does gilbert's disease exist?
TRANSCRIPT
363
The pathogenesis of intra-islet fibrosis in I.D.M. is unknown.This change may represent an injury to the islet cells resultingfrom a transplacental transfer of maternal anti-insulin anti-bodies,2 although the mothers of 4 of the I.D.M. with isletfibrosis had never received insulin before delivery. Hultquistand Olding suggest that the fibrosis may be associated withprevious eosinophilic cell infiltrates, consistent with the
frequently reported finding of islet eosinophilia in I.D.M. How-ever, we did not find increased eosinophilic cell infiltrate in theislets of the t.D.M. Furthermore, we noted significant intra-isletfibrosis in babies less than 24 h old, a time when the eosinophi-lic infiltrate is reported to be most prominent.2,3Our findings and those of Hultquist and Olding’ lead us to
speculate that there may be greater damage to the islets ofI.D.M. in utero than has been previously appreciated.Departments of Pathologyand Obstetrics-Gynecology,
University of Southern CaliforniaSchool of Medicine,and Women’s Hospital,
Los Angeles, California
L. NELSONS. TURKELI. SHULMANS. GABBE
PROPRANOLOL INFLUENCES SERUM T3 ANDREVERSE T3 IN HYPERTHYROIDISM
SIR,-The use of propranolol in the treatment of hyperthyr-oidism has often been discussed in The Lancet.4-7 In most stu-dies clinical improvement has not been associated with a de-crease in thyroid function measured by thyroidal 13’I uptakeand serum-protein-bound-iodine. A decrease in serum-T3 inhyperthyroid patients during propranolol therapy89 suggests a
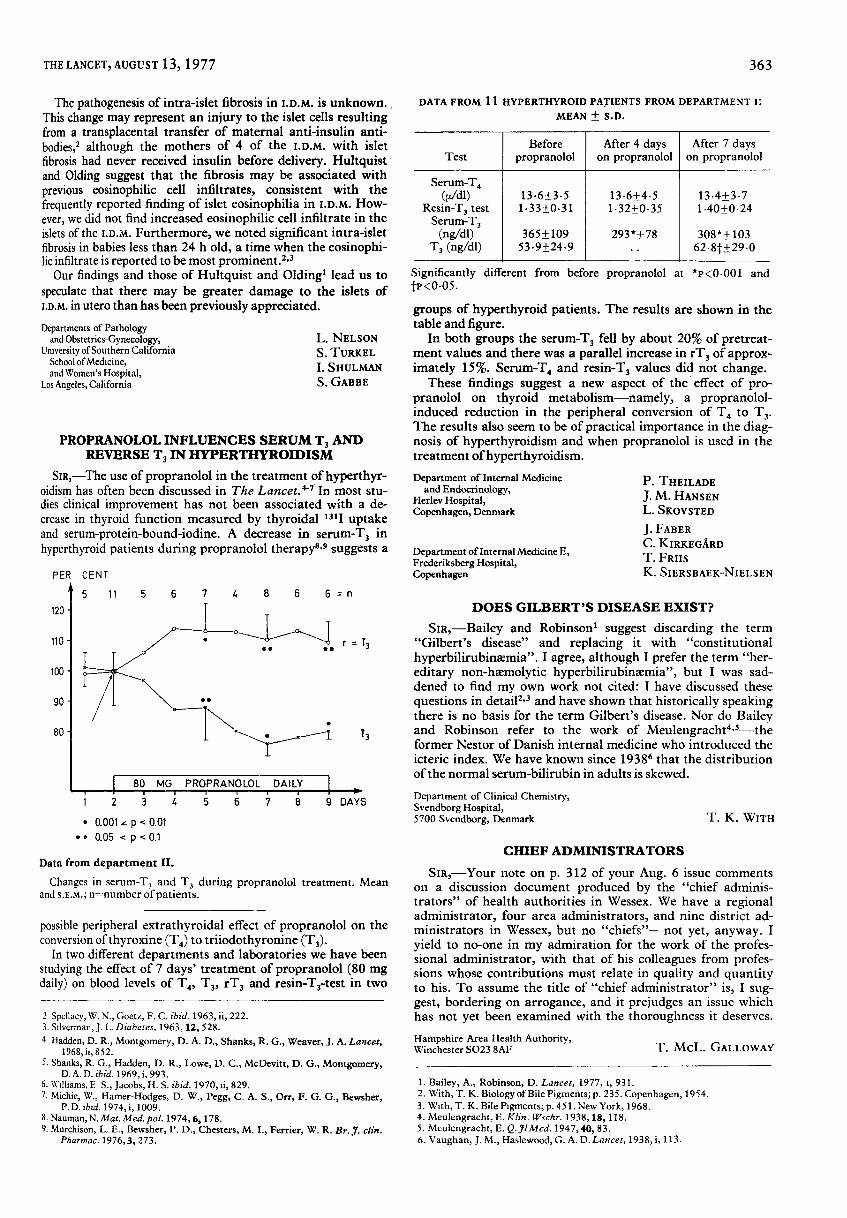
Data from department II.
Changes in serum-TJ and TJ during propranolol treatment. Meanand S.E.M.; n=number of patients.
possible peripheral extrathyroidal effect of propranolol on theconversion of thyroxine (Td) to triiodothyronine (T3)’
In two different departments and laboratories we have beenstudying the effect of 7 days’ treatment of propranolol (80 mgdaily) on blood levels of T4, T3, rT3 and resin-T3-test in two
2 Spellacy, W. N., Goetz, F. C. ibid. 1963, ii, 222.3. Silverman, J. L. Diabetes, 1963,12, 528.4 Hadden, D. R., Montgomery, D. A. D., Shanks, R. G., Weaver, J. A. Lancet,
1968, ii, 852.5. Shanks, R. G., Hadden, D. R., Lowe, D. C., McDevitt, D. G., Montgomery,
D. A. D. ibid. 1969, i, 993.6. Williams, E S., Jacobs, H. S. ibid. 1970, ii, 829.7. Michie, W., Hamer-Hodges, D. W., Pegg, C. A. S., Orr, F. G. G., Bewsher,
P. D. ibid. 1974, i, 1009.8. Nauman, N. Mat. Med. pol. 1974, 6, 178.9. Murchison, L. E., Bewsher, P. D., Chesters, M. I., Ferrier, W. R. Br. J. clin.
Pharmac. 1976, 3, 273.
DATA FROM 11 HYPERTHYROID PATIENTS FROM DEPARTMENT I:MEAN ± S.D.
i I I
Significantly different from before propranolol at *P<0001 andtop<0.05.
groups of hyperthyroid patients. The results are shown in thetable and figure.
In both groups the serum-T3 fell by about 20% of pretreat-ment values and there was a parallel increase in rT3 of approx-imately 15%. Serum-T4 and resin-T3 values did not change.
These findings suggest a new aspect of the effect of pro-pranolol on thyroid metabolism-namely, a propranolol-induced reduction in the peripheral conversion of T4 to T3.The results also seem to be of practical importance in the diag-nosis of hyperthyroidism and when propranolol is used in thetreatment of hyperthyroidism.Department of Internal Medicine
and Endocrinology,Herlev Hospital,Copenhagen, Denmark
Department of Internal Medicine E,Frederiksberg Hospital,Copenhagen
P. THEILADEJ. M. HANSENL. SKOVSTED
J. FABERC. KIRKEGÅRDT. FRIISK. SIERSBAEK-NIELSEN
DOES GILBERT’S DISEASE EXIST?
SIR,-Bailey and Robinson’ suggest discarding the term"Gilbert’s disease" and replacing it with "constitutional
hyperbilirubinsemia". I agree, although I prefer the term "her-editary non-haemolytic hyperbilirubinaemia", but I was sad-dened to find my own work not cited: I have discussed these
questions in details and have shown that historically speakingthere is no basis for the term Gilbert’s disease. Nor do Baileyand Robinson refer to the work of Meulengrachf*’—theformer Nestor of Danish internal medicine who introduced theicteric index. We have known since 19386 that the distributionof the normal serum-bilirubin in adults is skewed.
Department of Clinical Chemistry,Svendborg Hospital,5700 Svendborg, Denmark T. K. WITH
CHIEF ADMINISTRATORS
SIR,-Your note on p. 312 of your Aug. 6 issue commentson a discussion document produced by the "chief adminis-trators" of health authorities in Wessex. We have a regionaladministrator, four area administrators, and nine district ad-ministrators in Wessex, but no "chiefs"-not yet, anyway. Iyield to no-one in my admiration for the work of the profes-sional administrator, with that of his colleagues from profes-sions whose contributions must relate in quality and quantityto his. To assume the title of "chief administrator" is, I sug-gest, bordering on arrogance, and it prejudges an issue whichhas not yet been examined with the thoroughness it deserves.
Hampshire Area Health Authority,Winchester SO23 8AF T. MCL. GALLOWAY
1. Bailey, A., Robinson, D. Lancet, 1977, i, 931.2. With, T. K. Biology of Bile Pigments; p. 235. Copenhagen, 1954.3. With, T. K. Bile Pigments; p. 451. New York, 1968.4. Meulengracht, E. Klin. Wschr. 1938, 18, 118.5. Meulengracht, E. Q. Jl Med. 1947, 40, 83.6. Vaughan, J. M., Haslewood, G. A. D. Lancet, 1938, i, 113.