dod resource management -...
TRANSCRIPT

5-1September 2011
DoDResource Management
Walt W. Tinling, FACHE, CDFM-AVice President for Finance and Administration Principal Business Officer, F. Edward Hébert School of MedicineClinical Professor, Preventive Medicine and Biostatistics, Uniformed Services University [email protected]

5-2
Disclosures
• Walter W. Tinling (presenter) has no financial interest to disclose.
• This continuing education activity is managed and accredited by Professional Education Services Group in cooperation with the MedXellence Program. PESG, and MedXellence Staff, and accrediting organization do not support or endorse any product or service mentioned in this activity. PESG and MedXellence Program staff has no financial interest to disclose.

5-3
• At the conclusion of this activity, the participant will be able to:
Describe the: Military Health System, Services, and Medical Treatment Facility budget processes
Discuss the history and current state of play of the TRICARE contracts
Describe the current plans to resource for value, aka “pay for performance”
Learning Objectives
5- 3

5-45- 4

5-5
Total Federal Revenues
Personal Income Tax Payroll TaxCorporate Income Tax Excise, Estate, and other
33%
47%
9%
11%
Based on 2015 data

5-6
Total Federal Spending
Interest on the Federal Debt Discretionary SpendingMandatory Spending
65%
29%
6%
Based on 2015 data

5-7
Total Federal Spending
Military Veterans BenefitsHousing InternationalEnergy & Environment ScienceTransportation Food & AgricultureEducation GovernmentMedicare and Health
54%
Based on 2015 data
A

5-8
The Resource Management Process
• Planning• Programming• Budgeting• Accounting• Analysis and Reporting
5- 8

5-9
Planning• Mission, Vision, Organization Goals
• Strategic Planning
• Financial Planning
• Operational Planning
5- 9
5-10Critical Decision Making for Medical Executives: Keys to Improving Healthcare Delivery
DoD Resource Planning • Planning, Programming, and Budgeting
System (PPBS)• Created under the Kennedy Administration• Robert McNamara and the “Whiz Kids”
• Sometimes called PPBES • E for Execution• Robert Hale former OSD Comptroller “lets
put the big E back into PPBES”
5- 10

5-11
DoD Priorities for 2012• Assure allies and friends• Dissuade future military competition• Deter threats and coercion against U.S.
interests• If deterrence fails, decisively defeat any
adversary
5- 11

5-12
DoD Priorities for 2013• Prevail in today’s wars• Prevent and deter conflict• Prepare to defeat adversaries and succeed in
a wide range of contingencies• Preserve and enhance the All-Volunteer
Force• Reform the business and support functions of
the defense enterprise
5- 12

5-13
DoD Priorities for 2014• Act as Good Stewards of Taxpayer Dollars• Implement & Deepen Program Alignment to
New Strategic Guidance• Seek a Ready Force• People are Central
5- 13

5-14
DoD Priorities for 2015• Seek a Balanced Force• Prepare for Prolonged Readiness Challenges• Continue to Focus on Institutional Reform• Pursue Compensation Changes• Pursue Investments in Military Capabilities
5- 14

5-15
DoD Priorities for 2016• Seek a Balanced Force• Manage Enduring Readiness Challenges• Continue to Focus on Institutional Reform• Pursue Investments in Military Capabilities• Provide for People• Support Overseas Contingency Operations
5- 15

5-16
DoD PPBES• Provide the DoD with the most effective mix of
forces, equipment, manpower and support within fiscal constraints
• Aligns resources to prioritized capabilities based on strategy while balancing warfighting capabilities with risk, affordability and effectiveness
5- 16

5-17
DoD PPBES• A rigorous process to:
• Allocate resources -- among competing programs -- while considering perceived threats
• A repetitive cumbersome process ensures due process• Direct logic path from war plans to execution of
programs in the field• Multiple forums and hearings prior to final
decision• Requirements Driven
5- 17

5-18
PPBES
PLANNING BUDGETINGNATIONAL
SECURITY STRATEGY
CINCsAGENCIESSERVICES
WORLDSITUATION
NATIONALMILITARYSTRATEGY
OSDPLANNING
DHP MPG
DECISIONS
PROGRAMOBJECTIVES
MEMORANDUM(POM)
OSD - CAPEREVIEW
BUDGETPREPARATION/
REVIEW
OSD/OMBBUDGETSUBMIT
OSD COMP/OMBREVIEW
RESOURCEMANAGEMENT
DECISION(RMD)
PRESIDENT’SBUDGET
CONGRESS
APPROPRIATION
EXECUTE
FYBUDGET
PROGRAMMING
NATIONALDEFENSE
STRATEGY
STRATEGIC/JOINTPLANNING
GUIDANCE (SPG/JPG)&
FISCALGUIDANCE
PROGRAM DECISION
MEMORANDUM(PDM)
JOINT STAFFASSESSMENTS
ASSESSMENTS
$ 2-3 yrs in future$ 2-7 yrs in futureFuture Strategy Today
MTF/DTF
5- 18

5-19
PPBES Timeline
FY16 FY17 FY18 FY19 FY20 FY21 FY22 FY23
Programming YearsFuture Years Defense Plan (FYDP)
BudgetYear
ExecutionYear POM 19
5- 19
PPBES Timeline
President submits first Monday in February

5-205- 20
“The POM”

5-21
POM Wisdom
• “Most educated people know that the worst potential competition for any young organisms can come from its own kind……...They have the same requirements.”
• Frank Herbert, Dune
5- 21
5-22
POM Wisdom (cont)
• You can’t win, and you can’t not play• You can’t consult enough• If you aren’t dressed and on the bench
the coach can’t put you in • And “get a helmet on and get in the
game”
5- 22

5-23
POM Consequences
To many the glass is half empty…to others it is half
full
To a POM mechanic you have twice as much glass
as you need
5- 23

5-24
Creating the President’s Budget
• Administration provides guidelines (targets, limits) to federal agencies
• Agencies prepare budget requests
• OMB review and consolidation5- 24
5-25

5-26

5-27

5-28

5-29
Congressional Committees of Interest
• Budget• Revenue
• Ways and Means (House)• Finance (Senate)
• Appropriations• Authorizations
5- 29
5-30
Congressional Legislative Framework
U.S. Constitution - Article 1
• Section 8: The Congress shall have power to…provide for the common defense and general welfare...
• Section 9: ...No money shall be drawn from the treasury, but in consequence of appropriations made by law...
5- 30

5-31Critical Decision Making for Medical Executives: Keys to Improving Healthcare Delivery 4-31

5-32
Defense Related Appropriations & Authorizations
• Appropriations• HAC• SAC• Subcommittees
common to both:• Defense• Milcon/VA• Energy & Water• HHS/Labor/Education• Homeland Security
• Authorization• HASC• SASC
5- 32

5-335- 33

5-34
Federal Budget Process• Budget Formulation
• Congressional Action
• Budget Execution
• Review and Audit5- 34

5-35
Congressional Actions• Budget Resolution
• Committee hearings
• Floor Actions
• House Senate debate amendments
• House Senate versions
• Conference
• Passage (On or before 1 October)• Continuing Resolutions –
temporary appropriations
• President signature/veto
5- 35
5-36
Process Review
• Appropriation• Apportionment• Allotment• Commitment• Obligation• Expense (outlay)
5- 36

5-37
Defense Appropriations
• Operations and Maintenance (O&M)• Research Development Test and
Evaluation (RDT&E)• Procurement• Military Construction • Military Pay
5- 37

5-38
Budget Activity Groups (O&M BAGs)
• Bag 1: Direct Care• Bag 2: Private Sector Care• Bag 3: Consolidated Health• Bag 4: IM/IT• Bag 5: Management Headquarters• Bag 6: Education and Training• Bag 7: Base Operations/Communications
5- 38

5-39
Commodities• Personnel• Travel• Transportation• Communication/Utilities/Rent• Printing• Other Services (Contracts)• Supplies and Material• Equipment• Stipends/Grants
5- 39

5-40
Status of Funds• Commitment
• Plan to spend• Obligation
• Contract, Purchase Order, Civilian Hire• Expense
• (1) Goods received – services rendered, (2) valid invoice, and (3) valid purchase order (three way match)
• Available• Funds that are not committed, obligated, or
expensed
5- 40

5-41
Availability of Budgetary Resources
• Purpose• Funds may be obligated and expended only for the purposes
authorized in the appropriations acts or other laws• Time
• The period of time during which budgetary resources may incur new obligations is different from the period during which the budgetary resources may be used to incur expenditures
• Amount• Obligations and expenditures may not exceed the
amounts established in law
5 41

5-42
Legal Control of Funds• The legal control of funds is governed by the
legal authority of funds with regard to: • Purpose - 31 USC 1301
• Necessary expense doctrine• Reasonably related• Not prohibited by law• Not funded elsewhere
• Time – 31 USC 1502• Bona fide need rule
• Amount – 31 USC 1341, 31 USC 1517• ADA violation
5 42
5-43
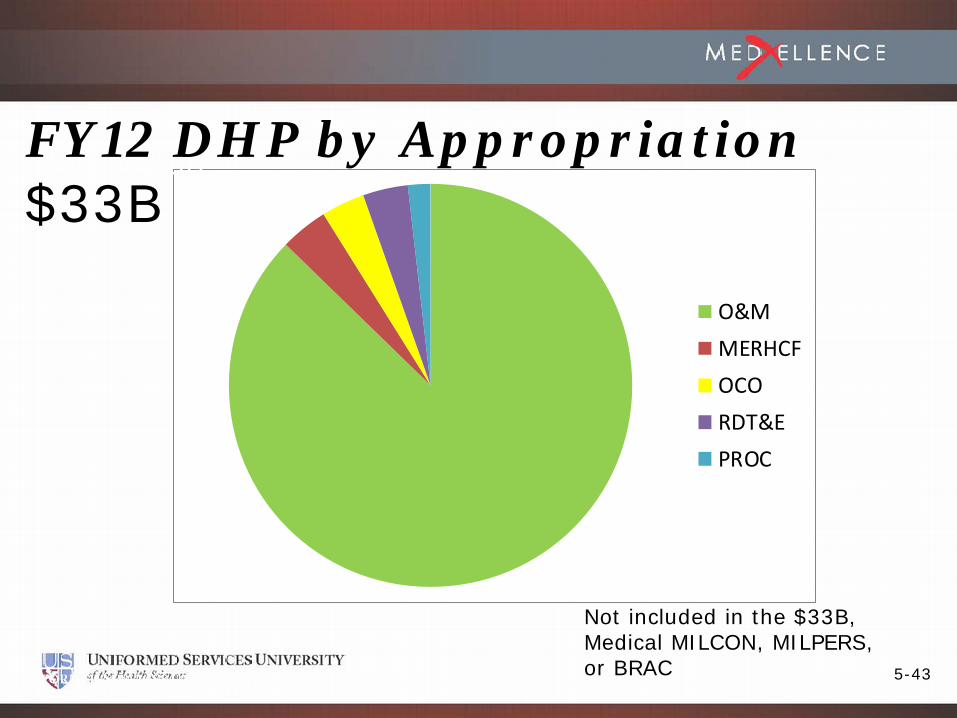
O&MMERHCFOCORDT&EPROC
Not included in the $33B,Medical MILCON, MILPERS,or BRAC
FY12 $52.5BFY12 DHP by Appropriation $33B
5-44
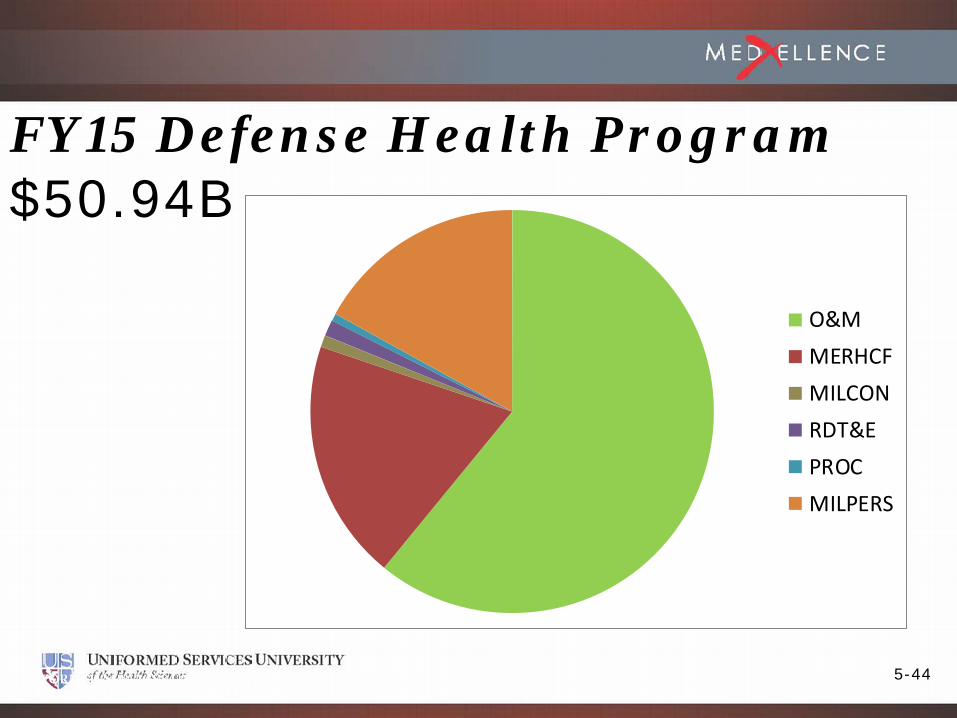
O&MMERHCFMILCONRDT&EPROCMILPERS
FY15 Defense Health Program$50.94B
5-45
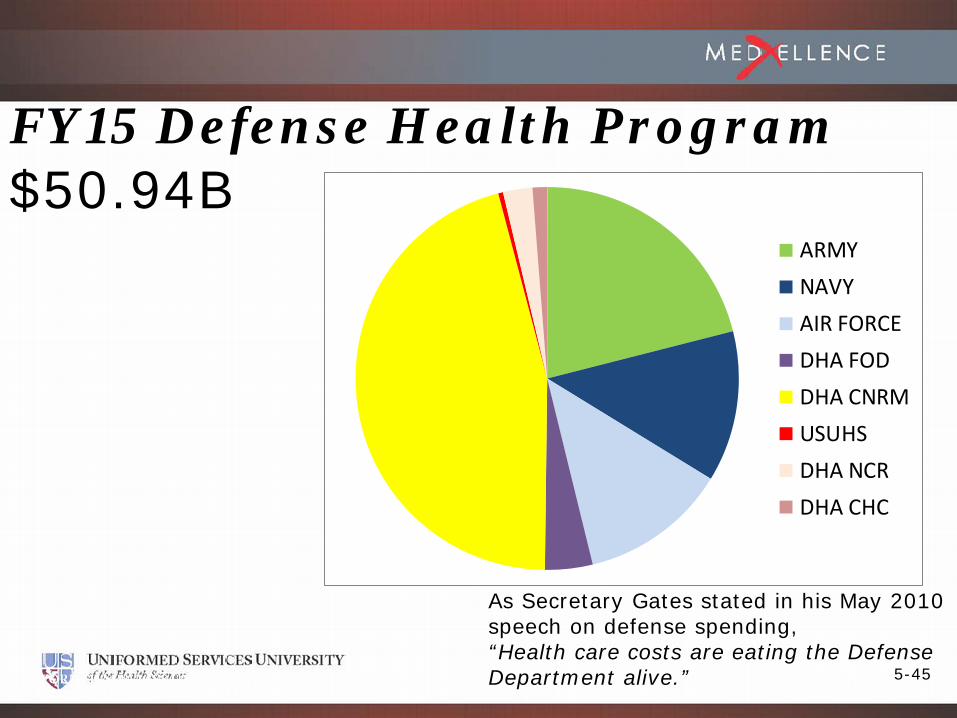
FY15 Defense Health Program$50.94B
5- 45
ARMYNAVYAIR FORCEDHA FODDHA CNRMUSUHSDHA NCRDHA CHC
As Secretary Gates stated in his May 2010 speech on defense spending, “Health care costs are eating the Defense Department alive.”

5-465- 46
ArmyNavyAir ForceUSUDHA CRMDHA NCRDHA FOD
Defense Health Program FY15 O&M $31B

5-47
O&M
MERHCF
OCO
RDT&E
PROC
Not included in the $32B,Medical MILCON, MILPERS,or BRAC
FY12 $52.5BFY16 DHP by Appropriation $32.2B

5-485- 48
Army
Navy
Air Force
USU
DHA CRM
DHA NCR
Defense Health Program FY16 all Appropriations $33.8B

5-49
FY17 PRES BUD REQUEST
DHP APPROPRIATIONO&M 32,231,390$ PROC 413,219$ RDT&E 822,907$
TOTAL 33,467,516$
DOD Support to the DHPMILPERS 8,651,404$ MILCON 312,454$
TOTAL 8,963,858$
MERHCFNCC 6,366,908$ MERHCF RECEIPTS 10,268,244$
GRAND TOTAL 59,066,526$
DHP Operations Overview

5-50TTotal = $30.903B

5-51
TRICARE Contracts
• National Quality Monitoring• Global Remote• Health Care and Support Services
(HCSS)• Retail Pharmacy
5- 51

5-52
TRICARE Contracts (cont)
• Mail Order Pharmacy• TRICARE Dual Eligible Fiscal
Intermediary• Marketing and Education• TRICARE Retiree Dental• Overseas SoS
5- 52
5-53
TRICARE Contracts History Review
• CHAMPUS Civilian Health and Medical Program of the Uniformed Services
• CRI CHAMPUS Reform Initiative• Foundation Health Corp (now Health Net) CA and
HI from 1988-1994
5- 53

5-54
TRICARE Contracts History Review
• CHAMPUS Civilian Health and Medical Program of the Uniformed Services
• CRI CHAMPUS Reform Initiative• Foundation Health Corp (now Health Net) CA and
HI from 1988-1994
5- 54

5-55
TRICARE Contracts History Review
• T1: 12 Regions, Lead Agent Model• T2: Introduced Resource Sharing• T3: Managed Care Enrollment Based
Capitation: B3
• Tnext One Contract 3 Awards 80/20 risk sharing Performance Guarantee, Award Fee for Customer Satisfaction, Underwriting Fee, moving base year
5- 55

5-56
TRICARE Overview
• Tnow – risk sharing eliminated,• Health care costs are a pass through• Performance and Satisfaction incentives
• T4 ?? Dr. Guy Clifton Author of Flatlined: Resuscitating American Medicine (a work in progress)
5- 56

5-57
Intended Benefits of Underwriting
• Shared risk promotes Government/contractor partnership to control purchased care costs
• Annual determination of target cost minimizes contractor’s long term risk• Reduces “risk premium” and potential for disputes
• Lack of adjustment for MTF usage creates strong incentive to maximize use of the MTF• More MTF care means less purchased care, more realized
fee for the contractor and less cost for the Government• Paying healthcare costs in real time improves budget
execution and predictability
5- 57

5-58
Resourcing for Value
• Prospective Payment System (PPS)• Performance Based Payments
• Health Affairs to the Services• Capitatoin• Potential Outcomes based adustments• Traditional Fee for Service
5- 58

5-59
Pay for Performance to drive to the MHS
• Prospective Payment System (PPS)• Performance Based Payments
• Health Affairs to the Services• Capitation• Potential Outcomes based adustments• Traditional Fee for Service
5- 59

5-60
PPS Value of Care
• Value of MTF Workload• Fee for Service rate for workload produced
• Rates based on price at which care can be purchased discounted for Military Labor• TMAC rates• Not MTF costs
• Computed at MTF level but allocated to the Services
5- 60

5-61
PPS WorkloadHow we got here
• Inpatient – MEPRS A Work centers• Non-Mental Health - Relative Weighted Products (RWPs)• Mental Health - Bed Days
• Outpatient – MEPRS B Work centers• Simple (Work) Relative Value Units (RVUs)
• In the Direct Care System ~70 cents of every dollar goes to labor; Military, civilian, and contract
5- 61
5-62
MHS Mantraor Why Recapture?
“The incremental cost of the next thing in the MHS is always less than the average cost of that same thing in the network”
5- 62
5-63
MENBA Pilot Project• QDR: “Capture the quantity, value, and expense of
readiness and military-unique services provided by MHS activities”
• Identify and List all Mission Essential/Non-Benefit Activities (MENBA) performed in the MHS
• On-site visits• 6 MTFs (1 small & 1 Large from each Service)• MTF Participation:
• Coordinate Schedule• Provide limited Documents (e.g., Committees List, Additional Duties
Rosters, etc.)• Be Part of the Team, Part of the Project!
• Work with MENBA WG to “sort out”, classify & develop Taxonomy for activities
5- 63
5-64
Next Steps• Ancillary• Pharmacy• Utilization Management/Capitation• Industry Standard Workload• Dental• Mission Essential Non-Benefit Activities• Paying for Quality
5- 64

5-65
PPS RoadmapInpatient
Outpatient
Ancillary
DataWeightsRates
PharmacyDataRates
Mission Essential
Data Weights Rates
Workload
Institutional
Professional
RiskAdjusters
ReinsurancePlan
MinimumEnrollment
HEDIS
SatisfactionORYX
Institutional
Professional
OtherBenefit
(HCPCs)DataWeightsRates
Capitation Performance
DentalDataWeightsRates
5- 65
5-66
Influencing the Cost of Military Medicine
Benefit Population
Force Structure
Mission5- 66

5-67
Obtaining CME/CE Credit• If you would like to receive continuing
education credit for this activity, please visit:• http://medxellence.cds.pesgce.com
5- 67

5-68