documentation “in today’s highly litigious society a nurse must keep basic principles in mind in...
TRANSCRIPT

DOCUMENTATION
““In today’s highly litigious society a nurse must keep In today’s highly litigious society a nurse must keep basic principles in mind in order to prevent litigation for basic principles in mind in order to prevent litigation for both the institution he or she works at and for the nurse both the institution he or she works at and for the nurse him/herself”.him/herself”.
-Flores, J. A.(2006). Proper charting for nurses and other health care professionals.

What people, disciplines or organizations can access and read
your notes?
Documentation has always been a part of the nurses role.

• 417 septicemia age 0-17 418 postoperative & post-traumatic infections
• 419 fever of unknown origin age >17 with complications, comorbidities
• 475 respiratory system diagnosis with ventilator support • 476 prostatic operating room procedure unrelated to principal
diagnosis • 477 non-extensive operating room procedure unrelated to
principal diagnosis • 514 cardiac defibrillator implant with cardiac catheterization (added
10-1-01) • 515 cardiac defibrillator implant without cardiac catheterization
(added 10-1-01) • 267 perianal & pilonidal procedures • 268 skin, subcutaneous tissue & breast plastic procedures • 352 other male reproductive system diagnoses • 353 pelvic evisceration, radical hysterectomy & radical vulvectomy • 118 cardiac pacemaker device replacement • 119 vein ligation & stripping

It is also a New Zealand Nursing Council requirement.
Let’s look at Domain 2
Domain Two: Management of Nursing Care
Competency 2.3 Ensures documentation is accurate and maintains confidentiality of information.
• Indicator: Maintains clear, concise, timely, accurate and current client records within a legal and ethical framework.
• Indicator: Demonstrates literacy and computer skills necessary to record, enter, store, retrieve and organise data essential for care delivery.
The College of Registered Nurses of British Columbia states:
“Clear, comprehensive and accurate documentation is a record of the judgment and critical thinking used in professional practice…(and can be) any written or electronically generated information about a client that describes the care or service provided to that client…”
-CRNBC (2003). Nursing documentation, p. 4.

CRNBC defines documentation.
“Documentation is any written or electronically generated information about a client that describes the care or service provided to that client. Health records may be paper documents or electronic documents, such as electronic medical records faxes, e-mails, audio or video tapes and images.
Through documentation, nurses communicate their observations, decisions, actions and outcomes of these actions for clients. Documentation is an accurate account of what occurred and when it occurred”
-CRNBC (2003). Nursing documentation, p. 2.


Purposes of Records
1. Communication2. Financial reimbursement3. Education4. Assessment5. Research6. Auditing7. Legal documentation8. Promote good nursing care9. To meet professional, legal & institutional
standards

What types of charting are there?
• Focus charting
• SOAP/SOAPIER/SOATAP/OPD charting
• Narrative charting
• Charting by exception
• Systems charting
• Telenursing

Let’s look at an example of POOR documentation
From an actual patient’s record:
18/12/99 0630 NSG
Obs stable, IVA given as charted. Slight SOB overnight. Taken inhaler, sats 95-96% on air. Nil other complaints.
Signature
Are there any gaps in this entry?
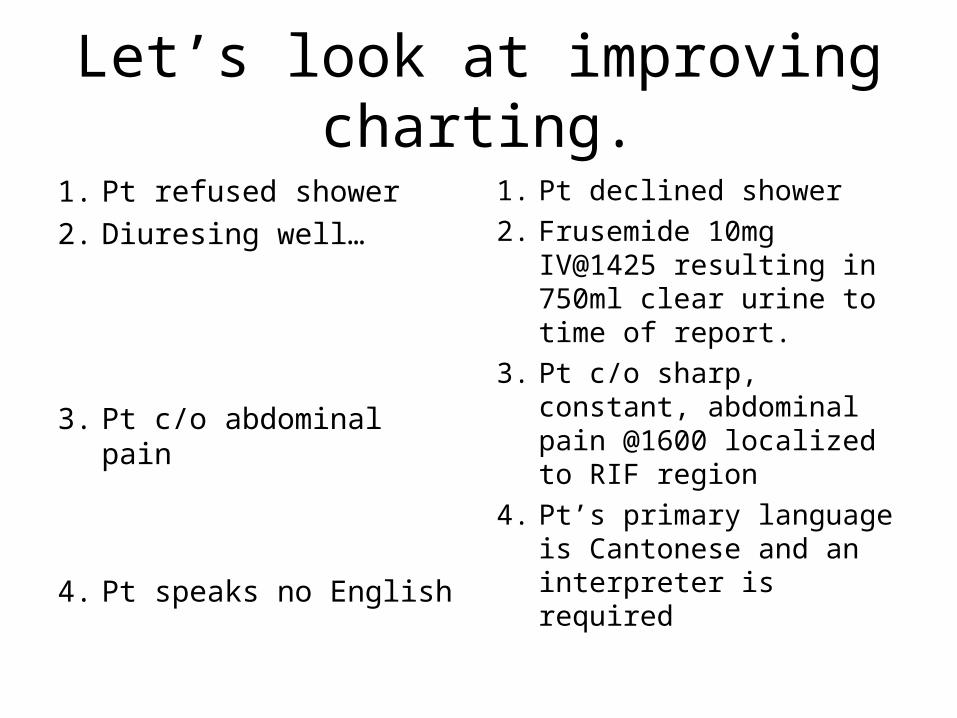
Let’s look at improving charting.
1. Pt refused shower
2. Diuresing well…
3. Pt c/o abdominal pain
4. Pt speaks no English
1. Pt declined shower
2. Frusemide 10mg IV@1425 resulting in 750ml clear urine to time of report.
3. Pt c/o sharp, constant, abdominal pain @1600 localized to RIF region
4. Pt’s primary language is Cantonese and an interpreter is required

Now you try.
• Walks with a limp
• Pt comfortable, good duty
• Eating and drinking well

Guidelines for Nursing Documentation
1. Write legibly in ink2. Sign all entries3. Document on agency forms4. Correct errors5. Document in chronological order with the correct time
and date for each entry6. Document concurrently or as close as possible to the
time care was given OR the event time7. Write concisely and factually8. Avoid bias9. Use appropriate abbreviations10. Document only from first-hand knowledge11. Care provided by auxiliary staff is document by
auxiliary staff12. Safeguard the confidentiality of documentation

Do’s of Documentation• Check that you have the correct chart before you begin writing.• Make sure your documentation reflects the nursing process and
your professional capabilities.• Write legibly.• Chart the time you gave a prn medication, the administration route,
and the patient’s response.• Chart precautions or preventative measures used, such as bed rails.• Record each phone call to a physician, including the exact time,
message, and response.• Chart patient care at the time you provide it.• If you remember an important point after you’ve completed your
documentation, chart the information with a notation that it’s a “late entry” Include the date and time of the late entry.
• Document enough to tell the whole entire story.

Don'ts of Nursing Documentation
• Don’t chart a symptom, such as “c/o pain” or “c/o SOB” without also charting what you did about it.
• Don’t alter a patient’s record – this is a criminal offense.• Don’t use shorthand or abbreviations that aren’t widely
accepted or accepted by the institution.• Don’t write imprecise descriptions, such as “bed soaked”
or “a large amount”, these are unclear.• Don’t chart what someone else said, heard, felt, or
smelled unless the information is critical. In that case, use quotations and attribute the remarks appropriately.
• Don’t chart care ahead of time – something may happen and you may be unable to actually give the care you’ve charted. Charting care that you have not done is considered fraud.

An example of good charting:Sample charting entry:13/08/0607:30 Received in bed resting quietly. Woken for breakfast, assisted to high fowlers position. Cloth given for hands and face. Stated that he did not sleep very well due to pain in right hip. States pain a 6/10. Describes pain as a constant burning but did not want to disturb the nurses for analgesia as he felt they were too busy. Encouraged to use call-bell to ring for nurse and inform them when having pain. Preceptor nurse notified at this time & given analgesia by same. Will r/v patient in one hour.-------------------------------- B. Rommer, Nsg Student (2) Unitec.--------------------------------------------------------------------------------------------08:30 States is feeling much more comfortable @ present. Pain now down to 3/10 & describes it as, “less intense” than earlier. Resting in bed in semi-fowler’s reading book. Reminded to call nurse if pain begins to increase. Call-bell in reach. Declined shower when offered, states, “will take his time today”. -------B. Rommer, Nsg Student (2) Unitec.---------------------------------------------------------------------------------------------14:00 CVS: T: 36.8 (oral), Radial pulse btwn 76-88 bpm through shift, strong and regular bilaterally and S1 S2 audible, BP @ 13:30 164/74 (L). Skin pink and warm to touch. Cap refill < 3 secs to upper extremities. I/V n/s infusing at 100ml/hr via IVAC into (R) arm with 600ml TBA. Site healthy, no redness or swelling noted. States site feels, “o.k.”. Slight non-pitting edema noted to lower limbs. Legs elevated on stool and instructed to elevate legs as much as possible to ↓ swelling. --------------------------------------- RESP: RR 24/min, deep and regular, no SOB/cyanosis noted. Lungs auscultated, ↓ A/E to RLL, but good A/E to other lobes. Encouraged to deep breath q 1-2 hours to encourage air entry to lower lobes in order to prevent complications. Used 02 once this shift at 2L/min via NP after walking with PT. States felt, “winded” and “needed some extra air” and felt improved after 02. No cough or sputum production noted.
GI: Ate 100% of brkfst tray and 50% of lunch tray. States he ate too much at brkfst and had little appetite for lunch. Denies nausea/abdominal pain. Had one large brown soft BM today, passing flatus. Active bowel sounds heard in all 4 quadrants. Has taken approx. 750ml fluid thus far this shift. MM pink and moist, skin turgor to upper chest elastic.---------------------------------------------------------------------------------------
GU: Using urinal to void as states, “sometimes it is hard to get to the toilet fast enough to pass water”. Urine clear, light amber in colour, non-offensive. Voiding btwn. 250-300ml in each void. Denies dysuria or other adverse urinary symptoms. --------------------------------------------------------------------------------------------
NEURO/MS: Up ambulating around ward per self without assistance. Gait equal and steady. Denies vertigo/syncope. Battery to (L) hearing aid dead, daughter notified @ 0900 today to bring in additional battery. Pt able to hear when spoken to quite closely.-----------------------------------------------------------------
SKIN: Intact, pink and warm. Small 2cm bruise noted to anterior of (R) leg, states hit his leg against beside chair two days ago.--------------------------------------------------------------------------------------------------------
GEN: For repeat Hgb & ECG in a.m. Family in to visit for 3 hours today. To see OT later this week. ----- B. Rommer, Nsg Student (2) Unitec-------------------------------------------------------------------------------------------