documentation - liveconferences.com · · 2013-06-07we must document to get reimbursed and be...
TRANSCRIPT

www.treatment2go.com & www.handtherapy.com
Treatment2Go
Welcome to Treatment2Go’s digital E-Books. Treatment2Go is a registered trademark of Exploring Hand Therapy. We are an AOTA approved provider. Our digital E-Books allows you to enjoy education with ease and comfort. You will read, learn and earn CEUs in the comfort of your home. After you have completed this course you are required to take an exam. Upon successful (75%) completion of the exam you will immediately be emailed your certificate. Sit back, relax, and begin.
Documentation: Dos and Don'ts, Billing Issues and Functinal G Codes
This course has active links. The table of contents is linked so you can just click and go (page 5). To access a web-site click the link. To return to the course, close the website by clicking the X. To navigate within the course, you can advance to the next page by any of the following options:
Click the arrows at the bottom of the PDF page
Click the enter button
Use the arrow keys on your keyboard
Use your mouse to scroll down using the slide bar on the right side of page
During the course you are asked to study and participate in writing labs via the CLICK HERE buttons which are linked and will direct you off your page. When you have completed the lab work, click the RED box that says “return to course, click here” and you will return to the course page you were on.
Linked websites provide additional content, which is not mandatory for the course, but is provided for supplemental information only. If a link is down contact: [email protected].
1)
2)
3)
4)
Upated

Treatment2Go
2
Index
handtherapy.com
Instructor
Elisa Marks, MS, OTR/L, CEAS, CHT
Editors:
REFERENCESAOTA website (aota.org)
Medicare website (medicare.gov)
Centers for Medicare Services (CMS) www.cms.gov
United Government Service Provider Seminars 2006-2007
Blue Cross Provider Manual
British Medical Journal 1996; 312:71-72 (13 January)
1)
2)
3)
4)
5)
6)
Nancy Falkenstein OTR/L, CHT Susan Weiss OTR/L, CHT

Treatment2Go
�
Index
handtherapy.com
The information provided in this course is not intended for the use of diagnosing or treating a health problem or disease. Further, the material in this course is provided for personal, educational, and informational purposes only and does not constitute a recommendation or endorsement with respect to any company, website, or product and is in no way considered a substitution for professional care. If you have questions or concerns about the course content, it is your responsibility to verify all information. Exploring Hand Therapy specifically disclaims any and all liability for any claims or damages which may result from any information discussed by the instructor or by a third party via links to this course. Exploring Hand Therapy site includes direct access to other Internet sites. Exploring Hand Therapy has not participated in the development of these other sites, and does not exert any editorial or other control over those other sites at anytime. Due to the nature of the internet and active links, at times off-site links may be “down”, unavailable, or deleted. EHT has taken every effort to ensure links are active at the time of this writing. Information from off-site companies is supportive information and is not critical information to this course.
Disclaimer

Treatment2Go
�
Index
handtherapy.com
Dos and Don’ts, Billing Issues and Functinal G Codes
Course Description
This documentation course will provide the clinician valuable insights for efficient, concise, and meaningful documentation that meets payer guidelines (private payers & Medicare). The course will cover rationales for thorough documentation, with special
emphasis on Medicare guidelines, recommendations for incorporating function into documentation, tips for goal setting, and examples of both rejected and paid documentation. The examples will cover all areas of adult occupational therapy practice.
Documentation Dos and Don’ts

Treatment2Go
�
Index
handtherapy.com
Objectives:
At the end of this course the therapist will be able to:
Identify several different methods of completing daily documentation
Identify necessary components of a thorough evaluation
identify key components of incorporating function into documentation
Define how to stay abreast of Medicare regulation changes
State 4 current Medicare regulatory requirements
Set meaningful goals that will meet payer guidelines and allow for payment of services to ensue.
Table of ContentsChapter 1: Purpose of documentation and formats for documenting (pg 6)
Chapter 2: Medicare Regulations – current regulations and how to find updates (pg 16)
Chapter 3: Medicare documentation and coding updates (pg 28) Functinal G Codes, Modifiers, PQRS
Chapter 4: Writing a therapy story via documentation (pg47)
Chapter 5: Setting relevant goals (pg 52)
Chapter 6: Incorporating function into documentation (52)
Chapter 7: Evidence based practice – why should I care? 56)
Chapter 8: Worksheets (pg 62)
References
1)
2)
3)
4)
5)
6)
Treatment2Go
�
Index
handtherapy.com
Chapter 1Documentation : Purpose and Format
Why do we need documentation?
Often times therapists wonder ......What is the purpose of daily documentation?
Why can’t I just do a biweekly or monthly note and be done with it?
Why does a payer need to know every single detail of my treatment session?
Therapists want to be properly and fairly reimbursed for their skilled work provided. Therefore it is critical therapists convey clear documentation portraying the skilled interventions that are meaningful and appropriate. If the documentation is not portraying a skilled level of care that is appropriate, the payer(s) may not reimburse for services rendered. Payer(s) responsibility is to provide reimbursement for appropriate and some times evidenced based skilled therapy. More and more payers want to pay for that which has been proven beneficial and will contribute to an improvement in patient status.
In addition to reimbursement, concise and comprehensive documentation will benefit therapists in other ways as well.
►
►
►
We must document to get reimbursed and be legally protected

Treatment2Go
�
Index
handtherapy.com
Documentation helps therapists with:
Additional legal protection if the therapist or medical records becomes part of a lawsuit or legal proceeding
Providing a record of ongoing care, allowing therapists to keep track of all treatments provided
Allowing other therapists to take over care and follow the treatment plan in case illness or other personal matter prevent the primary therapist from providing treatment
In today’s clinical environment, therapists are required to be productive and accountable for their time and treatments. Most
therapists agree that “paperwork” is a big “headache”. It is a daily challenge to efficiently and effectively complete paperwork and treatment responsibilities in a timely manner. Some therapists feel they treat to the “pen” and spend as much time documenting as they do performing patient
care. The key is learning how to document in a concise manner that preserves important information needed for getting paid while maintaining productivity and accountability. The primary goal of this course is to give the therapist tools, suggestions, and tips to streamline their documentation without neglecting key components that payers look for when approving or denying payment for servers rendered.
►
►
►

Treatment2Go
�
Index
handtherapy.com
Documentation Formats
Evaluation
Therapists use a variety of standardized, non-standardized tests and forms when conducting and completing an evaluation. The format used may vary depending on the practice setting and clientele demographics. This course covers basic information that should be included in an occupational therapy evaluation:
Patient age and diagnosis
Patient functional status prior to admission for this medical problem or start of care
Past Medical History
Current course of care
Assessment of performance components
Assessment of ADL and IADLs
Problem list
Goals
Plan of care
►
►
►
►
►
►
►
►
►

Treatment2Go
�
Index
handtherapy.com
Evaluations need to include some objective measures of current patient status. This is necessary to later show MEASURABLE progress in these areas. It will also help the therapist design measurable goals.Non-measurable goal: Patient will improve tolerance to handwritingMeasurable goal: Patient will increase writing tolerance from 5 minutes to 15 minutes without fatigue to complete bill paying
Examples of non-standardized evaluation tools include: Grading a patient on ADLs with a min/mod/max scale.
Examples of standardized evaluation tools include: 9-hole peg test
Allen Cognitive Level Screen (leather lacing test)
Dynamomter strength testing
Canadian Occupational Performance Test
Note: Goal setting will be addressed further in Chapter 5.
SOAP NOTES
The most utilized style or method of documentation is the “SOAP” note.S = Subjective
O = Objective
A = Assessment
P = Plan
This method of documentation is used across many disciplines. It is a standard design that addresses the entirety of a patient visit and experience. There are 4 distinct sections of the note, each with it’s own distinct purpose. Let’s define them:
►
►
►
►
►
►
►
►
►
S: feel tiredO: PRE, A/AA...A: tired because...P: add activity ....

Treatment2Go
10
Index
handtherapy.com
Subjective: Patient’s experience. Can include:Direct patient quote about their progress
Pain scale
Report of new symptoms
Objective: Therapist’s statement of fact. Can include:Listing of daily treatment activities (or reference to exercise log)
Measurable status (i.e. ROM/strength numbers, status for a transfer such as min assist, time to complete a standardized test such as 9 hole peg test)
Information regarding contacting other members of the healthcare team
Assessment: Therapist’s professional judgment of clinical progression. Can include:Statement regarding why patient progress is limited or exceeding expectations
Clinical reasoning for current patient status
Statement regarding patient motivation, participation
Plan: Therapist’s ongoing plan for future treatment and discharge planning.
Example of a SOAP Note Diagnosis: Finger Fracture
S: “Yesterday I was unable to hook my bra independently, and while trying I had 4/10 pain.”
O: Treatment today included: Paraffin for 8 minutes, AROM/PROM per flow sheet, functional manipulation tasks of coins, buttons, and jewelry, graded strengthening with gripper in preparation for functional lifting. After treatment PIP joint AROM: 20-75 degrees.
A: Patient’s ROM is likely limited by scarring around proximal phalanx. Tendon glide of extensor hood is limited, preventing full extension
P: Add strengthening as tolerated, begin PIP extension splinting next visit.
►
►
►
►
►
►
►
►
►

Treatment2Go
11
Index
handtherapy.com
Example of a Soap Note Diagnosis: CVA
S: “I needed help to open the refrigerator this morning for breakfast”
O: Functional mobility in kitchen with contact guard assist for light meal prep. Patient required mod A to open refrigerator and maintain balance while removing a gallon of milk. Education and proper patient demonstration on compensatory strategy of using countertop to move items through kitchen. Theraband exercises for elbow flexion, shoulder extension added to home program (2x/day 10 reps each).
A: Patient demonstrates good carryover of new exercises. Patient continues to need supervision for kitchen tasks.
P: Continue to address light meal prep and compensatory strategies for patient safety.
Complete the Soap Note worksheet (page 62)
Click button to go directly to the worksheet
Re-Evaluation/Progress Note
It is common practice to re-assess patient status on an ongoing basis. One method is to do a formal re-evaluation. Other therapists do some measures on a daily basis so that they can assess the effectiveness of their treatment to that point. Different insurers have different guidelines regarding the frequency of re-evaluation. Regulations regarding Medicare re-assessments will be addressed later in this book.
Treatment2Go
12
Index
handtherapy.com
Alternative Documentation Techniques
Two less commonly used documentation methods include:
Narrative Note:
This type of note is a simple narrative that includes similar information that is listed for the SOAP note above, however is written in a narrative format.
Problem Oriented Medical Record (POMR):
This documentation style helps with organizing a medical record. Information included in this type of record keeping has baseline data, a problem list, plan of care, and a progress note.
Electronic Documentation
More and More facilities are considering an electronic medical record. Some facilities have already made the switch. What impact does this have on documentation styles and regulations we have discussed? Why is the idea of an electronic medical record scary for some people? Is it a safer way of documenting? Do the rules change when we move to an electronic medical record?
Change can be scary for many people but in today’s technological environment computerized or electronic documentation is becoming the chosen format and it may not be too far off when paper documentation is a thing of the past.
There are some states that require electronic documentation but therapy
►

Treatment2Go
1�
Index
handtherapy.com
is typically not a mandated discipline. Regardless, many facilities are contemplating electronic documentation. Some considerations when deciding on electronic documentation include:
How many, if any, of the staff may have computer literacy issues that will slow their transition? Clinicians who are infrequent computer users may be especially fearful of the transition, requiring extra training and resources to help them transition to the computerized system.
Many facilities have eased into electronic medical record keeping by decreasing the productivity quota during the transition. This allows a chance for the clinicians to get hands-on practice with the system under a more relaxed schedule.
It may take weeks or even a few months for some clinicians to feel as though the time spent charting in an electronic medical record is similar to and improved, as compared to handwritten notes.
Some universities are introducing electronic documentation at the student level but this is not mandated by the AOTA nor the APTA at this time, but it may be soon.
Many facilities report that computerized documentation decreased documentation time allowing for increased and improved patient treatment sessions.
Some facilities find electronic documentation to be less stressful on the
therapists once the system is mastered by the therapists.
In 2009, Congress adapted the HITECH act. The HITECH act includes 419 Billion dollars for increasing the use of electronic health records by doctors and hospitals. Electronic health records will continue to be at the forefront of changes in our healthcare system. We as occupational therapists must ensure that our documentation is as valuable and meaningful electronically as it is on paper.
►
►
►
►
►
►

Treatment2Go
1�
Index
handtherapy.com
The Affordable Care Act signed into legislation by President Obama also includes regulations on the transition to electronic health records. These regulations begin going into effect in October 2012. There will be a series of changes including standardizing billing.
Every vendor of electronic medical records offers different templates, capabilities, and layouts. A clinic purchasing one of these systems must weigh the pros/cons of what each system offers. Many systems come with the ability for the creation of custom templates as well. Many of the systems utilized in therapy clinics have specific forms that allow for therapy specific evaluation, re-assessment, discharge, etc while others are more general. Some systems have AMA normative data and FCE programs as well. Hopefully if you are using electronic documentation, it is designed for rehabilitation therapists as some facilities have purchased a general nursing documentation system and forces the therapists to confirm to poorly designed therapy notes. This, rightfully so, can be frustrating but this section of this course will assume the electronic documentation is geared for rehabilitation therapists. When choosing the system for you or your clinic, it is best to make an assessment of which forms you use on a regular basis and decide how many of these forms need to be transcribed into the new system.
Safety
Is electronic documentation safer for patients? This is often disputed. However, some concepts cannot be disputed when it comes to patient safety.

Treatment2Go
1�
Index
handtherapy.com
Typed evaluations and notes instead of handwritten can minimize medical errors. Example: many of us have had to decipher a doctor’s prescription that was scribbled in under 30 seconds? If it was typed, would it be easier to read? Most clinicians would say yes.
Electronic documentation is generally easier for clinicians to share information quickly when it is transcribed into an electronic medical record, especially in a hospital setting or where networking is established.
Patients sometimes have concerns regarding hacking and electronic safety. Safeguards should be taken to ensure that all servers are well protected and inaccessible to non-related personnel.
When charting electronically, the regulations from insurers and Medicare do not change. You must continue to provide comprehensive & concise notes. If you need to change or edit a note, most systems have a tracking mechanism that shows changes, deletions, and additions to each record.
Generally, non-clinical personnel will not be allowed access to the medical notes & some systems have password protection.
Although a transition to an electronic medical record may seem scary to some, it is likely the future of documentation. With the proper time and training, all clinicians can become proficient at using an electronic medical record.
►
►
►
►
►

Treatment2Go
1�
Index
handtherapy.com
Chapter 2Regulations and How to Stay on Top of the Information
Why is there always so much focus on Medicare’s rules and regulations?
Medicare is one of the largest providers of reimbursement for many occupational & physical therapy services. Additionally, many other insurers follow the lead of Medicare in deciding what to reimburse. For example, when Medicare decided to pay for bariatric surgery, many other insurers began to follow suit. Therefore, many of Medicare’s mandates and regulations significantly influence the policy of many other health care insurers.
Medicare guidelines and changes can be found at their website
http://www.cms.hhs.gov/home/medicare.asp
A basic overview of Medicare’s outpatient requirements include:
Written treatment plan must be certified by a physician (and again reviewed every 90 days)
Services must be provided by a qualified professional which means an OT,PT,SLP. Qualified professionals may also include PTA and OTA when working under the supervision of a qualified therapist. Note assistants are limited in services they may provide and they may not supervise others according to Pub 1002-2 transmittal 88 section 230.1 and 230.2)
Services must require the skill or supervision of a qualified therapist
Services provided can not be for maintenance of function
Services must address a recent change in function
Services must be directed toward a reasonably expected change in function
►
►
►
►
►
►
WEBSITE NAVIGATION INSTRUCTIONSWhen you go to the Medicare website there are several ways to access information. The most recent updates are usually listed under CMS highlights on the home page. However, this may cover all aspects of Medicare, not just re-habiliation. You can also search under “transmittals” in the Links box. Here you have the option to search by certain keywords such as Occupational Therapy.
Treatment2Go
1�
Index
handtherapy.com
An important note for therapists to remember is that Medicare does not pay for therapy directed toward improving leisure, work-related skills, or driving evaluations. Therefore, if a patient is referred to you for elbow pain that is only noticeable when they golf, this will not be a covered Medicare benefit. The therapist can work with the patient to determine how the elbow pain limits their day-to-day ADL functioning (i.e. does this pain make it difficult for this patient to lift their grocery bags, hook their bra, or push a door open?). If so, the therapist may continue care with careful thought of relating treatment to function or ADLs, not specifically, golf. With good care that addresses their functional needs – hopefully this patient will also notice that their pain resolves with golf although this may not be the specific goal of treatment!
Medicare History
An understanding of Medicare’s history leads us to understand why Medicare does not pay for leisure or work related activity. When Medicare was created in the 1960s, the average lifespan was 70 years. Now the average lifespan is 78! Therefore, when Medicare was created it’s primary goal was to provide coverage for the final, sickest years of someone’s life. Generally, the population was retired and less active than today’s older Americans. The program was not created to deal with a healthy, active, working population receiving Medicare services for more than a decade. Although medicine, life expectancy, and prevention have progressed since the founding of Medicare, policies regarding therapy interventions have not addressed this trend.

Treatment2Go
1�
Index
handtherapy.com
HOW DO I FIND MEDICARE’S RULES AND REGULATIONS?
A frustration for many outpatient therapists is Medicare’s retrograde review system. Many of Medicare’s rules and regulations are laid out on their website and in printed material. However, due to the use of fiscal intermediaries, the rules can vary from region to region. A fiscal intermediary (FI) is the local administrator for Medicare. Many of Medicare’s regulations are left to interpretation by the fiscal intermediary. Staying up to date with your FI is an important part of ensuring that you are documenting appropriately for reimbursement.
*Go online and identify your fiscal intermediary
http://www.cms.hhs.gov/ContractingGeneralInformation/Downloads/02_ICdirectory.pdf Once you have identified your FI, find their website and
bookmark it so you know where to go for updates!
One example of the necessity of staying up to date on Medicare regulation is the outpatient therapy cap. As part of the Balanced Budget Act in 1997, congress placed new caps on the amount of dollars a medicare beneficiary could use for PT, SLP ($1500 combined), or OT ($1500). Over the years this annual amount has been adjusted for inflation. In 2012 the amount has risen to $1880. Each
WEBSITE NAVIGATION INSTRUCTIONS:
In order to identify your fiscal intermediary, use the “search by state” section of this document (beginning on page 4). If you are a private outpatient provider you would need the group for Part B medicare. If you are affiliated with a hos-pital you are likely billing under Part A. If you are Home Health Provider - look for the abbreviation RHHI (Regional Home Health Intermediary). Once you have the name of your fiscal intermediary, you can go directly to their website for even more detailed aspects of reimbursement that will affect your practice. Often, Medicare leaves certain regula-tion open to interpretation by the local fiscal intermediary. Therefore, it is in your facilities best interest to be aware of any determination they make as well.

Treatment2Go
1�
Index
handtherapy.com
year congress has made modifications to this rule including an exceptions process for Medicare recipients who may need more than $1880 in services. It is our job as clinicians to know when our patients may near the end of their available benefit and discharge plan accordingly.
Medicare is also charged with finding new ways of ensuring fair treatment reimbursement that may not use the current cap structure. As part of this process, in 2013 Medicare will look into how function is reflected in therapy claims. Further information will be forthcoming in late 2012 as to how Medicare will collect this data from clinicians. Again, this demonstrates how a therapist needs to be aware of the regulatory changes and their impact on day to day documentation.
For most outpatient therapists working independent of a hospital, the listing under their state is the administrator for Part B is their fiscal intermediary (FI). The fiscal intermediary can decide to audit/review charts at any time and ensure that your daily documentation meets their guidelines for reimbursement. If your charts are not meeting their guidelines for any number of reasons – they can withhold or refuse full payment, a unit of payment or an entire course of care.
The statutory Medicare Part B outpatient therapy cap for CY 2013 is $1,900 for occupational therapy and $1,900 for physical therapy and speech-language pathology, combined. The cap is forever changing and you must keep abreast of the changes per year. The cap continues to be an annual per beneficiary amount for each calendar year and applies to all outpatient settings,
Treatment2Go
20
Index
handtherapy.com
including hospital outpatient departments (HOPDs). Yes, that is correct hospital outpatient departments are now included in the cap. Services provided in Critical Access Hospitals (CAHs) will be counted toward a patient’s therapy total (as converted fee schedule amounts), but CAHs themselves will not be subject to the cap or to reviews over $3,700. Since 1977 the exceptions have been extended to the end of the year in question (typically the present year). What that means to OT is that there is a modifier (typically the KX modifier) to claims above the cap therapy services that are reasonable and necessary.
Multiple Procedure Payment Reduction
Congress has increased the multiple procedure payment reduction (MPPR) amount to 50% across all settings beginning April 1, 2013. This is an increase from the earlier rate of 20% in office settings and 25% in facilities and is expected to result in an estimated payment reduction to therapy of 7%. What is also problematic is the fact that the policy does not distinguish the three therapy disciplines (OT/PT/SLP) and apply the MPPR separately to each.
AOTA is a great place for keeping abreast of the OT profession and APTA for PT profession. You are encouraged to visit and join your association. You can look for news updated via advocancy news.
http://www.aota.org

Treatment2Go
21
Index
handtherapy.com
Medicare Denials: What to Watch Out For
Denials can range from small errors to large problems with the entire course of care. Some examples of reasons for denial include:
Date in chart does not match date billed. Why should an insurer pay for a day of care which does not appear to have happened since you did not create a daily note for that day?
CPT code billed does not match what activities were documented for the session (for example: patient did a dressing activity in session but therapeutic exercise was billed).
Patient is performing maintenance activity in ongoing therapy with no expectation for improvement in function.
Additional reasons for denial will be discussed throughout this chapter.
Let’s review each area of documentation and the general Medicare requirements: Note Billing issues (functinal G Codes) are discussed in Chapter 3
Evaluation
A thorough evaluation of your patient should include the following information in order to satisfy Medicare guidelines:
A date of injury must be listed. You can not list a vague date of injury such as “3 months ago”. A specific date of injury is required. If the patient is unable to recount a specific date, use the date on the doctor’s prescription as a guideline.
Current diagnosis
History prior to admission
Recount patient’s functional status prior to admission. Comparing current status in your evaluation to immediate prior functional status is an important aspect of the evaluation. Status should be the patient’s functional level immediately prior to his/her current medical condition. If the patient was fully independent, living alone, doing all cooking and cleaning, taking self to medical appointments, etc. prior to stroke 3 months ago, make this clear in your documentation.
When a patient’s complaints have been lingering for some time and it is hard to pinpoint a “before and after” status, it is still expected you establish a prior level of function.
►
►
►
►
►
►
►
►
►
Treatment2Go
22
Index
handtherapy.com
An example of establishing a prior level of function is:
A patient dealing with cardiopulmonary issues whose endurance has been declining.
This patient has been struggling for several months but is able to perform his/her daily routine by taking extra time for all ADLs.
This patient was so tired and short of breath 1 month ago that he/she hired a housekeeper to help with cleaning and home maintenance. It would be useful to use the 1 month ago time frame as the date for change in status.
History of present illness (HPI)
A clear course of care prior to current therapy treatment is essential: including hospitalizations, skilled nursing stays, home health services, caregiver assistance, etc.
Poor HPI: Patient sustained a left sided CVA 6 months ago and was hospitalized for 1 month.►
Identify what the change was in their life that made them seek medical care

Treatment2Go
2�
Index
handtherapy.com
Good HPI: Patient sustained a left sided CVA 6 months ago. the patient was in ICU for one week and transferred to acute rehab for 3 weeks.
Went to SNF for 2 months and was then transferred to home with a home health aide 5x/week and home PT/OT for 2.5 months. Home therapy ended 2 weeks ago. Patient continues to need home health aide for bathing 3x/week.
Evaluation of current status: Medicare’s Transmittal 63 defines the type of evaluations used to show the patient’s current status with ADLs. Assessment of skills must be measurable and Medicare suggests (although you are not limited to) several standardized evaluations.
If you choose to do a separate non-listed evaluation, your measure of status must meet the following requirements: ”Functional assessment scores [must be] from tests and measurements validated in the professional literature that are appropriate for thecondition/function being measured or other measurable progress towards identified goals for functioning in the home environment” (Medicare Transmittal 63)
http://www.cms.hhs.gov/Transmittals/Downloads/R63BP.pdfTherapist’s clinical judgment about patient’s current status and expectation for recovery Prognosis
Plan of Care
Frequency and Duration
Expected time frame for completion of therapy course
The four suggested standardized evaluations are:National Outcomes Measurement System (NOMS) by the American Speech-Language Hearing Association
Patient Inquiry by Focus on Therapeutic Outcomes, Inc. (FOTO)
Activity Measure – Post Acute Care (AM-PAC)
OPTIMAL by Cedaron through the American Physical Therapy Association
►
►
►
►
►
►►
►
►
►
►
►
►
►
TIP: It is recommended to include additional information to support medical necessity of skilled therapy such as: co-morbities, additional therapists, cognitive limitation, current level of care-giver support, emotional status & medications.

Treatment2Go
2�
Index
handtherapy.com
Daily Notes
Medicare does not dictate the exact formatting or nature of the daily daily treatment note. However, a therapist is required to complete a daily note that demonstrates treatments provided as they relate to billed codes.
For example, if you bill ADL/self care, your note may include language such as “lower body dressing x� with instruction in use of a dressing stick to lift pants, patient dressed with minimal assist”.
Daily notes must include an accounting of total treatment time and total timed codes.
Progress Reports
These reports must be completed every 30 days or every 10 treatment days – whichever comes first! If you see someone 3x/week, you need to do a progress report on the 10th visit. This is your chance to justify that indeed you are providing skilled, necessary care. It is important to note how the patient is progressing toward stated STGs and LTGs. The progress reports confirm the therapist is continuing to progress toward the established
Total treatment time is the entire billed time spent with a patient
Total timed codes is the total amount of time you billed for “timed” codes:
Examples of timed codes include:U/S = 7 minutes treatment; 1 minute set-up
Therapeutic exercises =1 unit 8 minutes; 2 units = minimum 22 minutes
►
►
Examples of non-timed codes include:
Evaluations, re-evaluations and some modalities.
Treatment2Go
2�
Index
handtherapy.com
goals and that the initial goals are still relevant & functional. Also the goals should be attained in a reasonable time frame. Medicare does not define “a reasonable time-frame.” It is left to the judgment of the clinician. However, if you have more than a few sessions of therapy in which your patient is not making progress in at least one area, it is imperative you reconsider your goals and treatment approach. Medicare and other payers are reluctant to pay for care which is not being supported by improved patient outcomes.
Discharge reports
These are required to be completed by Medicare. They are a variation of a progress report that covers the final interval of care. This is your final chance to prove that the care you provided made a meaningful, functional difference to the patient. Discharge notes do not need to be signed by the physician but must be part of the chart. It is according to the clinics policy and procedures if they choose to send the discharge note to the physician.

Treatment2Go
2�
Index
handtherapy.com
Other Insurers and Documentation
Other insurers have similar guidelines. However, it is in your best interest to review each insurers regulations when you begin seeing their patients. For example, Blue Cross defines the following is to be included in an occupational therapy evaluation:
“Prior functional level, specific standardized and non-standardized tools, analytic interpretation...including a summary of the baseline findings in a written report; objective, measurable, and functional descriptions of an individual’s deficits... summary of clinical reasoning and consideration of contextual factors with recommendations; plan of care with specific techniques....frequency and duration of treatment plan; functional, measurable, and time framed long term and short term goals….prognosis…discharge plan that is initiated at the start of the therapy care.”
This is very similar to Medicare’s guidelines. They go on to define what is covered in daily treatments and report treatments can be 15 min to 4 hours. However, they state that treatments longer than 1 hour are rare and would need to be supported with further documentation.

Treatment2Go
2�
Index
handtherapy.com
Denials
There are many reasons why a course of care, a certain portion of care, or even a particular CPT code may be denied payment by Medicare. Several basic reasons were discussed earlier in this chapter. Throughout your course of rehabilitation intervention with a patient, you should be asking yourself the following questions:
Does my care continue to require the need of a skilled therapist?
Am I doing the same exercises with the patient every session? Is there a reason the patient needs me to supervise or could he/she be taught to progress at home independently?
Do my notes focus on achieving the goals established in the initial evaluation?
Does my patient continue to have the potential for improvement with skilled care? How long will it take to achieve this improvement?
Will therapy goals occur in a reasonable time frame? If you will need a month of 3x/week therapy to improve someone’s speed of dressing from 30 min to 25 min, this may be considered an insignificant gain for the amount of therapy intervention recommended. Change has to occur in a reasonable time-frame and be significant.
Will I be able to achieve a decrease in the amount of caregiver assistance needed?
Will I be able to increase someone’s independent living? For example, will the client be able to step down from skilled nursing care to assisted living?
►
►
►
►
►
►
►
View the three links below for additional information
Click here to read (page ��)
TERMINOLOGY DOS AND DON’TS
Click here to read: (page ��)
Skilled Action Verbs
To Deny or not to Deny........ That is the Question?
Click here to read (page �0)

Treatment2Go
2�
Index
handtherapy.com
Chapter 3Medicare Documentation and Coding
Medicare Documentation and Coding Update
Medicare’s basic assumptions rarely change - providing health insurance for those over �� or disabled. However, the implementation of Medicare and how it reimburses frequently changes. This may be a source of frustration for many therapists. However, it highlights the needs of the practitioner to stay abreast of updates in public policy. One of the best resources for updates is your professional association. If you are not already a member, it may be time to consider professional membership! Additionally, CMS and your fiscal intermediary (FI) often release updates and rules via their websites.
PQRS (Physician Quality Reporting System)
The PQRS program was started in 200� as way to incentivize “quality care”. Each health care profession was involved in creating measures that improved health care. A measure was some type of care that was considered high quality that may not be uniformly practiced. If an outpatient practitioner reported 1-� different measures consistently on at least �0% of their Medicare patients, they would be allotted a bonus payment at the end of the year. Many professional associations had members who participated in these multi-disciplinary measure development groups. For PT and OT, reporting on fall risk of a patient was the first PQRI measure many practices used. This was considered an important aspect of outpatient care

Treatment2Go
2�
Index
handtherapy.com
that may lead to less clients falling. As the program has developed, more measures have been added.
Practitioners now have a wider variety of measures to choose from and care tailor them to their specific practice area. With changes in legislation and the passing of the Affordable Care Act, the PQRS program became permanent and instead of being an incentive, will now be mandatory. Practitioners will now face a penalty of 1.�% for not reporting these measures. For practices not reporting in 201� – they will see a penalty in 201�.
To summarize: Occupational therapists who: (1) work in private practice
(2) bill Medicare using an individual-level National Provider Identifier (NPI) are subject to PQRS rules and regulations. Occupational therapists working in hospitals or skilled nursing facilities whose employers’ bill for their services (Bill OT services) are not subject to the program rules.
All PQRS measures (i1�1, 1��, 1��) are administered on a two year cycle; incentives paid in CY 201� & CY 201� is based on reporting during CY 2011 & CY 2012. Payment penalties for unsatisfactory reporting, which take effect CY 201�, will be based on reporting done in CY 201�. Example: All PQRS measures are reviewed and updated by Medicare every 1-2 years. In the past, if you were reporting Measure 1�� you only had to report fall risk. Now 1�� you must include follow up plan via report measure 1��.
IMPORTANT: Participation is now critical - in order to avoid Medicare payment cuts beginning in 2015, eligible occupational therapists should begin reporting on quality measures now.
In 201� there are 11 measures that PTs are allowed to report on and 1� measures for OTs. Relevant measures can be found on the CMS
►►

Treatment2Go
�0
Index
handtherapy.com
website and professional associations websitewww.aota.org
www.apta.org
www.cms.gov
Several examples include:
Measure 131 in which a clinician must provide a multi faceted assessment of the client’s pain on evaluation and document a follow up plan
Measure 154 which assess a client’s fall risk and must be paired
Measure 155 in which the clinician documents a follow up plan if a fall risk is present
An example of proper documentation
Measure 131 example:
Pain in right CMC joint which increases with pinch activity
Pain at worst is 6/10, and at best/least pain is a 2/10
Client describes pain as sharp and shooting
A custom orthotic will be fabricated to immobilize joint and reduce pain during functional activities and night use.
In this example you see the clinician has addressed the pain in a multi faceted manner – including pain scale, location of the pain, and type of pain. A follow up on how the pain will be addressed is included. Hence, the custom orthotic is the follow up plan of care. This is in relation to what the clinician found on initial evaluation.
►►►
►
►
►
►
►
►
►
Treatment2Go
�1
Index
handtherapy.com
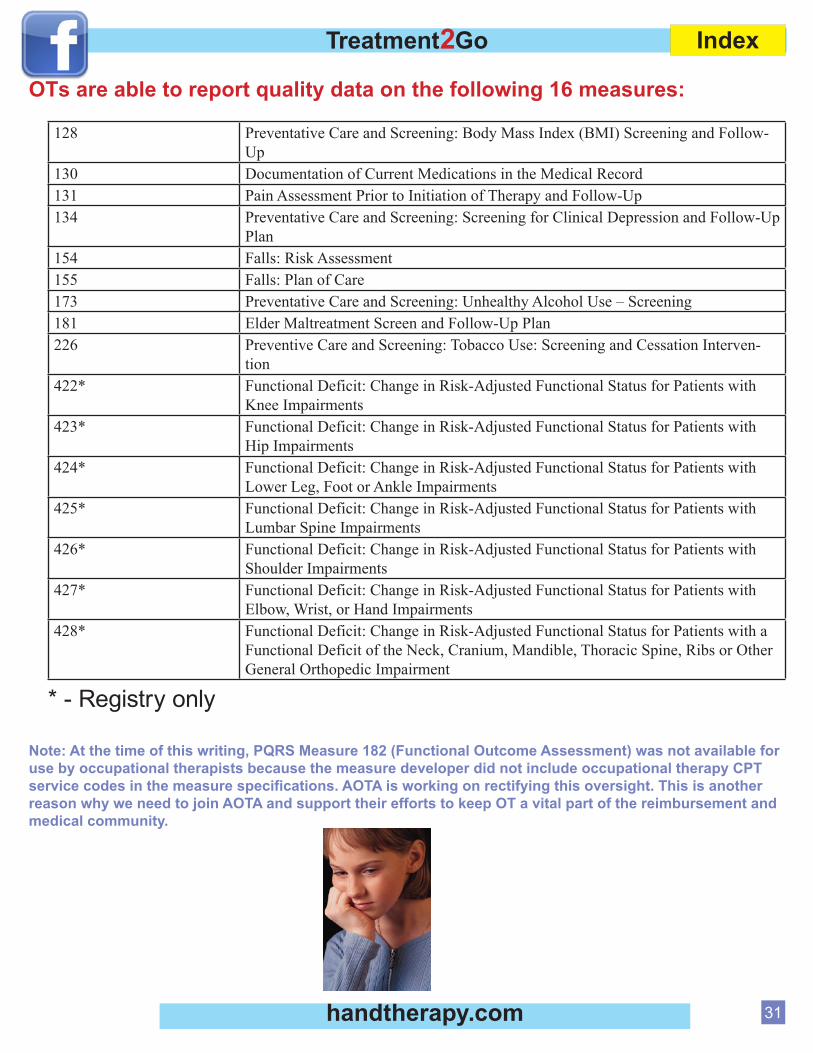
OTs are able to report quality data on the following 16 measures:
128 Preventative Care and Screening: Body Mass Index (BMI) Screening and Follow-Up
130 Documentation of Current Medications in the Medical Record131 Pain Assessment Prior to Initiation of Therapy and Follow-Up134 Preventative Care and Screening: Screening for Clinical Depression and Follow-Up
Plan154 Falls: Risk Assessment155 Falls: Plan of Care173 Preventative Care and Screening: Unhealthy Alcohol Use – Screening181 Elder Maltreatment Screen and Follow-Up Plan226 Preventive Care and Screening: Tobacco Use: Screening and Cessation Interven-
tion 422* Functional Deficit: Change in Risk-Adjusted Functional Status for Patients with
Knee Impairments423* Functional Deficit: Change in Risk-Adjusted Functional Status for Patients with
Hip Impairments424* Functional Deficit: Change in Risk-Adjusted Functional Status for Patients with
Lower Leg, Foot or Ankle Impairments425* Functional Deficit: Change in Risk-Adjusted Functional Status for Patients with
Lumbar Spine Impairments426* Functional Deficit: Change in Risk-Adjusted Functional Status for Patients with
Shoulder Impairments427* Functional Deficit: Change in Risk-Adjusted Functional Status for Patients with
Elbow, Wrist, or Hand Impairments428* Functional Deficit: Change in Risk-Adjusted Functional Status for Patients with a
Functional Deficit of the Neck, Cranium, Mandible, Thoracic Spine, Ribs or Other General Orthopedic Impairment
* - Registry only
Note: At the time of this writing, PQRS Measure 182 (Functional Outcome Assessment) was not available for use by occupational therapists because the measure developer did not include occupational therapy CPT service codes in the measure specifications. AOTA is working on rectifying this oversight. This is another reason why we need to join AOTA and support their efforts to keep OT a vital part of the reimbursement and medical community.
Treatment2Go
�2
Index
handtherapy.com
Functional G Code ReportingThis non-payable functional G code is for required reporting only. Functional G Codes is another change that occurred due to the Affordable Care Act. Change Request (CR) �00� which implements a new claims-based data collection requirement for outpatient therapy services by requiring reporting with �2 new non-payable functional G-codes and seven new modifiers on claims for Physical Therapy (PT), Occupational Therapy (OT), and Speech-Language Pathology (SLP) services. Be sure your billing staff knows of these new requirements.
This claims-based data collection system is being implemented to include both:
The reporting of data by therapy providers and practitioners furnishing therapy services, and
The collection of data by the contractors.
This reporting and collection system requires claims for therapy services to include non-payable G-codes and related modifiers. These non-payable G-codes and severity/complexity modifiers provide information about the beneficiary’s functional status at:
The outset of the therapy episode of care
Specified points during treatment
The time of discharge.
These non-payable functional G-codes and related modifiers are required on specified claims for outpatient therapy services – not just those over the therapy caps.
The reporting and collection requirements of beneficiary functional data apply to all claims for services furnished under the Medicare
►
►
►►►

Treatment2Go
��
Index
handtherapy.com
Part B outpatient therapy benefit and the PT, OT, and SLP services furnished under the Comprehensive Outpatient Rehabilitation Facility (CORF) benefit. They also apply to the therapy services furnished by a physician and certain Non-Physician Practitioners (NPPs), including, as applicable, Nurse Practitioners (NPs), Certified Nurse Specialists (CNSs), and Physician Assistants (PAs).
Services AffectedThese reporting requirements apply to the therapy services furnished by the following providers when billing Medicare Part B:
Hospitals
Critical Access Hospitals (CAHs)
Skilled Nursing Facilities (SNFs)
Comprehensive Outpatient Rehabilitation Facilities (CORFs) rehabilitation agencies
Home Health Agencies (HHAs) (when the beneficiary is not under a home health plan of care)
This new coding and documentation requirement went into effect 1/1/201� on voluntarily basis as of July 1, 201� it is mandatory.
As of July 1, 2013 any claims submitted without proper functional G coding will be returned as
incomplete - DENIED!!This new requirement must be determined and documented by the therapist; this is not for a billing/coding staff person to determine.
The purpose of the Functional G codes is to track the primary skill that is being addressed in therapy as well as the progress being made toward that goal.
This new requirement also changes the mandatory reporting period to every 10 visits.
CHANGE *** as previously the therapist could do their progress report every 30 days OR on the 10th visit (whichever was sooner), now only the 10 visit rule applies.
►
►
►
►
►
►►

Treatment2Go
��
Index
handtherapy.com
The functional G codes must be reported on initial evaluation and on/before the 10th visit.
What is a Functional G code?Functional G codes are the way a therapist notifies CMS of the primary goal they are addressing in therapy.
Currently there are �2 categories to choose from although 12 are most relevant to occupational and physical therapy.
Some examples of Functional G Codes include:
MobilityG8978 (Initial evaluation), Mobility: walking & moving around functional limitation, current status, at therapy episode outset and at reporting intervals.
Short descriptor: Mobility current status
G8979 (goal) , Mobility: walking & moving around functional limitation, projected goal status, at therapy episode outset, at reporting intervals, and at discharge or to end reporting.
Short descriptor: Mobility goal status
G8980 (D/C), Mobility: walking & moving around functional limitation, discharge status, at discharge from therapy or to end reporting.
Short descriptor: Mobility D/C status
Self-CareG8987 (Initial evaluation), Self care functional limitation, current status, at therapy episode outset and at reporting intervals
Short descriptor: Self care current status
G8988 (goal), Self care functional limitation, projected goal status, at therapy episode outset, at reporting intervals, and at discharge or to end reporting.
Short descriptor: Self care goal status
G8989 (D/C), Self care functional limitation, discharge status, at discharge from therapy or to end Reporting
Short descriptor: Self care D/C status
►
►
►
►
►
►
►
►
►
►
►
►

Treatment2Go
��
Index
handtherapy.com
Moving & Handling & Carrying ObjectsG8984 (Initital evaluation), Carrying, moving & handling objects functional limitation, current status, at therapy episode outset and at reporting intervals
Short descriptor: Carry current status
G8985 (goal), Carrying, moving & handling objects functional limitation, projected goal status, at therapy episode outset, at reporting intervals, and at discharge or to end reporting
Short descriptor: Carry goal status
G8986 (D/C), Carrying, moving & handling objects functional limitation, discharge status, at discharge from therapy or to end reporting
Short descriptor: Carry D/C status
Within each category there are 3 coding choices: A code for current status
A code for your goal in this category
A code for a client’s discharge status in this category.
On evaluation, the clinician must report current status and goal. G8984 CM (inital eval) Note the CM, CL are modifiers. They are discussed later.
G8985 CL (goal)
On the 10th visit a progress report is required and the clinician reports current status and goal
8985 CK (current status; note improved modifier from above)
8985 CI (goal)
On the discharge, therapist reports the discharge status8986 CI (at D/C functional status with Modifer addressing goal)
This is the modifier table for your convenience (to discuss in more detail shortly)Modifier Impairment Limitation/ RestrictionCH 0% 0 percent impaired, limited or restrictedCI 1-19% At least 1 percent but less than 20 percent impaired, limited or restrictedCJ 20-39% At least 20 percent but less than 40 percent impaired, limited or restrictedCK 40-59% At least 40 percent but less than 60 percent impaired, limited or restrictedCL 60-79% At least 60 percent but less than 80 percent impaired, limited or restrictedCMCN
80-99%100%
At least 80 percent but less than 100 percent impaired, limited or restricted 100% impaired, limited or restricted
►
►
►
►
►
►
►►►
►►
►►
►

Treatment2Go
��
Index
handtherapy.com
EXCEPTION of reporting G CODE:When a patient has achieved a set goal you would have to document the functional G code when they achieve the goal and not wait for the 10th visit.
You would then do a progress report showing goal(s) has been met, and
if appropriate, set a new goal (while also reporting current status)
Example of Exception to the 10 day reporting:
You plan to address grip strength as your goal for a client:Clinical goal on evaluations is:
Client will increase grip strenth from 5 lbs to 10 lbs to lift a grocery bag from car to house within 10 visits
G8984 CM (initial eval functional G Code and modifier)
G8985 CL (goal with modifier)
Exception of reporting:
Day �: Your clinet has met the above stated goal (note this is earlier than the 10 day mandatory reporting time frame - the exception). A re-evaluation report and/or a D/C note with G-code and modifier for the particular reporting period is needed for the specified goal.
8986 CL (this is the D/C G code with modifier at d/c)
You can now set a new goal and report the current status of that goal. In this example, you would be submitting three (�) G-codes:
The D/C Code (8986 CL) Note this is for moving/carrying objects
Establish new current status for another impairment (8988 CM). Now let’s use impairment in self care
The new goal in self care (8988 CK): Patient will increase grip strength from 10 pounds to 20 pounds to grasp a hair dryer for 20 minutes for personal hygeine
Now we have established the original goal on initial evaluation with modifiers and the current status. A re-evaluation was completed on day � (do not wait until 10th mandatory day due to goal achieved
►
►
►
►►
►
1)
2)
3)

Treatment2Go
��
Index
handtherapy.com
early). You addressed the original goal (G code) and current status (modifier). Then you established a new goal (G Code) with current status (Modifier).
In summary:
The functional G-codes are non-payable. Functional G codes require a corresponding severity modifier for certain Dates of Service (DOS). Functional G codes are non-billable and in addition, claims containing any of these functional G-codes must also contain another billable and separately payable (non-bundled) service. This non-payable G code is for required reporting only.
Only one functional limitation shall be reported at a given time for each related therapy plan of care (POC). However, functional reporting is required on claims throughout the entire episode of care; so, there will be instances where two or more functional limitations will be reported for one beneficiary’s POC, just not during the same time frame. This was illustrated in our “exception example”
In these situations, where reporting on the first reported functional limitation is complete and the need for treatment continues, reporting is required for a second functional limitation using another set of G-codes. Thus, reporting on more than one functional limitation may be required for some beneficiaries, but not simultaneously.
It should be making sense now... you should be getting the concept.

Treatment2Go
��
Index
handtherapy.com
Required Reporting of Functional G-codes and Severity Modifiers
Specifically, functional reporting, using the G-codes and modifiers, is required on therapy claims for certain Date of Service (DOS) as described below:
At the outset of a therapy episode of care, i.e., on the DOS for the initial therapy service
At least once every 10 treatment days -- which is the same as the newly-revised progress reporting period -- the functional reporting is required on the claim for services on same DOS that the services related to the progress report are furnished.
The same DOS that an evaluative procedure, including a re-evaluative one, is submitted on the claim (see below for applicable HCPCS/CPT codes)
At the time of discharge from the therapy episode of care, if data is available, and
On the same DOS the reporting of a particular functional limitation is ended in cases where the need for further therapy is necessary.
The below HCPCS/CPT Codes must have an accompanied Functional G-code(s) and appropriate Corresponding severity/complexity modifier(s) for reimbursement, effective July 1, 2013. Claims that do not include required functional reporting information will be returned or rejected.
�2�0� �2��� �2�0� �2�0� �2�10�2�11 �2�12 �2�1� �2�1� ��10���12� ��001 ��002 ��00� ��00
NOTE *** When functional reporting is required on a claim for therapy services, two G-codes will generally be required as noted in our previous examples
Two exceptions exist1. Therapy services under more than one therapy POC. Claims may contain more than two non-payable functional G-codes when in cases where a beneficiary receives therapy services under multiple POCs (PT, OT, and/or SLP) from the same therapy provider.
2. One-Time Therapy Visit. When a beneficiary is seen and future therapy services are either not medically indicated or are going to be furnished by another provider, the clinician reports on the claim for the DOS of the visit, all three G-codes in the appropriate code set (current status, goal status and discharge status), along with corresponding severity modifiers.
►
►
►
►
►
►
►
►

Treatment2Go
��
Index
handtherapy.com
Each reported functional G-code must also contain the following essential line of service information:
Functional severity modifier in the range CH - CN
Therapy modifier indicating the discipline of the POC –GP, GO or GN – for PT, OT, and SLP services, respectively
Date of the corresponding billable service
Nominal charge
Note: The therapist or physician/NPP furnishing the therapy services must not only report the functional information on the therapy claim, but, he/she must track and document the G-codes and modifiers used for this reporting in the beneficiary’s medical record of therapy services.
Evaluative Procedures: The presence of an HCPCS/CPT code on a claim for an evaluation or re-evaluation service listed as follows requires reporting of functional G-code(s) and corresponding modifier(s) for the same date of service:
In the example below, the G-codes for the mobility functional limitation (G8978 - 8980) are used to illustrate the timing of the functional reporting.
At the outset of therapy --the DOS the evaluative procedure is billed or the initial therapy services are furnished.
G8978 and G8979, along with the related severity modifiers, are used to report the current status and projected goal status of the mobility functional limitation.
At the end of each progress reporting period --the DOS when the progress report services are furnished.
G8978 and G8979, along with the related severity modifiers, are used to report the current status and projected goal status of the mobility functional limitation.
This above step is repeated as clinically appropriate
At the time the beneficiary is discharged from the therapy episode --the DOS the discharge progress report services are furnished.
G8979 and G8980, along with the related severity modifiers, are used to report the projected goal and discharge status of the mobility functional limitation.
►►
►►
►
►
►
►
►
►
►
►

Treatment2Go
�0
Index
handtherapy.com
In the above example, if further therapy is medically necessary once reporting for the mobility functional limitation has ended, the therapist begins reporting on another functional limitation using a different set of G codes.
Reporting of the next functional limitation is required on the DOS of the first treatment day after the reporting was ended for the mobility functional limitation.
To review again to ensure your understanding, you must report functional G codes at:
Start of care
At 10 day (or sooner if goal is achieved) progress report
Any time you bill for a re-evaluation
Upon completion of a goal
Upon discharge
What is a functional G code modifier?When reporting a G-code, you must also present a modifier. The modifier quantifies how the client is able to perform the skill. There are � modifiers to choose from.
Modifier Impairment Limitation/ RestrictionCH 0% 0 percent impaired, limited or restrictedCI 1-19% At least 1 percent but less than 20 percent impaired, limited or restrictedCJ 20-39% At least 20 percent but less than 40 percent impaired, limited or restrictedCK 40-59% At least 40 percent but less than 60 percent impaired, limited or restrictedCL 60-79% At least 60 percent but less than 80 percent impaired, limited or restrictedCM 80-99% At least 80 percent but less than 100 percent impaired, limited or restrictedCN 100% 100 percent impaired, limited or restricted
The functional G-codes and corresponding severity modifiers listed above are used in the required reporting on specified therapy claims for certain Dates of Service (DOS).
1)
2)
3)
4)
5)
Treatment2Go
�1
Index
handtherapy.com
Only one functional limitation shall be reported at a given time for each related
therapy plan of care (POC). However, functional reporting is required on claims throughout the entire episode of care; so, there will be instances where two or more functional limitations will be reported for one beneficiary’s POC, just not during the same time frame or reporting period.
In these situations, where reporting on the first reported functional limitation is complete and the need for treatment continues, reporting is required for a second functional limitation using another set of G-codes. Thus, reporting on more than one functional limitation may be required for some beneficiaries, but not simultaneously.
Therefore, you may use the self-care goal and then state that client’s current status is CK (�0-�0% limited/restricted), and your goal G code may report with a CI (1-1�% limited/restricted) modifier.Example:
Evaluation status: Pt. unable to use her right hand for ADLs including brushing teeth, dressing, and using eating utensils due to stiffness and increased pain >�/10
Goal: Pt. will be able to brush her teeth for 2 minutes using her right involved hand with reported pain of <�/10
Evaluation Self Care and current status (modifer): G8987 CK
Goal self care: G8988 CI
Modifier: Current StatusCK 40-59% At least 40 percent but less than 60 percent impaired, limited or restricted
►►
►

Treatment2Go
�2
Index
handtherapy.com
Modifier: Goal of patient 10th visit.CI 1-19% At least 1 percent but less than 20 percent impaired, limited or restricted
Frequently Asked Questions:Is it always mandatory to use a modifier with functional G Codes?
Is the modifier also changing every 2 years?
Is modifier part of the patient’s record or part of billing only?
Are the modifiers (impairment limitations restrictions) determined by a standard way or just “therapist knowledge” to choose how limited one is?
When therapists address the 10th visit note, do they address the limiting modifier and when they set a new goal are they choosing a new limiting modifier?
Does the QUICKDASH give the impairment rating?
Answers:Yes, it is always mandatory to provide a modifer (limitations/restrictions/impairment) with G Codes.
No. The modifiers do not change. Frequent changes refer to PQRS which is completely unrelated to functional G Codes and modifiers
Modifiers is listed in the billing but it is certainly beneficial on the therapist’s end to also document % of impairment. Follow the policy and procedure of your facility.
The modifiers are based on standarized outcome measures and should be determined based on outcome measures that the therapists may use. An example would be the QuickDash, Canadian Occupational Performance Measures, etc
Yes. It is recommended the therapists include the current status modifier (%) of the goal the client has achieved and, if appropriate, set a new goal with a new modifier (%) of achievement.
As an example, the QuickDash is scored on a 0-100 scale. The score easily translates into the same number for the modifier scale. However, other outcome measures may not be on a 0-100 scale. It is up to the therapists to convert their score to the appropriate impairment modifier. There are also third party tools online that allow you to pick your outcome tool, enter the score and the algorithm converts to a G code modifier for you.
Your documentation must support the functional G code that you have chosen and your rationale for
choosing the modifier you report.
►
1)
2)
3)
4)
5)
6)
1)
2)
3)
4)
5)
6)
Treatment2Go
��
Index
handtherapy.com
What this means is if you state your client is �0% impaired in picking up and transferring a pot from stove to sink; you should include why. “Client is �0% impaired because they can only lift a pot that is half full”Another Example:
Initial Evaluation patient presented with bulky post op dressing with hand in a dorsal blocking splint. Pt. unable to use hand due to risk of rupturing tendons and rendering her hand useless. Currently patient unable to care for self with right involved hand:
Functional G Code: SELF CARE G���� (Inital) and G���� (goal)
Modifier: Current status at evaluation: (DOS Jan 1, 20XX)Modifier CN = 100% impaired, limited or restricted. Your rationale is due to splint and risk of rupture so you would choose modifier CN or use the QuickDash
G8987CN
Goal: Patient will d/c splint in 5 weeks and begin to mildly incorporate right injured hand into less than 10% of assisting left hand for brushing teeth (note patient in therapy 2X week so 5 weeks is 10 visits)
Modifier CM = 80-99% At least 80 percent but less than 100%percent impaired, limited or restricted. Use this with:
G8988CM
On the 10th visit (� weeks later), a progress report for self care with reporting the G codes is required: DOS (FEB �, 20XX)Current Status: Patient achieved established goal of D/C splint and using right injured hand minimally assist with brushing teeth:
Modifier CM = 80-99%At least 80 percent but less than 100 percent impaired, limited or restricted
G8988CM
►
►
►
►
►
►

Treatment2Go
��
Index
handtherapy.com
New Goal: Patient will use the right dominant involved hand to dress self including buttons/zippers with �0% accuracy in 10 visits.
New Goal Modifier (note SELF CARE G8988 is still used)
Modifier CJ 20-39% = At least 20 percent but less than 40 percent impaired, limited or restricted
Progress report on the 10th visit (note this is the 2nd progress report or 20th visit)
Current Status: (March �, 20XX)
Achieved established goal and the current status as of DOS:
Modifier CJ 20-39% = At least 20 percent but less than 40 percent impaired, limited or restricted
G8988CJ
New Goal: Patient will have 100% use of hand for self care including dressing
Modifier of new established goal:Modifier CH 0% = 0 percent impaired, limited or restricted for the Goal
G8988CJ (this is the current status becasue the new goal is just established)
DOS: (March �0, 20XX) D/C functional G����, Self care functional limitation, discharge status, at discharge from therapy or to end Reporting
Current status at D/C Modifier:Modifier CH 0% = 0 percent impaired, limited or restricted
G8989 CH = D/c status with Goal Acheived
POC: D/C to home program with no restrictions.
►
►
►
►
►
►
►
►
Treatment2Go
��
Index
handtherapy.com
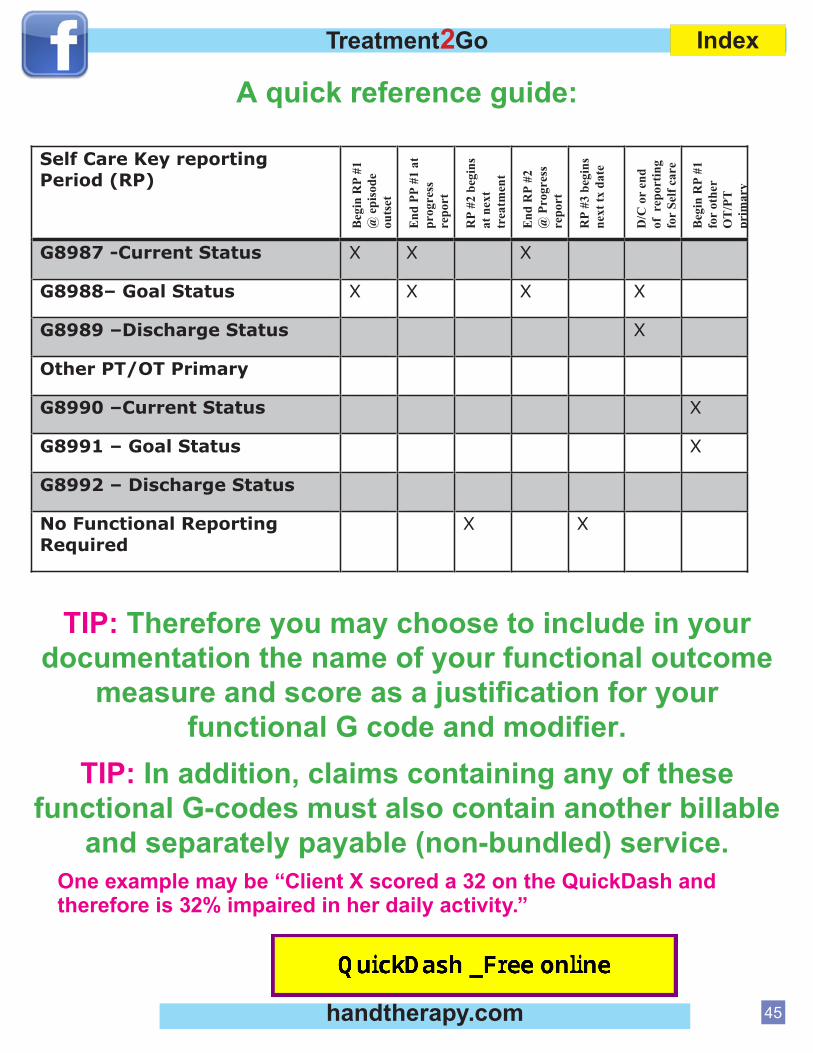
A quick reference guide:
TIP: Therefore you may choose to include in your documentation the name of your functional outcome
measure and score as a justification for your functional G code and modifier.
TIP: In addition, claims containing any of these functional G-codes must also contain another billable
and separately payable (non-bundled) service.One example may be “Client X scored a 32 on the QuickDash and therefore is 32% impaired in her daily activity.”
Self Care Key reporting Period (RP)
Beg
in R
P #1
@
epi
sode
ou
tset
End
PP
#1 a
t pr
ogre
ssre
port
RP
#2 b
egin
s at
nex
t tr
eatm
ent
End
RP
#2
@ P
rogr
ess
repo
rt
RP
#3 b
egin
s ne
xt tx
dat
e
D/C
or
end
of r
epor
ting
for
Self
care
Beg
in R
P #1
fo
r ot
her
OT
/PT
pr
imar
y
G8987 -Current Status X X X
G8988– Goal Status X X X X
G8989 –Discharge Status X
Other PT/OT Primary
G8990 –Current Status X
G8991 – Goal Status X
G8992 – Discharge Status
No Functional Reporting Required
X X

www.handtherapy.comExploringHandTherapy
Q: G‐Codes…What are they A: January 2013 CMS began accepting Claims‐Based Outcomes Reporting (CBOR) with Medicare Part B claims. Failure to report G‐code modifiers by July 1, 2013 will result in an automatic denial of the claim.
Q: Does coding (G ‐codes and modifiers) have to be in billing or just in charting documentation?
A: The G‐codes and modifiers must be in both documentation and on the claim.
Q: Do we continue to use the MD dx code and PT dx code along with our G‐codes? A: Yes. CBOR is purely an additive from a coding perspective. Change nothing else that you are doing. Q: If you didn’t realize the patient would be D/C , can you resubmit the last visit with the D/C code? A: If you did not plan on discharging the patient at that visit and no outcomes measure has been assessed, then you do not submit G codes with that visit. Q: IF you are treating a person for maintenance such as in Parkinson’s (neurological) how would the G‐code apply? A: Claims‐Based Outcome Reporting (CBOR) is independent from medical necessity and justifications for payment of therapy services. A patient’s reason for therapist must be made as a clinical and business judgment and stand on its own merit. If the patient/therapist decides therapy is reasonable and necessary and services are rendered, you must submit G‐codes to get paid. Whether or not the G‐codes change will not determine payment. Q: If a therapist is seeing a patient for at least two separate functional impairments such as fabrication of Orthotics and rehabilitation for flexor tendon injury, would this require two separate evaluations and two separate G codes. How does it work to see both situations at the same time? A: An occupational therapist seeing and treating the client for multiple impairments is perfectly acceptable. The therapists however must select one primary impairment and only apply 1 G code and modifiers to that one functional deficit. Only the primary functional deficit for each discipline treatment of the patient will be reported. Q: If the patient never returns to therapy and virtually self discharges what G code is needed? A: You do not have to supply a discharge G‐code if the patient self‐discharges and you do not have a reasonable estimate of their progress. Q: If you are treating for wound care clinics, debridement, Lymphedema and/or orthotics training how would G‐codes be applied?

www.handtherapy.comExploringHandTherapy
A: CMS provides impairment categories of “other” for impairments that do not fit into the other categories.
Q: What if the client is seen for only 1 Visit for home program or orthotics. How do I report G codes?
A: CMS states in their CR8005 MLN Matters that one time visits must be coded with three sets of G codes and modifiers for initial, goal and discharge.
Q: Can you enter more than one primary G code at a time? If not, what is recommended if a patient has multiple deficits that will be treated simultaneously? Example ‐memory and difficulty carry items. A: The primary deficit for each discipline is reported and the GN, GO, GP modifiers must be applied. If OT is seeing the patient for both memory and difficulty carrying items, only the one area of greatest clinical/treatment focus should be reported.
Q: When billing as a hospital would you bill the goal G‐code on each claim?
A: CMS has not published the specific claims processing requirements yet; however, they have stated claims timelines are independent from when G‐codes should be submitted. G‐Codes are submitted on evaluation, re‐evaluations, progress notes no less than every 10 treatment visits, change in primary condition, material change in current condition and upon discharge. Also, if any of the following procedure codes are billed, G‐codes must be on that date of service on the claim: 92506, 92597, 92607, 92608, 92610, 92611, 92612, 92614, 92616, 96105, 97001, 97002, 97003, 97004
Q: For a first claim would you have the evaluation and goal G‐codes on the claim? A: Yes, for each discipline treating the patient. Q: Are there free tools available for figuring out G‐code modifiers? A: Yes there are many. One of them is: www.mediserve.com/cbor‐old‐browser?assessment+FOTO+lumbar+Functional+status
Q: What about writing goals?
A: As long as the goals are functional and the documentation contains the G‐codes with modifiers somewhere, the requirements will be met.
Q: How would we use a progression from walking with a walker to a cane?
A: Moving from one assistive device to another is not likely to meet CMS requirements for objective, functional measurement instruments without further clarification of the functional deficit. As a suggestion, AM‐PAC or FOTO are good ways to provide a numeric value to the functional gains you are describing.

www.handtherapy.comExploringHandTherapy
Q: Do we really need to write goals, if we are using these tools and scales to justify our care
A: Yes. CMS maintains G‐codes are derivatives of the written and more explicated functional goals. In 2008, CMS updated the manual to include more requirements for functional outcomes reporting. Pub. 100–02, Chapter 15, Section 220.3, Subsection D) http://www.cms.gov/Regulations‐and‐Guidance/Guidance/Manuals/Downloads/bp102c15.pdf They assume everyone is already following these requirements and adding 2‐4 additional G‐codes on the claim are the only additional burden.
Q: How do you write out the codes in the documentation?
A: The requirements can be found at: http://www.cms.gov/outreach‐and‐education/medicare‐learning‐network‐mln/mlnmattersarticles/downloads/MM8005.pdf An example might be….An evaluation would have the following documentation in it: CPT Document standardized test used and score G code and description for the primary impairment C Modifier for current level (per translation from standardized test Score) Clinical text goal (Pt will ambulate household distances with rolling walker….etc..) C Modifier goal level Any other non‐primary goals per the patients plan of care
Q: These codes just go on IE, Re‐evals, and DC, correct?
A: From CMS Transmittal 163: “Specifically, functional reporting, using the G‐codes and modifiers, is required on therapy claims for certain DOS as described below: • At the outset of a therapy episode of care, i.e., on the DOS for the initial therapy service; • At least once every 10 treatment days — which is the same as the newly‐revised progress reporting period — the functional reporting is required on the claim for services on same DOS that the services related to the progress report are furnished; • The same DOS that an evaluative procedure, including a re‐evaluative one, is submitted on the claim (see below for applicable HCPCS/CPT codes);” Here is the list of evaluation codes requiring G‐codes on the same date of service: 92506, 92597, 92607, 92608, 92610, 92611, 92612, 92614, 92616, 96105, 97001, 97002, 97003, 97004, 96125. They have also stated needing G‐codes when switching from primary to subsequent areas of impairment and when a noticeable change in function warrants a reassessment.
Q: Can we use a non‐electronic outcome survey instrument such as the Berg?
A: Yes. CMS only recommends the AM‐PAC, FOTO, NOMS and OPTIMAL, but is clear that any valid functional measure can be used.

www.handtherapy.comExploringHandTherapy
Q: Do G codes/modifiers need to be reported for patients with Medicare as a secondary insurance, or just those with Medicare as primary?
A: Yes; CMS is going to require data collection when Medicare is both primary and secondary. Q: Where in the initial evaluation should the G‐codes and C modifiers be mentioned? Under demographics or in the goal section of the note?
A: There is no specific instructions on where to put it; however, if the audience you are trying to please is an auditor, I would put it in the assessment and goals section, especially if you are going to over ride the score with professional judgment. Q: On the 10th visit, if we forget to put the updated codes, will Medicare deny payments or will we be able to add them and resubmit? A: You will get denied initially; however, the appeal process has not been clarified yet. Q: Are we to only use one G‐code, even if there are multiple problems? Once one problem is resolved, and we are still working on another…do we then re‐establish new G and C? A: You can only code one functional area at a time. That requires two G‐codes. The Goal G‐code and either the Current Status or Discharge code. Yes, you must transition to a new functional area when the current area is no longer the primary functional area being treated. This transition must be done over two visits / documents. On visit x, you document the goal and discharge codes. On the next visit (visit x+1), you document the Current Status and goal codes for the new functional area of focus. Q: I have a patient that becomes eligible for Medicare Part B midway through his established therapy plan of care. On the first day… that Part B will be billed…does the therapist have to submit G codes and modifiers…as it might not be time for a progress summary. Or, can they wait till a progress summary is due? Does the therapist have to submit G codes and modifiers…as it might not be time for a progress summary. Or, can they wait till a progress summary is due? A: It’s a new insurance. They would be discharged from the previous payor with a new start date, evaluation and plan of care. G codes start that day. Many questions answered from MediServe: a Mediware Company. This service is a free conversion for measurement tools. This is one good free resource: http://www.mediserve.com/cbor‐old‐browser/?assessment+FOTO+lumbar+Functional+status

Treatment2Go
��
Index
handtherapy.com
Resources:http://www.cms.gov/outreach-and-education/medicare-learning-network-mln/mlnmattersarticles/downloads/MM8005.pdf
http://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R2622CP.pdf
Disclaimer:This chaper 3 may contain references or links to statutes, regulations, or other policy materials. The information provided is only intended to be a general summary. It is not intended to take the place of either the written law or regulations. We encourage readers to review the specific statutes, regulations and other interpretive materials for a full and accurate statement of their contents.
Bravo... you are now experts on reporting Functional G codes.
►
►
►

Treatment2Go
��
Index
handtherapy.com
Chapter 4TELLING THE THERAPY STORY
Documentation is the record of a patient’s course through the medical system. It is also an accounting of what you did with a patient in order to get reimbursed for your skilled intervention. Therefore, it is imperative that your recording (written or electronic notes) tells the thorough, yet concise, story of a patient’s therapy journey. The story begins on the day you meet and evaluate the patient, the middle of the story is your daily notes, and then, hopefully, a happy ending is your discharge evaluation.
Consider several movies or books you have loved. Why have you loved about them? You probably loved them because they had engaging characters (your patient), a good plot (your treatment plan), and good ending (discharge). Think again of a movie or book you hated or really disliked. Why did you have such a strong negative reaction to this? Often people do not like a book or movie that has too many characters, too many sub-plots, isn’t about what you thought the topic was, or drags on too long and becomes boring. Your documentation can easily fall into the good movie or bad movie category. Notes that are denied by insurers often have many of the same problems a bad movie or bad book might have.

Treatment2Go
��
Index
handtherapy.com
Here are some things to think about as you plan your course of care for a patient…
Do my goals cover all of the things I will need to accomplish in therapy? This is the outline of your plot. Make certain you set both short term and long term goals that will cover the entire course of care. This includes creating long term goals that will reflect patient’s improving status.
As I continue with my treatment sessions, am I following the original plan? If no, have I reasonably explained my deviation from the original plan?
Do I show how the therapeutic exercises reflect a functional activity that the patient needs to perform?
When you reflect on these questions regularly, you will have better directed notes that are less likely to be denied. Often times during a course of a care, a patient may suggest a functional task they would like to improve and you begin to incorporate this into your care without good documentation.
Here’s an example of a chart summary:
Patient was evaluated post-CVA for outpatient rehabilitation. The patient had Medicare for his/her insurance. Goals on the initial evaluation focused on returning the patient to independence with ADLs such as check writing, meal preparation, & fine motor tasks such as buttoning and zippering.
The patient’s primary complaint was decreased coordination of her dominant hand. This patient had not worked for 1 year prior to the stroke and lived alone.
The therapist’s daily notes showed a steady progression toward the stated goals for the first month of care. Following the first re-evaluation, the patient’s progress hit a plateau. The therapist tried various avenues of treatment in order to “jump-start” progress. The patient mentioned that she used to work as a manicurist and was hoping to return to work one day. Seizing the idea that this functional task also addressed fine motor
►
►
►

Treatment2Go
��
Index
handtherapy.com
coordination, the therapist began using nail painting/nail hygiene as a therapeutic task. For two weeks the patient’s sessions primarily focused on using a nail polish brush for both accuracy and timeliness. The patient began again to show progress in her fine motor skills.
Do you think this chart would be fully or partially reimbursed?
What is the basis of your decision?
This chart was denied for the three weeks of treatment that focused on nail painting. The therapist assumed if she/he included nail hygiene in her notes, it would qualify for skilled, necessary care. However, there are several problems with this portion of the chart and therapy sessions.
This patient has Medicare. Medicare does not reimburse for work related tasks. The therapist tried to portray the treatment as important for nail hygiene however she only worked on painting the nails, not cleaning the nails or trimming the nails.
The problem area of nail hygiene was never identified on the evaluation and a goal was never set addressing this area.
►
►
This would be an example of bringing in a sub-plot that detracts from the story and that is unjustified.

Treatment2Go
�0
Index
handtherapy.com
Please spend a few minutes reviewing this chart summary below and decide if it “tells the therapy
story”.Chart summary Review Example
A patient with an HMO insurance has been seen for �� visits of occupational therapy for lateral epicondylitis and then a lateral epicondylectomy. Therapy occurred from February to December. She had �0 visits prior to surgery and then �� visits following her surgery.
The therapist was requesting an appeal for additional visits after her first request was denied. The patient was a college student who was unable to spend more than a few minutes on the computer before the pain forced her to stop. She was unable to complete many assignments and exams that required computer access. Initial treatment focused on reducing the pain in order to allow greater time at the computer without pain. A variety of therapeutic exercises were prescribed that included forearm stretching, wrist curls, and digit extension exercises. Therapeutic modalities including ultrasound and electrical stimulation were also provided. When the patient continued to be limited after the first round of therapy, she received surgery.
Following surgery, the patient resumed therapy. The goals were similar including, tolerating the computer for longer periods of time without pain & being able to complete schoolwork.

Treatment2Go
�1
Index
handtherapy.com
Treatment again included therapeutic exercises, modalities, and now scar management techniques. Re-evaluations were initially submitted monthly. However, as treatment progressed and the patient attended therapy less regularly (2-�x/month) re-evaluations were more intermittent. The patient’s progress showed increased time at the computer from � minutes to � minutes until onset of pain that patient rated as a �/10. The review was requested after care ended in December due to lack of re-evaluation documentation. The last submitted re-evaluation with quantifiable measures was in July of that year.
Would you authorize additional visits? What questions would you need to have answered?
The request for additional visits were denied for several reasons:Patient should have been progressed to a home program. The exercises did not significantly change throughout the course of care. The patient should have been instructed on how to safely progress her exercise program at home.
Progress shows an increased time tolerated at the computer from 3 minutes to 8 minutes over several months. This would be considered very limited progress over several months. Eight minutes is not a functional amount of time to be able to use computer before needing a break. It is doubtful that this student could have completed much schoolwork in 8 minute intervals.
Lack of measurable re-assessments also lead to denial. There is no documentation of measurable gains after months of rehabilitation care. Therefore, it is
impossible to tell if therapy is/was beneficial for this patient.
►
►
►

Treatment2Go
�2
Index
handtherapy.com
CHAPTER 5WRITING RELEVANT GOALS
Insurance companies increasingly ask for therapy to be functionally oriented. Medicare, it is now mandatory (G codes) & other private insurace Co.are following CMS. Function is a meaningful measure of the success of rehabilitation. Yet all too often, therapists notes focus on the components of rehabilitation such as increasing range of motion, increasing strength, increasing endurance, and decreasing pain and ignoring specific function. The therapist may believe if a patient increases strength, their function will also improve. However, this is not always the case. Therapists need to spell it out for the payers.
Too often goals are written for the components but could be easily adjusted to incorporate function. A goal such as “patient will increase shoulder flexion to 120°” is not functionally oriented. However, the addition of four simple words makes this a meaningful goal. “Patient will increase shoulder flexion to 120° to don shirt independently.” This goal is functional, measurable, and meaningful.
Complete the worksheet “Documenting Functionally”... then return to the course.

Treatment2Go
��
Index
handtherapy.com
Patients sometimes have a difficult time identifying their own functional goals for the therapist. It is imperative that the therapist spend the time to help the patient find areas in which they are having difficulty. For example, the patient states “my hand is stiff, especially in the morning, but I manage to do everything." If the patient is “able to do everything,” do we need to be treating this patient? That is the question the insurance company hopes to see answered in your evaluation and reflected in your goals.
Pause here and think about 3 questions you might ask this patient to help create functional goals.
With the previous patient, you might ask:How long it takes for the patient to resolve the stiffness in the morning?
Does it delay the start of their day?
Are they getting less sleep because they have to wake up earlier to deal with their stiff hand?
Are they slower to get dressed because their hand is not as flexible and it’s difficult to button?
Does the patient have difficulty donning their bra because of this stiffness?
Probing with these types of questions will lead you down a road where it is easier to
create meaningful functional goals.
Good functional goals for such a patient may read as:Patient will reduce dressing time in AM by 10 minutes.
Patient will resume donning bra behind back (patient is compensating with front closure).
Patient will utilize injured hand to brush teeth for 90 seconds.
Patient will independently demonstrate contrast bath to decrease morning stiffness.
1)
2)
3)
4)
5)
1)
2)
3)
4)

Treatment2Go
��
Index
handtherapy.com
Regardless of your clinical setting, your goals for your patients must focus on specific complaints; therefore, addressing the patient’s primary concerns, but goals must tie into function. You may work on minimizing her stiffness through range of motion exercises and this can be one component of treatment as long as you show measurable progress. An example: the patient’s reduction of time for morning ADLs or the “getting ready” time in the AM. Additional ideas for documenting functional goals in daily notes will be addressed in the next chapter.
Meaningful Goals
It is important to have goals that are meaningful to the patient. Therapists should not be writing goals that are focused on what the therapist wants. A patient state he/she wants to improve dynamic balance to be able to return to ballroom dancing s/p stroke. However, this patient still has limitations in dressing which are limited by balance (requires assist to reach down and pull up pants without falling). Knowing that ballroom dancing is not a reimbursable goal per Medicare, the therapist establishes an ADL goal based on deficits noted during evaluation. However, when the therapist wants to address dressing in treatment (even explaining that it will ultimately help with balance for dance) the patient is uninterested and unwilling to participate. The therapist must plan goals with the patient. Functional goals that are not meaningful are not useful and can become frustrating for the patient and therapists. Well planned out treatment plan with the patient is critical for success.
TIP: Some standardized evaluations such as the Canadian Occupational Performance (CMOPS) will help address this situation.

Treatment2Go
��
Index
handtherapy.com
Creating both short term and long term goals is required by most insurers. Your short term goals should be a stepping stone toward reaching your long term goals. As was discussed in the previous chapter, you should be telling a story. The short term goal should get you to the middle of the story and the long term goal should get you to the end of the story (discharge).
Poor Short Term/Long Term goals:STG: Patient will increase grip by 20%
LTG: Patient will have sufficient grip to return to work.
These are poor goals for several reasons. The STG is measurable but not functional. The long term goal does not identify a numeric range of grip strength that is required for patient’s job duties.
Improved Short Term/Long Term goals:STG: Patient will increase grip by 20% to lift files from shelf to desk
LTG: Patient will have 50-75 lbs of grip to carry boxes of files 50 feet to the mail-room.
These goals are measurable, functional, meaningful and have a clear trajectory that one goal is preparation for the next goal. This patient will begin with moving a lighter object a short distance. As hsi grip strength improves, he will be able to grip a heavier load for a longer distance.
Having solid short term and long term goals should also help direct the therapist in providing relevant, focused treatment. Knowing that you need
to address grip strength can lead to the development of a treatment plan utilizing therapeutic exercise and activity that can be incorporated into function. Your documentation then becomes more meaningful in telling the therapy story.
►
►
►
►
Treatment2Go
��
Index
handtherapy.com
CHAPTER 6 INCORPORATING FUNCTION
Day to day treatment should reflect a focus that returns the patient to a higher level of function. Treatment notes that focus only on progressing an exercise program leave room for denials. These treatments risk being seen as a “gym” program or lacking the need for skilled care after several sessions. Keeping notes oriented toward functional goals is essential in meeting the regulations of insurers. We discussed Functional G codes and modifiers in Chapter 3.
A therapist may utilize certain exercises in order to facilitate changes in function over the longer term. This goal of a change in function is best addressed regularly in daily notes. For example, if the goal is to increase grip strength for lifting files, the therapist may be using progressive resistive exercises such as a hand helper device during the treatment session. However, following this it might be beneficial to have the patient practice lifting a book that weighs 3 lbs from their lap to the desk. The note for this part of the session may read: “hand helper 3 sets of 10 at 2 lbs, 3 sets of 10 at 4 lbs, functional lifting 3 lb book from lap to tabletop x 10 reps”. Use of a particular intervention technique such as Neuro Developmental Theory (NDT) to show the therapists skilled intervention, but if it is not linked to function it does not provide meaning for the reviewer. A note that reads “weight-bearing on affected side while seated x10 min” is improved when written as follows “weight-bearing on affected side x10 min to reduce tone. Reaching across body for clothing management while weight-bearing x3 with min assist.”

Treatment2Go
��
Index
handtherapy.com
There are key phrases you can use that can convey the functional purpose of your treatment. For example, instead of writing “reaching for cones while standing to improve dynamic balance” one might write “reaching out of base of support for clothing management while toileting.”
Some examples of functional phrasing:Small object manipulation (i.e coins, etc)
Functional lifting for household tasks
Overhead reaching to don shirt
Overhead reaching to wash hair
Increase ulnar deviation to open jars
Recall exercises for medication management
Clothing management when toileting
Increase elbow flexion to __ degrees to don/doff eyeglasses
Endurance training to cross street without needing rest
Internal rotation exercises in preparation to don bra
Pinch strength training to use nail clippers
Pinch strength training to turn ignition
Tracing with fat pen to increase legibility for signature
Thinking about outfitting your clinic with tools that are functional will help create therapy sessions that are functional. Good inexpensive tools to have in the clinic may include: nuts and bolts, clothespins, safety pins, coins, laundry baskets, plates, jars, containers, and medicine bottles of various sizes.
►
►
►
►
►
►
►
►
►
►
►
►
►
Complete the worksheet titled: “Functional, Yes or No?”
Return to course after completing worksheet

Treatment2Go
��
Index
handtherapy.com
Think about items you may have in the clinic that you can use for functional treatments including:
Staplers (require strength to use)
Paper (for folding and tearing)
Books (can patient turn pages, lift, etc)
Computer (for typing, mouse use)
Floors (can patient get themselves on and off the floor in case of a fall)
Phone and phone book (can patient call for assistance if needed)
Building directory (can patient find own way to appointments or new offices)
Think of three additional things in your office that could be incorporated into a functionally focused treatment session.
►
►
►
►
►
►
►
Veiw examples of components of skilled srvices.... Then return to course

Treatment2Go
��
Index
handtherapy.com
CHAPTER 7EVIDENCE BASED PRACTICE
WHY SHOULD I CARE?
The terminology “evidence based medicine” is increasingly used in the media and by insurance agencies. What does this term mean? The most frequently quoted definition is by Dr. Sackett – “Evidence Based Medicine is “the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of the individual patient. It means integrating individual clinical expertise with the best available external clinical evidence from systematic research.” (Sackett D, 1996). This means that we should be using the best available scientific information to guide our clinical decision making. If your clinical reasoning is based on your last best or worst outcome, you are relying on anecdotal evidence, not science.
Many insurers are moving to a model where they will only pay for certain procedures/treatments if there is evidence showing that your treatment is proven to be effective. If you are documenting for success, it is most important to know what treatments are considered reimbursable. Many insurers follow the lead of Medicare in deciding what they will reimburse. However, each insurer may vary. Therefore, it is important
Treatment2Go
�0
Index
handtherapy.com
to review the guidelines for your payers, especially regarding controversial treatments such as iontophoresis, cranio-sacral therapy, phonophoresis, low level laser therapy, and constraint induced movement therapy. Additionally, new technologies often have questionable reimbursement until enough research has been established to prove efficacy.
This increasing focus on evidence based practice will likely cause practitioners to stay abreast of the latest scientific research in their field. Reviewing journals or searching databases is an essential clinical skill. Occasionally, an insurance company may ask for further evidence on a treatment in order to decide if they will pay. How to search databases and find evidence is not covered in this course. However, professional associations such as AOTA & APTA have resources to assist members with evidence based practice. For example, AOTA members can access evidence briefs on a variety of diagnoses, read quick summaries in AOTA’s professional publications, and access databases through their website. Many continuing education providers also offer seminars in how to practice with an evidence based approach. Skills in these areas will help practitioners provide and document in a manner that will meet the regulations of insurers. Two popular databases to use for accessing scientific articles include www.pubmed.com and www.cochrane.org.

Treatment2Go
�1
Index
handtherapy.com
The following excerpts on the following pages were linked during the course and are the worksheets and assignments to complete the course.
Find two articles online that would support the rationale for a treatment you use regularly. For ex-ample, if you regularly treat arthritis patients, find two articles that support the need for splints with arthritis patients. Use the above websites.
WEBSITE NAVIGATION INSTRUCTIONS:
When you search for your articles, make certain to put in very narrow search terms. For example, on pubmed, search iontophoresis brings up several THOUSAND articles. However, when the search is narrowed to iontophoresis lateral epicondylitis, the results are narrowed to 10 choices. When using pubmed, also use the pulldown menu to display abstracts to allow you to see summaries of the arti-cles of interest. Use a critical eye and look for articles with larger sample sizes and longer follow up periods. Double blind randomized controlled studies are considered the gold standard.
CONCLUSIONA well documented chart increases the likelihood of successful reimbursement. Despite variances in the ways therapists document, all charts should tell a concise but meaningful story of the patient’s therapy journey. Utilizing the tools you learned in this course, your stories can be thorough without being overly burdensome. Staying abreast of the latest updates in Medicare, insurance regulations and evidence to help you document for success!

Treatment2Go
�2
Index
handtherapy.com
Return to course page 11
click here
SOAP NOTE Worksheet
Write a SOAP note for each of the following situations:
1) Patient is a �2 y.o female recovering from a total hip replacement. Her home health aide comes everyday to do lower body dressing. She currently requires mod assist. This is your second session with her and you begin to address standing balance to help with lower body dressing. You also review the use of adaptive devices.
2) Patient is a �2 year old office worker with bilateral forearm overuse injury. He has been attending therapy 2x/week for � months. He reports he is 20% improved since the beginning of therapy. His session includes postural retraining exercises, wrist curls, ultrasound, soft tissue massage, and forearm stretching.
�) Patient is a �0 y.o. male who is recovering from cervical spinal fusion. He also has ALS. He was independent before surgery but now reports decreased coordination in both hands (R>L) and significant sensory loss in both hands (L>R). He cancels therapy frequently but requests to attend therapy 2x/week times for at least two months. His goals include improved writing, feeding with right hand and lifting with both hands.
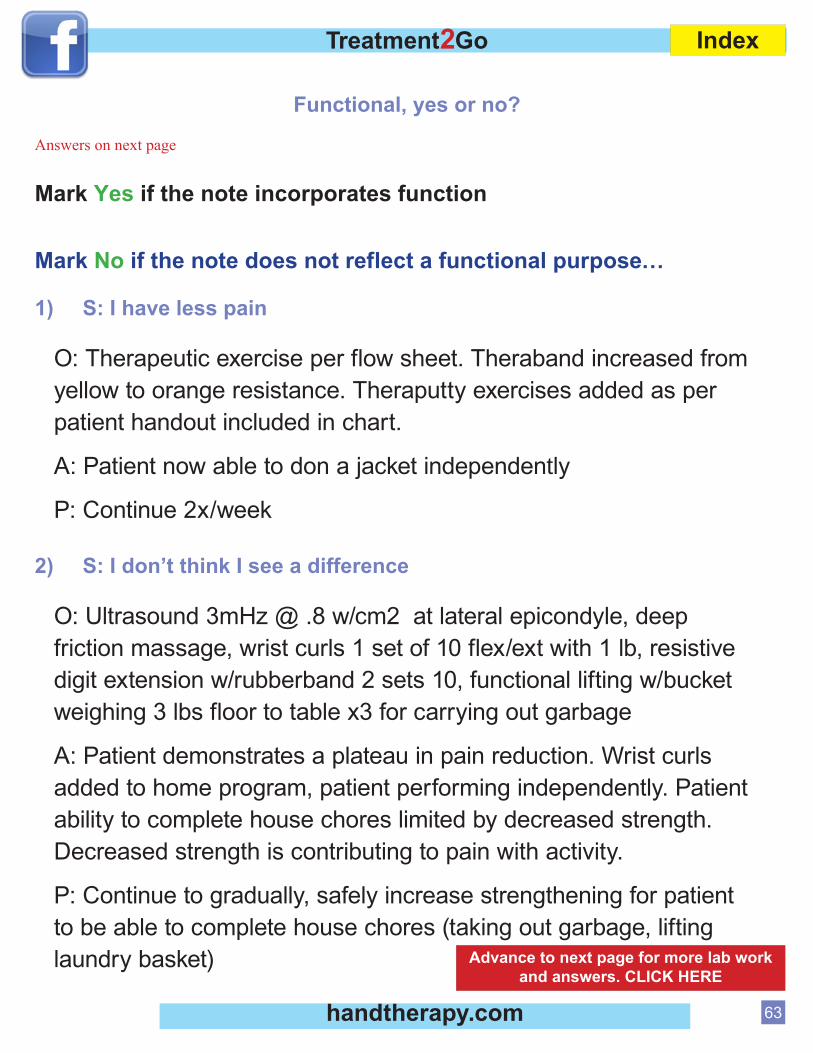
Treatment2Go
��
Index
handtherapy.com
Functional, yes or no?
Answers on next page
Mark Yes if the note incorporates function
Mark No if the note does not reflect a functional purpose…
1) S: I have less pain
O: Therapeutic exercise per flow sheet. Theraband increased from yellow to orange resistance. Theraputty exercises added as per patient handout included in chart.
A: Patient now able to don a jacket independently
P: Continue 2x/week
2) S: I don’t think I see a difference
O: Ultrasound �mHz @ .� w/cm2 at lateral epicondyle, deep friction massage, wrist curls 1 set of 10 flex/ext with 1 lb, resistive digit extension w/rubberband 2 sets 10, functional lifting w/bucket weighing � lbs floor to table x� for carrying out garbage
A: Patient demonstrates a plateau in pain reduction. Wrist curls added to home program, patient performing independently. Patient ability to complete house chores limited by decreased strength. Decreased strength is contributing to pain with activity.
P: Continue to gradually, safely increase strengthening for patient to be able to complete house chores (taking out garbage, lifting laundry basket) Advance to next page for more lab work
and answers. CLICK HERE

Treatment2Go
��
Index
handtherapy.com
3) S: I fell while transferring to my wheelchair
O: Mat to chair transfer with contact guard assist x �, Mat to chair transfer w/supervision x 1. Education and hands-on demonstration to caregiver to provide CGA. Review safety precautions with patient on transferring with assist.
A: Caregiver independent to provide contact guard assist. Patient remains unsafe without caregiver as he is unable (without verbal cues) to state � situations when he is a fall risk.
P: Try sliding board next visit to increase patient safety during transfer.
ANSWERS Although the assessment addresses an ADL, the treatment does not show how the function and ADLs are being addressed. The therapist could have added “Decreased upper extremity strength limits ability to don shirt overhead” Additionally the treatment session would have increased relevance if upper extremity dressing had been practiced.
Great focus! This note is very focused on modalities and therapeutic exercise. The therapist ties these treatments to the functional activity of lifting in the objective section. In the assessment the therapist does a nice job of elaborating why these exercises are being used. In the plan, the therapist gives the reviewer a preview of the remainder of the “therapy story”
Good functional treatment session with a goal of patient safety. Includes information on future plans to increase patient safety and why patient continues to need treatment.
1)
2)
3)
Return to course page 57click here

Treatment2Go
��
Index
handtherapy.com
Documenting Functionally
Rewrite the Following Goals to be functional:
Suggested Answers on next page:
1) Patient will have 0-�/10 pain
2) Patient will independently lift 20 lbs.
�) Patient will finish the � hole peg test in �0 seconds
�) Patient will increase supination to �0 degrees
�) Patient will improve pinch strength to 12 lbs
�) Patient will tolerate 1� minutes on treadmill
�) Patient will increase writing legibility
�) Patient will remember �/� words after 10 minutes
�) Patient will be able to follow � step commands independently
10) Patient will attend to left side without verbal cues
Click here to advance to next page for answers

Treatment2Go
��
Index
handtherapy.com
Suggested answers:
1) Patient will have 0-�/10 pain when dressing and will not need to stop for breaks.
2) Patient will independently lift 20lbs in order to lift child
�) Patient will increase fine motor coordination to lift � coins without dropping any coins
�) Patient will increase supination in order to open a door independently with affected arm
�) Patient will improve pinch strength to pull plates off kitchen shelf
�) Patient will increase endurance to walk from car to grocery store without a rest.
�) Patient will increase writing legibility for signing checks
�) Patient will remember �/� words after 10 minutes in order to remember a street address
�) Patient will follow three step commands independently in order to make tea
10) Patient will attend to left side without verbal cues in order to walk through kitchen without tripping on a chair.
Return to course page 52
click here

Treatment2Go
��
Index
handtherapy.com
Avoid phrases like:
Continued routines practice
Drill work continued
Slow progress
Observed/monitored behavior
Reviewed previously learned material
Little progress noted
Patient agitated, confused
Unable to learn
Disoriented to time and place
Poor attention span
General practice techniques continued
No problems noted
Carried out maintenance program
Little hope of progress
►
►
►
►
►
►
►
►
►
►
►
►
►
►
Use phrases specific to medicare guidelines:
Redirected patient’s behavior
Assessed mobility skills
Designed and implemented maintenance programs
Instructed in use of compensators for feeding/swallowing techniques
Adapted procedures for patient’s condition
Individualized training programs to maximize performance
Complexity of condition required modification of program
Customized treatment approach to match condition of patient
Safety issues addressed with positive results
Techniques to teach new skills added to program
Analyzed behaviors and provided feedback as necessary
Conditions continues to require skilled services
Deficits continued to compromise safety
►
►
►
►
►
►
►
►
►
►
►
►
►
Terminology Dos and Don’ts
Return to course page 27
Click here

Treatment2Go
��
Index
handtherapy.com
Skilled Action VerbsWhen documenting “skilled intervention” provided on daily/weekly notes, include skilled action (verb). Examples below:
PT instructed safe sequencing for sit to stand transfer; patient returned demonstration with 50% accuracy
OT designed compensatory tools to aid in sequencing of dressing tasks
ST facilitated production of multi-syllablic words in isolation with focus on accuracy
►
►
►
Administered
Advised
Analyzed
Augmented
Concentrated
Conducted
Consulted
Coordinated
Corrected
Delivered
Developed
Designed
Devised
Educated
Engineered
Enhanced
Established
Evaluated
Facilitated
Focused
Fostered
Guided
Implemented
Incorporated
Increased
Induced
Initiated
Installed
Instructed
Interviewed
Intensified
Introduced
Lowered
Maximized
Minimized
Mobilized
Modified
Performed
Positioned
Prepared
Promoted
Re-engineered
Recommended
Resolved
Restored
Restructured
Revised
Secured
Solved
Started
Stimulated
Structured
Supervised
Synchronized
Targeted
Trained
Upgrades
Return to courseclick here page 27

Treatment2Go
��
Index
handtherapy.com
Components of Skilled servicesDiagnostic & assessment services
BERG balance Scale
Tinetti Balance Scale
Boston Diagnostic Assessment
Ross Information Processing Assessment
The Canadian Occupational Performance (CMOPS)
Designing treatment programs
Dysphagia protocol
Gait training program
Balance training program for ADLs
Dressing/bathing program
Training compensatory Skills designed to improve function
Associative language activities
Chin tuck, cyclic ingestion, supraglottic swallow technique
Visual scanning strategies
Gait pattern techniques
One handed dressing techniques
Adaptive equipment strategies/compensatory strategies
Analyzing and Modifying behaviors to improve function
Modified dysphagia protocol to include chin tuck technique
Analyzed upper body dressing & modified adaptive equipment to include long handled sponge
Analyzed assistive walking device & recommended rolling walker
►
►
►
►
►
►
►
►
►
►
►
►
►
►
►
►
►
►
Go to next pageclick here

Treatment2Go
�0
Index
handtherapy.com
Providing Instruction to patient/caregiver to augment restorative treatment or to establish a maintenance program
Instructed patient to double swallow with each bite of solid food
Instructed patient in the proper hand placement for rolling walker
Instructed patient in the use of sock aid and long handled shoe shorn
Instructed patient in shower transfer techniques to a shower bench
Instructed and demonstrated patient in bathroom safety to include maneuvering walker in space, flushing toilet
stowing shower accessormangin
►
►
►
►
►
►
Return to courseclick here page 58

To Deny or Not to Deny –That Is the QuestionThat Is the Question
R E V I E W T H E F O L L O W I N G S L I D E S A N D D E C I D E I F T H E N O T E W O U L D J U S T I F Y
C O N T I N U E D C A R E C O N T I N U E D C A R E . W H E N Y O U H A V E M A D E Y O U R D E C I S I O N ,
C L I C K T O T H E N E X T S L I D E A N D S E E I F Y O U W E R E C O R R E C T !W E R E C O R R E C T !

Case #1 – CVA patient, 2nd month of care, / k Li / h iseen 3x/week. Lives w/ 24 hour caregiver
S: I still need help to get dressedO: Lower body dressing with min verbal cues to start with O: Lower body dressing with min verbal cues to start with hemiplegic leg. Patient able to successfully complete one independent trial (no v.c.’s) after 5 trials. Upper body dressing independent. Weightbearing on left while reaching for clothes.PNF patterns (therapist assisted)
t d 10 hseated x10 each.A: Patient has improved from mod verbal cues to min verbal cues for lower body dressing verbal cues for lower body dressing. P: Progress patient to independent lower body dressing in 1 week Continue facilitation techniques to decrease in 1 week. Continue facilitation techniques to decrease tone in left UE for household tasks.

Case #1 - CVA
G d Nt !Good Note!Shows progress from mod assist to min assist for lower body dressing with reasonable timeframe to attain independencedressing with reasonable timeframe to attain independenceSkilled care continues to be needed for neuro-facilitationtechniquesq
BUT – THIS NOTE IS MISSING ONE CRUCIAL ELEMENT….what is it?

Case #1 - CVA
Thi i i i ti f ti d d d This is missing an accounting of timed codes and total treatment time….
T t l ti d d i 6 i ( l ti d d d)Total timed codes is 60 min (only timed codes were used)Total treatment time is 60 minCodes billed were ADL/self care x2 Therapeutic Exercise x2Codes billed were ADL/self-care x2, Therapeutic Exercise x2

Case 2 – Cardiopulmonary Deconditioning, 2nd
th f / kmonth of care, 2x/week
S I h b i d k h f dS: I have been too tired to take a shower for 3 days.O: Upper body ergometer x 15 min, therabandexercises 10 each orange resistance: shoulder flex exercises 10 each, orange resistance: shoulder flex, shoulder ER, shoulder abduction, elbow flex/ext, and wrist flex/ext. Bucket lifts (to simulate grocery bags) / g y gwith 5 lbs for 10 repsA: Patient progressing well, tolerates 45 min sessionP: Continue to increase tolerance to a 60 min sessionTotal timed codes: 60 min-Total treatment time: 60
i min Codes Billed: Therapeutic exercise x3, Therapeutic activity (bucket lifts) x1 activity (bucket lifts) x1

Case #2 - Cardiopulmonaryp y
DENIED NOTEDENIED NOTEReasons for denial
If these exercises are similar session to session, there is an If these exercises are similar session to session, there is an expectation that this program could be completed independently by the patient in a community based exercise program such as a gym or YMCAprogram such as a gym or YMCA.Although the practicioner tried to put a functional element in the treatment session with the bucket lift this is not enough to
f h h l ld h b b f hjustify the session. This element would have been better if the quality of the activity was noted, such as floor to table height and then increased from floor to counter height.

Case #3 – Carpal Tunnel Syndrome, one visit only for wrist cock-up splintso y o st coc up sp ts
HPI: Patient has been having tingling and numbness in right 1st, 2nd, 3rd fingers x 2 months. Must stop work and g 3 g pshake out hands to resume sensation. No functional limitations. No previous therapy intervention for this diagnosisTreatment today: Splint fabrication for right wrist cock-up. A/P: Patient is independent in wear/care of splint. Patient will be seen for one additional visit as needed for splint will be seen for one additional visit as needed for splint adjustment. Otherwise, patient to follow-up with MD.Total treatment time: 60 min, Total Timed Codes: 0 minC d Bill d E l ti LC d f li ti ( ith Codes Billed: Evaluation, L-Code for splinting (neither are timed codes)
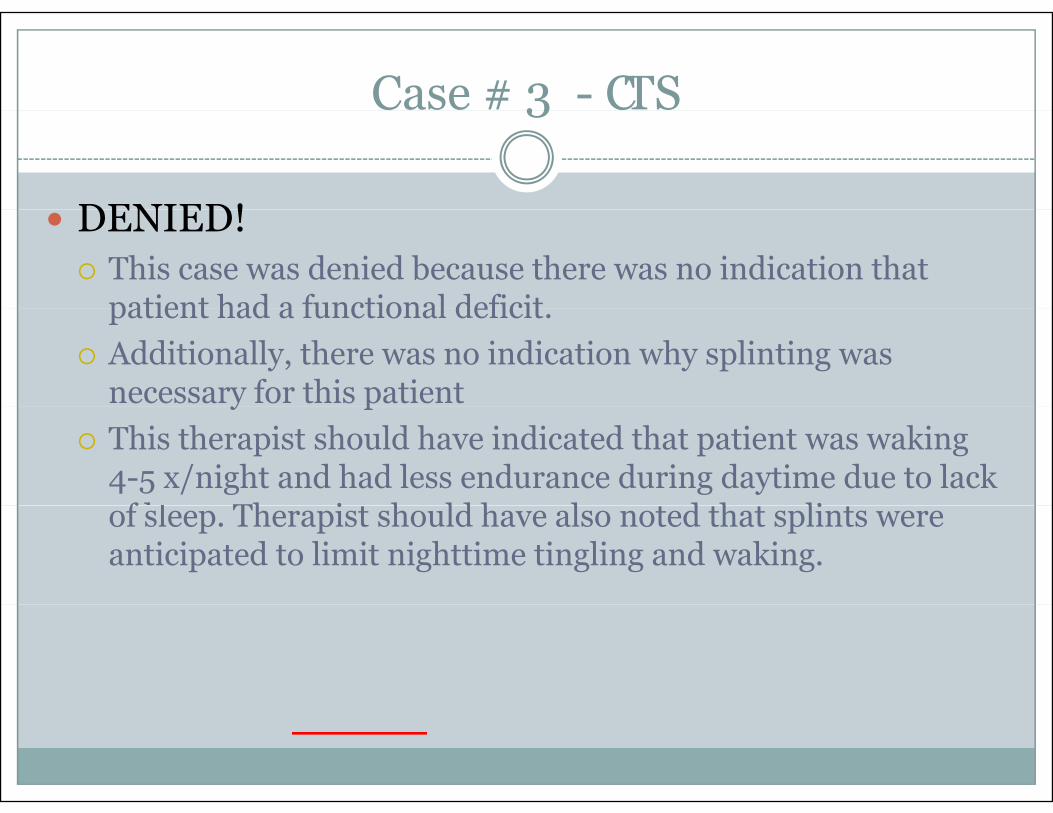
Case # 3 - CTS3
DENIED!DENIED!This case was denied because there was no indication that patient had a functional deficitpatient had a functional deficit.Additionally, there was no indication why splinting was necessary for this patienty pThis therapist should have indicated that patient was waking 4-5 x/night and had less endurance during daytime due to lack
f l Th i h ld h l d h li of sleep. Therapist should have also noted that splints were anticipated to limit nighttime tingling and waking.