
u Baltimore
The Hood…
Portland
The real Hood….

Laryngeal Trauma
Paul W. Flint, MD
Otolaryngology – Head & Neck SurgeryOregon Health & Science University

5th Edition 2010
Guri Sandhu, MBBS, FRCSConsultant OtolaryngologistImperial College Healthcare NHS Trust, Charing Cross Hospital
Key Points
u Laryngeal trauma is rare although life threateningu Multiple etiologies: blunt, penetrating, intubation
caustic, thermal, radiation u Evaluation and Airway managementu Timing of interventionu Sequelae

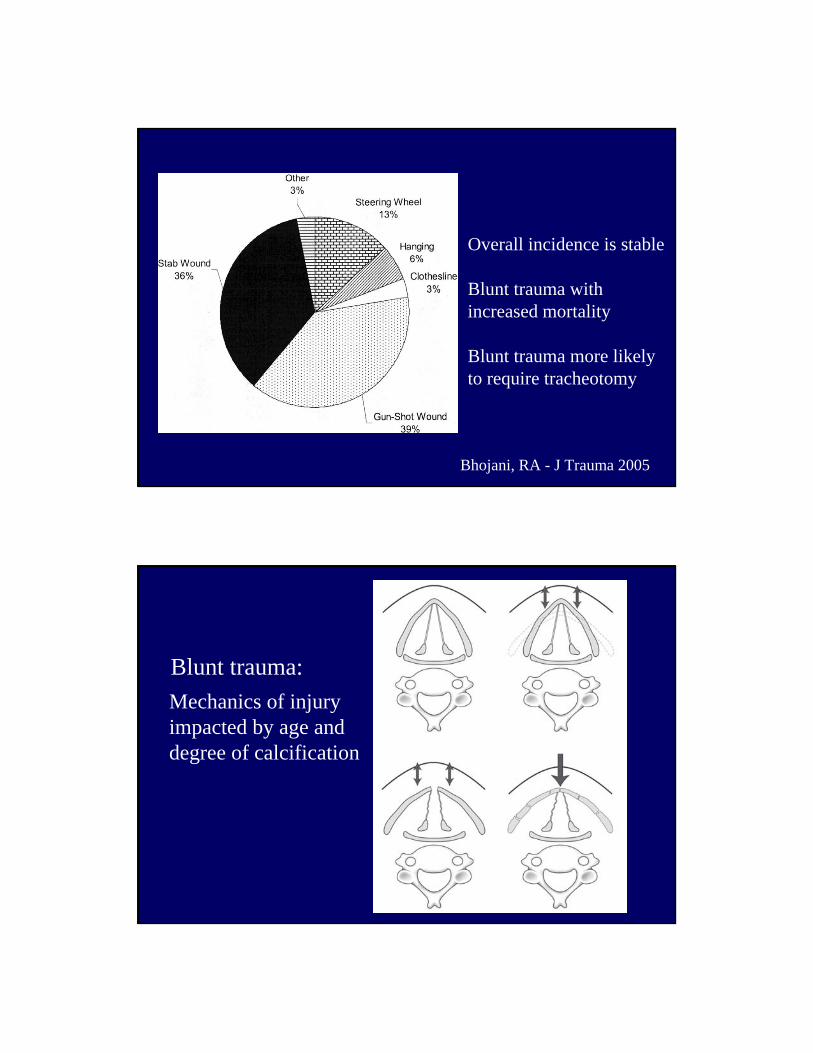
Bhojani, RA - J Trauma 2005
Overall incidence is stable
Blunt trauma withincreased mortality
Blunt trauma more likely to require tracheotomy
Mechanics of injury impacted by age and degree of calcification
Blunt trauma:
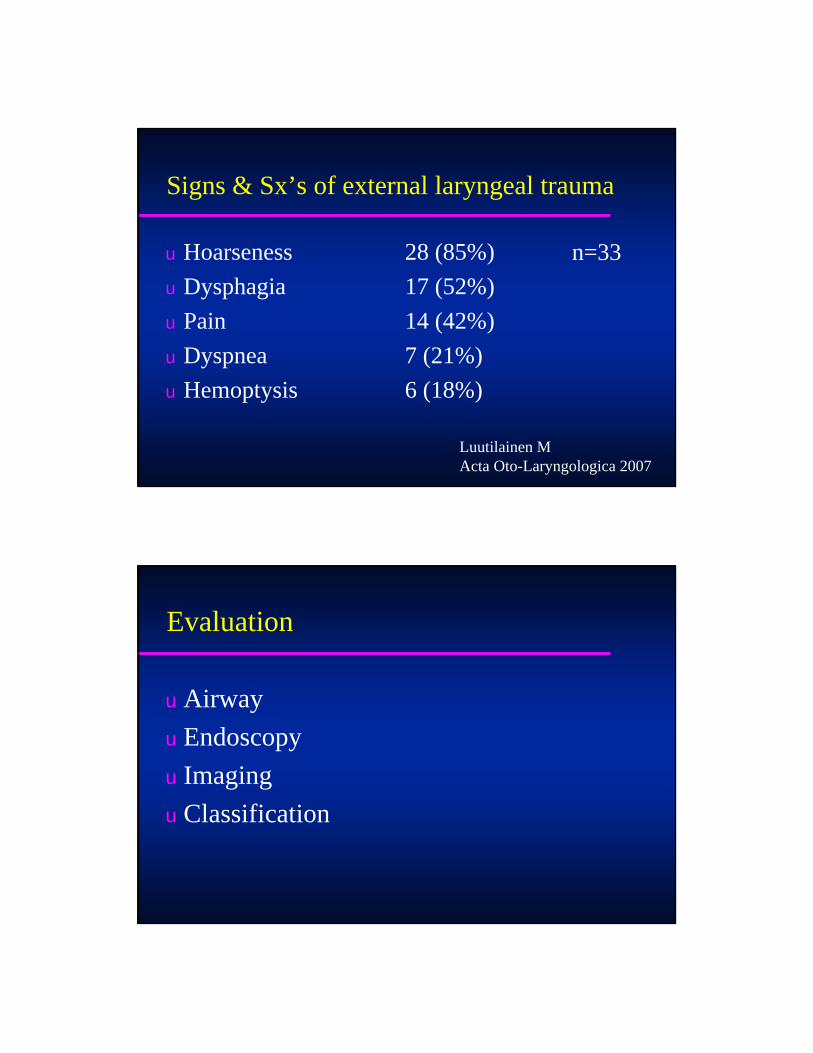
Signs & Sx’s of external laryngeal trauma
u Hoarseness 28 (85%)u Dysphagia 17 (52%)u Pain 14 (42%)u Dyspnea 7 (21%)u Hemoptysis 6 (18%)
Luutilainen MActa Oto-Laryngologica 2007
n=33
Evaluation
u Airwayu Endoscopyu Imagingu Classification
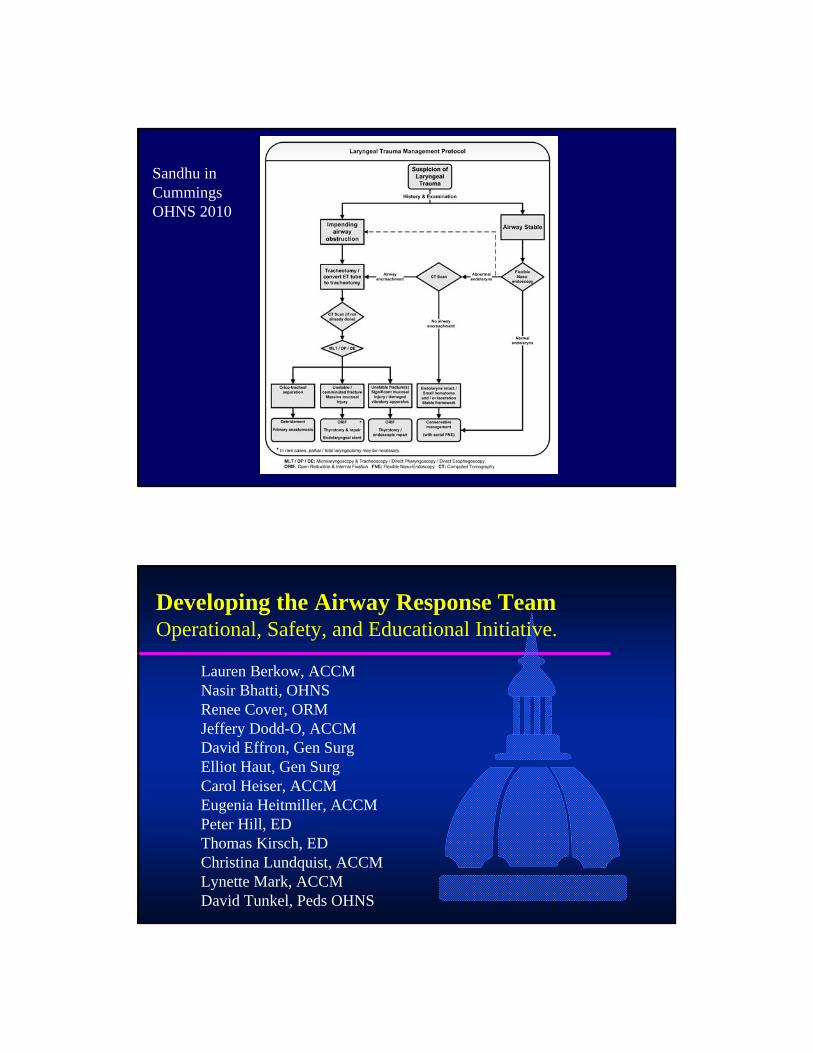
Sandhu in Cummings OHNS 2010
Developing the Airway Response TeamOperational, Safety, and Educational Initiative.
Lauren Berkow, ACCMNasir Bhatti, OHNSRenee Cover, ORMJeffery Dodd-O, ACCMDavid Effron, Gen SurgElliot Haut, Gen SurgCarol Heiser, ACCMEugenia Heitmiller, ACCMPeter Hill, EDThomas Kirsch, EDChristina Lundquist, ACCMLynette Mark, ACCMDavid Tunkel, Peds OHNS
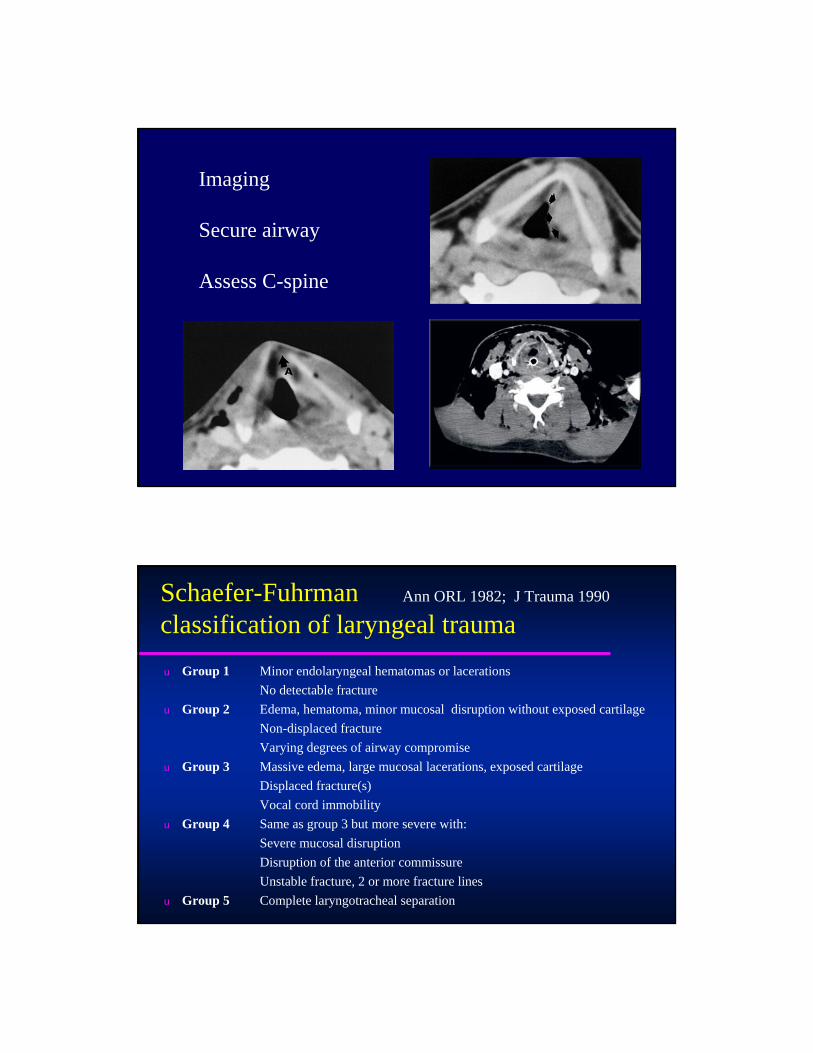
Imaging
Secure airway
Assess C-spine
Schaefer-Fuhrman classification of laryngeal traumau Group 1 Minor endolaryngeal hematomas or lacerations
No detectable fractureu Group 2 Edema, hematoma, minor mucosal disruption without exposed cartilage
Non-displaced fractureVarying degrees of airway compromise
u Group 3 Massive edema, large mucosal lacerations, exposed cartilageDisplaced fracture(s)Vocal cord immobility
u Group 4 Same as group 3 but more severe with:Severe mucosal disruptionDisruption of the anterior commissureUnstable fracture, 2 or more fracture lines
u Group 5 Complete laryngotracheal separation
Ann ORL 1982; J Trauma 1990
Approach to assess need for surgical intervention
u Laryngeal Framework
u Laryngeal Mucosa
u Vibratory Apparatus
u Laryngotracheal junction
Sandhu in Cummings OHNS 2010
Approach to assess need for surgical intervention
u Laryngeal Framework– Stable
No fracturesA single non-displaced fracture
– UnstableA single displaced fracture>1 fracture lineCricoid fracture
– Potentially non-viableFramework comminution with devitalized cartilage fragments
Sandhu in Cummings OHNS 2010
Approach to assess need for surgical intervention
u Laryngeal Framework– Stable
No fracturesA single non-displaced fracture
– UnstableA single displaced fracture>1 fracture lineCricoid fracture
– Potentially non-viableFramework comminution with devitalized cartilage fragments
Sandhu in Cummings OHNS 2010
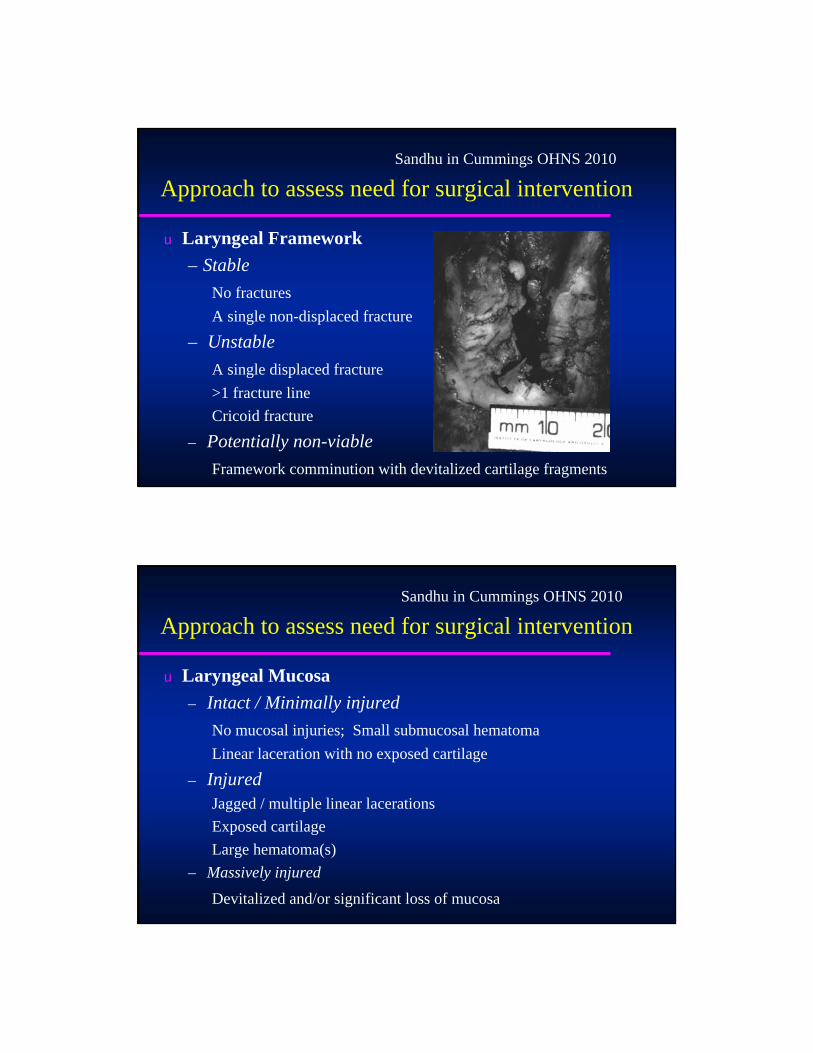
Approach to assess need for surgical intervention
u Laryngeal Mucosa– Intact / Minimally injured
No mucosal injuries; Small submucosal hematomaLinear laceration with no exposed cartilage
– InjuredJagged / multiple linear lacerations Exposed cartilageLarge hematoma(s)
– Massively injured
Devitalized and/or significant loss of mucosa
Sandhu in Cummings OHNS 2010
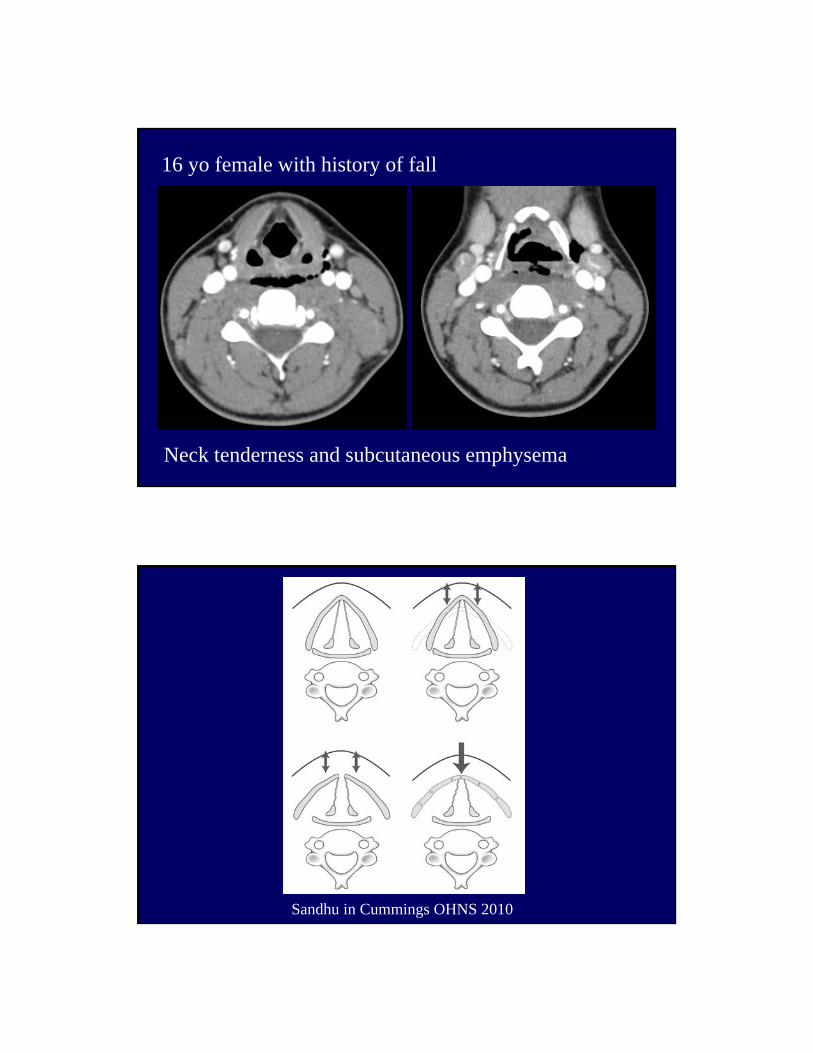
16 yo female with history of fall
Neck tenderness and subcutaneous emphysema
Sandhu in Cummings OHNS 2010

Concomitant injuries with laryngeal trauma
Injury (%)u Open Neck Injury 18u Maxillofacial Fractures 18u Intracranial Injuries 17u Cervical Spine Fracture 13u Chest Injury 13u Other Facial Injury 10u Skull Fracture 7u Open Pharyngeal Injury 4
Jewett, Arch Otol-HNS 1999
Management
u Acute trauma

Sandhu in Cummings OHNS 2010
17 yo HS student struck in neck with lacrosse stick
PainHoarseness


Approach to assess need for surgical intervention
u Vibratory Apparatus– Intact– Injured
Anterior commissureVibrating edge of the vocal cord(s)Arytenoid dislocation
Sandhu in Cummings OHNS 2010
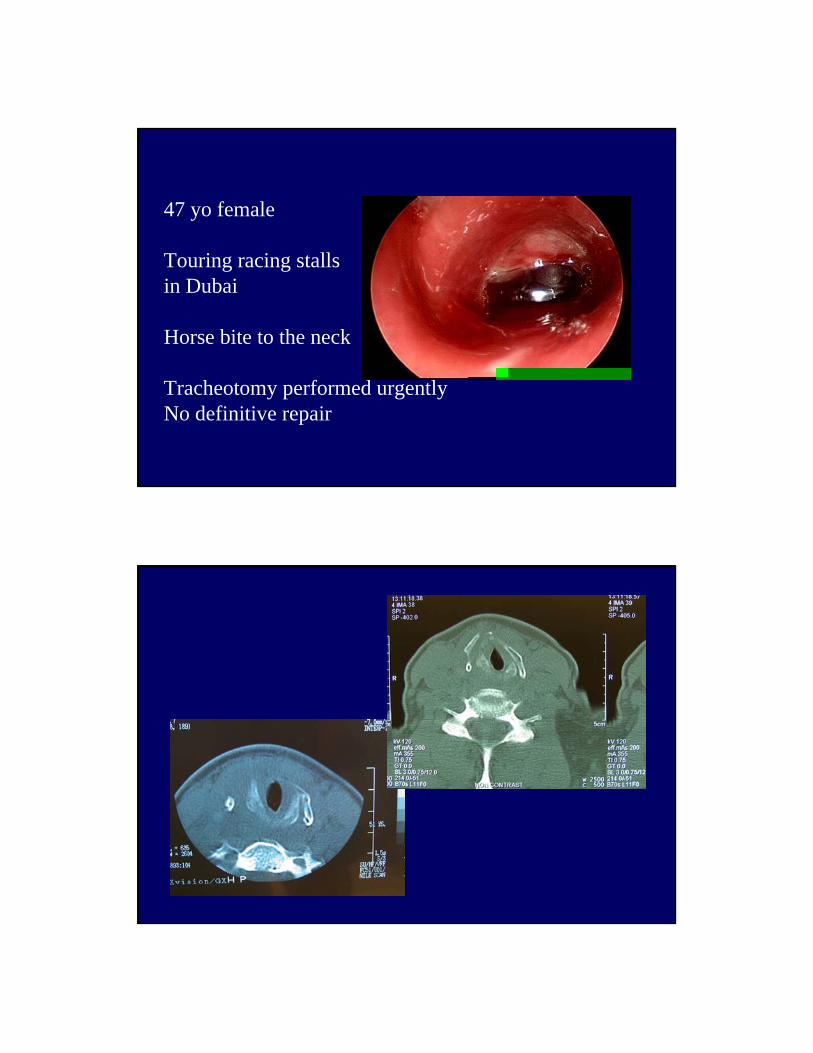
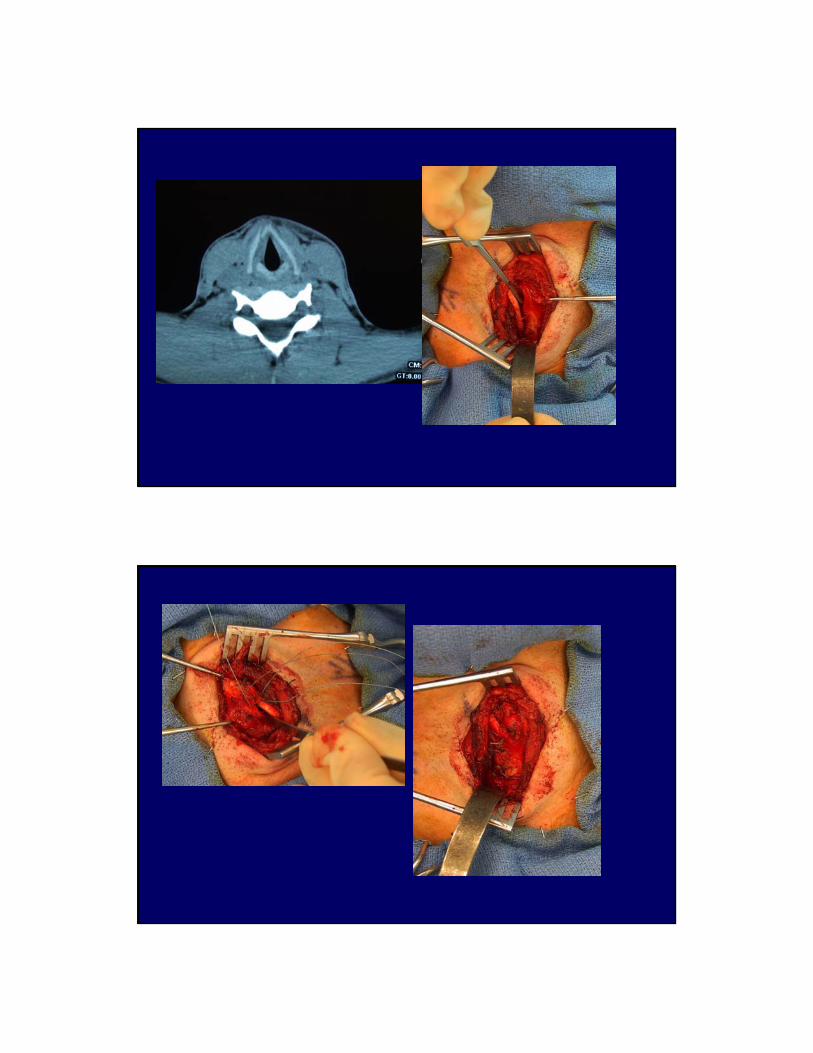
47 yo female
Touring racing stalls in Dubai
Horse bite to the neck
Tracheotomy performed urgentlyNo definitive repair
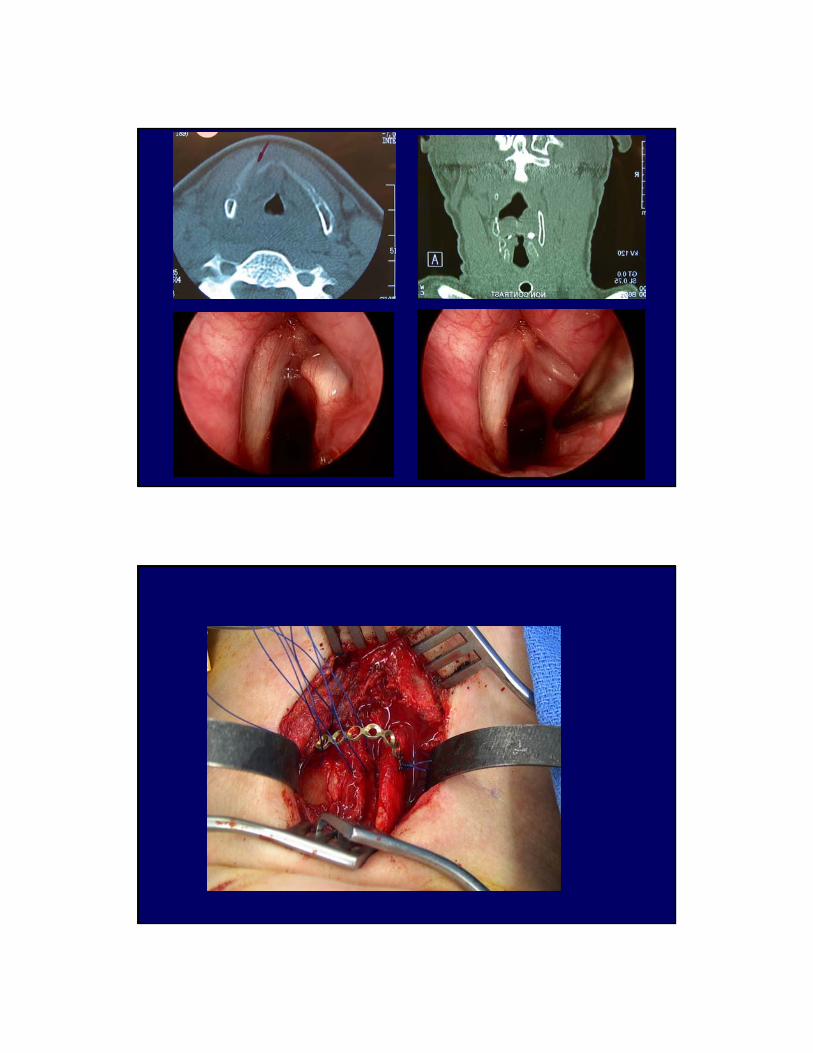

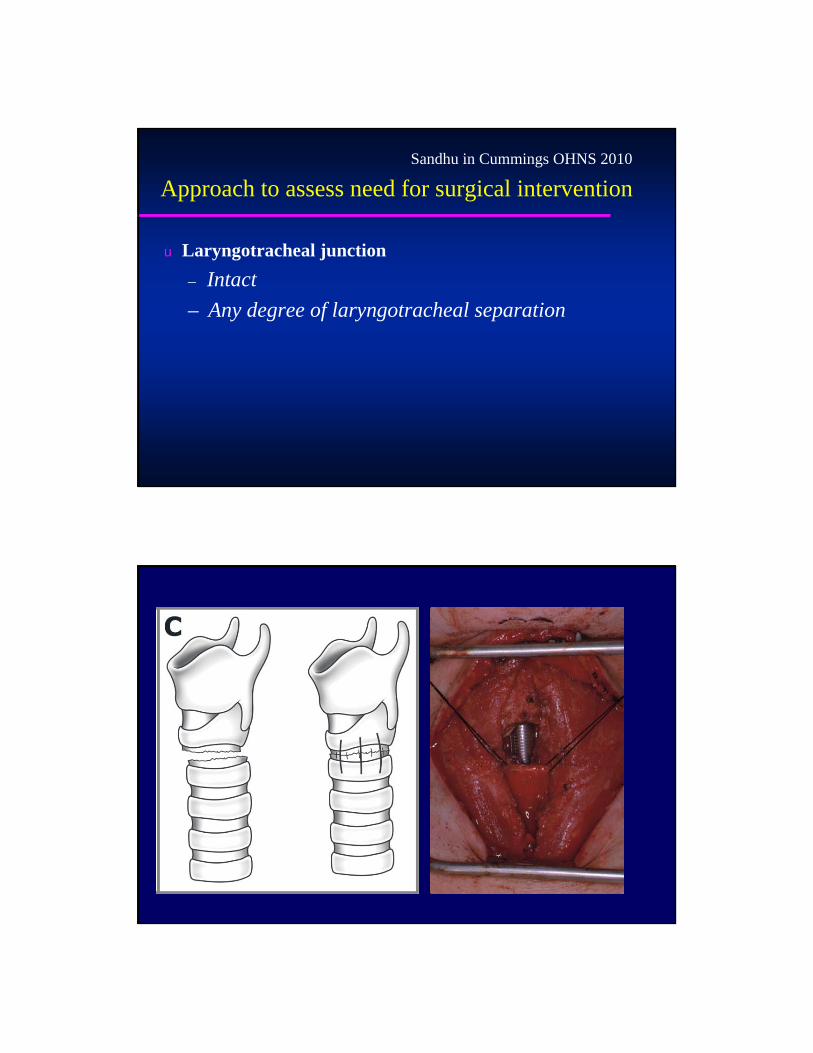
Approach to assess need for surgical intervention
u Laryngotracheal junction– Intact– Any degree of laryngotracheal separation
Sandhu in Cummings OHNS 2010
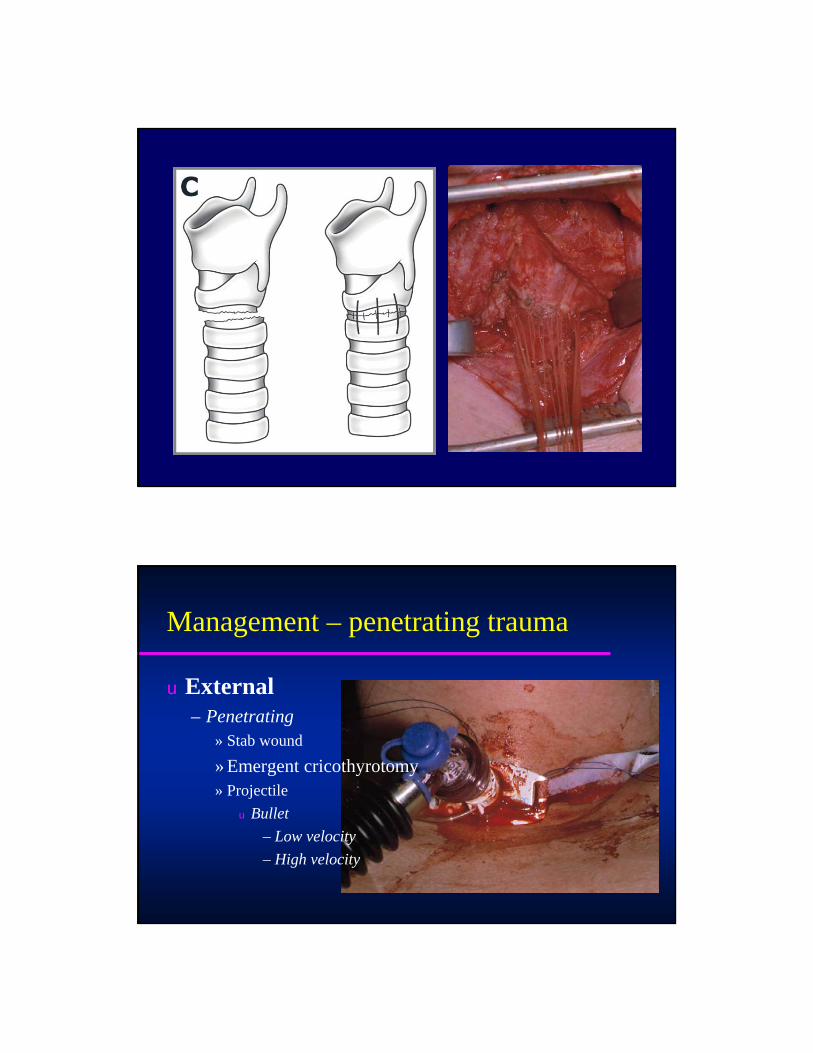
Management – penetrating trauma
u External– Penetrating
» Stab wound
» Emergent cricothyrotomy» Projectile
u Bullet– Low velocity– High velocity
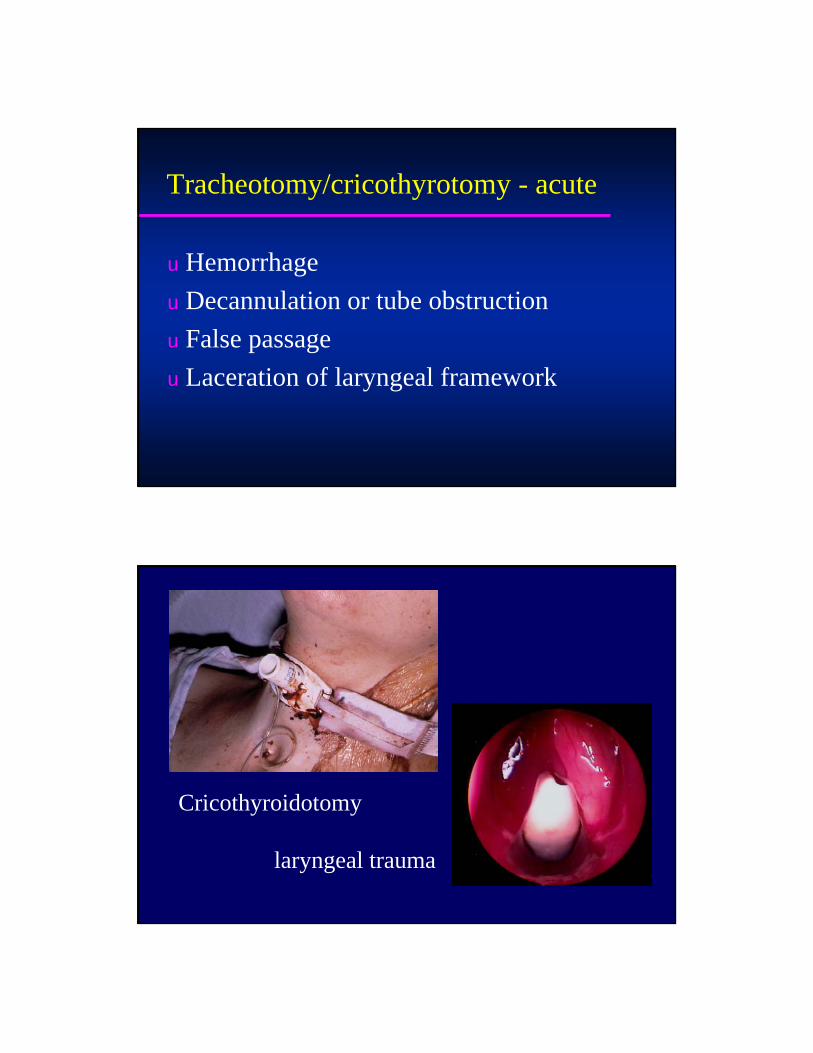
Tracheotomy/cricothyrotomy - acute
u Hemorrhageu Decannulation or tube obstructionu False passageu Laceration of laryngeal framework
Cricothyroidotomy
laryngeal trauma

“Slash”Cricothyroidotomy
necessitates earlyearly endoscopic evaluation and repair
Voice outcome following laryngeal trauma
u Results from SchaeferGroup Voice outcome Airway outcome
Good Fair Poor Good Fair Poor1 20 0 0 20 0 02 38 3 0 40 1 03 18 3 0 21 0 04 22 10 0 31 0 2
u Results from Luutilainen et al2 12 4 0 16 0 03 7 6 0 13 0 04 1 3 0 4 0 0
Cummings OHNS 2010
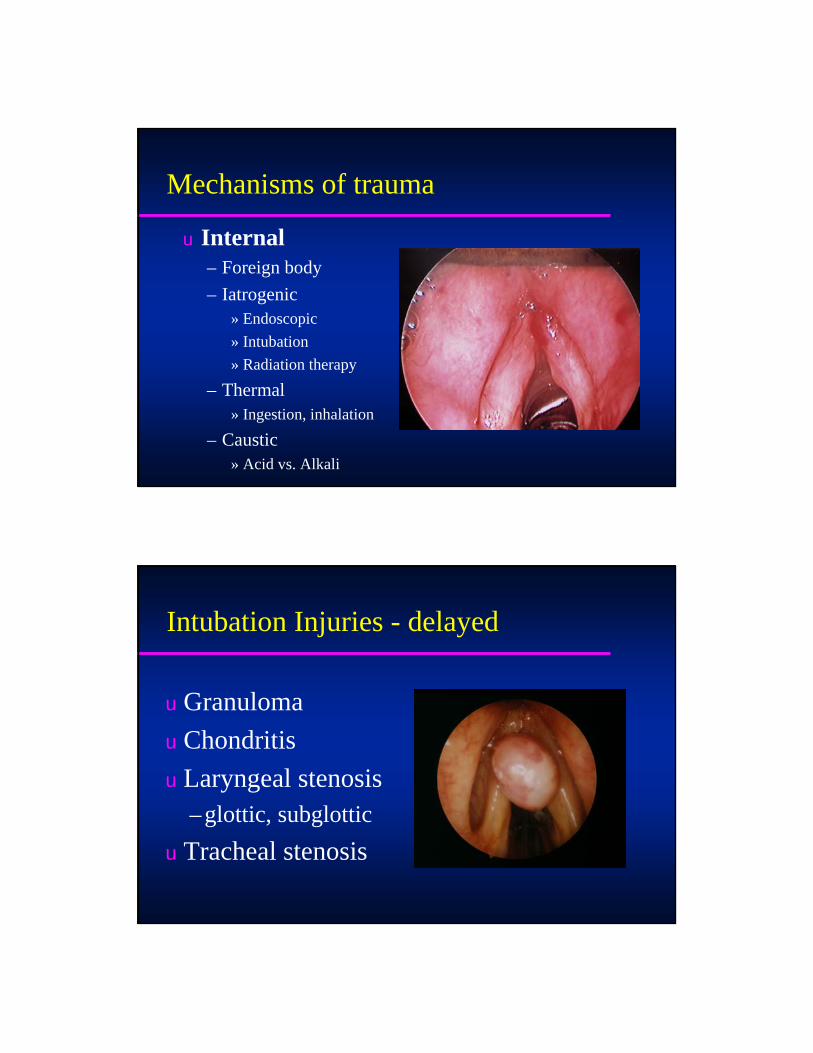
Mechanisms of trauma
u Internal– Foreign body– Iatrogenic
» Endoscopic» Intubation» Radiation therapy
– Thermal» Ingestion, inhalation
– Caustic» Acid vs. Alkali
Intubation Injuries - delayed
u Granulomau Chondritisu Laryngeal stenosis
– glottic, subglotticu Tracheal stenosis

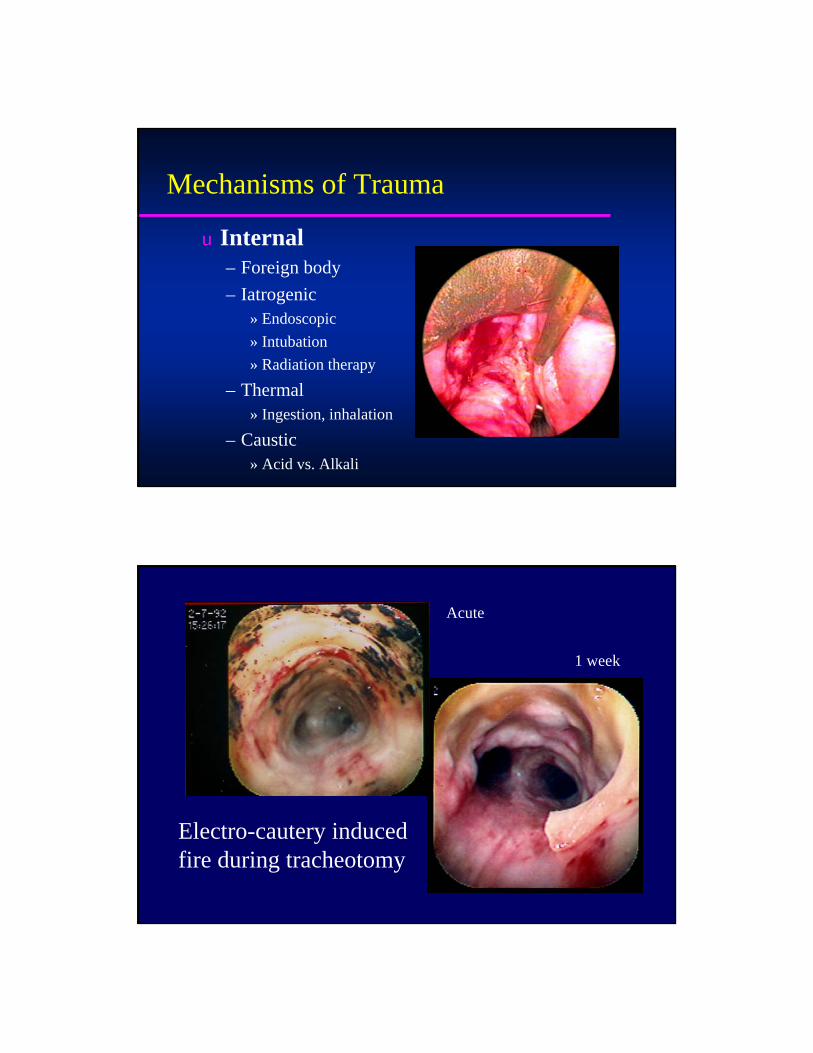
Mechanisms of Trauma
u Internal– Foreign body– Iatrogenic
» Endoscopic» Intubation» Radiation therapy
– Thermal» Ingestion, inhalation
– Caustic» Acid vs. Alkali
Prolonged intubationdefined by hours
-Weymuller
Mechanisms of Trauma
u Internal– Foreign body– Iatrogenic
» Endoscopic» Intubation» Radiation therapy
– Thermal» Ingestion, inhalation
– Caustic» Acid vs. Alkali
Electro-cautery inducedfire during tracheotomy
Acute
1 week

Management
u Sequelae
Long term sequelae
u Vocal fold motion impairment– Paralysis– Dislocation– Joint fixation
u Stenosis
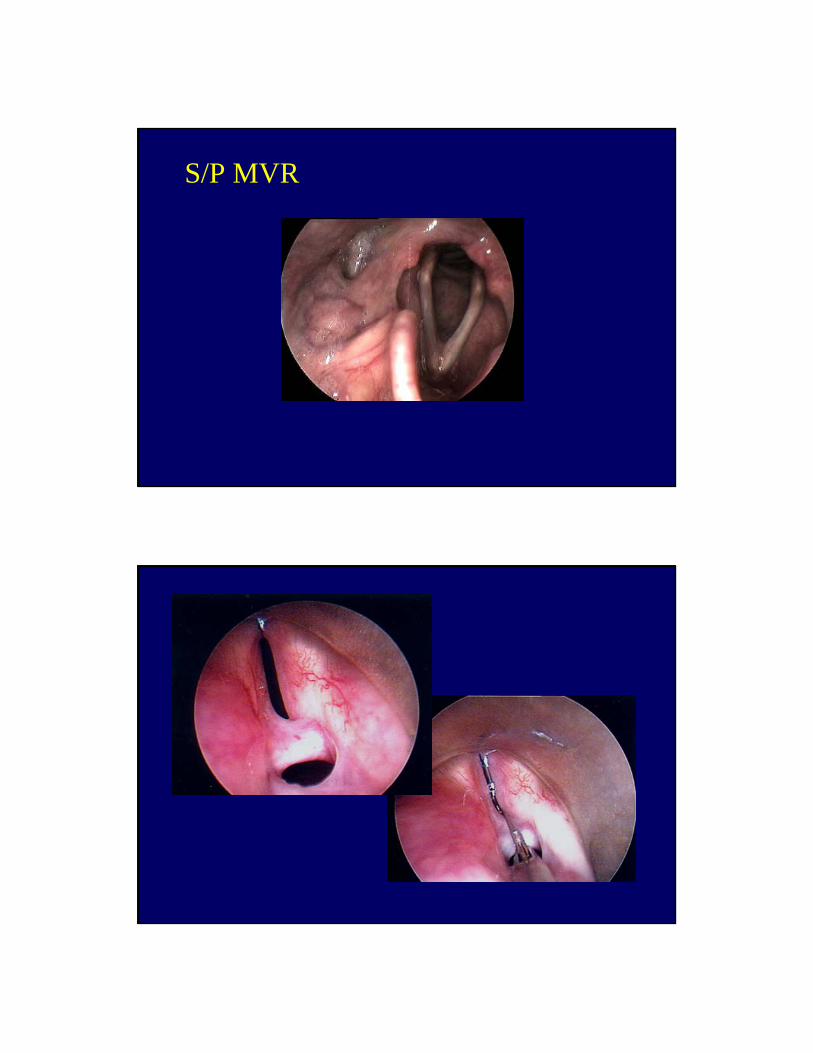
S/P MVR

Posterior glotticfibrosis
Posterior cricoid split with graft

Posterior graft in position

Post op examPre op exam
Posterior cricoid split & rib graft
23 yo female with poly traumasecondary to MVA
Tracheotomy in the field
Unable to decannulate
Multiple endoscopic procedures
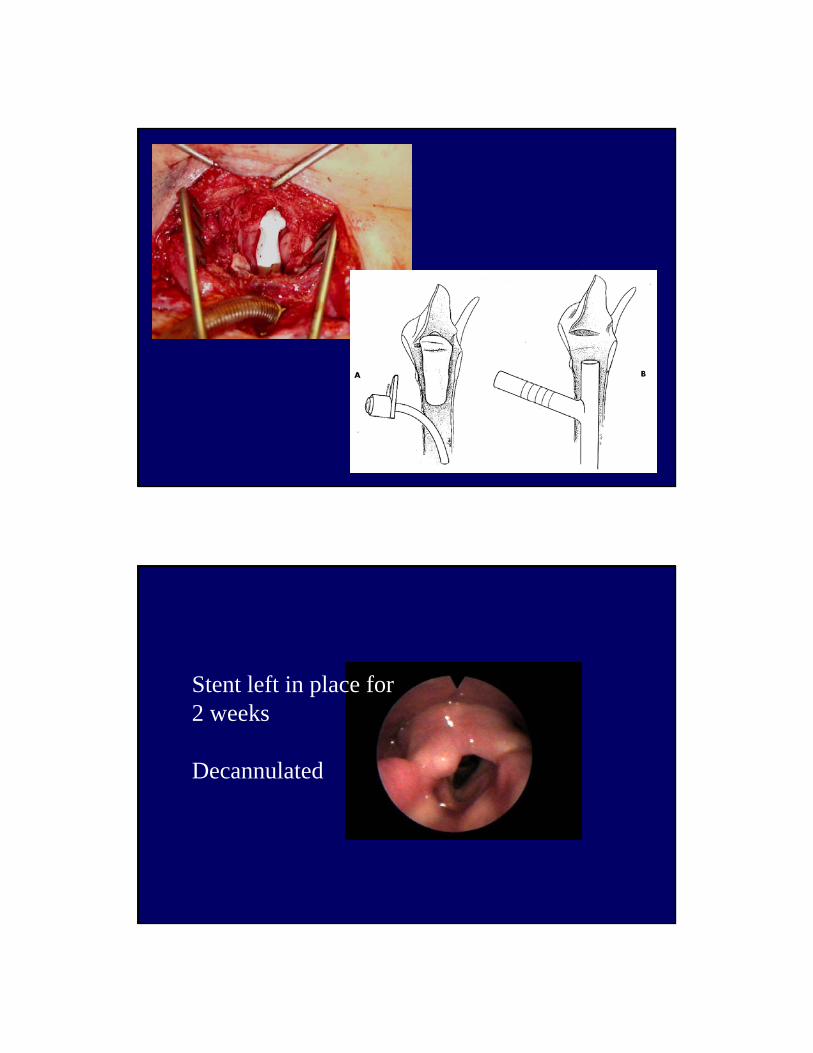
Stent left in place for 2 weeks
Decannulated
Intubation Injuries - Contributing factors
u Technique– visualization vs. blind, laryngeal blade
u ETT– size, duration, material
u Vent pressure, ETT fixation
Intubation Injuries - Contributing factors
u Patient activity - motionu Unconscious patientu NG tube, GERu Obesity, DM, nutritional status...
Intubation Injuries - Prevention
u Preop laryngoscopy?u Smallest tube, shortest durationu Anti-reflux regimenu Avoid rigid NGT
Intubation Injuries - Prevention
u Monitor vent/cuff pressuresu Early trach in high risk patientsu Endoscopic assessment
– steroid injection may be beneficial
Key Points
u Laryngeal trauma is rare although life threateningu Multiple etiologies: blunt, penetrating, intubation
caustic, thermal, radiation u Evaluation and Airway managementu Timing/sequence of interventionu Sequelae


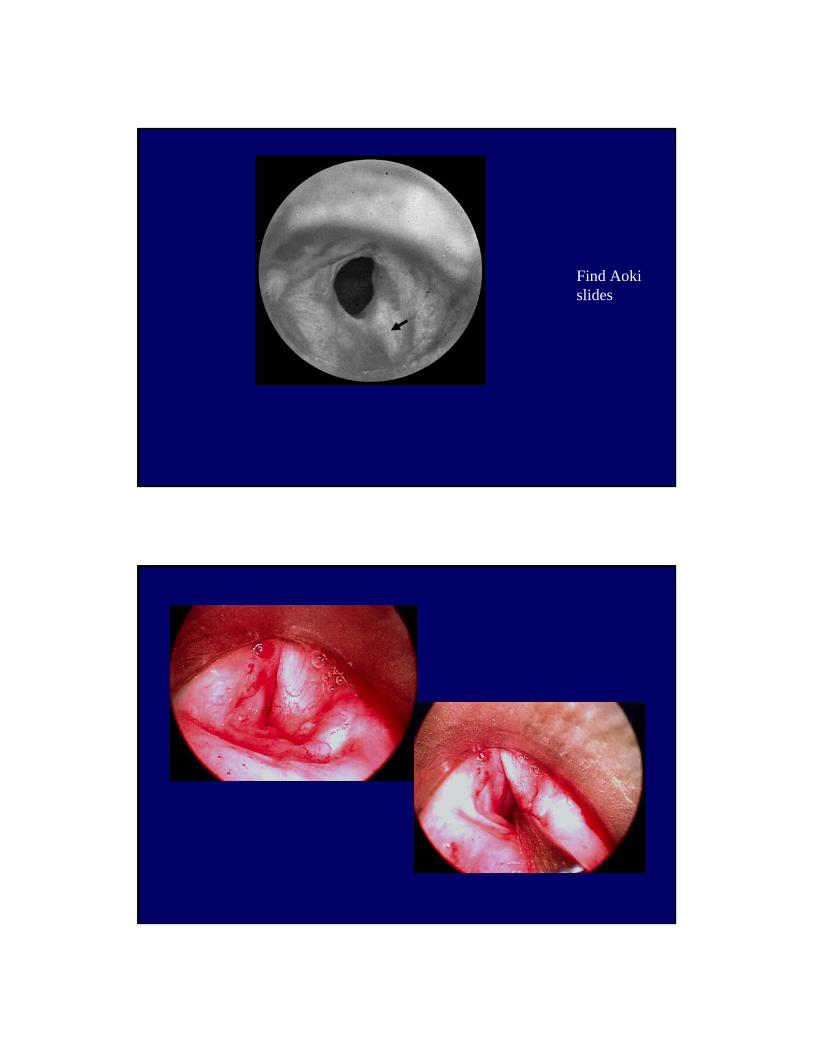
Find Aoki slides

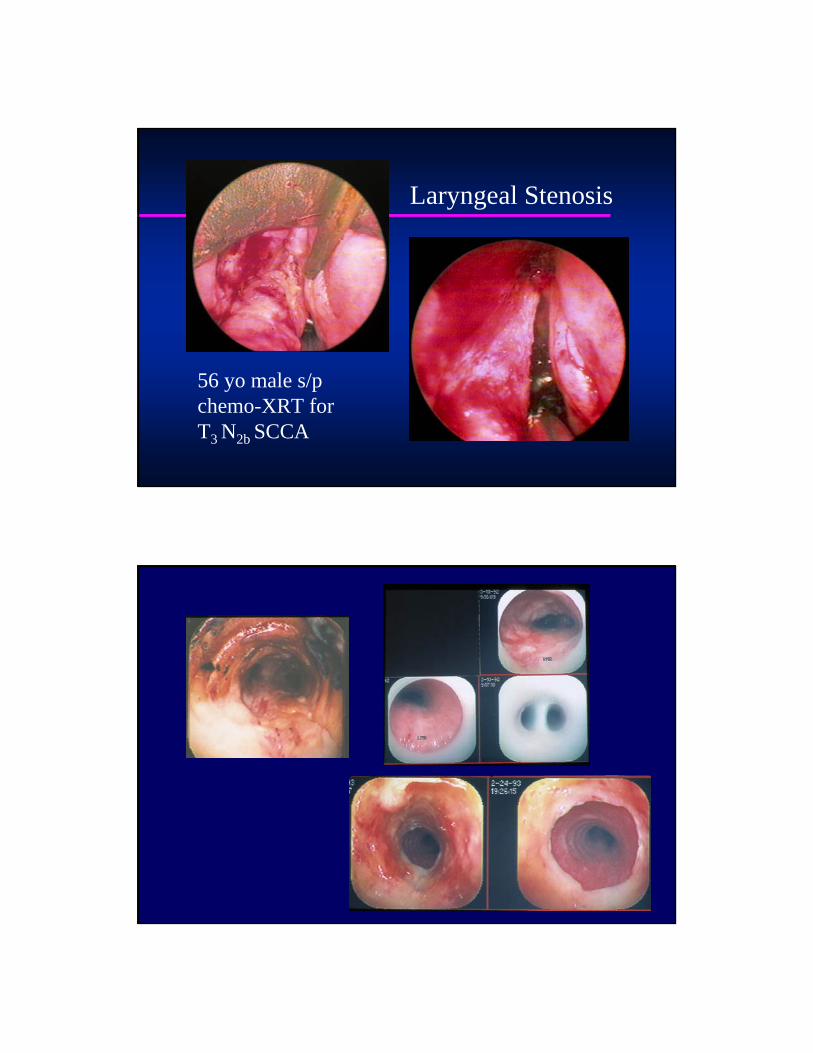
Laryngeal Stenosis
56 yo male s/pchemo-XRT for T3 N2b SCCA

Laryngeal Paralysis

Vocal fold polyp

Subglottic stenosis
Endoscopic resectionand placement of T-tube through trach site
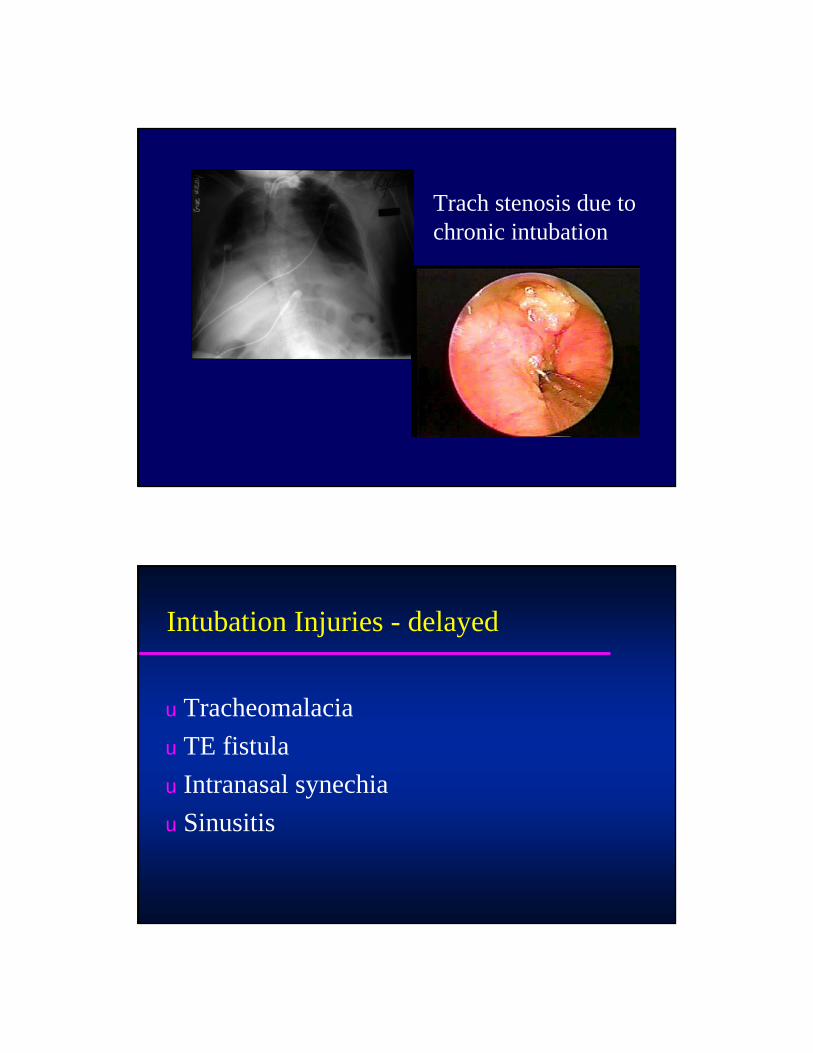
Trach stenosis due to chronic intubation
Intubation Injuries - delayed
u Tracheomalaciau TE fistulau Intranasal synechiau Sinusitis

Intubation Injuries - acute
u Dental injuryu Soft tissue trauma
– nasal, oral, pharyngeal, hypopharyngealu Vocal fold contusion, lacerationu Vocal fold motion impairment
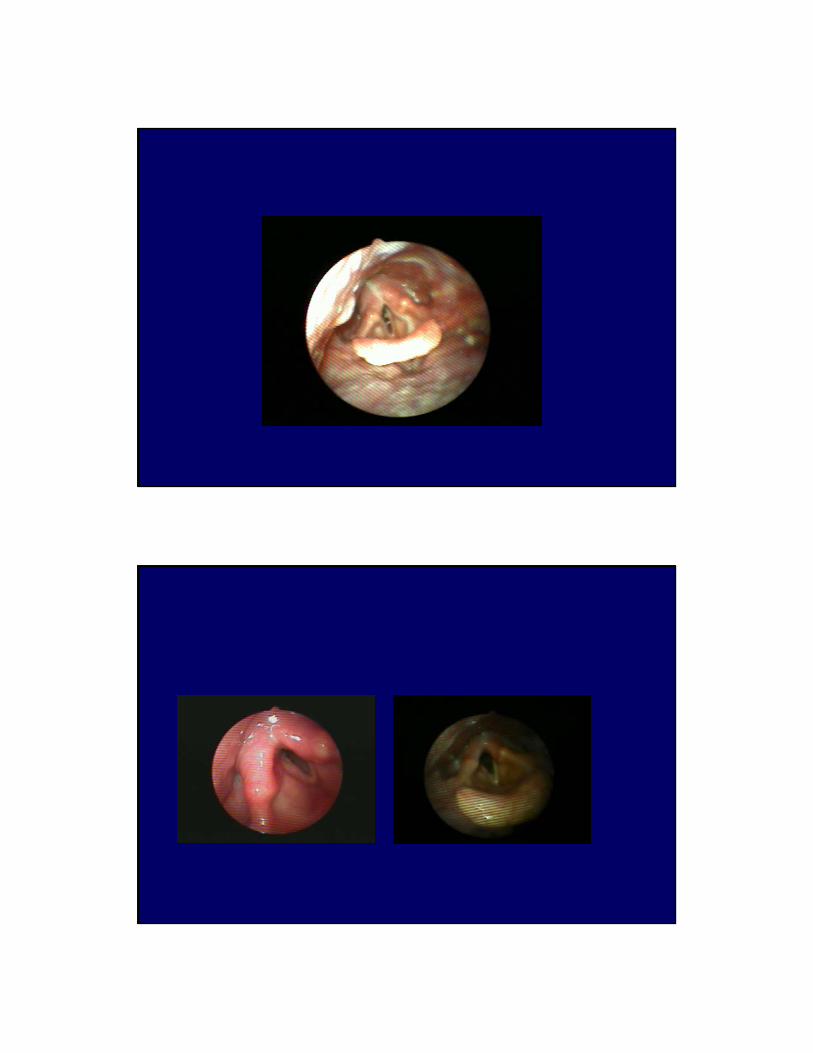
70 yo maleintubated 7 days S/P CABGwith NGT

69 yo female prolongedintubation S/P CABG

Mechanisms of Trauma
u ExternalBlunt
» Hanging» Clothesline injury» Sports Injury» Motor Vehicle Accident
u Internal
Penetrating» Stab wound» Emergent cricothyrotomy» Projectile
BulletLow velocityHigh velocity
Management
u ExternalBluntPenetrating

Post cricoid split – endoscopic view







![Kan waa guri - arts.unimelb.edu.au · Kan waa guri ! Sue Worcester Somali ! LEVEL 1 KAN WAA GURI SOMALI Title : Kan waa guri [This is a house] Author: Sue Worcester Translator: Ali](https://cdn.vdocuments.us/doc/165x107/5c5b91f809d3f240368bf74e/kan-waa-guri-arts-kan-waa-guri-sue-worcester-somali-level-1-kan-waa-guri.jpg)