donor selection: sibling. prof miguel a sanz
TRANSCRIPT

MIGUEL A SANZ, MDValencia, Spain
• Professor and Head of Department, of Oncology, Hematology and Bone Marrow Transplant Unit, University Hospital La Fe in Valencia, Spain
• Professor Sanz is chairman of the Spanish PETHEMA Group and leads the working parties of acute promyelocytic leukemia, acute myeloid leukemia and infections in neutropenic patients. He is currently a reviewer for numerous high-profile medical journals including all top hematology journals, and has authored more than 470 peer-reviewed papers, numerous book chapters, and in excess of 1000 abstracts at national and international meetings. Professor Sanz has also lectured widely in Europe, North, central and South America, as well as in Middle East and Asia, serving as lecturer at the American Society of Hematology in 2004, 2005 and 2010.

Donor selection for hematopoietic cell transplantation when a matched
sibling donor is available
The 6th International Hematologic Malignancies Conference: Bridging the Gap 2015 (BTG2015)
Beijing, China (January 31, 2014)
Miguel A. SanzDepartamento de Medicina de la Universidad de Valencia
Servicio de Hematología y HemoterapiaHospital Universitario La Fe
Valencia, Spain

• Requirements for donating bone marrow or blood for HCT.
• Variables to be considered in donor selection:
- Age of the donor
- Sex and parity
- CMV status
- ABO compatibility
• Bone marrow versus peripheral blood as source for allogeneic HSCT from HLA-identical sibling donor
Donor selection for HSCTOutline
3
Donor selection for HCTRequirements for donating BM/PB for HCT
4
• The donor must be in good health that permits the safe collection of the cells from either bone marrow or peripheral blood:
– Adequate cardiac, pulmonary, hepatic, and renal function.
– If being considered for bone marrow harvest, the donor must be able to tolerate anesthesia (either general or regional).
– For sibling donors with a history of a malignant condition, a five-year disease-free period without recurrence is usually considered adequate for subsequent collection.

Donor selection for HCTRequirements for donating BM/PB for HCT
5
• Donors must be negative for both anti-HIV antibodies and HIV RNA.
• Serologic tests for hepatitis B and C are also required at most transplant centers.
• Donors with active viral hepatitis are usually excluded, although exceptions are occasionally made with sibling donors, depending upon the clinical urgency.
• In certain circumstances, antiviral therapy may be considered if time permits for an adequate course1.
1. Strasser SI, McDonald GB. Hepatitis viruses and hematopoietic cell transplantation: A guide to patient and donor management.Blood. 1999;93(4):1127

Donor selection for HCT when ≥2 HLA-matched siblings are available
6
Sibling donors and recipients are usually of similar age

Having a younger-adult donor was a predictor of less GVHD, better OS and DFS.
Matched sibling donorsThe effect of donor age
7Kollman C et al. Blood 2001;98:2043-2051

8
Would it be better to choose a young, matched unrelated donor instead of
an older-aged sibling?
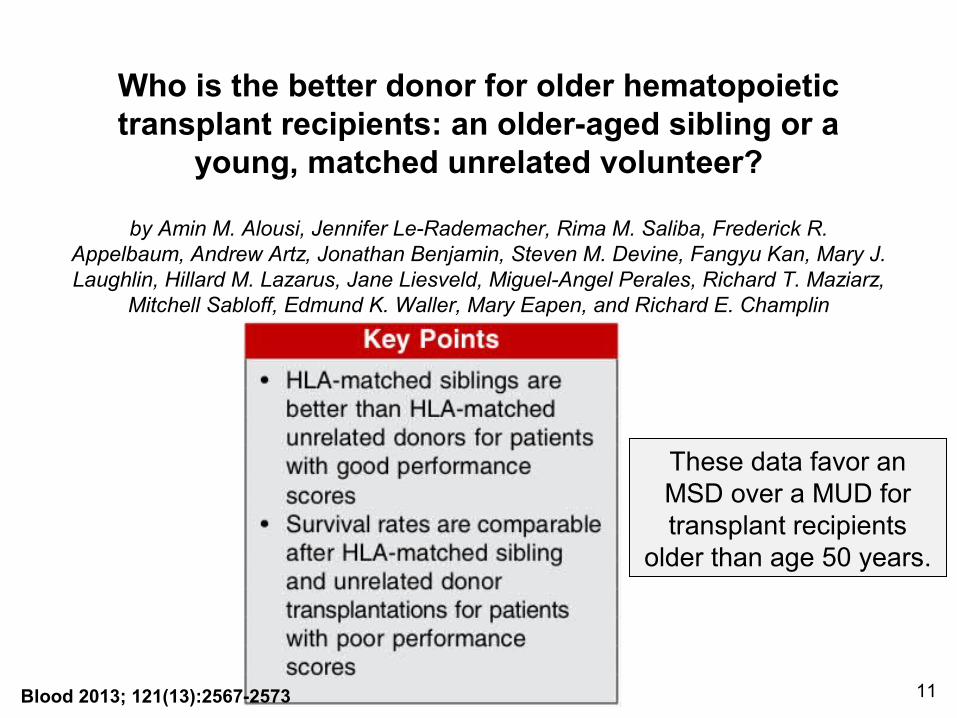
Who is the better donor for older hematopoietic transplant recipients: an older-aged sibling or a
young, matched unrelated volunteer?
by Amin M. Alousi, Jennifer Le-Rademacher, Rima M. Saliba, Frederick R. Appelbaum, Andrew Artz, Jonathan Benjamin, Steven M. Devine, Fangyu Kan, Mary J. Laughlin, Hillard M. Lazarus, Jane Liesveld, Miguel-Angel Perales, Richard T. Maziarz,
Mitchell Sabloff, Edmund K. Waller, Mary Eapen, and Richard E. Champlin
BloodVolume 121(13):2567-2573
March 28, 2013
These data favor an MSD over a MUD for transplant recipients
older than age 50 years.
11Blood 2013; 121(13):2567-2573
Donor selection for HCT when ≥2 HLA-matched siblings are available
12

Matched sibling donorsThe effect of donor sex and parity
13Kollman C et al. Blood 2001;98:2043-2051
The sex of neither donor nor recipient affected survival.

Matched sibling donorsThe effect of donor sex and parity
14Kollman C et al. Blood 2001;98:2043-2051
The cumulative incidence of chronic GVHD was higher with multiparous female donors.

Donor selection for HCT when ≥2 HLA-matched siblings are available
15

CMV serostatus still has an important prognostic impact in de novo acute leukemia patients after
allogeneic stem cell transplantation: a report from the Acute Leukemia Working Party of EBMT
by Martin Schmidt-Hieber, Myriam Labopin, Dietrich Beelen, Liisa Volin, Gerhard Ehninger, Jürgen Finke, Gerard Socié, Rainer Schwerdtfeger, Nicolaus Kröger, Arnold Ganser, Dietger Niederwieser, Emmanuelle Polge, Igor W. Blau, and Mohamad Mohty
BloodVolume 122(19):3359-3364
November 7, 2013
16
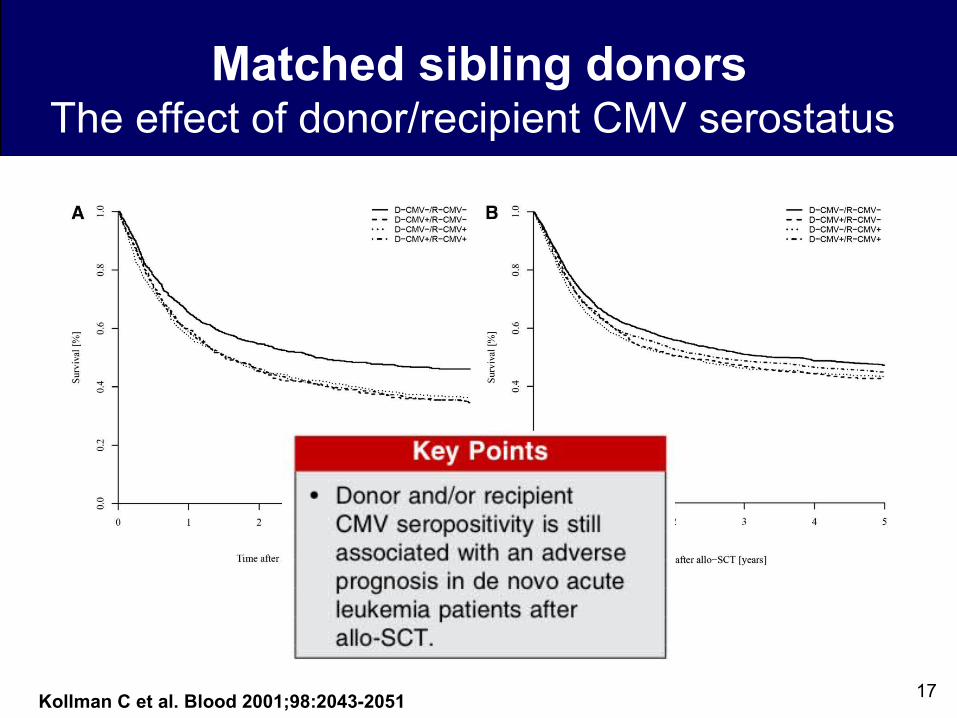
Matched sibling donorsThe effect of donor/recipient CMV serostatus
17Kollman C et al. Blood 2001;98:2043-2051

Donor selection for HCT when ≥2 HLA-matched siblings are available
19

Matched sibling donorsThe effect of ABO and Rh compatibility
20
• Donor-recipient Rh mismatch is not a risk factor in allo-HCT and does not affect transplant outcomes.
• ABO compatibility between the donor and recipient is not required:
- If major mismatches are present, additional manipulation of the hematopoietic cell product, such as depleting the product of red cells, is required.
- Hemolysis, delayed erythropoietic engraftment, and pure red cell aplasia may complicate ABO-incompatible transplantation after either marrow or PBPC transplantation. However, these complications are not common.
- A meta-analysis with 1208 cases demonstrates no adverse association between any ABO mismatching and survival.

Matched sibling donorsThe effect of ABO and Rh compatibility
21
Among related stem cell recipients, ABO matching had no significant influence on OS
Kanda J, et al.Transfusion. 2009;49(4):624.

Donor selection for HCT when ≥2 HLA-matched siblings are available
22
younger donor age preferable
matching for CMV status preferred
males and nulliparous females preferredPreferred
No>minor>major mismatches

23
Peripheral Blood versus Bone Marrow as a Source for Allogeneic
Hematopoietic Cell Transplantation from Matched-Sibling Donor

Donor selection for HCT when ≥2 HLA-matched siblings are available
24

BM vs. PB allogeneic hematopietic stem cell transplantation
• PBSC is the optimal stem cell source in terms of both overall and quality-adjusted life expectancy, except in conditions with a very low relapse probability, in which BM provides optimal outcomes:
- Severe aplastic anaemia
- Congenital marrow failures
- Malignancies with <5% risk of relapse at 1 y
Holtick U, et al. Cochrane Database Syst Rev. 2014 25

• High-quality evidence that overall survival following allo-HSCT using the current clinical standard stem cell source - PBSC - was similar to BMSC in adults with hematological malignancies.
• Moderate-quality evidence that PBSCT was associated with:
- faster engraftment of neutrophils and platelets
- higher risk of GvHD (in terms of more overall and extensive chronic GvHD).
• Quality of life, which is severely affected by GvHD, was not evaluated.
BM vs. PB allogeneic hematopietic stem cell transplantation
Holtick U, et al. Cochrane Database Syst Rev. 2014 26

27

Allogeneic HCT from HLA-identical sibling by stem cell source in Spain
28
PB 83%PB 83%
