documents session: high tech, high cost: who …€¦ · web viewand ladies home journal was and is...
TRANSCRIPT

DOCUMENTS SESSION: High Tech, High Cost: Who pays?
In the documents and secondary sources you read for class, some of which have been extracted below, you learned of different approaches to paying for medical care in the US, and about the different interests and rationales represented by each of the many proposed schemes. Today, we will focus more closely on particular actors, historical moments, and overall contexts in the emergence of today’s mixed State/third-party payer system of coverage. What I want you to do is to think about what kinds of QUESTIONS can be asked of (and answered by) these documents. Think in terms of class themes and concepts such as professionalization, authority-building, orthodoxy, gender, the doctor-patient relationship, technology, and the relative roles of the State, the consumer, and the practitioner…Think too in terms of Maioni’s article, and her three broad categories of factors influencing the divergence of health care systems and solutions between the US and Canada (‘social forces’, ‘state actors’, and ‘the impact of state structures and political institutions’). Which do you see at work in the documents below – and which do you feel offers the most compelling explanation of the paradox of US healthcare?
From your readings, you should also be able to define/identify and know the significance of:Harry Truman ‘third party payer’ Nonprofit/not-for-profit
Medicare Boston Women’s Health Course Collective
Voluntarism/voluntary sector
Medicaid Medical-industrial complex For-profit/investor-ownedSocial Security American Hospitals Association ‘managed care’
Document 1.

Document 2:
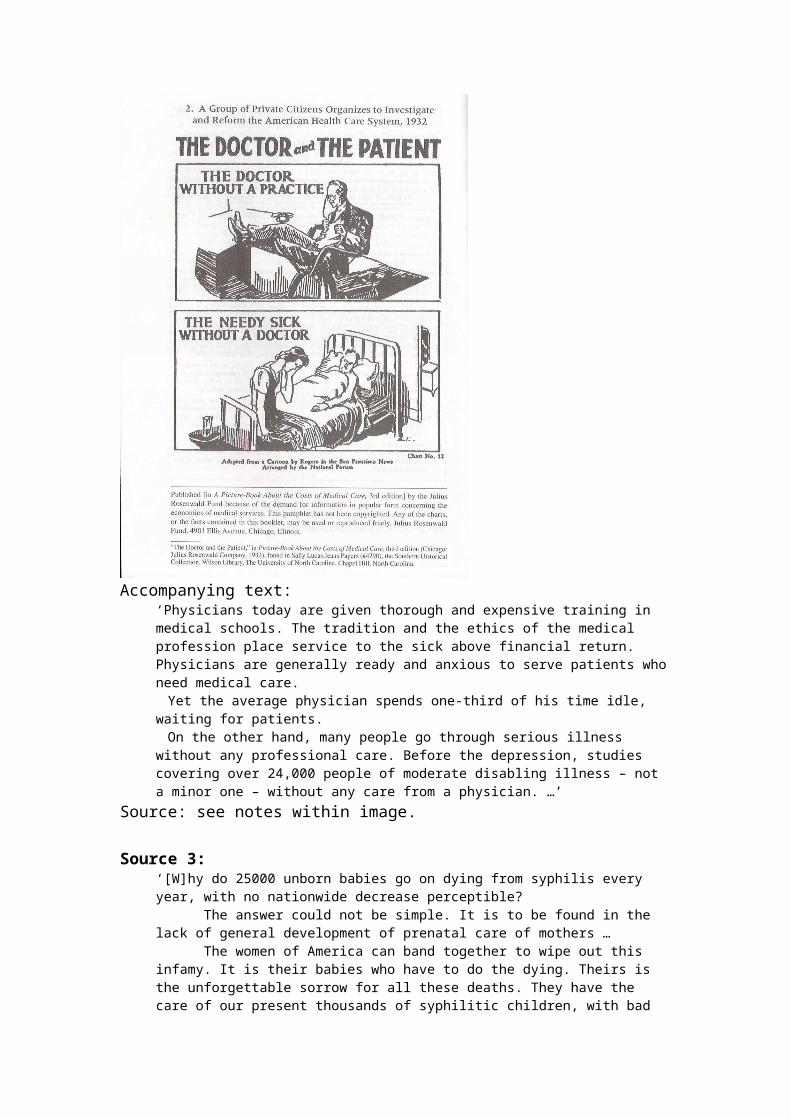
Accompanying text: ‘Physicians today are given thorough and expensive training in medical schools. The tradition and the ethics of the medical profession place service to the sick above financial return. Physicians are generally ready and anxious to serve patients who need medical care.
Yet the average physician spends one-third of his time idle, waiting for patients.
On the other hand, many people go through serious illness without any professional care. Before the depression, studies covering over 24,000 people of moderate disabling illness – not a minor one – without any care from a physician. …’
Source: see notes within image.
Source 3: ‘[W]hy do 25000 unborn babies go on dying from syphilis every year, with no nationwide decrease perceptible?
The answer could not be simple. It is to be found in the lack of general development of prenatal care of mothers …
The women of America can band together to wipe out this infamy. It is their babies who have to do the dying. Theirs is the unforgettable sorrow for all these deaths. They have the care of our present thousands of syphilitic children, with bad eyes, or blind, or deaf, or maimed … Knowing as they now can know that this mass tragedy is almost entirely preventable, theirs too must be the self-accusation, the bitter “it-need-not-have-been”.
They, the women of America, not only have the power to lead this fight; they have the tradition. Famed obstetrician Williams – he is the very one who made the practical prevention of this horror possible – admits that
the great movement for prenatal care was not of medical origin mainly: For this lifesaving movement, Doctor Williams gives the credit to Mrs William Putnam, plain laywoman of Boston. …
And the general prenatal care of America’s expectant mothers, by America’s physicians, scientists, and nurses will be exactly as good as women demand. There are plenty of doctors who, if they are properly paid for it, will be able to perform this service.
… Our bands of crusading women will be asked this awful question: … Where are you going to get the money?
To this our fighting bands of women can give, not a sentimental but an entirely practical, a hard-boiled, a business answer.
To the mayors and councils of their communities, to the governors and budget balancers of their states, to our national Congress, and yes, to the head of our nation, himself, our women can say:
“We are not demanding the weapons to wipe out this syphilis of the innocent because of our tears for babies born dead who might be alive and strong … Nor do we even ask you to sympathize with our sadness the thousands of children with impaired eyes, or blind, or deaf, or crippled, demented when they are preparing for useful citizenship. No. In the name of our anguished taxpayers, we only plead that you, our rulers, be economical.” ’
Source: Paul de Kruif and Thomas Parran, ‘We can end this sorrow’, Ladies Home Journal (August 1937): pp. 23. 88-90.De Kruif was, by this time, a renowned science journalist. Thomas Parran was the Surgeon General and already a noted and radical public health campaigner against syphilis via his book and subsequent national public health informational campaign ‘Shadow on the Land’. And Ladies Home Journal was and is still a resolutely down-to-earth (but still aspirational) monthly magazine intended for homemakers, mothers, and housewives of the lower-middle and middle classes.
Document 4:‘Healthy citizens constitute our greatest national resource. In times of peace as well as in time of war, our ultimate strength stems from the vigour of our people. The welfare and security of our Nation demand that the opportunity for good health be made available to all, regardless of residence, race, or economic status.…We still face a shortage of hospitals, physicians, dentists, and nurses. Those we have are unfairly distributed. …In the last analysis the patient’s ability to pay for the services of
physicians or dentists, or hospital care determines the distribution of doctors and the location of hospitals. Few doctors can be expected to practice today in sparsely settled areas where prospective patients are unable to pay for their services. … The unequal distribution of doctors and hospitals will plague this Nation until means are found to finance modern medical care for all of our people.National health insurance is the most effective single way to meet the
Nation’s health needs.… Although the individual or even small groups of individuals cannot successfully or economically plan to meet the cost of illness, large groups of people can do so. If the financial risk of illness is among all our people, no one person is overburdened. More important, if the cost is spread in this manner, more persons can see their doctors, and will see them earlier. This goal can be reached only through a national medical-insurance program, under which all people who are covered by an insurance fund are entitled to necessary medical, hospital, and related services.A national health insurance program is a logical extension of the
present social-security system which is so firmly entrenched in our American democracy. Of the four basic risks to the security of working people and their families – unemployment, old age, death, and sickness – we have provided some insurance protection against three. Protection
against the fourth – sickness – is the major missing element in our national insurance program.… Under the program which I have proposed patients can and will be as free to select their own doctors as they are today. Doctors and hospitals can and will be free to participate or to reject participation. And a national health insurance plan can and should provide for administration through State and local agencies, subject only to reasonable national standards.’
Source: President Harry S. Truman, ‘National Health and Disability Insurance Programs – Message from the President of the US’, House, May 19, 1947, Congressional Record H261, pp. 5490-5491. The Congressional Record is the US equivalent of Hansard’s. This text is taken from a speech made by the President to the US Congress. Note that Truman was FDR’s vice-president when Roosevelt died in office; in subsequent election campaigns, he proposed ‘Fair Deal’ democracy. His initial political successes were built on his career and heroic record in WWI. And he was in office as Commander-in-Chief when the atom bombs were dropped on Japan.
Document 5:‘The past-president of manufacturers had a progressive mind, as he freely confessed, and so he realised that organised medicine must find some way of enabling people with small incomes to procure adequate medical care for themselves – to procure the kind of care for which the convention was repeatedly congratulating itself. He had applied hard thought to the problem, especially in relation to “politicians and reformers”. And he had reached a conclusion: that we should be wise to adopt “the voluntary plans for hospital and health insurance” that the AMA recommends.
That was what he was brought to Atlantic City [site of the AMA Annual Meeting 1947] to say. And in the course of his inaugural address, the new president of the American Medical Association found occasion to say it again. They were talking about a fearful bugaboo, a national health program, and they were voicing the party line… In organized medicine there is a general realization that such a program is certain to come, a realization something like that of a town that which learns by telephone that the dam up the alley has burst and a flood is on the way. The dam burst long ago and year by year the AMA has prepared to meet the flood by saying that it must not get here, that the flood waters are communistic, that we shall all be lost if they reach the city limits.
Systematically and tirelessly, with all the means available to one of the most powerful pressure groups and propaganda machines in the country, the AMA has opposed every measure in which it detected any connection whatever with what is surely coming. It has done so sometimes suavely, sometimes with amazing crudity, sometimes by individual pressure the most dishonourable … the rulers are now defending what they regard as the citadel itself.
That ultimate and minimum is this: There must be no federally controlled health program; the program whose coming is seen
to be inevitable must be based on states rights. There must be no national imposition of medical standards apart from those which organized medicine itself imposes. There must be no federal control over the practice of medicine, and no government of public control of the bodies that will ultimately direct the program: all effective power must be reserved to organized medicine. There must be no form of compulsory health insurance – since this would make the previous provision impossible. There must be no “third-party intervention” by any non-medical board or panel or supervisor, between doctor and patient. (Medical third-party intervention is all right, and non-medical third-party interventions are accepted for the poor.) And nothing, at least nothing not a part of organized medicine, must interfere with “the free choice of the physician”, a freedom which only a minute percentage of our population have now, which that percentage relinquish when they patronize any of the famous clinics, and which only a few of those who have it can exercise except ignorantly, and as an act of faith. To sum up: organized medicine insists on complete, unsupervised control of any health program that may evolve; and it requires that plan to interfere with the fee-for-service system as little as possible, not at all wherever there is any way to maintain the system.
This stand is of course so unrealistic that it suggests the need of psychiatric scrutiny…”
Source: Bernard Devoto, ‘Doctors on the Boardwalk’, Harper’s Magazine 195 (1947): 215-244. Devoto was a journalist and historian from Utah, an authority on Mark Twain, and a frequent contributor to Harper’s. He was known for his liberal viewpoint. Launched in 1850, Harper’s is one of the oldest continuously published magazines in the US, covering general-interest topics in the arts, politics, science, finance and current events from a generally liberal point of view.
Document 6:“Doctors attitudes towards patients are terrible condescending, especially towards women. You aren’t supposed to read the record of your own body, and you are scolded like a child if you do. Doctors withhold information … In playing God, their attitude is that you must have complete confidence in them to make all of your decisions for you. Why should they make your decisions? … The system fails to provide basic preventive medicine for people. For example cancer of the cervix or the uterus can be totally cured by early detection by the Pap smear and early treatment. The Pap smear was developed about thirty years ago, and yet today (1970) only 12% of American women regularly ge Pap smears. It would be simple (but boring) to have a mass screening campaign. A great proportion of the 14,000 deaths per year from uterine cancer could have been prevented. A young internist recently remarked that he rarely did pelvic examinations of his women patients because it embarrassed him. How many women die because doctors have hang-ups about genitals?
On the other hand, unnecessary and cruel surgery is often performed. In a study at Columbia, one-third of the hysterectomies reviewed were judged as having been done without medical justification. … In Appalachia, doctors have removed healthy reproductive organs from 11 and 12 year old girls to get the $250 fee. Unnecessary surgery is common in America. We have twice as much surgery, per capita, as England. The unnecessary

operations are called “remunerectomies” … How many remunerative testectomies do you think are done? …
The AMA (America Medical Association) has been an extremely powerful force in insuring that medicine is practiced for the doctors, not the patients. Although it does not speak for every doctor as an individual, it does write the ruls that all doctors must follow. Milford O. Rouse, M.D., last year’s AMA president has asserted that there is a threat to medicine in the concept of healthcare as a right rather than a privilege. The AMA has the richest lobby in Washington, spending $1.1 million in 1965. …It is estimated that five times this amount is spent at the local level. …
The AMA has opposed free inoculations against diphtheria and polio, free vaccinations against smallpox, the establishment of Red Cross blood-banks, federal grants for medical school construction and medical student loans, national health care and Medicare. … In 1955, after Salk developed his vaccine, the AMA House of Delegates passed a resolution demanding “immediate termination” of free distribution of the vaccine. The Federal Government’s program to inoculate people was called “a violation of the principles of free enterprise.” In New Jersey, the state medical society forbade physicians to participate in free programs except where the patients were paupers. Half of the vaccine purchased by the Federal Government went unused in the first year of the program, due to doctors’ unwillingness to participate in free programs. The doctors charged $5 a shot. They get most vaccines free.
The AMA has fought any form of practice that promotes preventive measures rather than curative treatment. The AMA’s positions on pollution, smoking, car safety, and working conditions all show that they put the freedom of corporations above the concern of keeping people healthy. 45% of the AMA’s operating budget comes from the drug and medical supply industries, so the AMA is interested in laws which bolster the exorbitant profits of these industries. … Dr. Milton Rouse has stated the purpose of the AMA by saying that the AMA should “concentrate [its] attention on the single obligation to protect the American Way of Life. That way can be described in one word: capitalism”. ’
Source: The Boston Women’s Health Course Collective. Our Bodies Ourselves. New York and Boston: Simon and Schuster, 1971. First edition of a classic text in feminism, the feminist health movement, and the feminist critique of medicine. Intended for patients/consumers, and particularly, if not exclusively, women.
Document 7:‘Can we really leave health care to the marketplace? Even if we believe in the free market as an efficient and equitable mechanism for the distribution of most goods and services, there are many reasons to be worried about the industrialization of health care. … health care is different from most of the commodities bought and sold in the marketplace. … It is a public rather than a private good, and in recognition of this fact, a large fraction of the cost of medical research and medical care in this country is being subsidized by public funds. … They also reimburse the charges for health-care services. Through Medicare and Medicaid and other types of public programs, more and more of our citizens are receiving tax-supported medical care. … most consumers (i.e., patients) are not “consumers” in the Adam Smith sense at all. As Kingman Brewster recently observed, health insurance converts patients from consumers to claimants, who want medical care virtually without concern for price. … Hence, the classic laws of supply and demand do not operate because health-care consumers do not have the usual incentives to be prudent, discriminating purchasers. …
All of these special characteristics of the medical market conspire to produce an anomalous situation when private business enters the scene. A private corporation in the health-care business uses technology often develpped at public expense, and it sells services that most Americans regard as their basic right – services that are heavily subsidised by public funds, largely allocated through the decisions of physicians rather than consumers, and almost entirely paid for through third-party insurance. The possibilities for abuse and for distortion or social purposes in such a market are obvious.
Health care has experienced an extraordinary inflation during the past few decades, not just in prices but in the use of services. A major challenge – in fact the major

challenge – facing the health-care establishment today is to moderate use of our medical resources, and yet protect equity, access and quality. … If physicians are to represent their patients’ interests in the new medical marketplace, they should have no economic conflict of interest and therefore no pecuniary association with the medical-industrial complex. … The medical profession would be in a stronger position, and its voice would carry more moral authority with the public and the government, if it adopted the principle that practicing physicians should provide no financial benefit from the health-care market except for their own professional services.’
Source: Arnold S. Relman, ‘The New Medical-Industrial Complex’, New England Journal of Medicine 303 (1980): 963-970. Relman was the editor of NEJM, one of the US’s top two medical journals (and one of the most recognized and respected medical journals in the world).
Source: Dan Perkins (Tom Tomorrow), This Modern World, http://www.workingforchange.com/webgraphics/WFC/TMW07-04-07colorlowres.jpg July 4, 2007 [accessed 15/04/2008].This Modern World is a syndicated weekly editorial cartoon, appearing in the print media (generally in urban mainstream but left-leaning publications), as well as on-line with Salon.com and Working for Change (a health-care advocacy and lobbying group).