doctorate in clinical psychology - home | university of hertfordshire · pdf...
TRANSCRIPT

Doctorate in Clinical Psychology
Supervisor Handbook
November 2011 revision

2
Contents
1. Introduction 4
1.1 Background
1.2 Course Philosophy
1.3 Committee Structure
1.4 Staff
2. Clinical Placements 7
2.1 Overview of the placement rotations
2.2 How placements are allocated
2.3 Honorary contracts
2.4 Physical requirements
2.5 Supervision
2.6 UH supervisor training
2.7 Pre-placement visits
2.8 Placement contracts
2.9 Induction and orientation
2.10 Transition to independent work
2.11 Work Load
2.12 Integrating Theory and Practice
2.13 The development of professionalism
3. Competencies and Experience 12
3.1 Essential Experience 3.2 Core Competencies
4. Placement Monitoring 18
4.1 Clinical tutorials
4.2 Mid-placement reviews
4.3 End of placement reviews
4.4 Placement difficulties
4.5 Placement Feedback & Placement Audit
5. Clinical Evaluation 21
5.1 Assessment of Clinical Competence: Summary of requirements
5.2 Log of Clinical Experience
5.3 The Supervisor Evaluation of Clinical Competence form
5.4 Examples of Clinical Work
5.5. Submission of Placement Documents
5.6 Placement Marking
5.7 Placement Outcomes
5.8 Procedure for placement failure
Appendices 27

3
Appendices Appendix 1: BPS Committee on Training in Clinical Psychology
Guidelines on Clinical Supervision 28
Appendix 2: Protocol for Managing Clinical Psychology Trainees 33 Appendix 3: Professional Practise Guidelines on Teaching Training and Supervision 36 Appendix 4: Placement Contract 38 Appendix 5: Criteria for the Accreditation of Postgraduate Training Programmes in
Clinical Psychology 46 Appendix 6: Clinical Tutorial form 56 Appendix 7: Placement Review form 57
Appendix 8: Log of Clinical Experience 66 Appendix 9: Summary Log of Clinical Experience 75 Appendix 10: Supervisor Evaluation of Clinical Competence form 80 Appendix 11: Trainee Placement Feedback & Placement Audit forms 92 Appendix 12: Policy on Managing Difficulties on Placement 101 Appendix 13: Placement Marking Guidelines 103 Appendix 14: Trainee Guidelines: Examples of Clinical work 113 Appendix 15: Guidelines on Consent 129 Appendix 16: Trainee Guidelines: Clinical Case Reports 135

4
1. Introduction 1.1 Background
The DClinPsy programme is based in the School of Psychology, which is located within the Faculty of
Health and Human Sciences of the University. The School has an excellent reputation for both its
teaching and research achievements.
The School of Psychology has been closely involved in health research developments in the Faculty,
including the successful establishment of the Centre for Research in Primary and Community Care,
the Health Research and Development Support Unit, and a primary care research network. The new
Health Research Building, associated with a postgraduate medical school, opened in 2006, and is the
base for the DClinPsy programme.
The UH DClinPsy programme commenced with its first cohort of trainees in April 2001, having been
accredited by the British Psychological Society Committee on Training in Clinical Psychology. The
programme was re-accredited in 2003 for a further five year period and again in 2008. In 2005, it was
considered as part of the major review by the Quality Assurance Agency of healthcare programmes at
the University, and the reviewers indicated confidence in the academic and practitioner standards
achieved by the programme. The programme is funded by the Essex Workforce Development
Confederation and the Bedfordshire and Hertfordshire Workforce Development Directorate.
The Doctorate in Clinical Psychology has been designed to:
satisfy the criteria stipulated by the British Psychological Society and Health Professions
Council for training in clinical psychology and have quality assurance procedures to ensure
those criteria continue to be satisfied
build on the close partnerships with NHS Trusts in the region so that research, academic and
professional links are extended and strengthened
collaborate with existing providers of clinical training by developing additional placement
opportunities for trainees
be based in a School with an excellent reputation for high standards in academic quality and
research activity, as well as benefiting from expertise in developing and managing clinical
placements for health professionals
be based on a prestigious site in Hertfordshire, easily accessible by road and rail, with
excellent bus links to NHS hospitals and health centres
meet the training needs of Hertfordshire, Essex, and Bedfordshire. 1.2 The Course Philosophy Programme Purpose
The Doctorate in Clinical Psychology at the University of Hertfordshire has been set up to prepare
trainees to function effectively as clinical psychologists within the National Health Service (NHS) and
in related settings. The Programme has a particular remit to train clinical psychologists to take up NHS
posts in Hertfordshire, Essex and Bedfordshire. It will train psychologists to use their expertise in a
way that respects and protects the well being of others, their clients, pupils and other staff and enables
them to gain Chartered Clinical Psychologist status from the British Psychological Society and to
register as Clinical Psychologists with the Health Professions Council.
Programme Objectives
The objectives of the Doctorate in Clinical Psychology Programme are to provide trainees with:

5
knowledge and understanding of a range of psychological models relevant to clinical psychology
competency in the appropriate application of a number of psychological models in clinical
situations
the clinical skills and experience necessary to use psychological models across a range of
problems and client groups
a sound knowledge and understanding of the organisational, professional, practice, ethical, and
legal frameworks of the Health Professions Council, the British Psychological Society and the
NHS
the skills needed to be a self-reflective, reflective and critical practitioner
the skills needed for self-directed learning
Aims of the Programme
The Programme aims to develop trainees who, at the end of their programme of study, have achieved
a high level of competence and professionalism that will enable them to apply a broad range of
psychological theories and concepts to both clinical practice and clinical research.
It also aims to:
establish and maintain productive, professional, working relationships with local clinical
psychologists and other health providers, particularly in Bedfordshire, Hertfordshire and Essex.
This will ensure that clinical training reflects the needs of the individual and local communities as
well as the demands of the National Health Service
foster an inquiring and evaluative attitude towards all aspects of clinical psychology; and equip
trainees with the research skills necessary to conduct investigations (both quantitative and
qualitative), to appraise empirical evidence, and to take part in evidence based care.
support the general personal and professional development of trainees as well as the
development of trainees' specific personal interests and skills.
Core Philosophy The overall programme philosophy is constructivist and constructionist in nature. This involves an emphasis on how the individual constructs their personal and social world as well as how that world is constructed for them by powerful, external influences. This philosophy is reflected in the following aspects of the programme:
Acknowledgement that there are numerous viable alternative models of psychological problems and their treatment, and therefore intensive input is given on four major models (cognitive-behavioural, personal construct, psychodynamic, and systemic).
Acknowledgement of individual differences in preferences for these models, and therefore provision of the opportunity for trainees to select therapeutic models in which to obtain advanced input in their final year.
Recognition of the importance of testing out constructions of one’s world, and therefore of the scientist-practitioner approach.
Recognition that clinical practice should be evidence-based, coupled with recognition that ‘evidence’ is personally and socially constructed.
Emphasis on the range of research skills, both quantitative and qualitative, which are essential for the effective scientist-practitioner.
The promotion of a holistic, biopsychosocial approach, in which there is recognition of the

6
importance of biological, psychological, and social constructions of all clinical problems.
Emphasis on reflexive and reflective practice, involving self-monitoring and critical evaluation of the practitioner’s constructions.
The use of a range of teaching methods, but with an emphasis on interactive, participatory teaching sessions and self-directed learning.
Commitment to ethical practice, which does not favour the constructions of any particular social group and therefore promotes equality for all, regardless of race, gender, creed, age, disability, or sexual orientation.
Ownership and Currency of the Programme
The core purpose and philosophy of the programme was originally developed within the School of
Psychology, particularly by the Programme Team. However, a wider group, including local clinical
psychologists, placement supervisors and trainees, has taken ownership through representation on
the Training Course Committee.
There are various other opportunities for stakeholders in the course to provide continuing input and
feedback to it. For example, the Programme Team has incorporated a number of suggestions from
local clinical psychologists into the planning of the course programme.
One particular opportunity for stakeholders to provide input to the programme is the Annual Course
Review. This allows the Training Course Committee to consider any limitations of the programme of
study and make suggestions for change on a regular basis.
1.3 Committee Structure
In order to ensure that the quality and content of the DClinPsy Training Programme meets the needs of Clinical Psychologists in Training and fulfils the requirements for accreditation by the British Psychological Society, a system of accountability has been established. The Programme is responsible to the University of Hertfordshire, to the East of England Strategic Health Authority who provide funding, and to the Regional Clinical Psychologists in providing trained Clinical Psychologists to meet local needs. In order to show appropriate accountability to these stakeholders and a commitment to the trainees, the organisational structure involves a central role for the Training Course Committee. This Committee is accountable to all stakeholders. In order to communicate with as wide a group of interested people in the region as possible, a Course Review, to which all stakeholders are invited, is convened annually. Specific advice is required from Regional Clinical Psychologists and from placement supervisors. This is provided by the Eastern Regional Advisory Committee in Psychology. To enable the Programme to be managed on a day to day basis, there is a Training Course Executive, which is responsible to the Training Course Committee. The Training Course Executive is supported by the following Sub-Committees:
Academic (chaired by the Academic Tutor)
Research (chaired by the Research Tutor)
Clinical Skills Training (chaired by the Senior Clinical Tutor)
Selection and Outcome (chaired by the Admissions Tutor) Each Sub-Committee includes representation from regional clinical psychologists as well as trainee representation.

7
1.4 Staff
The DClinPsy Programme is managed on a day to day basis by a programme team consisting of the
Programme Director, the Deputy Programme Director, the Clinical, Academic and Research Tutors,
and the Clinical Lecturers. The programme staff are as follows: Programme Director: Prof David Winter Deputy Programme Director: Steve Davies Senior Clinical Tutor: Dr Barbara Mason Academic Tutor: Dr Pieter Nel Research Tutor: Dr Nick Wood Deputy Senior Clinical Tutor Wendy Solomons Clinical Lecturer: (& Admissions Tutor Dr Saskia Keville Clinical Lecturer/Tutor Dr Clare Norris Clinical Lecturer (Vacancy) Clinical Lecturer/Tutor Dr Tejinder Kondel Locum Clinical Tutor Dr Emma Berry Course Administrator Ms Wendy Figg Administrative Assistant Ms Cathy Lambert Four associate clinical tutors also contribute to the programme team. They work an average of 17 days per year and assist with the monitoring of trainees’ clinical skills development on placement. Our associate clinical tutors are: Dr’s Maria Gennoy, Nicole Singer, Sarah Tarzi, and Sarah Flurry.
2. Clinical placements Most of the clinical part of training takes place on clinical placement where trainees receive supervision from appropriately qualified and experienced clinical psychologists. The Clinical Skills Module in the academic programme, together with the Clinical Case Discussions and Presentations, also contribute directly to the clinical part of training.
Training Course Committee
Training Course Executive
Academic Sub-committee
Clinical Skills Sub-committee
Research Sub-committee
Selections & Outcomes Sub-committee
Regional Advisory Group for Applied Psychology

8
2.1 Overview of the placement rotations All trainees are required to acquire a range of core competencies in clinical work over the duration of their training. Trainees are also required to gain experience across a range of different client groups, service settings and problem areas in acquiring the necessary competencies. In order to ensure the necessary range of experience, trainees undertake a range of placements during their training. Most of these are of six months duration and some may be of one-year duration. Trainees usually undertake placements involving work with working age adults, older people, children and adolescents and people with learning disabilities during the first two years of their training. In the third year placements are tailored to meet specific training needs for individual trainees. In addition there is usually the opportunity for trainees to develop more specific areas of interest, once their training needs have been accounted for. Placements are usually of 22-26 weeks duration (or double this in the case of one-year placements). During term time trainees are on placement on Mondays, Tuesdays and Wednesdays with one half day out of the three days on placement being allocated to placement-related study (and in some placements to placement-related research). Trainees are expected to negotiate a regular time for the study session with their placement supervisor. This may either be taken as one half day per week or as one full day per fortnight at the discretion of the supervisor. During term time trainees attend the university on Thursdays and Fridays for the academic programme. During academic breaks trainees spend more time on placement or (in the second and third years) on research. 2.2 How placements are allocated UH clinical placements are located in Bedfordshire, Essex and Hertfordshire. Before each round of placement allocations the clinical tutors update the list of placements in Bedfordshire, Hertfordshire and Essex to confirm availability. Trainees are given the opportunity prior to allocation to indicate any specific training needs (e.g. for supervision in a specific model, or work with a particular client group) and their preferences regarding geographic location of placements and to alert the team to any special needs they might have (e.g. disability or carer responsibilities), which might restrict the placements suitable for them. Placement allocations are undertaken by the clinical tutor team in collaboration with neighbouring courses. Trainee preferences are accommodated as far as is possible. However, specific training needs (for example, arising from gaps in experience on previous placements) are considered a priority in the allocation of placements. The UH Programme Team aims to provide each trainee with the opportunity to undertake their placements within a reasonable geographical region, although this may be constrained by placement availability and specific training needs. Please note that placement allocations are done by the clinical tutors; trainees may not organise their own placements independently of this process. In the third year there may be some opportunity for trainees to undertake placements in areas of interest after training needs and gaps in experience have been taken into account. Trainees will be given specific guidance from the clinical tutors regarding the placement allocation process for third year placements. After discussing their training needs and their interests with a clinical tutor, trainees may then be advised to contact possible supervisors within the UH placement catchment area to discuss potential placements. However the final placement allocations will be done by the clinical tutors, taking into account trainees’ gaps in experience, training needs and any special needs, and matching these as far as possible with what placement supervisors are able to offer. In the rare cases where out of region placements are arranged, this is done by the clinical tutors of the courses involved. Trainees may not liaise directly with out of region supervisors regarding placements. 2.3 Honorary contracts Trainees are NHS employees as they are employed by Cambridgeshire & Peterborough Foundation Trust as a Trainee Clinical Psychologist. However, placement trusts may wish to arrange an honorary contract for trainees on placement as well, and many placement trusts insist on this. The employing Trust is responsible for undertaking Criminal Records Bureau (CRB), occupational health and any other required checks as well as for mandatory training. Confirmation of these checks may be obtained directly from the employing Trust, or in the case of CRB clearances, from the trainee. Further

9
details regarding this are provided to supervisors in a letter of confirmation prior to trainees commencing on placement. 2.4 Physical requirements The placement Trust is expected to provide a safe working environment for trainees. It is a requirement of the BPS Committee for Training in Clinical Psychology (CTCP) that trainees have at least their own desk in a shared office and access to appropriate rooms in which to see clients. Trainees are also expected to have access to appropriate administrative support, as well as to at least a shared computer, photocopying, the necessary clinical materials and secure storage for clinical records. 2.5 Supervision Trainees must be supervised by a clinical psychologist with appropriate qualifications, Health Professions Council registration, and experience. The BPS Committee on Training in Clinical Psychology (CTCP) guidelines state that all trainees should normally be supervised by a clinical psychologist who has at least two years experience after being eligible for registration as a Chartered Clinical Psychologist in the National Health Service, or a designated individual of equivalent clinical experience. In some cases a trainee may be co-supervised by a more junior clinical psychologist, a counselling psychologist or other appropriately qualified psychologist or psychotherapist. In cases where trainees have more than one supervisor, a primary supervisor is identified. The primary supervisor must meet the requirements stipulated by the BPS CTCP and the HPC. The primary supervisor is responsible for co-ordinating the placement and supervision. Trainees and supervisors are required to meet for formal supervision on a regular, scheduled basis. A minimum of one hour of formal supervision each week must be provided. There will be times when additional supervision is required. Supervisors are also expected to be available for informal discussion of issues that may arise between formal supervision sessions. The total expected contact between supervisor and trainee should be at least three hours per week. In the case of team or group supervision, trainees must always receive regular formal individual supervision as well to allow time for discussion of professional and personal issues as well as general workload and case-related material. Appropriate arrangements should be put in place to manage situations where urgent supervision is required outside of the usual supervision time. Details of the requirements for clinical supervision are provided in the BPS CTCP Guidelines on Clinical Supervision contained in Appendix 1 and in the Protocol for Managing Trainees on Placement (Appendix 2). The Professional Practice Guidelines on Teaching, Training and Supervision (DCP, 1995) are provided in Appendix 3 for information. 2.6 UH supervisor training Supervisor training workshops are organised for both new and experienced supervisors. All new supervisors are expected to attend the Good Practise in Supervision training workshops, which comprise a series of two 2-day workshops providing core training in supervisory practise.. These workshops provide supervisors with an introduction to the UH course requirements and aim to meet the key learning objectives for supervisor training recommended by the BPS. The workshop series has been approved by the British Psychological Society Learning Centre for the purposes of Continuing Professional Development (CPD).Experienced supervisors are encouraged to attend the continuing professional development (CPD) workshops on clinical supervision. Specific topics covered are informed by requests and feedback from regional supervisors and also by issues that may be noted by the programme team. Examples of topics addressed in CPD workshops on supervision include: skills in giving feedback to trainees, dealing with difficult issues in supervision, diversity and power issues in clinical supervision, assessment of clinical competence, using audio/video tapes in supervision, and skills in teaching specific therapies. 2.7 Pre-placement visits Clinical Tutor A clinical tutor has a pre-placement meeting with all new placement supervisors prior to a trainee beginning the placement. New placements are those where the supervisor is new to supervision or has not supervised a trainee before, and those placements that have not had an UH trainee before.

10
The purpose of these visits is to provide the supervisor and the clinical tutor with the opportunity to meet, to discuss the placement, to review the placement requirements, to address any potential difficulties and to undertake preliminary planning for the placement. Trainee Trainees are expected to make contact with their supervisor before beginning on placement. It is recommended that trainees visit the placement in order to meet their new supervisor face-to-face. The pre-placement visit enables supervisors to establish what the trainee’s training needs are, to review expectations and to clarify details such as days and hours of work. This can be helpful in informing pre-placement planning. 2.8 Placement contracts Placement supervisors are required to draw up a placement contract with the trainee at the outset of the placement. A copy of the agreed placement contract must be given to the trainee’s clinical tutor within the first two weeks of him/her commencing the placement. This will usually happen at the clinical tutorial held at the beginning of the placement, where the trainee and his/her clinical tutor will review the placement contract. Trainee and supervisor must sign the final version of the contract and should each keep a copy. An electronic copy of the final agreed version must be sent to the clinical tutor. The purpose of the contract is to set out the goals for the placement and to document explicitly the work that the trainee will undertake. The contract ensures that both trainee and supervisor are clear about the goals of the placement and what has been agreed. The guidelines on core competencies and experience in this handbook, the trainee’s prior experience and training needs, and the opportunities available in the specific placement should all inform the details of the contract. The contract provides a benchmark for monitoring the placement and should alert trainee, supervisor and Programme Team to any potential gaps in experience. This should allow these to be addressed as soon as possible (see Appendix 4 for contract form). 2.9 Induction and orientation All placements should begin with a period of induction and orientation. Individual supervisors may tailor the induction period to fit in with the particular placement, their own style and the particular needs of individual trainees. The induction phase will usually involve some pre-planned meetings with key people, the trainees attending scheduled meetings with their supervisors, formal and informal discussions between trainee and supervisor, shadowing and reading relevant literature. This might include literature on the theory and basic skills that trainees will need from the outset of the placement and also policy documents and guidelines about the service. The following issues should be covered during the induction: General issues
Health and safety requirements e.g. safety procedures, where the emergency alarms are, fire procedures etc.
General expectations and information e.g. dress code, hours of work, where to get lunch, where the toilets are etc.
Office procedures e.g. access to computers, how to book a room, photocopying arrangements etc.
Clinical administration e.g. how to respond to referrals, make appointments, deal with DNA’s, where files are kept, where test materials and other resources are kept, the service standards for sending out reports, record keeping policies & procedures etc.
Organisational orientation e.g. meeting the other staff, finding out who’s who, finding out what happens when etc.
Policy Documents e.g. where to access relevant Trust and other policies and guidelines including (but not limited to) health and safety policy, equal opportunities policy etc.
Supervision-related issues
Supervisory arrangements e.g. arrangements for supervision, formal vs. informal contact, how to contact you, cover arrangements and what to do in the event of a clinical emergency.

11
Previous experience & learning needs e.g. establishing what previous experience the trainee has, what areas have been flagged for development etc. This may involve reviewing the Placement Continuation form from the trainee’s previous placement.
The trainee’s learning style, how s/he prefers to get feedback, and what s/he has found helpful/unhelpful in past supervision/learning experiences.
Basic clinical skill requirements e.g. what the trainee might read by way of introduction to the placement.
Your expectations as a supervisor along with your preferences e.g. theoretical orientation, style of working, your expectations about how the trainee asks for help or communicates their needs to you.
Course-related issues
Academic teaching – you might wish to ask your trainee what teaching they have covered that is relevant to the placement. Trainees may provide you with copies of their academic timetables and relevant module outlines from the Course Handbook.
Placement Reviews – you should discuss the arrangements for placement reviews; the clinical tutor will provide your trainee with a list of possible dates.
While supervisors are expected to have set up at least some aspects of induction prior to the trainee starting on placement, trainees are encouraged to take an active role in the induction process. They are encouraged to ask questions and to be proactive in approaching you about the things they need to cover. 2.10 Learning & teaching and the transition to independent work It is expected that trainees will need guidance and direction from their supervisor in order to develop the required skills and competencies. Typically trainees will usually need to begin by observing their supervisor, then move on to joint working and then on to independent work. The rate at which this progression is made will depend in part on the trainee’s prior experience and skills, the nature of the placement, and whether this is a first or later placement. In a first placement, trainees are likely to feel de-skilled. This is a normal response. New trainees are not expected to be competent clinicians from the outset. Rather they are expected to learn and develop the core competencies required of the clinical psychologist throughout their training. There should be a range of learning and teaching methods available to trainees on placement, for example, discussion, teaching, feedback and reflection in the context of supervision, observation of their supervisor and/or other practitioners, being observed, undertaking joint clinical and/or other work, receiving feedback on recordings of their work, undertaking self-directed learning and reading, role play and demonstration where appropriate, and the experience of applying knowledge in practise. As adult learners, trainees are encouraged to take and active role in their own learning and to discuss their learning needs with their supervisors. Supervisors are encouraged to contribute to this dialogue and to think together with the trainee about how best to enable their learning and development. 2.11 Work Load It is important for trainees to have an appropriate balance and quantity of work. Too little work may limit the range of experience and opportunity to learn, while too much work will reduce the trainee’s time for preparation and reflecting upon practice. The specific number of clients will vary depending on the nature of the placement and the nature of the work being done. However, it is expected that trainees will usually have a caseload of about 6 to 8 clients at any one time. Trainee and supervisor need to ensure that the appropriate balance is maintained between direct client work, indirect client work, organisational work, teaching and service related research. 2.12 Integrating Theory and Practice On placement trainees are expected to develop their clinical skills and to have practice in integrating their theoretical knowledge with their clinical practice. Supervisors are encouraged to suggest relevant reading material and research for the trainee to review.

12
2.13 The development of professionalism A theme common to all placements is the development of professionalism. This encompasses several aspects: Interpersonal style and communication Trainees need to develop an interpersonal style that is appropriate to their professional role, the situations in which they find themselves, and their interactions with both other professionals and clients. Trainees are expected to develop competencies in both verbal and written communication in order to support effective professional functioning. Risk In all areas of professional practice trainees need to consider issues of risk. This includes minimising risk to self. Trainees must understand local and national policies and procedures on risk management. Trainees are also expected to learn about the legal aspects of clinical work and their responsibilities. Supervisors have an important role to play in assisting trainees to think about issues of risk and to understand these in relation to their clinical work on placement. Trainees need to familiarise themselves with service related risk policies and supervisors should provide any relevant documentation (or instruct the trainee as to where this can be obtained). Adopting an ethical approach Trainees are expected to uphold the ethical guidelines of the profession as outlined in the Health Professions Council Guidance on Conduct and Ethics for Students (2009), the BPS Code of Ethics and Conduct (2009), the BPS Generic Professional Practice Guidelines (2008) and the Division of Clinical Psychology Guidelines for the Professional Practice of Clinical Psychology (1995, revised 2001). However, adopting an ethical approach extends beyond a rote knowledge of codes of conduct or ethical guidelines. Trainees need to learn how to apply these in their everyday practice and when to seek advice. It is expected that these issues will be considered within the context of supervision. Personal issues Trainees need to consider their own constructed position in the world. This may include their beliefs and assumptions, past and current life events and other relevant context. Trainees have to consider how these might impact upon their client work. Trainees also need to develop the personal skills that support effective functioning as a professional (e.g. stress modulation and time management). Issues such as these, insofar as they relate to clinical and professional practice, may be appropriately addressed in supervision. However, if trainees have personal difficulties, it may not be appropriate to deal with these in the supervisory situation. There are a range of supports available to trainees including course tutors, personal advisors, and the university counselling service. Trainees’ personal advisors and/or members of the programme team can provide them with guidance on finding a personal therapist.
3. Competencies and Experience 3.1 Essential Experience Over the course of the three year training programme certain experience is considered essential in order for trainees to develop the required competencies. This is based on the requirements specified in the BPS Committee on Training in Clinical Psychology’s Criteria for the Accreditation of Post-graduate Training Programmes in Clinical Psychology (2007) and also maps onto the Health Professions Council Standards of Proficiency for Practitioner Psychologists. An extract from the full BPS course accreditation criteria are included in Appendix 5 for information, and the HPC Standards of Proficiency are available on the HPC website: www.hpc-uk.org . Trainees are required to work with a range of clients across a range of settings, using a variety of modes of working. The clients, settings and modes of working include the following:

13
Clients
A fundamental principle is that trainees must work with clients across the lifespan, such that they see a range of clients whose difficulties are representative of problems across all stages of development. In this context, trainees must demonstrate competence to work clinically with:
a wide breadth of clinical presentations – from acute to enduring and from mild to severe;
problems ranging from those with mainly biological and/or neuropsychological causation to those emanating mainly from psychosocial factors;
problems of coping, adaptation and resilience to adverse circumstances and life events, including bereavement and other chronic physical and mental health conditions; and
clients from a range of backgrounds reflecting the demographic characteristics of the population. Trainees will need to understand the impact of difference and diversity on people’s lives (including sexuality, disability, ethnicity, culture, faith, cohort differences of age, socio-economic status), and their implications for working practices. It is also essential that trainees work with:
clients with significant levels of challenging behaviour;
clients across a range of levels of intellectual functioning over a range of ages, specifically to include experience with clients with developmental learning disabilities and acquired cognitive impairment;
clients whose disability makes it difficult for them to communicate; and
carers and families of clients.
Service Delivery systems Trainees must undertake substantial pieces of clinical work over a substantial period of time in each of a range of settings, including:
in-patient or other residential facilities for individuals with high dependency needs, both acute and long term;
secondary health care; and
community and primary care
Modes and type of work Trainees must demonstrate competence in undertaking:
direct work with clients;
indirect work, through staff and/or carers;
work within multi-disciplinary teams and specialist service systems, including some observation or other experience of change and planning in service systems;
work in at least two evidence-based models of formal psychological therapy. This must include cognitive-behaviour therapy and at least one other evidence-based approach.
work across a range of perspectives, demonstrating flexibility in application of whichever approach is most appropriate for the client or system.
Trainees should be critical of their own approach, and aware of how to practise in the absence of reliable evidence, as well as being able to contribute from their work to the evidence base.
The UK health care context Trainees’ work will need to be informed by an appreciation of the legislative and organisational contexts within which clinical practice is undertaken, including for example:

14
legislation relevant to England and the devolved nations (e.g. Mental Health Act, Mental Capacity Act, Children Act, Disability Discrimination Act, Health and Social Care Act, Data Protection Act, employment legislation, etc.);
Government policy statements (e.g. National Service Frameworks, Ten Essential Shared Capabilities, Knowledge and Skills Framework, etc.); and
organisation of the NHS and social care in England and the devolved nations. Trainees will not be in a position to cover the entire range of experience in every placement; however it is important to gain the range of experience and related competencies over the duration of the training so they and the supervisor should make the most of experience that is available on each placement. The range of experience covered will be assessed via the Logs of Clinical Experience and subject to ongoing monitoring via the Summary Log of Clinical Experience. However, the person who will be most aware of any gaps in training will be the trainee. It is the trainee’s responsibility to monitor their own range of experience and to alert their clinical tutor and supervisors to gaps in experience. 3.2 Core Competencies The BPS Committee on Training in Clinical Psychology’s Criteria for the Accreditation of Post-graduate Training Programmes in Clinical Psychology (2007) specify several required learning outcomes for clinical psychology training. Following from these they provide an overview of broad competencies, which trainees need to acquire over the course of their training. The competencies outlined below are based on these. An extract from the full course accreditation criteria are included in Appendix 5 for information. The core competencies also map onto the Health Professions Council Standards of Proficiency for Practitioner Psychologists, which are available on the HPC website: www.hpc-uk.org . Transferable skills
Trainees need to become competent in deciding, using a broad evidence and knowledge base, how to assess, formulate and intervene psychologically, from a range of possible models and modes of intervention with clients, carers and service systems. Trainees should be able to generalise and synthesise prior knowledge and experience in order to apply them in different settings and novel situations Trainees must develop self-awareness and the ability to work as a reflective practitioner Trainees must demonstrate the ability to think critically, reflectively and evaluatively. By the end of their training, trainees must be able to make informed judgements on complex issues in specialist fields, often in the absence of complete information. Trainees must be able to communicate psychologically-informed ideas and conclusions clearly and effectively to specialist and non-specialist audiences, in order to facilitate problem solving and decision making. Trainees must demonstrate the capacity to exercise personal responsibility and to take initiative in complex and unpredictable situations in professional practice By the end of their training, they should be able to draw on their psychological knowledge of complex developmental, social and neuropsychological processes across the lifespan to facilitate adaptability and change in individuals, groups, families, organisations and communities. Trainees must demonstrate the ability to work effectively whilst holding in mind alternative, competing explanations. Psychological Assessment Trainees must be able to develop and maintain effective working alliances with clients, including individuals, carers and services.

15
Trainees must learn to choose, use and interpret a broad range of assessment methods appropriate:
to the client and service delivery system in which the assessment takes place; and
to the type of intervention which is likely to be required. Trainees must demonstrate competence in:
formal procedures (use of standardised instruments);
systematic interviewing procedures;
other structured methods of assessment (e.g. observation or gathering information from others); and
assessment of social context and organisations. Trainees must achieve competence in conducting appropriate risk assessment and using this to guide practice. Psychological Formulation Trainees must be able to develop formulations of presenting problems or situations which integrate information from assessments within a coherent framework that draws upon psychological theory and evidence and which incorporates interpersonal, societal, cultural and biological factors. Trainees must learn to use formulations with clients to facilitate their understanding of their experience. Trainees must demonstrate competence in using formulations to plan appropriate interventions that take the client’s perspective into account. Trainees must acquire the skills needed to use formulations to assist multi-professional communication, and the understanding of clients and their care. Trainees need to become competent in revising formulations in the light of ongoing intervention and when necessary re-formulating the problem.
Psychological Intervention On the basis of a formulation, trainees must demonstrate competence in implementing psychological therapy or other interventions appropriate to the presenting problem and to the psychological and social circumstances of the client(s), and to do this in a collaborative manner with:
individuals
couples, families or groups
services/organisations By the end of training, trainees must demonstrate an understanding of therapeutic techniques and processes as applied to a range of different individuals, including those who experience difficulties related to: anxiety, mood, adjustment to adverse circumstances or life events, eating, psychosis and use of substances, and those with somatoform, psychosexual, developmental, personality, cognitive and neurological presentations. By the end of training, trainees must be able to integrate and implement therapeutic interventions based on knowledge and practice in at least two evidence-based models of formal psychological therapy, one on which must be cognitive-behaviour therapy. Trainees must attain competence in implementing indirect intervention, i.e. implementing interventions through and with other professions and/or with individuals who are formal (professional) carers for a client, or who care for a client by virtue of family or partnership arrangements. Trainees must have an understanding of social approaches to intervention for example, those informed by community, critical, and social constructionist perspectives.

16
Trainees must have an awareness of the impact of pharmacological and other clinical interventions. Trainees must learn to recognise when (further) intervention is inappropriate, or unlikely to be helpful, and communicate this sensitively to clients and carers. Evaluation Trainees need to learn how to evaluate the effectiveness, acceptability and broader impact of interventions (both individual and organisational), and to use this information to inform and continuously improve practice. Where appropriate this may involve devising innovative procedures and methodology for achieving this outcome. Trainees must develop the skills to audit clinical effectiveness
Research
1
Trainees must be able to identify and critically appraise research evidence relevant to practice. They must have an understanding of applicable techniques for clinical research and advanced academic enquiry, including quantitative and qualitative approaches. Trainees must acquire the necessary knowledge and skills to conduct service evaluation, research with small numbers of participants, and collaborative research. Trainees must be able to conceptualise, design and conduct independent original research of a quality to satisfy peer review: including. identifying research questions, demonstrating an understanding of ethical issues, choosing appropriate research methods and analysis, reporting outcomes and identifying appropriate pathways for dissemination.
Personal and Professional Skills Trainees must demonstrate an understanding of ethical issues and the application of these in complex clinical contexts, ensuring that informed consent underpins all contact with clients and research participants. Trainees must develop an appreciation of the inherent power imbalance between practitioners and clients and how abuse of this can be minimised. Trainees need to understand the impact of difference and diversity on people’s lives, and its implications for working practices. Trainees should understand the impact of their own value base upon clinical practice. Trainees must work effectively at an appropriate level of autonomy, with awareness of the limits of their own competence, and accepting accountability to relevant professional and service managers. Trainees must learn to manage their own personal learning needs and develop strategies for meeting these. Trainees must be able to use supervision to reflect on practice, and make appropriate use of feedback received. Trainees need to develop strategies to handle the emotional and physical impact of their own practice and to seek appropriate support when necessary, with good awareness of boundary issues. Trainees must demonstrate the ability to work collaboratively and constructively with fellow psychologists and other colleagues and users of services, respecting diverse viewpoints.
1The research competencies are included here for completeness. It is expected that for the most part research
competencies will be developed via research teaching at the university, relevant private study and reading, and
experience of carrying out both service-related and large-scale independent research.

17
Trainees must have the competence to monitor and maintain health, safety and security of self and others. Communication and Teaching Trainees must be able to communicate effectively clinical and non-clinical information from a psychological perspective in a style appropriate to a variety of different audiences (e.g. to professional colleagues, and to users and their carers). Trainees must acquire skills in adapting style of communication to people with a wide range of levels of cognitive ability, sensory acuity and modes of communication. Trainees should demonstrate competence in preparing and delivering teaching and training which takes into account the needs and goals of the participants (for example by appropriate adaptations to methods and content). Trainees should understand the supervision process for both supervisee and supervisor roles. Trainees need to develop an understanding the process of providing expert psychological opinion and advice, including the preparation and presentation of evidence in formal settings.
Trainees need to develop an understanding the process of communicating effectively through interpreters and having an awareness of the limitations thereof.
Trainees need to develop the knowledge and skills necessary to support others’ learning in the application of psychological skills, knowledge, practices and procedures.
Service Delivery Trainees must acquire the knowledge and skills to adapt their practice to a range of organisational contexts, on the basis of an understanding of pertinent organisational and cultural issues. Trainees must develop an understanding of consultancy models and the contribution of consultancy to practice. Trainees must develop an understanding of leadership theories and models and their application to service development and delivery. Trainees should develop the knowledge and skills to enable them to provide supervision within their own sphere of competence. Trainees must have an awareness of the legislative and national planning context of service delivery and clinical practice. Trainees should learn to work with users and carers to facilitate their involvement in service planning and delivery. Trainees must demonstrate competence in working effectively in multi-disciplinary teams together with an understanding of the roles of different professionals. Trainees need to develop the knowledge and skills needed to work effectively with formal service systems and procedures. Trainees should understand relevant quality assurance principles and processes. It is expected that the knowledge and skills needed to support the above competencies will be acquired through a combination of academic teaching, self-directed learning and reading, experience on placement, clinical supervision, research assignments and the personal development aspects of the course.

18
4. Placement Monitoring Trainees' progress is monitored over the duration of the three year programme to ensure that they gain the necessary range of clinical experience and that they develop the expected level of clinical competency across the range. Monitoring is seen as an ongoing and continuous process. The trainee, the placement supervisor, the clinical tutor and the Programme Team are all responsible for monitoring the trainee’s clinical progress. It is expected that monitoring will form a part of the supervision process (along with the other functions of supervision). Members of the Programme Team also monitor trainees’ progress at regular tutorial meetings. Teaching exercises and case presentations at the university also contribute to ongoing monitoring of trainee progress and development. Formal monitoring of clinical skills and experience is carried out via clinical tutorials (Appendix 6), mid- and end-of-placement reviews (Appendix 7), the Log of Clinical Experience (Appendix 8), the Summary Log of Clinical Experience (Appendix 9), and the Supervisor Evaluation of Clinical Competence (Appendix 10). These are described in more detail below. 4.1 Clinical Tutorials The trainee’s clinical tutor meets with him/her during the first month of each placement for a clinical tutorial. The purpose of the clinical tutorial held early in the placement is to monitor the trainee’s progress, to ensure continuity from one placement to the next, and to ensure that the trainee gains the necessary range of experience and skills over the duration of his/her training. Clinical tutorials take place at the university. Trainees are expected to take their Placement Contract and their Summary Log of Clinical Experience to the tutorial. It is therefore important that the Placement Contract is completed within the first two weeks of placement, prior to the clinical tutorial. The tutor brings a copy of the last End-of Placement Review (EPR) form and the Continuation Sheet. The specific tasks of the clinical tutorial include:
A review of training needs arising from previous placements
Monitoring of the Summary Log of Clinical Experience and gaps in the trainee’s range of experience
A review of the new placement contract Other issues may also be covered in clinical tutorials as they arise. Trainees and clinical tutors may arrange additional clinical tutorials if necessary.
4.2 Mid-placement reviews Goals The purpose of the mid-placement review is to monitor the placement, the clinical experiences and competencies the trainee has gained, and the supervision provided, mid-way through the placement. It offers an opportunity to resolve any problems that may have arisen and to identify unmet goals. The placement visit is deemed essential by the BPS CTCP. Specific goals of the mid-placement review are:
to review experience gained so far on the placement, to compare this to the placement contract agreed at the outset of placement, to identify gaps in experience and to plan how these gaps in experience may be addressed over the remainder of the placement;
to review trainee progress in terms of their development, acquisition of skills and clinical competence, to identify areas of strength and weakness and to discuss how the trainee may be supported in developing any areas of weakness;
to review the placement and the supervision arrangements, to identify any difficulties and to discuss how these might be addressed; and
to offer both trainee and supervisor the opportunity to discuss any other issues of concern and to facilitate constructive problem solving around this.
Organisation Approximately half–way into the placement the clinical tutor meets with the trainee and the placement supervisor for the mid-placement review. The date and time for the mid-placement review are set at the beginning of each placement. This is usually negotiated when the placement contract is agreed. It is the trainee’s responsibility to negotiate a time that is suitable for placement supervisor and clinical

19
tutor. The mid-placement review is held at the placement base, not at the university. In the case of one year placements, trainees will usually have two MPRs (approximately one third and two thirds of the way through the placement respectively) and one EPR at the very end of the placement. The mid-placement review meeting usually lasts about 1hr30mins to 2hrs. During the first part of the MPR, the clinical tutor meets with the trainee alone. In the second part the clinical tutor meets with the supervisor alone. There is then a joint meeting between the clinical tutor, the trainee and the supervisor. The contents of the individual meetings are treated as confidential. However, in each of these meetings specific feedback is agreed for inclusion in the summary of the placement meeting, which will be circulated to trainee, supervisor and tutor. The joint meeting allows the opportunity for discussion of any issues arising in the individual meetings and for trainee, supervisor and tutor to agree goals and action plans for the remainder of the placement. A summary of the issues covered, and of the agreed goals and action points arising in the mid-placement review is written up by the clinical tutor. Copies are sent to the trainee, the placement supervisor and the trainee’s personal course tutor. 4.3 End of placement reviews Goals At the end of placement review feedback is given by the supervisor and by the trainee. The goals of the end-placement review are:
to obtain feedback from the supervisor on the trainee’s clinical competence and to discuss any issues arising from this;
to obtain feedback from the trainee about the placement and supervision and to discuss any issues arising from this; and
to review the trainee’s range of experience and ratify the information recorded in the Log of Clinical Experience (Appendix 8).
to identify training needs and gaps in experience, which is recorded on the Placement Continuation form (contained in Appendix 7) for communication with the trainee’s next supervisor.
Organisation The end of placement review usually takes place during the last few weeks of the placement, the date having been agreed by the mid-placement review at the latest. The end of placement review usually takes up to 1h30mins in total and follows the same format as the mid-placement review. First the clinical tutor meets with the trainee. In this time the trainee is asked for feedback about the placement and the trainee’s range of experience is reviewed and the trainee is asked to evaluate his/her own competencies. The trainee is also given the opportunity to ask any questions about the Log of Clinical Experience, the examples of clinical work s/he plans to submit and the clinical case report. The clinical tutor then meets with the placement supervisor. In this meeting the supervisor gives feedback on the trainee’s clinical competence based on the completed Supervisor Evaluation of Clinical Competence form. The supervisor also makes a formal recommendation on the overall rating for the placement. Finally the clinical tutor meets with trainee and supervisor jointly. The purpose of this meeting is to facilitate feedback between trainee and supervisor, to discuss any areas of difficulty and to agree on what information to include in the Placement Continuation form. The Placement Continuation form will be sent on to the trainee’s next supervisor to ensure continuity between one placement and the next. In some circumstances, it is possible for the End of Placement Review to be carried out via telephone. Telephone EPRs will only be used when there have been no concerns at mid-placement review and when trainee, supervisor and tutor all agree that this is appropriate. At the end of the placement period, the trainee will have the opportunity to read and consider the completed Supervisor Evaluation of Clinical Competence form (Appendix 10) and to write down any comments and points of disagreement. The Supervisor Evaluation of Clinical Competence form is counter-signed by the trainee to indicate that s/he has read it and noted any points of disagreement. Similarly the supervisor is given the opportunity to read and consider the Trainee Placement Feedback

20
and Placement Audit forms (Appendix 11) and to note any comments and points of disagreement. The Trainee Placement Feedback and Placement Audit forms must be counter-signed by the supervisor to indicate that s/he has read it and noted any points of disagreement. The Log of Clinical Experience (Appendix 8) also must be counter-signed by the supervisor to confirm that the contents are a fair reflection of the trainee’s activities while on placement. The signed Log of Clinical Experience, Supervisor Evaluation of Clinical Competence form and Trainee Placement Feedback and Placement Audit forms, as well as the example of clinical work (discussed below) must be submitted to the Programme Administrator by the deadlines specified on the timetable provided to trainees (usually one week after the end of the placement). In the case of one-year placements, a single end of placement review will take place at the end of the placement. However trainees and supervisors are still required to submit all the required evaluations after each placement period, as specified on the timetable. This means that two sets of evaluations are required for one-year placements because they extend over two placement periods. 4.4 Placement difficulties Where minor difficulties occur on placement, in the first instance trainee and supervisor should attempt to resolve the problem together. However where this is not possible or not appropriate either trainee or supervisor should contact the trainee’s clinical tutor or the Senior Clinical Tutor. Where appropriate the trainee’s clinical tutor or the Senior Clinical Tutor will arrange a joint meeting with trainee and supervisor to discuss the problem at hand. It is preferable to seek advice earlier rather than later so that concerns or difficulties can be addressed as soon as possible. Supervisors are advised to contact the trainee’s clinical tutor or the Senior Clinical Tutor in case of any concerns. Where there are serious concerns on the part of a supervisor about a trainee, it is the responsibility of the supervisor to inform the clinical tutor about these concerns as soon as possible. Similarly, where there are serious concerns on the part of a trainee about the placement or the supervision, it is the responsibility of the trainee to inform the clinical tutor in a likewise timely manner. Apart from exceptional circumstances, any trainee who is in danger of failing a placement should have been alerted to this at the mid-placement review in order to give them an opportunity to improve or rectify their performance before the end of the placement. The detailed policy on placement difficulties is contained in Appendix 12. 4.5 Placement Feedback & Audit At the end of each placement period, trainees are required to complete and submit Trainee Placement Feedback and Placement Audit forms (Appendix 11). The Trainee Placement Feedback form provides feedback on the placement and the supervision. The specific aims are:
1. To provide the basis for discussion between trainee, supervisor and tutor about the placement
and the supervision at the end of placement review, 2. To provide feedback to the Programme Team about what the placement offers, thereby
enhancing the matching of future trainees’ needs to specific placements in the placement allocations process,
3. To identify strengths, weaknesses and areas for development, which the supervisor may use to inform his/her own professional development, and the Programme Team may use to identify where further support or training may be necessary, and
4. To Flag up any specific problems on the placement, addressed as per the policy on placement difficulties (Appendix 12).
The Placement Audit form is used to gather information relating to the minimum requirements for placements. The specific aims are to collect information that will allow the programme (1) to identify where minimum standards are not being met and to offer support to supervisors and/or services in addressing these issues, as appropriate, and (2) to gather information relating to these minimum standards for the purposes of placement audit. Only cumulative and anonymised data is reported in the placement audit. The results of the placement audit are presented at the Annual Course Review, and reported to other stakeholders where appropriate.
21
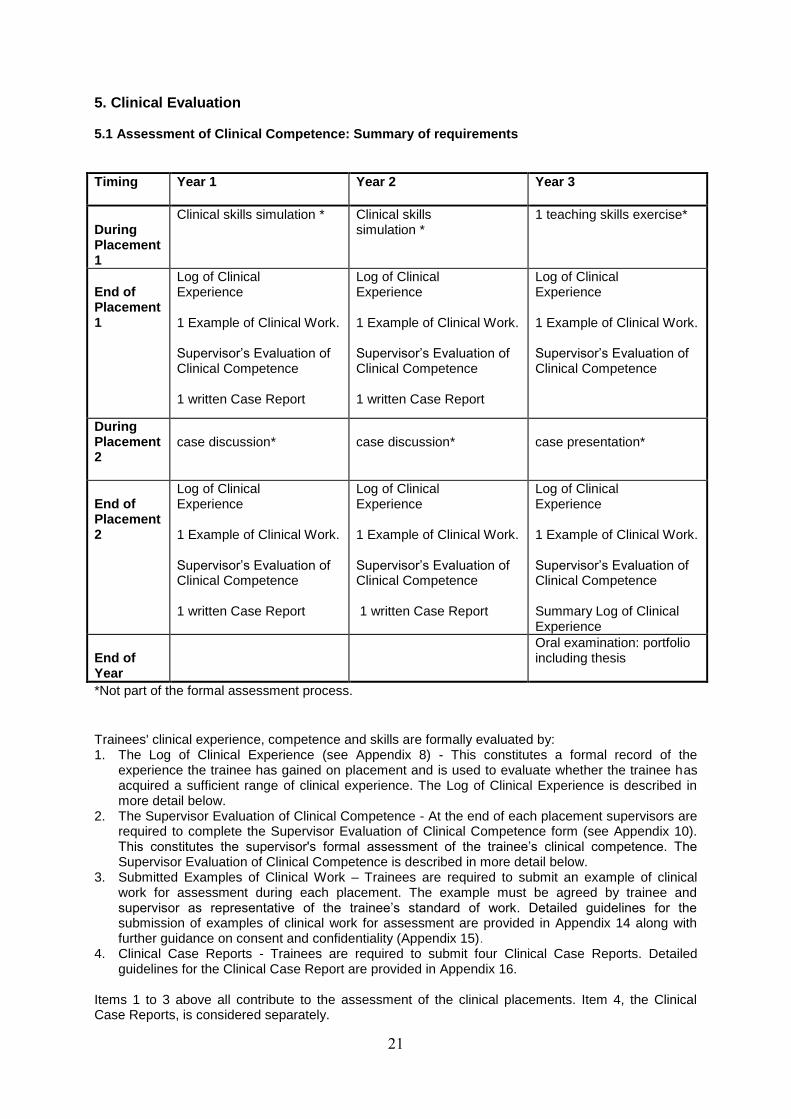
5. Clinical Evaluation 5.1 Assessment of Clinical Competence: Summary of requirements
Timing
Year 1 Year 2 Year 3
During Placement 1
Clinical skills simulation * Clinical skills simulation *
1 teaching skills exercise*
End of Placement 1
Log of Clinical Experience 1 Example of Clinical Work. Supervisor’s Evaluation of Clinical Competence 1 written Case Report
Log of Clinical Experience 1 Example of Clinical Work. Supervisor’s Evaluation of Clinical Competence 1 written Case Report
Log of Clinical Experience 1 Example of Clinical Work. Supervisor’s Evaluation of Clinical Competence
During Placement 2
case discussion*
case discussion*
case presentation*
End of Placement 2
Log of Clinical Experience 1 Example of Clinical Work. Supervisor’s Evaluation of Clinical Competence 1 written Case Report
Log of Clinical Experience 1 Example of Clinical Work. Supervisor’s Evaluation of Clinical Competence 1 written Case Report
Log of Clinical Experience 1 Example of Clinical Work. Supervisor’s Evaluation of Clinical Competence Summary Log of Clinical Experience
End of Year
Oral examination: portfolio including thesis
*Not part of the formal assessment process.
Trainees' clinical experience, competence and skills are formally evaluated by: 1. The Log of Clinical Experience (see Appendix 8) - This constitutes a formal record of the
experience the trainee has gained on placement and is used to evaluate whether the trainee has acquired a sufficient range of clinical experience. The Log of Clinical Experience is described in more detail below.
2. The Supervisor Evaluation of Clinical Competence - At the end of each placement supervisors are required to complete the Supervisor Evaluation of Clinical Competence form (see Appendix 10). This constitutes the supervisor's formal assessment of the trainee’s clinical competence. The Supervisor Evaluation of Clinical Competence is described in more detail below.
3. Submitted Examples of Clinical Work – Trainees are required to submit an example of clinical work for assessment during each placement. The example must be agreed by trainee and supervisor as representative of the trainee’s standard of work. Detailed guidelines for the submission of examples of clinical work for assessment are provided in Appendix 14 along with further guidance on consent and confidentiality (Appendix 15).
4. Clinical Case Reports - Trainees are required to submit four Clinical Case Reports. Detailed guidelines for the Clinical Case Report are provided in Appendix 16.
Items 1 to 3 above all contribute to the assessment of the clinical placements. Item 4, the Clinical Case Reports, is considered separately.

22
In addition, trainees are required to present one case per year to their peers and to the Programme Team. Clinical skills exercises are assigned as a part of the clinical skills teaching programme at the university. While none of these contribute to the formal evaluation of trainee clinical competence, they provide an opportunity for trainees to receive regular feedback on their skills. 5.2 Log of Clinical Experience & Summary Log of Clinical Experience Trainees are required to keep a record of all experiences gained on placement in a Log of Clinical Experience (see Appendix 8). A Log of Clinical Experience is completed for each of the placements undertaken over the three years. The Logs of Clinical Experience are used to monitor trainee experience during each placement and to inform goal setting in subsequent placements. The Logs of Clinical Experience provide a formal record of trainee experience, which become part of the portfolio of work that is submitted for oral examination. Trainees are also required to complete a Summary Log of Clinical Experience (see Appendix 9). This is a summary of the essential experience that they are expected to have acquired over the course of their training. The Summary Log of Clinical Experience is carried over from one placement to the next. The Summary Log of Clinical Experience does not constitute a part of formal evaluation; rather it is intended to facilitate monitoring of the range of clinical experience over the three years, to inform goal setting and to provide a link between one placement and the next. Trainees are expected to review their Summary Log of Clinical Experience with their clinical tutors at regular clinical tutorials and to submit it along with their other placement documents at the end of their final placement. 5.3 The Supervisor Evaluation of Clinical Competence form The Supervisor Evaluation of Clinical Competence form is completed by placement supervisors at the end of each placement. This constitutes a part of the formal evaluation of trainee clinical competence. Supervisors should have discussed progress with their trainees from time to time throughout the placement and therefore the contents of the Supervisor Evaluation of Clinical Competence form should not be unexpected. However the feedback will be more formal and comprehensive and can offer an opportunity to highlight strengths and needs more clearly. In the case of placement failure, the grounds for failure must be stated explicitly by the placement supervisor and where possible, examples and evidence should be provided. The procedure that is followed in the case of placement failure is described below. 5.4 Examples of Clinical Work Trainees are required to submit one example of clinical work at the end of each placement from the following list. They may choose in what order to submit the examples; however they are required to submit one audio/video tape example within each academic year of the programme. 1. An audio or video recording of an initial clinical interview. 2. An audio or video recording of a therapy session. 3. An audio or a video recording of a therapy session OR detailed process notes of a therapy session. 4. One written piece of communication (report or letter) with a critical commentary. 5. A written letter OR a transcript of a section of a tape in which formulation is used to facilitate a client’s understanding of his/her difficulties OR in which formulation is used to facilitate a carer’s understanding of a client’s difficulties (Here ‘carer’ refers to a family member or other non-professional carer). 6. A psychometric assessment report with a critique and evaluation of one of the tests used. Further information and detailed guidelines on Examples of Clinical Work are provided in Appendix 14. 5.5 Submission of Placement Documents

23
All placement documents must be submitted by the stated deadline; this is usually one week after the last day of the placement
2. Late submissions will usually result in placement failure. Any requests for
extensions must be made before the submission deadline. The Log of Clinical Experience, Supervisor Evaluation of Clinical Competence form, Example of Clinical Work and Trainee Placement Feedback and Placement Audit forms must all be submitted to the Programme Administrator by 2 pm on the submission date. It is preferable for all documents to be submitted together along with the Placement Documents Checklist (which is available on Studynet). Trainees should submit 1 copy of the full set of documents and 2 copies of the Example of clinical work, one of which must be anonymised for blind marking. What this means is that all information that might identify the trainee should be removed i.e. name, supervisor’s name and the specific placement location. The blind markers’ copies should be identified by student number alone. All documentation must be anonymous for client information (Refer to Appendix 15). Trainees should retain a copy of all placement related submissions for their records as these will need to be included in their final portfolio. 5.6 Placement Marking Log of Clinical Experience The Log of Clinical Experience is reviewed by the clinical tutor, who will be aware of any circumstances related to the placement, which might have influenced the range of experience available to the trainee. Marking criteria for the evaluation of the Log of Clinical Experience are contained in Appendix 13. The Example of Clinical Work The Example of Clinical Work is assessed by the clinical tutor and by a member of the Programme team. The former will have knowledge of the candidate and the placement so will not be blind to the evaluation process. The latter will, wherever possible, be blind to the identity of the trainee and the placement supervisor. The marking criteria for the evaluation of the Examples of Clinical Work are contained in Appendix 14. Supervisor Evaluation of Clinical Competence: The supervisor evaluation of clinical competence form is reviewed by the trainee’s clinical tutor (who is not blind to the trainee’s identity). The supervisor evaluation of clinical competence carries with it a recommendation from the supervisor for a pass, conditional pass or fail. In most cases the supervisor’s grading is simply transferred to the placement marking sheet; however the final decision regarding the overall outcome of the placement rests with the Progression Board of Examiners. It is possible that this may be different from the supervisor recommendation, for example, where the supervisor recommendation is not consistent with the marking guidelines, or where performance on other aspects, such as the Example of Clinical Work or the Log of Clinical Experience, results in an overall outcome different from that on the Supervisor Evaluation of Clinical Competence form. In circumstances where the clinical tutor reviewing the placement recommends an outcome different to that on the Supervisor Evaluation of Clinical Competence form, a second marker, who is blind to the identity of the trainee and the supervisor, will also assess the placement documents. The criteria used to evaluate clinical competence as a pass, conditional pass or a fail are contained in Appendix 13.This appendix also contains flowcharts that map out the marking process for placement submissions. 5.7 Placement Outcomes A placement may be evaluated as a pass, a pass with minor amendments, a conditional pass or a fail. Pass: This follows when all aspects of the placement are passed i.e. the Supervisor Evaluation of Clinical Competence, the Log of Clinical Experience and the Example of Clinical Work.
2 In the case of one-year placements, it is required that placement documents are submitted for each placement
period. What this means is that trainees submit a Log of Clinical Experience, an Example of Clinical Work, A
Supervisor Evaluation of Clinical Competence and a Trainee Placement Evaluation after the first placement
period (usually 6 months in) and again at the end of the second placement period (at the end of the year).

24
Pass with minor amendments: This follows when all aspects of the placement are passed but where minor corrections are required, for example, minor changes required to how information is recorded in the Log of Clinical Experience or minor slips in anonymisation. Conditional Pass: This will normally follow when the supervisor evaluation of clinical competence indicates a conditional pass rating and/or the log of clinical experience is given a conditional pass due to an insufficient range of experience and/or insufficient days having been completed on the placement, usually due to a period of absence. and/or the example of clinical work is given a fail rating upon first submission. In the case of a conditional pass, the trainee will be required to fulfil certain requirements during the course of their next placement. Where the specified requirements are completed to the satisfaction of the original markers (and the Progression Board of Examiners) the trainee will be deemed to have passed the original placement. Where the specified requirements are not completed to the satisfaction of the original markers (and the Progression Board of Examiners) the trainee will be deemed to have failed the original placement. For example, where the conditional pass has arisen due to concerns on the part of the supervisor about specific areas of competence, the trainee may be required to demonstrate improvement in these areas which bring him/her back into line with what would be expected at his/her stage in training; where a conditional pass has arisen due to insufficient experience or insufficient days on placement, a trainee may be required to complete specified experience in a subsequent placement and/or to undertake additional placement days, thereby increasing the length of his/her training; where a conditional pass has arisen due to a failure on the example of clinical work, the trainee will be required to resubmit the example (or an example meeting the same criteria) within a specified time period. In the event of the example being failed upon re-submission, the trainee would automatically be deemed to have failed the original placement. Fail: Placement failure will normally follow if:
the Log of Clinical Experience is failed due to a failure to show a sufficient range of experiences other than where this has resulted from the lack of opportunity provided by the clinical placement.
and/or
the Supervisor Evaluation of Clinical Competence gives an overall ‘fail’ rating and/or
the trainee fails an example of clinical work upon resubmission and/or
the trainee, after appropriate investigatory procedures, is found guilty of professional misconduct or is deemed to have acted in a manner that jeopardises the welfare of another (whether patient, client, student or staff) - Trainees are required to abide by the Health Professions Council’s and the British Psychological Society's professional and practice guidelines at all times and ensure that their behaviour at no time, nor in any way, can be deemed as an act of professional misconduct or as professionally unsuitable. A failure to do so usually will result in instant dismissal with no possibility of repeating a placement or reassessment of work.
In the case of a placement failure the trainee will be required to repeat some or all of the clinical placement as required by the Progression Board of Examiners, apart from in circumstances that result

25
in withdrawal of registration. Only one placement may be failed. Failure on a second placement will result in course failure and withdrawal of registration. In all cases the final decision regarding placement pass/fail rests with the Principal Board of Examiners. 5.8 Procedure for conditional passes and placement failures Where a supervisor recommends a conditional pass or a fail rating for a placement:
This should be indicated to the clinical tutor at the End of Placement Review.
The clinical tutor will ask the supervisor for his/her reasons for the recommendation and where possible to provide examples/evidence of the particular weakness or problem. This will be noted by the clinical tutor in his/her EPR notes. The clinical tutor will also offer the trainee the opportunity to comment on the rating; the trainee’s views will be recorded by the clinical tutor in his/her EPR notes.
The supervisor must indicate the failure or conditional pass recommendation on the Supervisor Evaluation of Clinical Competence form and make the reasons for the rating explicit, both via indicating the grounds for the rating and by providing examples/evidence to support the rating. The trainee must sign the supervisor evaluation form and indicate any points of disagreement.
Placement submissions (i.e. the Supervisor Evaluation of Clinical Competence form, the Log of Clinical Experience and Example of Clinical Work) should be handed in as usual to the Programme Administrator by the stated deadline, which is usually one week after the end of the placement.
Placement related submissions will then be reviewed by the clinical tutor (who is not blind the trainee’s identity) and the example of clinical work will also be assessed by another member of the programme team (who is blind to the trainee’s identity) as per the degree regulations.
In circumstances where the clinical tutor recommends a different outcome to that recommended by the supervisor, a second marker who is blind to the identity of the trainee and the supervisor will review the placement documents as well.
Placements evaluated as a fail, will be referred to the external examiner.
In the case of referrals to the External Examiner the clinical tutor will prepare a report on the trainee’s performance and any relevant placement or supervisory issues to be sent to the External Examiner.
If deemed necessary by the internal assessor or by the external examiner, the assessor(s) will meet with the supervisor and the trainee in order to acquire further evidence and information before reaching a final rating for the placement.
As per the degree regulations, provisional marks and the external examiner’s recommendation will be considered at the Progression Board of Examiners and either ratified or amended.
Appeals against the decision of the Progression Board of Examiners may be made in accordance with the University appeals procedure for progression outcomes prior to final Year 3 Major Research Project viva (Student Complaints UPR AS/G/6.1 refers).
Where an example of clinical work is failed:
The piece of work usually will be referred to the external examiner
As per the degree regulations, provisional marks and the external examiner’s recommendation will be considered at the Progression Board of Examiners and either ratified or amended.
Where the subject Progression of Examiners ratify a fail rating on the example of clinical work, then the placement will at best be given a conditional pass (assuming other aspects of the placement have been passed).
As suggested above, the trainee and the clinical tutor should already have been alerted to the problems by the
clinical supervisor. It is recommended that problems be highlighted as early as possible in the placement to
ensure that remedial action may be taken if possible.

26
The trainee will be required to resubmit an example meeting the same criteria within a specified time period. The re-submitted example will be re-marked, usually by the original two markers. In the event of the re-submitted example of clinical work being failed, the original placement will be deemed to have been failed. (Refer to the flowchart in Appendix 13).
As per the degree regulations, marks will be considered at the Progression Board of Examiners and either ratified or amended.
Appeals against the decision of the Progression Board of Examiners may be made in accordance with the University appeals procedure (UPR AS/G/6.1 refers).
Following a conditional pass on a placement, the Statement of Conditions form will be completed by the trainee’s clinical tutor (see Appendix 12). A copy of this form will be given to the trainee once s/he has been notified of the outcome of the placement. This form specifies the reasons for the conditional pass, the specific conditions to be met in order for the placement to be passed and details as to who will assess this. Where applicable a copy of the Statement of Conditions form will also be given to the supervisor who will be involved in supervising and assessing the specified areas of work. If the conditions are met to the satisfaction of the Progression Board of Examiners then the original placement will be deemed to have been passed. If the conditions are not met to the satisfaction of the Progression Board of Examiners, then the original placement will be deemed to have been failed.
Following a failed placement, a trainee may be required to repeat some of or the entire clinical placement. Only one placement may be repeated. A failure of a second placement will usually constitute a programme failure.

27
Appendices Appendix 1: BPS Committee on Training in Clinical Psychology
Guidelines on Clinical Supervision 28
Appendix 2: Protocol for Managing Clinical Psychology Trainees 33 Appendix 3: Professional Practise Guidelines on Teaching Training and Supervision 36 Appendix 4: Placement Contract 38 Appendix 5: Criteria for the Accreditation of Postgraduate Training Programmes in
Clinical Psychology 46 Appendix 6: Clinical Tutorial form 56 Appendix 7: Placement Review form 57
Appendix 8: Log of Clinical Experience 66 Appendix 9: Summary Log of Clinical Experience 75 Appendix 10: Supervisor Evaluation of Clinical Competence form 80 Appendix 11: Trainee Placement Feedback & Placement Audit forms 92 Appendix 12: Policy on Managing Difficulties on Placement 101 Appendix 13: Placement Marking Guidelines 103 Appendix 14: Trainee Guidelines: Examples of Clinical work 113 Appendix 15: Guidelines on Consent 129 Appendix 16: Trainee Guidelines: Clinical Case Reports 135

28
Appendix 1: BPS Committee on Training in Clinical Psychology - Guidelines on Clinical Supervision
THE BRITISH PSYCHOLOGICAL SOCIETY Membership and Qualifications Board
Committee on Training in Clinical Psychology Guidelines on Clinical Supervision Introduction The following guidelines set out the minimum standards necessary to achieve good practice in the supervision of clinical trainees. In practice it is often helpful to adapt these guidelines and customise them to the specific programme. It is important that these guidelines are read in conjunction with the criteria for accreditation. [reviewed by CTCP 2007] 1. Qualifications of supervisors 1.1 All trainees should normally be supervised by a clinical psychologist who has at least two years experience after being eligible for registration as a Chartered Psychologist in the National Health Service, or a designated individual of equivalent clinical experience. This includes a clinical psychologist with at least two years’ experience who has recently gained a Statement of Equivalence and eligibility for Chartered Status. More junior clinical psychologists, applied psychologists or an appropriately qualified and experienced member of another profession participating in team supervision, may be involved in supplementing this supervision in limited areas at the discretion of the Programme Director or Clinical Tutor. Where a trainee works in an educational, social services or other setting, it is preferable that supervision be provided by a clinical psychologist who has full service involvement in the setting concerned. Where this is not possible, day-to-day supervision may be provided by an experienced applied psychologist working on-site with formal supervision provided by a clinical psychologist as designated above. 1.2 In certain circumstances a Clinical Psychologist who has at least one year’s experience after gaining the qualification and experience for registration as a Chartered Clinical Psychologist and who has clinical responsibilities in the unit or service in which the work is carried out, may carry out the main supervision at the discretion of the Programme Director or Clinical Tutor. 2. Supervisors Workshops and Meetings 2.1 Programmes must organise regular supervision workshops to train supervisors in methods of supervision; these should be designed with the needs of new as well as experienced supervisors in mind. Supervisors are expected to attend workshops on supervision. There should also be regular meetings at which supervisors have an opportunity to share information and discuss problems. Where programmes make use of team supervision, viz. where the ratio of trainee to supervisor is other than 1:1, the Programme must ensure that appropriate guidance is given to supervisors and trainees on the procedures, which are necessary for good team supervision. It will probably be necessary to establish supervisor workshops related specifically to team supervision. 2.2 It is important that supervisors keep abreast of theoretical, research and professional developments in their fields of work and participate in continuing professional development. 3. Allocation to Clinical Placements 3.1 There should be an explicit procedure for allocating trainees to clinical placements. All trainees and supervisors involved should understand the procedure and know how to influence decisions about clinical placements. The person responsible for arranging placements should give primacy to general training requirements but should also take account of the needs

29
of individual trainees. Information should be provided about the experience obtainable in the various placements to help trainees and programme staff to make placement decisions. 3.2 The Programme should try to ensure effective co-working for trainees who are sharing the same placement. This is especially important where there is team supervision, with two trainees allocated to one supervisor, or when two or more trainees receive supervision from a team of supervisors, within the same placement. 4. Setting up the Placement 4.1 Both trainee(s) and supervisor(s) must have an opportunity to meet either before, or at the very beginning of the placement to discuss the range of experience, which is to be provided, and the expectations (hours, days of work, etc) of the trainee(s). The general aims of the placement should normally be agreed within the first two weeks of the placement and a clinical contract should be written. Attention must be paid in the clinical contract to the range of opportunities available in the placement, and to the needs, interests and previous experience of the trainee. Particular efforts should be made to fill major gaps in the trainee’s experience, and records of the trainee’s previous experience should be available for this purpose. The Programme Director or Clinical Tutor will have played a major role in the assessment of the trainee’s strengths and needs and in the sequence of placements. 4.2 In cases where there is more than one supervisor involved in a trainee’s placement (team supervision) a primary supervisor must be identified for each trainee who will take responsibility for the planning and co-ordination of that trainee's placement, supervision and assessment, and for liaison with Programme staff. 4.3 The supervisor must plan an induction for the trainee, arrange for cover in the event of annual or other leave and should plan casework well in advance. 4.4 Care should be taken to ensure that the trainee has access to (at least) shared office space, telephone and a desk. There must be adequate arrangements for secretarial and IT support for placement work and trainees must be given guidance on the facilities available. 4.5 Supervisors must remember that they have clinical and legal responsibilities for their trainees throughout the training period. It is good practice for supervisors to be insured, for trainees to be aware of relevant legal boundaries (e.g. re. the Data Protection Act, the Children Act). It is essential that trainees have appropriate (substantive or honorary) contracts that allow them to work in their placement. 5. Placement Content 5.1 Programme training committees must develop, in consultation with the Division of Clinical Psychology’s Faculties and Special Interest Groups and local supervisors, guidelines on the required experience in clinical placements, recommending an appropriate amount of clinical work. In doing this, reference should also be made to section B of the CTCP Criteria for the Accreditation of Postgraduate Training Programmes in Clinical Psychology. 5.2 The local guidelines on placement content should be taken into account in the provision of placement experience for the trainee. The level of his/her experience and expertise and the stage of training will determine the particular balance of work for each individual trainee. 5.3 Supervisors should ensure that trainees undertake an appropriate quantity of clinical work. There are dangers in both extremes: too little work reduces the opportunity for learning and too much may reduce trainees' capacity for planning or reflecting upon the work. Supervisors should monitor the balance of time spent by the trainee on work at different levels (direct client work, indirect and organisational work). This balance will vary according to the stage of training and the type of placement. Supervisors should be alert to the dangers of time being lost at the start of the placement through suitable work not being available and should take this into account in preparing for the arrival of the trainee.

30
5.4 A log must be kept of the work a trainee has done in a clinical placement. The Programme must ensure that the Clinical Tutor appropriately uses these records in planning future placements and by future clinical supervisors in discussing what experience they should provide. 5.5 With team supervision, the Programme should give clear guidelines about the experience to be acquired so that the placement may be planned to make optimal use of others, such as other applied psychologists, involved in supervision. 6. Clinical Supervision 6.1 There must be a formal, scheduled supervision meeting each week that must be of at least an hour's duration. Longer supervision will sometimes be needed, especially where team or group supervision is used. In addition, supervisors should try to make themselves available for informal discussion of matters that arise between formal supervision sessions. The total contact between the trainee(s) and supervisor(s) must be at least three hours a week, and will need to be considerably longer than this time at the beginning of training. 6.2 In cases of team or group supervision, trainees must always receive, in addition, an appropriate amount of individual supervision. Individual supervision must provide opportunities to discuss personal issues, professional development, overall workload and organisational difficulties as well as on-going casework. 6.3 Adequate time for clinically relevant reading must be made available to the trainee on placement. In addition, supervisors have a crucial role in contributing to the integration of the academic and practical aspects of the Programme. They should discuss literature relevant to the clinical work in hand and suggest suitable reading to the trainee. In general they should help trainees to develop a scholarly and critical approach to their clinical work. 6.4 In addition to discussing clinical work, it is essential that the trainees and supervisors have opportunities to observe each other at work: the trainee can learn much more from this and it is essential in order for the supervisor to give the trainee accurate and constructive feedback. Placements differ in the most appropriate opportunities for such direct contact: some may use joint clinical work of some kind; others may prefer audiotape, videotape or a one-way screen. Some form of mutual observation of clinical work is regarded as essential. 7. Quality of Clinical Supervision 7.1 The quality of the supervision that is provided for the trainee will depend upon many factors. The care taken in the early stages to build up a good relationship will enhance the quality of the clinical supervision. 7.2 Supervisors should be prepared to adapt their style of supervision to the stage of the programme a trainee has reached. It is necessary to be prepared to describe basic clinical procedures in detail and to ensure that trainees have an adequate grasp of techniques they are asked to use. Detailed training in techniques should also be available too more experienced trainees if required. 7.3 Trainees and supervisors may find that they have a different orientation and interests. Where this happens tolerance should be shown on both sides. Trainees should be helped to see that they might learn much that is valuable from a supervisor whose approach they may not ultimately wish to adopt. On the other hand, supervisors should see it as one of their functions to help trainees develop their own interests in an appropriate way. Where supervisors decide they must overrule the way the trainee wishes to work, they should explain their reasons with care, rather than simply asserting that this is how things should be done. 7.4 Supervisors should be prepared to discuss seriously and sympathetically any general issues of relationships with patients or staff that arise in the programme of clinical work. They should be sensitive to any personal issues that arise for the trainees in relation to clients and be prepared to discuss these in a supportive way when they are considered to affect the trainee’s work. The range of personal issues that can be raised by clinical work is wide and includes, for example, over-involvement, dealing with anger and despair, workload and time management problems.

31
8. Clinical Reports and Communication 8.1 Communication with other members of clinical teams and networks involves both written and verbal reports. Verbal reporting and discussion are often more important than formal written reports in terms of their effects on clinical decisions and action. Since the relative importance of written and oral communication is likely to vary between settings, supervisors will need to identify the most important channels of communication in their placement and teach the trainee to use these channels effectively and efficiently. Training in effective communication will involve both observation of the supervisor’s behaviour, and practice by the trainee with ample opportunity for feedback. 8.2 There is a wide variation within the profession in how clinical reports are written and presented, particularly with respect to the amount of detailed information provided. Trainees need to be acquainted with a variety of report and letter writing styles. If there is agreement about minimal requirements of clarity and relevance in reports, exposure to individual differences between supervisors is more likely to be constructive than confusing. Trainees should be encouraged to write reports that are appropriate to the recipient (whether this is a professional colleague or a client), avoid jargon, distinguish clearly between fact and opinion, and provide consistent clarity of expression. Both supervisor and trainee should be aware of the potential conflict between communicating fully to professional colleagues and maintaining confidentiality. 9. Review Meetings and Feedback 9.1 There must be a formal process during each placement whereby the Programme team monitors the clinical experience of trainees and the supervision provided, and helps to resolve any problems that may have arisen. The aims of this are: a) to review the progress of the clinical Contract b) to give feedback to the trainee on his/her clinical performance c) to allow the trainee to comment on the adequacy of the placement d) to set targets based upon the above for the remainder of the placement e) to give feedback to the supervisor on his/her performance. 9.2 When a trainee is involved with some form of team supervision, the Programme must ensure that each trainee’s experience is monitored on an individual basis. Other review or feedback of meetings that may be held at the beginning and end of a placement should also allow for individual time allocation for each trainee. If possible, all team supervisors involved with any single trainee should be involved in the monitoring process (and beginning and end of placement meetings). Where it is not possible for all a trainee's supervisors to be present at a key review meeting, one designated supervisor should seek views from other team supervisors prior to the meeting, and provide feedback after the meeting. 9.3 Matters such as the physical resources available to the trainee (room space, secretarial backup, etc) and theory-practice links (see 6.3) may also be usefully discussed at this time. Supervisors and trainees may find it helpful the review to go through the rating forms that will be used at the end of the placement. 9.4 In general, it is expected that the Programme staff member conducting the monitoring will hold discussions with the trainee and supervisor separately and then hold a joint discussion. In this way more accurate feedback about the trainee’s performance and about the quality of the supervision provided may be obtained. The timing of the monitoring is important if sufficient time is to be left for improvements to be made. A plan and timetable for the review should be agreed at the start of the placement. 9.5 Mid placement qualitative feedback is essential both for the supervisor and the trainee. Supervisors should try to set aside positive or negative personal feelings about trainees when making evaluations. Feedback should be detailed and constructive and designed to help trainees develop a range of effective and appropriate skills; thus, feedback should be critical but not wholly negative.

32
9.6 If seriously dissatisfied about aspects of a trainee's performance, supervisors should regard themselves as under an obligation to the profession to indicate this to the Programme staff. 9.7 The trainee also has a responsibility to the Programme and to the profession to give feedback to the Programme staff about the quality of the placement and the supervision. 9.8 At the end of the placement the supervisor must give the trainee full feedback on his/her clinical performance. The trainee must see the supervisor's written assessment. Any major points that the supervisor is concerned about should have been raised well beforehand, at least during the formal monitoring process, to allow the trainee time to improve. The trainee must also have ample opportunity to comment on the placement, for example, on the experience and the supervision received. The trainee's views should be recorded formally as part of the general evaluation of the placement. Feedback forms and forms for rating clinical competence should always be completed at the time of the end of placement review and returned promptly. 9.9 The points made in section 9.5 concerning the provision of balanced, constructive and detailed feedback to the trainee also apply to the end of placement review. The supervisor should, in addition, help the trainee to identify gaps in his/her experience to facilitate planning for subsequent placements. It is important for the supervisor and trainee to forward this information to the person responsible for co-ordinating placements. 10. Assessment of Clinical Competence 10.1 It is important that Supervisors are familiar with the examination and continuous assessment requirements for trainees and the guidelines and regulations for these. 10.2 In cases of team supervision, all supervisors who have been involved with the trainee(s) must be familiar with the Programme's assessment procedure and must give feedback on the trainee(s) clinical competence. 10.3 Supervisors must be familiar with the specific criteria for passing and failing in the assessment of clinical competence set by the Programme. In addition, supervisors should be aware of appeals procedures. In cases where trainees have displayed unsatisfactory behaviour, such as regular and serious lateness for clinical appointments, professional misconduct, or failure to acquire an adequate level of clinical competence, trainees must be left in no doubt about the problem. The supervisors should discuss with the Clinical Tutor what action should be taken and it may be helpful to have a member of the Programme staff present at the time of the end of placement review. Revised November 2002

33
Appendix 2: Protocol for Managing Clinical Psychology Trainees
Lifespan Healthcare NHS Trust*
Introduction
This protocol sets out the legal requirements for employers and others responsible for the Clinical Psychology Trainees during their training and in particular their placements. It also provides a code of good practice in which the Trust, all Placement trusts and others responsible for the welfare of the Trainees and the respective Trainees are expected to operate.
Policies and Procedures
The Clinical Supervisors will ensure that Trainees have access to copies of all policies and procedures which apply to them whilst located in the Placement trust and ensure that the Trainees receive an induction into each Placement trust.
Such policies include those specifically referred to in this protocol and any other policies which apply to any individuals working or training on the Placement trust’s premises such as the Placement trust’s Fire regulations.
Grievance and disciplinary Matters
Any misconduct or poor performance of Trainees should be reported by the Placement trust to the relevant University Tutor. Serious misconduct may result in the Trainee’s placement being terminated. In cases of alleged serious misconduct there may be a requirement for the Trainees to leave the Placement trust premises pending an investigation. On any issues concerning academic or University rules the University will deal with it using its procedures. On issues concerning conduct whilst in a Placement trust, or other employment related issues the Trust’s policy should be used. The Trust’s Human Resources Department must be made aware of any disciplinary issues. During the course of the placement Trainees will be exposed to confidential information concerning patients and staff. Such information must not be disclosed to any unauthorised person except to ensure adequate completion of assignments and project work. Unauthorised disclosure is considered a disciplinary issue. Any grievance by Trainees must be referred to the relevant University Tutor, who will investigate as appropriate. The Trust’s grievance policy and the University’s appeals procedure and grievance policy will be used as appropriate.
*Lifespan HealthCare is the employing NHS trust. It is referred to as the Trust thought this document.
The trusts where the trainee is on placement is referred to as the Placement trust.
Health and Safety
The Placement trust has an obligation under the Health & Safety at Work Act 1974 to provide safe and healthy working conditions and methods. All staff and Trainees involved in practice placements should co-operate with the management of the Placement trust in discharging its responsibilities under the Act; and take reasonable care for Health and Safety of themselves and others. Trainees specifically have a responsibility to work in a safe manner at all times. The
Since this document was drawn up, Lifespan Healthcare Trust has been subsumed under the Cambridgeshire and
Peterborough Mental Health Partnership Trust

34
Placement trust will ensure that staff and Trainees are aware of their responsibility to behave in a manner that does not cause the possibility of injury to themselves or others.
Absence Reporting
If for any reason, for example sickness, Trainees are unable to attend their placement they should advise the University and their Clinical Supervisor in line with the practice of both the Placement trust and the University rules. The relevant University Tutor will inform the Trust payroll of any absence. If a trainee is still on sick absence after 3 calendar days they should complete a self-certificate form, this can be obtained from the Trusts payroll department. If they remain sick after 7 days, they must provide a medical certificate.
Reporting and Investigation of Incidents
Trainees are required to assist the Placement trust’s management in the investigation of any untoward incidents as required.
Professional Conduct
Trainees are required to conduct themselves in a manner appropriate to the Placement trust in which they are placed. They should at all times adhere to the University’s Regulations Governing Studies involving the use of Human Subjects and the British Psychological Society’s Professional Practice and Ethical Guidelines. The University will ensure that the Trainees have an understanding of the code of conduct expected in dealing with communication with patients and visitors. Clinical supervisors will make Trainees aware of the standards of conduct and appearance expected within the department and the reason for those standards for example, time keeping, communications and safety. Trainees must also be aware that the Placement trust or Trust does not accept responsibility for personal property lost or damaged on its premises and recommend that these are insured by the owner. The University and the Trust will ensure that the Trainees are equipped with personal identification and that this is available for inspection when on the Placements trust’s premises. Placement trust may supplement this by their own identification badge.
Quality Standards
The University and the Placement trusts will ensure that the quality of practice placements is maintained in accordance with the accreditation criteria and guidelines of the British Psychological Society and will co-operate with collaborative education audits of placements. The Placement trust will ensure that adequate supervision and safe systems are provided to ensure that the Trainee is not placed in position of risk to patients or to themselves.
Objectives of the placement, monitoring and feedback
The university will ensure that the Trainee is aware of the learning objectives of each placement. Both the University and the Placement trust will contribute to the identification and achievement of the learning outcomes for each placement. The Placement trusts will allow free access by the University’s in order that the Trainee’s progress can be monitored. Course staff will respect the confidentiality of information in relation to patients and their families.

35
The placement trust will provide feedback to the University’s on the outcome of the placement in accordance with evaluation requirements. The University will provide feedback to the Placement trust on the quality of the placement. The Placement trust shall be responsible for providing appropriate qualified Clinical Supervisors to all Trainees who will fulfil all of their obligations to the Trainees, including in respect of Trainee’s assessment.
Library Facilities and Resources
The Placement trust will provide reasonable access to its own library services for Trainees on placement, during the normal operating times of the organisation’s library. The Placement trust will provide the Trainees with all other resources, facilities and space as reasonably required by the Trainees in order that they may carry out their jobs.
Reporting Arrangements
Following Liaison with the Placement trust Clinical Supervisor the University will advise Trainees of their professional reporting arrangements.
36
Appendix 3: Professional Practice Guidelines on Teaching, Training and Supervision
Professional Practice Guidelines on Teaching, Training and Supervision
Division of Clinical Psychology, 1995, p42-45. There is an expectation that all psychologists will be actively involved in transmitting skills and expertise to others. This included providing training and supervision to both trainees and assistant psychologists and to members of others professions. There will also be situations in which this is provided to carers, voluntary organisations and other non-psychologists. The practice of clinical psychology is changing and developing rapidly. In recognition of this, psychologists are expected to take corporate responsibility for keeping themselves up-to-date. Clinical Psychologists: basic training The training process carries mutual professional responsibilities for Courses trainees and qualified clinical psychologist, and depends upon effective, collaborative relationships between them. Principles 1. Tutors, teachers and supervisors should adhere to CTCP procedures and guidelines. 2. Supervisors and academic tutors must ensure that trainees have a copy of the Guidelines for the Professional Practice of Clinical Psychology and are aware of their duty to abide by these Guidelines. The organisers of training course should ensure that their syllabus includes teaching which addresses the range of ethical issues and good practice recommendations therein. Supervisors should take every available opportunity to relate the Guidelines to trainees’ routine clinical experience on placement. 3. Supervisors and tutors must be aware of the importance of boundary and power issues within their supervisory and teaching relationship. Dual personal and supervisory or teaching relationships should be avoided, so that any potential abuse of power is minimised and the teaching role is not compromised. Should such a relationship exist, the supervisor or teacher must withdraw from any professional responsibility towards the trainee. Supervisors who are also teachers must not exploit the trainee’s vulnerability in being dependent on reports of competence, or exploit the relationship of trust for improper personal or financial gain. In this respect, the principles described within the Personal Conduct section apply just as much to relationships with trainees as they do to relationships with clients. 4. Trainees and supervisors or teachers should be free to pursue their professional and academic activities without any kind of overt or covert sexual harassment. Supervisors and teachers have a duty to maintain workplaces free from such harassment and intimidation and should endeavour to ensure that satisfactory procedures for complaint are available. Any form of sexual advance or quest for sexual favours by supervisors, trainers or teachers engaged in a professional relationship with trainees is unacceptable. Trainees should be informed that agreed procedures for complaint exist within the BPS, and be made aware of local procedures within universities and NHS Trusts and other health providers. 5. Supervisors should make clear to trainees that as trainees they are individually responsible for their conduct with clients, and the extent to which responsibility for clinical work is shared with the supervisor. 6. Although trainees may be concerned at doing so, they should inform clients of their training status and that they will be discussing information about them with their supervisor, in confidence, and that information about them may be used anonymously in case reports for examination purposes only. Trainees and supervisors should consider the best way to raising this issue with potential clients, perhaps by discussing with them advantages and disadvantages of being seen by a trainee. Training courses should establish guidelines in this respect.

37
7. Supervisors and trainees must ensure that the trainees’ work does not exceed their competence, whilst enabling new learning to take place at an appropriate pace. This will involve adequate prior discussion and preparation before new strategies are employed, and sufficient time for review and revision. If the clinical needs of a client exceed the competence of a trainee, the supervisor must consider whether to take over the client themselves or refer elsewhere. This will need to be balanced against the intensity of supervision which can be provided, the potential for the trainees to develop, the value of the current therapy relationship to the client and the consequences of ending the current therapy. 8. The accurate monitoring of competence needs to include some level of observation, either by direct observation (e.g. one-way screen, sitting in, joint work) or indirect observation (e.g. video or audio tape recording). This is best done at more than one time point during a placement, and should involve both assessment and intervention sessions. Trainees and supervisors need to develop strategies to facilitate the constructive use of observation, and to desensitise all parties involved. The requirements of confidentiality, will apply to audio and video recording. 9. When using case material in teaching sessions teachers must adhere to confidentiality and ensure that material does not allow clients to be identified. 10. When writing up client details for their case studies, trainee must ensure that they do no include information that would enable their clients to be identified by those reading the studies. Specifically, client names should be altered or not used and the names of all health care professionals involved with the client should be removed, as should details of location. Course organisers must ensure that all case studies are held in a secure place which prohibits access by other professionals or the public, and that materials for examination are posted using as secure means as possible. 11. Effective teaching and learning is the mutual responsibility of both parties, supervisors or teachers and trainees. This involves active participation in both supervision and teaching sessions. 12. Supervisors and trainees should respect each others’ perspectives, particularly where these involve differences of opinion and preferred practice, which may relate to cultural factors. Trainees should be guided by a supervisor’s advice, be prepared to test out interventions and cease a specific course of action if instructed to do so. Supervisors should respect the trainees’ right to develop an individual orientation to their work. Trainees have a right to refuse to undertake certain actions on ethical or other legitimate grounds. In the case of disagreement, a third party may be consulted as arbiter. 13. Supervisors should act within their competence, and should arrange for additional supervision from another psychologist if the needs of supervision exceed their current abilities. Psychologists should resist pressures or temptations to supervise before they have two years’ post-qualification experience after becoming eligible for Chartered status. They should attend relevant workshops on supervision before undertaking supervision. 14. Supervisors should make assessments of trainees’ competence that are not influenced by personal differences, including those relating to race and culture. They will provide constructive, accurate and impartial feedback on trainees’ performance, which takes account of the possible distress which feedback may cause. Difficulties should be dealt with as they arise, with sensitivity and objectivity. 15. Supervisors, tutors and trainees should recognise the importance of personal development and its relation to professional development. All parties need to be open to recognising personal issues which interact with clinical work, and the value of understanding that interaction. Supervisors and tutors should help trainees to identify such issues. If personal therapy would be useful, they should facilitate trainee access to a suitable therapist rather than take on that role themselves.

38
Appendix 4: Placement Contract
University of Hertfordshire
Doctorate in Clinical Psychology
Placement Contract
Trainee
Supervisor
Placement
Placement Dates
Placement number
1 2 3 4 5 6
Location
Placement supervisors are responsible for drawing up a placement contract with the trainee, at the outset of the placement. The purpose of this contract is to set out the goals for the placement and to document explicitly the work the trainee will undertake. The contract provides a benchmark for monitoring the quality of the placement and the trainee’s performance. Feedback forms and records of the trainee’s actual experience will be compared with the placement contract during and at the end of the placement. This should alert trainee, supervisor and course team to any gaps and discrepancies between planned and actual experience and competencies. Opportunities will then be made to address these. When you draw up the contract you will need to consider the essential experience and core
competencies detailed in the placement guidelines, the trainee’s prior experience and specific training needs, and the opportunities available in the specific placement. You may also choose to refer to the information provided from the previous placement on the Placement Continuation form. You may wish to draft some aspects of the contract as a part of your pre-placement planning, however the bulk of the contract should be drawn up in conjunction with the trainee. This document should be used as a skeleton contract. Additional information may be added where appropriate A copy of the placement contract must be given to the trainee’s clinical tutor within the first two weeks of the trainee commencing the placement prior to the clinical tutorial where the contract will be reviewed with the tutor. Signed copies of the final version of the contract should be kept by both the trainee and the supervisor and an electronic copy of the final version should be sent to the clinical tutor to be kept on record. The placement contract should also be brought to the mid- and end-of-placement reviews by the trainee for reference purposes.
The placement guidelines are integrated into Section 3 of the Supervisor Handbook and
Section 6.2 of the Course Handbook.

39
Practical Arrangements: (This information must be negotiated between trainee and supervisor)
Start date
Date for mid-placement review
Date for end of placement review
End date
Planned annual leave dates
Planned attendance of conferences/courses?
Weekly Timetable: (Some of this information will be provided by the trainee. Please include study/ research time, days at university, days on placement and location.)
Monday Tuesday Wednesday Thursday Friday
AM
PM
List regular meetings to be attended:

40
Supervision Arrangements:
Day and time for regular supervision
Arrangements for contacting supervisor in the event of a difficulty arising in between scheduled supervision times
Arrangements for co-supervision (if applicable)
Arrangements for supervisor absence (e.g. during periods of annual leave)
Methods of learning available: (Tick the methods of learning available to the trainee on this placement)
Trainee observation of supervisor
Supervisor observation of trainee
Joint clinical work
Joint attendance of meetings, reviews etc.
Audio recording of clinical work & review/ discussion in supervision
Video recording of clinical work & review/discussion in supervision
Participation in live supervision (e.g. family therapy screen team)
Library / books / information resources
In supervision:
Discussion /review /
Feedback & constructive challenge
Reflection
Instruction / teaching / advice/ guidance
Demonstration/modelling/role play
Others:

41
Plans for Induction : (Please provide details of plans for the trainee’s induction. Refer to the guidance on Induction in the Supervisor Handbook, Section 2.9)

42
Strengths and weaknesses: (Please note any perceived strengths and weaknesses of trainee, supervisor and placement that should be considered in planning this placement.)
Of the Trainee Of the Supervisor Of the Placement
Strengths:
Weaknesses:
Specific training needs: (This should be based on a consideration of specific competencies that need to be developed as well as experiences which need to be acquired. Refer to the Placement Continuation form from the trainee’s previous placement).

43
Range of Experience (Refer to Section 6.2.1 of the Course Handbook or Section 3.1 of the Supervisor Handbook)
Client Range: (Age range? Ethnicity/culture? Intellectual functioning? Carers and families?)
Problem range: (acute/enduring? Mild/severe? Functional/organic? Adjustment? )
Settings / Service Delivery systems: (Inpatient/residential? Outpatient? Primary/secondary/tertiary care settings?)
Modes & Types of work: (Direct interventions? Indirect interventions with staff and carers? Work within MDTs? Models of psychological therapy?)

44
Learning Goals (Refer to Section 6.2.2 of the Course Handbook or Section 3.2 of the Supervisor Handbook)
Personal & Professional Skills: (Please identify goals. Specify the activities to be undertaken in order to meet the goals. Include goals relating to: professional behaviour, ethics, awareness of issues of power and diversity, managing priorities and own learning needs, understanding and use of supervision, self reflection and self-care)
Knowledge & Critical thinking skills: (Please identify any goals relating to: knowledge of psychological theory & techniques, knowledge, skills and understanding to identify and critically appraise research evidence relevant to practice.)
Psychological Assessment Skills: (Please identify goals relating to assessment skills. Specify the activities to be undertaken in order to meet the goals. Include goals relating to: assessment methods and specific procedures to be learned e.g. clinical interviewing, behavioural observation, specific psychometric tests, risk assessment etc.)
Models and Psychological Formulation: (Please identify goals. Detail specific activities to be undertaken in order to meet the goals. Include goals relating to models to be learned, development of formulation skills, use of formulation to inform treatment, use of formulation with clients and colleagues etc.)
Intervention skills: (Please identify goals. Specify the activities to be undertaken in order to meet the goals. Include details of theories, methods and techniques to be used and learned for both direct therapies and indirect interventions)
Monitoring & Evaluation: (Please identify goals and specify activities to be undertaken. Include goals relating to monitoring of client progress, outcome evaluation and skills in choosing methods appropriate to client, context, theory etc.)
Multidisciplinary Team Work & Consultancy (Please identify goals and specify activities to be undertaken to meet these goals. Include goals relating to MDT work, understanding inter-professional roles and consultation.)

45
Communication, reporting & Teaching: (Please identify goals. Specify the activities to be undertaken in order to meet the goals. Include goals relating to verbal and written communication, teaching, presentations etc.)
Service Delivery & Understanding the organisation and the context: (Please identify goals. Specify the activities to be undertaken in order to meet the goals. Include goals relating to the local organisation e.g. understanding local referral networks, the voluntary sector, user involvement etc. and goals relating to broader areas of policy and service context e.g. NHS policy, national legislation etc.)
Research, audit and evaluation: (Identify goals for service-based research and/or outcome evaluation, if applicable, and document the specific activities this will entail)
Plans for visits: (Note plans for trainee visits to other agencies, services or teams)
Other Relevant Information: Supervisor: Signed: Date: Trainee: Signed: Date:

46
Appendix 5: Criteria for the Accreditation of Postgraduate Training Programmes in Clinical Psychology
Accreditation Criteria Extract from: Committee on Training in Clinical Psychology Criteria for the Accreditation of Post-graduate Training Programmes in Clinical Psychology (September 2007 revision)
What do clinical psychologists do? Clinical psychologists aim to reduce psychological distress and to enhance and promote psychological well-being by the systematic application of knowledge derived from psychological theory and research. Clinical psychology services aim to enable service users to have the necessary skills and abilities to cope with their emotional needs and daily lives in order to maximise psychological and physical well-being; to develop and use their capacity to make informed choices in order to enhance and maximise independence and autonomy; to have a sense of self-understanding, self-respect and self worth; to be able to enjoy good social and personal relationships; and to access commonly valued social and environmental facilities. Clinical psychology services aim to enable other service providers to develop psychologically informed ways of thinking; to use psychological knowledge to enhance and develop their professional practice to the benefit of their clients; to be able to enhance their sense of self-understanding, self-respect and self-worth; and to use psychological data to aid decision-making at a clinical, organisational and societal level. Clinical psychologists also work with staff from other professional groups, including psychological therapists, to develop, monitor and improve practice, basing this on a breadth and depth of understanding of relevant psychological theory, and on the psychologist’s evaluative and reflective competencies. Clinical psychologists as scientist practitioners Clinical psychologists are more than psychological therapists. While many do practise psychotherapy at a high level, this is not a skill distinct to clinical psychologists, nor should it be. The background and training of clinical psychologists is rooted in the science of psychology, and clinical psychology is one of the applications of psychological science to help address human problems. The ability to design and carry out innovative applied research is a skill developed to doctoral level in training and is important for the development and delivery of evidence-based practice. In addition, one element of research competence is critical evaluation of research activity. While there are data that support many clinical activities, there are still major gaps in the knowledge base. One of the contributions made by clinical psychologists is the development and testing of new interventions and activities, based on psychological theory. Thus practice feeds and draws on research and theory that in turn influences practice. Clinical psychologists as reflective practitioners Clinical psychologists are cognisant of the importance of self-awareness and the need to appraise and reflect on their own practice. They are also aware of the importance of diversity, the social and cultural context of their work, working within an ethical framework, and the need for continuing professional and personal development. Use of clinical psychology services

47
Clinical psychologists work with individuals, couples, families, groups (therapeutic, staff, informal carers) and at the organisational and community level. They work in a variety of settings, including hospital wards, day centres, Community Mental Health Teams, NHS Trusts, primary and social care contexts and forensic settings, and with all age groups from very young children to older people. 9 They work with people with mild, moderate and severe mental health problems, developmental and learning disabilities, physical and sensory disability, and brain injury; people who have substance misuse problems and people with a range of physical health problems (including HIV and AIDS, cancer, heart disease, pain, diabetes). Required capabilities and competencies This section of the document has explained what clinical psychologists do, or in other words, the capabilities they demonstrate by using and applying their competencies and knowledge base. The statements in section 1.1 set out the skills, knowledge and values trainee clinical psychologists need to develop during the course of their training, and, in section 1.2, the learning outcomes that training programmes will need to have in order to enable trainees to achieve these goals. The competencies that clinical psychologists need in order to be able to work in the ways described are outlined in further detail in section 1.3. Section 2 provides additional information on the knowledge base clinical psychologists draw on in their practice.
1. The required learning outcomes 1.1. Programmes must enable trainees to work as clinical psychologists with the range of
clients and services specified below in a range of settings, especially those seen as having high priority within the National Health Service. Newly qualified clinical psychologists should understand and embrace the core purpose and philosophy of the profession as described in the document prepared by the Division of Clinical Psychology (DCP). They should be committed to reducing psychological distress and enhancing and promoting psychological well-being through the systematic application of knowledge derived from psychological theory and evidence. Their work will be based on the fundamental acknowledgement that all people have the same human value and the right to be treated as unique individuals. Programmes that meet these criteria will be considered to appropriately reflect current NHS policies such as The Ten Essential Shared Capabilities (See Appendix 1 for a list of current publications that complement these criteria, and Appendix 2 for further information on The Ten Essential Shared Capabilities). Thus by the end of their programme, trainees will have:
1.1.1. The skills, knowledge and values to develop working alliances with clients,
including individuals, carers and/or services, in order to carry out psychological assessment, develop a formulation based on psychological theories and knowledge, carry out psychological interventions, evaluate their work and communicate effectively with clients, referrers and others, orally, electronically and in writing;
1.1.2. The skills, knowledge and values to work effectively with clients from a diverse
range of backgrounds, understanding and respecting the impact of difference and diversity upon their lives;
1.1.3. The skills, knowledge and values to work effectively with systems relevant to
clients, including for example statutory and voluntary services, self-help and

48
advocacy groups, user-led systems and other elements of the wider community;
1.1.4. The skills, knowledge and values to work in a range of indirect ways to
improve psychological aspects of health and healthcare;
1.1.5. The skills, knowledge and values to conduct research that enables the profession to develop its knowledge base and to monitor and improve the effectiveness of its work; and
1.1.6. High level skills in managing a personal learning agenda and self-care, and in
critical reflection and self-awareness that enable transfer of knowledge and skills to new settings and problems.
1.2. In order to achieve these goals Programmes will have the following learning
outcomes.
1.2.1. Knowledge and understanding of psychological theory and evidence, encompassing specialist client group knowledge across the profession of Clinical Psychology and the knowledge required to underpin clinical and research practice.
1.2.2. A professional and ethical value base, including that set out in the BPS Code
of Ethics and Conduct, the DCP statement of the Core Purpose and Philosophy of the profession and the DCP Professional Practice Guidelines.
1.2.3. Clinical and research skills that demonstrate work with clients and systems
based on a scientist-practitioner and reflective-practitioner model that incorporates a cycle of assessment, formulation, intervention and evaluation.
1.2.4. Professional competence relating to personal and professional development
and awareness of the clinical, professional and social context within which the work is undertaken.
1.3. The following statements are intended as broad, high-level summaries of the
required objectives that demonstrate competence.
1.3.1. Transferable skills
Deciding, using a broad evidence and knowledge base, how to assess, formulate and intervene psychologically, from a range of possible models and modes of intervention with clients, carers and service systems.
Generalising and synthesising prior knowledge and experience in order to apply them critically and creatively in different settings and novel situations.
Demonstrating self-awareness and sensitivity, and working as a reflective practitioner.
Ability to think critically, reflectively and evaluatively.
Making informed judgements on complex issues in specialist fields, often in the absence of complete information.

49
Ability to communicate psychologically-informed ideas and conclusions clearly and effectively to specialist and non-specialist audiences, in order to facilitate problem solving and decision making.
Exercising personal responsibility and largely autonomous initiative in complex and unpredictable situations in professional practice.
Drawing on psychological knowledge of complex developmental, social and neuropsychological processes across the lifespan to facilitate adaptability and change in individuals, groups, families, organisations and communities.
Ability to work effectively whilst holding in mind alternative, competing explanations.
1.3.2. Psychological Assessment
Developing and maintaining effective working alliances with clients, including individuals, carers and services.
Ability to choose, use and interpret a broad range of assessment methods appropriate: - to the client and service delivery system in which the assessment takes place - to the type of intervention which is likely to be required
Assessment procedures in which competence is demonstrated will include:
- formal procedures (use of standardised psychometric instruments) - systematic interviewing procedures - other structured methods of assessment (e.g. observation, or gathering information from others); and - assessment of social context and organisations.
Conducting appropriate risk assessment and using this to guide practice.
1.3.3. Psychological Formulation
Developing formulations of presenting problems or situations which integrate information from assessments within a coherent framework that draws upon psychological theory and evidence and which incorporates interpersonal, societal, cultural and biological factors.
Using formulations with clients to facilitate their understanding of their experience.
Using formulations to plan appropriate interventions that take the client’s perspective into account.
Using formulations to assist multi-professional communication, and the understanding of clients and their care.
Revising formulations in the light of ongoing intervention and when necessary reformulating the problem.

50
1.3.4. Psychological Intervention
On the basis of a formulation, implementing psychological therapy or other interventions appropriate to the presenting problem and to the psychological and social circumstances of the client(s), and to do this in a collaborative manner with:
- individuals - couples, families or groups - services/organisations
Understanding therapeutic techniques and processes as applied when working with a range of different individuals in distress, including those who experience difficulties related to: anxiety, mood, adjustment to adverse circumstances or life events, eating, psychosis and use of substances, and those with somatoform, psychosexual, developmental, personality, cognitive and neurological presentations.
Ability to integrate and implement therapeutic interventions based on knowledge and practice in at least two evidence-based models of formal psychological therapy. This must include cognitive-behaviour therapy and at least one other evidence-based approach, such as brief psychodynamic or interpersonal psychotherapy, systemic, or integrative interventions.
Having an awareness of the impact of psychopharmacological and other clinical interventions.
Understanding social approaches to intervention; for example, those informed by community, critical, and social constructionist perspectives. Implementing interventions and care plans through and with other professions and/or with individuals who are formal (professional) carers for a client, or who care for a client by virtue of family or partnership arrangements.
Recognising when (further) intervention is inappropriate, or unlikely to be helpful, and communicating this sensitively to clients and carers.
1.3.5. Evaluation
Selecting and implementing appropriate methods to evaluate the effectiveness, acceptability and broader impact of interventions (both individual and organisational), and using this information to inform and shape practice.
Where appropriate this will also involve devising innovative procedures.
Auditing clinical effectiveness.
1.3.6. Research
Identifying, reviewing and critically appraising a substantial body of research evidence which is at the forefront of clinical psychology practice.
Understanding applicable techniques for clinical research and advanced academic enquiry, including quantitative and qualitative approaches.

51
Conducting service evaluation and small N research.
Conducting collaborative research.
Conceptualising, designing and conducting independent, original research of a quality to satisfy peer review, extend the forefront of the discipline, and merit publication: including identifying research questions, demonstrating an understanding of ethical issues, choosing appropriate research methods and analysis, reporting outcomes and identifying appropriate pathways for dissemination.
Understanding the need and value of undertaking clinical research and development post-qualification, contributing substantially to the development of theory and practice in clinical psychology.
1.3.7. Personal and Professional Skills and Values
Understanding of ethical issues and applying these in complex clinical contexts, ensuring that informed consent underpins all contact with clients and research participants.
Appreciating the inherent power imbalance between practitioners and clients and how abuse of this can be minimised.
Understanding the impact of differences, diversity and social inequalities on people’s lives, and their implications for working practices.
Understanding the impact of one’s own value base upon clinical practice.
Working effectively at an appropriate level of autonomy, with awareness of the limits of own competence, and accepting accountability to relevant professional and service managers.
Managing own personal learning needs and developing strategies for meeting these.
Using supervision to reflect on practice, and making appropriate use of feedback received.
Developing strategies to handle the emotional and physical impact of own practice and seeking appropriate support when necessary, with good awareness of boundary issues.
Working collaboratively and constructively with fellow psychologists and other colleagues and users of services, respecting diverse viewpoints.
Monitoring and maintaining the health, safety, and security of self and others.
1.3.8. Communication and Teaching
Communicating effectively clinical and non-clinical information from a psychological perspective in a style appropriate to a variety of different
52
audiences (for example, to professional colleagues, and to users and their carers).
Adapting style of communication to people with a wide range of levels of cognitive ability, sensory acuity and modes of communication.
Preparing and delivering teaching and training which takes into account the needs and goals of the participants (for example, by appropriate adaptations to methods and content).
Understanding of the supervision process for both supervisee and supervisor roles.
Understanding the process of providing expert psychological opinion and advice, including the preparation and presentation of evidence in formal settings.
Understanding the process of communicating effectively through interpreters and having an awareness of the limitations thereof.
Supporting others’ learning in the application of psychological skills, knowledge, practices and procedures.
1.3.9 Service Delivery
Adapting practice to a range of organisational contexts, on the basis of an understanding of pertinent organisational and cultural issues.
Providing supervision at an appropriate level within own sphere of competence.
Understanding of consultancy models and the contribution of consultancy to practice.
Understanding of leadership theories and models, and their application to service development and delivery.
Awareness of the legislative and national planning context of service delivery and clinical practice.
Working effectively with formal service systems and procedures.
Working with users and carers to facilitate their involvement in service planning and delivery.
Working effectively in multi-disciplinary teams. Understanding of change processes in service delivery systems.
Understanding quality assurance principles and processes.
53
2. The structure of training 2.1. It is essential that programmes provide a holistic experience of training that enables
trainees to develop an integrated set of learning outcomes. 2.2. Programmes must provide a balanced and developmental set of academic, research
and clinical experiences throughout training. The academic component needs to provide an integrated curriculum supporting the clinical and research training. The research training needs to be carefully planned and have sufficient time devoted to it to enable trainees to conduct research at a postgraduate level and to be in a position to contribute to the knowledge base of the profession. The clinical experience component of training needs to be delivered within the following framework.
2.3. The parameters described below aim to provide the framework for pathways through
training, delineating client populations, clinical contexts and learning outcomes which contribute to a generic training in clinical psychology. It is important to recognise that the scope of clinical psychology is so great that initial training provides a foundation for the range of skills and knowledge demonstrated by the profession. Further skills and knowledge will need to be acquired through continuing professional development appropriate to the specific employment pathways taken by newly qualified psychologists.
2.4. Clinical experience will be gained in service delivery systems that offer a coherent
clinical context. This will usually be a setting oriented towards a population defined by age (e.g. child, adult, older people), by special needs (e.g. learning disabilities, serious mental health problems, health-related problems, substance abuse), or by a service delivery focus (e.g. psychological therapy). In addition, clinical experience will be gained in a range of service contexts (primary, secondary and tertiary care, in-patient, out-patient, community), with service delivery models ranging from independently organised work through to integrated inter-professional working.
2.5. Programmes will be expected to structure the training patterns of their cohorts so that
they reflect workforce-planning requirements within the NHS. These requirements will be shaped in part by National Service Frameworks and national policies, as well as by evidence of recruitment problems (for example, vacant posts) paying particular attention to specialities which have recruitment difficulties. National standards as set out by the Division of Clinical Psychology’s Faculties and Special Interest Groups must also guide training patterns for each cohort of trainees (see Appendix 1 for a list of current documents). Not all trainees will necessarily follow the same pathway through training. Programmes therefore need to ensure, in consultation with local Faculties and SIGs and local placement providers, that – across the trainee cohort – there is optimum, effective and efficient use of all available placements.
2.6. Clients, services and modes of work:
The learning objectives described above need to be demonstrated with a range of clients and across a range of settings. These are not defined prescriptively, and there are multiple pathways through which the required goals may be achieved. The range of clients and settings is outlined below, together with an outline of the knowledge base that trainees need to develop to support their practice.
2.6.1. Clients
A fundamental principle is that trainees must work with clients across the lifespan, such that they see a range of clients whose difficulties are

54
representative of problems across all stages of development. In this context, trainees must demonstrate competence to be able to work clinically with:
a wide breadth of presentations – from acute to enduring and from mild
to severe; problems ranging from those with mainly biological and/or
neuropsychological causation to those emanating mainly from psychosocial factors;
problems of coping, adaptation and resilience to adverse circumstances and life events, including bereavement and other chronic, physical and mental health conditions; and
clients from a range of backgrounds reflecting the demographic characteristics of the population. Trainees will need to understand the impact of difference and diversity on people’s lives (including sexuality, disability, ethnicity, culture, faith, cohort differences of age, socio-economic status), and their implications for working practices.
It is also essential that trainees work with:
clients with significant levels of challenging behaviour;
clients across a range of levels of intellectual functioning over a range of ages, specifically to include experience with clients with developmental learning disabilities and acquired cognitive impairment;
clients whose disability makes it difficult for them to communicate; and
carers and families.
2.6.2. Service delivery systems
Trainees must undertake substantial pieces of clinical work over a substantial period of time in each of a range of settings, including:
in-patient or other residential facilities for individuals with high dependency needs, both acute and long term;
secondary health care; and
community or primary care.
2.6.3. Modes and type of work
direct work;
indirect, through staff and/or carers;
work within multi-disciplinary teams and specialist service systems, including some observation or other experience of change and planning in service systems;
work (practice, teach, advise) in at least two evidence-based models of formal psychological therapy. This must include cognitive-behaviour therapy and at least one other evidence-based approach, such as brief psychodynamic or interpersonal psychotherapy, systemic, or integrative interventions.
work with complexity across a range of perspectives, demonstrating flexibility in application of whichever approach is most appropriate for the client or system; and
be critical of their own approach, and aware of how to practice in the absence of reliable evidence, as well as being able to contribute from their work to the evidence base.

55
2.6.4. The UK health care context and the application of clinical psychology
Trainees’ work will need to be informed by a substantial appreciation of the legislative and organisational contexts within which clinical practice is undertaken, including for example:
legislation relevant to England and the devolved nations (e.g. Mental Health Act, Mental Capacity Act, Children Act, Disability Discrimination Act, Health and Social Care Act, Data Protection Act, employment legislation, etc.);
Government policy statements (e.g. National Service Frameworks, Ten Essential Shared Capabilities, Knowledge and Skills Framework, etc.); and
organisation of the NHS and social care in England and the devolved nations.
2.7. Where programmes are providing training for the Society’s Statement of Equivalence
in Clinical Psychology through the accredited programmes route, they must ensure that the quality assurance arrangements pertaining to this aspect of their provision are broadly consistent with those of the main, accredited programme.
2.8. Of the total programme time (exclusive of annual leave), at least fifty per cent must
be allocated to supervised clinical experience. In addition, at least ten per cent must be available to trainees for self-directed study throughout the programme. Of the remaining time there must be an appropriate balance between research activity, and learning and teaching, to ensure that the criteria outlined in sections 10 and 11 can be met.

56
Appendix 6: Clinical Tutorial form
Clinical Tutorial Form
Trainee:
Supervisor:
Placement:
Date of Review:
Clinical Tutor:
Gaps in Experience: (Note to tutor: review Summary Log of Clinical Experience)
Training needs: (Note to tutor: review previous EPR notes & placement continuation form)
Review placement contract for current placement (Note to tutor: consider how gaps in experience might be covered; ensure training needs are accommodated in contract; check that appropriate induction has been planned & that arrangements for supervision etc. are adequate)
Dates for MPR and EPR
Other items: Note to tutor: 1. Check that trainee has made contact with their personal advisor. 2. Check if the trainee has been directed to relevant Placement Trust policies relating to health and safety, equality & diversity etc. 3. Ask trainee if s/he has offered supervisor a copy of relevant academic timetable and module outlines. 4. Any other issues raised by trainee
A typed (electronic) version of the form to be sent by the trainee’s clinical tutor to the named senior clinical tutor at the university, for inclusion in the trainee’s (confidential) file and circulation to the trainee.

57
Appendix 7: Placement Review form
University of Hertfordshire Doctorate in Clinical Psychology
Placement Review Form
Trainee:
Supervisor:
Placement:
Date of Review: MPR / EPR (circle)
Clinical Tutor:
Notes: This form is to be used for both MPR and EPR visits. A typed (electronic) version will be sent by the visiting clinical tutor to the named senior clinical tutor at the university following the placement visit. A copy of the form (Part A) will be sent to the trainee and supervisor(s), and a copy will be kept in the trainee’s (confidential) file. The first section of the form (Part A) is considered open between trainee, supervisor and UH clinical tutor team; this should be made clear by the visiting clinical tutor. The second part of the form (Part B) provides space for any confidential comments, which trainee, supervisor or tutor would prefer not to have disclosed. This information will remain confidential within the UH clinical tutor team. At the EPR an additional Placement Continuation form should be completed. This contains a summary of agreed learning needs, goals and gaps in experience to be passed on to the trainee’s next placement supervisor. This information will assist the new supervisor in planning the placement and preparing the draft placement contract.

58
Part A: (open)
Placement Evaluation (Note to tutor: Review the placement, the opportunities for learning, the resources and the supervision; check that minimum standards are being met. Refer to Handbook)
Trainee Evaluation Supervisor Evaluation Action points Tutor comments Overall impression of the placement as a learning environment
Physical resources, admin support, computers, library etc.
Access to relevant policy documents
Range of experience available
Quality and quantity of supervision
Opportunities for observation (has the trainee been observed yet? Use of recording in supervision? Joint work?)

59
Range of experience (Note to tutor: What has the trainee done on the placement so far? How does this match with the placement goals? What are the remaining gaps in experience? Goals for the rest of the placement and/or for future placements? Refer back to the Placement Contract and to the guidelines on experience in the Handbook).
Experience acquired Gaps Goals/Plans Tutor comments Client Range (age, gender, ethnicity, ability level etc.)
Problem range:
Settings
Modes and type of work (direct/indirect? Individual/group? Models: CBT? Other models? specify)

60
Trainee Evaluation Supervisor Evaluation Targets/goals Tutor comments
Review of Competencies (Note to tutor: Review the various competence areas with trainee and supervisor; monitor progress; note areas for development, any concerns and learning goals for the remainder of the placement and for future placements; if necessary refer to the Supervisor Evaluation form for further details on the competence areas. )
Professional Behaviour
Ethics
Awareness of issues of power, difference and diversity
Autonomy & Independence
Organising workload, managing priorities & learning needs
Use of supervision
Self reflection
Knowledge(& ability to generalise knowledge)
Critical Thinking
Evidence-based practice

61
Trainee Evaluation Supervisor Evaluation Targets/goals Tutor comments
Relationship Factors (with clients & carers– rapport, therapeutic alliance etc.)
Assessment (knowledge, skills, choice of procedure, administration, scoring, interpretation, risk assessment etc.)
Formulation
Intervention – psychological therapies
Indirect intervention
Communication & Reporting (incl. note keeping)

62
Trainee Evaluation Supervisor Evaluation Targets/goals Tutor comments
Team Working (i.e. ability to work within an MDT etc.)
Inter-professional working (incl. understanding roles of other team members)
Relationship factors (with colleagues, dealing with conflict etc.)
Consultation
Teaching & presentation skills
Leadership (understanding leadership role of the psychologist in practise).
Knowledge of the Organisation
Awareness of wider organisational issues & service context

63
General Comments / Summary: I confirm that both trainee and supervisor have agreed to their comments included above being communicated to each other.
Clinical Tutor: Signed:

64
Part B. (Confidential) Additional confidential feedback from trainee: What will be done with this information?/ Action: Additional confidential feedback from supervisor: What will be done with this information?/ Action: Additional confidential comments and observations from clinical tutor: What will be done with this information?/ Action:

University of Hertfordshire Doctorate in Clinical Psychology
Placement Continuation Form
This form is completed by the trainee’s clinical tutor at the End of Placement review in consultation with the clinical supervisor and the trainee. The continuation sheet will be passed on to the trainee’s next clinical supervisor. Name of Trainee: Name of Supervisor: Placement: Date: Training Needs (note any areas which may require further development or specific attention; consider each of the competence areas) Gaps in Experience (note any gaps in the trainee’s experience so far) Clinical Tutor: Signed:
66
Appendix 8: Log of Clinical Experience
University of Hertfordshire Doctorate in Clinical Psychology
Log of Clinical Experience
Trainee
Placement
Placement Dates
Placement Period 1 2 3 4 5 6
Location
Supervisor
Confirmation of contents of Log:
Trainees Signature:
Date:
Supervisors Signature:
Date:
The Log of Clinical Experience serves as a formal record of the experience and skills that you gain on each placement. Please ensure that you keep your Log of Clinical Experience up to date. You must record details of all work undertaken on placement in the appropriate tables that follow. The Log of Clinical Experience should be typed. The Log should be taken to mid- and end-of placement reviews for monitoring purposes. The completed and signed Log of Clinical Experience must be handed to the course administrator along with your other placement evaluation forms within one week of completing the placement, by the deadline specified on your timetable.

67
1. Clinical Work: Dates Observed,
Joint or Independent
No. of Sessions
Client Characteristics
(age, sex, ethnicity, intellectual functioning)
Setting(s)
(primary/secondary/ tertiary level? inpatient/residential or outpatient?)
Problem
(acute/enduring? mild/severe? functional/organic/ adjustment? + details of specific problems)
Assessment methods
(interviews? tests used? other procedures? Risk assessment? Context?)
Description of Intervention
(direct/indirect? individual/couple/ family/group? Carers/staff? model/s? + details of specific intervention)
Communication
(reports? Feedback/liaison? To whom?)
Evaluation
(methods used? Outcome?

68
Dates Observed, Joint or Independent
No. of Sessions
Client Characteristics
(age, sex, ethnicity, intellectual functioning)
Setting(s)
(primary/secondary/ tertiary level? inpatient/residential or outpatient?)
Problem
(acute/enduring? mild/severe? functional/organic/ adjustment? + details of specific problems)
Assessment methods
(interviews? tests used? other procedures? Risk assessment?)
Description of Intervention
(direct/indirect? individual/couple/ family/group? Carers/staff? model/s? + details of specific intervention)
Communication
(reports? Feedback/liaison? To whom?)
Evaluation
(methods used? Outcome?

69
Dates Observed, Joint or Independent
No. of Sessions
Client Characteristics
(age, sex, ethnicity, intellectual functioning)
Setting(s)
(primary/secondary/ tertiary level? inpatient/residential or outpatient?)
Problem
(acute/enduring? mild/severe? functional/organic/ adjustment? + details of specific problems)
Assessment methods
(interviews? tests used? other procedures? Risk assessment?)
Description of Intervention
(direct/indirect? individual/couple/ family/group? Carers/staff? model/s? + details of specific intervention)
Communication
(reports? Feedback/liaison? To whom?)
Evaluation
(methods used? Outcome?

70
Dates Observed, Joint or Independent
No. of Sessions
Client Characteristics
(age, sex, ethnicity, intellectual functioning)
Setting(s)
(primary/secondary/ tertiary level? inpatient/residential or outpatient?)
Problem
(acute/enduring? mild/severe? functional/organic/ adjustment? + details of specific problems)
Assessment methods
(interviews? tests used? other procedures? Risk assessment?)
Description of Intervention
(direct/indirect? individual/couple/ family/group? Carers/staff? model/s? + details of specific intervention)
Communication
(reports? Feedback/liaison? To whom?)
Evaluation
(methods used? Outcome?

71
2. Multidisciplinary Working, Inter-professional Learning & Consultancy Describe your experiences in multidisciplinary working, consultancy and any other forms of inter-professional working. This includes participation in multi-disciplinary team meetings and ward rounds, liaison with other professionals about clients, examples of co-working and formal consultation. Describe the extent of your involvement. Please include dates.
3. Meetings /visits/ observations This includes psychology meetings, visits to other services or agencies and observation of or meetings with other professionals (not related to specific client work). Please include dates.

72
4. Teaching /presentation Describe any teaching you did or presentations you made.
Dates To whom?
(profession & numbers)
Context
(e.g. in-house training, journal club, case conference)
Topic Format or teaching method
Evaluation of Outcome
5. Research on placement Describe any research you conducted/initiated or collaborated on while on placement.

73
6. Attendance of educational activities, courses or training events
Date & Venue Topic Speaker/ organiser Evaluation/ learning
outcome
7. Other experiences not recorded elsewhere

74
11. Gaps in experience Describe any gaps in your experience. Are there goals in the placement contract that you were unable to meet? This is important to ensure that gaps in experience are integrated into future placement plans.
12. Total Number of Days on Placement: (excluding days on AL or sick leave, and excluding placement study time)
75
Appendix 9: Summary Log of Clinical Experience
Doctorate in Clinical Psychology
Summary Log of Clinical Experience Please complete this summary form at the end of each placement. The same form should be used for the duration of the three years thereby demonstrating accumulating experience. You should keep the original yourself. A copy should be taken to every clinical tutorial and placement review meeting for monitoring purposes. It is preferable for you to use an electronic version of this form so that entries may be typed and updated. The completed Summary Log is submitted with the placement documents at the end of Placement 6. Please note that you are not expected to gain experience in every area on each placement, but that experience in every area is required by the end of the programme of training. For each category of experience, please indicate whether the experience reflects direct independent work (I), joint work (with your supervisor or another colleague) (J), or observed work (e.g. observing your supervisor) (O). Please record an ‘I’, ‘J’, or an ‘O’ for each piece of work as this provides a broad indication of the amount of work you have undertaken in each area. For the section on Modes and Type of Work, you should also indicate the number of session undertaken for each case, thus a case where you worked independently and did 12 sessions would be recorded as I(12), and a joint case involving 2 sessions would be recorded as J(2).
Placement 1 Placement 2 Placement 3 Placement 4 Placement 5 Placement 6
Clients:
Example
OOJII OJII JJIII
Children
Adolescents
Working age adults
Older adults
Carers and families
Diversity / clients with different culture/class/ethnicity to trainee
Range of intellectual functioning: Average range & above
Range of intellectual functioning: Borderline to mild learning disability and/or acquired cognitive impairment
Range of intellectual functioning: Moderate to severe learning disability and/or

76
acquired cognitive impairment
Clients with significant levels of challenging behaviour
Clients whose disability makes it difficult for them to communicate
Problem Range:
Acute problems
Enduring problems
Mild presentation
Severe presentation
Problems of mainly biological and/or neuropsychological causation.
Problems of mainly psychosocial causation
Problems of adjustment/coping with adverse circumstances (e.g. physical disability, illness, bereavement)
Service Delivery Systems:
In-patient and/or residential facilities for patients with high dependency needs - acute
In-patient and/or residential facilities for patients with high dependency needs – long term
Secondary health care
Community and primary care

77
Modes and type of work
Example (indicating number of sessions per case)
O(1), J(1), I(6), I(8), I(12), I(1)
J(2), O(1), J(1), I(6)
J(1), J(1), I(12)
I(2), I(3), I(1), I(4), I(2), I(3)
J(4), J(8), J(4), I(10)
I(16), I(12), I(16), I(16)
Direct work – individual
Direct work – couple/ family
Direct work – group
Indirect work through staff and carers
Work within multi-disciplinary teams
Experience and/or observation of change within services and/or service planning
Work within more than one evidence-based model of psychological therapy:
3
Model 1: CBT
Work within more than one evidence-based model of psychological therapy: Model 2: …………
Work within more than one recognised model of psychological therapy: Model : …………
Work within more than one recognised model of psychological therapy: Model : …………
3 Direct experience of (and competence in) working within at least two evidence-based models of therapy is
essential. Additional spaces are provided as frequently trainees have additional experience of more than two models of working, although some of these may be at a lower level eg. Observed or joint work.

78
Summary of Placements
YEAR 1
YEAR 2 YEAR 3
Placement period 1 Placement period 2 Placement period 3 Placement period 4 Placement period 5 Placement period 6
Placement
Location
Supervisor(s)
Clinical Tutor
MPR date
EPR date
Number of days
(excluding study time and leave)
Annual Leave4
(no. of days AL taken from placement time)
Sick/special leave
(no. of days sick leave taken from placement time)
Example of Clinical Work
5
Clinical Case Report6
4 A maximum of 12.5 days of annual leave may be taken from placement (P) time per annum, with a maximum of 7.5 days of the 12.5 total
taken during any single placement period. This excludes annual leave taken from placement study (PS) time. 5 Specify type of example submitted for each placement period. Note that one example per year must be of a type that includes a recording of
clinical work. Refer to guidelines for details. 6 Specify type of case report. Refer to guidelines on case reports for the five types of case report required over the 3-year period.

79
University of Hertfordshire Doctorate in Clinical Psychology
Summary Log of Clinical Experience:
Supervisor Confirmation
I confirm that I have reviewed the Trainee’s Summary Log of Clinical Experience, and that the entries made for the time on my placement are correct.
Placement
Supervisor
Signature
Date
1
2
3
4
5
6

80
Appendix 10: Supervisor Evaluation of Clinical Competence
University of Hertfordshire
Doctorate in Clinical Psychology
Supervisor Evaluation of Clinical Competence: Part A
Trainee
Supervisor
Placement
Placement Dates
Placement period
1 2 3 4 5 6
Location
This form is to be completed by the placement supervisor at the end of the placement being assessed. It is a key part of the formal assessment of the trainee’s clinical competence. Part A of the Supervisor Evaluation form covers: 1. Personal and Professional Skills, 2. Knowledge and Critical Thinking, 3. Clinical Skills, and 4. Multidisciplinary working, organisational knowledge, teaching and consultation. You will be asked to rate several types of competency in each of these areas. Please provide comments on the trainee’s strengths and weaknesses in each area and illustrate your comments with examples. You will be asked to provide an overall recommended rating for the placement at the end of Part A. Deadline: The completed and signed Supervisor Evaluation of Clinical Competence form must be returned to the Course Administrator within one week of the end of the placement. It is the responsibility of the supervisor to ensure that the evaluation is completed in time. The form may either be sent directly to the Course Administrator or preferably given to the trainee to submit along with their other placement documents. Please note that late submissions may result in placement failure.

81
Rating Scale: For each area being assessed you are asked to rate the trainee on the following scale. The purpose of using this scale is to provide a cross-sectional view of the trainee’s current level of competence relative to their stage in training. The scale is provided below:
N/O Unable to rate; no opportunity to observe this on the
current placement
0 Serious concerns in this area
1 Poor (relative to stage in training)
2 Below Average (relative to stage in training)
3 Average (i.e. appropriate to stage in training)
4 Above average (relative to stage in training)
5 Excellent (relative to stage in training)
Trainee Observation: Please indicate how many times you have observed the trainee’s skills in each of the following ways:
Direct in vivo observation
Audio-tapes
Video-tapes
Live supervision via a screen
Joint work (clinical)
Observation of the trainee in meetings
Observation of teaching and/or case presentations by the trainee
Observation during supervision (e.g. of case conceptualisation skills)
Indirect observation via review of detailed psychotherapy process notes
Other (please specify)
Further comments:

82
1. Personal & Professional Skills Please rate and provide comments on the following:
Professional Behaviour
maintains appropriate professional role & interpersonal boundaries;
maintains appropriate time boundaries;
is reliable e.g. attends meetings, supervision sessions etc. as agreed
works collaboratively & constructively with colleagues and service users and is able to respect diverse viewpoints
Comments:
Rating: N/O 0 1 2 3 4 5
Ethics
upholds professional ethics;
is aware of ethical issues & understands how these apply in clinical context;
ensures informed consent
Comments:
Rating: N/O 0 1 2 3 4 5
Awareness of issues of power, difference and
diversity
understands the inherent power imbalance between practitioner and client;
shows awareness of and sensitivity to issues pertaining to minority groups; understands the impact of difference and diversity;
is able to work sensitively with these issues in clinical practise
Comments:
Rating: N/O 0 1 2 3 4 5
Autonomy & Independence
works at a level appropriate to own competence;
accepts accountability to professional and service managers
is able to exercise personal responsibility & take initiative at a level appropriate to stage in training.
Comments:
Rating: N/O 0 1 2 3 4 5

83
Organising workload, managing priorities & learning needs
is able to manage priorities and workload;
meets necessary deadlines;
manages own personal learning needs and has strategies for meeting these (e.g. requesting reading, using study time effectively, monitoring gaps in experience and own training needs)
Comments:
Rating: N/O 0 1 2 3 4 5
Use of supervision
makes appropriate use of supervision;
is adequately prepared for supervision;
makes appropriate use of feedback;
contributes ideas;
uses supervision to reflect on practise;
understands the supervision process for both supervisee and supervisor
Comments:
Rating: N/O 0 1 2 3 4 5
Self reflection
is able to reflect on own practise;
recognises strengths and weaknesses without being overly self-critical;
considers role of own beliefs and assumptions
demonstrates self-awareness
Comments:
Rating: N/O 0 1 2 3 4 5
Self-care
is able to handle the emotional and physical impact of own practice;
seeks appropriate support when necessary
Comments:
Rating: N/O 0 1 2 3 4 5

84
2. Knowledge and critical thinking skills Please rate and provide comments on the following:
Knowledge
knowledge and understanding of psychological theory and evidence;
ability to generalise and synthesise prior knowledge and experience in order to apply them in different settings and novel situations
Comments:
Rating: N/O 0 1 2 3 4 5
Critical Thinking
ability to think critically, reflectively and evaluatively
ability to be critical of own approach/ preferred model
Comments:
Rating: N/O 0 1 2 3 4 5
Evidence–based practice
Knowledge, skills and understanding to identify and critically appraise research evidence relevant to practice;
Knowledge, skills, understanding and values to use a broad evidence and knowledge base, to assess, formulate and intervene psychologically, from a range of possible models and modes of intervention with clients, carers and service systems
Comments:
Rating: N/O 0 1 2 3 4 5

85
3. Clinical Skills Please rate and provide comments on the following:
Relationship Factors
ability to develop and maintain effective working alliances with clients
ability to establish rapport,
sensitivity to client(s) communications, appropriate empathy,
ability to handle difficult situations
Comments:
Rating: N/O 0 1 2 3 4 5
Assessment
knowledge of assessment methods and procedures;
application of this knowledge in choosing assessment methods appropriate to service context, client problem and likely intervention method;
specific skills in administering and interpreting psychometric tools;
appropriate use of test results;
specific skills in interviewing,
skills in using other forms of assessment eg. behavioural observation;
knowledge of and skills in conducting appropriate risk assessment and using this to guide practice
Comments:
Rating: N/O 0 1 2 3 4 5
Formulation
ability to integrate information from assessments within a coherent framework that draws upon psychological theory and evidence;
ability to incorporate multiple levels (e.g. intrapersonal, interpersonal, societal, cultural & biological) into psychological formulation;
ability to use formulations to set appropriate goals and plan appropriate interventions;
ability to reformulate when new information arises;
ability to use formulations with clients and multi-professional colleagues to facilitate understanding of the client’s problems
Comments:
Rating: N/O 0 1 2 3 4 5
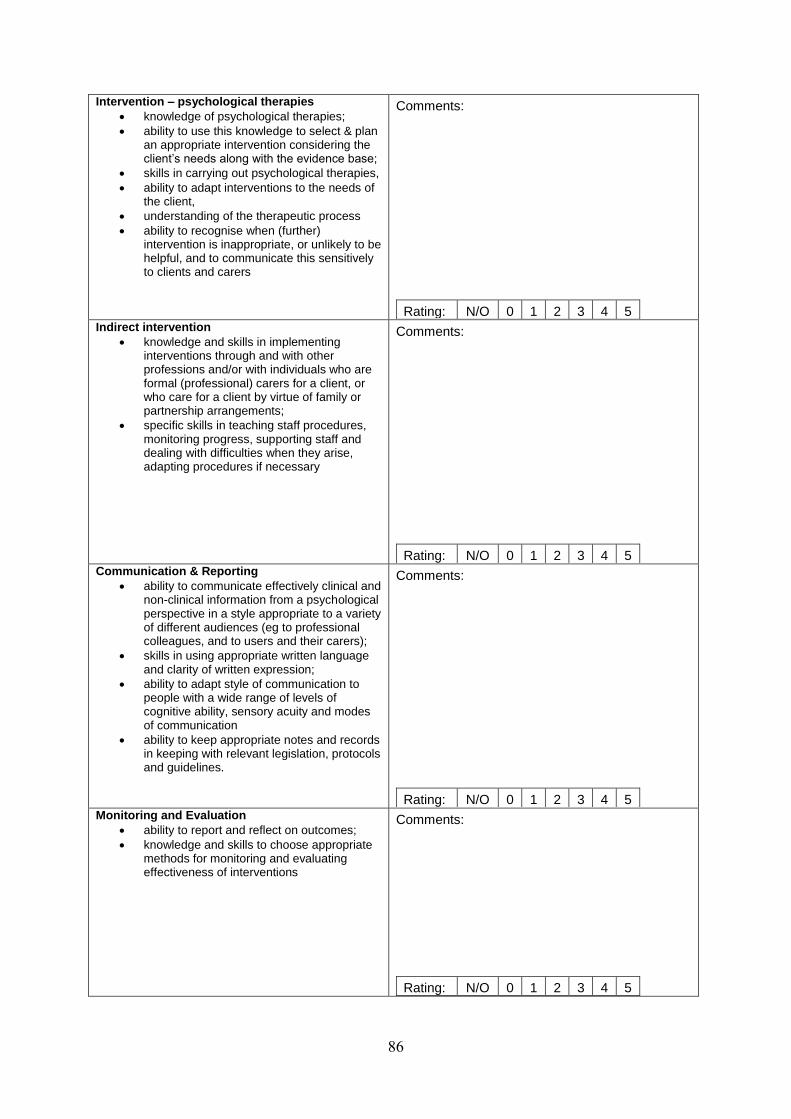
86
Intervention – psychological therapies
knowledge of psychological therapies;
ability to use this knowledge to select & plan an appropriate intervention considering the client’s needs along with the evidence base;
skills in carrying out psychological therapies,
ability to adapt interventions to the needs of the client,
understanding of the therapeutic process
ability to recognise when (further) intervention is inappropriate, or unlikely to be helpful, and to communicate this sensitively to clients and carers
Comments:
Rating: N/O 0 1 2 3 4 5
Indirect intervention
knowledge and skills in implementing interventions through and with other professions and/or with individuals who are formal (professional) carers for a client, or who care for a client by virtue of family or partnership arrangements;
specific skills in teaching staff procedures, monitoring progress, supporting staff and dealing with difficulties when they arise, adapting procedures if necessary
Comments:
Rating: N/O 0 1 2 3 4 5
Communication & Reporting
ability to communicate effectively clinical and non-clinical information from a psychological perspective in a style appropriate to a variety of different audiences (eg to professional colleagues, and to users and their carers);
skills in using appropriate written language and clarity of written expression;
ability to adapt style of communication to people with a wide range of levels of cognitive ability, sensory acuity and modes of communication
ability to keep appropriate notes and records in keeping with relevant legislation, protocols and guidelines.
Comments:
Rating: N/O 0 1 2 3 4 5
Monitoring and Evaluation
ability to report and reflect on outcomes;
knowledge and skills to choose appropriate methods for monitoring and evaluating effectiveness of interventions
Comments:
Rating: N/O 0 1 2 3 4 5

87
4. Multidisciplinary working, organisational knowledge, teaching and consultation Please rate and provide comments on the following:
Team Working
ability to work effectively within a multidisciplinary team;
contribution to multi-disciplinary team;
understanding of roles within the team;
ability to deal with difference of opinion within the team
Comments:
Rating: N/O 0 1 2 3 4 5
Relationship factors
ability to establish positive working alliances with staff and colleagues;
deals with conflict appropriately
Comments:
Rating: N/O 0 1 2 3 4 5
Consultation
understanding of consultancy model;
ability to use psychological knowledge & skills to assist multidisciplinary colleagues, services or other agencies with clinical issues, and/or matters of service delivery or service development
Comments:
Rating: N/O 0 1 2 3 4 5

88
Teaching & presentation skills
appropriate planning & preparation; presentation/teaching skills;
content appropriate to audience and takes into account the needs and goals of the participants
Comments:
Rating: N/O 0 1 2 3 4 5
Leadership
understanding of the leadership role of the clinical psychologist in practice & the application of leadership models/theory to service delivery and development
Comments:
Rating: N/O 0 1 2 3 4 5
Knowledge of the Organisation
understanding of the local service, its organisation, the functions of committees, and the channels of communication;
ability to take effective action within the organisation including use of referral networks;
Comments:
Rating: N/O 0 1 2 3 4 5
Awareness of wider organisational issues & service context
knowledge and understanding of relevant NHS and local authority policies;
awareness of the legislative and national planning context of service delivery and clinical practice;
understanding of change processes in service delivery systems
knowledge, understanding and skills to adapt practice to a range of organisational contexts, on the basis of an understanding of pertinent organisational and cultural issues
understanding and experience of the involvement of service users and carers to facilitate service planning and delivery
Comments:
Rating: N/O 0 1 2 3 4 5

89
University of Hertfordshire Doctorate in Clinical Psychology
Supervisor Evaluation of Clinical Competence: Part B
Overall Pass / Fail Recommendation
Trainee: Supervisor: Placement: Overall rating: PASS CONDITIONAL PASS FAIL
Please use the following criteria to provide an overall rating of the trainee’s performance on this placement. Pass: This rating reflects a level of competence appropriate to the trainee’s stage in training. The trainee should have received ratings of at least average for his/her stage in training across most of the areas of competency. If the trainee has underperformed in any areas, this underperformance should be balanced by good performance across other areas, should not give rise to significant concern about the trainee’s overall competence, and there should have been evidence of progress over the duration of the placement in the areas of underperformance. Usually the trainee will have achieved the placement goals (unless due to lack of opportunity) and will be sufficiently competent to move on to the next stage of training. The trainee will have undertaken a reasonable workload and carried out the work competently. The trainee will have shown evidence of learning/progress over the duration of the placement. Conditional Pass: This rating indicates some concerns about the trainee’s competence and/or range of experience. This is likely to reflect underperformance across one or more areas, lack of progress across one or more areas, insufficient time spent on the placement to fulfil the gaols (e.g. due to extended periods of absence) or failure to carryout a sufficient range of work. A trainee given this rating may be given a ‘conditional pass’ for the placement, with requirements to undertake specific work in a subsequent placement and/or to demonstrate improvement in certain competencies during the next placement which bring the trainee back in line with the level expected relative to stage in training. Should the trainee fail to meet the specified targets, then s/he will be deemed to have failed the original placement. Fail: This rating indicates serious concerns about the trainee’s competence (not arising from lack of opportunity on the placement), in one or more areas.

90
A fail rating will usually reflect at least one of the following:
1. Serious concerns in at least one area of clinical work 2. Persistent underperformance across several areas of work 3. Lack of evidence of learning and development over the duration of the placement 4. Serious concerns about aspects of professional behaviour 5. Serious concerns about use of supervision
6. Gross incompetence or negligence resulting in potential or actual harm to patients/clients or
the public, including failure to inform supervisor of critical actions/situations when this could
be reasonably expected.
7. Abuse of patients/clients: physical violence, verbal abuse or intimidation, exploitation for
financial or material gain, entering into a sexual relationship.
8. Other gross and/or persistent unprofessional conduct, including contravention of national or
local health service policy, British Psychological Society ethical and professional guidelines,
or Health Professions Council standards of conduct performance and ethics.
A failure on the grounds of criteria 1 to 5 will usually result in the trainee being required to repeat all or some of the clinical placement. However only one placement may be repeated; two placement failures will therefore usually result in course failure and withdrawal of registration. Failure on the grounds of criteria 6 to 8 will usually result in direct withdrawal of registration and expulsion from the course, following appropriate investigatory procedures. In all cases the final decision regarding placement pass/fail rests with the Progression Board of Examiners. Supporting Evidence for Conditional Pass or Fail Recommendations: Please provide examples and evidence to support your recommendation (attach a separate page if necessary). If you are recommending a ‘conditional pass’, please also provide a recommendation as to what additional work and/or competencies need to be demonstrated during the next placement.

91
University of Hertfordshire Doctorate in Clinical Psychology
Supervisor Evaluation of Clinical Competence: Part C
Trainees Comments on Accuracy of Feedback: Please provide comments on the accuracy of the feedback. Please note any points of disagreement. Supervisor: Signed: Date: Trainee: Signed: Date:

92
Appendix 11: Trainee Placement Feedback & Audit forms
Doctorate in Clinical Psychology
Trainee Placement Feedback Form
Trainee
Supervisor
Placement Type
Placement Dates
Placement number
1 2 3 4 5 6
Location
This feedback form must be completed at the end of each placement period. The purposes of the form are:
1. To provide the basis for discussion between trainee, supervisor and tutor about the placement and the supervision at the end of the placement;
2. To provide feedback to the Course Team about what the placement offers, thereby enhancing the matching of future trainees’ needs to specific placements in the placement allocations process;
3. To identify strengths, weaknesses and areas for development, which the supervisor may use to inform his/her own professional development, and the Course Team may use to identify where further support or training may be necessary;
4. To flag up any specific problems on the placement. The completed and signed Trainee Placement Feedback form must be returned to the course administrator within one week of the end of the placement, by the stated deadline. The supervisor must have the opportunity to see the form and to add his/her comments.

93
Section 1: Feedback: Supervision Please rate these aspects of the supervision and provide comments below.
Poor / limited Acceptable Good
Discussion of case work: clinical advice and case management
Discussion of case work: formulation and theory-practise links
Teaching/instruction on specific clinical skills (e.g. specific therapeutic techniques, specific methods of assessment).
Discussion of professional issues: workload, organisational issues, ethical issues, impact of power imbalances and diversity etc.
Opportunities for reflection: self reflection and discussion of process issues
Supervision process: agenda set collaboratively, supervision contract discussed and reviewed at least once, opportunities for mutual feedback
Feedback: constructive feedback provided by supervisor, highlighting strengths and areas for further development
Boundaries: time boundaries & personal-professional boundaries upheld appropriately
Time: sufficient protected time set aside for supervision
Observation: opportunities for mutual observation, joint work, live supervision and use of recordings
Comments:

94
Section 2: Feedback: Placement Environment Please provide feedback on the following aspects of the placement and provide comments in the space below.
Poor/limited Acceptable Good
Informal support from other trainees, and psychology colleagues
Attitude of wider service towards psychology
Opportunities within the psychology dept for learning (eg. journal clubs, case discussion groups)
Library Facilities
Work environment (e.g. office and desk space, access to clinical rooms)
Comments: Section 3: Feedback: Main Strengths & Weaknesses of Placement Please identify the main strengths and weaknesses of this placement. List them below.
Strengths: Weaknesses:

95
Section 4: Description of experience available on the placement Please provide feedback on the range of experience available on this placement and provide comments below. Please note that it is not necessarily expected that all placements will provide experience across all areas. For example, a specialist therapy placement may be model specific and may largely be limited to direct individual interventions.
Opportunity to work with ……. No opportunity / Not available on this placement
Limited opportunities
Good Opporunities
Males and females from across the age range specified
Clients of different ethnic/cultural background
Range of problems
Opportunity to work in …….
A range of settings
Multi-disciplinary team
Opportunity to carry out…….
Assessments (clinical, interviews, observation etc.)
Psychometric assessment
Therapy with individuals
Couple/family interventions
Group interventions
Indirect interventions with staff/carers
Consultation
Opportunity to …….
Consider more than one theoretical model
Teach others
Present clinical work
Liaise with other agencies
Learn about the service context and organisational environment
Comments:

96
Section 5: General Comments Please provide any other general comments about the placement or supervision and give an overall rating of the placement and supervision.
Overall Rating: Poor Satisfactory Good Supervisor’s Comments on the Feedback: Please provide comments on the feedback provided and note any points of disagreement.
Trainee: Signature: Date: Supervisor: Signature:
Date:

97
Doctorate in Clinical Psychology
Placement Audit Form
Trainee
Supervisor
Placement Type
Placement Dates
Placement number
1 2 3 4 5 6
Placement length
6 months 1 year Other
Location
Clinical Tutor
This audit form must be completed at the end of each placement period. The purposes of the form are:
1. For the course to identify where minimum standards are not being met and to offer
support to supervisors and/or services in addressing these issues, as appropriate. 2. For the course to identify where minimum standards are/are not being met for the
purposes of placement audit. For the purposes of the Placement Audit only anonymous cumulative data will be reported. The completed and signed Placement Audit form must be returned to the course administrator within one week of the end of the placement, by the stated deadline. The supervisor must have the opportunity to see the form and to add his/her comments.

98
Section 1: Minimum Standards: Practical aspects Please rate the following practical aspects of the placement and provide comments in the space below.
Minimum standard Unsatisfactory (does not meet minimum standards)
Satisfactory (meets minimum standards)
Good (surpasses minimum standards)
Accommodation: office/ desk space
Use of a desk on placement days in (at least) a shared office.
Administrative support
Access to adequate administrative support
Photocopying Access to photocopying
Access to computers
Access to (at least) shared computer for word processing
Interview Rooms Clinical rooms for client work that can be booked on a regular and reliable basis (if required)
Materials Access to appropriate clinical and test materials
Secure storage Access to secure storage for client records
Health and Safety
Safe working conditions and access to health and safety policies
Comments:
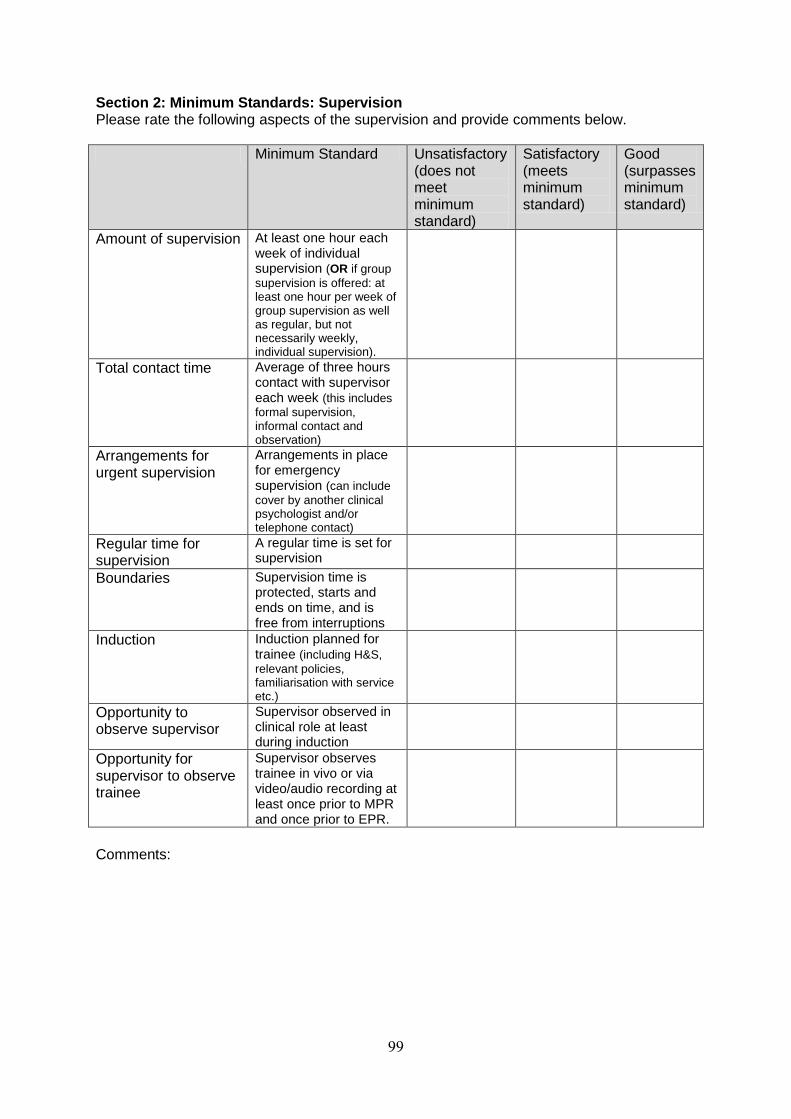
99
Section 2: Minimum Standards: Supervision Please rate the following aspects of the supervision and provide comments below.
Minimum Standard Unsatisfactory (does not meet minimum standard)
Satisfactory (meets minimum standard)
Good (surpasses minimum standard)
Amount of supervision At least one hour each week of individual supervision (OR if group
supervision is offered: at least one hour per week of group supervision as well as regular, but not necessarily weekly, individual supervision).
Total contact time Average of three hours contact with supervisor each week (this includes
formal supervision, informal contact and observation)
Arrangements for urgent supervision
Arrangements in place for emergency supervision (can include
cover by another clinical psychologist and/or telephone contact)
Regular time for supervision
A regular time is set for supervision
Boundaries Supervision time is protected, starts and ends on time, and is free from interruptions
Induction Induction planned for trainee (including H&S,
relevant policies, familiarisation with service etc.)
Opportunity to observe supervisor
Supervisor observed in clinical role at least during induction
Opportunity for supervisor to observe trainee
Supervisor observes trainee in vivo or via video/audio recording at least once prior to MPR and once prior to EPR.
Comments:

100
Section 3: Minimum Standards: Placement Monitoring
Minimum standard Unsatisfactory (does not meet minimum standards)
Satisfactory (meets minimum standards)
Good (surpasses minimum standards)
Placement Contract
Contract drawn up within first two weeks of placement and sent to Clinical Tutor
Clinical tutorial Clinical Tutorial held within the first month of the placement
Mid-Placement Review
Face-to-face Mid-placement review visit by Clinical Tutor held mid-way through the placement and MPR report received by trainee and supervisor within 3 weeks of the meeting (timing of the visits may vary for 1-year placements).
End-of Placement Review
End-of –Placement review held within the last two weeks of placement (usually by telephone if agreed by all parties) and EPR report circulated to trainee and supervisor.
Comments: Supervisor Comments: Trainee: Signed: Date: Supervisor: Signed: Date:

101
Appendix 12: Policy on Managing Difficulties on Placement
Managing Difficulties on Placement
Dealing with placement difficulties Problems arise on placements from time to time. In most cases these are minor concerns, which are easily dealt with by supervisor, trainee and clinical tutor. Occasionally concerns may be more serious. Whilst problems usually immerge during the course of the placement, sometimes they may only come to light at the end of the placement; however the principles regarding how they are approached remain essentially the same. Problems and concerns usually relate to the way in which the trainee is approaching their work or problems with their performance, aspects of how the placement is organised or aspects of the supervision. Dealing with ‘minor’ concerns Concerns on the part of either trainee or supervisor should be discussed with the trainee’s clinical tutor. It is best to alert the clinical tutor to any concerns sooner rather than later. The clinical tutor will usually discuss the concerns with both trainee and supervisor in an attempt to facilitate a resolution of the difficulties. In some instances this discussion may simply require a telephone conversation, while in other cases a placement visit will be arranged. In practise most minor placement difficulties are easily resolved at the mid-placement review. The senior member of the programme team responsible for supervision of the trainee’s clinical tutor (usually a senior clinical tutor) will be kept informed of any placement difficulties and the actions taken by the clinical tutor. Where ‘minor’ concerns are not resolved following the initial intervention by the trainee’s clinical tutor, a senior member of the programme team (usually the senior clinical tutor) will become directly involved in investigating the concerns of trainee and/or supervisor and exploring appropriate action together with the trainee, the supervisor and the clinical tutor. The actions will depend on the nature of the difficulties and could include things such as specific targets for the trainee, an agreement regarding how the trainee will prepare for supervision, agreements about the amount and timing of supervision offered, or plans for co-supervision by another supervisor. Dealing with serious concerns about a trainee There may be times when supervisors have very serious concerns about a trainee (beyond those, which might be dealt with as above or as a placement failure issue). These very serious concerns would include breach of the BPS Code of Ethics and Conduct (2009), the BPS Generic Professional Practice Guidelines (2008), the Division of Clinical Psychology Guidelines for the Professional Practice of Clinical Psychology (1995, revised 2001), the Health Professions Council Guidance on Conduct and Ethics for Students (2009), or professional misconduct. In such cases concerns should be reported immediately to the trainee’s clinical tutor, who will inform a senior member of the course team, or directly to a senior member of the course team (usually the senior clinical tutor or a programme director). An investigation will usually follow in accordance with the relevant NHS Trust and/or University policies and procedures.
In accordance with the Protocol for Managing Clinical Trainees on Placement drawn up by the trainees’ employing trust, any misconduct or poor performance of trainees should be reported by the placement trust (usually the supervisor) to the relevant university tutor (usually the clinical tutor). Serious misconduct may result in the trainee’s placement being terminated. In cases of alleged serious misconduct there may be a requirement for the trainee to leave the placement trust premises pending an investigation. On any issues concerning academic or university rules the University will deal with it using its procedures. On issues concerning conduct whilst in a placement trust, or other employment related issues the employing Trust’s policy should be used. The employing Trust’s Human Resources Department must be made aware of any disciplinary issues. Dealing with more serious concerns about the placement and/or supervision
7
7 This section of the policy draws heavily on the statement from the North Thames Courses
on how they will manage problems with supervision on placements. Since placements are
sometimes shared between UH and the North Thames courses, it was considered sensible to

102
Sometimes a problem emerges with a placement that raises concern either about the provision or quality of supervision, or the clinical capacity of the supervisor, or of aspects of the placement itself. In such instances the course has a duty of care to trainees, and potentially to patients, and on this basis would need to investigate any concerns in a more formal manner. Examples of a serious concern include: gross deviations from good practice in supervision; clear evidence that the quality of supervision fell significantly below the standard expected of a qualified psychologist (e.g. offering advice at clear variance with accepted professional practice, unethical professional practice, breaches of the BPS Code of Conduct, breaches of the HPC Standards of Conduct, Performance and Ethics, breaches of NHS policies and procedures, and/or serious doubts about the clinical competence of the supervisor); major problems with the placement such as bullying by another member of staff (not the supervisor) or major disruptions to service provision, resulting in little opportunity for the trainee to undertake appropriate work. In conformity with NHS principles and procedures, the course would initially carry out a confidential enquiry, to ensure that there were indeed appropriate grounds for concern. Usually a senior member of the course team would meet with the trainee and the relevant clinical tutor to consider the issues being raised. If, after discussion, the matter was felt to warrant further investigation the course would raise any concerns directly and - usually - promptly with the supervisor, with the caveat that trainees sometimes request that such discussions occur only after they have left the placement (because they worry that their criticism will influence a supervisor’s evaluation). Therefore the course may delay taking the matter further until the MPR, or after the placement ends. However, if the course considered the concerns raised to be very serious, a decision may be made to override the trainee’s anxieties and take up the issue directly and immediately. Usually a senior member of the course staff would meet with the supervisor, detail the concerns and discuss them with the supervisor. Hopefully the spirit of this meeting would be open rather than adversarial, with the aim of clarifying concerns. Outcomes from this meeting would vary. For example: a) It may become clear that there are no substantial grounds for concerns, and hence that no further
action is warranted or necessary. b) The supervisor and the course may agree that aspects of the placement or the supervision were
problematic and agree an appropriate action plan. c) There may be serious concerns about the placement or the service itself, in which case there may
also be a responsibility to inform a line manager or service manager and to involve him/her in agreeing an appropriate action plan.
d) In some cases, concerns raised about supervision may raise significant questions about a
supervisor’s professional and/or clinical capacities. The course would still hope to discuss an appropriate action plan directly with the supervisor (which could include a decision not to use the placement in future). However, some concerns may be sufficient to make it inevitable that duty of care requires the course to inform the supervisor’s professional or line manager. (Examples would be practice which appears to be significantly at variance with acceptable standards, or breaches of the BPS Code of Conduct and relevant Trust procedures). Supervisors would of course be informed of this action. This step would not be taken unless careful discussion with senior course staff indicated that such a step was warranted.
In cases of formal grievance by the trainee, the employing Trust’s grievance policy and the University’s appeals procedure and grievance policy will be used as appropriate.
maintain consistency between the neighbouring courses as to how placement difficulties
would be managed.

103
Appendix 13: Placement Marking Guidelines
Placement Marking Guidelines Placement related submissions are reviewed by the trainee’s clinical tutor (who is not blind to the trainee’s identity). In situations where the outcome recommended by the clinical tutor differs from that recommended by the placement supervisor, the placement documents will be reviewed by a second marker who is blind to the identity of both the trainee and the supervisor. The Example of Clinical Work is double marked from the outset by the trainee’s clinical tutor (who is not blind to their identity) along with another member of the course team (who is blind to the trainee’s identity). Placement related submissions are evaluated for each placement ‘period’. This usually corresponds to a standard 6 month placement. In the case of year-long placements, evaluations are required for two placement ‘periods’.
Log of Clinical Experience This constitutes the formal record of the trainee’s range and quantity of experience on placement. The Log of Clinical Experience is evaluated on the basis of both the amount of work undertaken and the range of experience covered. As placements vary considerably, there is no single set of criteria for evaluating the log of clinical experience, rather the markers are expected to use their judgement in assessing whether the amount and range of experience is sufficient. Trainees should not be penalised for gaps in their experience which have arisen due to lack of opportunity on the placement. The log of clinical experience may be graded as a pass, a pass with minor amendments (for example where minor details need to be added or corrected), a conditional pass, or a fail. Grounds for a conditional pass or fail rating are as follows:
a log of clinical experience that fails to show a sufficient range of experience (for example, where a trainee has consistently failed to undertake any intervention work despite opportunity on the placement),
a log of clinical experience that fails to show a sufficient quantity of experience (for example, where a trainee has spent large amounts of time on one or two cases to the exclusion of other cases despite opportunity on placement),
and/or insufficient days completed on placement (this would usually have been due to an extended period of leave taken during the placement).
A conditional pass would usually be given where it is considered reasonable for the trainee to make up for the deficits in quantity or range of experience during a subsequent placement. A fail rating would usually be given where the deficits in range and/or quantity of experience are such that the trainee would need to undertake an additional placement (or a large part of an additional placement) to make up the shortfall. Example of Clinical Work The examples of clinical work each have specific marking criteria. These are detailed in Appendix 13 (Chapter 6) of the Course Handbook. The relevant marking criteria should be used to assess the particular example of clinical work submitted. Supervisor Evaluation of Clinical Competence Supervisors provide a recommended rating of ‘pass’, ‘conditional pass’ or ‘fail’ on the Supervisor Evaluation of Clinical Competence form. In most cases this rating is simply transferred to the summary sheet. In rare circumstances the supervisor recommendation may be over-ruled by the markers where the rating is in contravention of the criteria set out below. The criteria used for evaluation by Supervisors on the Supervisor Evaluation of Clinical Competence form are as follows:

104
Pass: This rating reflects a level of competence appropriate to the trainee’s stage in training. The trainee should have received ratings of at least average for his/her stage in training across most of the areas of competency. If the trainee has underperformed in any areas, this underperformance should be balanced by good performance across other areas, should not give rise to significant concern about the trainee’s overall competence, and there should have been evidence of progress over the duration of the placement in the areas of underperformance. Usually the trainee will have achieved the placement goals (unless due to lack of opportunity) and will be sufficiently competent to move on to the next stage of training. The trainee will have undertaken a reasonable workload and carried out the work competently. The trainee will have shown evidence of learning/progress over the duration of the placement. Conditional Pass: This rating indicates some concerns about the trainee’s competence and/or range of experience. This is likely to reflect underperformance across one or more areas, lack of progress across one or more areas, insufficient time spent on the placement to fulfil the gaols (e.g. due to extended periods of absence) or failure to carryout a sufficient range of work. A trainee given this rating may be given a ‘conditional pass’ for the placement, with requirements to undertake specific work in a subsequent placement and/or to demonstrate improvement in certain competencies during the next placement which bring the trainee back in line with the level expected relative to stage in training. Should the trainee fail to meet the specified targets, then s/he will be deemed to have failed the original placement. Fail: This rating indicates serious concerns about the trainee’s competence (not arising from lack of opportunity on the placement), in one or more areas. A fail rating will usually reflect at least one of the following:
1. Serious concerns in at least one area of clinical work 2. Persistent underperformance across several areas of work 3. Lack of evidence of learning and development over the duration of the placement 4. Serious concerns about aspects of professional behaviour 5. Serious concerns about use of supervision
6. Gross incompetence or negligence resulting in potential or actual harm to patients/clients or
the public, including failure to inform supervisor of critical actions/situations when this could
be reasonably expected.
7. Abuse of patients/clients: physical violence, verbal abuse or intimidation, exploitation for
financial or material gain, entering into a sexual relationship.
8. Other gross and/or persistent unprofessional conduct, including contravention of national or
local health service policy, British Psychological Society ethical and professional guidelines,
or Health Professions Council standards of conduct, performance and ethics.
A failure on the grounds of criteria 1 to 5 will usually result in the trainee being required to repeat all or some of the clinical placement. However only one placement may be repeated; two placement failures will therefore usually result in course failure and withdrawal of registration. Failure on the grounds of criteria 6 to 8 will usually result in direct withdrawal of registration and expulsion from the course, following appropriate investigatory procedures.
Overall Placement Outcome The ratings for the Example of Clinical Work, the Log of Clinical Experience and the Supervisor Evaluation of Clinical Competence are transferred to the summary assessment form, which follows. A placement may be evaluated as a pass, a pass with minor amendments, a conditional pass or a fail. Pass: This follows when all aspects of the placement are passed i.e. the Supervisor Evaluation of Clinical Competence, the Log of Clinical Experience and the Example of Clinical Work.

105
Pass with minor amendments: This follows when all aspects of the placement are passed but where minor corrections are required, for example, minor failures in anonymisation or changes required to how information is recorded in the Log of Clinical Experience. Conditional Pass: This will normally follow when The supervisor evaluation of clinical competence gives a conditional pass rating And/or The log of clinical experience is given a conditional pass due to an insufficient range or amount of experience and/or insufficient days having been completed on the placement. And/or The example of clinical work is given a fail rating. In the case of a conditional pass, the trainee will be required to fulfil certain requirements during the course of their next placement. Where the specified requirements are completed to the satisfaction of the original markers (and the Progression Board of Examiners) the trainee will be deemed to have passed the original placement. Where the specified requirements are not completed to the satisfaction of the original markers (and the Progression Board of Examiners) the trainee will be deemed to have failed the original placement. Fail: Placement failure will normally follow if:
the Log of Clinical Experience is failed due to a failure to show a sufficient range or amount of experience other than where this has resulted from the lack of opportunity provided by the clinical placement.
and / or
the Supervisor Evaluation of Clinical Competence gives an overall ‘fail’ rating and/or
the trainee is found guilty of Professional misconduct - Trainees are required to abide by the Health Professions Council and the British Psychological Society's Professional and practice guidelines at all times and ensure that their behaviour at no time, nor in any way, can be deemed as an act of professional misconduct or as professionally unsuitable. A failure to do so normally will result in instant dismissal with no possibility of repeating a placement or reassessment of work.
and/or
the trainee fails an example of clinical work upon resubmission The final decision regarding the overall outcome of a placement rests with the Progression Board of Examiners.

106
University of Hertfordshire Doctorate in Clinical Psychology
Clinical Placements
Summary Assessment Form
Trainee (or Code): Placement Type: Placement Period: Assessor: Submission date: Mark date(s): Supervisor ECC Log of Clinical Experience Example of Clinical Work OVERALL COMMENTS
Fail Conditional Pass with minor Pass
Pass amendments
[ ] [ ] [ ]
[ ] [ ] [ ] [ ]
[ ] [ ] [ ]
[ ] [ ] [ ] [ ]

107
University of Hertfordshire Doctorate in Clinical Psychology
Conditional Pass: Statement of Conditions
This form is completed by the trainee’s clinical tutor in the event that markers agree on an outcome of ‘conditional pass’ for a placement. When the trainee is informed of the outcome of the placement he/she will be given a copy of this statement of conditions. Where applicable, a copy will also be given to the supervisor who will be involved in supervising and assessing the work specified below. Name of Trainee: Placement: Date: Reasons for conditional pass (please specify what the reasons for the conditional pass are, including specific reference to areas of underperformance and/or lack of experience) Conditions for passing the placement (please provide a clear statement of what conditions the trainee must meet in order to pass the placement in question). Date by which conditions must be met: To be assessed by: Please note that the original two markers will formally evaluate the outcome and make a recommendation to the Progression Board of Examiners. Where the conditions include aspects of clinical competence, then the current supervisor may be asked to assess these and provide a recommendation for the consideration of the original markers. The final outcome rests with the Progression Board of examiners. Clinical Tutor: Signed:

108
University of Hertfordshire Doctorate in Clinical Psychology
Conditional Pass: Assessment of Outcome
Name of Trainee: Placement: Date: Conditions for passing the placement (copied from Statement of Conditions). Date by which conditions must be met: To be assessed by: Please note that the original two markers will formally evaluate the outcome and make a recommendation to the Progression Board of Examiners. Where the conditions include aspects of clinical competence, then the current supervisor may be asked to assess these and provide a recommendation for the consideration of the original markers. The final outcome rests with the Progression Board of Examiners. Recommended Outcome: Clinical Tutor: Signed:

109
Placement Marking Process
Pre-Submission Support: General guidance and advice from clinical tutor Supervision of work from Clinical Placement Supervisor.
Placement Documents & Example of Clinical Work 1
st Submission
Allocation to markers by Senior Clinical Tutor: EoCW: 1
st marker clinical tutor; 2
nd marker independent blind marker from Course Team
Placements: reviewed by clinical tutor (and 2nd
independent marker in the case of disagreement with supervisor recommended outcome).
Overall Outcome: Conditional Pass on Placement (or Fail if Placement Docs failed as well)
Marking Results: Examples of Clinical Work
EoCW: 1st marker: Pass & 2
nd marker:
Pass
EoCW: 1
st & 2
nd marker disagree
EoCW to External Examiner to confirm Fail
PASS on Example of Clinical Work
EoCW: 1
st marker Fail & 2
nd marker
Fail
Module leader facilitates discussion of outcome to reach agreement / suggests moderated outcome
FAIL on Example of Clinical Work
Work goes to EE to confirm moderated outcome.

110
Marking Results: Placement Documents
Senior clinical tutor facilitates discussion between the two reviewers to reach agreed outcome and if necessary suggests moderated outcome.
All Placement Documents & Clinical Tutor’s report to External Examiner to confirm Fail
2nd
marker confirms outcome recommended by Clinical Tutor
Work goes to EE to confirm
moderated outcome.
2nd
marker disagrees with outcome recommended by Clinical Tutor
Placement Documents: Supervisor: Pass Clinical tutor: Confirms pass
Placement Documents: Supervisor: Conditional Pass Clinical tutor: Confirms Conditional Pass
PASS on Placement Documents
Placement Documents: Supervisor: Fail Clinical Tutor: Confirms Fail
Placement Documents reviewed by blind independent 2
nd marker from the course
team.
FAIL on Placement Documents
Placement Documents: Clinical tutor does not agree with Supervisor recommendation for outcome and/or does not pass the Log
Conditional PASS on Placement Documents
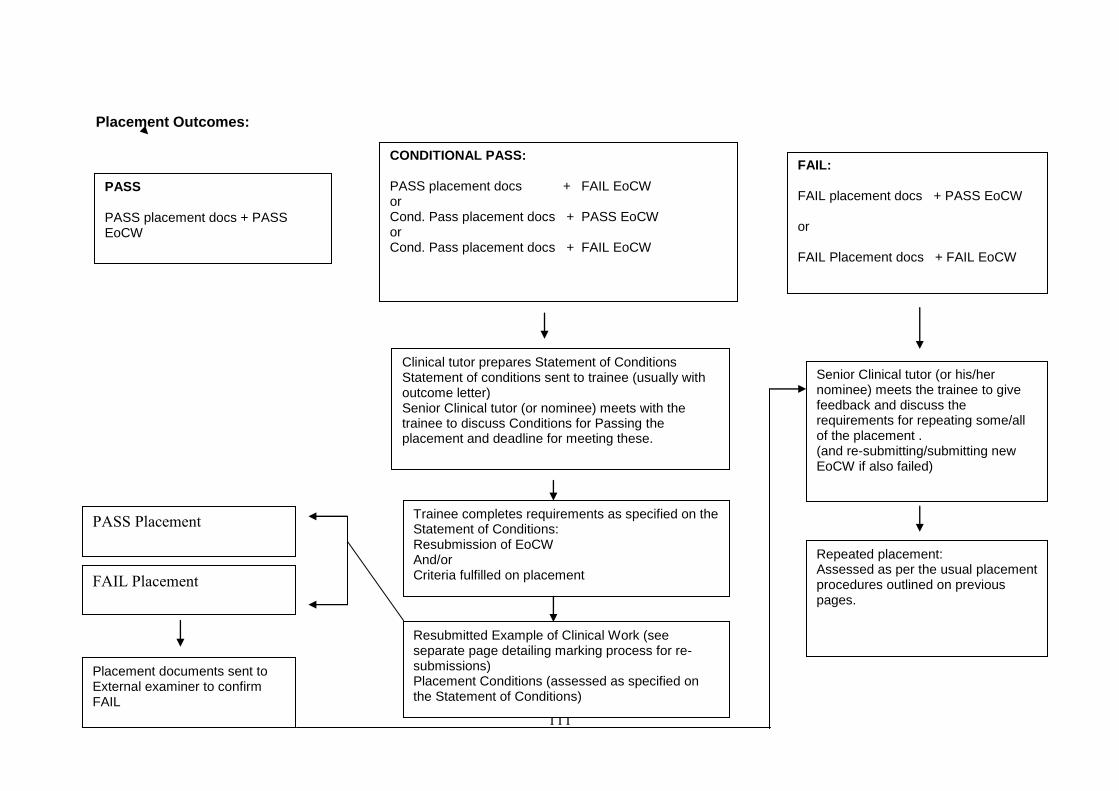
111
Placement Outcomes:
PASS PASS placement docs + PASS EoCW
CONDITIONAL PASS: PASS placement docs + FAIL EoCW or Cond. Pass placement docs + PASS EoCW or Cond. Pass placement docs + FAIL EoCW
FAIL: FAIL placement docs + PASS EoCW or FAIL Placement docs + FAIL EoCW
Clinical tutor prepares Statement of Conditions Statement of conditions sent to trainee (usually with outcome letter) Senior Clinical tutor (or nominee) meets with the trainee to discuss Conditions for Passing the placement and deadline for meeting these.
Senior Clinical tutor (or his/her nominee) meets the trainee to give feedback and discuss the requirements for repeating some/all of the placement . (and re-submitting/submitting new EoCW if also failed)
Trainee completes requirements as specified on the Statement of Conditions: Resubmission of EoCW And/or Criteria fulfilled on placement
Resubmitted Example of Clinical Work (see separate page detailing marking process for re-submissions) Placement Conditions (assessed as specified on the Statement of Conditions)
Repeated placement: Assessed as per the usual placement procedures outlined on previous pages.
PASS Placement
FAIL Placement
Placement documents sent to External examiner to confirm FAIL

112
Resubmission: Example of Clinical Work
Feedback meeting with Senior Clinical Tutor (or his/her nominee) - Discussion of feedback and of the amendments required - Confirmation of re-submission deadline - Feedback on one written draft before re-submission OR - Supervision on new example by Placement Supervisor
Re- submission of Example of Clinical Work along with covering sheet outlining the changes made (for resubmission) or indicating that it is a new piece of work.
Senior Clinical Tutor (or nominee): Re-submitted work sent back to the original markers along
with original mark sheets and summary of changes.
Marking Results
2 Passes: Both accept amendments as satisfactory
Disagreement as to whether amendments merit a pass 2 Fails: Both reject
amendments as insufficient
PASS SCT facilitates discussion of outcome to reach agreement / suggests moderated outcome.
FAIL
Work goes to EE to confirm outcome
Work goes to EE to confirm moderated outcome.

113
Appendix 14: Trainee Guidelines: Examples of Clinical Work
Guidelines: Examples of Clinical Work You are required to submit one example of your clinical work at the end of each placement period. You will therefore submit six examples in total by the end of your training. These examples form a part of the formal evaluation of your clinical competence. The example for each placement period must be submitted to the Course Administrator, along with the other placement related documents (the Log of Clinical Experience, the Supervisor Evaluation of Clinical Competence form, the Trainee Placement Feedback form and the Placement audit form) by the stated deadline. This is usually one week from the last day of the placement period. The example must include a cover sheet, which is signed by your supervisor
8, confirming that the work submitted
was completed by you on the placement, and that all necessary client consent (including written consent for recording of sessions) was obtained. You should submit two copies of the example, one of which must be anonymised for your identity, i.e. any information which identifies you should be removed and your work should be identified by student number alone. You are required to submit one of each of the following examples. You may choose in what order you wish to submit the examples, however you are required to submit one audio/video recording example for every academic year of the programme i.e. each year you will need to submit one of Examples 1, 2 or 3 below. The example should be a different case to the one you are writing up for your clinical case report. 1. An audio or video recording of an initial clinical interview 2. An audio or video recording of a therapy session 3. An audio or a video recording of a therapy session OR detailed process notes of a therapy session 4. One written piece of communication (report or letter) with a critical commentary. 5. A letter OR a transcript of a section of a tape in which formulation is used to facilitate a client’s understanding of his/her difficulties OR in which formulation is used to facilitate a family member’s understanding of a client’s difficulties. 6. A psychometric assessment report with a critical commentary.
Example 1: Audio/Video recording of an initial clinical interview You are required to submit either an audio recording or a video recording of an ‘intake’ assessment or an initial clinical interview. The interview may be with an individual client or with a family. The interview must be carried out by you independently. Please ensure that the recording is clearly audible by testing equipment prior to the interview. In the event that recording equipment is not readily available on placement, this may be borrowed from the School of Psychology technical support (via John Bain). It is preferable for audio recordings to be submitted in electronic format. In addition to the recording of the session, you are required to submit a written page(s), which includes the following: a. brief background information including the referral question (this should be no more than a paragraph); b. your pre-interview hypotheses and questions, and your plan for the interview (one or two paragraphs);
8 A cover sheet follows later in these guidelines.

114
c. a summary of what you thought were the salient points arising from the interview, as well as a comment on what information you may still be missing; d. your post-interview hypotheses and your plan of action (this might be for intervention or for further investigation). e. a brief reflection on what you thought were the strengths and weaknesses of the session, any thoughts on what you might have done differently. The written page(s) should usually be in the region of 800 to 1000 words long, with a maximum word limit of 1000 words. Examples 2&3: Audio or video recording of a therapy session (and/or detailed process notes) You are required to submit either an audio or a video recording of a therapy session conducted independently by you. In the case of family therapy, you must have taken the lead therapist role. For ONE of the two required recordings of a therapy session you may submit detailed process notes as an alternative; this option is aimed at those trainees who undertake a placement where the predominant theoretical model holds that recording of sessions is problematic. The submission of detailed process notes offers an alternative to a recording of a session; however this may only be done for one of the two required therapy recordings. Please ensure that the recording is clearly audible. In the event that recording equipment is not readily available on placement, this may be borrowed from the School of Psychology technical support (via John Bain). It is preferable for audio recordings to be submitted in electronic format. In addition to the recording of the session (or detailed process notes), you are required to submit a written page(s), which includes the following: a. brief overview of the client’s presenting problem and any key information about the client (one or two paragraphs); b. a summary of your formulation or understanding of the client’s difficulties and your plan for therapy (two or three paragraphs); d. the context of the recorded session (i.e. What session was it? What was being worked on at the time? Were there specific goals for this session? etc.); e. a brief reflection on what you thought were the strengths and weaknesses of the session, any thoughts on what you might have done differently. The written page(s) should usually be region of 800 to 1000 words long, with a maximum word limit of 1000 words. Example 4: Written communication with critical commentary You are required to submit an example of a written communication (i.e. report or letter). You will be assessed (amongst other things) on your skills in communicating psychological information in a form appropriate to the recipient and to the context. Along with the letter/report itself, you are required to submit a critical commentary on the written communication. In the critical commentary you should discuss your reasoning behind what you decided to include and exclude from the letter/report, as well as your choices pertaining to the structure and language of the communication. You may wish to include some reflection on any dilemmas you may have faced in making these decisions, as well as your thoughts about the relevant interpersonal and contextual factors involved. It is expected that your critical commentary will be in the region of 800 words long, with a maximum word limit of 1000 words. Example 5: Communication of formulation to a client or family member You should submit an example of yourself discussing/communicating a formulation either with a client or with a family member. The example may take the form of a letter written to a client or family member in which the main focus of the letter is the communication of a formulation to facilitate

115
understanding. Alternatively, the example may take the form of a transcript of a section of a session in which you discuss a formulation verbally with a client or family member. This example will be used to assess, amongst other things, your style of communicating with clients/family members, your ability to communicate psychological information to a client/family member in a constructive way and your ability to link psychological concepts with a client’s lived experience. You also are required to submit background information and a reflective commentary along with the letter or transcript. This should include: a. brief overview of the client’s presenting problem and any key information about the client (one or two paragraphs); b. a summary of your understanding of the client’s difficulties and your plan for treatment (or in the case of an assessment case, your recommendations); c. the context in which the communication of formulation took place (i.e. when in the process) and your goal in communicating the formulation; d. a short reflection on your communication, what you thought worked well, what you might say differently, whether you felt it was helpful. Your background/commentary page(s) should usually be between 800 and 1000 words long, with a maximum word limit of 1000 words. Example 6: Psychometric Assessment Report and critique of a test You must submit a copy of a full psychological report on an assessment you have undertaken on placement. The assessment must include the use of psychometric tests. In addition to the assessment report, you must submit a critical commentary which covers the following: a. a brief account of why you undertook the psychometric assessment and your rationale for choosing the assessment method and tests that you used (one or two paragraphs). b. a critique of one of the tests that you used; this should include consideration of issues such as the appropriateness of the test for use with this client in this context, the standardisation and reliability of the test, the different aspects of test validity (e.g. face validity, content validity, concurrent/predictive validity, conceptual validity, clinical validity). This should not merely be ‘lifted’ from the test manual but should demonstrate your own critical understanding of the issues involved in test selection. c. a brief reflection on what you see as the strengths and limitations of the report and/or the assessment itself(one or two paragraphs). It is expected that your critical commentary will be in the region of 800 to 1000 words long, with a maximum word limit of 1000 words. Consent and Confidentiality All identifying information must be removed from the examples of clinical work that you submit. This includes both the client’s details and those of colleagues. In the case of a letter therefore, you would delete all of the client’s identifying information as well as the name and address of the person to whom you are writing, and any details of the location where you saw the client. You need to obtain explicit written consent from your client(s) in advance if you intend to record your sessions. This should be discussed with your supervisor. There may be Trust procedures that need to be completed before clients are recorded on audio or video. Your supervisor may have a template consent form, which is appropriate for you to use. As with obtaining consent to participate in research or consent to treatment, clients need to be given sufficient information and time to make an informed decision. Clients must also understand that the choice to withhold their consent to recording will not affect their access to services. If the Trust consent form for recording does not include mention of the recordings being submitted for examination purposes, then you need to obtain consent specifically for this. All identifying information should be erased from recordings submitted for examination as far as is possible. By its very nature the client’s identity cannot be hidden completely in a recording. It is therefore crucial that recordings are kept secure and confidential and that the material is only seen by those who have explicit consent from the client to do so (e.g. the trainee, the clinical supervisor, and the examiners). Recordings must

116
be kept secure and should be deleted after use (Refer to the Guidelines on Consent in Appendix 14). Note that any signed client consent forms should be retained in the client’s NHS file, and not submitted with your recordings, as they would obviously compromise confidentiality. Please note that written material submitted for examination purposes is kept securely on UH premises for 5 years after the trainee qualifies; however, recordings are destroyed upon the trainee’s graduation.

117
University of Hertfordshire Doctorate in Clinical Psychology
Examples of Clinical Work – Cover Sheet
Trainee
Placement
Placement Dates
Placement number 1 2 3 4 5 6
Location
Supervisor
Example of Clinical Work: For recordings and transcripts: I confirm that I have obtained informed written consent to record the material presented and for the use of this recording for examination purposes.
Trainee’s signature: Date:
I confirm that the client has given informed written consent to record the material presented and for the use of this recording for examination purposes.
Supervisors Signature: Date:
For all examples of clinical work: I agree that the example of my clinical work listed above and submitted with this form is a reflection of my work while undertaking this placement, and that consent and anonymisation have been addressed as appropriate. Trainees Signature: Date:
I agree that the example of clinical work listed above and submitted with this form is a fair reflection of ……………………………..’s clinical work while undertaking this placement, and that consent and anonymisation have been addressed as appropriate.
Supervisors Signature: Date:

118
Ratings of Initial Interviews Recorded on Audio or Video Tape
Trainee: Date:
Supervisor: Rater:
Please provide ratings for the following aspects of the recorded session. These ratings should inform
your overall rating; however the overall pass fail rating should reflect your judgement as to whether
the competencies demonstrated by the trainee in the recorded session and covering page are
appropriate to his/her stage in training. Please provide qualitative comments to support your overall
rating.
Session Content
YES NO OTHER (specify)
Appropriate introductions and sets up the session e.g.
explaining confidentiality, note taking, purpose of interview etc.
Explores the presenting problem(s) e.g. nature of the difficulty,
frequency, intensity, duration, impact etc.
Obtains history of presenting problem e.g. triggers, onset,
course, previous treatment/help etc.
Obtains background and contextual info on client(s) e.g.
development, family, current relationships, occupation/ school,
significant life events etc.
Explores other relevant information as appropriate (e.g. risk
relevant medical history, substance use etc.)
Elicits client’s strengths/ resources
Gives feedback on preliminary formulation and/or plan (incl.
discussion of reports/ letters and/or plans for future
appointments)
Trainee Characteristics
YES NO OTHER (specify)
Uses appropriate style of questioning
Communication appropriate to client(s) ability/age
Summarizes
Listens reflectively
Is empathic
Is genuine
Expresses appropriate non-contingent warmth
Is non-judgemental

119
Covering Page
Absent Poor Satisfactory Good
Pre-interview hypotheses and plan
Summary of salient information
Post-interview hypotheses and plan
Reflection on session
Appropriately anonymised (in written commentary)?
YES NO
Comments: Overall rating: Pass Pass with Minor Amendments Fail

120
Ratings of Therapy Interviews Recorded on Audio or Video
Trainee: Date:
Supervisor: Rater:
Please provide ratings for the following aspects of the recorded session. These ratings should inform
your overall rating; however the overall pass fail rating should reflect your judgement as to whether
the competencies demonstrated by the trainee in the recorded session and covering page are
appropriate to his/her stage in training. Please provide qualitative comments to support your overall
rating.
Session Content / Trainee Skills
YES NO OTHER (specify)
Evidence of appropriate use of a therapeutic model
Technical skills in keeping with the theoretical model
Demonstrates skills in developing and maintaining therapeutic
alliance
Structure and content of the session consistent with stated
formulation, therapy plan and session plan
Appropriate use of silences/appropriate pacing of the session
Does the trainee demonstrate some unconditional positive
regard during the session?
Does the trainee demonstrate therapeutic congruence in
speech and behaviour during the session?
Does the trainee demonstrate a development of accurate
empathic understanding during the session?
Does the trainee demonstrate an appropriate level of mirroring
of material and summarising during the session?
Covering Page
Absent Poor Satisfactory Good
Formulation and overall therapy plan
Session context and plan
Reflection on session

121
Appropriately anonymised (in written commentary)?
YES NO
Comments: Overall rating: Pass Pass with Minor Amendments Fail

122
Ratings of Process Notes
Trainee: Date:
Supervisor: Rater:
Please provide ratings for the following aspects of the process notes and the accompanying covering
page. These ratings should inform your overall rating; however the overall pass fail rating should
reflect your judgement as to whether the competencies demonstrated by the trainee in the report and
critique are appropriate to his/her stage in training. Please provide qualitative comments to support
your overall rating.
Process Notes:
YES NO OTHER (specify)
The notes are fully and clearly presented with appropriate
detail
The notes pay attention to the whole therapeutic situation,
including
client’s appearance, manner and non-verbal behaviours, as
well as
their verbal interactions.
Notes show evidence of skills in keeping with the therapeutic
model
(For example if working psychodynamically, a capacity to work
with the
client’s unconscious as well as conscious processes, and a
capacity to
work within the transference)
Interventions/ psychodynamic interpretations are appropriate
to the clinical
material presented and closely follow that material
Notes show evidence of appropriate timing of interpretations /
interventions
Notes show evidence of appropriate emotional response to
client /
Interpretations appropriate to the client’s level of affect
The notes show the trainee’s ability to reflect on their own
counter-transference responses to the client
Covering Page
Absent Poor Satisfactory Good
Formulation and overall therapy plan
Session context and plan
Reflection on session

123
Appropriately anonymised?
YES NO
Comments: Overall rating: Pass Pass with Minor Amendments Fail

124
Ratings of letter or transcript of section of session communicating formulation to client or family member
Trainee: Date:
Supervisor: Rater
Please provide ratings for the following aspects of the transcript or letter. These ratings should inform
your overall rating; however the overall pass fail rating should reflect your judgement as to whether
the competencies demonstrated by the trainee in the transcript or letter are appropriate to his/her
stage in training. Please provide qualitative comments to support your overall rating.
Transcript/letter
YES NO OTHER (specify)
Uses appropriate language (i.e. appropriate to the recipient
Formulation is coherent (i.e makes ‘psychological sense’)
Evidence of supporting theory
Formulation is client focussed rather than model focussed
Feedback given to client/family member is appropriately
tentative and sensitively communicated
Communication conveys appropriate empathy/warmth
Is responsive to feedback from recipient (transcripts
Letter free of grammatical and spelling errors
Appropriately anonnymised
Covering page
Absent Poor Satisfactory Good
Brief background/contextual information
Understanding of client’s problem and appropriateness of
plan
Reflective commentary on letter/transcript

125
Comments:
Overall rating: Pass Pass with Minor Amendments Fail

126
Ratings of letter or report with critical commentary
Trainee: Date:
Supervisor: Rater
Please provide ratings for the following aspects of the letter/report and critical commentary. These
ratings should inform your overall rating; however the overall pass fail rating should reflect your
judgement as to whether the competencies demonstrated by the trainee in the letter/report and critical
commentary are appropriate to his/her stage in training. Please provide qualitative comments to
support your overall rating.
Letter/Report
YES NO OTHER (specify)
Language used is appropriate to recipient
Content is appropriate to recipient & to purpose of the
letter/report
Report/letter is well structured and follows a logical sequence
Letter/report is free of grammatical and spelling errors
Appropriately anonymised
Critical Commentary
Absent Poor Satisfactory Good
Rationale for structure/language
Rationale for content
Discussion of issues of context
Reflection
Comments
Overall rating: Pass Pass with Minor Amendments Fail

127
Ratings of Psychometric Assessment Reports
Trainee: Date:
Supervisor: Rater:
Please provide ratings for the following aspects of the report and critique. These ratings should inform
your overall rating; however the overall pass fail rating should reflect your judgement as to whether
the competencies demonstrated by the trainee in the report and critique are appropriate to his/her
stage in training. Please provide qualitative comments to support your overall rating.
Report Content and Structure
YES NO OTHER (specify)
Uses appropriate language
Explains technical terms
Report free of grammatical and spelling errors
Makes use of sub-headings
Includes information on reason for referral and presenting problem
Includes history/background information
Includes information on testing process/behaviour during testing
Includes appropriate description of tests used
Includes results of testing(appropriately reported)
Includes interpretation of results
Includes appropriate summary
Includes appropriate conclusions
and recommendations
Includes cautionary notes on the limitations
of testing
Appropriately anonymised

128
Critical Commentary
Absent Poor Satisfactory Good
Rationale for the assessment
Reflective comments of the report and/or assessment
Critique of specific test:
Discusses test development & standardisation
Discusses reliability
Discusses validity (e.g. criterion-related validity, face
validity, clinical validity, construct validity)
Provides justification for use
Discussion of alternative test/assessment methods
Discusses issues relating to conceptual validity
Comments: Overall rating: Pass Pass with Minor Amendments Fail

129
Appendix 15: Guidelines on Consent
Guidelines on Consent All trainees and clinical placement supervisors are expected to abide by the Guidelines for the Professional Practice of Clinical Psychology (DCP, 1995, revised 2001) as well as the other relevant British Psychological Society and Health Professions Council codes of conduct, performance and ethics. The following should be considered in conjunction with the aforementioned DCP guidelines, as well as the BPS and HPC codes of conduct, performance and ethics. The following sections of the Guidelines for the Professional Practice of Clinical Psychology (DCP, 1995, revised 2001) are of particular relevance: Chapter 4 – Informed consent Chapter 6 – Confidentiality Chapter 9- Teaching, training and supervision Consent to assessment/treatment by a trainee Trainees need to inform their clients that they are trainees, and what the implications of their being a trainee are. Clients should be told that the trainee will discuss information about them with their supervisor in confidence and that information about them may be used anonymously in case reports or case presentations for examination purposes only. It should be made clear that this would always be anonymous and that the trainee would discuss the use of material with them beforehand to get their consent. It is recommended that trainees discuss informing clients of their training status with their supervisors before commencing work with a client and consider how best to address this issue, giving appropriate consideration to potential impact on the therapeutic process, the ethical requirements and any relevant Trust policies. Psychology departments who take trainees on a regular basis may consider having a standard letter or information sheet, which may be sent to clients in advance of their seeing a trainee. The advantages and disadvantages of this approach may differ depending on the nature of the service, therefore psychology departments should consider what is most appropriate in their particular context. An example of one such information sheet is attached for information. Consent to material being written up as a case report, example of clinical work or presented as a clinical presentation It is recommended that when trainees inform clients of their training status and obtain the client’s consent to treatment, they also mention the possibility of material being used anonymously for examination purposes. Should a trainee then wish to write-up/present a particular piece of work, s/he should discuss this with the client, being sure to provide the client with all of the necessary information about anonymity and access to the information. The trainee should then obtain the client’s consent to this (assuming the client is willing to consent). It is preferable for written consent to be obtained, however this should be discussed with the placement supervisor and appropriate consideration given to the potential impact on the client and the therapeutic process, ethical guidelines and any relevant Trust requirements. Any material presented or written up as a clinical case report or example of clinical work must be anonymous. All identifying information must be removed including names, addresses, specific place references and any other information that may compromise the anonymity of the client. Consent to video taping and/or audio taping sessions It is an ethical requirement that trainees must obtain clients’ written informed consent before audio or video taping their interactions with them. Clients should receive written information about the recording of sessions before they are asked to give their consent. Information must include who will have access to the recording, what the purpose of the recordings is (e.g. supervision or examination),

130
how long the tapes will be kept and when they will be erased, and that the client has the right to withdraw consent. Point 6.1.5 of the DCP Professional Practice Guidelines (1995, p30) refers. Trainees should discuss obtaining consent to recording of sessions with their placement supervisor in the first instance, as there may also be additional Trust policies on recording interactions with clients, which would need to be adhered to. An example of a consent form and information sheet relating specifically to recording for supervision and examination purposes is attached for information. Capacity to provide consent If a client is unable to provide their informed consent in any of the circumstances described above, consent should be obtained from an appropriate key worker and/or family member. Trainees should discuss this with their placement supervisor to identify the most appropriate person, and decisions must comply with existing Trust policies on consent.

131
EXAMPLE
Information for Clients about Trainee Clinical Psychologists
Working in Our Service You have recently been offered an appointment to see a Trainee Clinical Psychologist. This information sheet provides some information about Trainee Clinical Psychologists and what it will mean for you to see a Trainee Clinical Psychologist in our service. A Trainee Clinical Psychologist has a degree in Psychology and has usually worked as an Assistant Psychologist for some years before being accepted onto a Clinical Psychology training course. The Clinical Psychology Training Course is a three-year doctorate, and Trainee Clinical Psychologists spend some of their time at the university and more than half of their time working on placement in the NHS. We believe that it is essential to assist with the training of Clinical Psychologists to work in the NHS and so we offer placements within our service for Clinical Psychologists in Training. Trainee Clinical Psychologists are closely supervised by a qualified and experienced Clinical Psychologist. Sometimes you might be asked if the supervisor can sit in on your session to observe the trainee. You might also be asked for your consent to record (on audio or video tape) sessions so that the supervisor may review the Trainee Clinical Psychologist’s skills and progress. You may choose not to give your consent if you do not wish to have sessions recorded. As a part of their training, Trainee Clinical Psychologists may be required to present some of their casework for teaching or examination purposes. The Trainee Clinical Psychologist would discuss this with you first. If you have any questions, your Psychologist should be able to answer these at your first appointment. Alternatively you may call [the psychologist or head of department] on [telephone number].

132
EXAMPLE
INFORMATION FOR CLIENTS ABOUT THE USE OF VIDEO & AUDIO TAPES
WHY TAPE SESSIONS? We make videotapes and audiotapes of clinical work, where possible, as it can be very helpful in our work. Videotapes and audiotapes allow us to look over or listen to an interview in detail, so we can think more about the clients and about our work with them. We also sometimes use tapes for supervision and teaching. When we have trainee therapists working in our service it can be especially useful for them to tape their sessions so that their clinical supervisor may review their sessions with them and help them to learn and improve their skills. Sometimes trainees may ask for permission to record a session to submit for examination purposes. Tapes submitted for examination purposes will only be heard by the examiners, who are Clinical Psychologists and are bound by the rules of confidentiality. CONSENT Although we find videotaping and/or audiotaping helps us in our work, we also want to make clear that everyone has the right to refuse permission. If you agree to recordings being made we will ask you to sign a consent form. You have the right at any time to ask that all the recordings be erased. CONFIDENTIALITY Videotapes and audiotapes are treated as confidential records. This means that they are kept secure and that only those for whom you have given permission to see/hear the tape will be entitled to do so. We undertake to safeguard tapes at all times. If you only give permission for the recordings to be used for clinical and supervision purposes, the tapes will be erased after your treatment has finished. If you give consent for the tapes to be used for examination purposes, tapes will be kept securely locked in the offices of the Doctor of Clinical Psychology training course at the university. Tapes submitted for examination purposes will be erased after the trainee graduates. This means that the tape is not usually kept for more that 3 years.

133
EXAMPLE
CONSENT FORM FOR VIDEO/AUDIO RECORDING OF THERAPY SESSIONS
FOR SUPERVISION PURPOSES: The undersigned trainee Clinical Psychologist has explained the purposes for recording my/our therapy sessions. I/we understand that even after giving my/our consent to the recording. I/we can ask for all recordings to be erased at any time during or after completion of the therapy. I/we have been assured that confidentiality will be preserved. It is made clear that it is totally up to me/us whether or not to decide to agree to the sessions being recorded. I/we will be treated in the same way, whether or not I/we choose to have my/our sessions recorded. It is on this basis that I/we give consent for my /our treatment to be recorded. The recordings may be shown to/heard by the undersigned trainee Clinical Psychologist and his/her clinical Supervisor for purposes directly related to my treatment and to the supervision of the undersigned trainee Clinical Psychologist. If consent is given for the recordings only to be used for clinical and supervision purposes the tapes will be erased after the treatment has finished. Name of ______________________________________________________________ Signature____________________________________________________________ Date____________________ Name_______________________________________________________________ Signature____________________________________________________________ Date____________________
Name of Trainee Clinical Psychologist: Signature: Date: Name of supervising Clinical Psychologist: Signature:
Date:

134
EXAMPLE
CONSENT FORM FOR VIDEO/AUDIO RECORDING OF THERAPY SESSIONS
FOR EXAMINATION PURPOSES: The undersigned trainee Clinical Psychologist has explained the purposes for recording my/our therapy sessions. I/we understand that even after giving my/our consent to the recording. I/we can ask for all recordings to be erased at any time during or after completion of the therapy. I/we have been assured that confidentiality will be preserved. It is made clear that it is totally up to me/us whether or not to decide to agree to the sessions being recorded. I/we will be treated in the same way, whether or not I/we choose to have my/our sessions recorded. It is on this basis that I/we give consent for my /our treatment to be recorded. The recordings may be shown to/heard by the undersigned trainee Clinical Psychologist and to the examiners who will be qualified Clinical Psychologists. I/we understand that recordings submitted for examination purposes will be kept securely at the University and that recordings will be erased after the undersigned trainee Clinical Psychologist graduates (usually a maximum of 3 years from the time of recording). Name of ______________________________________________________________ Signature____________________________________________________________ Date____________________ Name_______________________________________________________________ Signature____________________________________________________________ Date____________________
Name of Trainee Clinical Psychologist: Signature: Date: Name of supervising Clinical Psychologist: Signature: Date:

135
Appendix 16: Trainee Guidelines: Clinical Case Reports
Requirements & Guidelines: Clinical Case Reports
Part A: General Information about Case Reports Aims of Case Reports Case reports are intended to give you the opportunity to demonstrate:
a) your developing clinical competence across a range of different types of work and setting, and in the context of a range of theoretical perspectives b) your ability to integrate academic and theoretical ideas with your clinical experience c) your ability to reflect on the way in which clinical, professional, ethical and wider social contexts interact and impact on your work
This follows directly from the Core Competences set out by the BPS and HPC to guide training of Clinical Psychologists. Because these competences are central to the psychologist's role, the course uses case reports as a measure of your development, and as one of the indicators of your capacity to function as an HPC registered Clinical Psychologist. Requirements Four case reports are submitted over the course of the training, and these are included in the final portfolio of work. Deadlines are included in the timetable for each year and, unless otherwise specified, are three weeks after the last day of the placement. Case reports will usually reflect work carried out during the most recent placement, but exceptions may appropriate in some circumstances, and should be discussed with the clinical tutor. A submitted Example of Clinical Work and a Clinical Case Report should not reflect work on the same case. As the case reports are intended to allow you to demonstrate a range of clinical competences and experiences, the 4 reports submitted must differ in terms of the type of report, nature of the clinical work reported, presentations problems and the clients themselves. Types of Case Report The following types of case report are to be submitted (not necessarily in this order):
i. Report of a psychometric assessment ii. Report of an individual therapy case iii. Report of therapy with a couple OR a family OR a group iv. Report of an indirect intervention OR consultation
Detailed guidelines for each of these are given in Section B. Although you may choose the order in which to tackle these different types of report, some are generally more suited to later stages of training. You should therefore discuss your selection of case report with your clinical tutor. Breadth of Content The material presented across the four case reports should represent a range of clinical experience in terms of the clients, contexts, clinical presentations and approaches taken. The portfolio of reports must therefore include: a) A range of cases drawn from across the lifespan: This is defined as at least:
one case of work with a child (under 16)
one case with a working-age adult (between 16/18 and 60)
one case with an adult in later life (aged 60+)

136
These age-bands indicate the spread of ages required, and are not intended to be interpreted rigidly. The important point is that cases should be chosen to show competence in working with individuals across the life-span, and the different developmental issues that are pertinent in this work. b) A range of severity, chronicity of presentation and communication ability: The meaning of terms such as severity and chronicity may vary across different client contexts, but the portfolio of cases should describe individuals with a range of presenting problems – from acute onset through to serious and enduring presentations. At least one report should present a psychological intervention with an individual who has difficulty in expressing their needs verbally (for example, because of their level of psychological disturbance, because of neurological problems such as severe dementia or brain injury, or because of intellectual disability). c) A range of psychological approaches:
You should be able to demonstrate competence in more than one model of formal psychological therapy. Bear in mind that in this context ‘model’ is a reference to broad approaches – eg, cognitive-behavioural, constructivist, psychodynamic, systemic, humanistic, or integrationist. On this basis, breadth would not be represented by variations on cognitive approaches, or by Kleinian as contrasted to Freudian modes of psychodynamic therapy. d) Different settings Where possible, it is desirable that more than one type of work setting is reported on (eg, community team, primary care, inpatient psychiatric unit, medical setting). At least one report should relate to work undertaken in the context of inter-professional working. Covering this range of presentations is a major factor in selecting your four cases. Although this may seem like a large number of criteria to meet in only 4 reports, remember that any one report will cover more than one of the criteria described above. In order to ensure that these requirements are achieved, you should discuss the appropriateness of cases with your course tutor before you start writing reports. Cases that you have carried out jointly with someone else are not usually appropriate. You must have carried out an identifiable piece of work independently. A client seen jointly by yourself and your supervisor for assessment and therapy would not be appropriate. However a client seen individually by you and in a group by another therapist would be acceptable. One further factor to consider…Although the case reports are designed to demonstrate your clinical competence as well as ability to combine theory with practice, this does not mean that the piece of clinical work presented in the report need necessarily have been “straightforward”, successful or even completed. Rather, you should aim to demonstrate that difficulties have been reflected on and dealt with appropriately. Reporting on more complex and challenging cases or unsuccessful interventions often provides more opportunity for you to demonstrate your ability to problem-solve and think about problems from different perspectives, as well as providing rich material to critique and reflect on learning points. Length and Presentation of Reports Reports should be typed and referenced following the BPS Style Guide (in the Appendix section of this handbook), and each page numbered. The cover sheet should include the title of the case report in two respects: the number in your series of four reports (ie, “Case Report 1” being the first submitted); and the type of report (eg, Report of Therapy with a Family). This is essential, as the marking criteria for examiners are different for different types of report. You must indicate your student number on the cover of your case report and at the bottom/top of each page; you should not put your name on your case report. The cover sheet must also state the word count. The word limit for case reports is 5000 words, excluding references and appendices, and in the case of a Process Report, the transcript. Details of material suitable for appendices can be found below. You should not attempt to circumvent the word limit by putting other material in the appendices. Please refer to the course policy for written work which is submitted over the word limit, in chapter 4 of this handbook.

137
An electronic copy of each report should be submitted via Studynet, in addition to 2 hard copies. You should also retain a hard copy of each report as well as an electronic back-up copy. All copies must be fully anonymised for blind marking (i.e. all details that may identify you as the author should be removed). Confidentiality and Consent It is essential that nobody reading the case report should be able to work out the identity of your client. This means that you must delete any reference to your own identity, the identity of the clients, or any professionals, services or institutions to which you refer (including Trust logo / headed paper in appended letters and reports). In order to protect the identity of your clients, you may need to go further than simply changing or removing names. Some details of the history (for example size of family, ages and sex of family members, occupations, timing of problem onset, specific details of the problem) may provide identifying information to somebody reading the work. This risk increases if you include a lot of specific details which, taken together, could add up to hint at a client's identity. You should include only necessary items of demographic and clinical information, and take appropriate steps to disguise some of it, while ensuring that you do not distort relevant issues. For example, you should always remove a client’s precise date of birth but need to report the client’s age in years (and in the case of some psychometric assessments, sometimes of months), as this is often highly relevant in understanding their presentation. You need to get the balance between giving the minimum information needed to grasp the pertinent issues, while not depriving the reader of important details. If the nature of the case is such that it is impossible to protect confidentiality then it will unsuitable for writing up as a report. You are required to obtain all clients’ consent to write up your work with them in a case report. This must be informed consent: therefore you must provide the client with sufficient information about the nature of the information that will be presented in the report, and who will have access to the report. Where audiotape or videotape of a meeting is to be submitted, written consent must be given by clients, using either the standard form provided in this handbook by the course for this purpose (see Appendix 14), or the standard form provided by the placement Trust. Note that any signed client consent forms should be retained in the client’s NHS file, and not submitted with your case report, as they would obviously compromise confidentiality. Note that written material is kept securely on UH premises for 5 years after a trainee qualifies; however, recordings are destroyed upon the trainee’s graduation. Involving your clinical supervisor You may wish to show a first draft of your report to your clinical supervisor, since s/he will be familiar with the case you are presenting, and may be able to give valuable feedback. Confirming Consent and the Contents of Case Report You will be expected to sign a standard covering page for your clinical case report. This confirms that the work is your own work and that you have obtained appropriate consent from the client. A copy of the covering page may be found at the end of Part A of the guidelines. Only one covering page needs to be included with the two hard copies of your case report, which you submit for marking. General Guidelines on Structure and Content Because the nature of case reports varies widely, no one structure will fit all. In structuring each report, you should consider its aims and the detailed guidance for the different types of reports given below in Part B. You should also consider the marking guidelines given to examiners for each type of case report. However, some general points apply to most reports. You should begin with an introduction, which briefly sets out the main clinical and conceptual issues with which the report is concerned, and outlines the material to be covered. The examiners marking the case report will not be familiar with where you have been working or any of the details of the case. It is therefore necessary for you to provide sufficient information for the examiner to follow the rationale for what you did, why and how.
138
Information about the client(s) provided at the outset should include age, sex and cultural background. If you are outlining the assessment of the problem, consider what aspects of the history and what relevant background information the reader needs. Try to be concise, but include enough detail so that the reader is supplied with all the basic facts they need at an early stage (rather than embedding relevant material at a later point). Try to be clear about the source of “facts” presented - eg, “Mary told me that she thought John had become depressed last year” rather than “John became depressed last year”; or where you are stating your opinion; and where your opinion differs from the client's view or that of fellow-professionals. Formulation
9 of the case should be as comprehensive as possible, though a number of reports start
with a set of preliminary hypotheses, which are elaborated into a formulation later in the report. Formulations should fit with the history, and (as far as possible) explain how the problem developed, what is maintaining it, and (by implication) how it might change. Psychological theory and relevant literature should inform both your hypotheses and your formulation. It is important that formulations and the report show some coherence in relation to the model you are using. For example, a psychodynamic formulation followed by a behavioural intervention might be difficult to justify. Equally inappropriate would be a report in which an intervention which claimed to represent one modality actually used techniques from an alternative approach, without acknowledging this as an issue. Discussion of the intervention should try to show how the formulation and the intervention link together in a 'dynamic' manner. This usually means selecting relevant (i.e. illustrative) clinical material, and limiting yourself to details that are strictly necessary to showing your developing understanding of the case. You should include any methods you used to evaluate your work, and any numerical data you collected. Raw data is usually included in an appendix. The concluding discussion depends on the type of report you have written, but should usually include some reflection on the work that you have done. This reflection can include consideration of wider issues raised by the case and its impact on you, as well as an appropriately critical appraisal. In this context ‘appropriate’ means that you should not invent criticism for the sake of it! If you include suggestions about other ways in which the case could have been approached or managed, try to make sure that these are realistic (and not a ‘wish-list’ of alternative approaches). All letters, reports etc that you have written regarding the client(s) must be included in the appendices. (Any potential difficulty with this – eg, in the case of a large group with many clients - should be discussed with the clinical tutor.) Quality of writing, grammar and spelling Case reports are submitted as part of the portfolio of work submitted for doctoral examination. There is therefore an expectation that reports are written to doctoral standards – the writing should be clear, with few spelling or grammatical errors. Although content is the main focus, you will be required to revise reports which contain a large number of grammatical or spelling errors.
9 There are several references that may be helpful in providing some guidance on formulation. For example:
Johnstone, L. & Dallos, R. (Eds) (2006). Formulation in psychology and psychotherapy : making sense
of people’s problems, London: Routledge.
Eels, T. (Ed) (1997). Handbook of Psychotherapy Case Formulation. New York: Guildford.
Butler, G. (1998). Clinical formulation. In: A.G.Bellack and M.Hersen (Eds) Comprehensive Clinical
Psychology, Elsevier.

139
University of Hertfordshire Doctorate in Clinical Psychology
Clinical Case Report Cover Sheet
Trainee number
Submission date
Placement
Case report number (1-4)
1 2 3 4
Case report type eg, Type 3b: report of a group intervention
1 2 3a 3b 4
Client group
Main Psychological Models used in clinical work and/or during formulation / report
□ I confirm that the clinical case report submitted with this form is based on my own independent clinical work while undertaking this placement.
□ I confirm that I have obtained informed consent from the client(s) concerned,
and that this is recorded in the client’s clinical notes.
□ I confirm that all information that could identify the client(s) or service has been removed from the Clinical Case Report and from the Appendices.
Trainee’s Signature: Date:

140
Requirements & Guidelines: Clinical Case Reports Part B: Guidelines for the Format of Reports CASE REPORT TYPE 1: REPORT OF PSYCHOMETRIC ASSESSMENT CASE Aim The aim of this report is to describe your assessment of an individual client, and the clinical thinking behind this. This should reflect the scientist-practitioner and reflective-practitioner models, incorporating a cycle of planning, assessment, formulation, and recommendations, and (importantly) your learning as a result of this process. What the examiners are looking for A major focus of the report should be on presenting your clinical thinking in your work. This should include clear presentation of the considerations which led you to make specific choices at specific times (eg, in selecting the particular assessment instruments) and of your understanding of the case. Given the word count, you should present the salient details which enable the reader to understand and evaluate the clinical decisions, interpretations and recommendations that you made from this information, integrated with theory, research and any other information you feel to have been relevant. Although the examiners will want to assess the competence of your decisions (and hence your clinical work), this does not imply that every action reported on needs to be “right”: it is entirely appropriate to report on, for example, difficulties in the assessment process or the need to pursue additional information following your first phase of assessment. Type of material Any psychometric assessment that you have conducted independently with an individual client, whatever its outcome, may be presented. In almost all cases, you will have conducted the entire assessment yourself. (An exception to this would be for services which routinely make use of multi-professional assessment interviews in the first phase of assessment). The assessment should be completed at the time of writing the case report, although the case may still be open to you or to a colleague (for example, when the assessment resulted in a recommended intervention). Suggested Structure and Content The examiners marking the case report will not be familiar with where you have been working or any of the details of the case. It is therefore necessary for you to provide sufficient information for the examiner to follow the rationale for what you did, and how you did it. It is important that you present the case in a logical sequence. Although the structure will vary depending on the particular nature of the assessment, a possible structure for the case report might be:
Referral
Preliminary (pre-assessment) Hypotheses
Assessment Plan
Clinical Interview & Collateral Information
Psychometric Testing
Results
Interpretation (bearing in mind any process, clinical or behavioural issues that may have affected the results)
Formulation (combining the results of the testing with clinical, historical, familial and any other relevant information, and drawing on psychological and neuropsychological theory where appropriate).

141
Recommendations
Critical review & Evidence of Learning and Self-Reflection
References and Appendices Referral In this section you give a brief account of how the case came to be referred to the service and/or how the client came to be seen by you. Brief details of the services involved may also be relevant here. Preliminary Hypotheses These would follow from the referral, and any additional information you have (eg, about the services involved) prior to your assessment. Your assessment plan should then follow logically from your ideas about how to test out these hypotheses. Assessment plan In this section you describe your assessment plan and your rationale for the plan. You would be expected to link this to your initial working hypotheses or questions arising from the referral. It may be appropriate to refer to relevant theory, research or professional guidelines (e.g. SIGs, NSFs, NICE). Clinical Interview & Collateral Information In most cases you would have information other than that obtained through the formal testing process. This might be information from a direct interview with the client and/ or from an interview with a carer. You might also have information obtained from other sources, for example, from medical records or previous assessments. The specific details of the case in question will dictate the exact order of these sections and whether they need to be subdivided. Where you have a lot of collateral information, you will need to consider what the most salient details are, as it is unlikely that you will be able to present all of the information given the word limit, and some information may compromise the client’s anonymity. Psychometric Testing In this section you would describe what you did, the tests you used and why you chose them. You will need to make reference to relevant literature in justifying your choice of tests, even if you are following a standard procedure in your service setting. You should also describe any relevant aspects of the process of assessment, for example, whether the assessment was carried out over more than one session, the testing conditions, and relevant aspects of the client’s behaviour – including environmental and clinical information that may have influenced the client’s performance on tests. Results In this section you would present the test results. It is usually best to present results in a form that enables the reader to interpret the meaning of the results, for example, by presenting percentiles or z-scores rather than raw scores. You should note what norms you have used and whether the standardisation sample is appropriate. Any actual data or examples of tests should be included (anonymised) in the appendices where appropriate. Formulation In this section you should provide your understanding of the case and your hypotheses. Your formulation in a psychometric case should not be dissimilar from any other formulation, and provides the opportunity to consider the various interacting factors that might explain the client’s current difficulties. This section provides the opportunity to make links between psychological theory and your findings and observations. Your formulation should follow from your findings. It should draw not only on the results of the psychometric assessment, but on the other information that you might have from other sources (e.g. clinical interview and collateral information). Recommendations Your recommendations should follow logically from your findings and your formulation. Your recommendations might include recommendations for intervention or for further assessment. Critical review In the final section you have the opportunity to reflect on what you have done, what you have learned and what you might do differently. You might want to include information about the appropriateness of the referral, why you felt that it was necessary to conduct a psychometric assessment on the client,

142
and what, in hindsight, you would have done differently with respect to the tests you used (if anything). This section should also include: Evidence of Learning and Self Reflection Markers will expect to see evidence of learning and self-reflection. This might include reflection on your responses to the client in particular and to the case in general. You might reflect on what you have learned, on what you think you did well and on what you might have done differently, and how your future approach to similar cases has been influenced by this work. Alternative Structures The structure suggested above may well vary. For example, it is possible that your assessment and findings may result in hypotheses that in turn lead to further investigation. You might therefore have a structure such as:
Referral
Assessment plan
Initial assessment and testing
Results
Hypotheses
Further investigation
Results and interpretation
Formulation
Recommendations
Critical Review These structures are intended to provide you with guidance as to how you might present your case report. There may be occasions where it makes sense to alter the structure. What is most important is that your case report follows a logical sequence that enables the examiner to follow the process of what you have done and why.

143
CASE REPORT TYPE 2: REPORT OF AN INDIVIDUAL THERAPY CASE Aim The aim of this report is to describe the process of your work with an individual client, and the clinical thinking behind this. This should reflect the scientist-practitioner and reflective-practitioner models, incorporating a cycle of assessment, formulation, intervention and evaluation, and (importantly) your learning as a result of this process. What the examiners are looking for A major focus of the report should be on presenting your clinical thinking in your work. This should include clear presentation of the considerations which led you to make specific choices at specific times (eg, in the design of intervention; choosing to follow particular themes in therapy; subsequent adaptations to this plan in light of the client’s ongoing responses). Given the word count, you should not attempt to present all the details you have gleaned about the client’s life, or a “blow-by-blow” account of the work. Rather, you should present the salient details which enable the reader to understand and evaluate the clinical decisions that you made from this information, integrated with theory and any other information you feel to have been relevant. Although the examiners will want to assess the competence of your decisions (and hence your clinical work), this does not imply that every action reported on needs to be “right”: it is entirely appropriate to report on, for example, your attempt to work on the theme which turned out to be a “red herring”. A good case report would make clear why you initially chose to follow this theme, how you then used client response to realise that this was not proving useful, how you reformulated, selected another course of action, and later reflected on what you had learned from this experience. Type of material Any clinical intervention that you have conducted independently with an individual client, whatever its outcome may be presented. In almost all cases, you will also have conducted the assessment yourself. (An exception to this would be for services in which assessments are routinely conducted separately from treatment, or which routinely make use of multi-professional assessment interviews.) The intervention will usually be “closed” to you at the time of writing: either because the intervention was completed as planned; or because it was ended prematurely (eg, client “dropped out”, or became ill and unsuitable for continued psychological treatment of this sort; or because you left the service, and passed the client to another professional). Suggested Structure and Content The examiners marking the case report will not be familiar with where you have been working or any of the details of the case. It is therefore necessary for you to provide sufficient information for the examiner to follow the rationale for what you did, and how you did it. However, because of the limit to the length of the case report, it will not be possible to provide every detail of the case and a blow-by blow account of what you did. Normally the background information would be kept to a minimum and your clinical thinking both during and after the intervention would be given the most weight. It is important that you present the case in a logical sequence. Although the structure will vary depending on the theoretical orientation and particular circumstances of the report, a possible structure for the case report might be:
1. Referral 2. Preliminary (pre-assessment) hypotheses
Assessment of the problem 1. Formulation
Action plan
Implementation of plan / Intervention
Outcome
Critical review & Evidence of Learning and Self-Reflection
144
References and Appendices Referral In this section you give a brief account of how the case came to be referred to the service and/or how the client came to be seen by you. Brief details of the services involved may also be relevant here. Preliminary hypotheses These would follow from the referral, and any additional information you have (eg, about the services involved) prior to your assessment. Your assessment plan should then follow logically from your ideas about how to test out these hypotheses. This would also usually include reference to relevant literature and possibly professional guidelines (eg, DCP/SIG, NSF, NICE). Assessment of the problem Here you would describe how you went about assessing the problem, your rationale for what you did, and what you found. You would usually begin by describing your assessment plan and your rationale for the intended assessment procedure, linking these to your initial hypotheses. You would then usually describe what you actually did (eg, clinical interview focusing on current functioning and early childhood experiences; psychometric measures; liaison with CMHT regarding previous contact with the client). Finally you would describe what you found through the assessment. In this section you would usually include a more detailed description of the problem and the background to the problem, and the client’s clinical presentation during the assessment. If you carried out any formal testing you would present your findings. However, given the limitations of the word count, details of background information will usually be limited to what is essential to the clinical understanding of the case and your clinical decisions. Your assessment may have entailed more than one stage. For example, following an initial interview with a client you may have several working hypotheses which you choose to investigate further by carrying out a behavioural observation or arranging to interview a carer. It is useful to describe this process, showing how your hypotheses have guided your subsequent investigations in the assessment process. The specifics of what you include in the assessment section will be guided by the nature of the case and the approach you have adopted. Be explicit about what you did, why you did it, and what you found. It is useful to bear in mind that, in order to provide an evaluation of outcome, it is useful to include some form of pre-intervention evaluation during the assessment phase. Formulation In this section you should provide your understanding and hypotheses about the case ‘so far’. These may change over the course of the intervention and you will have the opportunity to reflect on this later in the report and /or in the Critical Review section of the case report. There should be a clear link between what you found through the process of assessment and your formulation. It is expected that you will consider more than one theoretical model in discussing your initial formulation. This section provides you with the opportunity to demonstrate your theoretical understanding and how you have used this to inform your thinking about the case. You should consider questions such as: What are the problems? How did they arise? How are they maintained? What are the intervention goals? What strengths and resources have been identified which may be used in future? Sometimes diagrams can be useful in presenting your formulation. However, the written (prose) formulation should be sufficient to “stand alone” – ie, would be sufficient to describe your understanding without use of diagrams. You should also take care to ensure that you are presenting a case-specific formulation, rather than a generic model (eg, of depression). Action plan In this section you should describe your plan of action along with a rationale for why you have chosen one approach or plan over another. This should follow from the formulation. As before, it may also include use of empirical evidence and appropriate professional guidelines (eg, NICE), clinical

145
experience (your own and that of your supervisor), service guidelines, application of theory-practice links and clinical judgements. Implementation of plan / Intervention In this section you should describe what you did. Given the word limit of the case report, you will not be able to provide a verbatim account of your intervention. You might instead choose to give an overall description of what you did with a more detailed description of key phases in the intervention. It might be useful to include some segments out of sessions, or possibly a detailed description of one session in order to give a flavour for what you did or to illustrate a point. There are many different options here. The key is that the examiner is able to gain a clear idea of what you did and how, the order and timing of your interventions, how the client responded, and how you modified your intervention in light of these responses. In this section you also should provide the examiner with an insight into what the central themes and issues were. You may choose to include examples of, for example, thought diaries or rating scales in the appendices as appropriate. Outcome In this section you need to discuss the outcome of the implementation of the action plan. You should provide explicit evidence of outcome. This might be from self-report questionnaires, diaries, tests, behavioural observation, client/carer feedback etc. You should include these in the appendices. How and what you choose to assess at the outcome stage should relate back to the initial goals of the intervention. Once again, you should be clear about how and why you have chosen certain methods over others. Critical review This is a very important part of the case report. In this final section you have the opportunity to reflect on the case, the intervention, and how you see things now. In this section you should refer back to you initial formulation. Were your initial hypotheses confirmed? How might you reformulate the case now? In the light of this, would your action plan be any different? What were the strengths and weaknesses of the intervention? What have you learned? This section should also include: Evidence of learning and self reflection Markers will be looking for evidence that you have learned from your experience and that you can demonstrate this ability clearly. Reflection may include self-reflection on how the therapy process affected you, how you think your own beliefs and feelings may have impacted on the therapy process, what you have learned as a therapist, and how you would modify your practice in future. Reflection on the experience is also likely to include reflection on the therapeutic process. Evidence of self-reflection and learning may be demonstrated throughout the case report, but should also be an important aspect of your critical review. Appendices You should include letters and/or reports you have written in the appendices, but not letters or reports written by others. Insofar as it is useful to illustrate aspects of the assessment or intervention, you may also include examples of client materials, for example, diaries or thought records (all client, trainee and service details having been removed).

146
CASE REPORT TYPE 3a: REPORT ON A COUPLE OR FAMILY INTERVENTION Aim The aim of this report is to describe the process of and clinical thinking behind your work with a couple or family. This should reflect the scientist-practitioner and reflective-practitioner models, typically incorporating a cycle of assessment, formulation, intervention and evaluation, and (importantly) your learning as a result of this process. What the examiners are looking for A major focus of the report should be on presenting your clinical thinking in your work. This should include clear presentation of the considerations which led you to make specific choices at specific times (e.g., in the design of intervention; subsequent adaptations to this plan in light of the couple/family’s ongoing responses). Given the word count, you should not attempt to present all the details you have gleaned about the couple/family, or a “blow-by-blow” account of the work. Rather, you should present the salient details which enable the reader to understand and evaluate the clinical decisions that you made from this information, integrated with theory and any other information you feel to have been relevant. Although the examiners will want to assess the competence of your decisions (and hence your clinical work), this does not imply that every action reported on needs to be “right”: it is entirely appropriate to report on, for example, an intervention with a couple or family that required revision. A good case report would make clear why you initially chose a particular intervention strategy, what went wrong, how you reformulated, selected another course of action, and later reflected on what you had learned from this experience. Type of material Any intervention that you have conducted with a couple or family, whatever its outcome, may be presented. It may be a case that you have worked on independently or jointly with other therapist(s). If the case involved co-therapy or working with a team of therapists you would need to have taken the lead in conducting the assessment and intervening with the couple/ family. It would not be appropriate to submit a case report on a couple or family where your role had been limited to acting as part of the team. Suggested Structure and Content The examiners marking the case report will not be familiar with where you have been working or any of the details of the case. It is therefore necessary for you to provide sufficient information for the examiner to follow the rationale for what you did, and how you did it. However, because of the limit to the length of the case report, it will not be possible to provide every detail of the case. It is important that you present the work in a logical sequence. Although the structure will vary depending on the theoretical orientation and particular circumstances of the report, a possible structure for a report on a couple/family:
3. Referral Context 4. Preliminary Hypotheses
Assessment 2. Formulation
Action plan
Implementation of plan / Intervention
Outcome
Critical review & Evidence of Learning and Self-Reflection
References and Appendices A report on a couple/family may vary from this format depending on the nature of the case, the number of family members attending, and the nature of the problem(s) being addressed. However the

147
basic cycle of assessment/investigation, formulating/hypothesising, intervening, evaluating outcome and reflecting on the process still follows albeit in a somewhat different guise. It is recognised that case reports on systemic therapy with a client/family fit less easily into the above categories as they do not reflect the actual process of therapy (that is, assessment, hypothesising and intervention may run through-out the work and there may be a less clear distinction between these different activities). You may, therefore, want to present the case in a different format. However, it is important to bear in mind that all the above categories need to be represented in your report. You may find it useful to refer to Donovan et al’s (2002) article that outlines some guidelines for systemic reports and case presentations. Referral Context In this section you give a brief account who was the referred client(s), why they were referred to the service and how they came to been seen by you. Brief details of the service involved may also be relevant here. For instance, does the service accept referrals of family/couples or was an individual client referred? If the latter, how did it come about that the clients were seen along with their partner or family? In systemic case reports additional emphasis may be placed on systemic issues at this point e.g. who defined the ‘problem determined system? (e.g. the GP, social services, parents etc.) How was this determined? How was it decided who should be invited to the initial assessment? Preliminary hypotheses These would follow from the referral, and any additional information you have prior to your assessment. Your assessment plan should then follow logically from your ideas about how to test out these hypotheses. This would also usually include reference to relevant literature and possibly professional guidelines (eg, DCP/SIG, NSF, NICE). In a systemic case report your preliminary hypotheses may have resulted from a team discussion. Assessment Here you would describe how you went about assessing the presenting difficulties in the context of the couple/family relationships. You need to include your rationale for what you did, and what you found. You would usually begin by describing your assessment plan and your rationale for the intended assessment procedure. You would then usually describe what you actually did (eg, clinical interview with family/couple, standardised assessment tools, liaison with colleagues regarding previous contact with the family/couple, behavioural observations). Finally you would briefly describe what you found through the assessment. In this section you would usually include a more detailed description of the problem and the background to the problem. In a family/couple assessment it is important to focus on family and couple relationship factors such as the dynamics, interaction patterns, shared belief, life stage issues etc. If you carried out any formal testing you would present your findings. (However, given the limitations of the word count, details of background information will usually be limited to what is essential to the clinical understanding of the case and your clinical decisions). You may also wish to include a family genogram. The specifics of what you include in the assessment section will be guided by the nature of the case and the approach you have adopted. Be explicit about what you did, why you did it, and what you found. Be clear about what you did yourself and what you set up but had others implement. You should also bear in mind that, in order to provide an evaluation of outcome, it is useful to include some form of pre-intervention evaluation during the assessment phase. Formulation In this section you should provide your understanding of the family/couple’s difficulties. There should be a clear link between what you found through the process of assessment and your formulation. It is expected that you will consider more than one theoretical model in discussing your initial formulation. This section provides you with the opportunity to demonstrate your theoretical understanding and how you have used this to inform your thinking about the case. If you are using a family therapy model you should be clear about which specific model(s) of family therapy you are drawing on. You should

148
consider questions such as: What are the presenting difficulties? How have they arisen in the context of the family/couple’s relationships and stage in their life cycle? How are they maintained? What are the intervention goals? What are the couple’s/family’s strengths and resources that may help them to achieve their therapeutic goals? Sometimes diagrams can be useful in presenting your formulation. However, the written (prose) formulation should be sufficient to “stand alone” – ie, would be sufficient to describe your understanding without use of diagrams. In systemic case reports it is recognised that there often appears to be two levels of formulation running concurrently in systemic practice (Campbell et al. 1998); an overarching formulation and a constantly evolving formulation comprised of working hypotheses. The overarching formulation is what needs to be presented in this section. It represents your understanding of the family/couple’s difficulties, drawing together the information you have gleaned in the assessment and relating it to relevant theoretical models. You may choose to present your working hypotheses, which guide your interviewing with families/couples during each session, in the intervention section as you give an account of each session. Action plan In this section you should describe your plan of action along with a rationale for why you have chosen one approach or plan over another (e.g. a family/couple intervention as opposed to an individual intervention). This should follow from the formulation. It may also include use of empirical evidence and appropriate professional guidelines (eg, NICE), clinical experience (your own and that of your supervisor), service guidelines, application of theory-practice links and clinical judgements. Implementation of plan / Intervention In this section you should describe what you did. Given the word limit of the case report, you will not be able to provide a verbatim account of your intervention. You might instead choose to give an overall description of what you did with a more detailed description of key phases in the intervention. It might be useful to include some segments out of sessions, or possibly a detailed description of one session in order to give a flavour for what you did or to illustrate a point. As mentioned before, in a systemic case report you may want to outline your working hypotheses for certain sessions, how they influenced your interviewing in the session and whether they were confirmed or refuted. There are many different options here. The key is that the examiner is able to gain a clear idea of what you did and how, the order and timing of your interventions, how the family/couple responded, and how you modified your intervention in light of these responses. In this section you also should provide the examiner with an insight into what the central themes and issues were. Outcome In this section you need to discuss the outcome of the implementation of the action plan for the couple and family as a unit and for each individual member. You should provide explicit evidence of outcome. This might be from self-report questionnaires, diaries, tests, behavioural observation, feedback from the couple/family etc. You should include these in the appendices where applicable. How and what you choose to assess at the outcome stage should relate back to the initial goals of the intervention. Once again, you should be clear about how and why you have chosen certain methods over others. In systemic therapy, changes in the family’s construction of meaning of their situation or shifts in the meaning of the symptoms among the members of the problem determined system (e.g. school, GP etc.) might be as important an outcome as any observable changes in the referral problem. It is therefore important to include these less observable outcomes in your report. Critical review This is a very important part of the case report. In this final section you have the opportunity to reflect on the case, the intervention, and how you see things now. In this section you should refer back to you initial formulation. Were your initial hypotheses confirmed? How might you reformulate the case now? In the light of this, would your action plan be any different? What were the strengths and

149
weaknesses of the intervention? What have you learned? Did this piece of work raise any issues relating to diversity or professional or ethical issues? This section should also include: Evidence of learning and self reflection Markers will be looking for evidence that you have learned from your experience and that you can demonstrate this ability clearly. Reflection may include self-reflection on how the process affected you, how you think your own beliefs and feelings may have impacted on the process, what you have learned as a clinician, and how you would modify your practice in future. Evidence of self-reflection and learning may be demonstrated throughout the case report, but should also be an important aspect of your critical review. Appendices You should include letters and/or reports you have written in the appendices, but not letters or reports written by others. Insofar as it is useful to illustrate aspects of the assessment or intervention, you may also include examples of client materials, for example, diaries or thought records (all client, trainee and service details having been removed). References Donovan, M., K. Mastroyannopoulou and R. Cobner (2002) ‘Guidelines for Systemic Case Reports and Presentations’ Clinical Psychology Issue 9, January 2002, 28-32 Campbell, D., Draper, R., and Huffington, C. (1998) Second Thoughts on the Theory on Practice of the Milan Approach to Family Therapy London:Karnac Dallos, R. & Stedman, J. (2006). Systemic formulation: mapping the family dance. In Johnstone, L. & Dallos, R. (Eds) Formulation in Psychology and Psychotherapy : Making Sense of People’s Problems, London: Routledge. CASE REPORT TYPE 3b: REPORT ON A GROUP INTERVENTION Aim The aim of this report is to describe the process of and clinical thinking behind your work in the organisation and implementation of a group intervention. This should reflect the scientist-practitioner and reflective-practitioner models, typically incorporating a cycle of assessment, formulation, intervention and evaluation, and (importantly) your learning as a result of this process. What the examiners are looking for A major focus of the report should be on presenting your clinical thinking in your work. This should include clear presentation of the considerations which led you to make specific choices at specific times (e.g., in the design of intervention; subsequent adaptations to this plan in light of the ongoing responses from clients). Given the word count, you should not attempt to present all the details you have gleaned about the client’s life, or a “blow-by-blow” account of the work. Rather, you should present the salient details which enable the reader to understand and evaluate the clinical decisions that you made from this information, integrated with theory and any other information you feel to have been relevant. Although the examiners will want to assess the competence of your decisions (and hence your clinical work), this does not imply that every action reported on needs to be “right”: it is entirely appropriate to report on, for example, your attempt to set up a group intervention that required revision. A good case report would make clear why you initially chose a particular intervention strategy, what went wrong, how you reformulated, selected another course of action, and later reflected on what you had learned from this experience. Type of material

150
Any group intervention that you have conducted, whatever its outcome, may be presented. It may be a group that you have organised and run independently or jointly with other colleagues. In all cases you need to have taken a major role in the planning and the organisation of the group and in carrying out assessments on clients to determine their suitability for the group intervention. (The only exception to this would be for a service in which assessments are conducted separately from interventions and clients are therefore assessed and referred for a group intervention by other colleagues). Suggested Structure and Content The examiners marking the case report will not be familiar with where you have been working or any of the details of the case. It is therefore necessary for you to provide sufficient information for the examiner to follow the rationale for what you did, and how you did it. However, because of the limit to the length of the case report, it will not be possible to provide every detail of the case. It is important that you present the work in a logical sequence. Although the structure will vary depending on the theoretical orientation and particular circumstances of the report, a possible structure for a report on a group intervention might be:
5. Background/Rationale 6. Referrals
Assessment 3. Formulation
Action plan
Implementation of plan / Intervention
Outcome
Critical review & Evidence of Learning and Self-Reflection
References and Appendices A report on a group intervention may vary from this format depending on the nature of the group, for example, there may be less focus on the assessment, formulation, actions plan and intervention for individual clients and more focus on the rationale for the group itself, the therapy process within the group and the evaluation of the group intervention as a whole. Background/Rationale Initially it might be helpful to give some background information on the service you are working in, the group intervention and the rationale behind it e.g. is it a group routinely run by the service or a new group that you have devised to meet the needs of clients referred to the service. Referral In this section you give a brief account of how the clients came to be referred to the service and to the group. Assessment Here you might describe how you went about assessing the clients’ presenting difficulties and their suitability for the group. You need to include your rationale for what you did, and what you found. You would usually begin by describing your assessment plan and your rationale for the intended assessment procedure, followed by what you did and what you found. It would be important to report on the client’s suitability of the group, their motivation, their goals and how they would be met by the group intervention. You might also include some form of pre-intervention evaluation during the assessment phase. In some types of groups you may not have assessed the group participants prior to their joining the group. For example in ‘open’groups members tend to come and go and are often referred by other colleagues. In this case it might be more appropriate to discuss the referral criteria and/or inclusion and exclusion criteria for the group along with a rationale for these, rather than attempting to describe every individual client.

151
Formulation If you have undertaken assessments for each group member then you might provide your understanding of the clients’ difficulties in this section. There should be a clear link between what you found through the process of assessment and your formulation. This section provides you with the opportunity to demonstrate your theoretical understanding and how you have used this to inform your thinking about the clients in the group. You should consider questions such as: What are the problems? How did they arise? How are they maintained? What are the intervention goals? What strengths and resources have been identified which may be used in future? In the case of a report on a group, your may be presenting a generic formulation which applies to the clients within the group. However, it is important to show how this formulation fits the clients’ specific circumstances. Given the word count limitations it may not be possible to do this for all clients. You may therefore want to focus on one or two cases in detail as an example. In some types of groups client focussed formulations may not be appropriate and you may wish instead to provide a ‘formulation’ of the group itself, making links between the presenting difficulties, the goal of the group and the theory underpinning the intervention. Action plan In this section you would describe your plan of action along with a rationale for why you have chosen one approach or plan over another (e.g. a group as opposed to an individual intervention). This should follow from the formulation. It may also include use of empirical evidence and appropriate professional guidelines (eg, NICE), clinical experience (your own and that of your supervisor), service guidelines, application of theory-practice links and clinical judgements. Implementation of plan / Intervention In this section you should describe what you did. Given the word limit of the case report, you will not be able to provide a verbatim account of your intervention. You might instead choose to give an overall description of what the group programme included and then to give a brief account of each session. Alternatively if the group included a large number of sessions, you may want to give a more detailed description of certain key sessions, or to give extracts from certain sessions to give us a flavour of what you did or to illustrate a point. You may describe key change moments and illustrate these with examples. You should provide the examiner with an insight into what the central themes and issues were. There are many different options here. The key is that the examiner is able to gain a clear idea of what you did and how, the order and timing of your interventions, how the clients responded, and how you modified your intervention in light of these responses. In the case of a group intervention it is important to include details of the group interaction and dynamics. You may wish to focus on key points in the group process, illustrating these with examples and commenting on changes that did (or did not) happen. Whilst group process must be discussed, the extent to which you focus on this will be dependent on the nature and theoretical underpinnings of the group. You may choose to include examples of, for example, thought diaries or rating scales in the appendices as appropriate. Outcome In this section you need to discuss the outcome of the implementation of the action plan. If your case report has focussed on the individual clients then you should discuss outcome for each client who attended the group. You should provide explicit evidence of outcome. This might be from self-report questionnaires, diaries, tests, behavioural observation, client/carer/staff feedback etc. You should include these in the appendices where applicable. How and what you choose to assess at the outcome stage should relate back to the initial goals of the group intervention. Once again, you should be clear about how and why you have chosen certain methods over others. You may want to include your recommendations for each client following the intervention e.g. case closed, referred for individual therapy etc.

152
Critical review This is a very important part of the case report. In this final section you have the opportunity to reflect on the group intervention, its effectiveness and how it well it met the clients’ needs and goals. What were the strengths and weaknesses of the group intervention? Did it benefit some clients over others? Would it lead you to re-formulate any of the clients’ difficulties? What were the benefits or disadvantages of the group intervention? Did it raise any ethical or professional issues? In the light of this, would your action plan be any different? What have you learned from carrying out the intervention? This section should also include: Evidence of learning and self reflection Markers will be looking for evidence that you have learned from your experience and that you can demonstrate this ability clearly. Reflection may include self-reflection on how the process affected you, how you think your own beliefs and feelings may have impacted on the process, what you have learned as a clinician, and how you would modify your practice in future. Evidence of self-reflection and learning may be demonstrated throughout the case report, but should also be an important aspect of your critical review. Appendices You should include letters and/or reports you have written in the appendices, but not letters or reports written by others. Insofar as it is useful to illustrate aspects of the assessment or intervention, you may also include examples of client materials, for example, diaries or thought records (all client, trainee and service details having been removed) if applicable. In the case of a structured group you might include copies of your plans for each session.

153
CASE REPORT TYPE 4: REPORT ON AN INDIRECT INTERVENTION OR CONSULTATION Aim The aim of this report is to describe the process of and clinical thinking behind your work on a case where a significant part of the work was carried out indirectly OR via consultation. This should reflect the scientist-practitioner and reflective-practitioner models, typically incorporating a cycle of assessment, formulation, intervention and evaluation, and (importantly) your learning as a result of this process. What the examiners are looking for A major focus of the report should be on presenting your clinical thinking in your work. This should include clear presentation of the considerations which led you to make specific choices at specific times (eg, in the design of intervention; subsequent adaptations to this plan in light of the ongoing responses from client and/or staff). Given the word count, you should not attempt to present all the details you have gleaned about the client’s life, or a “blow-by-blow” account of the work. Rather, you should present the salient details which enable the reader to understand and evaluate the clinical decisions that you made from this information, integrated with theory and any other information you feel to have been relevant. Although the examiners will want to assess the competence of your decisions (and hence your clinical work), this does not imply that every action reported on needs to be “right”: it is entirely appropriate to report on, for example, your attempt to set up an indirect intervention that required revision. A good case report would make clear why you initially chose a particular intervention strategy, what went wrong, how you reformulated, selected another course of action, and later reflected on what you had learned from this experience. Type of material Any indirect clinical intervention or consultation that you have conducted independently, whatever its outcome may be presented. In the case of an indirect intervention you may have conducted the initial assessment yourself and then implemented an intervention via other staff members or carers, or the assessment process may also have been carried out indirectly, for example, via interviews with staff and carers and behavioural observations set up by you but carried out by others. In the case of consultation you may describe a process of consultation on one or a group of cases, with one or more colleagues. The consultation should have been carried out independently by you (although your supervisor may have been present as an observer on one or more occasions). Suggested Structure and Content The examiners marking the case report will not be familiar with where you have been working or any of the details of the case. It is therefore necessary for you to provide sufficient information for the examiner to follow the rationale for what you did, and how you did it. However, because of the limit to the length of the case report, it will not be possible to provide every detail of the case. It is important that you present the work in a logical sequence. Although the structure will vary depending on the theoretical orientation and particular circumstances of the report, a possible structure for a report on an indirect piece of work might be:
Referral
Preliminary (pre-assessment) hypotheses
Assessment of the problem 4. Formulation
Action plan
Implementation of plan / Intervention
Outcome
Critical review & Evidence of Learning and Self-Reflection

154
References and Appendices A report on a consultation may vary from this format depending on the nature of the consultation process, whether it is with one or more people, and the nature of the problem(s) being addressed. However the basic cycle of assessment/investigation, formulating/hypothesising, intervening, evaluating outcome and reflecting on the process still follows albeit in a somewhat different guise. Referral In this section you give a brief account of how the case came to be referred to the service and/or seen by you. Brief details of the services involved may also be relevant here. Preliminary hypotheses These would follow from the referral, and any additional information you have (eg, about the services involved) prior to your assessment. Your assessment plan should then follow logically from your ideas about how to test out these hypotheses. This would also usually include reference to relevant literature and possibly professional guidelines (eg, DCP/SIG, NSF, NICE). In the case of consultancy, you will still need to present your hypotheses about the presenting problem. However the presenting problem may not be that of an individual client, but rather a problem or set of problems presented by a staff member or a staff group. Assessment of the problem Here you would describe how you went about assessing the problem, your rationale for what you did, and what you found. You would usually begin by describing your assessment plan and your rationale for the intended assessment procedure, linking these to your initial hypotheses. You would then usually describe what you actually did (eg, clinical interview, interviews with staff and/or carers, psychometric measures, liaison with colleagues regarding previous contact with the client, behavioural observations). Finally you would describe what you found through the assessment. In this section you would usually include a more detailed description of the problem and the background to the problem, and the client’s clinical presentation during the assessment. If you carried out any formal testing you would present your findings. However, given the limitations of the word count, details of background information will usually be limited to what is essential to the clinical understanding of the case and your clinical decisions. Detailed data from psychometric assessment or behavioural observations would usually be provided in the appendices. Your assessment may have entailed more than one stage. For example, following an initial interview with a client you may have several working hypotheses which you choose to investigate further by carrying out a behavioural observation or arranging to interview a carer. It is useful to describe this process, showing how your hypotheses have guided your subsequent investigations in the assessment process. The specifics of what you include in the assessment section will be guided by the nature of the case and the approach you have adopted. Be explicit about what you did, why you did it, and what you found. Be clear about what you did yourself and what you set up but had others implement. You should also bear in mind that, in order to provide an evaluation of outcome, it is useful to include some form of pre-intervention evaluation during the assessment phase. In the case of consultation, your assessment may not be a formal clinical assessment in the usual sense, but rather an information gathering process carried out via discussions with those to whom you are consulting. Although perhaps not ‘assessment’ in the usual sense this process is essential to guiding your working hypotheses and your planned intervention, and as such would need to be described in the case report. Formulation In this section you should provide your understanding and hypotheses about the case ‘so far’. These may change over the course of the intervention and you will have the opportunity to reflect on this later in the report and /or in the Critical Review section of the case report. There should be a clear link

155
between what you found through the process of assessment and your formulation. It is expected that you will consider more than one theoretical model in discussing your initial formulation. This section provides you with the opportunity to demonstrate your theoretical understanding and how you have used this to inform your thinking about the case. You should consider questions such as: What are the problems? How did they arise? How are they maintained? What are the intervention goals? What strengths and resources have been identified which may be used in future? Sometimes diagrams can be useful in presenting your formulation. However, the written (prose) formulation should be sufficient to “stand alone” – ie, would be sufficient to describe your understanding without use of diagrams. You should also take care to ensure that you are presenting a case-specific formulation, rather than a generic model (eg, of depression). In the case of a report on a consultation, your formulation may or may not relate to a specific client. Depending on the nature of the consultation your formulation may relate to your understanding of an organisational system rather than to a specific client. This remains a crucial element of your case report and the guidance on formulation of individual clinical cases applies equally to your ‘formulations’ regarding services or organisations. Action plan In this section you should describe your plan of action along with a rationale for why you have chosen one approach or plan over another. This should follow from the formulation. As before, it may also include use of empirical evidence and appropriate professional guidelines (eg, NICE), clinical experience (your own and that of your supervisor), service guidelines, application of theory-practice links and clinical judgements. Implementation of plan / Intervention In this section you should describe the intervention. This might include a description of your contact with the carer/staff member carrying out the intervention and their accounts of the client’s progress. Given the word limit of the case report, you will not be able to provide a verbatim account of the intervention. You might instead choose to give an overall description of what you did with a more detailed description of key phases in the intervention. There are many different options here. The key is that the examiner is able to gain a clear idea of what you did and how, the order and timing of your interventions, how the carer/staff member(s) reacted and carried out your suggestions, how the client responded, and how you modified your intervention in light of these responses. You may choose to include examples of, for example, behavioural observation diaries or rating scales in the appendices as appropriate. In the case of consultation, in this section you would describe the process of consultation and what you did. You might give a description of the overall intervention along with a more detailed account of one or more sessions to give a flavour of the consultation, or you might describe the intervention on the basis of themes and issues arising during the course of the consultation. As with descriptions of direct or indirect clinical interventions, there are many different options. Outcome In this section you need to discuss the outcome of the implementation of the action plan. You should provide explicit evidence of outcome. This might be from self-report questionnaires, diaries, tests, behavioural observation, client/carer/staff feedback etc. You should include these in the appendices where applicable. How and what you choose to assess at the outcome stage should relate back to the initial goals of the intervention/consultation. Once again, you should be clear about how and why you have chosen certain methods over others. Critical review This is a very important part of the case report. In this final section you have the opportunity to reflect on the case, the intervention, and how you see things now. In this section you should refer back to you initial formulation. Were your initial hypotheses confirmed? How might you reformulate the case now? In the light of this, would your action plan be any different? What were the strengths and weaknesses of the intervention/consultation? What have you learned? This section should also include:

156
Evidence of learning and self reflection Markers will be looking for evidence that you have learned from your experience and that you can demonstrate this ability clearly. Reflection may include self-reflection on how the process affected you, how you think your own beliefs and feelings may have impacted on the process, what you have learned as a clinician, and how you would modify your practice in future. Evidence of self-reflection and learning may be demonstrated throughout the case report, but should also be an important aspect of your critical review. Appendices You should include letters and/or reports you have written in the appendices, but not letters or reports written by others. Insofar as it is useful to illustrate aspects of the assessment or intervention, you may also include examples of client materials, for example, diaries or thought records (all client, trainee and service details having been removed).

157
Doctorate in Clinical Psychology
CLINICAL CASE REPORT ASSESSMENT FORM
Psychometric Assessment Cases
Trainee (or code): Title of exercise: Assessor: Submission date: Date handed in: Date mark due: Date marked:
ASPECT RATING
Fail
Borderline Pass
Structure and Presentation (logical and sequential, clear expression of ideas,
appropriate use of language, appropriate referencing)
Referral Background & Preliminary Hypotheses (relevant background info
presented re. referral and setting, leading to preliminary hypotheses,)
Assessment Plan (follows from presenting problem and hypotheses, appropriate choice of
method/tests; choices justified with links to theory/research/policy)
Presentation and Interpretation of Results (accurate scoring and interpretation
in the context of information learned from the assessment, behavioural and clinical observations
and process issues. Interpretations justified where appropriate, appropriate presentation of results)
Formulation (follows from the assessment; draws on relevant psychological and
neuropsychological models where appropriate; presents trainee’s understanding of the case)
Recommendations (follow from assessment and formulation, show appropriate
understanding of issues)
Critical Review (presents balanced critique of the piece of work, comments on possible
alternative approaches and reformulates as appropriate)
Theory-Practice Links (shows appropriate links between theory, research and practice
throughout)
Ethical and Professional Issues (the work is carried out in an ethical and professional
manner, ethics and professional issues, including difference and diversity, are considered and
reflected upon)
Evidence of Learning and Self-Reflection (shows evidence of self-reflection and
learning, identifies strengths and weaknesses; reflects on role of own values, history etc. as
appropriate; considers how learning from this case might affect future clinical work)
OVERALL MARK Fail Pass
In the event of minor failures of anonymisation Pass subject to amendments
Comments: (Please note that this mark sheet with the comments that you provide will be made available to the Trainee as
feedback. It is therefore important that you write in an appropriate and constructive style which encourages trainees to take
on board comments)
JOINT MARK AGREED WITH SECOND ASSESSOR:
FAIL / PASS / PASS Subject to Amendments
Comments: (e.g. regarding discrepancies)

158
CLINICAL CASE REPORT ASSESSMENT FORM
Therapeutic Cases: Individual, Indirect, Family
Trainee (or code):
Title of exercise:
Assessor:
Submission date: Date handed in:
Date mark due: Date marked:
ASPECT RATING
Fail
Borderline Pass
Structure and Presentation (logical and sequential, clear expression of ideas,
appropriate use of language, appropriate referencing)
Referral Background & Preliminary Hypotheses (relevant background info
presented re. referral and setting, leading to preliminary hypotheses,)
Initial Assessment (appropriate choice of method linked to initial hypotheses & context; accurate scoring, reporting
and interpretation of results)
Formulation (follows from the assessment; draws on relevant psychological models; presents
trainee’s understanding of the case; makes psychological sense; client focussed rather than model
focussed)
Action Plan (follows logically from the formulation; presents rationale for choice and goals of proposed
intervention)
Intervention (competence of implementation; appropriateness of choice, including changes of direction in
response to feedback / changes in situation / reformulation)
Outcome Assessment (appropriate choice of method and presentation of outcome)
Ethical and Professional Issues (work is carried out in an ethical and professional manner; ethics and professional issues, including
issues of diversity and difference, are reflected upon appropriately)
Theory-Practice Links (shows appropriate links between theory, research and practice throughout)
Critical Review (presents balanced critique of the piece of work, comments on possible alternative approaches and
reformulates as appropriate)
Evidence of Learning and Self-Reflection (reflects on: personal strengths and areas for personal / professional development; role of the
trainee’s personal style/ history/ circumstances in affecting decision-making & therapeutic process;
how learning from this case might affect future clinical work)
OVERALL MARK Fail Pass
In the event of minor failures of anonymisation Pass subject to amendments
Comments: (Please note that this mark sheet with the comments that you provide will be made available to the Trainee as
feedback. It is therefore important that you write in an appropriate and constructive style which encourages trainees to take
on board comments)

159
JOINT MARK AGREED WITH SECOND ASSESSOR:
FAIL / PASS / PASS Subject to Amendments
Comments: (e.g. regarding discrepancies)

160
Doctorate in Clinical Psychology
CLINICAL CASE REPORT ASSESSMENT FORM
Therapeutic Cases: Groups
Trainee (or code):
Title of exercise:
Assessor:
Submission date: Date handed in:
Date mark due: Date marked:
ASPECT RATING
Fail
Borderline Pass
Structure and Presentation (logical and sequential, clear expression of ideas,
appropriate use of language, appropriate referencing)
Background & Preliminary Hypotheses (relevant background info presented re.
referral and setting, context etc.)
Initial Assessment / Referral Criteria (For client based assessments: appropriate choice of method, reporting of results, interpretations
etc. OR appropriate group inclusion /exclusion criteria linked to some form of assessment)
Formulation / Rationale (follows from the assessment; draws on relevant psychological models in context; presents
trainee’s understanding of the cases AND/OR rationale for the group as a whole and ‘group’
formulation’)
Intervention (competence of implementation; appropriateness of choice, including changes of direction in
response to feedback / changes in situation / reformulation)
Group Process (Discussion of group process & dynamics and role of process in intervention; comments on key
change moments)
Outcome Assessment (appropriate choice of method and presentation of outcome; either for each client or for
group as a whole)
Ethical and Professional Issues (work is carried out in an ethical and professional manner; ethics and professional issues (including
issues of diversity and difference)are reflected upon appropriately)
Theory-Practice Links (shows appropriate links between theory and practice throughout)
Critical Review (presents balanced critique of the piece of work, comments on possible alternative approaches and
reformulates as appropriate)
Evidence of Learning and Self-Reflection (reflects on: personal strengths and areas for personal / professional development; role of the
trainee’s personal style/ history/ circumstances in affecting decision-making & therapeutic process;
how learning from this case might affect future clinical work)
OVERALL MARK Fail Pass
In the event of minor failures of anonymisation Pass subject to amendments
161
Comments: (Please note that this mark sheet with the comments that you provide will be made available to the Trainee as
feedback. It is therefore important that you write in an appropriate and constructive style which encourages trainees to take
on board comments)
JOINT MARK AGREED WITH SECOND ASSESSOR:
FAIL / PASS / PASS Subject to Amendments
Comments: (e.g. regarding discrepancies)