dmards
TRANSCRIPT

DMARDS
MODERATOR: DR. V. K. VERMA
RESIDENT: FARIHA FATIMA



PHARMACOLOGICAL MANAGEMENT
The drugs most frequently used in initial therapy are the
'disease-modifying antirheumatic drugs' (DMARD) and the
NSAIDS.
Unlike the NSAIDS, which reduce the symptoms but not the
progress of the disease, the former group may halt or reverse
the underlying disease itself.

The term 'DMARD' is a latex concept that can be stretched
to cover a heterologous group of agents with unrelated
chemical structures and different mechanisms of action.
Included in this category are methotrexate, sulfasalazine,
gold compounds, penicillamine and chloroquine and other
antimalarials and various immunosuppressant drugs.

The DMARD were often referred to as second-line drugs,
with the implication that they were only resorted to when
other therapies (eg.NSAIDS) failed.
Today, however, DMARD therapy may be initiated as soon
as a definite diagnosis has been reached.
Their clinical effects are usually slow (months) in onset, and
it is usual to provide NSAID 'cover' during this induction
phase.

If therapy is successful, concomitant NSAID (or
glucocorticoid) therapy can generally be dramatically
reduced.


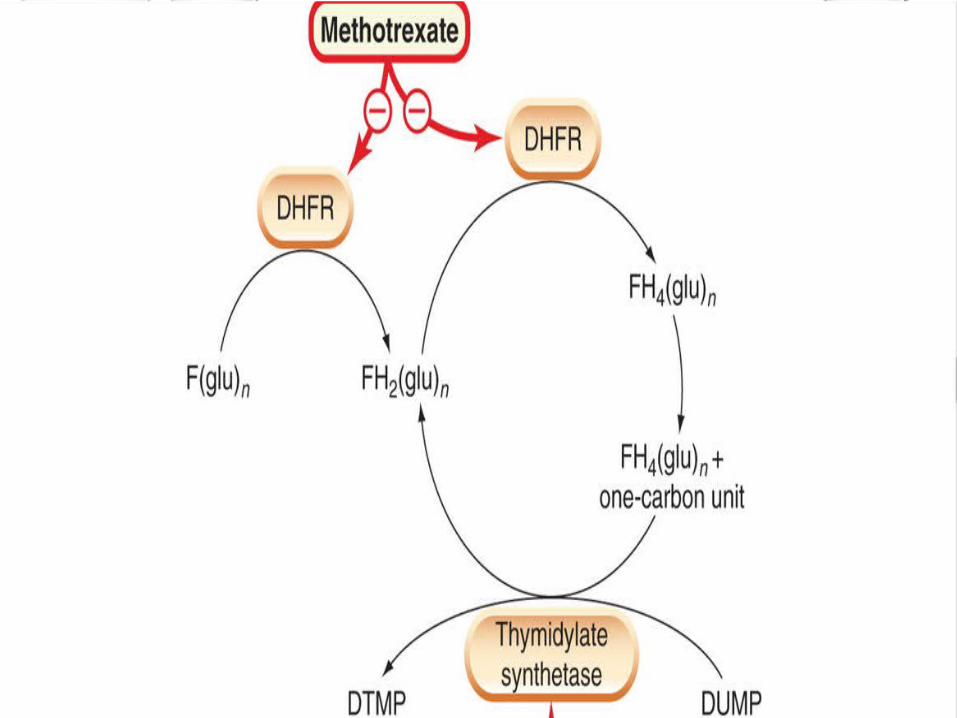
METHOTREXATE
Methotrexate is a folic acid antagonist with cytotoxic and
immunosuppressant activity and potent antirheumatoid
action.
It is a common first-choice drug.
It has a more rapid onset of action than other Dmards,
Pharmacokinetics:
Methotrexate is usually given orally but can also be given
intramuscularly, intravenously or intrathecally.
The drug has low lipid solubility and thus does not readily
cross the blood-brain barrier.
Dose : 15 – 25 mg weekly,orally.
Indications:
Methotrexate is also used as an immunosuppressant drug to
treat rheumatoid arthritis and other autoimmune conditions.
Side effects:
Depression of the bone marrow and damage to the
epithelium of the gastrointestinal tract. Pneumonitis can
occur.
Blood dyscrasias .
Liver cirrhosis.

SULFASALAZINESulfasalazine, a common first-choice DMARD ,
It produces remission in active rheumatoid arthritis and is also used
for chronic inflammatory bowel disease .
It may act by scavenging the toxic oxygen metabolites produced by
neutrophils.
Side Effects : gastrointestinal disturbances,
malaise,
headache
leucopenia
decreased sperm count

PHARMACOKINETIC PROFILE:
Half life of the drug is 6 – 15 hrs
Dose = 500 mg daily for 7 days orally and increased by 500
mg every week to a maximum of 3g/day in 2 to 3 divided
doses.

PENICILLAMINE
Penicillamine is dimethylcysteine; it is produced by hydrolysis
of penicillin.
The D-isomer is used in the therapy of rheumatoid disease.
About 75% of patients with rheumatoid arthritis respond to
penicillamine.
Mechanism of Action: Penicillamine is thought to modify
rheumatoid disease partly by decreasing the immune response,
IL-1 generation and/or partly by an effect on collagen synthesis,
preventing the maturation of newly synthesised collagen.

However, the precise mechanism of action is still a matter of conjecture.
Pharmacokinetic profile:
Penicillamine is given orally, and only half the dose administered is absorbed.
It reaches peak plasma concentrations in 1-2 h and is excreted in the urine.
Dosage is started low and increased only gradually to minimise unwanted effects.
Side Effects:
Rashes and stomatitis are the most common unwanted effects but may resolve if the dosage is lowered.
Anorexia, fever, nausea and vomiting, and disturbances of
taste (the last related to the chelation of zinc) are seen, but
often disappear with continued treatment.
Proteinuria occurs in 20% of patients and should be
monitored.

GOLD COMPOUNDS
Gold is administered in the form of organic complexes;
sodium aurothiomalate and auranofin are the two most
common preparations.
The effect of gold compounds develops slowly over 3-4
months.
Pain and joint swelling subside, and the progression of bone
and joint damage diminishes.

The mechanism of action is not clear, but auranofin,
although not aurothiomalate, inhibits the induction of IL-1
and TNF-alpha.

Pharmacokinetics:
Sodium aurothiomalate is given by deep intramuscular
injection; auranofin is given orally.
The half-life is 7 days initially but increases with treatment,
so the drug is usually given first at weekly, then at monthly
intervals.
Unwanted effects with auranofin are less frequent and less
severe. Important unwanted effects include skin rashes ,
mouth ulcers, proteinuria, thrombocytopenia and blood
dyscrasias.
Encephalopathy, peripheral neuropathy and hepatitis can
occur.
If therapy is stopped when the early symptoms appear, the
incidence of serious toxic effects is relatively low.

HYDROXYCHLOROQUINE AND CHLOROQUINE
Chloroquine is usually reserved for cases where other
treatments have failed.
The antirheumatic effects do not appear until a month or
more after the drug is started, and only about half the
patients treated respond.

The mechanism of the anti-inflammatory action : unclear.
The following mechanisms have been proposed:
suppression of t-lymphocyte responses to Mitogens,
decreased leukocyte chemotaxis,
stabilization of lysosomal Enzymes,
inhibition of DNA and RNA synthesis, and the
Trapping of free radicals.

IMMUNOSUPPRESSANT DRUGS
They can be roughly characterised as:
Drugs that inhibit IL-2 production or action (eg.
Ciclosporin, tacrolimus)
Drugs that inhibit cytokine gene expression (eg.
corticosteroids)
Drugs that inhibit purine or pyrimidine synthesis (eg.
Azathioprine).
To slow the progress of rheumatoid and other arthritic
diseases including psoriatic arthritis, ankylosis spondylitis,
juvenile arthritis:
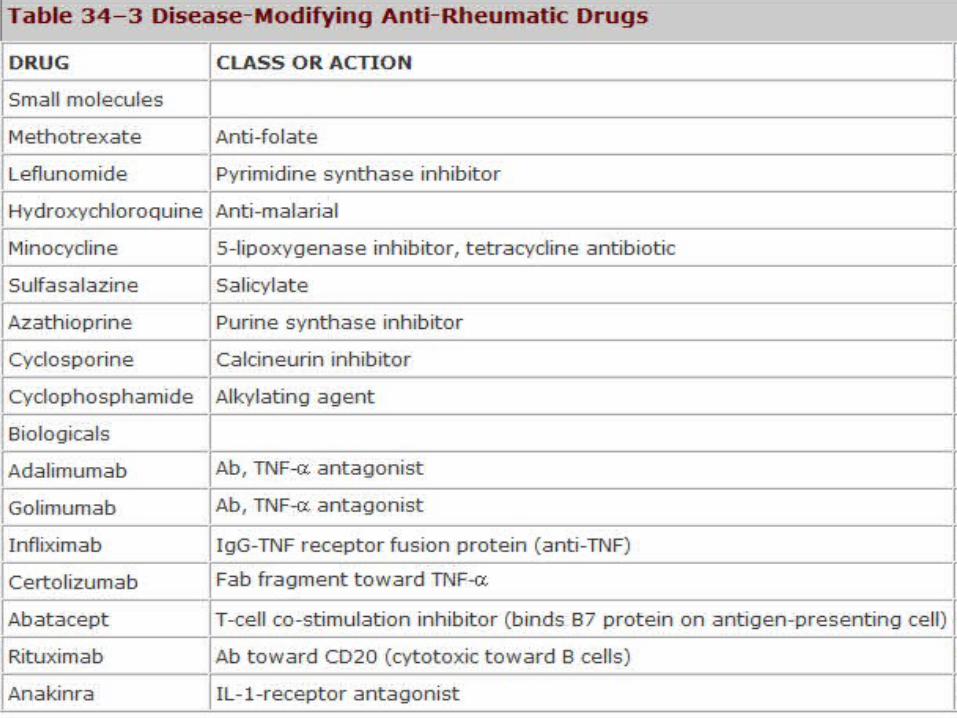
disease-modifying anti-rheumatic drugs (DMARDS), eg.
Methotrexate, leflunomide, ciclosporin;
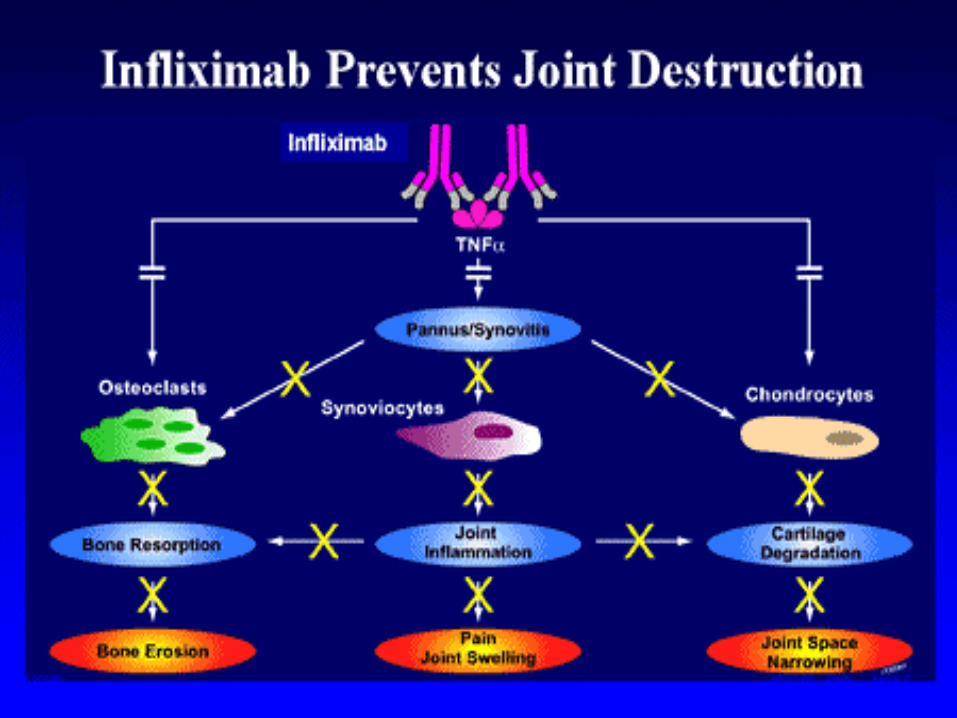
cytokine modulators (eg. Adalimumab, etanercept,
infliximab) are used when the response to methotrexate or
other DMARDS has been inadequate.

Leflunomide
Leflunomide has a relatively specific inhibitory effect on activated T cells
It is orally active and well absorbed from the gastrointestinal tract.
It has a long plasma half-life.
Unwanted effects include diarrhoea, alopecia, raised liver enzymes and indeed a risk of hepatic failure.