
Investor science conference call ASH 2009 New Orleans, 8 December 2009

2
Forward-looking statements
This presentation contains certain forward-looking statements. These forward-looking statements may be identified by words such as ‘believes’, ‘expects’, ‘anticipates’, ‘projects’, ‘intends’, ‘should’, ‘seeks’, ‘estimates’, ‘future’ or similarexpressions or by discussion of, among other things, strategy, goals, plans or intentions. Various factors may cause actual results to differ materially in the future from those reflected in forward-looking statements contained in this presentation, among others:1 pricing and product initiatives of competitors;2 legislative and regulatory developments and economic conditions;3 delay or inability in obtaining regulatory approvals or bringing products to market; 4 fluctuations in currency exchange rates and general financial market conditions; 5 uncertainties in the discovery, development or marketing of new products or new uses of existing products, including
without limitation negative results of clinical trials or research projects, unexpected side-effects of pipeline or marketed products;
6 increased government pricing pressures; 7 interruptions in production; 8 loss of or inability to obtain adequate protection for intellectual property rights; 9 litigation;10 loss of key executives or other employees; and11 adverse publicity and news coverage.
Any statements regarding earnings per share growth is not a profit forecast and should not be interpreted to mean that Roche’s earnings or earnings per share for this year or any subsequent period will necessarily match or exceed the historical published earnings or earnings per share of Roche.
Please see www.roche.com for full information on Roche products mentioned.

Introduction
Dr. Karl Mahler, Head of Investor Relations
4
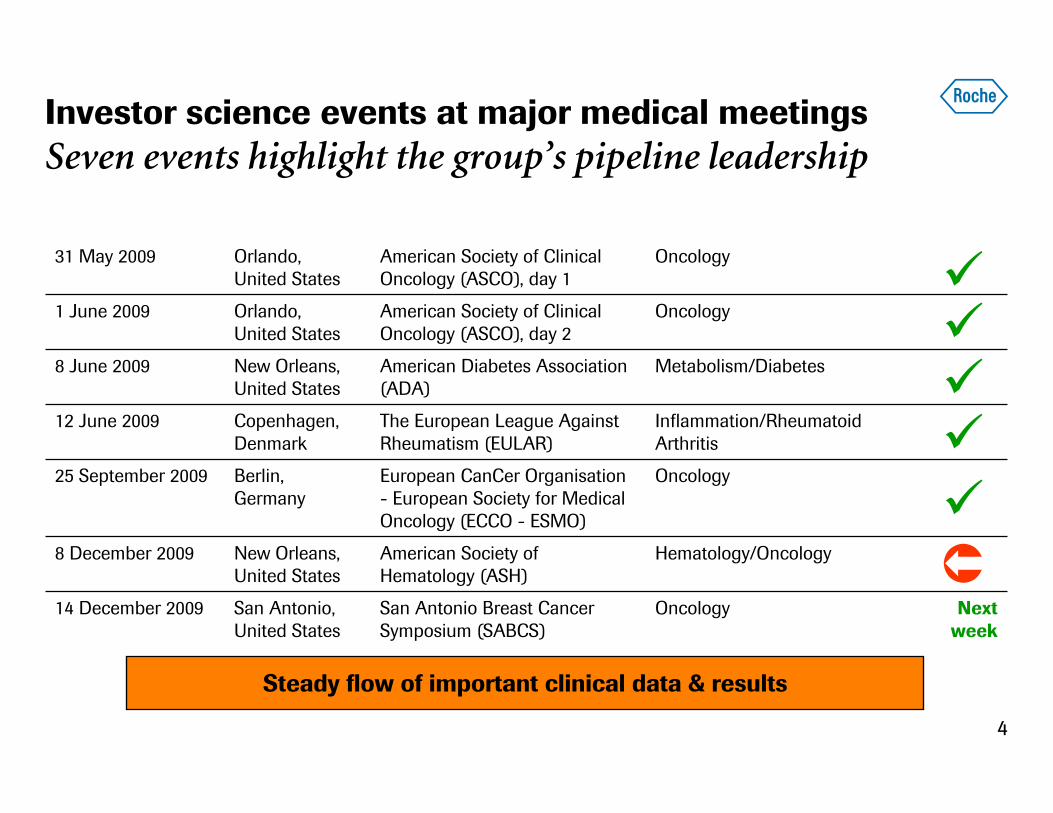
Investor science events at major medical meetingsSeven events highlight the group’s pipeline leadership
Next week
OncologySan Antonio Breast Cancer Symposium (SABCS)
San Antonio, United States
14 December 2009
Hematology/OncologyAmerican Society of Hematology (ASH)
New Orleans, United States
8 December 2009
Berlin, Germany
Copenhagen, Denmark
New Orleans, United States
Orlando,United States
Orlando, United States
OncologyAmerican Society of Clinical Oncology (ASCO), day 2
1 June 2009
OncologyEuropean CanCer Organisation - European Society for Medical Oncology (ECCO - ESMO)
25 September 2009
Inflammation/Rheumatoid Arthritis
The European League Against Rheumatism (EULAR)
12 June 2009
Metabolism/DiabetesAmerican Diabetes Association (ADA)
8 June 2009
OncologyAmerican Society of Clinical Oncology (ASCO), day 1
31 May 2009
Steady flow of important clinical data & results

5
AgendaLeader in hematology
• Hematology pipeline overview– Dr. Sandra Horning, Sr. VP, Global Head, Clinical Development
Hematology/Oncology
• Important clinical data at ASH 2009– Dr. Nancy Valente, Sr. Group Director, Clinical Development
Hematology/Oncology
• Leader in hematology — commercial overview & opportunities– Dr. Myriam Mendila, Hematology Franchise Leader
• Questions & AnswersTotal duration: Up to 1½ hour
Dr. Sandra Horning, Sr. VP, Global Head, Clinical Development Hematology/Oncology
Hematology pipeline overview

7
Pipeline overview
Pipeline highlights

8
Hematology development strategy
• Our goal
– To use our science to continue developing a number of therapeutics like MabThera/Rituxan that significantly improve the lives of people with hematological malignancies
• Targeting the right drug to the right patient
– Identify the best drugs for patients based on the biologic characteristics of the tumor and the individual
– Integrate diagnostics and therapeutics to deliver personalised healthcare

9
Phase IIIPhase Ib/IIPhase I
RG3636/SGN-40(dace-tuzumab)3 Anti-CD40 DLBCL, iNHL, MM
RG3639(dulanermin)2
DR4/DR5 agonist iNHL
RG7425DR5 agonist iNHL
RG7433/ABT-2631
BH3 mimetic CLL, lymphoid malignancies
The clinical pipeline in hematology:Translating science to patient benefit
RG7159/GA101Next-gen anti-CD20 CLL, iNHL Moving to Phase III
DLBCL=Diffuse Large B-Cell Lymphoma, MM=Multiple Myeloma, iNHL=indolent Non-Hodgkin’s Lymphoma1In partnership w/Abbott 2In partnership w/Amgen 3In partnership w/Seattle Genetics
RG7422/GDC-0980PI3 kinase inhibitor NHL
AvastinAnti-angiogenic DLBCL, MM (phase II)
RG7112MDM2 antagonist Hematological tumorsN
N
N
N
O Cl
ClO
SO
O

10
Multiple hallmarks of hematological malignancies
RG7159/GA101 (Next-gen anti-CD20)
RG7425 (DR5 agonist)
RG3639(dulanermin)2 (DR4/DR5 agonist)
RG3636/SGN-40(dacetuzumab)3 (Anti-CD40)
RG7422/GDC-0980 (PI3 kinase inhibitor)
RG7112 (MDM2 antagonist)
Evading apoptosis
RG7433/ABT-2631 (BH3 mimetic)
The clinical pipeline in hematology:Targeting the underlying biology
Hanahan & Weinberg, The Hallmarks of Cancer, Cell, vol 100, pp 57-70, copyright Elsevier (2000)1In partnership w/Abbott 2In partnership w/Amgen 3In partnership w/Seattle Genetics
Sustained angiogenesis
Avastin(bevacizumab)

11
Pipeline overview
Pipeline highlights

12
RG7159/GA101 (Next-gen anti-CD20):First glyco-engineered type II CD20 mAb
• Increased direct cell-death induction– Unique type II epitope and elbow-
hinge modification
• Enhanced antibody-dependentcell-mediated cytotoxicity (ADCC)– Increased affinity to the ‘ADCC
receptor’ FcgRIIIA
• Lower complement-dependent cytotoxicity (CDC) activity– Due to recognition of type II epitope
Umaña et al, Blood 2006; 108, abstract 229, Umaña et al, Ann Oncology 2008, 19 (suppl 4), abstract 098
CD20 peptide
Type II recognition & elbow-hinge
residues
Carbohydrateglycoengineered
(GlycoMabTM
technology)

13
B-cell depletion whole-blood assay in B-CLL patients (24 h)
CD
19+
Dep
leti
on (
%) 100
60
40
0
0
20
20 200 2000 20,000
80 GA101
Rituximab
Ab conc. (ng/mL) Time after cell transplantation (days)
n=10
Tum
or v
olum
e (m
m3 )
med
ian ±
IQR
Vehicle Rituximab30 mg/kg
GA10130 mg/kg
Rituximab1st line
2500
22 25 28 31 34 37 40 43 46 49 52 55 58 61
2000
1500
1000
500
0
SU-DHL-4NHL xenograft in mice pretreated with MabThera/Rituxan(rituximab)
Non-ADCC competent s.c. xenograft model (SCID beige)
RG7159/GA101 (Next-gen anti-CD20):Rapid B-cell depletion and superior tumor remissions in preclinical models

14
RG7433/ABT-2631 (BH3 mimetic):Acts as a BH3 mimetic to induce apoptosis
1In partnership w/Abbott
Bcl-xL
Apoptosis
Bim BidPuma
BikBmf
BadNoxaHrk
Bak
Bax
Caspase activation
activated
BAX / BAK
Mitochondria
Cyt CBcl-2
DNA damaging
agents
Anti-mitotics
Rituxan
TDM-1
Tarceva
GA101
Other ADC
PI3K
PI3K/mTOR
AKTMEK
Cytotoxic Chemo
Antibody-drug conjugates
Anti-CD20
EGFR targeted agents
Erbitux
ABT-263
• BCL-2 is a target for tumor biology driven over-expression in lymphoid cancers and SCLC
• BCL-2 is a target for tumor biology driven over-expression in lymphoid cancers and SCLC

15
RG7433/ABT-2631 (BH3 mimetic):Acts as a BH3 mimetic to induce apoptosis
1In partnership w/Abbott
Bcl-xL
Apoptosis
Bak
Bax
Caspase activation
activated
BAX / BAK
Mitochondria
Cyt C
Bcl-2
ABT-263
• Strongly inhibits Bcl-xL, Bcl-2
• Oral bioavailability
• Flexible dosing

16
Technology: Antibody drug conjugatesProof-of-concept in hematology; phase II in mBC HER2+
The premiseCytotoxic
Chemical linker
Antibody
Target cell
Antibody-drug conjugate (ADC)
Antibody/target Linker Drug
Expression on tumor butnot on vital tissue
Stable in circulationReleased in tumor
Highly potentNon-immunogenic
gRED=Genentech Research & Early Development, NHL=Non-Hodgkin’s Lymphoma, CLL=Chronic Lymphocytic Leukemia, MM=Multiple Myeloma
Advantages
• Greater tumor kill
• Normal tissue sparing
Preclinical gRED pipeline
• New NHL, CLL, MM targets
Proof of concept (POC)/clinical development
• ASH 2009: ADC in Hodgkin’s lymphoma
• SABCS 2009: RG3502/T-DM1(trastuzumab DM1): New phase II data in mBC 3rd line HER2+

Dr. Nancy Valente, Sr. Group Director, Clinical Development
Important clinical data at ASH 2009

18
ASH 2009: Selected clinical highlightsMabThera/Rituxan consolidating its position in CLL; early-mid stage pipeline moving ahead
• MabThera/Rituxan– New data from the phase III study CLL-8 (ASH 2008) are the first to show that a
specific first-line treatment for CLL results in an improved overall survival– New data with chemotherapies other than those used in the CLL-8 study (FC) show
encouraging efficacy and acceptable safety for patients with untreated CLL
• RG7159/GA101– New findings from the first phase I/II study GAUGUIN (BO20999, ASH 2008)
demonstrate safety and efficacy in the CLL cohort – New data from the second phase I/II study GAUSS (BO21003) show promising
efficacy in heavily-pretreated patients with B-cell hematological malignancies
• RG7433/ABT-2631
– New data from ongoing phase I study in relapsed or refractory CLL show encouraging single-agent activity and acceptable safety
1In partnership w/Abbott
19
MabThera/Rituxan
RG7159/GA101
RG7433/ABT-263

20
CLL8 Study Design
Patients with untreated, active
CLL and good physical
fitness(CIRS ≤ 6, creatinine
clearance ≥ 70 ml/min)
R
FCR
FC
6 courses
Follow up
C1 C2 C3 C4 C5 C6
Updated results of the 2nd analysis at a median observation time of 37.7 months.
ASH 2009, abstract 535, Hallek et al.

21
Patients: ITT population (n=817) of the CLL8 protocol
FC (n = 409) FCR (n = 408)Female 105 (26%) 105 (26%)
Male 304 (74%) 303 (74%)
Median age 61 (range 36-81) 61 (range 30-80)
Binet A 22 (5.4%) 18 (4.4%)
Binet B 259 (63.6%) 263 (64.6%)
Binet C 126 (31%) 126 (31%)
B symptoms* 197 (48%) 167 (41%)
Median cumulative illness rating scale (CIRS) 1 (range 0-8) 1 (range 0-7)
Trisomy 12 14.4% 9.6%
Del(13q) 59.7% 53.8%
Del(11q23) 22.5% 26.8%
Del(17p13) 9.5% 7.0%
*P<0,05

22
Adverse events CTC grade 3 and 4
FC FCR pTotal number of patients with≥ 1 grade 3/4 event
248 (62.9%) 309 (76.5%) < 0.0001
Hematological toxicity 39.6% 55.7 % < 0.0001
Neutropenia 21.0% 33.7% < 0.0001
Leukocytopenia 12.1% 24.0% < 0.0001
Thrombocytopenia 11.1% 7.4% 0.07
Anemia 6.8% 5.4% 0.42
Infection 21.5% 25.5% 0.18
Tumor lysis syndrome 0.5% 0.2% 0.55
Cytokine release syndrome 0.0% 0.2% 0.32
ASH 2009, abstract 535, Hallek et al.
Treatment related mortality 2% for both arms.

23
Best response to treatment
FC FCR
CR* 21.8% 44.1%PR 66.6% 51.0%
Overall response rate 88.4% 95.1%
All includedin PR
**CRu 4.6% 3.6%**CRi 1.9% 2.3%nPR 5.7% 3.4%
SD 7.8% 3.9%PD 3.8% 1.0%
*According NCI WG Criteria, confirmatory BM assessment performed up to 6 months after final restagingP < 0.01ASH 2009, abstract 535, Hallek et al.

24
Progression free survival: FCR versus FC
ASH 2009, abstract 535, Hallek et al.
Median PFS: 32.3 months for FC vs 42.8 months for FCR
ASH 2008
p=0.000007
Median PFS: 32.8 months for FC vs 51.8 months for FCR, n=790, HR 0.563, ranges 0.460-0.689PFS rate 3 yrs post randomization: FC: 44.7%, FCR: 64.9%
p<0.001
ASH 2009

25
Overall survival
Overall survival 3 years post randomization:FCR: 87.2%FC: 82.5%
n=817, HR 0.664, p=0.012
ASH 2009, abstract 535, Hallek et al.

26
Summary: FCR improves outcome
• The addition of rituximab to FC first line therapy improves theoutcome of patients with advanced, symptomatic CLL withregard to
– Response rates (CR, ORR, MRD)
– Progression-free survival
– Overall survival
• Acheiving a CR produces a longer survival
• First randomized trial to demonstrate that the choice of firstline therapy improves the natural course of CLL.
ASH 2009, abstract 535, Hallek et al.
27
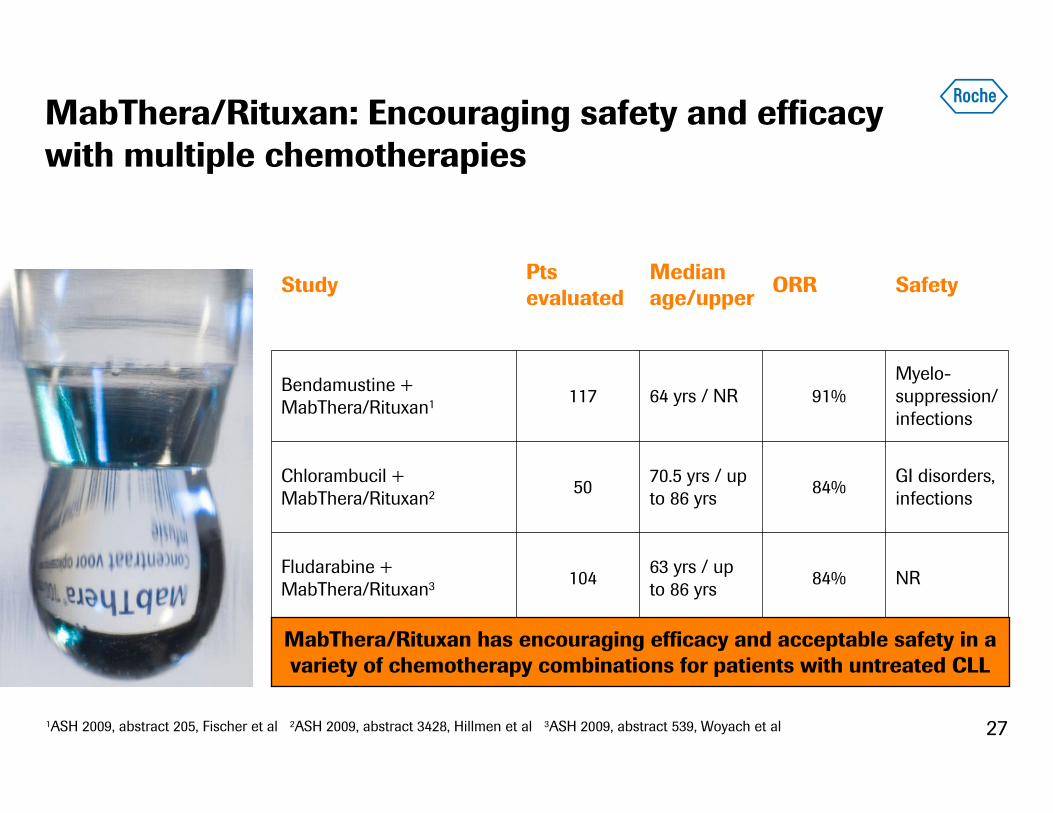
MabThera/Rituxan: Encouraging safety and efficacy with multiple chemotherapies
Myelo-suppression/ infections
91%64 yrs / NR117Bendamustine + MabThera/Rituxan1
NR84%63 yrs / up to 86 yrs
104Fludarabine + MabThera/Rituxan3
GI disorders, infections
84%70.5 yrs / up to 86 yrs
50Chlorambucil + MabThera/Rituxan2
SafetyORRMedian age/upper
PtsevaluatedStudy
MabThera/Rituxan has encouraging efficacy and acceptable safety in a variety of chemotherapy combinations for patients with untreated CLL
1ASH 2009, abstract 205, Fischer et al 2ASH 2009, abstract 3428, Hillmen et al 3ASH 2009, abstract 539, Woyach et al

28
MabThera/Rituxan
RG7159/GA101
RG7433/ABT-263

29
RG7159/GA101 (Next-gen anti-CD20) GAUGUIN study:Phase I dose-escalation (3+3 design)
• CD20+ CLL for whom “no therapy of higher priority was available”
• n = 3 per cohort– Successive cohorts initiated
if no DLT
• Enrolment from July to November 2008 at 7 sites in France
Cohort group
GA101 doseDose 1/Doses 2–9
1 400/800 mg
2 800/1200 mg
31 1200/2000 mg
4 1000/1000 mg
3 6 9 12 15 18 21 weeks
Tumor assessment
25
GA101 single agent (total 9 doses)
1 33
GA101 administered as per rituximab administration guidelines; 14 patients enrolled in cohort at 1200/2000 mg dose levelASH 2009, abstract 884, Morschhauser et al
30
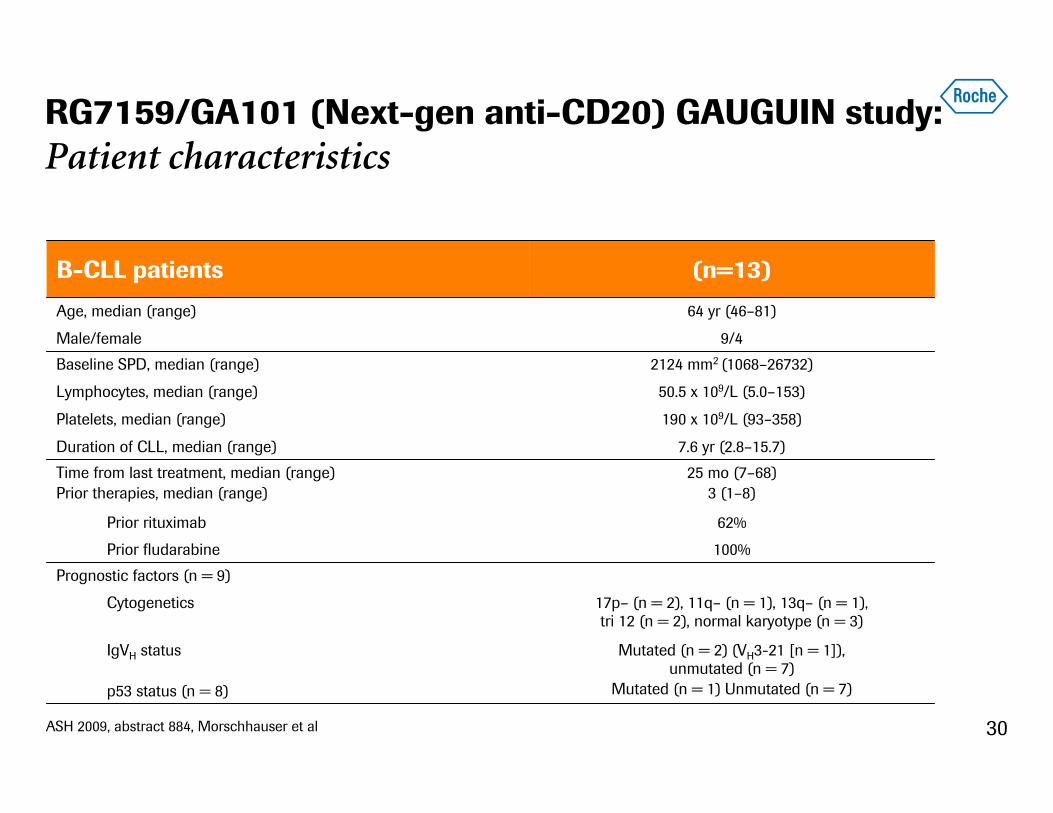
RG7159/GA101 (Next-gen anti-CD20) GAUGUIN study:Patient characteristics
ASH 2009, abstract 884, Morschhauser et al
2124 mm2 (1068–26732)Baseline SPD, median (range)
50.5 x 109/L (5.0–153)Lymphocytes, median (range)
190 x 109/L (93–358)Platelets, median (range)
B-CLL patients (n=13)
Age, median (range) 64 yr (46–81)
Male/female 9/4
Duration of CLL, median (range) 7.6 yr (2.8–15.7)
Time from last treatment, median (range)Prior therapies, median (range)
25 mo (7–68)3 (1–8)
Prior rituximab 62%
Prior fludarabine 100%
Prognostic factors (n = 9)
Cytogenetics 17p– (n = 2), 11q– (n = 1), 13q– (n = 1),tri 12 (n = 2), normal karyotype (n = 3)
IgVH status
p53 status (n = 8)
Mutated (n = 2) (VH3-21 [n = 1]),unmutated (n = 7)
Mutated (n = 1) Unmutated (n = 7)
31
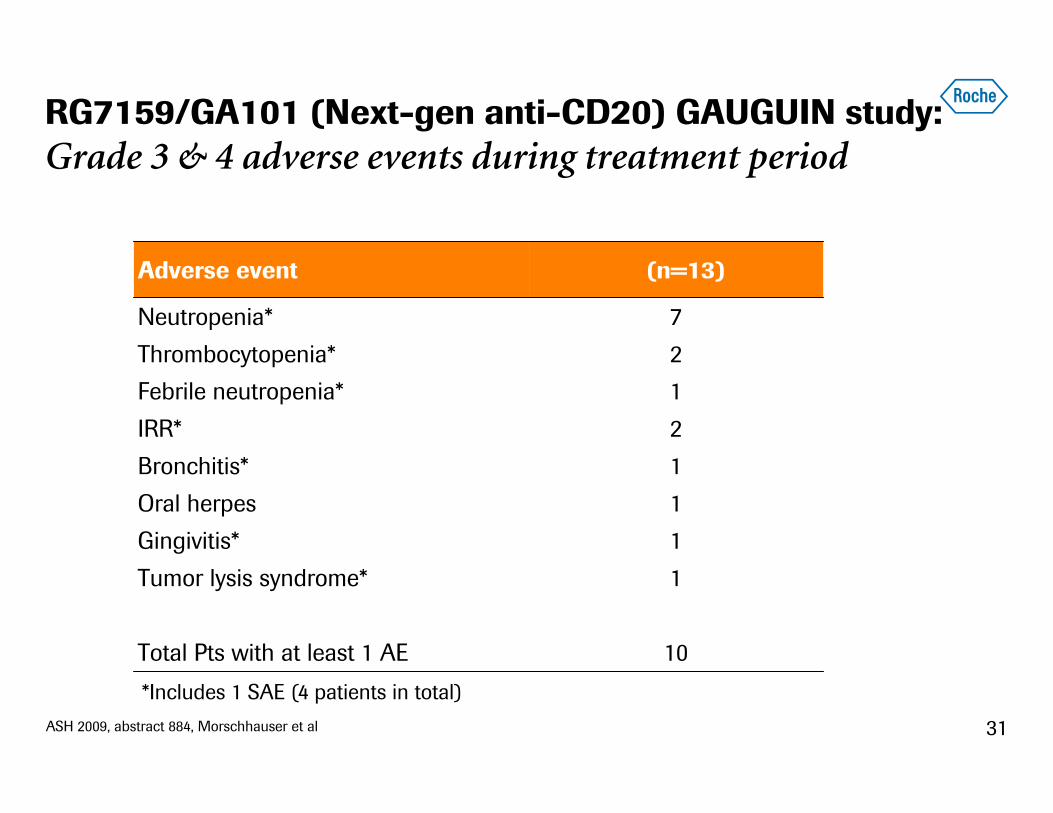
RG7159/GA101 (Next-gen anti-CD20) GAUGUIN study:Grade 3 & 4 adverse events during treatment period
ASH 2009, abstract 884, Morschhauser et al
2IRR*
1Bronchitis*
1Oral herpes
1Gingivitis*
1Tumor lysis syndrome*
10Total Pts with at least 1 AE
Adverse event (n=13)
Neutropenia* 7
Thrombocytopenia* 2
Febrile neutropenia* 1
*Includes 1 SAE (4 patients in total)

32
RG7159/GA101 (Next-gen anti-CD20) GAUGUIN study:Grade 3 & 4 neutropenia
• 12 CTC Grade 3 & 4 neutropenic episodes in 9 patients
• During treatment, 8 transient neutropenic episodes
– 3 occurred during Cycle 1
– 1 patient experienced febrile neutropenia
– All patients completed treatment phase, receiving all 9 scheduled infusions
– No dose reductions
• 4 episodes after treatment
• Median duration: 10 days (range 1–28); 7 patients received G-CSF
• No clear dose relationship
ASH 2009, abstract 884, Morschhauser et al

33
RG7159/GA101 (Next-gen anti-CD20) GAUGUIN study:Best overall response 62%1
Cohort CR PR SD PD
400/800 mg x x x
800/1200mg x x x
1200/2000 mg x x x x
1000/1000 mg x x x
Total (n=13) 1 7 5 0
• Median duration of response 8+ months [range 2.2-10.4 months]
• 6 responding patients currently ongoing [1 CR, 5 PR], 2 patients SD in follow-up; 5 patients PD
ASH 2009, abstract 884, Morschhauser et al1Response assessment based on revised CLL criteria, Hallek et al, Blood 2008; 111:5446–5456

34
RG7159/GA101 (Next-gen anti-CD20) GAUGUIN study: All 13 patients achieve tumour shrinkage1
-100
-80
-60
-40
-20
0
Tum
or b
urde
n de
crea
se (
%)
Patients (n=13)
ASH 2009, abstract 884, Morschhauser et al1Response assessment based on revised CLL criteria, Hallek et al, Blood 2008; 111:5446–5456

35
RG7159/GA101 (Next-gen anti-CD20) GAUGUIN study:Conclusions
• Safety profile
– GA101 is well tolerated in CLL with no DLTs
– Similar to GA101 phase I safety profile in NHL except neutropenia
– Higher rate of reversible grade 3 & 4 neutropenia in CLL
• Very encouraging efficacy observed as single agent in relapsed/ refractory CLL
– ORR: 62% (8/13)
– Rapid and sustained hematologic response in all patients (including two patients with 17p–)
– All patients demonstrate reduction in lymph nodes
ASH 2009, abstract 884, Morschhauser et al

36
• CD20+ malignant disease for which ‘no therapy of higher priority was available’
• N = 3 per cohort– Successive cohorts initiated if no DLT
• Enrolment from January 2008 to January 2009 at 5 sites in Canada
GA101 administered as per Rituximab administration guidelines
2 3 4 weeks
Response assessment
13
GA101 single-agent (total 4 doses)
1
RG7159/GA101 (Next-gen anti-CD20) GAUSS study:Phase I dose escalation (3+3 design), induction dosing
ASH 2009, abstract 934, Sehn et al
1000 / 1000 mg61200 / 2000 mg5
Cohort group
GA101 doseDose 1/doses 2–4
1 100 / 200 mg2 200 / 400 mg3 400 / 800 mg4 800 / 1200 mg

37
RG7159/GA101 (Next-gen anti-CD20) GAUSS study:Patient demographics and disease characteristics
ASH 2009, abstract 934, Sehn et al
1High-Risk (III and IV)4Intermediate (I and II)
Rai StageCLL Patients (n=5)
4 (40)High risk: 3-5 risk factors3 (30)Intermediate risk: 2 risk factors3 (30)Low risk: 0-1 risk factor
Follicular lymphoma prognostic index (n=10)15 (89)III / IV2 (11)I / II
Clinical Stage (Ann Arbor)NHL Patients (n=17)
Characteristic (n=22) No. of patients (%)Median age [range] 60 [47-77]Male / female 13 / 9Histological subtype (n=22)
Diffuse large B-Cell lymphoma 3 (14)Other aggressive pathologies (MCL + transformed MZL) 2 (9)Follicular lymphoma 10 (45)Small lymphocytic lymphoma 2 (9)Chronic lymphocytic leukaemia 5 (23)

38
RG7159/GA101 (Next-gen anti-CD20) GAUSS study:Prior treatment regimens and response
Chronic Lymphocytic Leukemia (n=5)
Non-Hodgkin’s Lymphoma (n=17)
Variable No of patients (%)
No. of prior therapies, median (range) 4 (1–7)
Types of previous therapy
Percentage receiving prior rituximab-containing regimens (n=22) 19 (86)
No. of prior rituximab-containing regimens, median (range) 2 (1-4)
No. of rituximab-refractory patients (n=22) 11 (50)
NHL patients with prior anthracycline 11 (65)
NHL patients with prior ASCT 3 (18)
CLL patients refractory to fludarabine 5 (100)
ASH 2009, abstract 934, Sehn et al

39
RG7159/GA101 (Next-gen anti-CD20) GAUSS study:Most common adverse events by severity during induction
Adverse event (AE)
No. of patients (%)
Induction (n=22)
All grades Grade 3 & 4
Non-hematologic AEs
Infusion-related reactions 16 (73) 4
Infections 6 (27) -
Headache 4 (18) 1
Nausea 4 (18) -
Pyrexia 4 (18) -
Diarrhea 3 (14) -
Fatigue 3 (14) -
Hematologic AEs
Neutropenia 4 (18) 4
Febrile neutropenia 1 (5) 1
Thrombocytopenia 1 (5) 1
ASH 2009, abstract 934, Sehn et al

40
RG7159/GA101 (Next-gen anti-CD20) GAUSS study:Overall response following induction, by dose, 13 wks
Dose No. of patients CR PR SD PD Non evaluable
100/200 mg 3 1 2
200/400 mg 3 2 1
400/800 mg 3 2 1
800/1200 mg 3 3
1200/2000 mg 3 3
1000/1000 mg 7 4 2 1
Total 22 5 13 3 1
Percent 24% 62% 14%
ASH 2009, abstract 934, Sehn et al

41
RG7159/GA101 (Next-gen anti-CD20) GAUSS study:Overall response following induction, by histology, 13 wks
1113 Diffuse large B-Cell lymphoma
112Other aggressive histologies (MCL + transformed MZL)
17210 Follicular lymphoma
112Small lymphocytic lymphoma
145Chronic lymphocytic leukemia
Histology No. of patients CR PR SD PD Non
evaluable
ASH 2009, abstract 934, Sehn et al

42
Dose Cohort (mg) Diagnosis
End of induction response
Duration of GA-101 treatment to date Best Response
Progression (Y/N)
100/ 200 MZL PR 9 months PR Y
200/ 400 DLBCL PR 4 month PR Y
FL SD 17 months PR* N
FL PR 17 months PR N
400/ 800 SLL PR 14 months PR N
FL PR 17 months PR N
1200/ 2000 CLL SD 3 months SD Y
FL SD 9 months SD N
RG7159/GA101 (Next-gen anti-CD20) GAUSS study: Treatment response in patients receiving extended therapy
ASH 2009, abstract 934, Sehn et al

43
RG7159/GA101 (Next-gen anti-CD20) GAUSS study:Conclusions
• GA101 safety profile
– Well tolerated
– No dose-limiting toxicities
– Infusion reactions primarily limited to first cycle
– Safety profile similar to that of rituximab
• Efficacy observed in highly pre-treated patients
– Phase II study now going head to head in indolent lymphoma
• Extended therapy is safe and may improve efficacy
ASH 2009, abstract 934, Sehn et al

44
RG7159/GA101 (Next-gen anti-CD20) GAUSS study:Study being expanded by large phase II cohort in iNHL
First head to head trial against rituximab monotherapy
Relapsed CD20+
indolent NHL (N=180)
GA101
1000 mg
Weekly x 4
Rituximab375mg/m2
Weekly x 4
CR PR SD
GA101 extended treatment (1000mg
once every 2 months, up to 2 years)
Rituximab extended treatment (375 mg/m2 once
every 2 months, up to 2 years)
Randomization
ASH 2009, abstract 934, Sehn et al

45
RG7159/GA101 (Next-gen anti-CD20):Clinical development; beyond MabThera/Rituxan
Phase I/II studies
– BO21000 iNHL, n=56, RG7159/GA101 + FC or RG7159/GA101 + CHOP
– GUIGUIN (BO20999) aNHL, iNHL as well as CLL cohort, total n=133
– GAUSS (BO21003) iNHL, total n= approx 200
– Data flow to continue at upcoming medical meetings
Phase III program (initial studies only)
– GAO4753g iNHL refractory (n=360)• Bendamustine +/- RG7159/GA101• FPI Q2 2010; filing expected post 2012
– BO21004 CLL 1st line (n=780)• Chlorambucil +/- RG7159/GA101 or chlorambucil + MabThera/Rituxan• FPI Q4 2009; filing expected 2012
RG7159/GA101: Extensive clinical program well underway

46
MabThera/Rituxan
RG7159/GA101
RG7433/ABT-263

47
n = 3250 mg n = 3200 mgn = 6110 mgn = 310 mg
Dose levels
RG7433/ABT-2631: Phase I in relapsed/refractory CLLM06-873 study design
Screening 14d on/7d off
15 Patients
Safety
PK
MTD
21d on / 0d offSafety
PK
MTD14 Patients
Intermittent
Continuous with lead in
Screening
7d 100mg
ASH 2009, abstract 883, Roberts et al1In partnership w/Abbott
n = 4300 mg n = 3250 mgn = 4200 mgn = 3125 mg
Dose levels
48
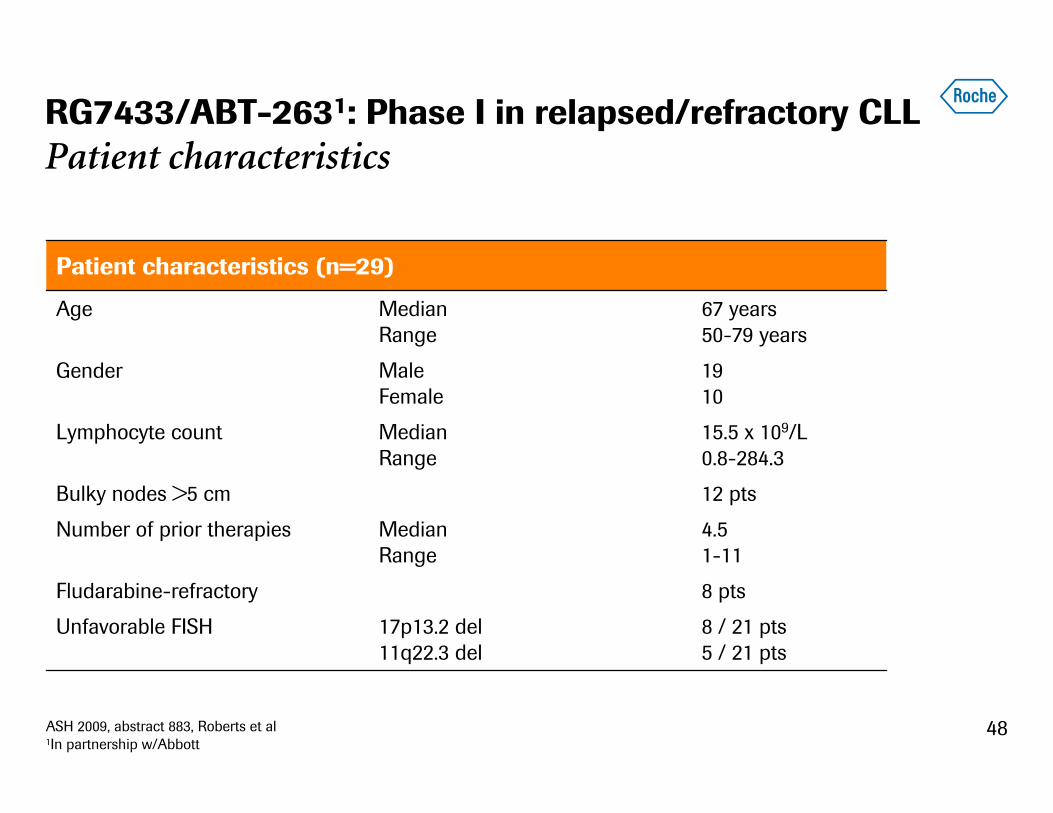
RG7433/ABT-2631: Phase I in relapsed/refractory CLLPatient characteristics
17p13.2 del11q22.3 del
MedianRange
MedianRange
Male Female
MedianRange
8 / 21 pts 5 / 21 pts
Unfavorable FISH
8 ptsFludarabine-refractory
4.51-11
Number of prior therapies
12 ptsBulky nodes >5 cm
15.5 x 109/L 0.8-284.3
Lymphocyte count
1910
Gender
67 years 50-79 years
Age
Patient characteristics (n=29)
ASH 2009, abstract 883, Roberts et al1In partnership w/Abbott

49
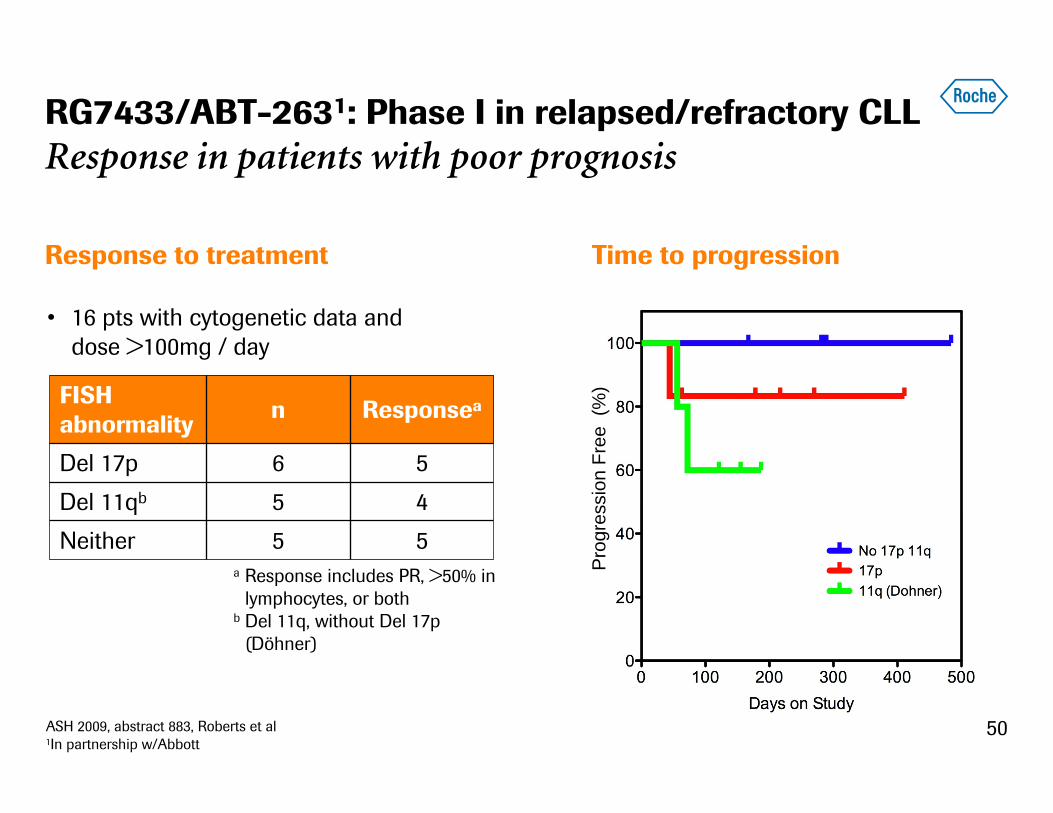
RG7433/ABT-2631: Phase I in relapsed/refractory CLLPromising results in CLL
Efficacy
• Overall response rate (ORR): 29% (7/24)
• ORR excluding 3 pts treated at doses <110 mg: 33% (7/21)
• Median progression-free survival not reached
– Median time on study 9 months (range 1-16 months)
• Fludarabine-refractory pts (5/6 evaluable treated at >100mg)
– 2 partial responses (PR)
– 2 nodal reductions 49% and 47%, respectively
7Stable disease (SD) with >50% peripheral lymphocyte reductions >2mths
2Progressive disease (PD)8Stable disease (SD)
7Partial response (PR)
nResponse type
Pre-treatment After 7 cycles
72-yr male, 7 prior txs, fludarabine-refractory, 17p del
ASH 2009, abstract 883, Roberts et al1In partnership w/Abbott
50
Prog
ress
ion
Free
(%
)
Time to progression
RG7433/ABT-2631: Phase I in relapsed/refractory CLLResponse in patients with poor prognosis
Response to treatment
FISH abnormality
n Responsea
Del 17p 6 5
Del 11qb 5 4
Neither 5 5
• 16 pts with cytogenetic data and dose >100mg / day
ASH 2009, abstract 883, Roberts et al1In partnership w/Abbott
a Response includes PR, >50% in lymphocytes, or both
b Del 11q, without Del 17p (Döhner)

51
RG7433/ABT-2631: Phase I in relapsed/refractory CLLConclusions
• Acceptable safety profile with thrombocytopenia as the dose limiting toxicity (due to Bcl-xL inhibition)
• Single-agent activity observed in relapsed, refractory CLL
• Preliminary evidence of sustained clinical activity with ongoing dosing
– In some fludarabine-refractory patients
– In some patients with 17p del CLL and 11q del CLL
RG7433/ABT-263: Promising data in CLLASH 2009, abstract 883, Roberts et al1In partnership w/Abbott
Dr. Myriam Mendila, Hematology Franchise Leader
Leader in hematology — commercial overview & opportunities

53
MabThera/Rituxan: Leading hematology productTop products commonly used to treat hematological malignancies
Q3-97
Q1-98
Q3-98
Q1-99
Q3-99
Q1-00
Q3-00
Q1-01
Q3-01
Q1-02
Q3-02
Q1-03
Q3-03
Q1-04
Q3-04
Q1-05
Q3-05
Q1-06
Q3-06
Q1-07
Q3-07
Q1-08
Q3-08
Q1-09
MabThera/RituxanImatinibBortezomibLenalidomideDoxorubicinDasatinibDexamethasoneThalidomideTopotecanBendamustinePrednisoneNilotinibFludarabineMelphalanCyclophosphamideAlemtuzumabVincristineBleomycinCladribineIbritumomab tiuxetanChlorambucil
Global sales1
1Source: IMS MIDAS in PADDS as of Q2 2009
54
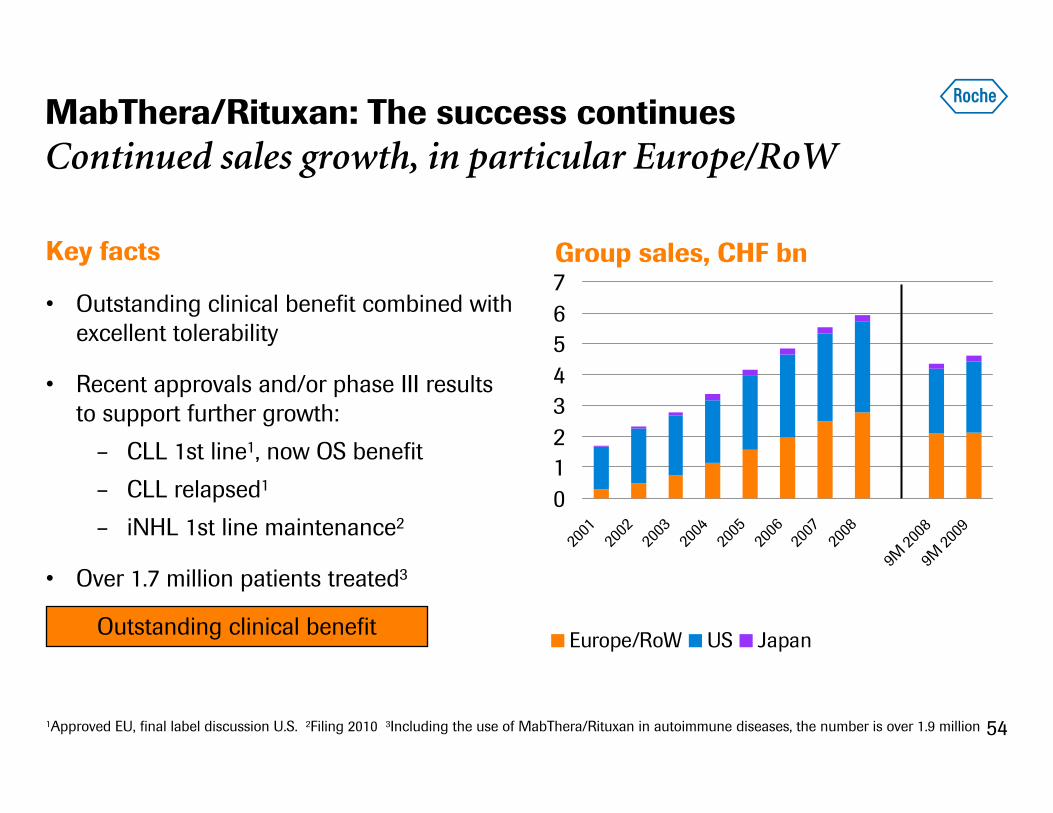
MabThera/Rituxan: The success continuesContinued sales growth, in particular Europe/RoW
Key facts
• Outstanding clinical benefit combined with excellent tolerability
• Recent approvals and/or phase III results to support further growth:
– CLL 1st line1, now OS benefit
– CLL relapsed1
– iNHL 1st line maintenance2
• Over 1.7 million patients treated3
01234567
2001
2002
2003
2004
2005
2006
2007
2008
9M 20
089M
2009
Europe/RoW US Japan
Group sales, CHF bn
1Approved EU, final label discussion U.S. 2Filing 2010 3Including the use of MabThera/Rituxan in autoimmune diseases, the number is over 1.9 million
Outstanding clinical benefit

55
0
10
20
30
40
50
60
70
iNHL
iNHLm
aint
aNHL
CLL
iNHL
iNHLm
aint
aNHL
CLL
iNHL
iNHLm
aint
aNHL
CLL
MabThera/Rituxan: Growth opportunities in EU/RoWPRIMA1 and OS benefit in CLL to drive further uptake
U.S.2 Top-5 EU E73
Growth opportunities
Thou
sand
pat
ient
s tr
eate
d
No MabThera/Rituxan
MabThera/Rituxan1PRIMA study in iNHL 1st line maintenance (filing 2010) 2CLLfinal label discussion U.S. 3E7: Brazil, Russia, China, Mexico, Turkey, South Korea, India

56
MabThera/Rituxan: S.c. formulation in developmentPhase I study has enrolled its first patient
• New formulation will have all the current benefits of MabThera/Rituxan
• Additional benefits for patients, payers and prescribers:– Possibility of non-hospital/self administration – Improved patient convenience and preference provide for greater
independence– Potential for less infusion-related reactions– Less resource-intensive and much faster than current i.v. administration– Reduced medical resource utilization (address capacity issues)
• Proprietary Roche Diagnostics-developed injection device
• First-patient-in in phase I trial in Q3-2009
Maximizing the overall hematology franchise
57
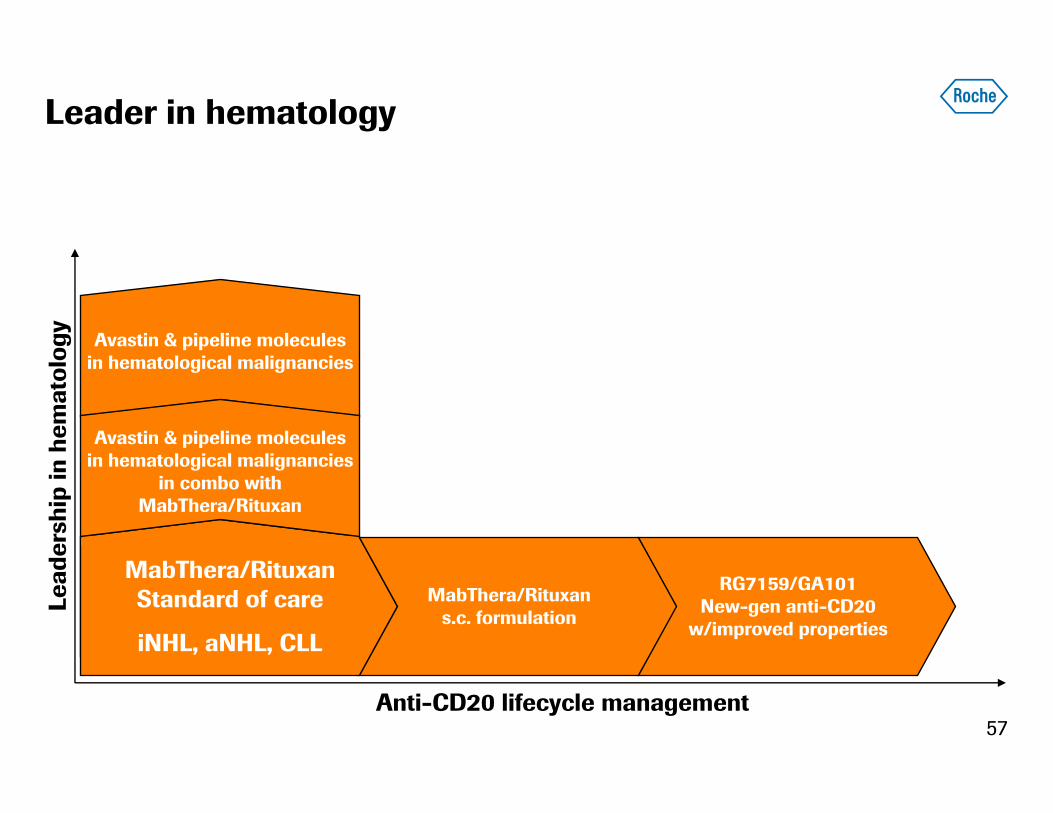
Leader in hematology
MabThera/RituxanStandard of care
iNHL, aNHL, CLL
MabThera/Rituxans.c. formulation
RG7159/GA101New-gen anti-CD20
w/improved properties
Avastin & pipeline molecules in hematological malignancies
Avastin & pipeline molecules in hematological malignancies
in combo with MabThera/Rituxan
Anti-CD20 lifecycle management
Lead
ersh
ip in
hem
atol
ogy

Moderator: Dr. Karl Mahler, Head of Investor Relations
Questions & Answers

59
We Innovate Healthcare







