disseminated eosinophilic infiltration ofa newborninfant ... · there was nobirth asphyxia, regular...
TRANSCRIPT

66 Shinozaki, Saito, and Shiraki
infant who acquired hepatitis from her mother. Br Med J1970; iv: 719-21.
3 Bancroft W H, Warkel R L, Talbert A A, Russell P K.Family with hepatitis-associated antigen. JAMA 1971;217:1817-20.McCarthy J W. Hepatitis B antigen (HBAg)-positivechronic aggressive hepatitis and cirrhosis in an 8-month-old infant. A case report. JPediatr 1973; 83: 638-9.
5 Fujiwara T, Abe M, Tachi N, Jo M, Shiroda M.HBsAg-positive infantile hepatitis associated with chronicaggressive hepatitis (in Japanese). Shonika Rinsho 1975;28:1303-6.
6 Yoshida A, Tozawa M, Furukawa N, Oya N, Kusunoki T,Kiyosawa N. HBsAg-positive chronic active hepatitis ina 1 and 1/2 year-old-child (in Japanese). Shonika Shinryo1977;40: 1246-50.
Correspondence to Dr T Shinozaki, Department ofPaediatrics, Teikyo University School of Medicine, 11-1Kaga, 2 Chome, Itabashi-ku, Tokyo 173, Japan.
Received 26 November 1979
Disseminated eosinophilic infiltration of a newborn infant, withperforation of the terminal ileum and bile duct obstruction
S M MURRAY AND C J WOODS
Department ofPathology and Department ofPaediatrics, Victoria Hospital, Blackpool
SUMMARY A preterm boy died 4 days after deliveryfrom septicaemia which at necropsy was found to bedue to perforation of an eosinophilic lesion of theterminal ileum. Eosinophilic infiltration was alsofound in kidney, lymph node, bone marrow, portaltracts of liver, gall bladder, and bile duct with associ-ated obstruction of the cystic duct and mucocele ofthe gall bladder. No allergic cause for the infiltratewas found in either the infant or his mother. Eosino-philic infiltration of neonatal spleen, lymph node,intestinal mucosa, epicardium, thymus, pancreas,portal tracts of the liver, and skin has been reportedbut the aggressive behaviour of the infiltrate in thispatient bears more resemblance to the eosinophilicgastroenteritis that has been described in olderchildren and adults.
Eosinophilic infiltration of the alimentary tract of theadult occurs in two forms-namely eosinophilicgastroenteritis and inflammatory fibroid polyp of thegastrointestinal tract-each has been compre-hensively reviewed by Johnstone and Morson.1-2The condition is described much less often in childrenand in two reviews3-4 only 13 cases were recorded inchildren under 12 years, the youngest being a 2-year-old boy. Eosinophilic infiltration of the gastro-intestinal tract has also been described in neonatalnecrotising enterocolitis5 but the significance of thisinfiltrate is unknown. No reference to disseminatedeosinophilic infiltration in the neonate followed byintestinal perforation has been found in a search ofthe recent literature.
Case report
A white boy, weighing 1490 g, was born by spon-taneous vertex delivery at 35 weeks' gestation to ahealthy 19-year-old rubella-immune group A Rh-positive mother, who had a severe antepartumhaemorrhage due to placenta praevia. The pregnancyhad been uneventful, apart from vaginal bleeding at13 and 18 weeks which had settled without treatmenton each occasion. No drugs had been taken during thepregnancy.There was no birth asphyxia, regular respirations
were established within 1 minute and, apart frombeing preterm, there were no abnormalities onclinical examination. 1-mg of vitamin K1 wasgiven intramuscularly. Intermittent intragastric tubefeeding with low solute milk was started and, apartfrom occasional regurgitation of small amounts offeed, the infant made satisfactory progress.Meconium was first passed at age 8 hours.At age 48 hours the infant's condition deteriorated
suddenly with the clinical picture of peripheralcirculatory failure. There was no significantabdominal distention. Cerebrospinal fluid showedonly 1 lymphocyte/mm3 and no organisms werefound on microscopical examination or culture.The haemoglobin was 10 9 g/dl, packed cell volume33.9%/, and white blood count 1000 x 109/l. Thescanty nucleated cells seen in the blood film wereeither lymphocytes or normoblasts with no increasein eosinophils.
Septicaemia was diagnosed and treatment withintravenous gentamicin and cloxacillin was started.
on January 5, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.1.66 on 1 January 1981. Dow
nloaded from

Disseminated eosinophilic infiltration ofa newborn infant 67
Oral feeding was stopped and intravenous dextrosesaline started. Blood culture subsequently grewEscherichia coli sensitive to gentamicin.At age 53 hours the infant had a severe apnoeic
attack requiring endotracheal intubation and inter-mittent positive pressure ventilation. 30-ml of bloodwere transfused and metabolic acidosis correctedwith intravenous sodium bicarbonate. However, atage 72 hours abdominal distension developed andthe limbs showed sclerematous changes. Refractoryhypoxaemia and acidosis ensued and despite con-tinued mechanical ventilation the infant died. He wasaged 90 hours.
Necropsy findings
Perforation of a severely congested short segment ofterminal ileum had caused acute peritonitis. The gallbladder was distended with clear mucus and althoughthe common bile duct and hepatic ducts appeared to
be patent even a fine probe could not be passed alongthe cystic duct. The lungs were severely congested.The other organs appeared normal.
Histological examination. The perforated segment ofterminal ileum showed intense congestion andoedema with infiltration of the entire thickness of thewall by large numbers of eosinophils together withsome lymphocytes and plasma cells (Figs 1 and 2).The serosal surface showed a fibrino-purulent exu-date containing, in addition to polymorphonuclearleucocytes, numerous clumps of Gram-negativebacilli and moderate numbers of eosinophils. Thegall bladder showed mild focal infiltration of its wallby mononuclear cells and eosinophils while the bileducts, particularly the cystic duct, showed severecongestion and oedema with cellular infiltrationresembling that of the ileum. The liver showedhaematopoiesis of normal extent for a preterm infantof this size but eosinophils were absent from these
Fig. 1 Full thickness section of- terminal ileum near point of
-l_ N perforation showing cellularinfiltration. Prominent dilatedblood vessels are seen in thesubmucosa. (H and E x 178).
on January 5, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.1.66 on 1 January 1981. Dow
nloaded from

68 Murray and Woods
Fig. 2 Greater magnification ofboxed area of Fig. 1. 49% of thecells in this field are eosinophils.(H and E x 1650).
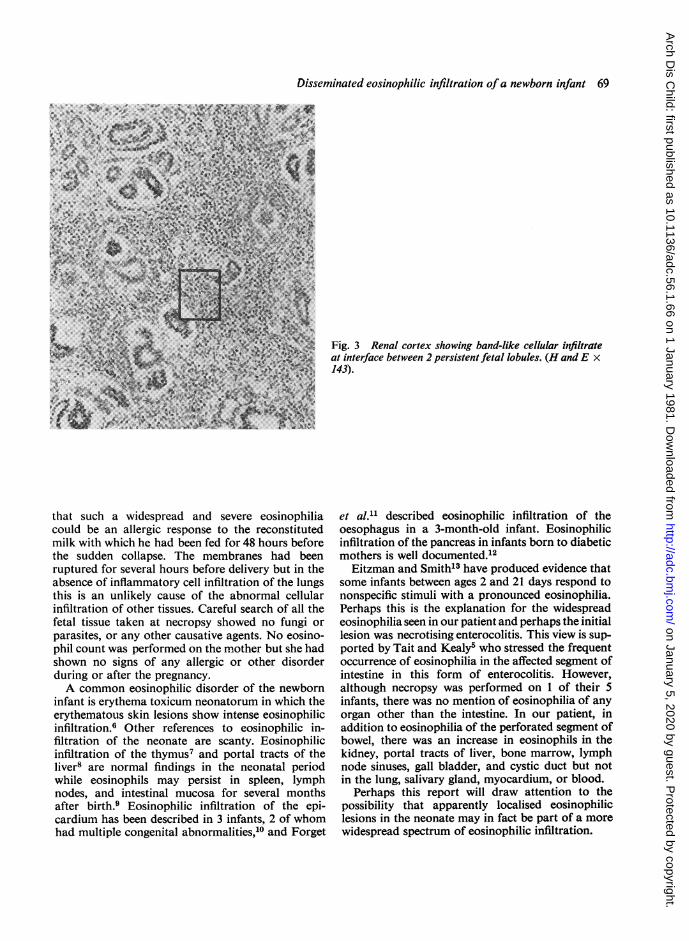
haematopoietic foci. The portal tracts containednumerous eosinophils but there was no significantincrease in portal fibrous tissue.The subcapsular region of the kidney showed
infiltration by eosinophils which extended deeplyinto the cortex in a linear manner associated with thenephrogenic formations at the margins of persistentfetal lobules (Figs 3 and 4). The lungs showedintense congestion and intra-alveolar haemorrhagebut there was no inflammatory cell infiltration and noeosinophil infiltration. Extra medullary haemato-poiesis was not present in the lung. Bone marrowfrom sternum and upper end of femur was modera-tely cellular and contained large numbers of matureand immature eosinophils. The subcapsular sinusesof a lymph node from the neck were infiltrated byeosinophils but these were not seen elsewhere in thenode. Salivary gland and myocardium appeared
normal. In all the tissues except bone marrow theeosinophils were of mature form. Mast cells were notgreatly increased in any of the tissues.
Discussion
The sequence of events in this infant appeared to beeosinophilic infiltration of various organs, particu-larly the terminal ileum, followed by perforation ofthe terminal ileum and death from E. coli peritonitis.The main interest is in the nature of the eosinophilicinfiltrate and this suggests an inflammatory ratherthan a neoplastic process. The abnormal histiocyticcells characteristic of Letterer Siwe's disease are notseen and the findings do not support a diagnosis ofeosinophilic leukaemia.The infant lived for only 4 days and it is unlikely
on January 5, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.1.66 on 1 January 1981. Dow
nloaded from
Disseminated eosinophlilic infiltration ofa newborn infant 69
that such a widespread and severe eosinophiliacould be an allergic response to the reconstitutedmilk with which he had been fed for 48 hours beforethe sudden collapse. The membranes had beenruptured for several hours before delivery but in theabsence of inflammatory cell infiltration of the lungsthis is an unlikely cause of the abnormal cellularinfiltration of other tissues. Careful search of all thefetal tissue taken at necropsy showed no fungi or
parasites, or any other causative agents. No eosino-phil count was performed on the mother but she hadshown no signs of any allergic or other disorderduring or after the pregnancy.A common eosinophilic disorder of the newborn
infant is erythema toxicum neonatorum in which theerythematous skin lesions show intense eosinophilicinfiltration.6 Other references to eosinophilic in-filtration of the neonate are scanty. Eosinophilicinfiltration of the thymus7 and portal tracts of theliver8 are normal findings in the neonatal periodwhile eosinophils may persist in spleen, lymphnodes, and intestinal mucosa for several monthsafter birth.9 Eosinophilic infiltration of the epi-cardium has been described in 3 infants, 2 of whomhad multiple congenital abnormalities,10 and Forget
Fig. 3 Renal cortex showing band-like cellular infiltrateat interface between 2 persistent fetal lobules. (H and E x143).
et al.11 described eosinophilic infiltration of theoesophagus in a 3-month-old infant. Eosinophilicinfiltration of the pancreas in infants born to diabeticmothers is well documented.12Eitzman and Smith'3 have produced evidence that
some infants between ages 2 and 21 days respond tononspecific stimuli with a pronounced eosinophilia.Perhaps this is the explanation for the widespreadeosinophilia seen in our patient and perhaps the initiallesion was necrotising enterocolitis. This view is sup-ported by Tait and Kealy5 who stressed the frequentoccurrence of eosinophilia in the affected segment ofintestine in this form of enterocolitis. However,although necropsy was performed on 1 of their 5infants, there was no mention of eosinophilia of anyorgan other than the intestine. In our patient, inaddition to eosinophilia of the perforated segment ofbowel, there was an increase in eosinophils in thekidney, portal tracts of liver, bone marrow, lymphnode sinuses, gall bladder, and cystic duct but notin the lung, salivary gland, myocardium, or blood.
Perhaps this report will draw attention to thepossibility that apparently localised eosinophiliclesions in the neonate may in fact be part of a morewidespread spectrum of eosinophilic infiltration.
on January 5, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.1.66 on 1 January 1981. Dow
nloaded from

70 Murray and Woods
.......AW.......
..........
X:
;: .%:
XXX,X
....................
N
X.X
...... ....
2
.......
..............
X X
Fig. 4 Greater magnification ofboxed area of Fig. 3. Eosinophilsare indicated by arrows. (H and
.:.:::.:.A.:.:.:.:.. 1450).
..................
References
' Johnstone J M, Morson B C. Eosinophilic gastroenteritis.Histopathology 1978; 2: 335-48.
2 Johnstone J M, Morson B C. Inflammatory fibroid polypof the gastrointestinal tract. Histopathology 1978; 2:349-61.
3 Jona J Z, Belin R P, Burke J A. Eosinophilic infiltrationof the gastrointestinal tract in children. Am J Dis Child1976; 130: 1136-9.
4 Hoefer R A, Ziegler M M, Koop C E, Schnaufer L.Surgical manifestations of eosinophilic gastroenteritis inthe pediatric patient. JPediatr Surg 1977; 12: 955-62.
Tait R A, Kealy W F. Neonatal necrotising enterocolitis.J Clin Pathol 1979; 32: 1090-9.
6 Freeman R G, Spiller R, Knox J M. Histopathology oferythema toxicum neonatorum. Arch Dermatol 1960; 82:586-9.
7 Bhathal P S, Campbell P E. Eosinophil leucocytes in thechild's thymus. Australas Ann Med 1965; 14: 210-3.
8 Potter E L, Craig J M. Pathology of the fetus and theinfant. London: Lloyd-Luke, 1976: 395-6.
9 Dourov N. Les eosinophiles tissulaires au cours dela periode p6rinatale humaine. Pathol Eur 1967; 2:124-45.
10 Moragas A, Vidal M T. Granulomatous eosinophilic
on January 5, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.1.66 on 1 January 1981. Dow
nloaded from

Disseminated eosinophilic infiltration of a newborn infant 71
epicarditis in the newborn. Report of three cases. ArchPathol 1969; 88: 459-62.
11 Forget P, Eggermont E, Marchal G, Geboes K, Jaeken J,Melchior S. Eosinophilic infiltration of the oesophagus inan infant. Acta Paediatr Beig 1978; 31: 91-3.
12 Pedersen L M, Tygstrup I. Cell infiltration in the pancreasof newborn infants of diabetic mothers. Acta PatholMicrobiol Scand 1968; 73: 537-48.
13 Eitzman D V, Smith R T. The nonspecific inflammatorycycle in the neonatal infant. Am J Dis Child 1959; 97:326-34.
Correspondence to Dr S M Murray, Department ofPathology, Victoria Hospital, Blackpool FY3 8NR.
Received 29 January 1980.
Spontaneous oesophageal rupture with duodenal atresia in anewborn infant
HAJIME NAKAMURA, YOSHIHIKO KANAZAWA, MASAKI HAYANO, ANDSHINICHIRO MIMASU
Department ofPaediatrics, Kobe University School of Medicine, Japan
suMMARY A newborn infant with spontaneousoesophageal rupture associated with duodenalatresia is described. The diagnosis was established bythe pattern ofhydropneumothorax on the chest x-rayfilm and by the aspiration of gastric juice by thora-cocentesis. Necropsy showed a tear, which extendedfrom the oesophagogastric junction to the upperportion of the stomach.
Spontaneous oesophageal rupture in infancy is rare,but it is important to differentiate it from any otherdisease that causes serious respiratory distress orcyanosis shortly after birth. Since 1952, when thefirst case of oesophageal rupture was reported,'only 14 cases have been cited.2-3 The disease shows apattern of hydropneumothorax, a finding charac-teristic on chest x-ray films. It should therefore not betoo difficult to make an early diagnosis if one knowsof the existence of the disease. Some patients surviveearly surgical operation.
Case report
A Japanese boy was born after 38 weeks' gestationafter induction for hydramnios. Delivery had beenspontaneous with a vertex presentation. Birthweightwas 2 * 75 kg and he was the first child of a 26-year-oldmother. He cried spontaneously and required noresuscitation. Mucus was suctioned from the noseand nasopharynx, but no tube was passed into theoesophagus. Three hours after birth, breathing wasnoted to have become laboured and he was placed inan oxygen tent. By 19 hours, the infant was spittingsmall amounts of bright red blood and the respiration
was rapid, shallow, and grunting. He was transferredto this hospital.On initial examination he was moribund, in severe
respiratory distress, with pronounced cyanosis andcold extremities. The abdomen was distended andmovement was diminished on the right sideof the chest. Petechiae were found on the chestand abdominal walls. Plain x-ray film showedtension hydropneumothorax on the right (Figure).In addition, the stomach and duodenum weredistended, distal to which no gas was seen. Thoraco-centesis was performed; considerable amounts of airand 30 ml of bile-stained fluid were obtained.Respiratory effort was poor and he received assistedventilation: pH 6 98, Pao2 94 mmHg (12.5 kPa),Paco2 56 mmHg (7A4 kPa), base excess -16 mmol/l.At age 24 hours, a general haemorrhagic tendencyand sclerema neonatorum were noted. After exchangetransfusion with fresh heparinised blood, thetendency to bleed and the metabolic acidosis, as wellas his general condition were improved, but an x-rayfilm showed pneumoperitoneum.At age 92 hours, laparotomy was performed
through an upper midline incision. Purulent matterwas attached to the upper portion of lesser curvatureof stomach. When the stomach was pulled down, alongitudinal rupture 1 5 cm in length was found inthe anterolateral aspect of the lower end of theoesophagus, spanning the diaphragmatic hiatus andextending to the stomach. The rupture was closed.Atresia of the duodenum was found, the secondportion of which ended blindly at an annularpancreas. A duodenojejunostomy was fashioned. Agastrostomy was performed for feeding. The infanttolerated the procedures and chest x-ray showed
on January 5, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.56.1.66 on 1 January 1981. Dow
nloaded from