dka & hhs ahmad f. mady md 11/26/2015 10:30:08 pm 1
TRANSCRIPT

DKA & HHS
Ahmad F. Mady MD
04/18/23 04:04 PM
1

Diabetes
1552 BC, Diabetes 1st Described In Writing on 3rd
Dynasty Eqyptian papyrus by physician Hesy-Ra:
mentions polyuria as a symptom.
250 BC, Apollonius of Memphis coined the name
"diabetes” meaning "to go through" or siphon. He
understood that the disease drained more fluid than a
person could consume.
04/18/23 04:04 PM
2
Diabetes Mellitus
Gradually the Latin word for honey, "mellitus," was added to
diabetes because it made the urine sweet.
Up to 11th century diabetes was commonly diagnosed by
“water tasters” who drank the urine of those suspected of
having diabetes, as it was sweet-tasting.
04/18/23 04:04 PM
3

Early Diabetes Discoveries
In the 1869, Paul Langerhans, a German medical student
announced in a thesis, that the pancreas contains two systems
of cells.
In the1889 Oskar Minkowski and Joseph von Mering in France,
removed the pancreas from a dog to determine the effect of an
absent pancreas on digestion
04/18/23 04:04 PM
4

Fredrick Banting & Charles Best
04/18/23 04:04 PM
5

Leonard Thompson
04/18/23 04:04 PM
6

Three months later
04/18/23 04:04 PM
7

04/18/23 04:04 PM
8

04/18/23 04:04 PM
9

Ppt Factors of DKA&HHS
FactorApproximate frequency
Infection35%
Omission of insulin or inadequate insulin
30%
Initial presentation of
diabetes mellitus
20%
Medical illness10%
Unknown5%
04/18/23 04:04 PM
10

Clinical Presentation of DKA
History of polyuria, polydipsia, polyphagia, weight loss Nausea, vomiting, abdominal pain Acidemia leading to hyperventilation,Kussmaul
breathing,Ketotic odour. Clouding of sensorium, weakness, and coma Dehydration and shock
04/18/23 04:04 PM
11

Clinical Presentation of HHS
Similar to DKA but coma is more frequent Severe dehydration is the rule Focal neurologic deficits may be found at
presentation Usually more elderly patients Acidemia not pronounced
04/18/23 04:04 PM
12
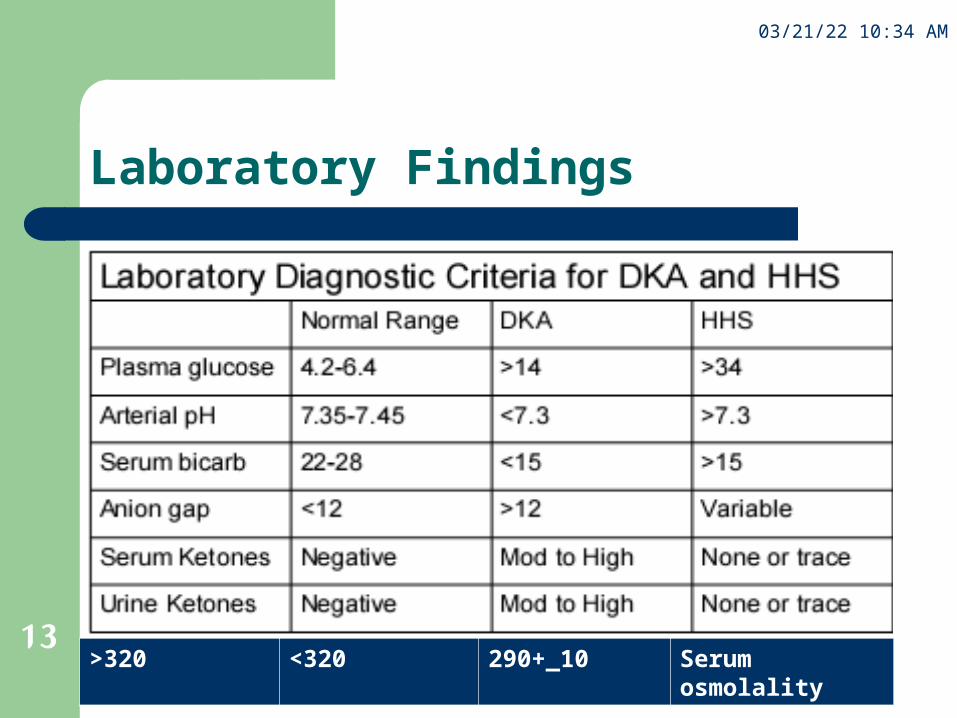
Laboratory Findings
Serum osmolality290+_10<320>320
04/18/23 04:04 PM
13

Treatment involves 5 key components:
Monitoring Fluid resuscitation Insulin and dextrose infusion Electrolyte repletion Treating underlying cause
Therapeutic goals
04/18/23 04:04 PM
14

Dehydration
WHY?……
04/18/23 04:04 PM
15

Fluids, fluids, fluids!
Restores circulatory volumeDiminish concentration of catecholamines, glucagon
04/18/23 04:04 PM
17

Caution!
Excessive therapy may result in ARDSCerebral edemaHyperchloremic acidosis
04/18/23 04:04 PM
18
Fluid replacement in DKA
Initial fluid = normal saline– 15ml to 20ml/kg, about 1-2L in 1 hour– 500 ml/h for next 2 hours or 1L /h if in shock– 500-250 ml/h according to hydration status (RBS 250mg/dl)
Subsequent change in fluids– half normal saline
START when urine output improves and BP stable– D5 1/2 NS
START when blood glucose <250 mg/dl Endpoint
- resolution of ketonemia and acidosis
- Se bicarbonate >18
04/18/23 04:04 PM
19

If SBP<90 mmHg
Initially give 1 litre of Normal Saline per hour.
If SBP>90 mmHg
0.45% N/S if serum sodium is high or normal
0.9% N/S if serum sodium is low.
Rate and volume as for DKA.
Rate should be adjusted for cardiac function
Fluid replacement in HHS
04/18/23 04:04 PM
20

Insulin administration in DKA&HHS
Withhold insulin therapy until the serum potassium
concentration has been determined.
Initial regular insulin
– Goal = reduce hourly glucose by 50-70 mg/dl
– Bolus = 0.15u/kg or 10u bolus
– IV infusion = 0.1u/kg/hr till RBS 250mg/dl then follow iv
infusion protocol
04/18/23 04:04 PM
21

Insulin administration in DKA&HHS
Endpoint for continuous/hourly regular insulin– Se bicarbonate >18, anion gap <14– Absence of serum ketones
Switch over to maintenance
Plasma glucose is less than 250 mg/dl
DKA has resolved
Patient is tolerating PO
It is important to give the first s.c. injection of insulin approximately 2 hours before stopping the i.v. route
04/18/23 04:04 PM
22

Intravenous Insulin Infusion Protocol
Capillary blood glucose in mg/dl (mmol/L)
Units of Insulin per Hour
<99 (5.5)0.5
100-149 (5.6-8.2)1
150-199 (8.3-11.0)2
200-249 (11.1-13.8)3
250-299 (13.9-16.6)4
300-349 (16.7-19.4)5
350-399 (19.5- 22.2)6
400-450 (22.3-24.9)8
>450 (24.9)10
04/18/23 04:04 PM
23

Who saved me: the insulin or the nurse ?
Who saved me: the insulin or the nurse ?
04/18/23 04:04 PM
24

Potassium Therapy
may be normal or elevated at the time of diagnosis
Goal is to maintain Se K between 4 and 5
If serum K>5 do not give K but recheck in one hour If serum K is 4-5 give KCl 20 mEq in each litre of fluid If serum K is 3-4 give KCl 30 mEq in each litre of fluid If serum K is <3 hold insuline,give KCl 40 mEq over 1hr then
recheck K
04/18/23 04:04 PM
26

Bicarbonate Therapy
Controversial– Most literature shows no benefit to using bicarbonate with
patients who have DKAor HHS No differences in reduction of glucose or ketoanion May increase hypokalemia, cerebral acidosis and
cardiac dysfunction– For patients with pH < 7.0, they may benefit from
bicarbonate therapy pH 6.9-7.0 may give 50 mEq of bicarb pH <6.9, may give 100 mEq of bicarb
04/18/23 04:04 PM
27

Phosphate Therapy
Phosphate deficiency– Osmotic diuresis → urinary phosphate losses– Insulin therapy → serum phosphate reenters intracellular compartment
Adverse complications may occur if P < 1.0 mg/dl
– Respiratory depression– Skeletal muscle weakness– Hemolytic anema– Cardiac dysfunction
May be useful to replace 1/3 potassium as K3PO4,reduce chloride load, prevent hyperchloremic acidosis.
04/18/23 04:04 PM
28

Investigations to be done
Serum glucose initially then hourly Serum K initially then hourly if <3 or >5 otherwise 2 hourly till stable Na, urea, creatinine initially then 4 hourly till stable ABG initially then as often as necessary Serum osmolality & Na hourly initially in HHS CBC with differential white count ECG, CXR Urine analysis Urine culture if pus cells or bacteria in U/A or patient is septic Blood culture if patient is febrile or WBC>12,000 Serum Mg and Ca Cardiac enzymes if ECG abnormal initially and after 8 hours Throat swab culture if signs of pharyngitis present Sputum culture if purulent looking or infiltrate on CXR Serum amylase (often raised-up to 10 times-even in the absence of pancreatitis)
04/18/23 04:04 PM
29

Avoid overhydration Note: Nitroprusside can be used to detect ketones but is not
accurate ….why? Prophylaxis small doses of LMW heparin Antibiotics: NOT routine Do consider anti-peptic ulcer prophylaxis
Considerations in management
04/18/23 04:04 PM
30

Complications
Lactic acidosis– Due to prolonged dehydration, shock, infection and tissue hypoxia
– Should be suspected in pt with refractory metabolic acidosis and
persistent anion gap Arterial thrombosis
– Stroke, MI, or an ischemic limb Cerebral edema
– Over hydration of free water, excessively rapid correction of
hyperglycemia are risk factors ARDS
– Excessive crystalloid infusion
– Pulmonary rales, increased AaO2 gradient
04/18/23 04:04 PM
31

Mortality from DKA
is due to?
1) Hyperglycemia
2) Acidosis
3) Sepsis
4) Hypokalemia
5) Cerebral edema
04/18/23 04:04 PM
32

Protocol
DKA
04/18/23 04:04 PM33

04/18/23 04:04 PM
34

Three Take Home Messages
1. DKA &HHS may be life threatening
2. Fluids and Insulin along with frequent
monitoring is essential
3. Watch for hypokalemia and cerebral edema
04/18/23 04:04 PM
35

Thank you for your attention
Thank you for saving me from DKA&HHS
Thank you for saving me from DKA&HHS
04/18/23 04:04 PM
36

Thank youThank you
AAHHMMAADD FF. . MMAADDYY MD MD