download the latest issue - green cross publishing
TRANSCRIPT

The Journal of the Irish Practice Nurses AssociationIssue 5 Volume 4 September/October 2011
MulTIMOrbIdITy – PArT 1Jane CampionDr Mary Byrne
cySTIc fIbrOSISYvonne McDonaghCatherine Meagher
SPIrOMeTry TeSTINgMaria McNeil
dePreSSION – SyMPTOMS, dIAgNOSIS
ANd TreATMeNTAlison Lane
Q ANd AMary O’connor,
National Honorary Treasurer
Are your patients at risk?
Pneumococcal DiseaseVaccinate your at-risk patients and those 65 years and over against serious pneumococcal disease.
09/11 IR00094c
age 65+
chronic lung, heart or renal
disease
weakenedimmunesystem
other at-risk groups**smoker
diabetes
infant*
Vaccinate your at-risk patients and those 65 years
v is i t one inseven. ie
Marketing authorisation holder: Sanofi Pasteur MSD Limited, Block A, Second Floor, Cookstown Court, Old Belgard Road, Tallaght, Dublin 24. Marketing authorisation number: PA 544/21/3 Legal category: POM
Information about adverse event reporting can be found at www.imb.ie. Adverse events and inadvertent vaccination during pregnancy should also be reported to Sanofi Pasteur MSD by calling 00 44 1628 785291.
* All infants are offered immunisation against pneumococcal disease as part of the National Immunisation Programme.** See Immunisation Guidelines for Ireland www.immunisation.ie

*IMPORTANT CHANGE: Prostap Dual Chamber Syringe (DCS) is replacing Prostap, so it’s necessary for prescriptions to reflect this change of name. A video demonstrating
the five steps of administration can be viewed at www.ProstateCancerUpdate.ie
Needle shown is not actual size
*
come as standardWhen it comes to the treatment of prostate cancer,look no further than Prostap DCS
Prescribing InformationPROSTAP *SR DCS, 3.75mg / PROSTAP *3 DCS, 11.25mg powder and solventfor prolonged-release suspension for injection in pre-filled syringe; LeuprorelinAcetate 1 month / 3 month Depot Injection Before prescribing PROSTAP SRDCS/PROSTAP 3 DCS, please refer to the full Summary of Product Characteristics(SmPC). PRESENTATION: Powder and solvent for prolonged- release suspension forinjection in pre-filled syringe (Dual Chamber Syringe); PROSTAP SR DCS Powder:Contains 3.75mg of leuprorelin acetate. PROSTAP 3 DCS Powder: Contains 11.25mgof leuprorelin acetate. INDICATIONS: PROSTAP SR DCS and PROSTAP 3 DCS:Management of prostatic carcinoma for which suppression of testosterone is indicated.Management of oestrogen dependent gynaecological disorders including themanagement of pain and lesions associated with endometriosis. Preoperativemanagement of uterine fibroids to reduce their size and associated bleeding.PROSTAP SR DCS is also indicated for: Endometrial preparation prior to intrauterinesurgical procedures including endometrial ablation or resection. DOSAGE ANDADMINISTRATION: Male adults: PROSTAP SR DCS: 3.75mg administered as a singlesubcutaneous or intramuscular injection every month. PROSTAP 3 DCS: 11.25mgadministered as a single subcutaneous or intramuscular injection every 3 months. Donot discontinue when remission or improvement occurs. Response to therapy shouldbe monitored clinically. Female adults: Treatment should be initiated during the first5 days of the menstrual cycle. PROSTAP SR DCS: 3.75mg administered as a singlesubcutaneous or intramuscular injection every month for a period of 6 months(endometriosis), for a maximum of 6 months (uterine fibrosis). Vary the injection siteperiodically. PROSTAP 3 DCS: 11.25mg administered as a single subcutaneous orintramuscular injection every 3 months: For a period of 6 months (endometriosis), fora maximum of 6 months (uterine fibroids). Vary the injection site periodically. Elderly:
As for adults. Children: Use in children not established. CONTRAINDICATIONS:Hypersensitivity to any of the ingredients or to synthetic GnRH or GnRH derivatives.Men: Use in patients insensitive to endocrine therapy or post-orchidectomy. Women:Use in women who are or may become pregnant, in women who are breastfeedingor who have undiagnosed abnormal vaginal bleeding. PRECAUTIONS ANDWARNINGS: Development or aggravation of diabetes may occur, therefore diabeticpatients may require more frequent monitoring of blood glucose. Hepatic dysfunctionand jaundice with elevated liver enzyme levels have been reported. Therefore, closeobservation should be made and appropriate measures taken if necessary. Spinalfracture, paralysis, hypotension and worsening of depression have been reported.Men: Should only be used under the direction of a clinician having appropriatefacilities for monitoring response to treatment. Testosterone should fall to castratelevels within 6 weeks; failure to do so requires reassessment. Initial transient rise inlevels of testosterone may be associated with tumour “flare” manifesting as systemicor neurological symptoms. Patients at risk of ureteric obstruction or spinal compressionshould be carefully considered and monitored during initial weeks of treatment. Ananti-androgen may be administered to reduce the risk of “flare” (see section 4.4 ofthe SmPC). Any urological or neurological complications which occur should betreated by appropriate specific measures. Women: Menstruation should stop duringtreatment; therefore the patient should notify her physician if regular menstruationpersists.Spotting/breakthrough bleeding may occur with PROSTAP SR DCS andPROSTAP 3 DCS treatment. An increase in clinical signs and symptoms may beobserved during the initial days of therapy as sex steroids temporarily rise abovebaseline. In the case of uterine fibroids, it is mandatory to confirm the diagnosis offibroids and exclude ovarian mass, before therapy is instituted. May cause an increasein uterine cervical resistance. The induced hypo-oestrogenic state results in a clinically
significant loss in bone density over the course of treatment, some of which may notbe reversible. The generally accepted level of bone loss with LHRH analogues suchas PROSTAP is 5%. During one 6 month treatment period, this bone loss should notbe important. In patients with major risk factors for decreased bone mineral contentsuch as chronic alcohol and/or tobacco use, strong family history of osteoporosis, orchronic use of drugs that can reduce bone mass, therapy may pose an additional risk.Treatment options for vasomotor symptoms and bone mineral density loss should beconsidered. In the treatment of endometriosis, the addition of HRT (an oestrogen andprogestogen) has been shown to reduce bone mineral density loss and vasomotorsymptoms. SIDE EFFECTS: Refer to section 4.8 of the SmPC in relation to other sideeffects Serious: Pituitary apoplexy, anaphylactic reactions, alteration of glucosetolerance which may affect diabetic control. Common: Weight gain, anorexia,depression (occasionally severe), headache, hot flushes, nausea, vomiting, muscleweakness, arthralgia, impotence, decreased libido, orchiatrophy, gynaecomastia,irritation at the injection site, sweating, fatigue, peripheral oedema, insomnia,parasthesia, increases in liver function test values (usually transient). Men: If tumourflare occurs, symptoms and signs due to disease may exacerbate e.g. bone pain andurinary obstruction, which should subside on continuation of therapy. Women:Adverse events occurring most frequently with PROSTAP SR DCS and PROSTAP 3DCS are associated with hypo-oestrogenism. The induced hypo-oestrogenic stateresults in a loss in bone density over the course of treatment, some of which may notbe reversible (see Precautions and Warnings). In women who have submucous fibroidsthere have been reports of severe bleeding following the administration of PROSTAPSR DCS and PROSTAP 3 DCS as a consequence of the acute degeneration of thefibroids. Patients should be warned of the possibility of abnormal bleeding or pain incase earlier surgical intervention is required. LEGAL CATEGORY: POM. PACKAGE
QUANTITIES: PROSTAP SR DCS: One dual chamber pre-filled syringe containing3.75mg leuprorelin acetate powder in the front chamber and 1ml of Sterile Solvent inthe rear chamber. One 25 gauge needle, one syringe plunger and one injection siteswab are included in a single injection pack. PROSTAP 3 DCS: One dual chamber pre-filled syringe containing 11.25mg leuprorelin acetate powder in the front chamberand 1ml of Sterile Solvent in the rear chamber. One 23 gauge needle, one syringeplunger and one injection site swab are included in a single injection pack. PRODUCTAUTHORISATION NUMBER: PROSTAP SR DCS PA 1547/3/3; PROSTAP 3 DCS PA1547/3/4. PRODUCT AUTHORISATION HOLDER: Takeda UK Limited, Takeda House,Mercury Park, Wooburn Green, High Wycombe, Bucks. HP10 0HH, UK. DATE OFPREPARATION: May 2011. Full prescribing information is available on request from:Takeda UK Limited, Takeda House, Mercury Park, Wooburn Green, High Wycombe,Bucks. HP10 0HH, UK. Tel: +44 1628 537900 * Trade mark of Takeda PS110525.
Date of preparation: August 2011 PT110703
Adverse events should be reported to the Pharmacovigilance Unit at the Irish Medicines Board
(IMB) ([email protected]). Information about adverse event reporting
can be found on the IMB website (www.imb.ie). Adverse events should also be reported to
Takeda UK Ltd. on +44 1628 537900.
PRI132 rocket ad AW_Layout 1 23/08/2011 12:22 Page 1

1
editorial
IPNA conference time is upon us once again and this year sees a conference with a difference. The South Tipperary branch has put together an interesting, stimulating and very relevant conference in Tullamore on Friday 14th and Saturday 15th October. The format has been changed to encourage attendance and introduce practice nurses to the IPNA and the benefits of membership. The conference brings together practice nurses from around
the country and provides an opportunity to meet, learn, discuss and to network with each other. For this year’s conference, it has been decided to open up the conference to practice nurses who are not members of the IPNA. This is a welcome and timely opportunity and never has been more in need given the current environments we find ourselves working in. We are, so often, isolated and alone in the world of general practice and the need for support is now evident more than ever if we are to sustain and maintain the level of skill and expertise that we have worked hard to develop over the last 20 years. As a member of the IPNA, you have the support and friendship of nurses in your local branch. Practice nurses who are not members don’t have this for whatever reason and the national conference now provides this valuable opportunity to them.
The South Tipperary branch has put together a programme which has a clinical focus. Friday afternoon opens the conference with workshops on venesection, teaching breast self-examination and ECG interpretation. The keynote speaker on Friday evening will be Dr Tony Humphries who will speak on motivation. Saturday morning opens with a presentation on psychiatry issues in general practice, sexual health and concludes with a practice nurse’s experience of nurse prescribing in general practice. The AGM will take place on Saturday afternoon. Throughout the conference a number of awards will be presented – the research bursary award, the clinical award and the Valerie Mangan Loyalty Award.
The IPNA brings together practice nurses new and experienced. It is a great opportunity to learn from each other and meet nurses who work in similar situations. The conference, once again, is supported by the pharmaceutical industry and again, this gives a valuable opportunity to access up to date research and clinical practice.
I wish the best of luck to the South Tipperary branch with a conference which I am sure will be stimulating and enjoyable. See you all in Tullamore.
Ruth Morrow
Annual conference – calling ALL practice nurses

Life. To be continued.
tiotropium
Long acting, specific antimuscarinic agent, available as hardcapsules of powder for inhalation, containing tiotropium bromidemonohydrate equivalent to 18 micrograms tiotropium. IndicationTiotropium is indicated as a maintenance bronchodilator treatmentto relieve symptoms of patients with chronic obstructivepulmonary disease (COPD). Dose Adults only age 18 years or over: Inhalation of the contents of one capsule once daily fromthe HandiHaler® device. Contra-indications Hypersensitivity totiotropium bromide, atropine or its derivatives, or to theexcipient lactose monohydrate which contains milk protein.Precautions Not for the initial treatment of acute episodes ofbronchospasm, i.e. rescue therapy. Immediate hypersensitivityreactions may occur after administration of tiotropium bromideinhalation powder. Caution in patients with narrow-angleglaucoma, prostatic hyperplasia or bladder-neck obstruction.Inhaled medicines may cause inhalation-induced bronchospasm.In patients with moderate to severe renal impairment tiotropiumbromide should be used only if the expected benefit outweighsthe potential risk. Patients should be cautioned to avoid gettingthe drug powder into their eyes. They should be advised that thismay result in precipitation or worsening of narrow-angleglaucoma, eye pain or discomfort, temporary blurring of vision,visual halos or coloured images in association with red eyes fromconjunctival congestion and corneal oedema. Should anycombination of these eye symptoms develop, patients shouldstop using tiotropium bromide and consult a specialist
immediately. Tiotropium bromide should not be used morefrequently than once a day. Spiriva capsules contain 5.5 mglactose monohydrate. Interactions Although no formal druginteraction studies have been performed tiotropium bromideinhalation powder has been used concomitantly with other drugswithout clinical evidence of drug interactions. These includesympathomimetic bronchodilators, methylxanthines, oral and inhaled steroids, commonly used in the treatment of COPD.The co-administration of tiotropium bromide with otheranticholinergic-containing drugs has not been studied and is therefore not recommended. Pregnancy and LactationNo clinical data on exposed pregnancies are available. Thepotential risk for humans is unknown. Spiriva should thereforeonly be used during pregnancy when clearly indicated. It isunknown whether tiotropium bromide is excreted in humanbreast milk. Use of Spiriva is not recommended during breastfeeding. A decision on whether to continue or discontinue breastfeeding or therapy with tiotropium bromide should be madetaking into account the benefit of breast feeding to the child and the benefit of tiotropium bromide therapy to the woman.Side-effects Common (≥1/100, <1/10): Dry mouth. Uncommon(≥1/1,000, <1/100): Dizziness, headache, taste disorders, visionblurred, cough, pharyngitis, dysphonia, rash, nausea, stomatitis,dysuria, urinary retention, gastrooesophageal reflux disease,atrial fibrillation, constipation. See SPC for other undesirableeffects. Events of unknown frequency not attributed to
tiotropium in clinical trials but considered to be adverse drugreactions: dehydration, dental caries, angioneurotic oedema,skin infection, skin ulcer, dry skin, joint swelling. An increase inanticholinergic effects may occur with increasing age. Pack sizesHandiHaler device and 30 capsules (3 blister strips); HandiHalerdevice plus 10 capsules (1 blister strip); 30 capsules (3 blisterstrips). Marketing authorisation number PA 775/2/1. Legalcategory POM Marketing Authorisation holder BoehringerIngelheim International GmbH, D-55216 Ingelheim am Rhein,Germany. For full prescribing information please see Summaryof Product Characteristics. Updated July 2009.
SPIRIVA has been developed by BoehringerIngelheim and is being co-promoted by Pfizer
Limited and Boehringer Ingelheim Limited.
Reference:1. SPIRIVA Summary of Product Characteristics. May 2010.
Prescribing Information (Ireland)SPIRIVA® (tiotropium)
Prescribe SPIRIVA® (tiotropium) and reduce the number of exacerbations in your COPD patients this winter1
NBCQ Date of preparation: August 2011 2011-SPI-033
SPI115 AD 297x210 AW_AW 26/08/2011 10:50 Page 1

3
Issue 5 Volume 2 September / October2009
ContentsThe Journal of the Irish Practice Nurses Association
Nursing in General Practice is published by GreenCross Publishing, 7 Adelaide Court, Adelaide Road, Dublin 2. Tel: 4189799 Fax: 4789449Email: [email protected]
EDITORMaura Henderson
CONSulTING EDITORSDarina lane and Ruth Morrow
COMMISSIONING EDITORJudith leavy
DESIGNERBarbara Vasic
PuBlISHERSGraham CookeMaura Henderson
DisclaimerThe views expressed in Nursing in General Practice are not necessarily those of the publishers, editor or editorial advisory board. While the publishers, editor and editorial advisory board have taken every care with regard to accuracy of editorial and advertisement contributions, they cannot be held responsible for any errors or omissions contained.
Issue 5 Volume 4 September/October 2011
*GreenCross Publishing is a recently established publishing house which is jointly owned by Graham Cooke and Maura Henderson.
© Copyright GreenCross Publishing 2011The contents of Nursing in General Practice are protected by copyright. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form by any means – electronic, mechanical or photocopy recording or otherwise – whole or in part, in any form whatsoever for advertising or promotional purposes without the prior written permission of the editor or publishers
1 edITOrIAl
5 NewS
12 Q ANd A Mary O’connor, National Honorary Treasurer
14 brANcH NewS
clINIcAl revIew
17 dePreSSION – SyMPTOMS, dIAgNOSIS ANd TreATMeNT
Alison lane
IN PrAcTIce
22 MulTIMOrbIdITy IN PrIMAry cAre PArT 1 Jane campion dr Mary byrne
clINIcAl revIew
26 cArINg fOr A PerSON wITH cySTIc fIbrOSIS yvonne Mcdonagh catherine Meagher
clINIcAl revIew
31 HeAdlIce – deTecTION, TreATMeNT ANd PreveNTION Sally whelan
IN PrAcTIce
34 NewS STANdArdS IN SPIrOMeTry TeSTINg Maria McNeil
AbSTrAcTS
37 fOcuS ON: dIAbeTeS
39 fOcuS ON: OSTeOPOrOSIS
43 PrOducTS
47 crOSSwOrd

Heel Balm
To receive trial products, samples and further information, please email [email protected]
Laderma Health (UK) Ltd. www.flexitol.com
n Contains 25% Urea in a highly concentrated, moisturising and emollient base
n Clinically tested to be more effective than creams containing 10% or less Urea 1
n Suitable for general and diabetic foot care in adults
n Effective treatment widely recommended by healthcare practitioners, including Podiatrists, Diabetes Specialists, Dermatologists GP’s and Nurses because it works!
1 Baird S.A., Skinner C.M., Trail S., Frankis J.S., 2002, ‘A study to compare the efficacy of the use of 10% Urea cream and 25% Urea cream on the control of Anhydrosis in the diabetic foot’, Glasgow Caledonian University, Glasgow.
The Medically Proven Treatment for Dry, Cracked Feet
BEFORE AFTER
LHINT Flexitol Ireland Heel Balm Nursing in General Practice Ad A4 P IRHBN-1.indd 1 15/03/11 1:07 PM

5
newsNEC NEWS
Nec MeeTINgS 2011Friday 14th October 2011 – Tullamore Court Hotel, Tullamore, Co Offaly – time to be confirmed.
IPNA webSITeThe IPNA website, www.irishpracticenurses.ie is updated constantly, so please log in regularly to get the latest news on study days, etc.
IPNA ANNuAl cONfereNce / AgM 2011• See IPNA website for conference registration forms and
programme.• Closing date for conference registrations is strictly Friday
30th September.• Members are encourage to book their conference place
as soon as possible because the educational part of the conference is being opened up to non-IPNA members this year – make sure you secure your place!
• Motions for AGM are available on the IPNA website.Contact lisa Nolan: Tel: 042-9692403 e-mail: [email protected]
coombe professor calls for fathers-to-be to take better care of health Professor Michael Turner from the Coombe Women and Infants university Hospital recently called for Irish fathers to take better care of their health by exercising more, by eating more healthily and by stopping smoking. Research from Dr Ross Kelly and his colleagues at the uCD Centre for Human Reproduction in the Coombe Women and Infants university Hospital (CWIuH) just published in an Australian journal found that one in six Irish fathers-to-be were obese. Half were also overweight and were likely to become obese as their children grow up.
Professor Michael Turner said “Obese fathers are more likely to get diabetes and heart disease, and they are more likely to die young. This is bad news not just for fathers but also for families if they are not able to care or provide for mothers and their children through ill health or death. Obese fathers are also 2-4 times more likely to have obese children. Fathers have a responsibility to their children as well as themselves to promote a healthy lifestyle for all the family. Obesity reverberates through the generations at great cost. We must all work to break this cycle of obesity.”
The main findings of this study are as follows:• Only 22% of couples were in the normal BMI category• Only one of three fathers-to-be had normal BMI• One in six fathers was already obese, increasing lifetime risks
such as diabetes which may affect his ability to support the family.This new research shows that paternal obesity is as common
as maternal obesity in Ireland but that men are twice as likely to be overweight. They also have more visceral fat, known more commonly as a ‘beer belly’, which is the fat that carries the highest risk of diabetes and heart disease. Also, 40% continue to smoke which also increases their risk of heart disease and cancer, as well as exposing their children to the risks of passive smoking.
Heel Balm
To receive trial products, samples and further information, please email [email protected]
Laderma Health (UK) Ltd. www.flexitol.com
n Contains 25% Urea in a highly concentrated, moisturising and emollient base
n Clinically tested to be more effective than creams containing 10% or less Urea 1
n Suitable for general and diabetic foot care in adults
n Effective treatment widely recommended by healthcare practitioners, including Podiatrists, Diabetes Specialists, Dermatologists GP’s and Nurses because it works!
1 Baird S.A., Skinner C.M., Trail S., Frankis J.S., 2002, ‘A study to compare the efficacy of the use of 10% Urea cream and 25% Urea cream on the control of Anhydrosis in the diabetic foot’, Glasgow Caledonian University, Glasgow.
The Medically Proven Treatment for Dry, Cracked Feet
BEFORE AFTER
LHINT Flexitol Ireland Heel Balm Nursing in General Practice Ad A4 P IRHBN-1.indd 1 15/03/11 1:07 PM
POM Further information is available from: MSD, Pelham House, South County Business Park, Leopardstown, Dublin 18, Ireland. Telephone: 01 299 8700
Marketing Authorisation Holder: Organon (Ireland) Ltd., P O Box 2857, Drynam Road, Swords, Co. Dublin.Date of preparation: June 2011
08-1
1-NU
V-20
10-IR
L-34
71-J

6
news
Nurses and GPs required to contribute in tackling obesityNurses and GPs throughout Ireland are invited to participate in the Weight Care Research Project. This all-Ireland project is led by researchers at the university of ulster and National university of Ireland, Galway who are conducting a survey of health professionals’ attitudes and assessment of body weight status.
The key project objectives are as follows: 1. To assess the attitudes, current practices/behaviours and
knowledge of key health professional groups of body weight status.
2. To assess the health professional groups’ ability to identify bodyweight categories in both adults and children. The health professional groups that are invited to
participate:• Public Health Nurses (community; postnatal home/clinic
visits and developmental checks);• Public Health Nurses (Schools);• GPs and Practice Nurses (primary care);• Occupational health nurses (workplace).
Nurses and GPs are required to participate in the following studies:1. Survey (mainly online but also paper-based; 10-15 mines) –
to determine the attitudes, current practices/behaviours and knowledge of health professionals of body weight status.
2. Online study (20-30 mins) – an online programme to assess health professionals’ ability to identify the body weight category of adults and children.If you participate in any of these studies, you will be part
of a valuable project, which will provide information on the attitudes, current practices/behaviours and knowledge of key health professional groups, and also their ability to identify body weight categories in both adults and children.
Ethical approval has been obtained for this project.If you would like further information on the Weight Care
Project or to discuss participating in any of the above studies, please contact the Weight Care Team using the following contact details: www.science.ulster.ac.uk/weightcareproject. E-mail: [email protected] Tel: +44 (0) 28 9036 8905
This September marks Heart Month and the Irish Heart Foundation is calling on Irish men to look after the most important motor they own, in a drive to reverse the worrying trend which sees five men under the age of 65 dying from heart attack every week. A new prevention campaign launched by the national charity fighting heart disease and stroke urges Irish men to take a different approach to their heart health. The campaign aims to reduce deaths from cardiovascular disease, the number one killer among men, and to save some of the hundreds of male lives that are lost prematurely here to heart attack every year.
‘A man’s guide to heart health’, a new manual published by the Irish Heart Foundation to mark Heart Month, urges men to compare their heart to the motor of their favourite car and recognise that in their lifetime it’s the most important engine that they’ll ever own.
Maureen Mulvihill, Health Promotion Manager at the Irish Heart Foundation explained: “like any motor, the heart needs to be fuelled properly and serviced regularly. You wouldn’t put diesel into a petrol engine, because it would break down, or leave your car not driven for years without expecting it to seize up. The same applies to the heart. For example, with 44% of men aged 51-64 overweight and 42% in this age group obese, this is clearly one part of their motor they are not taking care of. Across all ages, 7 in 10 Irish men are overweight or obese suggesting that being overweight has become the norm. This is despite the many risks for the heart and health, such as high blood pressure, high cholesterol and risk of Type 2 diabetes.
This September marks Heart month and the Irish Heart foundation is calling on Irish men to look after their hearts, with the launch of their new prevention booklet ‘A man’s guide to heart health’. The booklet will support the charity’s nationwide heart attack awareness campaign that was launched by westlife’s Nicky byrne and family. Pictured left to right, the byrne family: gillian gallagher, Nicky byrne, georgina byrne, yvonne byrne and Adam byrne.
Heart month targets men in bid to reduce heart attack mortality rates
Help close the gap to LDL-C goal in one step
According to the DYSIS* Ireland Survey 48% of patients with an ESC risk ≥5% are not achieving their LDL-C goal.1
FOR PATIENTS NOT CONTROLLED BY STATIN ALONE.
In patients with hypercholesterolemia, including patients with CHD and/or diabetes
EZETROL® ezetimibeABRIDGED PRODUCT INFORMATION Refer to Summary of Product Characteristics (SPC) before PrescribingPRESENTATION 10 mg Tablet containing 10 mg of ezetimibe. USES As adjunctive therapy to diet in: Primary hypercholesterolaemia: For co-administration with an HMG-CoA reductase inhibitor (statin) for patients with primary (heterozygous familial and non-familial) hypercholesterolaemia not appropriately controlled with a statin alone. Monotherapy: For use in patients with primary (heterozygous familial and non-familial) hypercholesterolaemia in whom a statin is considered inappropriate or is not tolerated. Homozygous Familial Hypercholesterolaemia (HoFH): For co-administration with a statin, for use in patients with HoFH. Patients may also receive adjunctive treatments (e.g. LDL apheresis). Homozygous sitosterolaemia (phytosterolaemia): For use in patients with homozygous familial sitosterolaemia. A beneficial effect of Ezetrol on cardiovascular morbidity and mortality has not yet been demonstrated. DOSAGE AND ADMINISTRATION For oral administration. Put patients on an appropriate lipid-lowering diet and continue during treatment. Recommended dose is one ‘Ezetrol’ 10 mg tablet daily, administered at any time of the day, with or without food. When added to a statin, either continue with the indicated usual initial dose of that particular statin or the already established higher statin dose. Consult the statin dosage instructions. Co-administration with bile acid sequestrants: Dosing should occur either ≥2 hours before or ≥4 hours after administration of a bile acid sequestrant. Use in paediatric patients: Initiation of treatment must be performed under review of a specialist. Adolescents ≥ 10 years): no dosage adjustment is required. The clinical experience in paediatric and adolescents patient (aged 10- 17 years old) is however limited. Children < 10 years: Ezetrol is not recommended due to insufficient data on safety and efficacy. Use in hepatic impairment. No dosage adjustment is required with mild hepatic insufficiency (Child Pugh score 5 to 6). Not recommended in patients with moderate (Child Pugh score 7 to 9) or severe (Child Pugh score >9) liver dysfunction. CONTRA-INDICATIONS Hypersensitivity to any component. When co-administered with a statin, refer to the SPC for that particular medicinal product. ‘Ezetrol’ co-administered with a statin during pregnancy and lactation. ‘Ezetrol’ co-administered with a statin in patients with active liver disease or unexplained persistent elevations in serum transaminases. PRECAUTIONS Liver enzymes: When co-administered with a statin, perform liver function tests at initiation of therapy and according to the SPC for that particular medicinal product. Skeletal muscle: In post-marketing experience with ‘Ezetrol’, myopathy and rhabdomyolysis have been reported. Most patients who developed rhabdomyolysis were taking a statin concomitantly with ‘Ezetrol. However, rhabdomyolysis has been reported very rarely with ‘Ezetrol’ monotherapy and very rarely with the addition of ‘Ezetrol’ to other agents known to be associated with increased risk of rhabdomyolysis. If myopathy is suspected based on muscle symptoms or is confirmed by a creatinine phosphokinase (CPK) level >10 times the ULN, immediately discontinue ‘Ezetrol’, any statin, and any of these other agents. Advise all patients starting therapy with ‘Ezetrol’ of the risk of myopathy and to report promptly any unexplained muscle pain, tenderness or weakness Hepatic insufficiency: Not recommended in patients with moderate or severe hepatic insufficiency due to the unknown effects of the increased exposure to ‘Ezetrol’. Fibrates: The safety and efficacy of co-administration have not been established. Fibrates may increase cholesterol excretion into the bile, leading to cholelithiasis. If cholelithiasis is suspected in a patient receiving ‘Ezetrol’ and fenofibrate, gallbladder investigations are indicated and this therapy should be discontinued. Ciclosporin: Exercise caution when initiating ‘Ezetrol’ in patients taking ciclosporin and monitor ciclosporin concentrations. Warfarin, another coumarin anticoagulant or fluindione: Monitor the International Normalised Ratio (INR) if taken together with ‘Ezetrol’. Excipient: ‘Ezetrol’ tablets contain lactose: do not use in patients with rare hereditary problems of galactose intolerance, Lapp lactase deficiency or glucose-galactose malabsorption. Interactions (studies have only been performed in adults): Cholestyramine: Concomitant cholestyramine administration decreased the mean AUC of total ‘Ezetrol’ approximately 55%. The incremental low-density lipoprotein cholesterol (LDL-C) reduction due to adding ‘Ezetrol’ to cholestyramine may be lessened by this interaction. Fibrates: Possible risk of cholelithiasis and gallbladder disease upon co-administration of fenofibrate with ‘Ezetrol’. Statins: No clinically significant pharmacokinetic interactions were seen upon co-administration with atorvastatin, simvastatin, pravastatin, lovastatin, fluvastatin, or rosuvastatin. Pregnancy and lactation: ‘Ezetrol’ co-administered with a statin is contra-indicated during pregnancy and lactation, refer to the SPC for that particular statin. Pregnancy: ‘Ezetrol’ should
be given to pregnant women only if clearly necessary. No clinical data are available on the use of ‘Ezetrol’ during pregnancy. Lactation: ‘Ezetrol’ is contra-indicated. Effects on ability to drive and use machines: No studies on the effects on the ability to drive and use machines have been performed. However, when driving vehicles or operating machines, it should be taken into account that dizziness has been reported. SIDE EFFECTS Refer to SPC for complete information on side effects. Clinical Studies In clinical studies where ‘Ezetrol’ was administered alone or with a statin or with fenofibrate, adverse reactions were usually mild and transient. The overall incidence of side effects was similar between ‘Ezetrol’ and placebo. Similarly, the discontinuation rate due to adverse experiences was comparable between ‘Ezetrol’ and placebo. The following common (≥1/100, <1/10) drug-related adverse experiences were reported in patients taking ‘Ezetrol’ (N=2396) and at a greater incidence than placebo (N=1159) or in patients treated with Ezetrol coadministered with a statin (N=11308) and at a greater incidence than statin administered alone (N=9361): or co-administered with fenofibrate: ‘Ezetrol’ administered alone: General disorders and administration site condition: fatigue. Gastro-intestinal disorders: abdominal pain, diarrhoea and flatulence. ‘Ezetrol’ co-administered with a statin: Investigations: ALT and/or AST increased. Nervous system disorders: headache. Musculoskeletal and connective tissue disorders: myalgia. ‘Ezetrol’ co-administered with fenofibrate: Gastrointestinal disorders: abdominal pain (common). Laboratory values. In controlled clinical monotherapy trials, the incidence of clinically important elevations in serum transaminases (ALT and/or AST ≥3 X ULN, consecutive) was similar between ‘Ezetrol’ (0.5%) and placebo (0.3%). In co-administration trials, the incidence was 1.3% for patients treated with ‘Ezetrol’ co-administered with a statin and 0.4% for patients treated with a statin alone. These elevations were generally asymptomatic, not associated with cholestasis, returning to baseline after discontinuation of therapy or with continued treatment. In clinical trials, CPK >10 X ULN was reported for 4 of 1,674 (0.2%) patients administered ‘Ezetrol’ alone vs 1 of 786 (0.1%) patients administered placebo, and for 1 of 917 (0.1%) patients co-administered ‘Ezetrol’ and a statin vs 4 of 929 (0.4%) patients administered a statin alone. There was no excess of myopathy or rhabdomyolysis associated with ‘Ezetrol’ compared with the relevant control arm (placebo or statin alone). In a study involving adolescent (10 to 17 years of age) patients with heterozygous familial hyperchlolesterolaemia (n = 248), elevations of ALT and/or AST (≥3X ULN, consecutive) were observed in 3% (4 patients) of the ezetimibe/simvastatin patients compared to 2% (2 patients) in the simvastatin monotherapy group; these figures were respectively 2% (2 patients) and 0% for elevation of CPK (≥ 10X ULN). No cases of myopathy were reported. This trial was not suited for comparison of rare adverse drug reactions. Post-marketing experience. The following additional adverse reactions have been reported in post marketing experience. Because these adverse experiences have been identified from spontaneous reports, their true frequencies are not known and cannot be estimated. Blood and lymphatic system disorders: thrombocytopaenia. Nervous system disorders: dizziness; paraesthesia. Respiratory, thoracic and mediastinal disorders: dyspnoea. Gastrointestinal disorders: pancreatitis; constipation. Skin and subcutaneous tissue disorders: erythema multiforme. Musculoskeletal and connective tissue disorders: myalgia; myopathy/rhabdomyolysis. General disorders and administration site conditions: asthenia. Immune system disorders: hypersensitivity, including rash, urticaria, anaphylaxis and angio-oedema. Hepatobiliary disorders: hepatitis; cholelithiasis; cholecystitis. Psychiatric disorders: depression. PACKAGE QUANTITIES 28 Tablets. Marketing Authorisation number: PA 1091/1/1. Marketing Authorisation holder: MSD-SP Limited, Hertford Road, Hoddesdon, Hertfordshire EN11 9BU, UK. Date of review: March 2010. ® denotes registered trademark of MSP Singapore Company, LLC © Merck Sharp & Dohme Limited, 2010 All rights reserved. Additional information is available on request or at www.medicines.ie. Legal Category: POM. API.EZE.(II/33) Reference: 1. Data on file. * DYSIS (The Dyslipidemia International Study) was a cross sectional multicentre epidemiological study of lipid levels of 22063 patients in Europe and Canada.
11-1
1-EZ
T-20
10-IR
L-38
98-J
Pelham House, South County Business Park, Leopardstown, Dublin 18, Ireland

8
news
Visit us at www.abbottnutrition.ie
More Taste, Less Waste.Ensure Plus –It’s the taste we love!
Ensure Plus -The preferred supplement1
Largest‡ ONS+ compliance studyn>1,700SUSTAIN study*
‡ No larger published study was identifi ed through literature reviews.
Largest ever blinded and randomised study investigating sensory factors, taste and compliance in oral nutritional supplements.+ Oral nutritional supplements.
* Study to improve Understanding of Sensory factors and Taste And their Impact on compliance with Nutritional drinks.
Reference available on request.
Abbott Laboratories Ltd., 4051 Kingswood Drive, Citywest Business Campus, Dublin 24Tel: (01) 4691500. Fax: (01) 4691501. Email: [email protected] of Preparation: June 2011 ANI/SIP/2011/021
ear care course – cherry OrchardPractice nurses attending the Ear Care Course held at Cherry Orchard Hospital on 22 August 2011.
The course is provided free of charge for practice nurses by the HSE through the Practice Development Co-ordinators at venues throughout the country. This one was facilitated by Rita lawlor.
The course is aimed at both experienced and new practice nurses to ensure uniformity and best practice in ear care.
Also in the photograph is Emma McAuley who presented Communication Tips and Hearing Aid Care and Information and was accompanied by Chester her Assistance Dog.
unique Health Identifiers – improves transparencyThe ability to identify the professionals and organisations who provide frontline services is a key requirement for a safe, transparent and accountable healthcare system.
The Health Information and Quality Authority has published Recommendations for unique Health Identifiers for Healthcare Practitioners and Organisations, which deals directly with this issue and presents guidance on the introduction of unique identifiers for healthcare practitioners and organisations in Ireland.
Speaking at the launch of the report, Professor Jane Grimson, Director of Health Information with HIQA said: “We have previously recommended the introduction of unique identifiers for individuals so that high quality and reliable healthcare which ensures maximum patient safety can be ensured. However, equally important is a national system for uniquely identifying healthcare practitioners and organisations.”
“under the proposed system, every health and social care practitioner in Ireland will be assigned a unique number, known as the Health Practitioner Identifier (HPI) which will follow them throughout the course of their career irrespective of whether they change post or move to a new location. Similarly, each health and social care organisation will be allocated a unique number known as the Healthcare Organisation Identifier (HOI).”
“HIQA is recommending that the upcoming Health Information Bill specifically legislates for the introduction of these identifiers through the establishment of a central directory or database which will act as a single authoritative reference point.” said Professor Grimson.

Visit us at www.abbottnutrition.ie
More Taste, Less Waste.Ensure Plus –It’s the taste we love!
Ensure Plus -The preferred supplement1
Largest‡ ONS+ compliance studyn>1,700SUSTAIN study*
‡ No larger published study was identifi ed through literature reviews.
Largest ever blinded and randomised study investigating sensory factors, taste and compliance in oral nutritional supplements.+ Oral nutritional supplements.
* Study to improve Understanding of Sensory factors and Taste And their Impact on compliance with Nutritional drinks.
Reference available on request.
Abbott Laboratories Ltd., 4051 Kingswood Drive, Citywest Business Campus, Dublin 24Tel: (01) 4691500. Fax: (01) 4691501. Email: [email protected] of Preparation: June 2011 ANI/SIP/2011/021

10
news
New podiatry service in KerryThe HSE has announced the commencement of a podiatry service in Co Kerry. In conjunction with the Diabetic Association of Ireland, the HSE has appointed two senior podiatrists this summer, marking the first phase of the new service.
The podiatry service will provide a combination of education, screening, evaluation and intervention, with the ultimate aim to prevent, reduce or delay the progression of foot related complications associated with some chronic diseases. low risk clients will continue to be managed by public health nurses, GPs and practice nurses while some very high risk clients maybe referred to the podiatry team in Cork university Hospital and South Infirmary Victoria university Hospital.
The podiatrists will enhance the existing diabetic service in Kerry, which has been developed in recent years with the provision of three dedicated consultant led diabetic clinics held monthly at Kerry General Hospital and 28 specialist diabetic nurse-led outpatient clinics monthly held in communities throughout the county.
Jan cumiskey, Podiatrist, Kerry community Services with dr Tom Higgins, consultant Physician, Kerry general Hospital and Helen crowley, diabetes Nurse Specialist, Kerry general Hospital at the announcement of the new podiatry service for Kerry.
National bowls tournament for older peopleActive Retirement Ireland recently announced details of its second annual National Bowls Tournament that will see more than 400 retired men and women participate. The tournament will take place from Monday, 26th – Thursday, 29th September in the Breaffy Events Arena in Castlebar, Co. Mayo.
During the tournament, 49 teams will compete for the Breaffy Perpetual Cup. Playing in mixed teams of four, competitors, who range in age from 55 to 90, will play against fellow Active Retirement members from all over the country for three days, with separate competitions for big bowls and small.
According to Maureen Kavanagh, Chief Executive of Active Retirement Ireland, the National Bowls Tournament presents a welcome opportunity for retired people to stay active through the medium of a fun and competitive activity.
“This is the second year we are organising the tournament, and judging on the response we have had so far, the event is becoming more and more popular. With almost 450 people already registered to attend, it has become one of the main events in our members’ calendar.
“In the past 18 months, we have observed a notable increase in the number of Active Retirement Associations taking up bowls as a key activity, with many associations instigating their own tournaments within their county or region.
“Bowls is of special importance in promoting a healthy lifestyle among our membership, as it’s a sport that people of almost any age can participate in, regardless of physical ability. One of the objectives of our national tournament is to promote the sport generally and more specifically to encourage more men to remain active during their retirement years. Research and anecdotal evidence from Ireland and across the western world shows that men are less likely than women to remain active once they have retired. Events like these can greatly help to combat isolation and depression among men, as well as helping to keep them physically active.
Active Retirement Ireland is the national representative body for 527 Active Retirement Associations, with a total membership of over 22,500 people.
For further information visit www.activeirl.ie
Practice nurse ear care course – Pearse StreetAn ear care course for practice nurses was held recently at Pearse Street Health centre in dublin. The course was facilitated by rita lawlor (Pdc) and is part of the national programme to ensure best practice in ear care for practice nurses.

Cialis offers your patients
CIALIS* (TADALAFIL) REPUBLIC OF IRELAND ABBREVIATED PRESCRIBING INFORMATION
Presentation Tablets 2.5mg, 5mg, 10mg, or 20mg of tadalafil. Also contains lactose. Uses Treatment of erectile dysfunction in adult males. Dosage and Administration Adult men: The recommended dose is 10mg orally, taken at least 30 minutes prior to sexual activity. In those patients in whom tadalafil 10mg does not produce an adequate effect, 20mg might be tried. Maximum dosing frequency, once per day. 10mg or 20mg tadalafil is not recommended for continuous daily use. In patients who anticipate a frequent use of Cialis (ie, at least twice weekly), a once daily regimen with the lowest doses of Cialis might be considered. The recommended dose is 5mg taken once a day at approximately the same time of day. The dose may be decreased to 2.5mg once a day based on individual tolerability. The appropriateness of continued use of the daily regimen should be reassessed periodically. Elderly: Dosage adjustment not required. Impaired renal or hepatic function: In patients with severe renal impairment the maximum recommended dose is 10mg. Once a day dosing of Cialis is not recommended in patients with severe renal impairment. In men with hepatic impairment the recommended dose is 10mg. There are no available data about the administration of doses higher than 10mg of tadalafil to patients with hepatic impairment. There is limited clinical data on the safety of Cialis in patients with severe hepatic impairment; if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Once a day dosing has not been evaluated in patients with hepatic impairment; therefore, if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Diabetes: Dosage adjustment not required. Use in children and adolescents: Cialis should not be used in individuals below 18 years of age. Not indicated for use by women. In clinical trials, Cialis demonstrated improvement in patients’ erectile function and the ability to have successful sexual intercourse up to 36 hours following dosing. Contra-indications Known hypersensitivity to any ingredient. Patients using any form of organic nitrates. In men with cardiac disease for whom sexual activity is inadvisable. Physicians should consider the potential cardiac risk of sexual activity in patients with pre-existing cardiovascular disease. Patients with myocardial infarction within the last 90 days, patients with unstable angina or angina occurring during sexual intercourse, patients with New York Heart Association class 2 or greater heart failure in the last 6 months, patients with uncontrolled arrhythmias, hypotension (<90/50mmHg), or uncontrolled hypertension, patients with a stroke within the last 6 months. Cialis is contra-indicated in patients who have loss of vision in one eye because of non-arteritic anterior ischaemic optic neuropathy (NAION), regardless of whether this episode was in connection or not with previous PDE5 inhibitor exposure. Warnings and Special Precautions Prior to any treatment for erectile dysfunction, physicians should consider the cardiovascular status of their patients, since there is a degree of cardiac risk associated with sexual activity. Tadalafil has vasodilator properties, resulting in mild and transient decreases in blood pressure. It augments the hypotensive effect of nitrates. Tadalafil (2.5mg and 5mg): In patients receiving concomitant antihypertensive medicines, tadalafil may induce a blood pressure decrease. When initiating daily treatment with tadalafil, appropriate clinical considerations should be given to a possible dose adjustment of the antihypertensive therapy. Serious cardiovascular events were reported either post-marketing and/or in clinical trials. Although most of the patients in whom these events have been observed had pre-existing cardiovascular risk factors, it is not possible to determine whether these events are related directly to these risk factors, to Cialis, to sexual activity, or to a combination of these or other factors. Visual defects and cases of NAION have been reported in connection with the intake of Cialis and other PDE5 inhibitors. In case of sudden visual defect, patients should be advised to stop taking Cialis and consult a physician immediately. Due to increased tadalafil exposure (AUC), limited clinical experience, and the lack of ability to influence clearance by dialysis, once a day dosing of Cialis is not recommended in patients with severe renal impairment. There is limited clinical data on the safety of single-dose administration of tadalafil in patients with severe hepatic insufficiency (Child-Pugh class C); if prescribed, a careful individual benefit/risk evaluation should be undertaken by the prescribing physician. Use with caution in patients who have conditions that might predispose them to priapism, or in patients with anatomical deformation of the penis. Patients who experience erections lasting 4 hours or more should be instructed to seek medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of
potency may result. It is not known if Cialis is effective in patients who have undergone pelvic surgery or radical non-nerve-sparing prostatectomy. Cialis should not be administered to patients with hereditary problems of galactose intolerance, the Lapp lactase deficiency, or glucose-galactose malabsorption. In patients who are taking alpha1-blockers, concomitant administration of Cialis may lead to symptomatic hypotension in some patients. The combination of tadalafil and doxazosin is not recommended. Caution should be exercised when prescribing Cialis to patients using potent CYP3A4 inhibitors (ritonavir, saquinavir, ketoconazole, itraconazole, and erythromycin) as increased tadalafil exposure (AUC) has been observed if the drugs are combined. The safety and efficacy of combinations of tadalafil and other PDE5 inhibitors or other treatments for erectile dysfunction have not been studied. Patients should be informed not to take Cialis with such combinations. Pregnancy and Lactation Not indicated for use by women. There are limited data from the use of tadalafil in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to pregnancy, embryonal/foetal development, parturition, or postnatal development. As a precautionary measure, it is preferable to avoid the use of Cialis during pregnancy. Available pharmacodynamic/toxicological data in animals have shown excretion of tadalafil in milk. A risk to the suckling child cannot be excluded. Cialis should not be used during breast-feeding. Driving, etc No studies on the effect on the ability to drive and use machines have been performed. Although the frequency of reports of dizziness in placebo and tadalafil arms in clinical trials was similar, patients should be aware of how they react to Cialis before driving or operating machinery. Undesirable Effects Very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), and not known (events not reported in registration trials cannot be estimated from post-marketing spontaneous reports). Very common: Headache. Common: Dizziness, flushing, dyspepsia, nasal congestion, back pain, myalgia. Uncommon: Hypersensitivity reactions, blurred vision, sensations described as eye pain, tachycardia, palpitations, hypotension (more commonly reported when tadalafil is given to patients who are already taking antihypertensive agents), hypertension, abdominal pain, gastro-oesophageal reflux, rash, hyperhidrosis (sweating), chest pain(1). Rare: Stroke(1) (including haemorrhagic events), syncope, transient ischaemic attacks(1), migraine(3), visual field defect, swelling of eyelids, conjunctival hyperaemia, myocardial infarction, urticaria, Stevens-Johnson syndrome(3), exfoliative dermatitis(3), prolonged erections, priapism(3), facial oedema(3), seizures, transient amnesia, NAION(3), retinal vascular occlusion(3), sudden hearing loss(2), unstable angina pectoris(3), ventricular arrhythmia(3), epistaxis, sudden cardiac death(1, 3). (1)Most of the patients in whom these events have been reported had pre-existing cardiovascular risk factors. (2)Sudden decrease or loss of hearing has been reported in a small number of post-marketing and clinical trial cases with the use of all PDE5 inhibitors, including tadalafil. (3)Post-marketing surveillance reported adverse reactions not observed in placebo-controlled clinical trials. Adverse reactions reported with tadalafil were transient, and generally mild or moderate. Adverse reaction data are limited in patients >75 years. A slightly higher incidence of ECG abnormalities, primarily sinus bradycardia, has been reported in patients treated with tadalafil once a day as compared with placebo. Most of these ECG abnormalities were not associated with adverse reactions. For full details of these and other side-effects, please see the Summary of Product Characteristics, which is available at http://www.medicines.ie/. Legal Category POM Marketing Authorisation Numbers and Holder EU/1/02/237/001 EU/1/02/237/002 EU/1/02/237/003 EU/1/02/237/004 EU/1/02/237/005 EU/1/02/237/006 EU/1/02/237/007 EU/1/02/237/008. Eli Lilly Nederland BV, Grootslag 1-5 3991, RA Houten, The Netherlands. Date of Preparation or Last Review March 2011. Full Prescribing Information is Available From Eli Lilly and Company Limited Lilly House, Priestley Road Basingstoke, Hampshire, RG24 9NL. Telephone: Basingstoke (01256) 315 000 E-mail: [email protected] or Eli Lilly and Company (Ireland) Limited Hyde House, 65 Adelaide Road, Dublin 2, Republic of Ireland. Telephone: Dublin (01) 661 4377. E-mail: [email protected]. *CIALIS (tadalafil) is a trademark of Eli Lilly and Company. Date of Preparation: September 2010. Date of Revision: March 2011 References: 1. Cialis Summary of Product Characteristics. 2. Dean, J. et al. Psychosocial outcomes and drug attributes affecting treatment choice in men receiving sildenafil citrate and tadalafil for the treatment of erectile dysfunction: Results of a multicenter, randomised, open label, crossover study. J Sex Med, 2006; 3:650-661. IECLS00172
Proven efficacy from 30 minutes up to 36 hours with sexual stimulation1
Greater sexual self-confidence and spontaneity than sildenafil2
A4 Young Couple new AP.indd 1 12/09/2011 16:21

12
Q&A
why did you decide to become a nurse?My career choices when I left school were a lot more limited than now. Civil service, bank, nursing or teaching. I wanted to know how to deliver a baby, so nursing was my obvious choice. I also had three Aunts who nursed in England after World War II. Their experiences were amazing; immunisation was in its infancy and parents had the same fears as they do today; fear of the unknown, refusing to allow their children be vaccinated – one case resulted in twin babies dying of diphtheria.
where did you train?I did my general training in the Meath Hospital (part of it was the former home of Dean Jonathan Swift ) in Heytesbury St, Dublin. The Meath closed down and amalgamated with the Adelaide Hospital and relocated to Tallaght where a brand new hospital was constructed. I qualified in Midwifery in the Coombe Hospital in Dublin. Midwifery was a marvellous experience.
what was your first job after qualifying?For family reasons it was necessary for me to move closer to home – longford – so I was lucky to get my first job in the General Hospital, Mullingar, Co Westmeath. I met some fantastic people there.
what is your proudest achievement?My four children have to be my proudest achievement. Ruth (16 yrs ), Eleanor (14 yrs), John (12 yrs), David (10 yrs) certainly keep me on my toes.
who would you consider your hero?Nelson Mandela and the Dalai lama spring immediately to mind but on further reflection it has to be the unsung heroes of the voluntary organistions, at home and abroad, who work tirelessly helping those less fortunate; especially those who go to some of the most inhospitable places stricken with war or natural disasters. They do not receive the accolades or publicity they deserve.
Is there anyone you would consider a villain?I would have to use the word villain for the inept people working in the political, financial and regultatory establishments that facilatated the current economic meltdown in this country. They have brought such devastation and heartbreak to so many people. But the Irish are resilient and we will recover.
what’s the best thing about practice nursing?I love it because it’s so varied. Through time you discover your special interests e.g. diabetes, women’s health and now it is possible to access education to enchance and build on your knowledge. The camaraderie among my colleagues is great. It is great to know that help or advice is only a phone call away.
Is there a single piece of advice that you would consider important to a new practice nurse?Join the IPNA – the Association has been very good to me. When I first became a practice nurse 17 years ago our only education was through our meetings and AGM. How things have progressed. Most of us work in isolation and it’s fantastic to have the support of your colleagues and lisa (Administrator) and Tracey (Membership Secretary) are only a phone call or email away. No need to mention the social occasions!
by the time this goes to print you will have handed over your role as honorary national treasurer to your successor, have you any advice for him/her? I have been Honorary Treasurer for the past two years. This past year has certainly been challenging. In financial terms the old saying “cut your cloth to your measure” has proven very apt. But I firmly believe that change, though often diffcult, can be a very postive experience. IPNA is a new organisation and we are on a learning curve. 2012 should bode very well for the IPNA.
what’s next for Mary O’connor?To quote a poet “to stop and stare” is my next goal. No more meetings in Dublin, only shopping trips I hope. My children and husband will have my undivided attention. I intend to peruse the educational booklet sent by Kathy McSharry (Western PDC). Oh and sign on for pilates, aqua aerobics, bridge, golf, etc.
Mary O’connor, National Honorary Treasurer, IPNAMary O’Connor was elected to the role of National Honorary Treasurer in 2009. She has also served as secretary and NEC rep in her local Mayo branch for 4 years.
Originally from longford, Mary has been a practice nurse for the past 17 years. She is RN and RM and was accredited CNS in primary healthcare.
Her special areas of interest are diabetes, women’s health and travel medicine. She has diplomas in women’s health (RCSI) asthma (Bradford) and in tropical nursing (RCSI).
Mary spent several years living and working in Australia and travelling in Asia and prior to settling in the West of Ireland she worked in travel health in the the Royal College of Surgeons.
She is Chairperson of the Claremorris Primary Care Team.Mary is actively involved in her local community in Claremorris and is
currently vice chair of Clar IRD, as well as director of Clar ICH, a voluntary housing association delivering services to the elderly throughout South West Mayo.
She is married with four children and her interests include walking, cooking and reading.

Abdominal Distension bothering your IBS patients?
The sensation of abdominal swelling (bloating) and the physical increase in girth size (distension) are troublesome features of Irritable Bowel Syndrome (IBS). Abdominal bloating is often ranked the most troublesome symptom for patients with IBS, being reported by up to 96% of patients1-6. It has been found that approximately half of these patients reporting the sensation of bloating actually exhibit an increase in girth size7.
Abdominal Bloating & Distension in IBS patients
A number of studies have demonstrated that Activia® helps reduce digestive discomfort8-11. Benefits have been demonstrated in healthy populations with various degrees of digestive discomfort. An IBS population group was used as a model to assess the effect of Activia®
on Gastrointestinal (GI) discomfort in some of these studies8,10. One of these studies, a randomised, controlled, double-blind parallel study of 34 women (20-69 years) with constipation predominant IBS, who consumed 2 x 125g servings of either Activia®* (n=17) or a non fermented dairy product (n=17) daily for 4 weeks demonstrated the following8:
Danone Activia® helps reduce Digestive Discomfort
78% reduction in the median change in maximal distension**†¤
Improved colonic** and orocaecal** transit time
Overall improvement in IBS symptom severity**
Figure 1: Comparison of the mean hourly abdominal distension measurements over the awake hours of the measurement after consuming the test product and control product
MEA
N D
ISTE
NSI
ON
(CM
)
HOURS
6
5
4
3
2
1
1 2 3 4 5 6 7 8 9 10 11 12 13
Danone Activia® groupControl group
Abdominal Distension Measurements
† Measured using a recently validated technique of Abdominal Inductance Plethysmography (AIP), based on the principle that a loop of inductance wire is stitched into a soft belt, worn by the patient and this then measures changes in girth size throughout the day. ¤ Change in maximal distension refers to the median percentage change between the final distension measurements taken before (day 0) consumption of Activia® versus after (day 27), in the Activia® group.* Activia® is a probiotic food containing the exclusive probiotic culture Bifidobacterium lactis DN 117 010 (Bifidus ActiRegularis®) which should be consumed as part of a healthy balanced diet and lifestyle.** p=<0.05.
References: 1Manning AP et al. (1978) BMJ 2, 653-654. 2Maxton DG et al. (1989) BMJ 99, 1138. 3Schmulson M et al. (1999) Am J Gastroenterol 94, 2929-2935. 4Lee O-Y et al. (2001) Am J Gastroenterol 96, 2184-2193. 5Chang L et al. (2001) Am J Gastroenterol 96, 3341-3347. 6Hungin APS et al. (2003) Aliment Pharmacol Ther 17, 643-650. 7Houghton LA (2006) Gastroenterology 131, 1003-1010. 8Agrawal A et al. (2008) Aliment Pharmacol Ther 29(1), 104-114. 9Guyonnet D et al. (2009) BJN 22, 1-9. 10Guyonnet D et al. (2007) Aliment Pharmacol Ther 26(3), 475-486. 11Guyonnet D et al. (2009) J Digest Dis 10, 61-70.
Untitled-1 1 05/05/2011 09:39

14
NEWS FOR IPNA BR ANCHES COuNTRY WIDEregional news
cOrKElAINE GOGGIN
We in the Cork Branch would like to take this opportunity to welcome everyone back after the summer break. We hope everyone is recharged and looking forward to our monthly meetings.
Our next meeting coincides with our summer outing at Fota Island Resort, Cork on Saturday, 10th September. This is kindly spon-sored by Ingrid Deutrom from Kora Healthcare and our guest speaker is Dr Teresa Bennett from the HSE who will talk to us about the vitamin D policy in the under 12 mths age. This meeting begins at 11.45 and will be followed by lunch at 1.00 (kindly sponsored by Ingrid). Members and non member practice nurses are welcome to this. Our branch meeting will take place afterwards for mem-bers.
Our October meeting is on Wednesday 5th October in Rochestown Park Hotel at 7.30, sponsored by Cathy O’Sullivan from Astra Zenica and guest speaker is Fiona Barton, CNS cardiovascular disease.
We are also looking forward to the IPNA National Conference in Tullamore in October and wish the South Tipperary branch our very best wishes. We look forward to the continued support from our members for the forthcoming year.
dONegAlElSIE STEWART
The Radisson Hotel, letterkenny, was the venue for the branch’s May meeting. The evening was very kindly sponsored by Petra O’Connell, MSD and proved to be very informative and interactive. liz Healy, a practice nurse working in Dublin, facilitated a first class presentation on the Implanon NXT implant device. liz’s presentation incorporated a training workshop and protocols used for insertion of the device in a nurse led clinic within her own GP practice. The beautiful setting of Castlegrove House Hotel was the venue for the June meeting at which Dr Martin Coyne gave an update on recent osteoporosis treatment, in particular on the six monthly injections of Prolia. Sincere thanks to Irene Walsh, who kindly sponsored the evening.
Following the summer break, the branch is due to met in September; date and venue to be arranged. It is hoped that this meeting will take the form of an AGM to formulate the election of a new branch committee.
As I will be stepping down as branch chairperson, I would like to take this opportunity to thank most sincerely my fellow committee members, lorraine Porter, secretary, Helen Mc laughlin, treasurer, for all their support and hard work over the past number of years and to wish the incoming committee every success.
On behalf of the Donegal branch I wish the South Tipperary Branch huge success on the upcoming IPNA Conference and AGM in Tullamore. The conference provides a great opportunity to network with the drug companies and to catch up with old friends while making new ones. Your support is vital to secure, not only the success of this year’s conference, but also that of years to come.
KIlKeNNy lEONIE FINNEGAN
Hello to all from the Kilkenny branch and trusting you all enjoyed the summer break. looking forward to seeing Kilkenny Branch members later this month before the onset of the hectic flu season! We are resuming our sessions this autumn with our initial meet-ing planned for September 28th in Pembroke Hotel with John leahy speaking on the topic of addiction and substance abuse. This education session is sponsored by lisa Dunworth on behalf of Johnson & Johnson.
We would also encourage PNs to support this year’s National Conference, and we hope to see many of you in Tullamore next month for the education and networking opportunities on offer.
weXfOrd JuNE D’ARCY
Hope this finds you all well. An update on our recent meetings: our March meeting covered the topic of hypertension and renal disease, and was most informative. In April, our speaker Ms Colette Blake spoke about urodynamics, bladder training and the unit/services available in Wexford General Hospital; again an excellent talk. The topic for our meeting in May was colposcopy and the colposcopy nurses from Wexford General Hospital informed and advised us regarding access to same, and the whole process involved. We are very fortunate to have such a high calibre of professionals, who are both approachable and accessible, attached to our local referring hospital.
We look forward to meeting up with our colleagues in October at the conference and wish the South Tipperary Branch every suc-cess.

15
rectuitment
Practice Nurserequired
glasnevin, dublin 9
Computerised, urban, five doctor practice seeks PN from November 2011. Duties include: immunisation, smear taking, phlebotomy and assisting with patient enquiries. The post is morning only, initially, 8.00am to 12 noon, 5 days per week.
Please email CV to:
Deadline for receipt is 1st October 2011.
Informal enquiries to: Dr John Burbridge 01 8373611 (9 to 5).
Practice NurseRequired
Bray, Co Wicklow
Practice nurse required for three doctor practice in BrayOne to two days per week initially.Please forward CV to:Duncairn Medical Centre9 Duncairn Terrace, Bray, Co WicklowOr phone: 01 2863812
experienced Practice Nurse
requireddublin 8
Friendly, busy GP practice in Dublin 8 requires experienced practice nurse for Maternity leave cover from mid-October 2011. 28 hours per week. Experience in phlebotomy essential. Fully computerised office (Socrates).
Please email CV by 26th September 2011 to:
Jennifer leeTalent Acquisition Specialistdiageo
email: [email protected]
Part-time practice nurse required for General Practice in Celbridge, Co. Kildare. 12-15 hours/week to include Monday, Wednesday and Friday morning and possibly one afternoon session.
Duties to include cervical screening, phlebotomy, immunisation, other practice nursing and associated administrative duties. Experience essential. Midwifery an advantage. Health One software.
Please apply with CV to Email: [email protected]
www.yourmedicines.ie
To advertise with us please contact yvonne Kiernan on 01 4189799 or at [email protected]

16
clinical review
Depression has been around for as long as records have been kept. It was first named as a condition about 2,400 years ago by Hippocrates, who called it melancholia. It is worth noting that depression is no respecter of fame or fortune – King Solomon, Abraham
lincoln and Winston Churchill all suffered from depression.GPs and practice nurses are well aware of the importance of an
awareness of depression, both in terms of its prevalence and the distress it causes to sufferers and their families. In general practice an increasing number of consultations are related to mental health, many of which can be managed within the primary care setting itself. In some cases a referral to a multi-disciplinary team specialising in mental health is the appropriate route (such as provided by the Dean Clinic).
Primary careThis article outlines a brief understanding of depression, causes, signs and symptoms and suggested treatment options. This may be useful to those working in primary care, which is often the first point of contact for the client suffering from depression. The recognition by a primary health carer that someone is suffering from mental ill health may be the patient’s first step on the road to recovery. A recent study into mental health attitudes in Ireland found that while 85% of people feel that mental health problems can affect anyone, 62% would not want anyone to know if they themselves had a problem (Shine, 2011). Stigma can prevent or make people extremely reluctant to seek help and support which means vigilance at primary care level is vital.
Depression – symptoms, diagnosis and treatmentAlISON lANe, COuNSEllOR/PSYCHOTHERAPIST, DEAN ClINIC, CORK
Depression is estimated to affect over 350 million people worldwide and in Ireland one in four people will experience it at some time in their life. According to the WHO, by 2020 depression will be the second leading contributor to the global burden of disease.

17
clinical review
definitionFirstly it is important to make the distinction between ‘dips in mood’ and a depressive illness. Dips in mood and feeling fed up or low are a familiar part of day-to-day life and usually happen in response to a particular circumstance. Often the term ‘I’m a bit depressed’ is used in everyday language but as we know, this does not mean depression in the diagnostic sense, instead describing a feeling of low mood which is not pervasive and importantly usually lasts a relatively short time. When sadness or feelings of depression occur – sometimes for no apparent reason – when those feelings last longer (more than 2 weeks) and are more intense, and interfere with day-to-day functioning, a diagnosis of clinical depression may be made.
Depression can vary in terms of onset (acute or gradual) and the stage of life at which it occurs. The severity of symptoms may vary considerably, and are usually classified as mild, moderate or severe. Duration is another variable, as is the frequency with which someone may experience depression.
causes and manifestationThe main causes of depression include biological and genetic factors, difficult early life experiences, social circumstances and the personality of the individual. Depression can be understood as the effect stress has on specific vulnerabilities in an individual’s biological make-up, their personality and social circumstances.
Depression affects many areas of ones life. Dr Chris Williams (2002) suggests this is seen clearly by examining five areas –• life situation, relationships, practical problems and
difficulties• Altered thinking• Altered emotions (moods/feelings)• Altered physical feelings, symptoms• Altered behaviour/activity levels
What a person thinks about a situation or problem may affect how they feel physically and emotionally, and also alters what they do (behaviour and activity). Each of the five areas interacts and impacts each other.
The following is a list (not exhaustive) of some of the symptoms that may be experienced by someone with depression.• unhappy most of the time (maybe slightly better in the
evenings).• loss of interest in day-to-day life• No pleasure in anything• Harder to make decisions
• Can’t cope with things in the usual way• utterly tired, not relieved by sleep• Restless and agitated• lose appetite and weight (or the reverse)• Sleep disturbance (taking longer fall asleep, can’t stay asleep,
waking earlier).• loss of interest in sex• loss of self-confidence• Feelings of uselessness, inadequacy, hopelessness• Avoidance of friends, family, social occasions• Irritability, anger• Intensity of feelings at a particular time of day, often the
mornings• Thoughts of self-harm or suicide.
Dr Tony Bates called depression, “a thief that steals from people; it robs them of their energy, vitality, self-esteem and any pleasure they may previously have enjoyed” (1999). Emotions seem to be affected particularly by a central symptom called ‘anhedonia’. This is derived from the greek language and means ‘without pleasure’. Anhedonia means the loss of capacity or ability to experience pleasure. Depression affects motivation to do things. A person can feel tired and sluggish with little interest in doing anything.
Depression also affects cognition (thinking) in two ways – it can impair concentration and memory and it can also manifest itself in terms of a person’s thinking style. Our thinking style determines much of how we see ourselves and the world around us. One of the key factors in identifying that someone has become depressed is recognising a change, in the way they are thinking, feeling or acting. Generally the depressed person will see themselves and often the world, in a negative way. They may describe feelings of worthlessness, loneliness and pessimism.
Key points
• Counselling/psychotherapy has been found to be effective and in particular, cognitive-behavioural therapy (CBT).
• CBT is an evidence-based and structured form of psychotherapy that aims to alter the unhelpful thinking patterns (cognitions) and behaviours that are part of depression.
• It is fully compatible with medication and studies have shown that use of CBT withanti-depressant medication is more effective than either treatment alone.
• According to NICE (National Institute for Health and Clinical Excellence) the guidelines recommend CBT as first-line treatment for mild depression, and they recommend anti-depressant medication alongside CBT for severe depression.
• It has also been shown that use of CBT leads to a reduction in relapse rates. (Williams 2002).
Thinking patternsThe following are some examples of unhelpful thinking styles;• Negative opinion of yourself – “I’m no good at anything”• Self-criticism and self-blame – “It’s all my fault” “I’m not
worthy of this”• Negative interpretation of events – “Everything is difficult
for me”• Mind-reading – assuming we know what others are
thinking. “He thinks I’m useless”.• emotional reasoning – “I feel bad so it must be bad” (I feel
anxious therefore I must actually be in danger)
It is fully compatible with medication and studies have shown that use of cbT with anti-depressant medication is more effective than either treatment alone.

18
clinical review
• Judgements – making evaluations or judgements about ourselves, events, others, the world, rather than taking a step back to look at the ‘evidence’
• Over-generalising – “last week was awful, nothing went right”
• extreme statements or rules – “It must be perfect, anything less means failure”
• catastrophising – imagining and believing that the worst possible thing will happen.
• Shoulds and musts – Thinking or saying “I should” or “I must” creates added pressure and unrealistic expectations.
There are some important factors to be aware of about negative thoughts. They tend to be automatic – not actually based on reason or logic but on the low opinion the depressed person has of themselves. The negative thoughts are unreasonable and serve no useful purpose. Discussing these thoughts with a trained healthcare professional will help to highlight this. Importantly, even though the thoughts are unreasonable, they often seem perfectly plausible and believable to the person themselves. Finally, the more a person believes these negative thoughts and accepts them as facts, the more depressed they will feel. (Beck & Greenberg). Cognitive Behaviour Therapy (CBT) challenges and addresses this.
TreatmentMedication The emotional centre of the brain is a particularly intricate system of inter-connecting nerve cells called the limbic system. Here messages from the outside world and memory interact to stimulate feelings. The smooth control of feelings is dependent upon adequately functioning nerve cells and proper amounts of chemical messengers. Extensive research into the chemistry
of moods suggests that two neurotransmitters are particularly affected – serotonin (5HT) and noradrenaline (McKeon, 1995). Anti-depressants increase concentrations of these two chemicals at the nerve endings and so seem to boost the function of those parts of the brain that use serotonin and noradrenaline. There are different groups of anti-depressant medication, the newer ones being SSRIs (selective serotonin re-uptake inhibitors). There are side-effects with anti-depressants and it is important to make a client aware of these. While generally not addictive, it is unwise to abruptly stop taking this type of medication as this can cause discontinuation effects, such as anxiety.
Talking therapyTalking therapy can play a very important role in enabling a person to live well, develop an understanding of themselves and their symptoms, to work towards living the life they want to live. The therapeutic relationship can provide a safe place and space to work through various issues, ensuring a person is ‘heard’.
The length and type of the counselling/psychotherapy process varies with each individual. There are many different types of talking therapy for people with mild or moderate depression.
Counselling/psychotherapy has been found to be effective and in particular, cognitive-behavioural therapy (CBT). CBT is an evidence-based and structured form of psychotherapy that aims to alter the unhelpful thinking patterns (cognitions) and behaviours that are part of depression. It is fully compatible with medication and studies have shown that use of CBT with anti-depressant medication is more effective than either treatment alone. According to NICE (National Institute for Health and Clinical Excellence) the guidelines recommend CBT as first-line treatment for mild depression, and they

19
clinical review
recommend anti-depressant medication alongside CBT for severe depression. It has also been shown that use of CBT leads to a reduction in relapse rates. (Williams 2002).
Self-helpSelf-help materials are widely available and increasingly popular with clients and healthcare professionals alike. Some useful websites and literature are mentioned at the end of this article.
looking at lifestyle issues can be a useful starting point in engaging with a client who is feeling depressed. It can be helpful to establish a day-to-day structure, incorporating a regular checklist which could include;• Talking to someone you trust• Engage in at least one physical activity• Eating and drinking sensibly
• Keeping in touch with friends• learning to ask for help/support• Taking a break/learning to relax.For any additional information about the community based mental health service, the Dean Clinic Cork, please email [email protected] or phone 01 6477733.
further readingDepression, the Common Sense Approach : Tony Bates (1999)Overcoming Depression : Paul Gilbert (2009)Overcoming Depression: A Five Areas Approach, Dr Chris Williams (2002)Coping with Depression and Elation : Dr Patrick Mc Keon (1995)Coping with Depression : Aaron T Beck and Ruth l GreenbergTaking Control of your Mental Health, Shine, 2011.
useful websiteswww.stpatrickshosp.iewww.aware.iewww.mentalhealthireland.iewww.yourmentalhealth.ie
recommended reading for clientsOvercoming Depression by Paul Gilbert (2009)Mind Over Mood (Change how you feel by changing the way you think) by Greenberg & Padesky (1995)Alison lane is a Counsellor/Psychotherapist in the Dean Clinic, Cork. This clinic is part of St Patrick’s university Hospital, Dublin and it offers community-based mental health care to people in the Munster region.
Offer more patient services and increasepractice revenue with Promed AdvancePerformance:
Come and see Promed at the IPNA Conferenceand AGM inTullamore, October 14th & 15th 2011
Charles Bloe will host the short free workshop in Tullamore onOctober the 14th. The Workshop is entitled “Patient preparation:correct lead positions and ensuring a quality trace.”
Visit our stand to get full details and explore howAdvance Performance can help generate revenue foryour practice!
• Resting ECG,• ABPM Monitoring,• Cryotherapy,• Spirometry,
• Ear Care,• INR Measurement,• Holter Monitoring,• ECG reading & more...
For further information on Promed AdvanceTraining or Promed Advance Performance please
ring Promed on freephone 1800 619 619
Promed is proud to be sponsoring the ECG workshop:“Patient preparation: correct lead positions and ensuring a quality trace”Presented by Charles Bloe BSc RGN NDN ITU cert, on behalf of PromedDate 14th October 2011
IPNAconfNEW:Layout 1 13/09/2011 10:03 Page 1
The more a person believes [their] negative thoughts and accepts them as facts, the more depressed they will feel.

20
in practice
backgroundThe World Health Organization (WHO) refers to chronic disease as an “invisible” global epidemic that must be controlled.2 Patients with chronic diseases account for:• 80% of GP consultations3
• 78% of all healthcare spend4
• 60% of all deaths worldwide,2 but 84% of all deaths in Ireland5
• 77% of Europe’s disease burden.6,7
Many people have more than one chronic condition, known as multimorbidity.8 Individuals with multimorbidity are more likely to: • Die prematurely9
• Suffer from depression10
• Receive multiple medications11
• Have problems adhering to treatments12
• Be major drivers of general practice workload because of clinical complexity and polypharmacyand have:
• longer hospital stays13
• Frequent emergency hospital admissions13,14
• Repeated investigations at high cost for both the individuals and the healthcare system15
• Poorer quality of life10
• loss of physical functioning16,17
• Higher use of specialists even for conditions normally managed in primary care.18
Multimorbidity in primary carePart 1
Multimorbidity (the co-occurrence of two or more chronic conditions)1 is of growing importance to the field of practice nursing. This paper aims to give the reader an overview of what is currently known about the prevalence, effects and management of multimorbidity. It also explores the potential for practice nurses to lead the way in in establishing innovative approaches to caring for patients with multimorbidity.
MS JANe cAMPION, RGN MHSC (PRIMARY CARE)dr MAry byrNe, PHD

21
in practice
International prevalence studies confirm that multimorbidity is particularly common in people aged over 65.8 This has implications for countries with an increasing age profile, like Ireland where the population >65 years is expected to rise from 11% in 2006 to 25% by 2026.19
‘community matron’ modelSome countries have developed models of care to manage patients with multimorbidity who are at a high risk of hospitalisation, such as the ‘community matron’ model in the uK.20 These models incorporate a case management approach. There is no such model in Ireland for this cohort of patients. Clinical Practice Guidelines have been developed to improve the quality of healthcare for many chronic conditions. However, most aren’t applicable to patients with multimorbidity because they are based on evidence for single diseases.21
Furthermore, they don’t refer to short and long-term goals, burden, or facilitate patient preferences into treatment plans, all of which may enhance care for patients with multimorbidity. Furthermore, there is emerging concern that methods used to measure the quality of care unfairly penalise providers caring for patients with multimorbidity. Healthcare professionals may suffer if pay-for-performance programmes create incentives that are misaligned with the needs of these patients.22
In Ireland, the Department of Health and Children’s policy document ‘Tackling Chronic Disease’7 and the National Health Strategy ‘Quality and Fairness’23 recognise that with an aging population will come a significant increase in chronic diseases, and emphasise the need for its prevention and management, for which primary care has a central role. The Health Service Executive’s ‘Transformation Programme’24 acknowledges and prioritises the need to address the inadequate and fragmented services for chronic diseases. It recognises the need to implement a model for the prevention and management of chronic diseases and multimorbidity, to achieve high quality care through comprehensive and integrated programmes in the community. Furthermore, Primary, Community and Continuing Care (PCCC) services are identified as the path to optimal care and cost effectiveness. Therefore, primary care is ideally placed to meet the challenges of caring for patients with multimorbidity.25
Multimorbidity presents many challenges for the individual, their families, carers, healthcare system and service providers.7,
10, 17, 26 Each chronic condition impacts on the management of other conditions, making caring for these individuals challenging.1,7, 17, 27 The scientific basis for managing this complex topic appears weak.28 There is an obvious need to address these challenges and find solutions.
research into multimorbidityChronic disease management is usually based on evidence from trials of single conditions.29 literature shows little evidence of research specifically addressing multimorbidity in the primary care setting, as most individuals with multimorbidity are excluded from studies to minimise bias, even though these patients are the most frequent attenders in primary care.15,2 In other cases, co-morbidities are frequently not reported in research participants.30
Most studies in the area are epidemiological in design29 (thus demonstrating that multimorbidity is a growing concern) rather than healthcare outcome-based. Whilst this may help identify prevalence, many do not take into account the disease burden8,15,29or examine interventions for improving outcomes. A Cochrane review15 to determine the effectiveness of interventions is ongoing.
The first difficulty researching multimorbidity is a lack of a consistent definition. In addition, the WHO’s definition of chronic diseases covers a huge number of conditions.15 Selection of disease combinations differ, as do the number of diseases they count as multimorbidity (some as two or more diseases, whereas others require three plus).26,3 Furthermore, researchers and healthcare professionals differ in their view as to what constitutes a chronic disease. For example, some see lipid lowering medication as risk factor management rather than chronic disease management.6 All this makes comparison and generalisation difficult.
Patients with multimorbidity report the poorest level of health-related quality of life (HRQOl). Simple disease-count has a weak correlation with HRQOl. Additional variables such as perceived social support, age, education, perceived economic status and residual Cumulative Illness Rating Scale (CIRS)1 need to be taken into account.31 These factors further complicate researching multimorbidty.31
In summary, the complexity of multimorbidity in its definition, identification, severity, burden, confounding variables, and the difficulty in examining outcomes simultaneously and on a multiple basis, in any one individual, combine to make researching multimorbidity a challenge. However, Fortin et al.28 are representative in their thinking that “it is essential to increase primary care research into multimorbidity, in order to develop a better understanding of this important topic”. An international virtual research community has been established to help address this.11
Research has demonstrated that family members play an integral (sometimes predominant) role in the management of multimorbidity,32 so patient care should not just be patient-centred but also family-centred. Furthermore, Fortin et al. (2005)8 argue that the wide extent of multimorbidity strongly supports the development of innovative interventions focused on collaborative practices to better share the burden.
case management of multimorbidityPatients with chronic diseases can be categorised into three broad groups (people may move between levels as their conditions improve or disimprove):7
1 CIRS is used to measure the burden of medical multimorbidity.
Primary care is optimally suited to the care of patients with multimorbidity as it provides longitudinal care with sustained relationships.

22
in practice
Case management is increasingly important because of the developing fragmentation of healthcare services, a trend towards primary care, rising costs and an aging population.33 A Cochrane protocol describes case management simply as the “explicit allocation of co-ordination tasks to an appointed individual.”34 The term case management, a relatively new concept in primary care despite its existence since the 1980s in social work,33 is used interchangeably with Chronic Care Models, Guided Care, Care Management and Coordinated Care. Starfield33 sees the “only common thread being the idea of a mechanism to find and coordinate diverse services where care must be received from a myriad of sources.”
Case management is not viewed as a profession in itself, but an area of practice within one’s profession.33Specialist training is recommended.32There is a common consensus across disciplines that it involves six core functions32-36
1. Patient centred assessment2. Care planning 3. linking of services 4. Ongoing monitoring of the patient and family 5. Encouraging advocacy 6. Providing outreach services.
Case management works on the premise that everyone benefits when an individual reaches their optimum level of wellness and functional capability, from a micro (individual and family) level up to a macro (population) level.35Case management is used for complex patients, for individual diseases and for multimorbidity (level 3).
It is difficult to compare models of case management between countries, because each healthcare system is quite different. Each country develops their own models to suit local needs, coming in a diverse range of titles and formats that are dependent upon the level, discipline, organisation, situation, and basic client care needs.37, 38 For example, in the uK the Community Matron model is used. It is estimated that 2% of patients with chronic diseases account for 30% of unplanned hospital admissions.39To tackle this, the NHS introduced the Community Matron in 2004, based on the uS Evercare model of case management. The Community Matron is a highly skilled nurse specialist in community care and inter-agency working. She identifies those at risk, assesses, plans and coordinates care with other healthcare professionals, and is responsible for integrating care to meet all the individual’s health and social needs. The role extends beyond coordination by incorporating clinical interventions, making referrals, prescribing medicines and requesting investigations.40 Each Community Matron has a caseload of 30-50 patients.
However, an evaluation of the Community Matron model by Gravelle et al.41 showed no significant effect on rates of emergency admissions, bed days or mortality, although it was highly valued by both patients and carers, as the Community Matron educated and empowered patients. Furthermore, psychosocial support was seen as of equal importance to patients as clinical care.42 Gravelle et al. recommended a radical system redesign to reduce the rate of hospital admissions.
In the uSA, the Evercare model of case management serves patients >65 years with a history of two or more emergency hospital admissions using Advanced Nurse Practitioners (ANPs) acting as case managers. It showed a 50% reduction in unplanned admissions, significant reduction in medications, 97% family and carer satisfaction rates and high physician satisfaction.41 Similarly, the Veterans model (serving low income, homeless, disabled, at-risk veterans with the patient and social worker acting collaboratively) showed an increase in clinic visits, tests and consultations, a 35% reduction in emergency visits and 50% reduction in bed days.43
So the evidence for the effectiveness of case management is inconclusive. The implementation of case management programmes is fraught with difficulty as there are so many stakeholders involved. An appreciation of individual cultural, socioeconomic, ethnic and other differences must be facilitated.36A Cochrane review entitled “Case management: effects on professional practice and healthcare outcomes” is ongoing.34
The role of primary careThere is a need for structured and organised care for multimorbidity.44 Policy documents23,7,24 all acknowledge the need and the key role for primary care to manage chronic diseases. Furthermore, PCCC services are identified as the path to optimal care and cost-effectiveness.23 General ractice can provide good quality care for patients with chronic diseases with support from specialist services using a systematic approach.45 In fact, countries with primary care orientated healthcare systems tend to have better health outcomes and lower health costs.33
figure 1 Pyramid of care3
each chronic condition impacts on the management of other conditions, making caring for these individuals challenging.

23
in practice
Primary care is optimally suited to the care of patients with multimorbidity as it provides longitudinal care with sustained relationships.44,45 Starfield33 sees that continuity of care is more likely when care is provided by generalists rather than specialists, and that primary care practitioners are more effective in dealing with multimorbidity than specialist providers.18 Good communication with patients and between healthcare professionals is key to continuity of care.46 Starfield25 states that “Primary care is the only level of service in a position to understand and deal with multimorbidity” and the setting is well poised to take the lead.
The Role of the Practice NursePNs provide much of the care for patients with chronic
diseases.47 A key finding of one unpublished Irish study showed they have vital role to play in chronic disease management in general practice, and that practices with a PN are more likely to have improvements in chronic disease management and practice targets at an advanced or optimum level.48
Furthermore, PNs tend to remain in one practice49 thus lending themselves to continuity of care. In the view of Von Korff et al50 healthcare provision that is sustained over time improves patient outcomes. In the uK, The Netherlands and Sweden, the role of PNs is well developed51,52,53 and has been shown to be effective at providing high-quality guideline-directed care.41
Advanced nursing practice is a controversial issue. There are those who argue that it involves taking on medical tasks and working outside traditional nursing roles.54 Others view it as expert nurses expanding the boundaries55 and it’s the unique experience as a nurse which enhances the role of advanced practice. Nurses are willing to show that they are capable to lead in healthcare development, without losing their unique nursing skills.55 The uK has 3,000-5,000 ANPs, including
those who work at a junior doctor level.54 ANPs can support GPs, not only in chronic disease management but also in the care of patients with complex needs. Indeed, a systematic review in this area showed high levels of patient satisfaction and high quality care.56Nursing is viewed as holistic, aiming to work with patients to identify and meet their individual needs.57PNs are ideally placed to identify problems and care needs for the cohort of patients with multimorbidity. Their experience and insight into the care of these patients may be invaluable in informing and developing future initiatives. With such an international and national focus on chronic disease management comes the opportunity for advancing nursing practice, and indeed for nursing as a profession to lead the way in establishing a primary care based health service for patients with multimorbidity.
PNs are ideally placed to identify problems and care needs for the cohort of patients with multimorbidity.
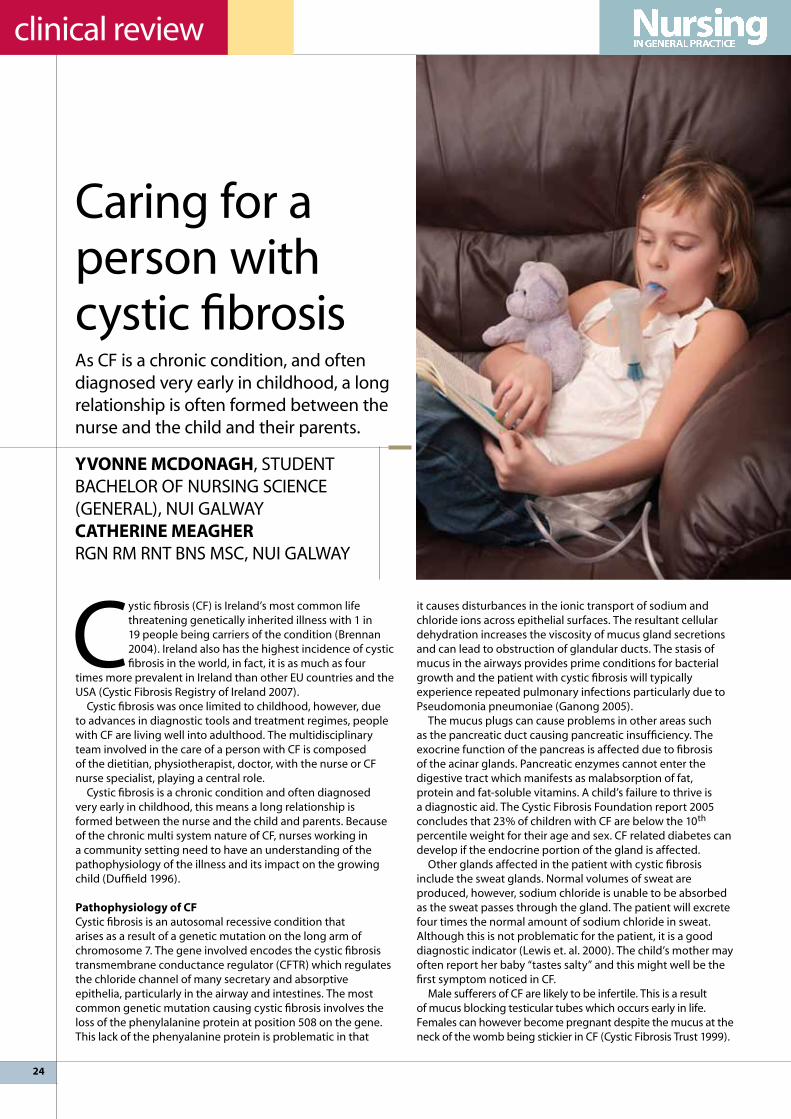
24
clinical review
Cystic fibrosis (CF) is Ireland’s most common life threatening genetically inherited illness with 1 in 19 people being carriers of the condition (Brennan 2004). Ireland also has the highest incidence of cystic fibrosis in the world, in fact, it is as much as four
times more prevalent in Ireland than other Eu countries and the uSA (Cystic Fibrosis Registry of Ireland 2007).
Cystic fibrosis was once limited to childhood, however, due to advances in diagnostic tools and treatment regimes, people with CF are living well into adulthood. The multidisciplinary team involved in the care of a person with CF is composed of the dietitian, physiotherapist, doctor, with the nurse or CF nurse specialist, playing a central role.
Cystic fibrosis is a chronic condition and often diagnosed very early in childhood, this means a long relationship is formed between the nurse and the child and parents. Because of the chronic multi system nature of CF, nurses working in a community setting need to have an understanding of the pathophysiology of the illness and its impact on the growing child (Duffield 1996).
Pathophysiology of cfCystic fibrosis is an autosomal recessive condition that arises as a result of a genetic mutation on the long arm of chromosome 7. The gene involved encodes the cystic fibrosis transmembrane conductance regulator (CFTR) which regulates the chloride channel of many secretary and absorptive epithelia, particularly in the airway and intestines. The most common genetic mutation causing cystic fibrosis involves the loss of the phenylalanine protein at position 508 on the gene. This lack of the phenyalanine protein is problematic in that
it causes disturbances in the ionic transport of sodium and chloride ions across epithelial surfaces. The resultant cellular dehydration increases the viscosity of mucus gland secretions and can lead to obstruction of glandular ducts. The stasis of mucus in the airways provides prime conditions for bacterial growth and the patient with cystic fibrosis will typically experience repeated pulmonary infections particularly due to Pseudomonia pneumoniae (Ganong 2005).
The mucus plugs can cause problems in other areas such as the pancreatic duct causing pancreatic insufficiency. The exocrine function of the pancreas is affected due to fibrosis of the acinar glands. Pancreatic enzymes cannot enter the digestive tract which manifests as malabsorption of fat, protein and fat-soluble vitamins. A child’s failure to thrive is a diagnostic aid. The Cystic Fibrosis Foundation report 2005 concludes that 23% of children with CF are below the 10th percentile weight for their age and sex. CF related diabetes can develop if the endocrine portion of the gland is affected.
Other glands affected in the patient with cystic fibrosis include the sweat glands. Normal volumes of sweat are produced, however, sodium chloride is unable to be absorbed as the sweat passes through the gland. The patient will excrete four times the normal amount of sodium chloride in sweat. Although this is not problematic for the patient, it is a good diagnostic indicator (lewis et. al. 2000). The child’s mother may often report her baby “tastes salty” and this might well be the first symptom noticed in CF.
Male sufferers of CF are likely to be infertile. This is a result of mucus blocking testicular tubes which occurs early in life. Females can however become pregnant despite the mucus at the neck of the womb being stickier in CF (Cystic Fibrosis Trust 1999).
Caring for a person with cystic fibrosisAs CF is a chronic condition, and often diagnosed very early in childhood, a long relationship is often formed between the nurse and the child and their parents.
yvONNe McdONAgH, STuDENT BACHElOR OF NuRSING SCIENCE (GENERAl), NuI GAlWAY cATHerINe MeAgHer RGN RM RNT BNS MSC, NuI GAlWAY

25
clinical review
laboratory tests and diagnosisAccording to the Cystic Fibrosis Foundation, diagnosis is achieved through certain criteria. These include:• Two sweat tests detecting elevated sodium chloride• Presence of obstructive pulmonary disease • Pancreatic insufficiency (or failure to thrive)• Family history (Genetic testing)
(Rosenstein and Cutting 1998)Other investigations employed to diagnose CF include chest
x-rays, stool specimens to detect the absence of pancreatic enzymes, genetic testing to confirm the 508 mutation and sputum cultures to detect the presence of bacteria typical of CF.
Presenting featuresCystic fibrosis is detected in the newborn by the presence of meconium ileus, an intestinal obstruction that is evidenced
by x-ray as distended bowel loops. Meconium ileus in the newborn merits a sweat test to be performed and cystic fibrosis is assumed unless proven otherwise (Cystic Fibrosis Association of Ireland). A child with CF will be failing to thrive and have poor respiratory health and CF can be diagnosed in the infant or toddler stage of development.
ScreeningHistorically, in Ireland, screening occurred in families where there was one child born with cystic fibrosis, following this, all successive children were screened at birth. However, because of its high prevalence in Ireland, there has been a strong consensus amongst the medical community that it was necessary for the introduction of a newborn screening for cystic fibrosis to be implemented. As of July 1st 2011, bloodspot screening for Cystic Fibrosis commenced in Ireland. The screening has been incorporated into the ‘heel-prick’ test, which now screens for six conditions, namely, Pheylketonuria, Congenital Hypothyroidism, Maple Syrup urine Disease, Classical Galactosaemia, Homosystinuria and now Cystic Fibrosis. Time will tell just how beneficial the introduction of this screening is to people with Cystic Fibrosis in terms of survival advantage, number of hospitalisations required and overall quality of life. However, some studies have shown that newborn screening programmes serve to provide a means for both early detection and intervention which in turn prevents early CF related deaths (Dankert-Roelse and Merelle 2005) and is associated with better survival when compared to delayed diagnosis (lai et. al. 2005).
cf and respiratory healthThe key principles in promoting respiratory health in persons with CF include:• Awareness• Education• Early intervention• Active management
According to Yankaskas 2001, pulmonary disease is the primary cause of death in 95% of CF, therefore, the nursing care of respira-tory complications is important in slowing the decline in respira-tory function. Most of the care of CF patients occurs in the home.

26
clinical review
Patients and their families need to be aware of the importance of concordance with medications and physiotherapy regimes, signs and symptoms of respiratory infections and lung function decline and also the importance of prompt action.
Educating patients and their families regarding avoiding contact with those who have infections such as influenza and importance of vaccinations is key. Promoting exercise to maintain good respiratory health is essential. The nurse must establish if the patient fully understands the technique when using inhalation therapies and provide teaching and education when appropriate.
Early intervention will improve the treatment outcome. Signs of infection should be noted early and dealt with to prevent further progression of the illness.
Active management occurs when patients present to hospital for either treatment of exacerbations of respiratory infections with antibiotics or for suppressive therapy during remissions when the patient is well. Isolation of immuno-compromised CF patients when admitted to hospital is a priority but not always possible due to bed restrictions. This is because of their susceptibility to infectious pathogens from other patients and poor infection control techniques of staff. Standard precautions must be exercised before and after contact with a CF patient. Sputum samples should be obtained 4 times a year and during each exacerbation (Yankaskas 2001). If it proves difficult to obtain a sample, the nurse should arrange for the physiotherapist to carry out airway clearance techniques with the patient in order to mobilize secretions.
Nutritional managementA child with CF can achieve normal growth, be better equipped to fight off infections and improve their lung function if their nutritional needs are met (Brennan 2004, booklet). Malabsorption is common in persons with CF as calories and nutrients are lost in their stool. A family centred approach should be adopted and parents should be educated on the appropriate diet for those with CF. Children spend most of their
week in school, hence the school canteen staff should also be aware of the dietary needs of children with CF.
Most children with CF lack the ability to digest their food adequately and pancreatic enzymes must be taken. The most common pancreatic enzyme taken in Ireland is Creon. A multi disciplinary approach is effective with the dietitian determining the correct dose on an individual basis based on stool amount and consistency and the level of abdominal pain. The patient and their family need to be aware of the importance of compliance with these doses and educated regarding how to take them, i.e. with food. Foods with higher fat content and bigger portions require higher doses of the enzyme. The enzymes must be swallowed whole, not mixed into food and taken at the right time.
Nutritional supplements can be used as an extra source of calories, not as a replacement for meals. These include, energy and protein-rich as well and carbohydrate-rich supplements. Vitamin deficiencies can arise due to malaborption in people with CF. Most will be prescribed vitamin supplements by the dietitian.
The nutritional health of the person with CF can be quantified by objective measures such as growth percentile charts and laboratory tests to determine vitamin levels in the blood.
Psychological care of the patient with cfParents of children with newly diagnosed CF can be in considerable shock and disbelief particularly if the child appears well to them. Reassurance to parents at the diagnosis stage is important and this can be achieved by avoiding bombarding them with information; it is a chronic condition and parents will need time to gain an insight into the condition. Some of the information may be out of date and can frighten parents. Referral to a CF nurse specialist can serve to alleviate some of the anxiety as she will have up-to-date treatment information. Novel treatments are expanding the life expectancy further and further and this will offer great hope to parents.
MOleculAr bASIS Of luNg dISeASe IN PATIeNTS wHO HAve cySTIc fIbrOSIS IS cOMPleXIn healthy individuals (top row), the main epithelial cells lining the airways (left panel) display at least two types of channels at the surface facing the air passages. One – the cfTr channel (red) – releases chloride into the passage; the other (blue) takes up sodium. This arrangement somehow enables mucus made by other cells to remain wet, thin and easy to remove from the airways (centre panel) and so the airways remain open (right panel). In patients with cystic fibrosis (bottom row), absence or malfunction of the cfTr channel prevents chloride movement (left panel) and indirectly causes cells to take up exta sodium.
EPITHElIAl CEllS SECTION OF EPITHElIuM AND AIR PASSAGE
CFTR CHANNEl
CHlORIDE
SODIuM
AIRWAY
SuBMuCOSAl GlANDEPITHElIAl CEll
CIlIA
MuCuS
INHAlED PARTIClE
MuCuS-SECRETING CEllS
AIRWAY
Chloride is secreted into airway and sodium is removed Wet, thin mucus traps inhaled particles, cilia push mucous to throat for removal
NO
RM
Al
luN
G
ABSENT OR DEFECTIVE CFTR CHANNEl
CHlORIDE
SODIuM
AlTERED SuBMuCOSAl GlAND
BACTERIA
DNA
IMMuNE CEllS
BACTERIA
Mucus becomes thick and difficult to remove. Bacteria proliferate and attack immune cells, which can damage healthy tissue. DNA released from bacteria and lung cells adds to the stickiness.
luN
G A
FFEC
TED
BY
CYS
TIC
FIB
RO
SIS
Chloride is barred from leaving cell and sodium uptake is enhanced.

27
clinical review
Acceptance can be a major factor in the psychological wellbeing of people with CF and their families, particularly as they get older. Casier et al 2008 support the idea that accepting the limitations of a chronic illness and readjusting life goals accordingly can have a positive effect on the psychological wellbeing of adolescents with CF. Peer groups and social networking groups such as Facebook groups can provide a connection between people with CF all over the world which can be influential, particularly at the cusp of entering adolescence.
The literature highlights a particularly vulnerable stage in the person with CF and refers to it as the “transition”. This occurs when the child leaves the paediatric services and enters the adult services. It is important to recognise that these teenagers may have fears arising from the fact the some of their peers may have already died from their illness and this may cause uncertainty for the future for them. Nurses are in a prime position to support and help both patients and families with the responsibility of managing their own care. Teenagers should be empowered to take control of their care and start by seeing the members of the multi disciplinary team on their own without their parents. This positive approach may help them to become independent and autonomous adults.
Pharmacological treatment of cfPeople with CF are now living well into adulthood, which can be attributable to earlier diagnosis, a multidisciplinary approach and effective methods of treatment (Abbott and Gee 1998). The three major treatment goals for patients with CF include:• providing for adequate nutrition with pancreatic enzymes
and vitamin supplements• prevention and treatment of respiratory infections with oral,
inhaled, nebulised or intravenous drugs• chest physiotherapy and the promotion of exercise to
improve lung function and airway clearance.(Beers and Berkow 1999).
respiratory treatmentThe main drugs used in the management of the respiratory complications in CF include• Bronchodilators to increase air entry• Anti-inflammatory drugs to slow the decline in lung function• Antibiotics to eradicate bacterial infections.
Aerosolized antibiotics have proven effective in both the eradication of the initial Pseudomonas aeruginosa infection common in CF and also for suppression of the chronic infection (Flume et al 2007). Aerolized (inhaled) treatments
reassurance to parents at the diagnosis stage is important and this can be achieved by avoiding bombarding them with information.
are preferable as they allow direct delivery to the infection site, hence smaller doses are needed which reduces the risk of systemic toxicity (Yankaskas and Knowles 2001). The drugs used include alfa dornase (pulmoezyme) and inhaled tobramycin.
Alfa dornase acts by fragmenting extra DNA particles found in the mucus of children with CF, this makes the mucus less viscous. The tobramycin is used to treat the source of lung infections while ibuprofen acts as an anti-inflammatory, thus slowing the decline in lung function (Strawhacker and Wellendorf 2004). Tobramycin can be both inhaled, to achieve the desired concentration in the airways, and also intravenously to reach the peripheries that are blocked by the mucus secretions. The inhalation route is the safer option as intravenous therapy must be administered in the hospital which puts the patient with CF at risk from developing a hospital acquired infection. The alfa dornase can cause hoarseness, voice alterations and pharyngitis, however, these are usually self-limiting (Yankaskas and Knowles 2001). The patient must be educated regarding the side effects of the treatments and be aware of the importance of reporting any symptoms in good time.
gastrointestinal treatmentEnzyme replacement therapy is the method of treating the pancreatic insufficiency commonly seen in people with CF. Pancreatin is the general name given to all pancreatic enzymes used as treatments. Creon is Ireland’s most popular drug for treating this condition. It is taken orally in capsule form but it is available in powder form also. The capsules have an enteric coat which aids digestion and the active drug is released in the small intestine. It mimics the function of the naturally occurring enzymes in a healthy individual. Creon Micro is used in very small infants. This type of treatment is a life-long therapy and children should be empowered to learn how to take their own medication from an early age. Enzymes can be taken with food and can be mixed in small amounts with baby food. However, skin irritation can arise around the mouth in the dribbling area if the enzymes are in direct contact with the skin. The irritation around the nipple can also be problematic for breast feeding mothers Vaseline is used as a barrier cream to prevent this (Tully 2006, booklet).
It is important to note that for the most part CF patients are well and living in the community. They are only required to attend the hospital during exacerbations of their illness, therefore, a large proportion of the care is community based with regular appointments to outpatient clinics. Compliance and concordance with medication regimes should be promoted.
conclusionThe ultimate aim in the management of CF is to find a cure, however, while we wait we must endeavour to promote research that will improve the current methods of treatment. The fact that therapies such as gene therapy are in the not too distant future offers hope to the many parents who give birth to children with CF, particularly in Ireland. Nurses need to be equipped with the knowledge of caring for those with CF as its prevalence increases, all the while never losing sight of the goal to promote health and keep people with CF out of hospital and living life to the full in their own home with their family.
Sources of informationInterested in Practice/Community Nursing, http://www.nuigalway.ie/courses/taught-postgraduate-courses/nursing-practice-community.html

Available in Pharmacies
NEW TO IRELAND 10 minShampoo Prevent
Spray15 minLotion
Linicin Shampoo is 100% effective in eliminating head lice• 10 minute treatment
• Non chemical formulation
• No risk of resistance
• Colourless, odourless
• Non-flammable
• No need to wash hair after use
• Suitable for children over 2 years
Linicin Lotion isnew to Ireland…new to head lice! • 15 minute treatment
• Active ingredient - Dimeticone
• Colourless, odourless
• No risk of resistance
• Suitable for children over 6 months
• Suitable for pregnant and breast feeding women
• Suitable for use in asthma patients
• Pack contains fine toothed stainless steel comb
Linicin Preventmakes hair ‘invisible’to head lice• 100% effective
• Contains no pesticides
• Easy to use, applied once daily,and does not need to be rinsed out
• Colourless with pleasantneutral scent
• Non-flammable
• Suitable for children over 2 years
• No risk of resistance
LINIcINEffective Treatment For Head Lice

29
clinical review
Although headlice are not going to kill anyone, they are an important issue for patients and parents. This article discusses the emotional, psychological, physical and financial impact of headlice infestation, and describes the health education needed by
patients in order to combat them. It also looks at the pros and cons and efficacy of different treatments for headlice.
ImpactMost patients are not physically affected by headlice, but people can react to the substance injected into the skin by the louse to stop blood clotting when it feeds on the scalp. This can cause the skin to be inflamed and itchy. If the itch is scratched and the skin’s integrity is broken, nosocomical, staphylococcal, or bacterial infections such as impetigo can develop. Headlice infestation has also been found to be a risk factor for peri-
operative complications in neurosurgical patients. (Divyesh 2007).
Headlice can also affect people emotionally and psychologically. Gorden (2007) found persistent infestation negatively affected people’s emotional and psychological well-being. He identified feelings of frustration, anger, exhaustion and revulsion that can be all-consuming, mortifying, and socially isolating. Also children’s friendships can be disrupted if parents feel their children are being infected by other children. Or, within families one child can be isolated from other family members. These feelings partly spring from the historical view of headlice as arising from poverty and dirt. This is a myth, as headlice affect all socioeconomic groups.
In the current economic climate the cost of treating headlice can be challenging. Most remedies cost about €10-15 for a relatively small 50-100ml quantity. These amounts usually only
Headlice – detection, treatment and preventionManagement of headlice infestations is a relatively common task in general practice as headlice affect about 1 in 10 school aged children at any one time.
SAlly wHelAN RGN RHV BA MA, PRACTICE NuRSE, GAlWAY
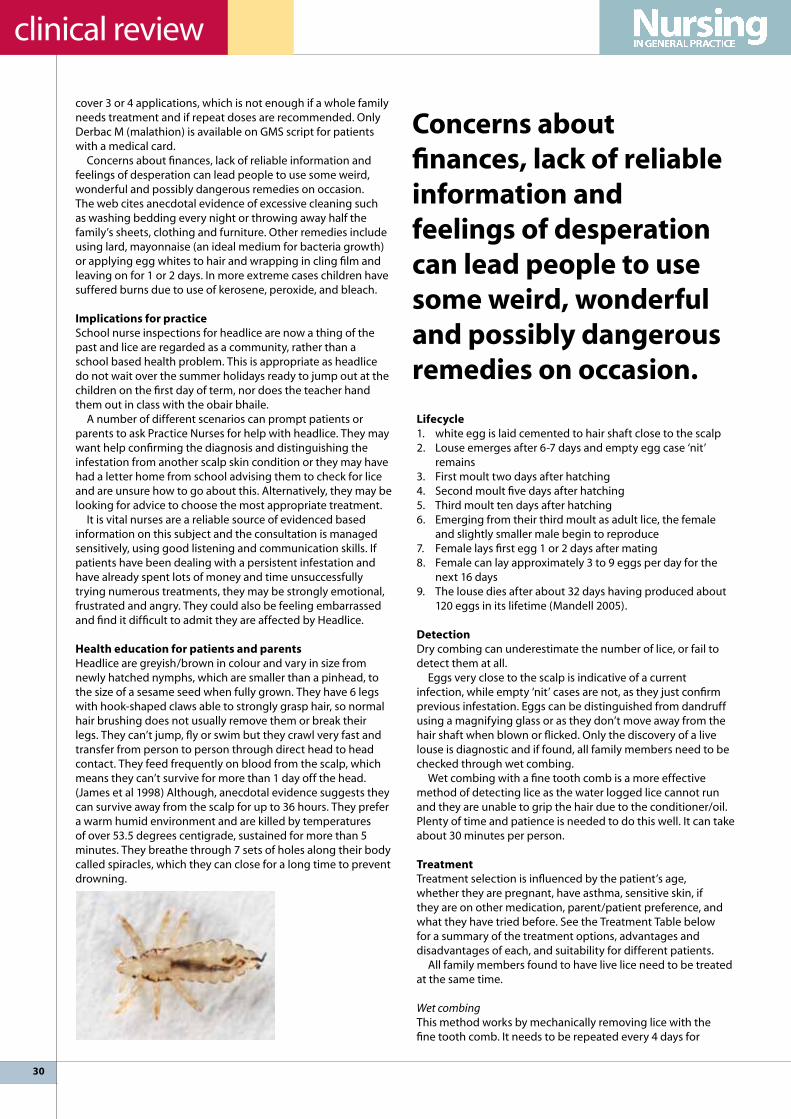
30
clinical review
cover 3 or 4 applications, which is not enough if a whole family needs treatment and if repeat doses are recommended. Only Derbac M (malathion) is available on GMS script for patients with a medical card.
Concerns about finances, lack of reliable information and feelings of desperation can lead people to use some weird, wonderful and possibly dangerous remedies on occasion. The web cites anecdotal evidence of excessive cleaning such as washing bedding every night or throwing away half the family’s sheets, clothing and furniture. Other remedies include using lard, mayonnaise (an ideal medium for bacteria growth) or applying egg whites to hair and wrapping in cling film and leaving on for 1 or 2 days. In more extreme cases children have suffered burns due to use of kerosene, peroxide, and bleach.
Implications for practiceSchool nurse inspections for headlice are now a thing of the past and lice are regarded as a community, rather than a school based health problem. This is appropriate as headlice do not wait over the summer holidays ready to jump out at the children on the first day of term, nor does the teacher hand them out in class with the obair bhaile.
A number of different scenarios can prompt patients or parents to ask Practice Nurses for help with headlice. They may want help confirming the diagnosis and distinguishing the infestation from another scalp skin condition or they may have had a letter home from school advising them to check for lice and are unsure how to go about this. Alternatively, they may be looking for advice to choose the most appropriate treatment.
It is vital nurses are a reliable source of evidenced based information on this subject and the consultation is managed sensitively, using good listening and communication skills. If patients have been dealing with a persistent infestation and have already spent lots of money and time unsuccessfully trying numerous treatments, they may be strongly emotional, frustrated and angry. They could also be feeling embarrassed and find it difficult to admit they are affected by Headlice.
Health education for patients and parents Headlice are greyish/brown in colour and vary in size from newly hatched nymphs, which are smaller than a pinhead, to the size of a sesame seed when fully grown. They have 6 legs with hook-shaped claws able to strongly grasp hair, so normal hair brushing does not usually remove them or break their legs. They can’t jump, fly or swim but they crawl very fast and transfer from person to person through direct head to head contact. They feed frequently on blood from the scalp, which means they can’t survive for more than 1 day off the head. (James et al 1998) Although, anecdotal evidence suggests they can survive away from the scalp for up to 36 hours. They prefer a warm humid environment and are killed by temperatures of over 53.5 degrees centigrade, sustained for more than 5 minutes. They breathe through 7 sets of holes along their body called spiracles, which they can close for a long time to prevent drowning.
lifecycle1. white egg is laid cemented to hair shaft close to the scalp2. louse emerges after 6-7 days and empty egg case ‘nit’
remains3. First moult two days after hatching4. Second moult five days after hatching5. Third moult ten days after hatching6. Emerging from their third moult as adult lice, the female
and slightly smaller male begin to reproduce7. Female lays first egg 1 or 2 days after mating8. Female can lay approximately 3 to 9 eggs per day for the
next 16 days9. The louse dies after about 32 days having produced about
120 eggs in its lifetime (Mandell 2005).
detectionDry combing can underestimate the number of lice, or fail to detect them at all.
Eggs very close to the scalp is indicative of a current infection, while empty ‘nit’ cases are not, as they just confirm previous infestation. Eggs can be distinguished from dandruff using a magnifying glass or as they don’t move away from the hair shaft when blown or flicked. Only the discovery of a live louse is diagnostic and if found, all family members need to be checked through wet combing.
Wet combing with a fine tooth comb is a more effective method of detecting lice as the water logged lice cannot run and they are unable to grip the hair due to the conditioner/oil. Plenty of time and patience is needed to do this well. It can take about 30 minutes per person.
Treatment Treatment selection is influenced by the patient’s age, whether they are pregnant, have asthma, sensitive skin, if they are on other medication, parent/patient preference, and what they have tried before. See the Treatment Table below for a summary of the treatment options, advantages and disadvantages of each, and suitability for different patients.
All family members found to have live lice need to be treated at the same time.
Wet combingThis method works by mechanically removing lice with the fine tooth comb. It needs to be repeated every 4 days for
concerns about finances, lack of reliable information and feelings of desperation can lead people to use some weird, wonderful and possibly dangerous remedies on occasion.

31
clinical review
a minimum of 2 weeks. This is because nymphs need to be removed after they hatch, before they reach adulthood and produce more eggs. Roberts (2000) compared the effectiveness of wet combing with malathion insecticide and found the latter twice as effective as wet combing. However, over 50% of people extended or shortened treatment intervals by 1 to 3 days. Another study found it was 57% effective after 14 days (DPT 2007).
SmotheringThis uses the wet combing method and requires the same amount of combing at the correct time intervals but also suffocates the lice by blocking the spiracles. The oil needs to be left on the head for at least 8 hours. Madhee (2000) recommends smothering and her research found it to be as effective as insecticides.
Insecticides Insecticides such as permethrin, malathion and phenothrin have been used since the 1960s. They are chemicals which damage the nervous system of the louse and eggs. In a Cochrane review, Dodd (2001) found that no one insecticide had a greater effect than another. DPT (2007) reports them to be approximately 75% effective. However, headlice have become resistant to the various insecticides in some areas at certain times. Rotating insecticides on a district wide basis is now considered outmoded and a more ‘mosaic’ pattern is recommended, where one uses a different insecticide if the first tried has failed.
Newer physical treatmentsThese contain silicone, such as dimeticone 4%, and work by damaging the outer coat of the louse, and blocking the spiracles. As lice try to excrete water through the spiracles they are unable to do so and they reflexively immobilise as if they are in water and die. If they have fed recently, their intestines also rupture. One such treatment, dimeticone 4% was 70% effective (Burgess, 2005). It needs to be left on for 8 hours and hair needs to be thoroughly covered during treatment to ensure success.
Some newer treatments are effective in only 10 minutes. For example, isopropyl myristate was found to be 82% effective, again with thorough coverage. Indeed, the authors recommended 100ml to 300ml bottles over the 59ml to enable satisfactory coverage to take place (Burgess 2005).
The newest product is called NYDA. This is stocked by Boots Ireland – 100ml for €11.99 – and contains Dimeticone 92%. A randomized, controlled observer blinded clinical trial involving 45 participants reported cure rates at day 9 of
97.2% (Heukelbach 2008). The study also reported cosmetic acceptability as good and only two mild product-related incidents occurred.
Mineral oil treatmentsThese treatments appear to have little to recommend them over wet combing methods (see treatment chart). Just because herbal or in a health shop and without insecticide doesn’t mean they are safe, as allergic responses have been noted. They are also more greasy and difficult to wash out then normal conditioner.
Electronic headlice combManufacturers claim this works by emitting an electronic charge and noise when a louse is caught in the teeth of the fine tooth comb. The charge stuns the louse allowing for physical removal of same. There is no independent research found to support its efficacy.
Non pharmacologic measuresCleaning of bedding and clothing is not generally needed to eliminate infection but it is prudent to wash and dry clothes and bedding used in the previous two days by the infected person. If they can not be laundered in temperatures greater than 53.5 degrees centigrade, or dry cleaned, then they should be placed in a sealed plastic bag for 2 weeks. (CDC 2011).
PreventionClinical studies suggest repellents are of uncertain value. Weekly wet combing is a sensible precaution.
Implications for practiceNo one treatment is 100% effective. Products requiring shorter contact time seem to have obvious advantages and it seems reasonable to recommend the newer treatments for this reason. However, nurses need to consider the cost of products and be able to discuss the pros and cons with patients and help them to find a product best suited to their needs and opinions.
To increase the chances of treatments working and being used correctly, patients need a good understanding of the lifecycle of lice and their physical characteristics. Treatment instructions need to be followed to the letter with sufficient solution applied, and the second application done exactly 7 days after the first.
resources:[email protected] lice line Tel: 01-8790647 (lyclear ) www.killnits.comwww.headlice.ie (Fullmarks)
wet combing• Wash the hair with normal shampoo and apply enough
conditioner to cover hair completely.• Comb the hair to remove tangles and divide into sections, using
hair grips or bands.• Ensure you have good light, sufficient warmth for comfort and
something to keep children amused and still. Start on the sections at the bottom of the head and divide the hair into very small pieces. Insert the fine tooth comb at the scalp and slowly draw it through the hair right to the tip of the hair. Check the comb for lice and wipe it on a white tissue after each pull through.vi) On finishing each section secure it away before starting on another one.vii) Continue until all sections of the hair have been combed.

32
in practice
Spirometry is a physiological test that measures how an individual inhales or exhales volumes of air as a function time. The primary signal measured in spirometry may be volume or flow.
When performed correctly spirometry is an invaluable screening and monitoring tool for respiratory health.
The most important aspects of spirometry are the forced vital capacity (FVC), which is the maximum amount of air that can be forcefully exhaled from fully inflated lungs and the forced expiratory volume in one second (FEV1), which is the volume delivered in the first second of an FVC manoeuvre.
Accurate spirometry requires co-operation between the subject and the examiner and the results obtained will depend on technical as well as personal factors. Accuracy of the result can be improved by ensuring that all healthcare professionals performing the test are competent and highly trained.
Currently the majority of spirometry is carried out by respiratory scientists in the acute hospital setting, however, the availability over recent years of affordable and portable computerised flow-based spirometers, makes it easier to test at primary care level.
Spirometry trainingIn 2005 the ATS/ERS Taskforce: Standardisation of lung Function Testing published International Standards for the measurement and interpretation of spirometry. The Irish Association of Respiratory Scientists (IARS) with the endorsement of the Irish Thoracic Society (ITS) have adopted these guidelines and have made them a minimum standard for all its members carrying out spirometry testing.
The IARS provides a training programme leading to a Certificate in Spirometry, to all practitioners of spirometry outside the Respiratory laboratory setting that have an interest in providing quality spirometry data and or are involved in the interpretation of spirometry. The Certificate in Spirometry became fully accredited by the Dublin Institute of Technology on 5th May 2011 and will carry an award of 15 ECTS credits. It is endorsed by the ITS and Category 1 approval is being sought from An Bord Altranais.
This course will be the national standard for spirometry performance and is supported by the National COPD Clinical Care Programme, The National Asthma Clinical Care Programme and Professional Development Co-ordinators for Practice Nurses (PDCPN).
IArS certificate in SpirometryThe IARS/DIT Certificate in Spirometry consists of 1 day theory
New standards for spirometry testing The IARS provides a training programme leading to a Certificate in Spirometry, to all practitioners of spirometry outside the Respiratory laboratory setting that are involved in the interpretation of spirometry.
MArIA McNeIl, CHAIRPERSON, IRISH ASSOCIATION OF RESPIRATORY SCIENTISTS
and practical training followed by a 6 month certification process which requires the completion of a log book, assignment, written and practical examination. The IARS provides a mentor and detailed guidelines for the certification process.
As, the IARS/DIT Certificate in Spirometry is soon to become the minimum standard for all healthcare professionals performing spirometry, and to take into account nurses who already perform spirometry to a very high standard, the IARS has put in place three entry levels to the certification process.
The certificate is valid for two years and re-certification may be achieved by completing a short MCQ and Spirometry practical. (I hour in total).
• level 1 – Nurses with no experience or training in spirometryAre required to undertake the training day followed by
completion of log book, assignment, written and practical examination.• level 2 – Nurses who have attended the IARS Spirometry
Training Day or equivalent training day On production of certificate of attendance may begin the
certification process (log book, assignment, written and practical exam).• level 3 – Experienced nurses currently performing high
volume spirometry (min 50 per year)Experienced nurses may undertake the written and practical
examination without attending the training day or completion of the log book or assignment.
Applications for entry at this level must be made prior to November 2011. All applications will be reviewed jointly on a case by case basis by the IARS and DIT.
All nurses who successfully complete the certification process will have their name placed on a Spirometry Register.
conclusionPerforming spirometry is an essential requirement for managing a large number of respiratory conditions and evidence is accumulating that measurements of FEV1 and FVC should be recorded on all patients over 35, who are short of breath and have a smoking history. Widening the scope for obtaining this data in a reliable way is needed so that we can get the best clinical value for our patients. undertaking the Certificate in Spirometry will ensure this standard of care for every patient.
Further details may be obtained on our website www.iars.ie or by emailing me directly at [email protected]

33
in practice
Type of Treatment Advantages disadvantages Product examples
Suitability
wet combing Cheap and safe. Good for people not wanting to use commercial products. Can be effective
Time consuming, Difficult for young children to sit still. Not suitable for everyone. Repeat every 4 days for 2 weeks at least
Bug Buster Kit. Can buy combs separately.
Everyone.
Mineral oils As effective as wet combing
Needs similar diligence to wet combing. Expensive. Some allergic reactions noted. Check ingredients carefully
e.g. Riddance contains almond oil
Caution with allergies, pregnancy, epilepsy or using homeopathic remedies.
Smothering Cheap oil and shower cap neededCan be effective.
Can be messy, need to cover hair completely and need to leave on for 8 hours. Proceed with wet combing. See above
Olive oil cheapest brand
Everyone.
Insecticidese.g Permethrine.g. Malathion liquid
Can be effective. lyclear takes 10 mins
Sometimes lice are resistant to them. Expensive. Parents may fear use of chemicals. No more than 3 doses 3 consecutive weeks. Needs pre-testing especially with colour treated hair in previous 4 weeks. Repeat in 7 days
Derbac takes 12 hoursAdvisable to repeat treatment in 7 days.
lyclear crème rinse
Derbac M
Suitable for asthmatics and from 6 months old
Suitable for asthma suffersand sensitive skin – from 6 months old.
Treatments with a physical action on the lice
cyclomethicone Isopropyl myistate
Effective treatment. No resistance. Odourless. Works in 10 mins
Advisable to retreat in 7 daysNeeds to be applied thoroughlyCan be very greasy and difficult to remove
Full Marks SolutionFull Marks Solution Spray
Suitable for asthma/sensitive skin. From age 2.
dimeticone 4% and Mineral oils
Hedrin applied to dry hairlyclear Spray-15mins onlylyclear Mouse – 10 mins onlyNondrip no odour easy to apply
Hedrin leave on for 8 hours.All need repeat dose 7 days later
Hedrinlyclear Spraylyclear Mousse
Suitable for asthmaticsFrom 2 years.
dimeticone 92% NYDA highly effective. Apply to dry hair then wet comb through. May not need second treatment.
leave on for 8 hours Check for live lice after 8-10 days. Repeat if needed.
Suitable from 2 years.
electronic headlice comb
Manufacturers say it picks up even the tinniest nymphs. Supposed to spare children the discomfort of repeated shampooin.
No independent research confirming its efficacy. Very expensive.
Not recommended with heart disease, epilepsy cardiac pacemakers.
repellante.g. Piperonal(Prevention method)
Of uncertain value in clinical trials. Number of adverse skin reactions noted. Has to be sprayed onto hair daily. Does not kill lice or eggsNo evidence to support use.
e.g. Rappell A number of reported adverse skin action.

Powerful glucose reductions to help get patients to goal1,a
For patients not adequately controlled on metformin alone,
(sitagliptin/metformin)
Glucose reductions at 24 weeks
PPGFPGJANUMET 50/1000 mg twice daily
HbA1c primary end point
–2.1%
–3.9 mmol/L – 6.5 mmol/L(n=180; mean
baseline 10.9 mmol/L; P≤0.001)(n=152; mean
baseline 15.9 mmol/L; P≤0.001)
vs placebo(n=178;
mean baseline 8.8%; P≤0.001)
All-patients-treated population.
Additional HbA1c results at 24 weeks1,a
• 1.3% placebo-adjusted HbA1c reduction with metformin 1000 mg twice daily (n=177; mean baseline 8.7%; P≤0.001)
• 1.6% placebo-adjusted HbA1c reduction with JANUMET™ (sitagliptin/metformin, MSD) 50/500 mg twice daily (n=183; mean baseline 8.8%; P≤0.001)
• 1.0% placebo-adjusted HbA1c reduction with metformin 500 mg twice daily (n=178; mean baseline 8.9%; P≤0.001)
• 0.8% placebo-adjusted HbA1c reduction with sitagliptin 100 mg once daily (n=175; mean baseline 8.9%; P≤0.001)
JANUMET: Powerful efficacy
to help get patients to goal1
As an adjunct to diet and exercise, For patients uncontrolled on metformin alone2
In combination with a glitazone or sulfonylurea2
In combination with insulin2
✔
✔
✔
07-1
2-JM
T-20
11-IR
L-47
07-J
JANUVIA® Sitagliptin JANUMET® Sitagliptin/metformin hydrochlorideABRIDGED PRESCRIBING INFORMATION Refer to Summary of Product Characteristics (SmPC) before prescribing PRESENTATION Januvia® 100 mg film-coated tablet containing 100 mg of sitagliptin. Janumet® 50 mg/850 mg and 50 mg/1000 mg tablets each contain-ing 50 mg sitagliptin and 850 mg or 1000 mg metformin hydrochloride. USES For patients with type 2 diabetes mellitus Januvia is indi-cated to improve glycaemic control: as monotherapy • in patients inadequately controlled by diet and exercise alone and for whom metformin is inappropriate due to contraindications or intolerance as dual oral therapy in combination with • metformin when diet and exercise plus metformin alone do not provide adequate glycaemic control • a sulphonylurea when diet and exercise plus maximal tolerated dose of a sulphonylurea alone do not provide adequate glycaemic control and when metformin is inappropriate due to con-tra-indications or intolerance • a PPARγ agonist (i.e. a thiazolidinedione) when use of a PPARγ agonist is appropriate and when diet and exercise plus the PPARγ agonist alone do not provide adequate glycaemic control as triple oral therapy in combination with • a sulphonylurea and metformin when diet and exercise plus dual therapy with these agents do not provide adequate glycaemic control. • a PPARγ agonist and metformin when use of a PPARγ agonist is appropriate and when diet and exercise plus dual therapy with these agents do not provide adequate glycaemic control. Januvia is also indicated as add-on to insulin (with or without metformin) when diet and exercise plus stable dosage of insulin do not provide adequate glycaemic control. Janumet: as an adjunct to diet and exercise to improve glycaemic control in patients inadequately controlled on their maximal tolerated dose of metformin alone or those already being treated with the combination of sitagliptin and metformin. • in combination with a sulphonylurea (i.e., triple combination therapy) as an adjunct to diet and exercise in patients inadequately controlled on their maximal tolerated dose of metformin and a sulphonylu-rea. • as triple combination therapy with a PPARγ agonist (i.e., a thiazolidinedione) as an adjunct to diet and exercise in patients inad-equately controlled on their maximal tolerated dose of metformin and a PPARγ agonist. • as add-on to insulin (i.e., triple combination therapy) as an adjunct to diet and exercise to improve glycaemic control in patients when stable dosage of insulin and metformin alone do not provide adequate glycaemic control. DOSAGE AND ADMINISTRATION Januvia - One 100 mg tablet once daily, with or without food. Janumet - The dose of antihyperglycaemic therapy with Janumet should be individualised on the basis of the patient’s current regimen, effectiveness, and tolerability while not exceeding the maximum recommended daily dose of 100 mg sitagliptin. For patients not adequately controlled on metformin alone, the usual starting dose of Janumet should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) plus the dose of metformin already being taken. For patients switching from co-administration of sitag-liptin and metformin, Janumet should be initiated at the dose of sitagliptin and metformin already being taken. For patients inadequate-ly controlled on dual combination therapy with the maximal tolerated dose of metformin and a sulphonylurea or with maximal tolerated dose of metformin and a PPARγ agonist or with maximal tolerated dose of metformin and insulin, the dose of Janumet should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose) and a dose of metformin similar to the dose already being taken. All patients should continue their diet with an adequate distribution of carbohydrate intake during the day. Overweight patients should continue their energy-restricted diet. Januvia and Janumet - In combination with a sulphonylurea or with insulin, consider a lower dose of sulphonylurea or insulin, to reduce risk of hypoglycaemia. Renal impairment: See Precautions. Hepatic impairment: For Janu-via only - no dosage adjustment necessary for patients with mild to moderate hepatic impairment. Januvia has not been studied in patients with severe hepatic impairment. For Janumet only – do not use. Elderly < 75 years: For Januvia only - no dosage adjustment necessary. For Janumet only - use with caution as age increases. Monitoring of renal function is necessary to aid prevention of met-formin-associated lactic acidosis. Elderly ≥ 75 years: Exercise care as there are limited safety data in this population. Children: not recommended below 18 years of age. CONTRA-INDICATIONS For Januvia - Hypersensitivity to active substance or excipients. For Janumet - Hypersensitivity. Diabetic ketoacidosis and diabetic pre-coma. Moderate and severe renal impairment (creatinine clear-ance < 60 ml/min). Acute conditions with the potential to alter renal function such as dehydration, severe infection, shock. Intravascu-lar administration of iodinated contrast agents. Acute or chronic disease which may cause tissue hypoxia such as cardiac or respira-tory failure, recent myocardial infarction, shock. Hepatic impairment. Acute alcohol intoxication, alcoholism. Lactation. PRECAUTIONS For Januvia and Janumet - General: do not use in patients with type 1 diabetes or for diabetic ketoacidosis. Pancreatitis: Post-market-ing experience - spontaneously reported adverse reactions of acute pancreatitis. Inform patients of the symptom of acute pancreati-tis: persistent, severe abdominal pain. Resolution of pancreatitis has been observed after discontinuation of sitagliptin, but very rare cases of necrotizing or haemorrhagic pancreatitis and/or death have been reported. If pancreatitis is suspected, Januvia or Janumet and other potentially suspect medicinal products should be discontinued. Hypoglycaemia when used with other anti-hyperglycaemic agents: Rates of hypoglycaemia reported with sitagliptin were generally similar to rates in patients taking placebo. When sitagliptin was added to a sulphonylurea or to insulin, the incidence of hypoglycaemia was increased over that of placebo; therefore consider a lower dose of sulphonylurea or insulin to reduce the risk of hypoglycaemia when administering Janumet or Januvia. Hypersensitivity reactions: Serious hypersensitivity reactions have been reported, including anaphylaxis, angioedema, and exfoliative skin conditions including Stevens-Johnson syndrome. Onset occurred within the first 3 months after initiation of treatment with some reports occur-ring after the first dose. If suspected, discontinue Januvia or Janumet. For Januvia only - As experience is limited, patients with moderate or severe renal impairment should not be treated with Januvia. For Janumet only - Lactic acidosis and renal function: a very rare, but serious, metabolic complication can occur due to metformin accumulation. Cases in patients on metformin have occurred primarily in diabetic patients with significant renal failure. Reduce incidence by assessing other associated risk factors. If suspected, discontinue treatment and hospitalise patient immediately. If changes in clinical status of patients with previously controlled type 2 diabetes occurs, evaluate promptly for evidence of ketoacidosis or lactic acidosis in any patient with type 2 diabetes previously well
controlled on Janumet who develops laboratory abnormalities or clinical illness (especially vague and poorly defined illness). If aci-dosis of either form occurs, stop Janumet immediately and initiate corrective measures.Determine serum creatinine concentrations regularly, i.e. at least once a year in patients with normal renal function and at least two to four times a year in patients with serum creatinine levels at or above the upper limit of normal and in elderly patients. Decreased renal function in elderly patients is frequent and asymptomatic. Exercise special caution where renal function may become impaired, e.g. when initiating antihypertensive or diu-retic therapy or when starting treatment with a non-steroidal anti-inflammatory drug (NSAID). Surgery: due to metformin hydrochlo-ride content of Janumet, discontinue treatment 48 hours before elective surgery with general, spinal or epidural anaesthesia. Do not resume earlier than 48 hours afterwards and only after renal function is normal. DRUG INTERACTIONS For Janumet only - Alcohol: avoid alcohol and medicinal products containing alcohol due to risk of lactic acidosis. Cationic agents that are eliminated by renal tubular secretion (e.g., cimetidine): these may interact with metformin by competing for common renal tubular transport systems. Consider close monitoring of glycaemic control, dose adjustment within the recommended posology and changes in diabetic treat-ment when these agents are co-administered. Iodinated contrast agents in radiological studies: intravascular administration of these agents may lead to renal failure, resulting in metformin accumulation and a risk of lactic acidosis. Discontinue Janumet prior to, or at the time of the test and do not reinstitute until 48 hours afterwards, and only after renal function is found to be normal. Combination requiring precautions for use: glucocorticoids (given by systemic and local routes) beta-2-agonists, and diuretics have intrinsic hyper-glycaemic activity. Inform the patient and perform more frequent blood glucose monitoring, especially at the beginning of treatment. If necessary, adjust dose of the anti-hyperglycaemic medicine during therapy with, or on discontinuation of the other medicine. ACE-inhibitors: as these may decrease the blood glucose levels, if necessary, adjust dose of the antihyperglycaemic during therapy with, or on discontinuation of the other medicine. For Januvia and Janumet - Low risk of clinically meaningful interactions with metformin and ciclosporin. Meaningful interactions would not be expected with other p-glycoprotein inhibitors. The primary enzyme responsible for the limited metabolism of sitagliptin is CYP3A4, with contribution from CYP2C8. Digoxin: sitagliptin had a small effect on plasma digoxin concentrations, and may be a mild inhibitor of p-glycoprotein in vivo. No dosage adjustment of digoxin is recommended, but monitor patients at risk of digoxin toxicity if the two are used together.Pregnancy and lactation: Do not use during pregnancy or breast-feeding. SIDE EFFECTS Refer to SmPC for complete information on side effects There have been no therapeutic clinical trials con-ducted with Janumet tablets however Janumet is bioequivalent to co-administered sitagliptin and metformin. Sitagliptin only: In stud-ies of sitagliptin 100 mg alone compared to placebo, adverse reactions considered as drug-related reported in patients treated with sitagliptin in excess (> 0.2 % and difference > 1 patient) of that in patients receiving placebo are headache, hypoglycaemia, constipa-tion, and dizziness. Also, adverse experiences reported regardless of causal relationship to medication and more commonly in pa-tients treated with sitagliptin included upper respiratory tract infection, nasopharyngitis, osteoarthritis and pain in extremity. Met-formin only: Clinical Trial Data and Post-marketing data: Very common (≥ 1/10): gastro-intestinal disorders; Common (≥ 1/100 to < 1/10): metallic taste; Very rare (< 1/10,000): urticaria, erythema; pruritis; lactic acidosis; vitamin B12 deficiency; liver function disorders, hepatitis. Sitagliptin with metformin: Common: nausea; Uncommon: somnolence; upper abdominal pain, diarrhoea, blood glucose de-creased, anorexia, weight decreased. Sitagliptin with a sulphonylurea: Common: hypoglycaemia. Sitagliptin with metformin and a sulphonylurea: Very common: hypoglycaemia; Common: constipation. Sitagliptin with a PPARγ agent (pioglitazone): Common: hypogly-caemia, flatulence, peripheral oedema. Sitagliptin with a PPARγ agent (rosiglitazone) and metformin: Common: headache, diarrhoea, vomiting, hypoglycaemia, peripheral oedema. Sitagliptin with insulin with/ without metformin: Common: headache, hypoglycaemia, influenza; Uncommon: dry mouth, constipation. Sitagliptin with metformin and insulin: very common: hypoglycaemia; uncommon: headache and dry mouth. Post-marketing experience additional side effects have been reported (frequency not known): hypersensi-tivity reactions, including anaphylaxis, angioedema, rash, urticaria, cutaneous vasculitis and exfoliative skin conditions including Stevens-Johnson syndrome (see precautions); acute pancreatitis, including fatal and non-fatal haemorrhagic and necrotizing pan-creatitis (see precautions); impaired renal function, including acute renal failure (sometimes requiring dialysis); vomiting. PACKAGE QUANTITIES Januvia 100 mg film-coated tablets 28 tablets Janumet 50mg/850mg and 50mg/1000mg film-coated tablets 56 tablets Marketing Authorisation Number Januvia 100 mg: EU/1/07/383/014 Janumet 50 mg/850 mg: EU/1/08/455/003 Janumet 50 mg/1000 mg: EU/1/08/455/010 Marketing Authorisation Holder Merck Sharp & Dohme Limited, Hertford Road, Hoddesdon, Hertfordshire EN11 9BU, UK POM Date of review of prescribing information: June 2011 © Merck Sharp & Dohme Limited,2011. All rights reserved. API.COM-BINED JANUMET/JANUVIA.JUN11.IRLReferences: 1. Goldstein BJ, Feinglos MN, Lunceford JK, et al; for the sitagliptin 036 study group. Effect of initial combination therapywith sitagliptin, a dipeptidyl peptidase-4 inhibitor, and metformin on glycemic control in patients with type 2 diabetes. Diabetes Care.2007;30(8):1979–1987. 2. Janumet SPC available at www.medicines.ie. a A randomized, double-blind, placebo-controlled, parallel-group study evaluating the combination of sitagliptin + metformin ad-
ministered as separate 50/850-mg or 50/1000-mg tablets compared with either agent alone in 1091 patients with type 2 diabetes inadequately controlled on diet and exercise (HbA1c ≥7.5% to ≤11%).1 FPG=fasting plasma glucose; PPG=postprandial glucose.
Further information is available on request from from MSD, Pelham House, South County Business Park, Leopardstown, Dublin 18 or from www.medicines.ie.
Copyright © 2010 Merck Sharp & Dohme Corp., a subsidiary of MSD, Pelham House, South County Business Park, Leopardstown, Dublin 18, Ireland. All rights reserved.
3089_JMT_A4_Ad_July2011.indd 1 14/07/2011 16:16

35
abstractsManaging blood glucose during and after exercise in type 1 diabetes: reproducibility of glucose response and a trial of a structured algorithm adjusting insulin and carbohydrate intake
Kilbride l, charlton J, Aitken g, Hill gw,
davison rc, McKnight JA.
Western General Hospital, NHS lothian and Honorary Reader,
university of Edinburgh, Edinburgh
Difficulties in managing blood glucose levels in type 1 diabetes whilst exercising is known to deter people from exercise. Currently there is a limited evidence base to aid healthcare professionals enable people with diabetes to exercise safely. This study sought to address this gap. A quasi-experimental study was under-taken amongst people with type 1 diabetes. Over 14 days, 14 participants undertook four exercise sessions (40 minutes at 50%VO(2max) ). Two sessions were undertaken in week 1 self-managing their diabetes and two sessions in week 2 using an algorithm for carbohydrate and insulin adjustment. The mean reduction of glucose levels detected by Continuous Glucose Monitoring during exercise was 3·1 (SD 2·03) mmol/l. Time spent within the range of 4-9mmol/l during exercise was not significantly different between the self-managed and the algorithm weeks (-3-22·4 min). The mean reduction of blood glucose for each individual over all four exercise sessions ranged between 0·8-5·95mmol/l. The technical error between days one and two was 2·4mmol/l (CV = 33·2%) and between days 3-4 the technical error was 2·7mmol/l (CV = 33·7%).
The results provide useful data about the reproducibility of the blood glucose response to moderate intensity exercise, despite the variability of individual responses 40 minutes of moderate intensity exercise decreases Continuous Glucose Monitoring glucose by 3mmol/l with or without a 30% decrease of insulin before exercise. This information provides valuable baseline information for people with diabetes and health care professionals who wish to encourage physical activity and undertake further research in this area.
Sex bias in studies selected for clinical guidelinesballantyne
AJ, rogers wA. Department of Primary
Health Care and General Practice, School of
Medicine and Health Sciences, Otago
university Wellington, New Zealand .
The aim of this study was to determine the proportions of female participants in research studies selected to inform the development of national clinical guidelines and to assess these against the proportions of women affected by the conditions. The authors assessed 392 published articles, involving a total of 5.2 million participants, cited as references in five influential clinical guidelines addressing the use of antiarrhythmics, chronic fatigue, depression, diabetes, and colorectal cancer. For each article, they extracted the number of female participants to determine any discrepancies in the sex of participants and if the proportion of female participants as research subjects reflected the sex distribution of patients affected by the condition. The overall and median percentages (per study) of females per guideline were: use of antiarrhythmics (35%, median 38%), chronic fatigue (70%, median 73%), colorectal cancer (67%, median 46%), depression (66%, median 66%), and diabetes (63%, median 50%). The baseline prevalence rates used for comparison purposes were (percentage female): antiarrhythmics (60% of patients 75(+) years); chronic fatigue (66%), colorectal cancer (46%), depression (66%), and diabetes (46%). The authors conclude that colorectal cancer, depression, and chronic fatigue guidelines were based on research populations that accurately reflected the sex distribution of the condition in the general population. Women were slightly overrepresented in the research studies supporting the diabetes guidelines and were significantly underrepresented in the research studies supporting the guidelines on the use of antiarrhythmics. Guideline developers should be aware of and comment on the potential impact of sex. Where the evidence base is lacking, guideline developers should highlight this and, where necessary, limit their specific conclusions to populations on whom the research was performed.
Adherence to hypoglycaemic medication among people with type 2 diabetes in primary care
white AJ, Kellar I, Prevost AT, Kinmonth
Al, Sutton S, canny M, griffin SJ.
Rookery Medical Centre, Newmarket,
Suffolk, Enlgand.
The authors sought to assess levels and correlates of adherence to hypoglycaemic medication among patients offered organised general practice diabetes care. 60 patients prescribed oral hypoglycaemic medication were recruited to a two-month prospective study. Prescribed doses taken and days on which the prescribed number of doses was taken were measured by MEMS (Medication Event Monitoring System). Overall 99.1% of prescribed doses were taken (median, IQR: 96.8-100%), this was inversely correlated with daily dose frequency (Spearman’s rho=0.37, p=0.004). Only 4 patients (6.7%) took less than 90% of pre-scribed doses. The prescribed dose was taken on 96.4% of days (median, IQR: 89.1-98.2%), this was correlated with age (rho=0.26, p=0.047) and inversely correlated with HbA(1c) levels (rho=-0.29, p=0.02) and daily dose frequency (rho=-0.33, p=0.009). Adherence to metformin was less than to other hypoglycaemic medication (Z=-3.48, p=0.0005).
The authors conclude that a dispensing practice with a well-run diabetes service can support high rates of adherence to hypoglycaemic medication. Before changing medication, low adherence might be considered as a possible cause of progressive hyperglycaemia, particularly among patients prescribed metformin more than once a day. Selective monitoring with MEMS may have a clinical as well as a research role in such people.
FocuS on: DIABETES

Calcium and/or vitamin D deficiency in the elderly can lead to lossof muscle tone and increased risk of falls and osteoporotic fractures.1-5
Calcichew-D3 Forte is indicated for the treatment and prevention of calcium and vitamin D deficiency.6
CALCICHEW-D3 FORTE CHEWABLE TABLETS PRESCRIBINGINFORMATION(Please refer to full Summary of Product Characteristicswhen prescribing) Presentation: Chewable tablet containing1250mg calcium carbonate (equivalent to 500mg of elementalcalcium) plus 400IU colecalciferol (equivalent to 10 microgramsvitamin D3). Uses: Prevention and treatment of vitaminD/calcium deficiency. Supplementation of vitamin D andcalcium as an adjunct to specific therapy for osteoporosis, inpregnancy, in established vitamin D dependent osteomalaciaand in other situations requiring therapeutic supplementation ofmalnutrition. Dosage and administration: Oral (suck orchew). Adults and elderly: Two tablets daily. Children: Notintended for use in children. Hepatic impairment: No doseadjustment required. Renal impairment: Should not be used inpatients with severe renal impairment. Contraindications:Diseases and/or conditions resulting in hypercalcaemia and/orhypercalciuria, severe renal impairment, renal stones,hypervitaminosis D, hypersensitivity to ingredient(s) especiallysoybean oil and peanut. Precautions: Monitor serum calciumand creatinine levels, particularly in patients on cardiacglycosides or diuretics and in patients with high tendency tocalculus formation. Use with caution in patients with impairedrenal function. Take into account risk of soft tissue calcification.Avoid in patients with phenylketonuria or sugar intolerance.Prescribe with caution in patients with sarcoidosis. Use with
caution in immobilised patients. Additional doses of calcium orvitamin D should only be taken under close medical supervision.Interactions: Tetracyclines (take 2 hours before, or 4 to 6 hoursafter Calcichew-D3 Forte), bisphosphonates or sodium fluoride(take 3 hours before Calcichew-D3 Forte), Quinolone antibiotics(take two hours before or after), levothyroxine (take four hoursbefore or after), thiazide diuretics, corticosteroids, cardiacglycosides, ion exchange resins (cholestyramine), laxatives(paraffin oil). Calcichew-D3 Forte should not be taken within 2hours of eating foods high in oxalic acid (e.g. spinach andrhubarb) or phytic acid (e.g. whole cereals). Side effects:Hypercalcaemia, hypercalciuria, constipation, dyspepsia,flatulence, nausea, abdominal pain, diarrhoea, pruritus, rash,urticaria. Very rarely (usually only seen on overdose) milk-alkalisyndrome. Use in pregnancy and lactation: Can be used incase of calcium and vitamin D deficiency. Daily intake inpregnancy should not exceed 1500mg calcium and 600IUcolecalciferol (15 micrograms vitamin D3). Avoid overdose aspermanent hypercalcaemia affects developing foetus. Calciumand vitamin D3 pass into breast milk so consider this whengiving additional vitamin D to the child. Pharmaceuticalprecautions: Do not store above 30°C. Keep container tightlyclosed to protect from moisture. Legal category: Pharmacyproduct. Product Authorisation No: 535/1/3. ProductAuthorisation holder: Shire Pharmaceuticals Ltd., HampshireInternational Business Park, Chineham, Basingstoke, Hampshire
RG24 8EP UK. Distributed in Republic of Ireland by: Cahill MayRoberts, P.O. Box 1090, Chapelizod, Dublin 20, Republic ofIreland. Further information is available on request. Date ofrevision: November 2010CALCICHEW is a registered trademark of Shire PharmaceuticalsLtd in the Republic of Ireland.
Adverse events should be reported to thePharmacovigilance Unit at the Irish Medicines Board (IMB)([email protected]). Information aboutadverse event reporting can be found on the IMB website(www.imb.ie). Adverse events may also be reported toShire Pharmaceuticals Ltd on +44 1256 894000.
References: 1. Perez-Lopez FR. Maturitas 2007;58: 117-137.2. Dawson-Hughes B & Bischoff-Ferrari HA. J Bone Miner Res2007; 22: S2; v59-v63. 3. Lin JT & Lane JM. Phys Med RehabilClin N Am 2005; 16: 109-128. 4. Heaney RP. Endocrinol MetabClin North Am 1998; 27(2): 255-265. 5. Hunter DJ & SambrookPN. Arthritis Res 2000; 2(6): 441-445. 6. Calcichew-D3 Forte.Summary of Product Characteristics. October 2010. 7. MIMS2011.
Date of preparation: January 2011. Item Code: IRE/CDF/11/0002
Their strength is our forte
HELP PROTECT THEFRAGILE ELDERLYNow
the lea
st expe
nsive
in cla
ss* - 4
0% le
ss tha
n
neares
t com
petito
r**7
*Referencing MIMS 2011 (calcium and vitamin Dcombination products at the indicated maintenance dose)**Referencing nearest competitor defined by market shareMAT IMS data December 2010
Calcichew Ad 2011 166x254:Layout 1 21/01/2011 11:11 Page 1

37
abstracts
Increases in dietary calcium intake in female population were not associated with further reductions in fracture risk or osteoporosis
warensjo e, byberg l, Melhus H
et al. Dietary calcium intake
and risk of fracture and osteoporosis:
prospective longitudinal cohort
study. BMJ 2011; 342:d1473 doi: 10.1136/
bmj.d1473.
Gradual increases in dietary calcium intake in a female population were not associated with further reductions in fracture risk or osteoporosis. The objective of the study was to investigate associations between long term dietary intake of calcium and risk of fracture of any type, hip fractures, and osteoporosis.
The design consisted of a longitudinal and prospective cohort study, based on the Swedish Mammography Cohort, including a subcohort, the Swedish Mammography Cohort Clinical with a population based cohort in Sweden established in 1987. The participants consisted of 61,433 women (born between 1914 and 1948) who were followed up for 19 years. Of these 5,022 women participated in the subcohort. Primary outcome measures were incident fractures of any type and hip fractures, which were identified from registry data. Secondary outcome was osteoporosis diagnosed by dual energy x-ray absorptiometry in the subcohort. Diet was assessed by repeated food frequency questionnaires.
During follow-up, 14 738 women (24%) experienced a first fracture of any type and among them 3871 (6%) a first hip fracture. Of the 5,022 women in the subcohort, 1,012 (20%) were measured as osteoporotic. The risk patterns with dietary calcium were non-linear. The crude rate of a first fracture of any type was 17.2/1000 person years at risk in the lowest quintile of calcium intake, and 14.0/1000 person years at risk in the third quintile, corresponding to a multivariable adjusted hazard ratio of 1.18 (95% confidence interval 1.12 to 1.25). The hazard ratio for a first hip fracture was 1.29 (1.17 to 1.43) and the odds ratio for osteoporosis was 1.47 (1.09 to 2.00). With a low vitamin D intake, the rate of fracture in the first calcium quintile was more pronounced. The highest quintile of calcium intake did not further reduce the risk of fractures of any type, or of osteoporosis, but was associated with a higher rate of hip fracture, hazard ratio 1.19 (1.06 to 1.32).
It was concluded from the results that gradual increases in dietary calcium intake above the first quintile in our female population were not associated with further reductions in fracture risk or osteoporosis.
Fractures at typical osteoporotic sites associated with increased mortality
S. Morin, l. M. lix,
M. Azimaee et al.
Mortality rates after incident non-traumatic fractures
in older men and women. Osteoporosis
International 2011: 22(9), 2439-2448.
Recent research has shown that fractures at typical osteoporotic sites are associated with increased mortality across all age groups, particularly in men.
Non-traumatic fractures at typical osteoporotic sites are associated with increased mortality across all age groups. Furthermore, in certain age subgroups of women and men, this rate remained elevated beyond five years for fractures of the hip, vertebrae, humerus, and other sites.
Increased mortality rates have been documented following non-traumatic hip, vertebral, and shoulder fractures. However, data are lacking as to the duration of excess mortality and whether there is increased mortality following fractures at other sites. This group determined mortality up to 15 years following incident fractures at typical osteoporotic sites.
using healthcare databases for the Province of Manitoba, Canada, individuals 50 years and older were identified with an incident non-traumatic fracture between 1986 and 2007. Each fracture case was matched to three fracture-free controls. Generalised linear models were used to test for trends in mortality and to estimate the relative risk for cases after adjusting for co-morbidity and living arrangements.
During the study period, 21,067 incident fractures were identified in men followed by 10,724 (50.1%) deaths and 49,197 incident fractures in women followed by 22,018 deaths (44.8%). Seventy-six percent of the fractures were at sites other than the hip and vertebrae. After adjustment for age, number of co-morbidities, and level of dependence in living arrangements, the risk of death in cases, relative to controls, was increased in both sexes for hip, vertebral, humerus, wrist (in men only), and other fracture sites. Post-fracture mortality was higher in men than women. Relative mortality was the highest in the younger age groups across the spectrum of fracture sites.
The authors added that better understanding of factors associated with increased post-fracture mortality should inform the development of management strategies.
FocuS on: oSTEoPoRoSIS
Help Protect Your Post-Menopausal Patients From OsteoporoticFractures
With 5600 IU
of Vitamin D
The Only Osteoporosis Therapy With 5600 IU of Vitamin D That Provides Demonstrated Fracture Prevention at the Hip and Spine,1,2
in one tablet
The Only Osteoporosis Therapy With 5600 IU of Vitamin D That Provides Demonstrated Fracture Prevention at the Hip and Spine,1,2
in one tablet Actual size
Updated NOF a guidelines recommend 800–1000 IU of vitamin D per day for adults ≥50 years 3
07-1
2-FS
P-20
10-IR
L-37
32-J
FOSAVANCE® 70 mg/2800 IU Tablets (70 mg alendronic acid as alendronate sodium trihydrate and 70 micrograms (2800 IU) colecalciferol (vitamin D3) FOSAVANCE® 70 mg/5600 IU Tablets (70 mg alendronic acid as alendronate sodium trihydrate and 140 micrograms (5600 IU) colecalciferol (vitamin D3) ABRIDGED PRODUCT INFORMATION Refer to Summary of Product Characteristics before prescribing. PRESENTATION FOSAVANCE® 70 mg/2800 IU Tablets Capsule-shaped, white to off-white tablets marked with an outline of a bone image on one side, and ‘710’ on the other, containing 70 mg alendronic acid as alendronate sodium trihydrate and 70 micrograms (2800 IU) colecalciferol (vitamin D3). FOSAVANCE® 70 mg/5600 IU Tablets Modified rectangle-shaped, white to off-white tablets, marked with an outline of a bone image on one side, and ’270’ on the other, containing 70 mg alendronic acid as alendronate sodium trihydrate and 140 micrograms (5600 IU) colecalciferol (vitamin D3). USES Treatment of postmenopausal osteoporosis in patients at risk of vitamin D insufficiency and for ’Fosavance’ 5600 for patients not receiving Vitamin D supplementation. ‘Fosavance’ reduces the risk of vertebral and hip fractures. DOSAGE AND ADMINISTRATION The recommended dose is one- tablet once weekly. Patients should be instructed that if they miss a dose of FOSAVANCE they should take one tablet on the morning after they remember. They should not take two tablets on the same day but should return to taking one tablet once a week, as originally scheduled on their chosen day. Due to the nature of the disease process in osteoporosis, ‘Fosavance’ is intended for long-term use. The optimal duration of bisphosphonate treatment for osteoporosis has not been established. The need for continued treatment should be re-evaluated periodically based on the benefits and potential risks of FOSAVANCE on an individual patient basis, particularly after 5 or more years of use. Patients must be advised to follow the instructions below: For adequate absorption of alendronate: ‘Fosavance’ must be taken with water only (not mineral water) at least 30 minutes before the first food, beverage, or medicinal product (including antacids, calcium supplements and vitamins) of the day. Other beverages (including mineral water), food and some medicinal products are likely to reduce the absorption of alendronate. The following instructions should be followed exactly in order to minimise the risk of oesophageal irritation and related reactions: • Swallow ‘Fosavance’ only upon arising for the day with a full glass of water (not less than 200 ml or 7 fl.oz.). • Patients should only swallow FOSAVANCE whole. Patients should not crush or chew the tablet or allow the tablet to dissolve in their mouths because of a potential for oropharyngeal ulceration. • Do not lie down until after the first food of the day • Do not lie down for at least 30 minutes after taking ‘Fosavance’. • Do not take at bedtime or before rising for the day. Patients should receive supplemental calcium if intake from diet is inadequate. Additional supplementation with vitamin D should be considered on an individual basis taking into account vitamin D intake from vitamins and dietary supplements. Equivalence of 2800IU of vitamin D3 weekly in ‘Fosavance’ to daily dosing of vitamin D 400 IU has not been studied. Equivalence of intake of 5600 IU of vitamin D3 weekly in FOSAVANCE to daily dosing of vitamin D 800 IU has not been studied. Use in the elderly: No dosage adjustment is necessary. Use in renal impairment: No dose adjustment is necessary for patients where GFR is greater than 35 ml/min. Alendronate is not recommended for patients with renal impairment where GFR is <35 ml/min. Use in children and adolescents: Not recommended. CONTRAINDICATIONS Oesophageal abnormalities and other factors which delay oesophageal emptying, such as stricture or achalasia. Inability to stand or sit upright for at least 30 minutes. Hypersensitivity to alendronate or to any of the excipients. Hypocalcaemia. PRECAUTIONS Alendronate can cause local irritation of the upper gastro-intestinal mucosa and potentially worsen any underlying disease. Because there is a potential for worsening of the underlying disease, caution should be used when alendronate is given to patients with active upper gastro-intestinal problems, such as dysphagia, oesophageal disease, gastritis, duodenitis, or ulcers, or with a recent history (within the previous year) of gastro-intestinal disease such as peptic ulcer, or active gastro-intestinal bleeding, or surgery of the upper gastro-intestinal tract other than pyloroplasty. In patients with known Barrett’s oesophagus, prescribers should consider the benefits and potential risks of alendronate on an individual patient basis. Oesophageal reactions (sometimes severe and requiring hospitalisation), such as oesophagitis, oesophageal ulcers and oesophageal erosions, rarely followed by oesophageal strictures, have been reported in patients receiving alendronate. Physicians should be alert to any signs or symptoms of a possible oesophageal reaction, and patients should be instructed to discontinue alendronate and seek medical attention if they develop symptoms of oesophageal irritation such as dysphagia, pain on swallowing, retrosternal pain, or new or worsening heartburn. The risk of severe oesophageal adverse reactions appear to be greater in patients who fail to take alendronate properly and/or continue to take alendronate after developing symptoms suggestive of oesophageal irritation. It is very important that the full dosing instructions are provided to, and understood by the patient. Patients should be informed that failure to follow these instructions may increase their risk of oesophageal problems. While no increased risk was observed in extensive clinical trials with alendronate, there have been rare (post-marketing) reports of gastric and duodenal ulcers, some severe and with complications. Osteonecrosis of the jaw, generally associated with tooth extraction and/or local infection (including osteomyelitis) has been reported in patients with cancer receiving treatment regimens including primarily intravenously administered bisphosphonates. Many of these patients were also receiving chemotherapy and corticosteroids. Osteonecrosis of the jaw has also been reported in patients with osteoporosis receiving oral bisphosphonates. The following risk factors should be considered when evaluating an individual’s risk of developing osteonecrosis of the jaw: potency of the bisphosphonate (highest for zoledronic acid), route of administration (see above) and cumulative dose, cancer, chemotherapy, radiotherapy, corticosteroids, smoking, a history of dental disease, poor oral hygiene, periodontal disease, invasive dental procedures and poorly fitting dentures. A dental examination with appropriate preventive dentistry should be considered prior to treatment with oral bisphosphonates in patients with poor dental status. While on treatment, these patients should avoid invasive dental procedures if possible. For patients who develop osteonecrosis of the jaw while on bisphosphonate therapy, dental surgery may exacerbate the condition. For patients requiring dental procedures, there are no data available to suggest whether discontinuation of bisphosphonate treatment reduces the risk of osteonecrosis of the jaw. During bisphosphonate treatment, all patients should be encouraged to maintain good oral hygiene, receive routine dental check-ups, and report any oral symptoms such as dental mobility, pain, or swelling. Clinical judgment of the treating physician should guide the management plan of each patient based on individual benefit/risk assessment. Bone, joint and/or muscle pain has been reported in patients taking bisphosphonates. In post-marketing experience, these symptoms have rarely been severe and/or incapacitating. The time to onset of symptoms varied from one day to several months after starting treatment. Most patients had relief of symptoms after stopping treatment. A subset had recurrence of symptoms when rechallenged with the same medicinal product or another bisphosphonate. Atypical subtrochanteric and diaphyseal femoral fractures have been reported with bisphosphonate therapy, primarily in patients receiving long-term treatment for osteoporosis. These transverse or short oblique, fractures can occur anywhere along the femur from just below the lesser trochanter to just above the supracondylar flare. These fractures occur after minimal or no trauma and some patients experience thigh or groin pain, often associated with imaging features of stress fractures, weeks to months before presenting with a completed femoral fracture. Fractures are often bilateral; therefore the contralateral femur should be examined in bisphosphonate-treated patients who have sustained a femoral shaft fracture. Poor healing of these fractures has also been reported. Discontinuation of bisphosphonate therapy in patients suspected to have an atypical femur fracture should be considered pending evaluation of the patient, based on an individual benefit risk assessment. During bisphosphonate treatment patients should be advised to report any thigh, hip or groin pain and any patient presenting with such symptoms should be evaluated for an incomplete femur fracture. Cause of osteoporosis
other than oestrogen deficiency and ageing should be considered. Hypocalcaemia must be corrected before initiating therapy with ’Fosavance’. Other disorders affecting mineral metabolism (such as vitamin D deficiency and hypoparathyroidism) should also be effectively treated before starting ’Fosavance’. The content of vitamin D in ‘Fosavance’ is not suitable for correction of vitamin D deficiency. In patients with these conditions, serum calcium and symptoms of hypocalcaemia should be monitored during therapy with ‘Fosavance’. Due to the positive effects of alendronate in increasing bone mineral, decreases in serum calcium and phosphate may occur especially in patients taking glucocorticoids in whom calcium absorption may be decreased. Colecalciferol: Vitamin D3 may increase the magnitude of hypercalcaemia and/or hypercalciuria when administered to patients with disease associated with unregulated overproduction of calcitriol (e.g. leukaemia, lymphoma, sarcoidosis). Urine and serum calcium should be monitored in these patients. Patients with malabsorption may not adequately absorb vitamin D3. Excipients: Patients with rare hereditary problems of fructose intolerance, galactose intolerance, the Lapp lactase deficiency, glucose-galactose malabsorption or sucrase isomaltase insufficiency should not take ‘Fosavance’. Drug interactions If taken at the same time, it is likely that food, beverages (including mineral water), calcium supplements, antacids, and some oral medicinal products will interfere with absorption of alendronate. Therefore, patients must wait at least 30 minutes after taking alendronate before taking any other oral medicinal product. Since NSAlD use is associated with gastrointestinal irritation, caution should be used during concomitant use with alendronate. Colecalciferol Olestra, mineral oils, orlistat, and bile acid sequestrants (e.g. cholestyramine, colestipol) may impair the absorption of vitamin D. Anticonvulsants, cimetidine and thiazides may increase the catabolism of vitamin D. Additional vitamin D supplements may be considered on an individual basis. Use in pregnancy and lactation: ’Fosavance’ is only intended for use in postmenopausal women and therefore it should not be used during pregnancy or in breast-feeding women. There are no adequate data from the use of ’Fosavance’ in pregnant women. It is not known whether alendronate is excreted into human breast milk. Colecalciferol and some of its active metabolites pass into breast milk. Fertility There are no data on fetal risk in humans. However, there is a theoretical risk of fetal harm, predominantly skeletal, if a woman becomes pregnant after completing a course of bisphosphonate therapy. EFFECTS ON ABILITY TO DRIVE AND USE MACHINES Certain adverse reactions that have been reported with FOSAVANCE may affect some patients’ ability to drive or operate machinery. Individual responses to FOSAVANCE may vary. SIDE EFFECTS Frequencies are defined as: very common (≥1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000), very rare (< 1/10,000)
Immune system disorders: Rare: hypersensitivity reactions including urticaria and angioedema
Metabolism and nutrition disorders: Rare: symptomatic hypocalcaemia, often in association with predisposing conditions
Nervous system disorders: Common: headache, dizziness† Uncommon: dysgeusia†
Eye disorders: Uncommon: eye inflammation (uveitis, scleritis, or episcleritis)
Ear and labyrinth disorders: Common: vertigo†
Gastrointestinal disorders: Common: abdominal pain, dyspepsia, constipation, diarrhoea, flatulence, oesophageal ulcer, dysphagia, abdominal distension, acid regurgitation Uncommon: nausea, vomiting, gastritis, oesophagitis, oesophageal erosions, melena† Rare: oesophageal stricture, oropharyngeal ulceration*, upper gastrointestinal PUBs (perforation, ulcers, bleeding)
Skin and subcutaneous tissue disorders:
Common: alopecia†, pruritus† Uncommon: rash, erythema Rare: rash with photosensitivity, severe skin reactions including Stevens-Johnson syndrome and toxic epidermal necrolysis‡
Musculoskeletal and connective tissue disorders:
Very common: musculoskeletal (bone, muscle or joint) pain which is sometimes severe†Common: joint swelling† Rare: osteonecrosis of the jaw‡; stress fractures of the proximal femoral shaft‡ atypical subtrochanteric and diaphyseal femoral fractures (bisphosphonate class adverse reaction)⊥
General disorders and administration site conditions:
Common: asthenia†, peripheral oedema† Uncommon: transient symptoms as in an acute-phase response (myalgia, malaise and rarely, fever), typically in association with initiation of treatment†
†Frequency in Clinical Trials was similar in the drug and placebo group. ‡This adverse reaction was identified through post-marketing surveillance. The frequency of rare was estimated based on relevant clinical trials. ⊥Identified in postmarketing experience. OVERDOSEAlendronate Hypocalcaemia, hypophosphataemia and upper gastrointestinal adverse reactions, such as upset stomach, heartburn, oesophagitis, gastritis, or ulcer, may result from oral overdose. No specific information is available on the treatment of overdose with alendronate. In case of overdose with FOSAVANCE, milk or antacids should be given to bind alendronate. Owing to the risk of oesophageal irritation, vomiting should not be induced and the patient should remain fully upright. Colecalciferol Vitamin D toxicity has not been documented during chronic therapy in generally healthy adults at a dose less than 10,000 IU/day. In a clinical study of healthy adults a 4,000 IU daily dose of vitamin D3 for up to five months was not associated with hypercalciuria or hypercalcaemia. PACKAGE QUANTITIES ‘Fosavance’ 70 mg/2800 IU Tablets 4 tablets. ‘Fosavance’ 70 mg/5600 IU Tablets 4 tablets. POM Date of review: June 2011 Date of preparation: June 2011 Marketing Authorisation numbers: ‘Fosavance’ 70 mg/2800 IU Tablets EU/1/05/310/002 ‘Fosavance’ 70 mg/5600 IU Tablets EU/1/05/310/007 Marketing Authorisation Holder: Merck Sharp & Dohme Limited, Hertford Road, Hoddesdon, Hertfordshire EN11 9BU, UK © Merck Sharp & Dohme Limited 2011. All rights reserved. API.FOS. (ART 20 & 31) AUGUST 2011 References: 1. Data on file, MSD 2. Fosavance Summary of Product Characteristics. Accessed June 2011. 3. NOF Scientific Statement. NOF Recommendations for Vitamin D available at http://www.nof.org/node/173. Accessed July 2011. a NOF=National Osteoporosis Foundation. Additional information is available on www.medicines.ie or on request from MSD Pelham House, South County Business Park, Leopardstown, Dublin 18
Pelham House, South County Business Park, Leopardstown, Dublin 18, Ireland

39
abstractscommon low-density lipoprotein receptor–related protein 5 (LRP5) gene variants associated with bone mineral density
van Meurs JbJ, Trikalinos TA,
ralston SH et al.
large-scale analysis of association between
LRP5 and LRP6 variants and osteoporosis. JAMA. 2008; 299(11): 1277-1290
Common low-density lipoprotein receptor–related protein 5 (LRP5) gene variants are consistently associ-ated with bone mineral density (BMD) and fracture risk across different white populations. Mutations in the low-density lipoprotein receptor–related protein 5 (LRP5) gene cause rare syndromes characterised by altered BMD. More common LRP5 variants may affect osteoporosis risk in the general population.
The objective of this international study was to generate large-scale evidence on whether two com-mon variants of LRP5 (Val667Met, Ala1330Val) and one variant of LRP6 (Ile1062Val) are associated with BMD and fracture risk.
It consisted of a prospective, multicentre, collaboration of individual-level data on 37,534 individu-als from 18 participating teams in Europe and North America. Data were collected between September 2004 and January 2007; analysis of the collected data was performed between February and May 2007. Bone mineral density was assessed by dual-energy x-ray absorptiometry. Fractures were identified via questionnaire, medical records, or radiographic documentation; incident fracture data were available for some cohorts, ascertained via routine surveillance methods, including radiographic examination for vertebral fractures.
Bone mineral density of the lumbar spine and femoral neck; prevalence of all fractures and vertebral fractures. The Met667 allele of LRP5 was associated with reduced lumbar spine BMD (n = 25 052 [number of participants with available data]; 20-mg/cm2 lower BMD per Met667 allele copy; P = 3.3 × 10−8), as was the Val1330 allele (n = 24 812; 14-mg/cm2 lower BMD per Val1330 copy; P = 2.6 × 10−9). Similar ef-fects were observed for femoral neck BMD, with a decrease of 11 mg/cm2 (P = 3.8 × 10−5) and 8 mg/cm2 (P = 5.0 × 10−6) for the Met667 and Val1330 alleles, respectively (n = 25 193). Findings were consistent across studies for both LRP5 alleles. Both alleles were associated with vertebral fractures (odds ratio [OR], 1.26; 95% confidence interval [CI], 1.08-1.47 for Met667 [2001 fractures among 20 488 individuals] and OR, 1.12; 95% CI, 1.01-1.24 for Val1330 [1988 fractures among 20 096 individuals]). Risk of all fractures was also increased with Met667 (OR, 1.14; 95% CI, 1.05-1.24 per allele [7876 fractures among 31 435 individuals)]) and Val1330 (OR, 1.06; 95% CI, 1.01-1.12 per allele [7802 fractures among 31 199 individuals]). Effects were similar when adjustments were made for age, weight, height, menopausal status, and use of hormone therapy. Fracture risks were partly attenuated by adjustment for BMD. Haplotype analysis indicated that Met667 and Val1330 variants both independently affected BMD. The LRP6 Ile1062Val polymorphism was not associated with any osteoporosis phenotype. All aforementioned associations except that between Val1330 and all fractures and vertebral fractures remained significant after multiple-comparison adjust-ments.
The authors found that the magnitude of the effect was modest. LRP5 may be the first gene to reach a genome-wide significance level (a conservative level of significance [herein, unadjusted P < 10−7] that accounts for the many possible comparisons in the human genome) for a phenotype related to oste-oporosis.
Doctors’ beliefs and knowledge on corticosteroid-induced osteoporosis: identifying barriers to improve prevention
duyvendak M, Naunton M,
van roon eN, brouwers Jr.
Department of Pharmacotherapy and
Pharmaceutical Care, university of Groningen,
Groningen, The Netherlands.
Despite the availability of effective treatments for the management of corticosteroid-induced osteoporo-sis (CIOP), the condition is undertreated. The authors objective was to assess prescribers’ knowledge and likely prescribing patterns concerning the diagnosis and treatment of CIOP. Another goal was to identify key barriers to the use of preventive therapy in patients using long-term corticosteroids.
The authors used a postal survey of general practitioners (GPs) and specialists in The Netherlands. The survey comprised of questions on: demographic data, perceived barriers to the use of preventive therapy for CIOP, and knowledge of diagnosis and treatment of CIOP. Case scenarios were questioned to assess practice patterns.
Responding prescribers correctly answered an average of 55% of knowledge questions and 69% of case scenarios. Multiple questions and cases showed that knowledge on the use of bone mineral density (BMD) determination was poor. BMD was determined in patients who, according to the national oste-oporosis guideline, should be treated with bisphosphonates independent of BMD. Moreover, only 18% of doctors correctly answered that the BMD cutoff in CIOP patients is a T-score of ≤-1 or ≤-1·5. Key barriers identified were: (i) GPs, significantly more than specialists, consider prescription of preventive therapy the responsibility of another doctor; (ii) discontinuation of anti-resorptive medication due to adverse effects and (iii) the reluctance to prescribe preventive therapy in patients already prescribed multiple medica-tions.
The authors concluded that doctors did not identify many barriers to the prescribing of anti-resorptive therapies. lack of knowledge, especially concerning use of BMD-results, likely led to the under-treatment of the presented patients.
FocuS on: oSTEoPoRoSIS

40
abstracts FocuS on: oSTEoPoRoSIS
The importance of taking care of osteoporosisrousière M.
Service de Rhumatologie,
Hôpital Saint-Antoine, Paris,
France.
Consequences in terms of mortality and morbidity of osteoporotic fractures are serious and recent data show that mortality related to osteoporosis is often a result of poor overall health. Prevalent fracture is one of the most important risk factors for incident fracture. The risk of subsequent fractures is highest immediately after initial fractures. It is essential to treat postmenopausal osteoporotic women who had experienced a fragility fracture. Efforts to raise awareness of osteoporosis among the general public and medical profession are essential because only a minority of women are treated after a typical osteoporotic fracture. We have effective treatments, varied and adapted to all situations encountered in clinical practice for the management of osteoporosis. All available treatments showed an effect on vertebral fractures and some demonstrated an effect on nonvertebral fractures or hip fractures. The lack of adherence is perfectly demonstrated in osteoporosis. As for all patients affected by a chronic disease, patient education should become part of the global care of patients with osteoporosis.
optimising bisphosphonate treatment outcomes in postmenopausal osteoporosis: review
rossini M, di Munno O, gatti d,
giannini S, Minisola S, varenna M, Adami S.
SourceRheumatology unit,
Department of Medicine,
university of Verona, Verona,
Italy.
This review aims to investigate ways to optimise treatment outcomes with bisphosphonate therapy of osteoporosis in general. Overall, poor adherence to bisphosphonate therapy is a major limiting factor in the treatment of osteoporosis, and is associated to a large extent with gastrointestinal adverse events. An improved patient-doctor relationship and patient motivation are critical factors to improving adherence. However, other medical interventions also play a significant role. Intermittent dosing regimens decrease gastrointestinal adverse events and improve adherence, and demonstrate at least equivalent efficacy to daily regimens. Intravenous formulations also improve gastrointestinal tolerability, and are recommend-ed in Italy for patients at high risk of this adverse event. Other recommendations in Italy to improve treat-ment outcomes include a case-finding approach to identify patients most suitable for bisphosphonate therapy, thus reducing the numbers needed to treat to avoid fractures. To facilitate this, a comprehensive assessment is advocated which incorporates bone mineral density, previous fractures, parental history of fractures, corticosteroid use and the presence of other diseases associated with secondary osteoporosis.
Amgen (Europe) GmbHDammstrasse 23, CH-6301 Zug, Switzerland.
GlaxoSmithKline,980 Great West Road, Brentford, Middlesex, TW8 9GS, UK.
Legal Category: POM. Presentation and Marketing Authorisation Number: PROLIA® 60 mg: Pack of 1 pre-filled syringe with automatic needle guard; EU/1/10/618/003. Marketing Authorisation Holder: Amgen Europe B.V., Minervum 7061, NL-4817 ZK Breda, The Netherlands. Further information is available from Amgen Limited, 240 Cambridge Science Park, Milton Road, Cambridge, CB4 0WD. Prolia® is a registered trademark of Amgen Inc.
DMB-IRL-AMG-177-2010IE/DNB/0001a/10Date of preparation: Nov 2010

41
product news
Amgen (Europe) GmbHDammstrasse 23, CH-6301 Zug, Switzerland.
GlaxoSmithKline,980 Great West Road, Brentford, Middlesex, TW8 9GS, UK.
Legal Category: POM. Presentation and Marketing Authorisation Number: PROLIA® 60 mg: Pack of 1 pre-filled syringe with automatic needle guard; EU/1/10/618/003. Marketing Authorisation Holder: Amgen Europe B.V., Minervum 7061, NL-4817 ZK Breda, The Netherlands. Further information is available from Amgen Limited, 240 Cambridge Science Park, Milton Road, Cambridge, CB4 0WD. Prolia® is a registered trademark of Amgen Inc.
DMB-IRL-AMG-177-2010IE/DNB/0001a/10Date of preparation: Nov 2010
Internet facilitates youth mental health well-being and awareness Minister of State with Responsibility for Mental Health, Kathleen lynch TD, recently launched a new study on young people’s attitudes when seeking help for mental health problems.
The research and evaluation report, learning to reach out: Young people, mental health literacy and the Internet, is the first of its kind in Ireland, and was conducted by ReachOut.com, a leading Irish youth mental health online support service that helps young people get through tough times. The report comprehensively deals with understanding and using online mental health resources safely, the mental health literacy of young people in Ireland, and the first ever ReachOut.com user-profile survey.
Some key findings in the report include:• 74% of respondents to the ReachOut.com survey reported
mild, moderate or severe levels of psychological distress;• 91% of people surveyed agreed that “anyone can experience
a mental health problem”, yet 59% of young people “wouldn’t want other people to know” if they had a mental health problem;
• Two-thirds of respondents would recommend ReachOut.com to a friend, with a similar proportion agreeing that it is “a site I can trust”;
• Of those who had spoken to a health professional in the past, 41% reported that they were “unlikely” or “very unlikely” to look for help from a health professional in the future.
Career opportunities for nurses
Janssen continues support of dermatology research. Pictured [l to r] are Siobhan Mulhern Haughey, Medical Scientific liaison, Janssen and brendan cosgrave, Account Manager, Janssen with dr gillian Murphy, consultant dermatologist beaumont Hospital and National Speciality director in dermatology who accepted a research Travel bursary awarded to dr Aine laing through the rcPI.’
Dermatology research travel bursary
OrÁN Ó MuIrÉ reSeArcH burSAryfirst Prize e1,500
The Asthma Society of Ireland invites applications for the Órán Ó Muiré Research Bursary. The focus of the 2011 awards is to support a new, nurse-led research project which when implemented will improve the quality of care delivered to
people with asthma and/or their families. This competition is open to all registered nurses in the Republic of Ireland.
PrOJecT crITerIA
Proposals must comprise a research project which will have a defined benefitor people with asthma and/or their families.
A project plan on how your new project will be implemented should also be outlined.
Previously completed projects will not be accepted in this call.
Electronic application forms and guidance notes are available from: [email protected]
or by mail to: louis Coyne, The Asthma Society of Ireland,
4th Floor, 42/43 Amiens Street, Dublin 1
The closing date for submission of projects is Friday 7th October 2011
eNTrIeS cANNOT be AccePTed AfTer THIS dATe THe JudgeS decISION IS fINAl
The Asthma Society of Ireland is dedicated to improving the health and well-being of the 470,000 people in Ireland with asthma
ORÁN Ó MUIRÉ RESEARCH BURSARYFirst Prize e1,500
The Asthma Society of Ireland invites applications for the Órán Ó Muiré Research Bursary. The focus of the 2011 awards is to support a new, nurse-led research project which when implemented will improve
the quality of care delivered to people with asthma and/or their families. This competition is open to all registered nurses in the Republic of Ireland.
PROJECT CRITERIAProposals must comprise a research project which will have a defined benefit for people with asthma
and/or their families. A project plan on how your new project will be implemented should also be outlined.
Previously completed projects will not be accepted in this call.
Electronic application forms and guidance notes are available from: [email protected]
or by mail to: Louis Coyne, The Asthma Society of Ireland, 4th Floor, 42/43 Amiens Street, Dublin 1
The closing date for submission of projects isFriday 7th October 2011
ENTRIES CANNOT BE ACCEPTED AFTER THIS DATE
THE JUDGES DECISION IS FINAL
The Asthma Society of Ireland is dedicated to improving the health and well-being of the 470,000 people in Ireland with asthma
Pictured at the launch of the Nursing Homes Ireland (NHI) brochure: rewarding career Opportunities for Nurses – working in a Nursing Home, are, from left, Professor brendan Mccormack, President of the All Ireland gerontological Nursing Association and director of the Institute of Nursing research at the university of ulster; Michael Mccoy, NHI chairperson; rena O’Hara, ryevale Nursing Home and NHI Nurse of the year;and Tadhg daly, NHI chief executive Officer. The brochure discusses the challenging and rewarding career prospects nursing homes offer nurses. It was launched at the NHI recruitment seminar, Nursing Homes: rewarding career Opportunities, which was held in the d4 Hotels (ballsbridge Inn), on Tuesday, August 23rd.

42
product news
Azithromycin Clonmel 250mg TabletsClonmel Healthcare is delighted to announce the launch of Azithromycin Clonmel 250mg tablets. This product will join our other antibiotic medicine product listings within the Ethical Prescription Division of Clonmel Healthcare.
Azithromycin Clonmel is an antibiotic belonging to a group called macrolides. It stops the growth of bacteria which cause infections by preventing the manufacture of protein in the bacteria.
Full prescribing information for Azithromycin Clonmel is available on request or go to www.clonmel-health.ie . This product is subject to medical prescription. Azithromycin Clonmel is GMS reimbursable from 1st September 2011.
Please contact Clonmel Healthcare on 01-6204000 if you require any additional information on Azithromycin Clonmel.
Gastrolief (Pantoprazole) 20mg Gastro-resistant TabletsClonmel Healthcare has nnounced the launch of Gastrolief (Pantoprazole) 20mg Gastro-resistant Tablets. This product will join our other non prescription medicine product listings within ClonMedica, the consumer division of Clonmel Healthcare.
Gastrolief is used for the short-term treatment of reflux systems (for example heartburn and acid regurgitation) in adults. Gastrolief is available in retail pharmacies.
Please contact Clonmel Healthcare on 01-6204000 if you require any additional information on Gastrolief.
letrozole 2.5mg film-coated TabletsClonmel Healthcare is delighted to announce the launch of letrozole 2.5mg film-coated tablets.
letrozole is the most recent addition to our oncology division and is used in the treatment of advanced breast cancer.
Full prescribing information for letrozole is available on request or go to www.clonmel-health.ie. This product is subject to medical prescription. letrozole is GMS reimbursable from 1st September 2011.
Please contact Clonmel Healthcare on 01-6204000 if you require any additional information on letrozole.
Takeda launches new presentation of leuprorelin acetate: Prostap DCSTakeda announced the launch of Prostap DCS (leuprorelin acetate dual chamber syringe). A new presentation of leuprorelin acetate (Prostap), a treatment for prostate cancer in men and endometriosis and uterine fibroids in women, Prostap DCS will be available in Ireland at no extra cost to the health service7 and will replace current presentations of Prostap when stocks are exhausted.
Prostap DCS is the only lHRH agonist delivered via a Dual Chamber Syringe (DCS), offering a more simple, intuitive and efficient delivery system compared to the original Prostap vial and syringe mechanism. As a result, Prostap DCS will allow healthcare professionals to have more patient-facing time.
Ms. Helen Forristal, Clinical Nurse Specialist, St. Vincent’s university Hospital, Dublin, commented, “The availability of Prostap DCS will offer a positive change to the treatment of prostate cancer. The simple device will save time in clinics while still providing the effectiveness that we see with Prostap. As a result, patient care will be improved as we will be able to deliver an effective medicine whilst spending more time with our patients, providing them with much needed support and advice.”
Prostap DCS delivers the same active ingredient contained within Prostap (leuprorelin acetate) and provides well-documented, long-term efficacy and survival outcomes in all stages of prostate cancer. It will be available in the same dosages as existing presentations: one-month Prostap SR DCS (leuprorelin acetate depot injection 3.75mg) and three-month Prostap 3 DCS (leuprorelin acetate depot injection 11.25mg). To ensure patients receive Prostap DCS as prescribed, it is necessary to reflect this important change of name on prescriptions with immediate effect to ensure patients receive continuous treatment with Prostap DCS.
Takeda has been involved with the management and treatment of prostate cancer since the discovery and development of leuprorelin acetate (Prostap) in the 1970s. As an organisation Takeda is committed to developing treatments such as Prostap DCS which offer an overall package of care: long-term efficacy and survival outcomes coupled with a simple and efficient delivery system.
Further information on Prostap DCS is available at www.ProstateCancerupdate.ie or from Takeda Medical Information contactable on [email protected] or +44 1628 537975.

43
product news
Neulasta(pegfilgrastim) and Aranesp (darbepoetin alfa): Improving needle safety for healthcare professionalsAmgen recently announced the introduction of an automatic needle guard (ANG) for Neulasta (pegfilgrastim) and Aranesp (darbepoetin alfa) prefilled syringes. The ANG will replace the current classic prefilled syringe for Neulasta indicated for the reduction in the duration of neutropenia and the incidence of febrile neutropenia in patients treated with cytotoxic chemotherapy for malignancy (with the exception of chronic myeloid leukaemia and myelodysplastic syndromes), and Aranesp for the treatment of symptomatic anaemia associated with chronic renal failure (CRF) in adults and paediatric patients, and the treatment of symptomatic anaemia in adult cancer patients with non-myeloid malignancies receiving chemotherapy.
According to the Health Information and Quality Authority (HIQA), an estimated 6,000 needle-stick injuries occur per year in Ireland, with up to 70% of these going unreported. It is anticipated that the introduction of the ANG to these products will reduce the risk of needle stick injuries for doctors, nursing staff and patients.
The transition to ANG will commence from the end of May 2011 however please note the ANG will only become available once all stocks of classic prefilled syringes have been depleted. unfortunately, Amgen cannot accept the return of cold chain products, however in order to prevent any product wastage, Amgen is working closely with all wholesalers during this transition phase.
The Aranesp10μg pre-filled syringe is unchanged and all strengths of Aranesp SureClick have an existing automatic needle guard and therefore remain unchanged. This wide range of Aranesp presentations allows healthcare professionals to select the best option for their needs and those of their patients.
For further information please contact Amgen Ireland ltd on 01-8527400. For medical queries, please contact the Medical Information department on 1800 88 29 61.
No 1. OTC Brand in Pharmacy* launches New Nurofen Express Nurofen, the No 1 selling OTC brand*, has just launched the most anticipated product of the year – Nurofen Express. As with all Nurofen products, new Nurofen Express is a pharmacy only product and targets pain twice as fast **.
The new Nurofen Express range will comprise of two unique new products: Nurofen Express 200mg tablets, available in packs of 12 & 24, and Nurofen Express Maximum Strength 400mg tablets – a one tablet dose solution and the only 400mg Ibuprofen tablet available OTC (also available in packs of 12 & 24).
The launch will be supported by a €1m marketing investment – making it the biggest OTC launch in pharmacy in recent years. The integrated consumer campaign will feature TV, outdoor, radio, digital advertising and huge consumer promotion – all driving consumers into your pharmacy.
The launch will also include first-in-class point-of-sale and training materials which are available to all pharmacies.
* Source : IMS OTC value sales MAT 2010** compared to standard Ibuprofen
la Roche-Posay Cicaplast – Epidermal Repair Accelerator
Speed up the skin’s repair process with this pro-recovery cream that protects the skin and stimulates the renewal of the damaged cells.
A triple action product for optimal healing – it works to protect from irritation, prevent bacterial infections and accelerates the repairing process for skin healing. use it on scrapes and cuts, bites, minor burns, dry patches, sunburn, cuticles and cracked heels.
A glide-on formula to ensure even spreading
Resists water and rubbing Moisturizing and non-sticky texture Allows easy make-up application while
enhancing recovery process. Result – soothed, protected and stimulated – the skin repairs rapidly with superior results.

44
product news
Actavis Ireland is delighted to announce the addition of Rosuvastatin Film-coated tablets to the company’s ever-growing product portfolio.
Rosuvastatin Actavis is a prescription only product and is indicated for primary hypercholesterolaemia (type IIa) or mixed dyslipidamia (type IIb) as an adjunct to diet when response to diet and other non-pharmacological treatments (e.g. exercise, weight reduction) is inadequate.
Rosuvastatin from Actavis is available in the following presentations.
Trade Price GMS Code
5mg x 28 film coated tablets €16.19 62830
10mg x 28 film coated tablets €19.91 62831
20mg x 28 film coated tablets €32.48 62832
40mg x 28 film coated tablets €33.36 62833
Annual Pharmacy Prize-giving Awards at uCCOn Thursday 16th June, university College Cork held their annual summer graduation conferring ceremony for the Bachelor of Pharmacy degree programme at the School of Pharmacy, uCC. Following the graduation ceremony, the Annual Pharmacy Prize-giving Awards took place in the stunning Aula Maxima. The Actavis Prize for Excellence in Pharmaceutics was awarded to top student Maria Donovan. Maria had achieved the highest mark in Pharmaceutics and drug delivery over the four year pharmacy degree.
Speaking at the event Actavis Ireland, Marketing Director Irene Sheehan said that “Actavis are delighted to be able to sponsor such a prestigious prize and are committed to supporting the work of Irish Healthcare Professionals at all levels. Maria is a worthy winner and has showed great dedication throughout her four years in uCC. On behalf of all at Actavis I would like to extend our congratulations to Maria and all the other graduates & wish them well in their future careers. Actavis Ireland looks forward to working closely with uCC on various projects in the coming months and years ahead”
Speaking at the event Dr Brendan Griffin, lecturer in Pharmaceutics said “The School of Pharmacy would like to acknowledge Actavis Ireland for their generous sponsorship of this prize, and for their continued interest in supporting uCC programmes. In particular I would like to thank Ms Irene Sheehan, Marketing Director, for taking the time out to present this award”
brendan griffin, lecturer, School of Pharmacy, Irene Sheehan Marketing director, Actavis Ireland, Maria donovan and Professor John Higgins, Head of college of Medicine & Health.
Pradaxa shows significant reduction in the risk of stroke in patients with atrial fibrillation New data from two RE-lY trial sub-group analyses show that dabigatran etexilate 150mg bid consistently reduces the risk of stroke in atrial fibrillation (AF) compared to well-controlled warfarin, irrespective of whether patients use antiplatelet or other concomitant therapies, such as the anti-arrhythmics amiodarone or verapamil. The relative benefits of dabigatran etexilate over well-controlled warfarin in the overall results of RE-lY were consistent across patients using these concomitant treatments . The data was presented at the European Society of Cardiology (ESC) Congress 2011.
Dabigatran etexilate is the only novel oral anticoagulant approved for stroke prevention in AF. Dabigatran etexilate 150mg bid has been shown to be superior to well-controlled warfarin (median TTR 67%5,6) in an intention to treat analysis. These groundbreaking results were demonstrated in RE-lY, a PROBE trial (prospective, randomized, open-label with blinded endpoint evaluation), comparing two fixed doses of the oral direct thrombin inhibitor dabigatran etexilate (110mg and 150mg bid) each administered in a blinded manner, with open label warfarin.
The new findings are significant because the long time standard of care warfarin is known to interact with numerous medications, including many common co-medications metabolised via the cytochtrome P450 pathway. In addition, approximately one in five patients with AF are being prescribed antiplatelet therapy alongside warfarin for conditions such as coronary artery disease, acute coronary syndrome, or recent coronary artery stenting.8The safety of antiplatelet therapy in combination with anticoagulants has been a physician concern, with the combination shown to increase major bleeding over the use of anticoagulation alone.
Prof. Antonio Dans, Department of Medicine, university of the Philippines College of Medicine said, “Even though combining antiplatelets with an anticoagulant bears the risk of increased bleeding, it is often required in AF patients with coronary artery disease. The new results are thus an important finding for clinical practice, because they show that the benefits of dabigatran etexilate over warfarin for the prevention of stroke in AF remain unchanged when patients use concomitant antiplatelet therapy.”
Actavis launches Rosuvastatin in IrelandRosuvastatin is an important product launch for Actavis. It
further demonstrates the group’s commitment to providing long term sustainable value across a broad product portfolio.
Actavis continues to develop a competitively priced, broad portfolio of products. Additional launches and line extensions are yet to come this year which will further underline Actavis’s current position as the fastest growing generic company on the Irish market.
For further information on the Actavis portfolio please contact us in Cork today on 1890 33 32 31 or email on [email protected]

45
crossword
Name:
Address:
Email:
Congratulations to the winner of last month’s crossword, Rosemary Bradley, Kilfoylan, Moate, Co Westmeath.
Please send your answers to the Editor, Nursing in General Practice, GreenCross Publishing, 7 Adelaide Court, Adeliade Road, Dublin 2. Closing date for entries: 1st November 2011.Winner will receive v50. Please note: the winners’ cheques will be sent out within 45 days.
Caltrate is a trademark. PA 172/38/1. Full prescribing information available from Wyeth Consumer Healthcare, Plaza 254, Ballycoolin, Dublin 15 or from www.medicines.ie
Across
1 Subtlety of ace nun (6)4 Frolicking lamb produces salve (4)8 dotdotdot dashdashdash dotdotdot,
according to Morse! (3)9 Mix me a less spotty condition (7)10 Relating to the end of the alimentary canal (4)11 Cherub seen from a different angle (5)14 It’s cruel that it could be peptic or hypostatic
(5)16 It secretes milk, but that’s an udder matter (4)18 unisil N treatment for diabetes (7)20 Hard water? (3)21 It is devoid of feeling (4)22 Mr. Hyde’s doctor? (6)
down1 Bouquet of a facial feature? (4)2 In play, poison associated with old lace (7)3 It’s got the hump! (5)5 A boring law, perhaps (3)6 Mussel, we hear, can be impaired by dystrophy
(6)7 A rat returns for a royal hill (4)12 Seriousness attributed to Newton? (7)13 One may get foot-sore in this bally place in
Kerry! (6)15 There’s bread in petrol lorries! (4)16 Stressed by the past, present or future? (5)17 A clanger in label layout! (4)19 America’s uncle! (3)
ANSwerS TO lAST MONTH’S crOSSwOrdAcross: 1 German , 4 Tomb, 8 Web, 9 Measles, 10 Clot, 11 Credo, 14 Award, 16 Hulk, 18 Vesicle, 20 Pad, 21 Soap, 22 Gaiety. down: 1 Gown, 2 Rubella, 3 Admit, 5 Oil, 6 Bishop, 7 Talc, 12 Eclipse, 13 Naevus, 15 Duck, 16 Hyena, 17 D day, 19 Spa.
1 2 3 4 5 6
7
8 9
10 11 12
13
14 15 16
22
17
18 19
21
20

Visit our website www.nutricia.ie
ON
-JU
NE
11-0
1
For further information, samples and patient information, call our customer care team on Freephone 1800 923 404
Nutricia Medical, Block 1, Deansgrange Business Park, Deansgrange, Co. Dublin. Email: [email protected]
Do your patients tire of milk and juice supplements?
pudding supplement 1
most loved
Ireland’s
#1
Try the perfect anytime supplement... High energy and protein
(200kcal & 11.9g protein per serving)
Easy to swallow and digest
Convenient and patient-friendly
4 great tasting flavours
Great alternative to nutritional drinks
and in just 7 easy spoonfuls!
Reference: 1. IMS Data, May 2011.
3
3
3
3
3