do human atherosclerotic lesions contain nitrotyrosine?
TRANSCRIPT

BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS 226, 346–351 (1996)ARTICLE NO. 1359
Do Human Atherosclerotic Lesions Contain Nitrotyrosine?
Patricia Evans,* Harparkash Kaur,* Malcolm J. Mitchinson,† and Barry Halliwell*
*International Antioxidant Research Centre, Pharmacology Group, King’s College, Manresa Road,London SW3 6LX United Kingdom; and †Department of Pathology, University of Cambridge,
Tennis Court Road, Cambridge CB2 1QP, United Kingdom
Received August 2, 1996
Nitrotyrosine has been widely used as a marker of peroxynitrite formation in normal and diseased tissues.However, studies of normal human aortic intima and atherosclerotic lesions at various stages of developmentfailed to reveal its presence except in a very few specimens of both normal and diseased tissues. Thetechniques used to detect nitrotyrosine-HPLC with photodiode array detection and Western blotting- wereable to identify nitrotyrosine after chemical nitration. Hence peroxynitrite may not be as important in theinitiation of atherosclerosis as has commonly been proposed. q 1996 Academic Press, Inc.
It is increasingly believed that oxidative damage plays a key role in the progression, andperhaps the initiation, of atherosclerosis [1,2]. For example, products of free radical damageto lipids have been detected in human atherosclerotic lesions [1,3,4] and it is widely acceptedthat lipid-laden foam cells characteristic of human lesions arise from the uptake of lipoproteins(especially low density lipoproteins, LDL) by macrophages in the lesions [5]. One of thealterations to LDL that causes their recognition by macrophage scavenger receptors is themodification of the amino groups of apolipoprotein B by aldehydes generated during LDLperoxidation [1,2]. However, it is uncertain how LDL oxidation is initiated in the vessel wall.
The various oxidants known to be produced by inflammatory cells include hypochlorousacid (HOCl), superoxide radical (O•0
2 ), nitric oxide (NOr) and hydrogen peroxide (H2O2) [6].NOr can react with O•0
2 to form the powerful oxidizing and nitrating species peroxynitrite(ONOO0) [7, 8]. Both HOCl and ONOO0 have been suggested to play a role in oxidativemodification of LDL [9,10]. In order to ascertain the contribution of these various species inatherosclerotic lesions, oxidation products that are characteristic of their action need to beidentified in vivo. For example, hydroxylation of phenylalanine to o- and m-tyrosine has beenused as a marker for OH• damage [11]. Peroxynitrite production may be implicated by measur-ing the end-products of its reactions with biomolecules such as proteins. Peroxynitrite decompo-sition leads to the production of both hydroxylating and nitrating species that have not beencompletely characterised as yet [8,12]. However, they can generate 3-nitrotyrosine from tyro-sine, both free and within proteins [8].
Since ONOO0 could explain the initiation of LDL oxidation in early atherosclerotic lesions[13], considerable interest was generated by the report of Beckman et al [14] that nitrotyrosineis present in human atherosclerotic lesions as shown by immunohistochemical staining usingmono- and polyclonal antisera directed against nitrotyrosine. Nitrotyrosine was reported to bepresent even in fatty streaks. However, only three lesions (two atherosclerotic and one fattystreak) were studied and it was not determined whether the nitrotyrosine was free or protein-bound. In order to see how widespread this phenomenon is, we conducted a systematic searchfor nitrotyrosine in both normal human arterial wall and atherosclerotic lesions histologicallycharacterised at various stages of development. Both HPLC and Western blotting techniques
0006-291X/96 $18.00Copyright q 1996 by Academic Press, Inc.All rights of reproduction in any form reserved.
346
AID BBRC 5357 / 6909$$$481 08-26-96 06:23:03 bbrca AP: BBRC

Vol. 226, No. 2, 1996 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
were used to identify 3-nitrotyrosine which was detected in the Western blots using monoclonalanti-nitrotyrosine antiserum to ensure specificity.
MATERIALS AND METHODS
Reagents. All reagents used were purchased from Sigma Chemical Company, Poole, Dorset, UK with the exceptionsstated below. Anti-mouse IgG alkaline phosphatase conjugate was Sigma product A3655 and nitrotyrosine-containingbands were revealed using Sigma Fast 5-bromo-4-chloro-3- indolyl phosphate / nitroblue tetrazolium (BCIP/NBT:Sigma product B5655, 1 tablet/10 ml). Anti-nitrotyrosine (mouse monoclonal IgG) was obtained from TCS BiologicalsLtd., Boltolph Claydon, Buckingham MK18 2LR, UK. Chromatography reagents were supplied by Bio-Rad Labora-tories Ltd., Bio-Rad House, Maylands Avenue, Hemel Hempstead, Herts, HP2 7TD, UK with the exception ofacrylamide/bisacrylamide which was purchased as a ready-mixed solution (30% w/v acrylamide / 0.8% w/v bisacrylam-ide) in Protogel from National Diagnostics, Unit 3, Chamberlain Road, Aylesbury, Bucks. HP19 3DY, UK.
Human aortic tissue samples from cadavers were obtained and characterised histologically as described in [15].The time lapse between death and the excision of samples varied between 28.3 and 118.5 hours (mean 62.8 hours).
Detection of nitrotyrosine in tissue extracts. Tissue extracts were prepared by homogenising known masses ofnormal and diseased human aortic tissue (usually 30 mg/ml) in 0.1 M phosphate buffer containing 0.1% (w/v) digitoninat pH 7.4. Homogenates were left to stand at room temperature for 15 min and then centrifuged at 3000 g for 10 minto remove tissue debris. Wherever possible, samples were processed within three months of removal.
For immunological detection of nitrotyrosine by Western blotting, 10 ml samples of the homogenates were immedi-ately treated with an equal volume of sample application buffer (0.17 M Tris, 1% SDS, 20% glycerol, 4% saturatedbromophenol blue solution and 10% 2-mercaptoethanol v/v at pH 6.8), heated to 1007C for 10 min and after cooling,10 ml of each sample (containing 1-5 mg protein) was applied to 12.5 % SDS-polyacrylamide gels for electrophoresis[16]. Resolved protein bands were transferred electrophoretically onto a nitrocellulose support medium at 15 vovernight using a transfer buffer of 25 mM tris base/192 mM glycine/20% methanol (pH unadjusted). The blots weredeveloped by blocking for one hour with 2% foetal calf serum in phosphate-buffered saline (PBS) followed by twowashed with 0.1% Tween 20 in PBS and then incubation for 2h at room temperature with anti-nitrotyrosine antiserum(mouse monoclonal IgG) diluted 1:2000 (1 mg/ml, final concentration) in PBS containing 2% foetal calf serum (FCS).Excess antiserum was removed by two 10 min washings with PBS containing 1% Tween 20 and the blots were thentreated with a 1:2000 dilution of anti-mouse IgG conjugated to alkaline phosphatase in PBS containing 2% FCS forone hour. After two washings in 0.05% Tween 20 in PBS, BCIP/NBT (Sigma-Fast) was added as a substrate for 5min to reveal any protein bands containing nitrotyrosine.
Nitrotyrosine was also determined by HPLC using the procedure described in [17] after protein hydrolysis whichwas performed by adding concentrated HCl to the samples to a final concentration of 6 M, followed by incubationin vacuo for 24 hours at 1207C, after which the hydrolysed protein was reconstituted in PBS for HPLC analysis.Identity was confirmed by spiking with standards and photodiode array detection.
Protein concentrations in homogenates were determined by the Coomassie Blue method [18].Nitration of proteins using tetranitromethane. Tissue homogenates and bovine serum albumin (5 mg/ml, 1.42 mM
in tyrosine, based on a relative molecular mass of 67 KD and 19 mol of tyrosine / mol BSA [19]) were nitrated usingtetranitromethane by treating either the homogenate as prepared above (30 mg tissue /ml in phosphate-buffereddigitonin) or serum albumin (5 mg/ml in 0.1 M ammonium acetate buffer at pH 7.4) with solutions of tetranitromethanedissolved in ethanol and diluted with ethanol to the appropriate concentration. After two hours incubation, a samplewas taken from each assay and diluted in SAB to a concentration of 0.2 mg/ml corresponding to a gel load of 2 mgprotein for Western blotting. A further sample was hydrolysed in 6M HCl as described above prior to HPLC analysisfor nitrotyrosine.
Determination of antiserum specificity. To investigate the specificity of the anti-nitrotyrosine antiserum, antiserum(1 mg/ml) was incubated overnight in PBS containing 2 % FCS and 3-nitrotyrosine/ 3-chlorotyrosine (10 mM) whichhad been adjusted to pH 7.4 prior to addition of the antiserum. A control sample without the tyrosine derivatives wasalso incubated. SDS-polyacrylamide gel electrophoresis and blot transfer were performed on four identical samplesof nitrated BSA. The blot was then carefully sectioned with the individual sections being treated separately with eithernormal anti-nitrotyrosine antiserum, or antiserum incubated with 3-nitrotyrosine, 3-chlorotyrosine or both substances.
BSA was chlorinated using HOCl in the same manner as nitration. Thus HOCl was prepared by acidification of asolution of sodium hypochlorite to pH 6.2 followed by measurement of its concentration at 235 nm [20]. BSA (5mg/ml) was then incubated with various concentrations of HOCl for 2h at room temperature after which a 5 ml sampleof each incubation was diluted in SAB to 0.2 mg/ml for application to an SDS-gel (10 ml), followed by blotting todetect any cross-reactivity of chlorinated tyrosines with the anti-nitrotyrosine antiserum. Chlorotyrosine was alsodetermined by HPLC using the procedure in [17] when chlorotyrosine eluted as a separate peak from the nitrotyrosineand tyrosine peaks. The peak was authenticated by measurement of its absorbance spectrum and spiking with astandard.
347
AID BBRC 5357 / 6909$$$482 08-26-96 06:23:03 bbrca AP: BBRC

Vol. 226, No. 2, 1996 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
FIG. 1. Western blots showing the specificity of anti-nitrotyrosine antiserum for tyrosine derivatives. SDS-poly-acrylamide gels were loaded with 2 mg BSA which had been treated with TNM (BSA: 5mg/ml, 1.42 mM in tyrosine,with 0.28 mM TNM at pH 7.4) and blotted onto nitrocellulose as given in the materials and methods. Primaryantiserum was monoclonal anti-nitrotyrosine (1 mg/ml in PBS containing 2% FCS) which had been pretreated overnightwith (a) chloro- and nitrotyrosine, both at 10 mM (b) nitrotyrosine, 10 mM (c) chlorotyrosine, 10 mM (d) no additionof tyrosine derivative. The position of the 67 KD band was determined by running and staining a second SDS gelcontaining standard proteins.
RESULTS
1. Study on the specificity of the anti-nitrotyrosine antiserum. Western blots were carried out onBSA samples which had been treated separately with either HOCl or tetranitromethane. For BSAsamples incubated with TNM, there was a clear band staining at the correct molecular mass forBSA with some additional minor bands, presumably due to fragmentation of BSA by the reagent(Fig 1d). No staining was observed for untreated BSA (not shown) and staining was markedlydiminished when the antiserum was preincubated with nitrotyrosine (1b), chlorotyrosine (1c) or amixture of both substances (1a). Despite the blocking of the staining by chlorotyrosine, there wasno detectable staining in BSA samples (5 mg/ml) which had been preincubated with HOCl atconcentrations ranging from 27 mM to 2.7 mM, even though chlorotyrosine (15% of total tyrosine)was detectable on HPLC analysis when 2.8 mM HOCl was incubated with 5 mg/ml BSA.
2. Attempts to detect nitrotyrosine in human atherosclerotic lesions at various stages ofdevelopment. Tissue homogenates were screened for the presence of nitrotyrosine residues byWestern blotting and HPLC analysis. Western blotting was unable to detect nitrotyrosine inany type of tissue taken from human aortic intima whether diseased or normal. A positivecontrol of chemically-nitrated BSA was included with each set of samples studied to checkthat the detection system was working correctly. Table 1 gives a summary of the resultsobtained and the tissues used which ranged from 10 specimens of normal aortic intima through8 specimens of fatty streaks, 1 intermediate macrophage and 1 intermediate fibrous-type lesion,4 advanced fibrous and 4 advanced macrophage-type lesions to 13 gruel (end-stage) lesions(lesion type was determined by histological examination). Nitrotyrosine was also not detectedby HPLC analysis in these samples except for two normal intima, one gruel and one advancedfibrous lesion. To validate the assay procedures used, vessel wall homogenates were nitratedusing TNM and then subjected to the same methods of analysis. Fig 2 shows that samplessubjected to chemical nitration do show bands of proteins staining using the immunochemicalprocedure and do contain nitrotyrosine as detected by HPLC analysis after acid hydrolysis.
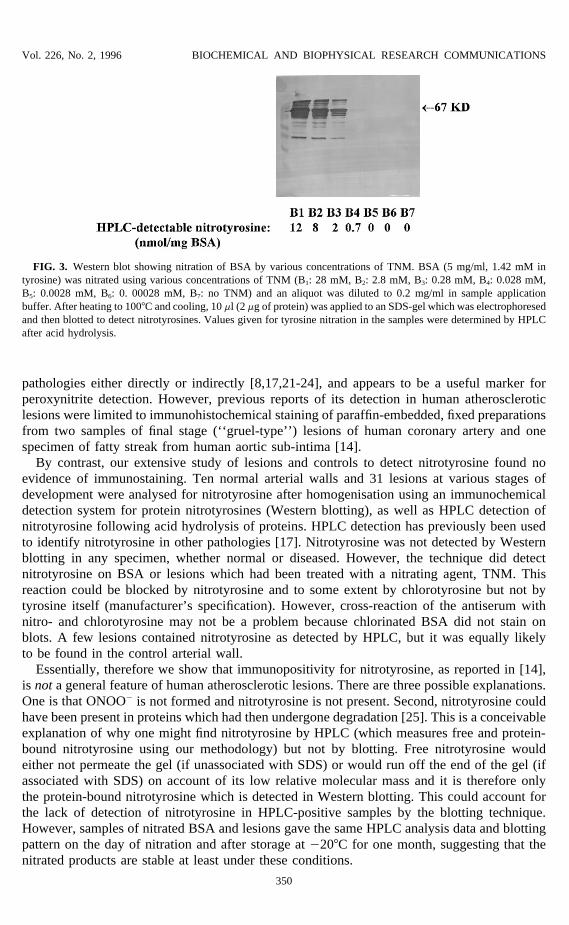
3. Determination of the detection limit for nitrotyrosine using a model system.BSA was nitratedwith various concentrations of TNM at pH 7.4 to determine the detection limit for nitrotyrosineusing both Western blotting and HPLC techniques. Fig 3 shows that the detection limit fornitrotyrosine using the Western blotting technique lies at a ratio of tetranitromethane to BSA-tyrosine of 1 : 50 or 1 TNM per 2.6 BSA molecules (4 experiments, representative blot shownin Fig 3 where the lowest detection point is at 0.028 mM TNM versus 1.42 mM BSA tyrosine).
348
AID BBRC 5357 / 6909$$$482 08-26-96 06:23:03 bbrca AP: BBRC

Vol. 226, No. 2, 1996 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
TABLE 1HPLC Detection of Nitrotyrosine in Normal and Diseased Human Aortic Intima
Number of HPLC-detectable nitrotyrosineHistology samples (nmol/mg of tissue)
Normal intima 8 ND1
1 0.221 0.10
Fatty streak 8 NDIntermediate macrophage 1 NDIntermediate fibrous 1 NDAdvanced macrophage 4 NDAdvanced fibrous 3 ND
1 0.35Gruel 12 ND
1 0.007
Normal and diseased aorta samples (30 mg, if adequate sample was available)were weighed on dri-ice, minced roughly and then homogenised and extracted in1 ml of phosphate-buffered digitonin at pH 7.4. After removing the tissue debrisby centrifugation, samples of extracts were acid hydrolysed and then subjected toHPLC analysis for nitrotyrosine.
1 nil detected.
This gives a maximal theoretical nitration of between 2 and 8% of available tyrosine dependingon the number of NO2 groups available for donation by TNM. HPLC analysis detected nitrotyrosinein samples with the same ratio of TNM:BSA tyrosine as shown in Figure 3. Decreasing BSAconcentration to 0.5 mg/ml made no difference to these detection limits.
DISCUSSIONThe ability of ONOO0 to oxidize LDL has led to suggestions that it is very important in
the development of atherosclerosis [13,14]. Nitrotyrosine has been detected in several human
FIG. 2. Western blotting of human aortic tissue extracts treated with TNM. Normal (N) and atherosclerotic gruel(G) (200 mg/ 6ml) were extracted as described in Table 1 and the extracts aliquoted into tubes containing 1 ml ofextract. TNM in ethanol was then added to each tube to the following final concentrations: N1/G1: (nil), N2/G2: 50mM, N3/G3: 5 mM, N4/G4: 0.5 mM, N5: 0.05 mM, N6: 0.005 mM. After 2h incubation at room temperature, a sample(20 ml, 5 mg of protein) was taken from each tube and added to an equal volume of sample application buffer. Afterheating to 1007C and cooling, 10 ml was loaded onto an SDS-gel, electrophoresed and then blotted for nitrotyrosine.Values given for tyrosine nitration in the samples were determined by HPLC after acid hydrolysis.
349
AID BBRC 5357 / 6909$$$482 08-26-96 06:23:03 bbrca AP: BBRC
Vol. 226, No. 2, 1996 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
FIG. 3. Western blot showing nitration of BSA by various concentrations of TNM. BSA (5 mg/ml, 1.42 mM intyrosine) was nitrated using various concentrations of TNM (B1: 28 mM, B2: 2.8 mM, B3: 0.28 mM, B4: 0.028 mM,B5: 0.0028 mM, B6: 0. 00028 mM, B7: no TNM) and an aliquot was diluted to 0.2 mg/ml in sample applicationbuffer. After heating to 1007C and cooling, 10 ml (2 mg of protein) was applied to an SDS-gel which was electrophoresedand then blotted to detect nitrotyrosines. Values given for tyrosine nitration in the samples were determined by HPLCafter acid hydrolysis.
pathologies either directly or indirectly [8,17,21-24], and appears to be a useful marker forperoxynitrite detection. However, previous reports of its detection in human atheroscleroticlesions were limited to immunohistochemical staining of paraffin-embedded, fixed preparationsfrom two samples of final stage (‘‘gruel-type’’) lesions of human coronary artery and onespecimen of fatty streak from human aortic sub-intima [14].
By contrast, our extensive study of lesions and controls to detect nitrotyrosine found noevidence of immunostaining. Ten normal arterial walls and 31 lesions at various stages ofdevelopment were analysed for nitrotyrosine after homogenisation using an immunochemicaldetection system for protein nitrotyrosines (Western blotting), as well as HPLC detection ofnitrotyrosine following acid hydrolysis of proteins. HPLC detection has previously been usedto identify nitrotyrosine in other pathologies [17]. Nitrotyrosine was not detected by Westernblotting in any specimen, whether normal or diseased. However, the technique did detectnitrotyrosine on BSA or lesions which had been treated with a nitrating agent, TNM. Thisreaction could be blocked by nitrotyrosine and to some extent by chlorotyrosine but not bytyrosine itself (manufacturer’s specification). However, cross-reaction of the antiserum withnitro- and chlorotyrosine may not be a problem because chlorinated BSA did not stain onblots. A few lesions contained nitrotyrosine as detected by HPLC, but it was equally likelyto be found in the control arterial wall.
Essentially, therefore we show that immunopositivity for nitrotyrosine, as reported in [14],is not a general feature of human atherosclerotic lesions. There are three possible explanations.One is that ONOO0 is not formed and nitrotyrosine is not present. Second, nitrotyrosine couldhave been present in proteins which had then undergone degradation [25]. This is a conceivableexplanation of why one might find nitrotyrosine by HPLC (which measures free and protein-bound nitrotyrosine using our methodology) but not by blotting. Free nitrotyrosine wouldeither not permeate the gel (if unassociated with SDS) or would run off the end of the gel (ifassociated with SDS) on account of its low relative molecular mass and it is therefore onlythe protein-bound nitrotyrosine which is detected in Western blotting. This could account forthe lack of detection of nitrotyrosine in HPLC-positive samples by the blotting technique.However, samples of nitrated BSA and lesions gave the same HPLC analysis data and blottingpattern on the day of nitration and after storage at 0207C for one month, suggesting that thenitrated products are stable at least under these conditions.
350
AID BBRC 5357 / 6909$$$482 08-26-96 06:23:03 bbrca AP: BBRC

Vol. 226, No. 2, 1996 BIOCHEMICAL AND BIOPHYSICAL RESEARCH COMMUNICATIONS
Third, our assays could be too insensitive to detect nitrotyrosine, ie it is present at a lowerlevel than our blotting and HPLC techniques can detect. Further analysis is needed to resolvethis problem. However our data raise important questions about the role of ONOO0 in humanatherosclerosis that need to be answered before assuming that this agent has a major pathologi-cal role.
ACKNOWLEDGMENTSMJM and BH are grateful to the British Heart Foundation for research support. PE thanks Drs R. Evans and C.
Joannou of the Division of Biochemistry and Molecular Biology, United Medical and Dental Schools of Guy’s andSt. Thomas, London for their assistance in setting up the blotting methods.
REFERENCES1. Steinberg, D., Parthasarathy, S., Carew, T. E., Khoo, J. C., and Witztum, J. L. (1989) New Engl. J. Med. 320,
915–924.2. Esterbauer, H., Gebicki, J., Puhl, H., and Jurgens, G. (1992) Free Rad. Biol. Med. 13, 341–390.3. Brooks, C. J., Steel, G., Gilbert, J. D., and Harland, W. A. (1971) Atherosclerosis 13, 223–237.4. Carpenter, K. L. H., Taylor, S. E., Ballantine, J. A., Fussell, B., Halliwell, B., and Mitchinson, M. J. (1993)
Biochim. Biophys. Acta 1167, 121–130.5. Aqel, N. M., Ball, R. Y., Waldman, H., and Mitchinson, M. J. (1985) J. Path. 146, 197–204.6. Weiss, S. J. (1989) N. Engl. J. Med. 320, 365–376.7. Huie, R. E., and Padmaja, S. (1993) Free Rad. Res. Comm. 18, 195–199.8. Beckman, J. S., Chen, J., Ischiropoulos, H., and Crow, J. P. (1994) Meth. Enzymol. 233, 229–240.9. Hazell, L. J., and Stocker, R. (1993) Biochem. J. 290, 165–172.
10. White, C. R., Brock, T. A., Chang, L-Y., Crapo, J., Briscoe, P., Ku, D., Bradley, W. A., Granturco, S. H., Gore,J., Freeman, B. A., and Tarpey, M. M. (1994) Proc. Natl. Acad. Sci. USA 91, 1044–1048.
11. Kaur, H., and Halliwell, B. (1994) Meth. Enzymol. 233, 67–82.12. van der Vliet, A., O’Neill, C. A., Halliwell, B., Cross, C. E., and Kaur, H. (1994) FEBS Lett. 339, 89–92.13. Graham, A., Hogg, N., Kalyanaraman, B., O’Leary, V., Darley-Usmar, V., and Moncada, S. (1993) FEBS Lett.
330, 181–185.14. Beckman, J. S., Yao, Z. Y., Anderson, P. G., Chen, J., Attavitti, M. A., Tarpey, M. M., and White, C. R. (1994)
Biochem. Hoppe Seyler 375, 81–88.15. Evans, P. J., Smith, C., Mitchinson, M. J., and Halliwell, B. (1995) Free Rad. Res. 23, 465–469.16. Laemmli, U. K. (1970) Nature 227, 680–685.17. Kaur, H., and Halliwell, B. (1994) FEBS Lett. 350, 9–12.18. Marcart, M., and Gerbaut, L. (1982) Clin. Chim. Acta 122, 93–101.19. Ischiropoulos, H., and Al-Mehdi, A. B. (1995) FEBS Lett. 364, 279–282.20. Wasil, M., Halliwell, B., Hutchison, D. C. S., and Baum, H. (1987) Biochem. J. 243, 219–223.21. Miller, M. J. S., Thompson, J. H., Zhang, X. J., Sadowska-Krowicka, H., Kakkis, J. L., Munshi, U. K., Snadoval,
M., Rossi, J. L., Eloby-Childress, S., Beckman, J. S., Ye, Y. Z., Rodi, C. P., Manning, P. T., Currie, M. G., andClark, D. A. (1995) Gastroenterology 109, 1475–1483.
22. Lipton, S. A., Choi, Y. B., Pan, Z. H., Lei, S. Z., Chen, H. S., Sucker, N. J., Loscalzo, J., Singel, D. J., andStamler, J. S. (1993) Nature 364, 626–632.
23. Culeasi, M., Lajon-Cazal, P., Pietri, S., and Bockaert, J. (1994) J. Biol. Chem. 269, 12589–12593.24. Haddad, I. Y., Pataki, G., Hu, P., Galliani, C., Beckman, J. S., and Matalon, S. (1994) J. Clin. Invest. 94, 2407–
2413.25. Gow, A. J., Duran, D., Malcolm, S., and Ischiropoulos, H. (1996) FEBS Lett. 385, 63–66.
351
AID BBRC 5357 / 6909$$$482 08-26-96 06:23:03 bbrca AP: BBRC