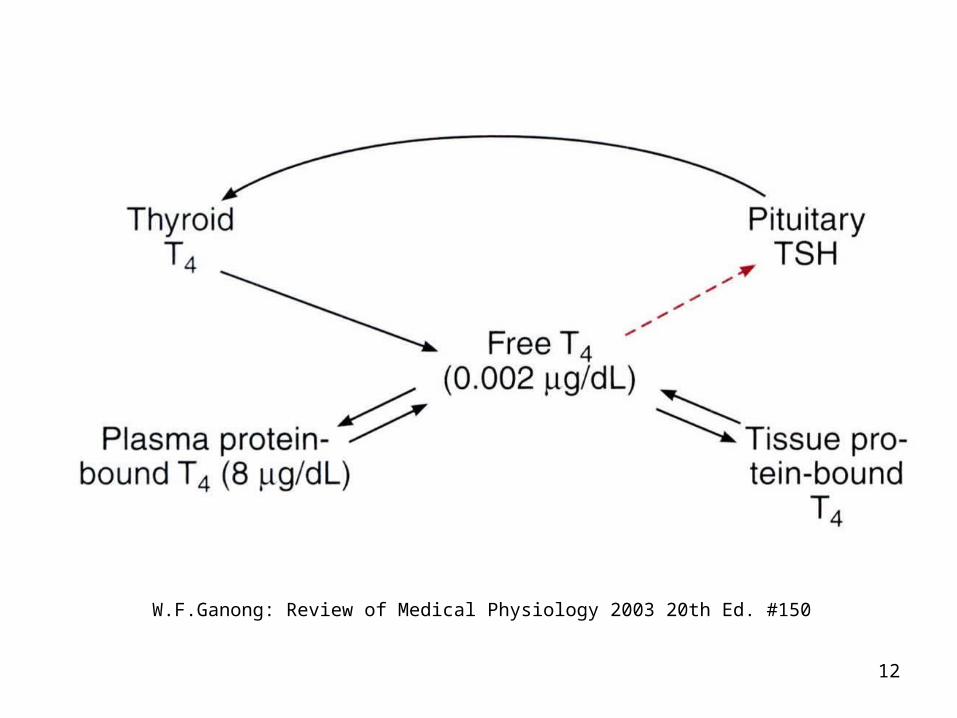
W.F.Ganong: Review of Medical Physiology 2003 20th Ed. #150

13
#1423

14F.S. Greenspan & D. G. Gardner : Basic &Clinical Endocrinology 7th ed.2004 p228 #1324
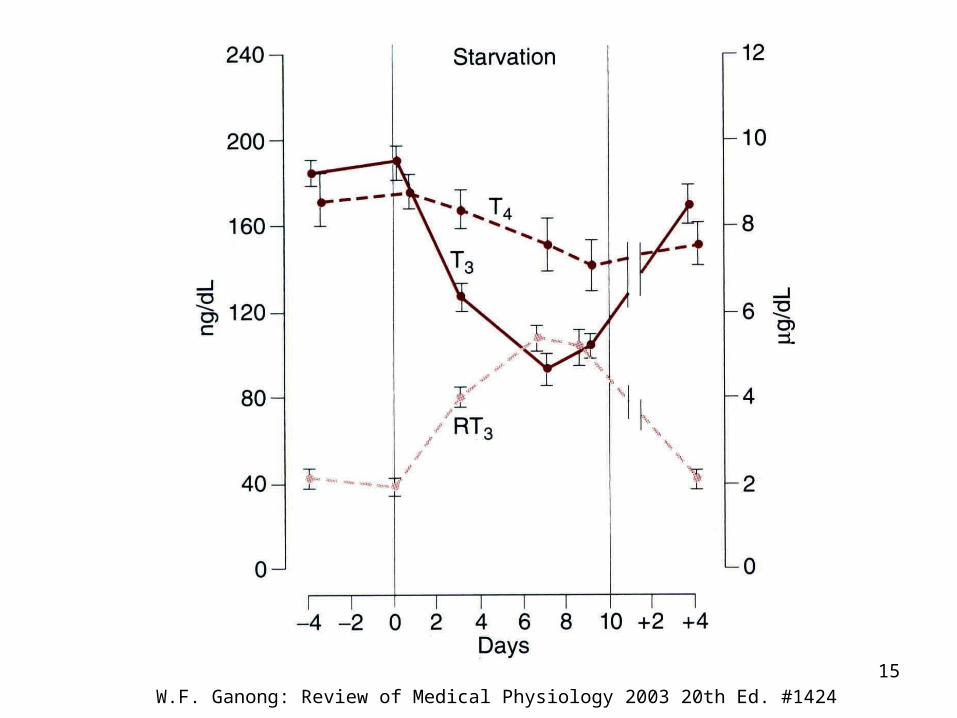
15W.F. Ganong: Review of Medical Physiology 2003 20th Ed. #1424
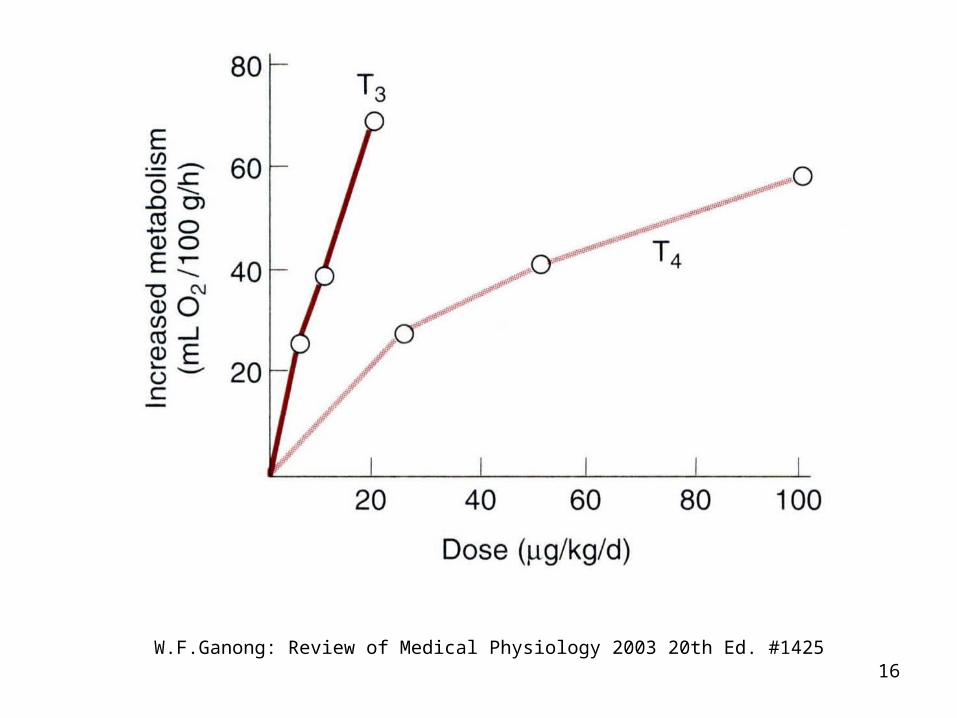
16W.F.Ganong: Review of Medical Physiology 2003 20th Ed. #1425
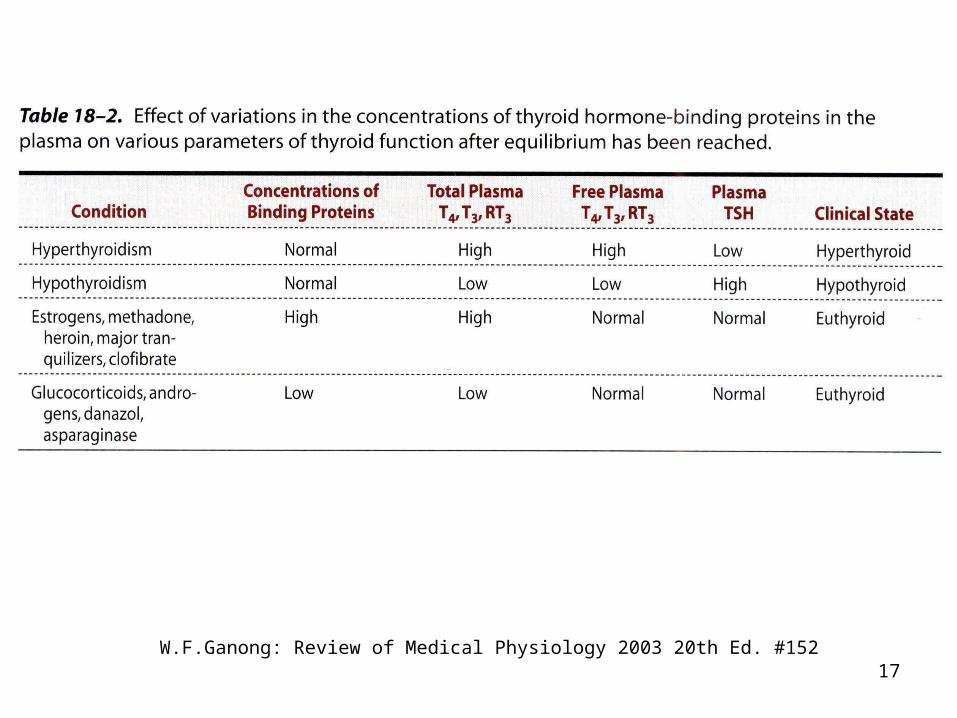
17W.F.Ganong: Review of Medical Physiology 2003 20th Ed. #152

18
Item T3 T4
No. of I 3 4
Biosynthesis
Biological Activity
Half –Life
Amount in Circulation
Free Form in Circulation
Binding Affinity with TBG
MIT+DIT
4-5
1 day
0.35%
1%
1
DIT+DIT
1
1 week
99.6%
0.1%
10
PS Wang/2004.0
5

19
J. Tepperman & H. M. Tepperman :Metabolic and Endocrine Physiology 5th ed.1987 p173 #1450

20M. E. Hadley: Endocrinology 2th ed. 1988 fig.13.10 #2021

21
A classification of antithyroid drugs and substances can be made according to mode of action
• Inhibition of iodide trapping:Thiocyanates ( raw soybeans, cabbage)Perchlorates
• Inhibition of thyroxin synthesis (iodination)ThiouracilPropylthiouracilMethylthiouracilThioureaMethimazole (Tapazole)
• Destruction of thyroid tissue:131I in large dosage
• Mode of action unknown :Iodides in much higher dosage than dietary requirements
PS Wang/2004. 05

22
J. Tepperman & H. M. Tepperman :Metabolic and Endocrine Physiology 5th ed.1987 p167 #145
24

23
• PBI = protein bound iodine. Determinations of blood levels of PBI have become a test of the amount of circulating T4 or T3.
• LATS = the long-acting thyroid stimulator, an abnormal immunoglobulin found in the plasma, may also cause a hyperthyroid state.
PS Wang/2004.0
5

24
LONG-ACTING THYROID STIMULATOR(LATS) Abnormonal factor in plasma of patients who have Graves’ disease.
• Protein; immunoactive against thyroid.• Different from TSH; stimulates thyroid more slow
ly, acts longer.• Cleared from blood more slowly than TSH.• Crosses placental barrier; neonate may have sy
mptoms of Graves’ disease.• Symptoms of Graves’ disease.
Produced by lymphocytes, not found in pituitary gland.
• May include group of 3 immunoglobulins.
PS Wang/2004.0
5

25
W.F.Ganong: Review of Medical Physiology 2003 20th
Ed. #154

26
L.E. Mcdonald:Veterinary Endocrinology and Reproduction. 1976 2nd Ed. p54 #23

27
Hypothyroidism• Causes ----
(1) endemic colloid goiter: I2↓ T4↓ TSH↑ thyroglobulin (colloid) ↑ thyroid size ↑
(2) idiopathic nontoxic colloid goiter : goitrogen T4 ↓(or normal) TSH↑ thyroid size ↑
• Symptoms ----sleeping 14-16 h/daymuscular sluggishheart rate ↓cardiac output ↓mental sluggishnessmyxedema (↑mucopolysaccharides bagginess
under the eyes & swelling of the face)arteriosclerosiscretinism
PS Wang/2004. 05

28
• Diagnosis ----
(1) protein-bound iodine (PBI) ↓
(2) basal metabolic rate (BMR) ↓
(3) uptake of radioactive iodine ↓
• Treatment----
(1) iodine
(2) T4
Hypothyroidism
PS Wang/2004. 05

29
Hyperthyrodism• Causes ----
hyperplastic thyroid, size ↑thyroid hormone secretion rate ↑plasma [ TSH ]↓plasma [ TSH ] ↑localized adenoma (tumor)
• Symptoms ---- intolerance to heatincreased sweatingweight lossdiarrheamuscular weaknessnervousness or the psychic disordersextreme fatigue but inability to sleeptremor of the handsexophthalmos ---- protrusion of the eyeballs
PS Wang/2004. 05
30
• Diagnosis ---- (1) PBI↑(2) BMR↑, 60%(3) uptake of 131I ↑
• Treatment ---- (1) Tx after administration of PTU (↓BMR) and high conc. of iodide
(↓thyroid size & ↓ blood supply ) operative mortality < 0.1%
(2) radiothyroidectomy by 131I (> 5 mCi)
Hyperthyrodism
PS Wang/2004. 05

31
Exophthalmos
This occurs in 50% of patients and often precedes the development of obvious hyperthyroidism. A subpopulation of fibroblasts in the orbits ultimately develop into adipocytes, and these preadipocyte fibroblasts contain TSH receptor protein. The current theory of the development of exophthalmos is that when stimulated by the TSH receptor-stimulating antibodies in the circulation, these cells release cytokines that promote inflammation and edema.
Ganong, W.F. Review of Medical Physiology 21st Edition, ©2003 by The Mc Graw-Hill Companies, Inc.
32
Hashimoto’s Thyroiditis
In Hashimoto’s thyroiditis, autoimmune antibodies destroy the thyroid with little if any stimulation, producing hypothyroidism.
Ganong, W.F. Review of Medical Physiology 21st Edition, ©2003 by The Mc Graw-Hill Companies, Inc.







