
11
Building the New Model for SU in Health Care Building the New Model for SU in Health Care
June M. Gertig, J.D.June M. Gertig, J.D.Senior AssociateSenior AssociateAltarum InstituteAltarum Institute
Michael T. Flaherty, Ph.D.Michael T. Flaherty, Ph.D.Institute for Research, Education and Training in AddictionsInstitute for Research, Education and Training in AddictionsNortheast Addiction Technology Transfer CenterNortheast Addiction Technology Transfer CenterPittsburgh, PA and Albany, NYPittsburgh, PA and Albany, NY
Strategic Planning for Providers to Improve Business Practices ConferenceStrategic Planning for Providers to Improve Business Practices ConferenceHyatt Regency Crystal CityHyatt Regency Crystal CityArlington, VirginiaArlington, VirginiaOctober 21, 2009October 21, 2009
22
Presentation OverviewPresentation Overview Our approach to understanding SUDs has expanded from a Our approach to understanding SUDs has expanded from a
predominant focus on the acute stages of the illness to include a focus predominant focus on the acute stages of the illness to include a focus on chronic aspects. Systems of care must now adapt to this shift.on chronic aspects. Systems of care must now adapt to this shift.
We will suggest a new view of SUDs over a continuum of care We will suggest a new view of SUDs over a continuum of care specifically related to this new common vision and a model for specifically related to this new common vision and a model for addressing the illness with this new understanding.addressing the illness with this new understanding.
We will establish a recovery focus to complement the current focus on We will establish a recovery focus to complement the current focus on pathology as dual components in defining and addressing the Illnesspathology as dual components in defining and addressing the Illness
We will provide you measures that can be used by your states and We will provide you measures that can be used by your states and agencies to “lead” in shifting to this recovery focused model, while agencies to “lead” in shifting to this recovery focused model, while enhancing and providing quality care. You will understand what is enhancing and providing quality care. You will understand what is meant by Recovery Oriented Systems of Care (ROSCs) and some of meant by Recovery Oriented Systems of Care (ROSCs) and some of the future implications of ROSCs for science, policy, reimbursement, the future implications of ROSCs for science, policy, reimbursement, prevention, intervention, treatment and recoveryprevention, intervention, treatment and recovery

After the PresentationAfter the Presentation
We will work together to begin to We will work together to begin to understand how to expand your understand how to expand your networks to include recovery support networks to include recovery support providers providers
33

44
Why We Are Here TodayWhy We Are Here Today
Of the over 7 million Americans ages 18-25 who were classified as Of the over 7 million Americans ages 18-25 who were classified as needing treating in the past year, only 7% received the help they needing treating in the past year, only 7% received the help they needed at a specialty care facility.needed at a specialty care facility. (SAMHSA, June 29, 2009)(SAMHSA, June 29, 2009)
In 2007, 20.8 million persons (8.4 percent of the population aged 12 In 2007, 20.8 million persons (8.4 percent of the population aged 12 or older) needed specialty treatment for an illicit drug or alcohol use or older) needed specialty treatment for an illicit drug or alcohol use problem but did not receive it.problem but did not receive it. (SAMHSA, 2008)(SAMHSA, 2008)
In 2005, federal, state and local government spending as a result of In 2005, federal, state and local government spending as a result of substance abuse and addiction was a least $467.7 billion or 10.7% of substance abuse and addiction was a least $467.7 billion or 10.7% of their combined $4.4 trillion budget.their combined $4.4 trillion budget. (CASA, 2009)(CASA, 2009)
55
Why We Are Here TodayWhy We Are Here Today Of every dollar Of every dollar federal and state governmentsfederal and state governments spent on substance abuse spent on substance abuse
and addiction in 2005 ($467.7 billion), 95.6 cents went to shoveling up and addiction in 2005 ($467.7 billion), 95.6 cents went to shoveling up the wreckage and only 1.9 cents to prevention and treatment, 0.4 cents the wreckage and only 1.9 cents to prevention and treatment, 0.4 cents to research, 1.4 cents to taxation or regulation and 0.7 cents to to research, 1.4 cents to taxation or regulation and 0.7 cents to
interdiction.interdiction. (CASA, 2009)(CASA, 2009)
Still, it is estimated that there are over 27 million Americans in recovery Still, it is estimated that there are over 27 million Americans in recovery today!today!
In 2008, there were 45-50 million individuals who were problematic users In 2008, there were 45-50 million individuals who were problematic users
of alcohol or drugs and 25 million who need treatment for sameof alcohol or drugs and 25 million who need treatment for same.. (Clark, 2008)(Clark, 2008)

Why We Are Here TodayWhy We Are Here TodayAddiction Affects:Addiction Affects:
1 in 10 Americans 1 in 10 Americans
1 in 5 families1 in 5 families
1 in 7 workers 1 in 7 workers
1 in 20 newborns1 in 20 newborns
35% of ALL school 35% of ALL school childrenchildren
1 in 8 veterans1 in 8 veterans
1 in 2 homeless1 in 2 homeless
1 in 4 elderly 1 in 4 elderly
80% of those in jail80% of those in jail
60% of families in children 60% of families in children and youth services and youth services
66

America’s #1 Health Problem!America’s #1 Health Problem!
Robert Wood Johnson Foundation, The. (1993). Robert Wood Johnson Foundation, The. (1993). Substance Abuse: The Substance Abuse: The Nation’s Number One Health ProblemNation’s Number One Health Problem, Key Indicators for Policy. , Key Indicators for Policy.
Princeton, N.J.: Schneider Institute for Health Policy, Brandeis UniversityPrinceton, N.J.: Schneider Institute for Health Policy, Brandeis University
Robert Wood Johnson Foundation, The. (2001). Robert Wood Johnson Foundation, The. (2001). Substance Substance Abuse: The Nation’s Number One Health ProblemAbuse: The Nation’s Number One Health Problem. Princeton, . Princeton, N.J.: Schneider Institute for Health Policy, Brandeis University.N.J.: Schneider Institute for Health Policy, Brandeis University.
77
What Do We Know About What Do We Know About Chronic Care?Chronic Care?
As we design chronic care models for As we design chronic care models for recovery from SUDs, what can we learn recovery from SUDs, what can we learn from the best chronic care models for from the best chronic care models for other illnesses? Diabetes? Asthma? other illnesses? Diabetes? Asthma? Chronic obstructive pulmonary disease? Chronic obstructive pulmonary disease? Congestive heart failure?Congestive heart failure?
88

Chronic Care ModelChronic Care Model
Wagner, E.H. (1998). Chronic Disease Management: What Will it Take to Wagner, E.H. (1998). Chronic Disease Management: What Will it Take to Improve Care for Chronic Illness? Improve Care for Chronic Illness? Effective Clinical PracticeEffective Clinical Practice, 1, 2-4., 1, 2-4.
99

1010
Chronic Care Model ElementsChronic Care Model Elements
Self-management support. Self-management support. Involve the patient in lifestyle Involve the patient in lifestyle changes and the development of illness management skills changes and the development of illness management skills using education, goal setting, action planning, problem solving using education, goal setting, action planning, problem solving and follow-up.and follow-up.
Delivery system designDelivery system design. Transform community practices . Transform community practices from a reactive physician model to a proactive model that from a reactive physician model to a proactive model that uses multidisciplinary care teams to provide planned care at uses multidisciplinary care teams to provide planned care at each appointment, including use of group appointments, and each appointment, including use of group appointments, and telephone and e-mail consultations. telephone and e-mail consultations.
Decision supportDecision support. Base care on effective evidence-based . Base care on effective evidence-based care guidelines and use systems to inform and prompt care guidelines and use systems to inform and prompt providers and patients about care needs. providers and patients about care needs.

Chronic Care Model ElementsChronic Care Model Elements
Clinical information systemsClinical information systems. Use of relatively simple . Use of relatively simple systems to identify and track patient information can improve systems to identify and track patient information can improve chronic care outcomes. chronic care outcomes.
Community.Community. Identify or develop resources and programs in Identify or develop resources and programs in the community to support healthy lifestyles and provide the community to support healthy lifestyles and provide information to patients on these resources. Primary care information to patients on these resources. Primary care practices do not have the resources necessary to provide all practices do not have the resources necessary to provide all the support patients with chronic conditions need to be the support patients with chronic conditions need to be healthy. healthy.
Health systems.Health systems. Create a quality-oriented culture for Create a quality-oriented culture for providers through leadership commitment, incentives for providers through leadership commitment, incentives for continuous quality improvement and strategies to align continuous quality improvement and strategies to align reimbursement with desired care.reimbursement with desired care.
1111

IOM Is Telling Us the Same ThingIOM Is Telling Us the Same Thing
Institute of Medicine. (2001). Institute of Medicine. (2001). Crossing the Quality Chasm: A Crossing the Quality Chasm: A New Health System for the 21New Health System for the 21stst Century. Century. Washington, D.C.: Washington, D.C.:
National Academy Press.National Academy Press.1212

1313
HealthcareHealthcare Reform:Reform:
Principles of Care for the 21Principles of Care for the 21stst Century Century Must be Must be specific tospecific to the needs of the needs of individualsindividuals who require more time, who require more time,
offering a broad array of resources over a offering a broad array of resources over a continuum of carecontinuum of care
Must provide Must provide coordinated and continuouscoordinated and continuous attention to the attention to the individual’s needs for information and behavioral changeindividual’s needs for information and behavioral change
Must provide access Must provide access to necessary clinicalto necessary clinical expertise expertise
From: Institute of Medicine. (2001). From: Institute of Medicine. (2001). Crossing the Quality Chasm: A New Health System for the 21Crossing the Quality Chasm: A New Health System for the 21stst Century. Century. Washington, D.C.: National Academy Press.Washington, D.C.: National Academy Press.

1414
HealthcareHealthcare ReformReform::
Principles of Care for the 21Principles of Care for the 21stst Century Century
Care is Care is person-centeredperson-centered and based on continuous healing and based on continuous healing relationshipsrelationships
Care is Care is customizedcustomized according to patient need and values according to patient need and values
The patient is the The patient is the source of controlsource of control
From: Institute of Medicine. (2001). From: Institute of Medicine. (2001). Crossing the Quality Chasm: A New Health System for the 21Crossing the Quality Chasm: A New Health System for the 21stst Century. Century.Washington, D.C.: National Academy Press.Washington, D.C.: National Academy Press.

1515
HealthcareHealthcare ReformReform::
Rules for a New ModelRules for a New Model
Knowledge is sharedKnowledge is shared and information flows and information flows freelyfreely
Decision making is Decision making is evidenced-basedevidenced-based
Needs are anticipatedNeeds are anticipated
WasteWaste is continuously is continuously decreaseddecreased
CooperationCooperation among clinicians is a priority among clinicians is a priority
From: Institute of Medicine. (2001). From: Institute of Medicine. (2001). Crossing the Quality Chasm: A New Health System for the 21Crossing the Quality Chasm: A New Health System for the 21stst Century. Century.Washington, D.C.: National Academy Press.Washington, D.C.: National Academy Press.

IOM Is Bringing These Concepts to SUDsIOM Is Bringing These Concepts to SUDs
Institute of Medicine. (2006). Institute of Medicine. (2006). Improving the Quality of Healthcare for Mental and Substance-Use Improving the Quality of Healthcare for Mental and Substance-Use Conditions.Conditions. Washington, DC: National Academies Press. Washington, DC: National Academies Press.
1616
1717
A Chronic Care Model for SUDsA Chronic Care Model for SUDs
““If addiction is best considered a If addiction is best considered a chronicchronic condition, then we condition, then we are are not providing appropriate treatmentnot providing appropriate treatment for many for many addicted patients.” addicted patients.” (McLellan, 2002)(McLellan, 2002)
““America may be treating a major health problem -- America may be treating a major health problem -- substance dependence -- with substance dependence -- with a treatment approach not a treatment approach not appropriate to the nature of the illness.” appropriate to the nature of the illness.” (Flaherty, 2006)(Flaherty, 2006)

1818
Justification for a Justification for a Chronic UnderstandingChronic Understanding
In 2008, 52% percent of admissions for treatment were 2nd In 2008, 52% percent of admissions for treatment were 2nd attempts and 33% were 3rd attempts or more.attempts and 33% were 3rd attempts or more.
Today, in America, on average it takes 3 to 4 treatment attempts Today, in America, on average it takes 3 to 4 treatment attempts before an individual achieves a year of sobriety. before an individual achieves a year of sobriety. ((Clark, 2008)Clark, 2008)
““We need a chronic understanding” We need a chronic understanding” (Clark, 2008)(Clark, 2008)

1919
The Continuum of CareThe Continuum of Care
Continuum of Care for a ChronicContinuum of Care for a Chronic IllnessIllness
Prevention-Intervention-Treatment-Recovery Supports*Prevention-Intervention-Treatment-Recovery Supports*
*R*Recovery linkage and supports are at each level of the continuum and ecovery linkage and supports are at each level of the continuum and surround all phases and levels of care. Also, all disciplines of practitioners surround all phases and levels of care. Also, all disciplines of practitioners from Prevention Experts, Primary Care Physicians, Interventionists/Health from Prevention Experts, Primary Care Physicians, Interventionists/Health Educators will become part of the workforce addressing the illness with the Educators will become part of the workforce addressing the illness with the traditional SU provider becoming the “Specialist Care” Provider and those in traditional SU provider becoming the “Specialist Care” Provider and those in recovery becoming the Peer-Based Recovery Specialist throughout the recovery becoming the Peer-Based Recovery Specialist throughout the continuum. continuum.
2020
A New Course is Set!A New Course is Set!
Substance dependenceSubstance dependence should be viewed as a should be viewed as a potentially chronic potentially chronic illnessillness (e.g., HIV, asthma, diabetes, and hypertension) and not as an (e.g., HIV, asthma, diabetes, and hypertension) and not as an acute illness (e.g., cold or flu). acute illness (e.g., cold or flu).
Systems of careSystems of care, including treatment, research and , including treatment, research and funding funding mechanismsmechanisms, must reflect the best practices proven to prevent and , must reflect the best practices proven to prevent and treat chronic illness and achieve treat chronic illness and achieve sustained recoverysustained recovery..
When treated as a chronic illnessWhen treated as a chronic illness, relapse rates for substance , relapse rates for substance
dependence are as good as or better than other chronic illnessesdependence are as good as or better than other chronic illnesses (McLellan, Lewis, O’Brien & Kleber, 2000)
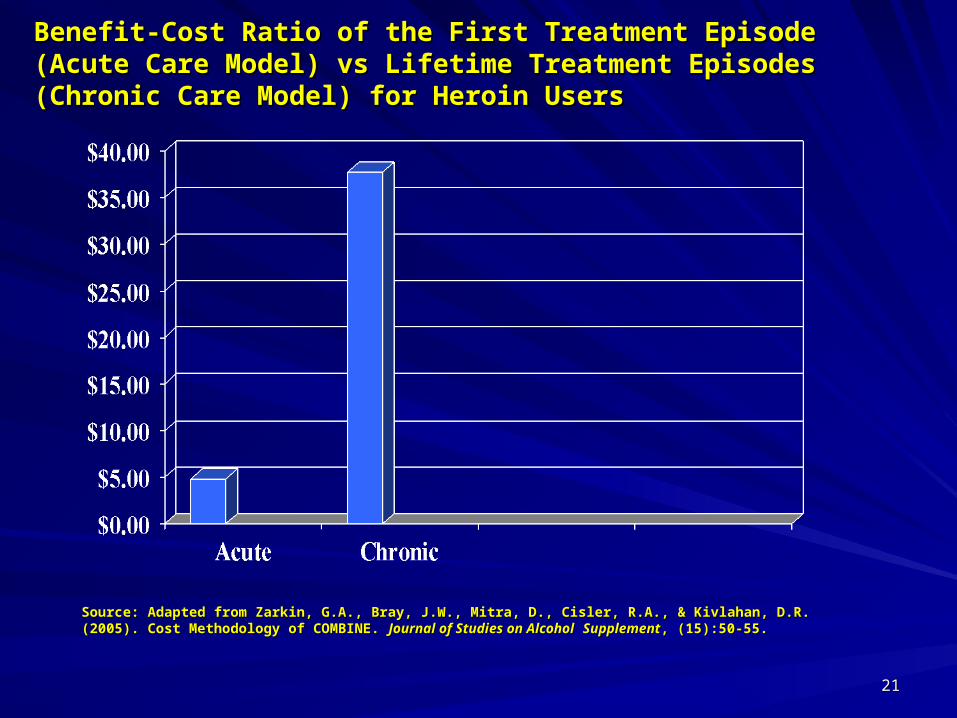
Benefit-Cost Ratio of the First Treatment Episode (Acute Care Benefit-Cost Ratio of the First Treatment Episode (Acute Care Model) vs Lifetime Treatment Episodes (Chronic Care Model) for Model) vs Lifetime Treatment Episodes (Chronic Care Model) for Heroin UsersHeroin Users
Source: Adapted from Zarkin, G.A., Bray, J.W., Mitra, D., Cisler, R.A., & Kivlahan, D.R. (2005). Cost Source: Adapted from Zarkin, G.A., Bray, J.W., Mitra, D., Cisler, R.A., & Kivlahan, D.R. (2005). Cost Methodology of COMBINE. Methodology of COMBINE. Journal of Studies on AlcoholJournal of Studies on Alcohol SupplementSupplement, (15):50-55., (15):50-55.
2121

2222
The Promise of a Recovery FocusThe Promise of a Recovery Focus
Individuals will enhance outcomes by staying longer in treatment Individuals will enhance outcomes by staying longer in treatment and/or recovery supports. (Today only 1 in 5 individuals use and/or recovery supports. (Today only 1 in 5 individuals use treatment and recovery support services concurrently.)treatment and recovery support services concurrently.) (Moos & Moos, 2005)
An individual’s rate of risk of future relapse will drop below 15% if An individual’s rate of risk of future relapse will drop below 15% if he/she remains in stable remission for 4-5 years.he/she remains in stable remission for 4-5 years. (Moos & Moos, 2005)
Individuals will be supported through episodes of reoccurrence Individuals will be supported through episodes of reoccurrence based on the fact that resolution of severe problems can span years based on the fact that resolution of severe problems can span years (sometimes decades) and that incorporation of recovery support (sometimes decades) and that incorporation of recovery support and ongoing care minimize reoccurrences.and ongoing care minimize reoccurrences. (Dennis, Scott & Hristova, 2002)

2323
The Promise of a Recovery FocusThe Promise of a Recovery Focus
Individuals will not experience reoccurrence within 90 Individuals will not experience reoccurrence within 90 days after discharge from treatment at such a high rate days after discharge from treatment at such a high rate (currently 80%). (currently 80%). (Humphreys, Moos & Cohen, 1997)(Humphreys, Moos & Cohen, 1997)
Individual wellness will increase and be measurable. Individual wellness will increase and be measurable. (Moos (Moos
& Moos, 2005)& Moos, 2005)

Shifting the Paradigm: Shifting the Paradigm: Building a Recovery Oriented System of Building a Recovery Oriented System of CareCare
White, W.L. (2008). White, W.L. (2008). Recovery Management and Recovery-oriented Systems of Care: Scientific Rationale and Recovery Management and Recovery-oriented Systems of Care: Scientific Rationale and Promising PracticesPromising Practices. Pittsburgh, PA: Northeast Addiction Technology Transfer Center, Great Lakes Addiction . Pittsburgh, PA: Northeast Addiction Technology Transfer Center, Great Lakes Addiction Technology Transfer Center, and Philadelphia Department of Behavioral Health/mental Retardation Services.Technology Transfer Center, and Philadelphia Department of Behavioral Health/mental Retardation Services.
2424

2525
Recovery-Oriented CareRecovery-Oriented CareTreatmentTreatment focuses on stabilizing the client and initiating remission, focuses on stabilizing the client and initiating remission, thereby creating the greatest opportunity for initial and sustained thereby creating the greatest opportunity for initial and sustained recovery.recovery.
Recovery-oriented care focuses on:
The acquisition and maintenance of recovery capital (internal and external assets required for recovery initiation and self-maintenance),
Measurable global health (physical, emotional, relational, and spiritual), and
Community integration (meaningful roles, relationships, and activities).
Building resiliency and wellness
2626
RRecovery-ecovery-OOriented riented SSystems of ystems of CCare:are:Building a Vision Building a Vision
ROSCROSC are are networksnetworks of formal and informal services developed and of formal and informal services developed and mobilized to address pathology and mobilized to address pathology and initiate and initiate and sustain long-term sustain long-term recoveryrecovery for individuals and families impacted by severe substance for individuals and families impacted by severe substance use disorders. use disorders.
The The systemsystem in ROSC is in ROSC is not a treatment agencynot a treatment agency but a macro level but a macro level organization of a community, a state or a nation.organization of a community, a state or a nation.
ROSC ROSC build on the strengthsbuild on the strengths of the individual, family and community of the individual, family and community while constantly implementing system improvement.while constantly implementing system improvement.

2727
Recovery Focused System Recovery Focused System Performance MeasuresPerformance Measures
Service ProcessService Process Measures:Measures:
a. treatment attraction and accessa. treatment attraction and access
b. screening, assessment and level of care placementb. screening, assessment and level of care placement
c. composition of service teamc. composition of service team
d. service relationship (engagement, retention, discharge) d. service relationship (engagement, retention, discharge)
e. service dose, scope and qualitye. service dose, scope and quality
f. locus of service delivery/influence on post treatment f. locus of service delivery/influence on post treatment
recovery environmentrecovery environment
g. assertive linkage to communities of recoveryg. assertive linkage to communities of recovery
h. post-treatment monitoring,support and early-re h. post-treatment monitoring,support and early-re
intervention intervention
2828
Recovery Focused System Recovery Focused System Performance MeasuresPerformance Measures
Recovery Outcome MeasuresRecovery Outcome Measures
A. Pre-post treatment changes in:A. Pre-post treatment changes in: AOD use/consequencesAOD use/consequences living environmentliving environment physical health and health care costsphysical health and health care costs emotional healthemotional health family relationships and family healthfamily relationships and family health citizenship (legal status, employment, community citizenship (legal status, employment, community participation, community service)participation, community service) quality of life (spirituality, life meaning, purpose)quality of life (spirituality, life meaning, purpose) B. Post-treatment ServiceB. Post-treatment Service utilization of professional servicesutilization of professional services utilization of indigenous recovery supportsutilization of indigenous recovery supports C. Changes in family and community recovery capital C. Changes in family and community recovery capital
White, W. – Recovery Management and Recovery-Oriented Systems of Care: Scientific Rationale and Promising Practices, Northeast ATTC, White, W. – Recovery Management and Recovery-Oriented Systems of Care: Scientific Rationale and Promising Practices, Northeast ATTC, Great Lakes ATTC and DBHMRS, Pittsburgh, Pa. 2008 Great Lakes ATTC and DBHMRS, Pittsburgh, Pa. 2008

Peer-Based Recovery Support TodayPeer-Based Recovery Support Today
White, W.L. (2009). Peer-based addiction recovery support: history, theory, practice, and scientific evaluation. Chicago, IL: Great Lakes Addiction Technology Transfer Center and Philadelphia Department of Behavioral Health and Mental Retardation Services.
2929

3030
Recovery Management Recovery Management
““Recovery managementRecovery management (RM) is a philosophical framework for (RM) is a philosophical framework for organizing addiction treatment servicesorganizing addiction treatment services to provide pre-recovery to provide pre-recovery identification and engagement, recovery initiation and stabilization, identification and engagement, recovery initiation and stabilization, long-term recovery maintenance, and long-term recovery maintenance, and quality of life enhancementquality of life enhancement for for
individuals and families affected by severe substance use disorders.”individuals and families affected by severe substance use disorders.” (White, 2008) (White, 2008)
““Peer-Based Recovery SupportPeer-Based Recovery Support (P-BRS) is the process of giving and (P-BRS) is the process of giving and receiving non-professional, non-clinical assistance to achieve and receiving non-professional, non-clinical assistance to achieve and
sustain long-term recovery from alcohol and other drugs.”sustain long-term recovery from alcohol and other drugs.” (Personal
Communication from W. White, 2008)
3131
Role Clarification and Workforce Role Clarification and Workforce DevelopmentDevelopment
Treatment professionalsTreatment professionals are formally and adequately educated and use are formally and adequately educated and use proven scientific and medical practices (e.g., EBPs) to support their proven scientific and medical practices (e.g., EBPs) to support their
professional knowledge and treatment approach to each individual.professional knowledge and treatment approach to each individual. (White, (White,
2009)2009)
Peer-Based Recovery SpecialistsPeer-Based Recovery Specialists use experiential knowledge without use experiential knowledge without extolling the superiority of a particular conceptual framework or method of extolling the superiority of a particular conceptual framework or method of treatment. PBR is founded on the premise that the nature of the helper treatment. PBR is founded on the premise that the nature of the helper and the helping relationship are more important than the source of and the helping relationship are more important than the source of authority upon which the helper draws.authority upon which the helper draws. (White, 2009)(White, 2009)

How do we shift our focus to recovery oriented systems of care?
3232

3333
Start with Critical Questions and the Need for SCIENCE! What is your “state” or community definition of recovery?What is your “state” or community definition of recovery?
When and where does recovery begin?When and where does recovery begin?
Can a person be in recovery in a day, week, month… year …an Can a person be in recovery in a day, week, month… year …an hour?hour?
What is recovery for an adolescent?What is recovery for an adolescent?
Is there such a thing as medication-assisted recovery? Is there such a thing as medication-assisted recovery?
Can a person be on methadone and be in recovery? Can a person be on methadone and be in recovery?
Can a person be off their drug of choice, still smoke 3 packs a day, Can a person be off their drug of choice, still smoke 3 packs a day, and be in recovery?and be in recovery?

3434
Scientific QuestionsScientific Questions
How many people in the US are in recovery?How many people in the US are in recovery?
Are there different trajectories into recovery for different groups and Are there different trajectories into recovery for different groups and individuals?individuals?
Are there common themes to recovery?Are there common themes to recovery?
How effective and cost effective are ROSC?How effective and cost effective are ROSC?
How do we study recovery qualitatively and quantitatively? How do we study recovery qualitatively and quantitatively?
What leads to sustained recovery?What leads to sustained recovery?
3535
Definitions of RecoveryDefinitions of RecoveryDefinitions of RecoveryDefinitions of Recovery
Recovery from alcohol, drug problems (or gambling) is a Recovery from alcohol, drug problems (or gambling) is a process of process of changechange through which an individual achieves abstinence through which an individual achieves abstinence andand improved health, wellness, and quality of life.improved health, wellness, and quality of life.
RecoveryRecovery will be measured by one’s achievement of abstinence and will be measured by one’s achievement of abstinence and other measuresother measures of life, health and community success.of life, health and community success.
(Center for Substance Abuse Treatment, 2006)
3636
Points of ClarificationPoints of Clarification
Recovery is not synonymous with any specific method of attaining it.Recovery is not synonymous with any specific method of attaining it.
Abstinence vs. sobriety vs. recoveryAbstinence vs. sobriety vs. recovery
Medication assisted treatment or Medication Assisted Recovery – Medication assisted treatment or Medication Assisted Recovery – addiction vs. substance dependenceaddiction vs. substance dependence
What about Tobacco?What about Tobacco?
When is one in recovery? When is one in recovery?
• when one quits usingwhen one quits using
• early sobriety: 1-12 months early sobriety: 1-12 months
• sustained recovery: 1-5 yearssustained recovery: 1-5 years
• stable recovery: 5+ yearsstable recovery: 5+ years
• full recovery: no other harmful substance dependencefull recovery: no other harmful substance dependence
Betty Ford Consensus Panel, 2009Betty Ford Consensus Panel, 2009

Definitions of RecoveryDefinitions of Recovery
RecoveryRecovery – A voluntarily maintained lifestyle comprised of – A voluntarily maintained lifestyle comprised of sobriety, personal health and citizenship. sobriety, personal health and citizenship.
Betty Ford Consensus Panel. (2007). What is recovery? A working definition from the Betty Ford Institute. Betty Ford Consensus Panel. (2007). What is recovery? A working definition from the Betty Ford Institute. Journal of Substance Abuse Treatment, 33(3), 221-228.Journal of Substance Abuse Treatment, 33(3), 221-228.
3737

3838
Definitions of Recovery
RecoveryRecovery refers to the ways in which persons with or affected refers to the ways in which persons with or affected by addiction by addiction tap tap resourcesresources within and beyond the self within and beyond the self to to move beyond experiencing these disorders to move beyond experiencing these disorders to managing themmanaging them and their residual effects to build full, meaningful lives in the and their residual effects to build full, meaningful lives in the community. community.
It is regaining wholeness, connection to the community, It is regaining wholeness, connection to the community, and a purpose-filled life.and a purpose-filled life.
White, W. and Davidson, L. (2006). White, W. and Davidson, L. (2006). Recovery: The bridge to integration? Part one.Recovery: The bridge to integration? Part one. Behavioral Healthcare Behavioral Healthcare..

3939
What is What is youryour definition definition ofof
Recovery ?Recovery ?

4040
Recovery-Oriented Systems of Care: The Paradigm Shift
Recovery-Oriented Systems of Care shift the question
from
“How do we get the client treatment?”
to to
“How do we initiate and support the process of recovery within the person’s life and environment?”

4141
Recovery-Oriented Systems of CareRecovery-Oriented Systems of Care
In this new “In this new “movementmovement” the ” the quality of carequality of care will be will be
concurrently measuredconcurrently measured with the with the recovery achievedrecovery achieved..

4242
Benefits of Moving into a Benefits of Moving into a Recovery-Oriented System of Care Recovery-Oriented System of Care
Most clients undergo Most clients undergo 4 to 5 episodes4 to 5 episodes of care before reaching a stable of care before reaching a stable state of abstinence. state of abstinence. ChronicChronic care approaches care approaches, including self-, including self-management management (Dennis, Scott & Funk, 2003)
Family supports, and integrated services, Family supports, and integrated services, improve recovery improve recovery outcomesoutcomes. . (Lorig & Holman, 2003; Jason et al., 2001; Weisner et al., 2001; Friedmann et al., 2000)
Integrated and collaborative Integrated and collaborative care has been shown to optimize recovery care has been shown to optimize recovery outcomes and outcomes and improve cost-effectivenessimprove cost-effectiveness. . (Smith, Meyers & Miller, 2001; Humphreys & Moos, 2001)
4343
Recovery-Oriented Systems of CareRecovery-Oriented Systems of Care
Support person-centered and self-directed approaches to Support person-centered and self-directed approaches to care that care that build on the build on the strengthsstrengths and and resilienceresilience of of individuals, families, and communities to take responsibility individuals, families, and communities to take responsibility for their sustained health, for their sustained health, wellnesswellness and and recoveryrecovery from from alcohol and drug problems.alcohol and drug problems.
(Center for Substance Abuse Treatment, 2007)(Center for Substance Abuse Treatment, 2007)

Recovery-Oriented Systems of Recovery-Oriented Systems of Care ApproachCare Approach In the recovery-oriented systems of care approach, the In the recovery-oriented systems of care approach, the treatmenttreatment
agency is viewed as agency is viewed as one of many resourcesone of many resources needed for a client’s needed for a client’s successful integration into the community.successful integration into the community.
No one sourceNo one source of support is more dominant than another.of support is more dominant than another.
Various supports need to work in harmony with the Various supports need to work in harmony with the client’s directionclient’s direction, , so that all possible supports are working for and with the person in so that all possible supports are working for and with the person in recovery.recovery.
Northwest Frontier ATTC. (2007).Northwest Frontier ATTC. (2007). Recovery-Oriented Systems of Care - Part 2: Elements of the System.Recovery-Oriented Systems of Care - Part 2: Elements of the System. Addiction Addiction MessengerMessenger, 10(11), Portland, OR: Northwest Frontier ATTC., 10(11), Portland, OR: Northwest Frontier ATTC.
4444

4545
Guiding Principles of RecoveryGuiding Principles of Recovery
Many pathwaysMany pathways
Self-directed & empoweringSelf-directed & empowering
Personal recognition of need Personal recognition of need for changefor change
HolisticHolistic
Cultural dimensionsCultural dimensions
Continuum improved health & Continuum improved health & wellnesswellness
CSAT, Principles of Recovery, 2008CSAT, Principles of Recovery, 2008
Hope & gratitudeHope & gratitude
Healing & self- redefinitionHealing & self- redefinition
Stigma, discrimination, Stigma, discrimination, transcends shametranscends shame
Peers & alliesPeers & allies
ReRejoining & joining & ReRebuilding life in building life in communitycommunity

4646
There are Many Pathways to There are Many Pathways to RecoveryRecovery
Individuals are unique – so is their recoveryIndividuals are unique – so is their recovery
Each person has specific needs, strengths, goals, Each person has specific needs, strengths, goals, attitudes, behaviors and expectationsattitudes, behaviors and expectations
Inpatient, IOP, AA/NA, pharmacological Tx, faith-based, Inpatient, IOP, AA/NA, pharmacological Tx, faith-based, community & family support, no Tx…(community & family support, no Tx…(yes …no yes …no treatmenttreatment ))
4747
Implications of ROSCImplications of ROSC
Care will be provided over a Care will be provided over a continuumcontinuum with the outcome of each with the outcome of each continuous episode over time being measured vs. measuring a level or continuous episode over time being measured vs. measuring a level or unit of care.unit of care.
Care will be provided through Care will be provided through an array of disciplines and an array of disciplines and professionalsprofessionals including new specialties such as interventionists, including new specialties such as interventionists, medical home practitioners, medication assisted recovery specialists, medical home practitioners, medication assisted recovery specialists, and addiction specialists.and addiction specialists.
Recovery will be measuredRecovery will be measured at intervals of at intervals of 90 days90 days, 6 months, 1 year, , 6 months, 1 year, long term (beyond 1 year), and at remission (5 years without long term (beyond 1 year), and at remission (5 years without reoccurrence). reoccurrence).

4848
Recovery Exists on a Continuum of Recovery Exists on a Continuum of Improved Health and WellnessImproved Health and Wellness
Recovery will Recovery will NOT be linearNOT be linear
It is based on It is based on continual growthcontinual growth & improved functioning& improved functioning
May involve May involve “reoccurrence”“reoccurrence” of symptoms in persons with addiction of symptoms in persons with addiction (vs. addicts or consumers)(vs. addicts or consumers)
Wellness is a result of improved care, balance of Wellness is a result of improved care, balance of mind, body & mind, body & spiritspirit..
4949
Recovery is a Process of Recovery is a Process of Healing and Self-RedefinitionHealing and Self-Redefinition
Recovery is a holistic Recovery is a holistic healing processhealing process where a person where a person develops a positive & meaningful self-identitydevelops a positive & meaningful self-identity
Recovery addresses how to transcend Recovery addresses how to transcend stigmastigma and and removes shameremoves shame

5050
Recovery is (Re)Joining and Recovery is (Re)Joining and (Re)Building a Life in the Community(Re)Building a Life in the Community
Process of building or re-building a quality lifeProcess of building or re-building a quality life
Health family, social & personal relationshipsHealth family, social & personal relationships
Obtaining education, employment & housingObtaining education, employment & housing
Becoming a productive member of society (i.e., Becoming a productive member of society (i.e., citizenship)citizenship)

5151
RECOVERY RECOVERY is ais aMeasurableMeasurableREALITYREALITY
It can, will and does happen!It can, will and does happen!
5252
Final ThoughtsFinal Thoughts
There is There is no magicno magic attached to any label, and we would do well to avoid attached to any label, and we would do well to avoid
creating a new vogue in the hopes of an instant solution to a complex creating a new vogue in the hopes of an instant solution to a complex
problem. There is, instead, the necessity that helpers relate not primarily problem. There is, instead, the necessity that helpers relate not primarily
through techniques, but through humanness. And, indeed, ex-addicts through techniques, but through humanness. And, indeed, ex-addicts
have frequently indicated a marked ability to do so. But this is not have frequently indicated a marked ability to do so. But this is not
because they once experienced drug addiction. because they once experienced drug addiction. It is, rather, because It is, rather, because
they completed their own recovery experiences, and emerged as they completed their own recovery experiences, and emerged as
men and women committed to this demanding way of life.men and women committed to this demanding way of life.
Deitch, D. & Casriel, D. (1967). The Role of the Ex-Addict in the Treatment of Addiction. Deitch, D. & Casriel, D. (1967). The Role of the Ex-Addict in the Treatment of Addiction. Federal Probation, 31Federal Probation, 31, 45., 45.

5353
Final Cautionary Thought Final Cautionary Thought
Building a recovery oriented system of care must be done in a way that Building a recovery oriented system of care must be done in a way that
avoids the “us and themavoids the “us and them” polarizations” polarizations between peer and between peer and
professional modelsprofessional models. The issue is not, “who is more valuable: a . The issue is not, “who is more valuable: a
doctor or a friend?” The issue is what individuals and families need at a doctor or a friend?” The issue is what individuals and families need at a
particular moment in time. It is not a question of one or the other. It is a particular moment in time. It is not a question of one or the other. It is a
community where both are available as needed.community where both are available as needed.
5454
What is the Unifying What is the Unifying Vision?Vision?
Treatment should provide the right care, at the right time, by Treatment should provide the right care, at the right time, by the right provider with the right resources every time – no the right provider with the right resources every time – no more, no less.more, no less.
All care provided should offer the best opportunity for All care provided should offer the best opportunity for recovery – each and every time.recovery – each and every time.

5555
ResourcesResources http://www.ireta.org/ – search recovery – search recovery
http://www.attcnetwork.org/ – search ROSC – search ROSC
William White, Chestnut Health SystemsWilliam White, Chestnut Health Systems
http://www.samhsa.gov/
http://www.csat.samhsa.gov/
http://www.niaaa.nih.gov/
[email protected] or 412-391-4449 or 412-391-4449
Thank you !!Thank you !!
June Gertig, J.D.June Gertig, J.D.
Altarum Institute Altarum Institute
and and
Michael T. Flaherty, Ph.D.Michael T. Flaherty, Ph.D.
Institute for research, Education and Institute for research, Education and
Training in the Addictions, Training in the Addictions,
Northeast ATTC Northeast ATTC
5656
5757
ReferencesReferencesCenter for Substance Abuse Treatment. (2006). National Summit on Recovery: Conference Report. DHHS Center for Substance Abuse Treatment. (2006). National Summit on Recovery: Conference Report. DHHS
Publication No. (SMA) 06-xxxx. Rockville, MD: Substance Abuse and mental Health Services Publication No. (SMA) 06-xxxx. Rockville, MD: Substance Abuse and mental Health Services Administration. Administration.
Clark, W. (2008). Tools for System Improvement in a Recovery-Oriented System of Care. Presentation at Clark, W. (2008). Tools for System Improvement in a Recovery-Oriented System of Care. Presentation at the 2008 SAAS Conference and NIATx Summit, Orlando, FL, June 22.the 2008 SAAS Conference and NIATx Summit, Orlando, FL, June 22.
Dennis, M. L., Scott, C. K., & Funk, R. (2003). An experimental evaluation of recovery management Dennis, M. L., Scott, C. K., & Funk, R. (2003). An experimental evaluation of recovery management checkups (RMC) for people with chronic substance use disorders. checkups (RMC) for people with chronic substance use disorders. Evaluation and Program PlanningEvaluation and Program Planning, , 26(3), 339-352.26(3), 339-352.
Dennis, M. L., Scott, C. K., & Hristova, L. (2002). The duration and correlates of substance abuse Dennis, M. L., Scott, C. K., & Hristova, L. (2002). The duration and correlates of substance abuse treatment careers among people entering publicly funded treatment in Chicago [Abstract], treatment careers among people entering publicly funded treatment in Chicago [Abstract], Drug and Drug and Alcohol Dependence, 66 Alcohol Dependence, 66 (Suppl. 2), 44.(Suppl. 2), 44.
Flaherty, M. (2006). Flaherty, M. (2006). A Unified Vision for the Prevention and Management of Substance Use Disorders: A Unified Vision for the Prevention and Management of Substance Use Disorders: Building Resiliency, Wellness and Recovery – A Shift from an Acute Care to a Sustained Care Recovery Building Resiliency, Wellness and Recovery – A Shift from an Acute Care to a Sustained Care Recovery Management Model.Management Model. Pittsburgh, PA: IRETA. Pittsburgh, PA: IRETA.
Humphreys, K., Moos, R. J., & Cohen, C. (1997). Social and community resources and long-term recovery Humphreys, K., Moos, R. J., & Cohen, C. (1997). Social and community resources and long-term recovery from treated and untreated alcoholism. from treated and untreated alcoholism. Journal of Studies on AlcoholJournal of Studies on Alcohol, , 5858(3), 231-238.(3), 231-238.
Jason, L., Davis, M., Ferrari, J., & Bishop, P. (2001). Oxford House: A review of research and implications Jason, L., Davis, M., Ferrari, J., & Bishop, P. (2001). Oxford House: A review of research and implications for substance abuse recovery and community research. for substance abuse recovery and community research. Journal of Drug Education,Journal of Drug Education, 3131(1), 1-27(1), 1-27
McLellan, A.T. (2002). Have we evaluated addiction treatment correctly? Implications from a chronic care McLellan, A.T. (2002). Have we evaluated addiction treatment correctly? Implications from a chronic care perspective. perspective. AddictionAddiction, 97, 249-252., 97, 249-252.

ReferencesReferencesMcLellan, A.T., Lewis, D. C., O’Brien, C. P., & Kleber, H. D. (2000). Drug dependence, a chronic McLellan, A.T., Lewis, D. C., O’Brien, C. P., & Kleber, H. D. (2000). Drug dependence, a chronic
medical illness: Implications for treatment, insurance, and outcomes evaluation. medical illness: Implications for treatment, insurance, and outcomes evaluation. Journal of the Journal of the American Medical AssociationAmerican Medical Association 284284(13), 1689-1695.(13), 1689-1695.
Moos, R. & Moos, B. (2005). Paths of entry into Alcoholics Anonymous: Consequences for Moos, R. & Moos, B. (2005). Paths of entry into Alcoholics Anonymous: Consequences for participation and remission. participation and remission. Alcoholism: Clinical & Experimental ResearchAlcoholism: Clinical & Experimental Research. . 2929(10), 1858-1868.(10), 1858-1868.
National Center on Addiction and Substance Abuse at Columbia University (CASA). (2009). National Center on Addiction and Substance Abuse at Columbia University (CASA). (2009). Shoveling Up II: The Impact of Substance Abuse on Federal, State and Local BudgetsShoveling Up II: The Impact of Substance Abuse on Federal, State and Local Budgets . New York: . New York: CASA.CASA.
Scott, C.K., Dennis, M.L., & Foss, M.A. (2005). Utilizing recovery management checkups to shorten Scott, C.K., Dennis, M.L., & Foss, M.A. (2005). Utilizing recovery management checkups to shorten the cycle of relapse, treatment re-entry, and recovery. the cycle of relapse, treatment re-entry, and recovery. Drug and Alcohol Dependence, 78Drug and Alcohol Dependence, 78(3), 325-(3), 325-338. 338.
Substance Abuse and Mental Health Services Administration (SAMHSA). (2008). Substance Abuse and Mental Health Services Administration (SAMHSA). (2008). Results from the Results from the 2007 National Survey on Drug Use and Health: National Findings 2007 National Survey on Drug Use and Health: National Findings (Office of Applied Studies, (Office of Applied Studies, NSDUH Series H-34, DHHS Publication No. SMA 08-4343). Rockville, MD.NSDUH Series H-34, DHHS Publication No. SMA 08-4343). Rockville, MD.
Weisner, C., Mertens, J., Parthasaratht, S., Moore, C., & Lu, Y. (2001). Integrating primary medical Weisner, C., Mertens, J., Parthasaratht, S., Moore, C., & Lu, Y. (2001). Integrating primary medical care with addiction treatment: A randomized controlled trial. care with addiction treatment: A randomized controlled trial. Journal of the American Medical Journal of the American Medical Association, 286Association, 286, 1715-1723., 1715-1723.
White, W. (2008). White, W. (2008). Recovery management and recovery-oriented systems of care: Scientific rationale Recovery management and recovery-oriented systems of care: Scientific rationale and promising practicesand promising practices. Pittsburgh, PA: Institute for Research, Education and Training in . Pittsburgh, PA: Institute for Research, Education and Training in Addictions.Addictions.
5858







