diseases of the esophagus prof. ferenc szalay md, phd budapest, 03.02.2003 lecture for students 1st...
TRANSCRIPT

DISEASES OF THE DISEASES OF THE ESOPHAGUSESOPHAGUS
DISEASES OF THE DISEASES OF THE ESOPHAGUSESOPHAGUS
Prof. Ferenc Szalay MD, PhD
Budapest, 03.02.2003 lecture for students
1st Department of Medicine of Semmelweis University 1st Department of Medicine of Semmelweis University Budapest, HungaryBudapest, Hungary
1st Department of Medicine of Semmelweis University 1st Department of Medicine of Semmelweis University Budapest, HungaryBudapest, Hungary

Diseases of the esophagusDiseases of the esophagusDiseases of the esophagusDiseases of the esophagusGERDGERDMotility disordersMotility disordersEsophagitisEsophagitis (infection, chemicals, pills)(infection, chemicals, pills)Neurological disordersNeurological disordersSkeletal muscle disordersSkeletal muscle disordersVaricesVarices Mallory-Weiss sy.Mallory-Weiss sy.BaBarrrreetttt’s’sTumorsTumors
GERDGERDMotility disordersMotility disordersEsophagitisEsophagitis (infection, chemicals, pills)(infection, chemicals, pills)Neurological disordersNeurological disordersSkeletal muscle disordersSkeletal muscle disordersVaricesVarices Mallory-Weiss sy.Mallory-Weiss sy.BaBarrrreetttt’s’sTumorsTumors
Common complainsCommon complainsWide range of symptomsWide range of symptomsCommon complainsCommon complainsWide range of symptomsWide range of symptoms

SwallowingSwallowingSwallowingSwallowingMany muscleMany muscle5 nerves : V, VII, IX, X, XII5 nerves : V, VII, IX, X, XIIStagesStages
oral oral - - voluntaryvoluntary
pharyngeal pharyngeal - - involuntaryinvoluntary
esophageal esophageal - - LES LES relaxedrelaxed1 second 5 steps1 second 5 steps
Many muscleMany muscle5 nerves : V, VII, IX, X, XII5 nerves : V, VII, IX, X, XIIStagesStages
oral oral - - voluntaryvoluntary
pharyngeal pharyngeal - - involuntaryinvoluntary
esophageal esophageal - - LES LES relaxedrelaxed1 second 5 steps1 second 5 steps

5 steps within 1 second5 steps within 1 second5 steps within 1 second5 steps within 1 second
1. Soft palate is elevated + retracted 1. Soft palate is elevated + retracted
to prevent nasopharingeal refluxto prevent nasopharingeal reflux
2. Vocal cords are closed2. Vocal cords are closed
Epiglottis swings backward Epiglottis swings backward closure the larynxclosure the larynx
3. UES relaxes3. UES relaxes
4. Larynx is pulled upward4. Larynx is pulled upward
streching, opening E and UESstreching, opening E and UES
5. Contractions of pharyngeal muscle5. Contractions of pharyngeal muscle
1. Soft palate is elevated + retracted 1. Soft palate is elevated + retracted
to prevent nasopharingeal refluxto prevent nasopharingeal reflux
2. Vocal cords are closed2. Vocal cords are closed
Epiglottis swings backward Epiglottis swings backward closure the larynxclosure the larynx
3. UES relaxes3. UES relaxes
4. Larynx is pulled upward4. Larynx is pulled upward
streching, opening E and UESstreching, opening E and UES
5. Contractions of pharyngeal muscle5. Contractions of pharyngeal muscle

Anatomy

Anatomy


Motility disorders of oropharynxMotility disorders of oropharynxMotility disorders of oropharynxMotility disorders of oropharynx• Dysfunction of the UES
Zenker’s diverticulum, Cricopharingeal bar
• Neurologic disorders (stroke)Cerebrovascular diseases, PoliomyelitisAmyotrophic lateral sclerosis, Multiple sclerosis, Brain stem tumor
• Skeletal musclular disordersMyastenia gravis, Metabolic myopathy (T4 toxicosis, myxedema, steroid)Muscular dystrophies
• Local structural lesionsNeoplasms, extinsic compression (Thyroid, cervical spur), Surgery
Common problem in the elderly patients and frequently associated with poor prognosis owing to a high incidence of aspiration

Zenker’s diverticulumZenker’s diverticulumZenker’s diverticulumZenker’s diverticulum

Motility disorders of the esophagusMotility disorders of the esophagusMotility disorders of the esophagusMotility disorders of the esophagus
Smooth muscle diseases (scleroderma)Smooth muscle diseases (scleroderma) Intrinsic nervous system Intrinsic nervous system
AAchalasiachalasia, Chagas disease, Chagas disease loss of ganglion cells in Auerbach plexusloss of ganglion cells in Auerbach plexus
LES LES no peristalsis no peristalsis
Diffuse esophagus spasmDiffuse esophagus spasm and its variants and its variants
Smooth muscle diseases (scleroderma)Smooth muscle diseases (scleroderma) Intrinsic nervous system Intrinsic nervous system
AAchalasiachalasia, Chagas disease, Chagas disease loss of ganglion cells in Auerbach plexusloss of ganglion cells in Auerbach plexus
LES LES no peristalsis no peristalsis
Diffuse esophagus spasmDiffuse esophagus spasm and its variants and its variants

Esophagus motility disorder: sclerodermaEsophagus motility disorder: sclerodermaEsophagus motility disorder: sclerodermaEsophagus motility disorder: scleroderma

Achalasia: Chagas’ diseaseAchalasia: Chagas’ diseaseAchalasia: Chagas’ diseaseAchalasia: Chagas’ disease
Cause:
Tripanosoma Cruzi inf.

Diffuse esophageal spasmsDiffuse esophageal spasmsDiffuse esophageal spasmsDiffuse esophageal spasms

Rings and WebsRings and WebsRings and WebsRings and Webs
Schatzki’s ringSchatzki’s ring- proximal or distal- proximal or distal- congenital or secondary to GERD- congenital or secondary to GERD
Plummer Vinson syndromePlummer Vinson syndrome- upper E web- upper E web- dysphagia- dysphagia- irondeficiency anemia- irondeficiency anemia
Symptoms if diameter < 13 mmSymptoms if diameter < 13 mm- intermittent dysphagia for solid food- intermittent dysphagia for solid food- sudden: “steak house syndrome”- sudden: “steak house syndrome”
TreatmentTreatment- mechanical dilators- mechanical dilators
Schatzki’s ringSchatzki’s ring- proximal or distal- proximal or distal- congenital or secondary to GERD- congenital or secondary to GERD
Plummer Vinson syndromePlummer Vinson syndrome- upper E web- upper E web- dysphagia- dysphagia- irondeficiency anemia- irondeficiency anemia
Symptoms if diameter < 13 mmSymptoms if diameter < 13 mm- intermittent dysphagia for solid food- intermittent dysphagia for solid food- sudden: “steak house syndrome”- sudden: “steak house syndrome”
TreatmentTreatment- mechanical dilators- mechanical dilators
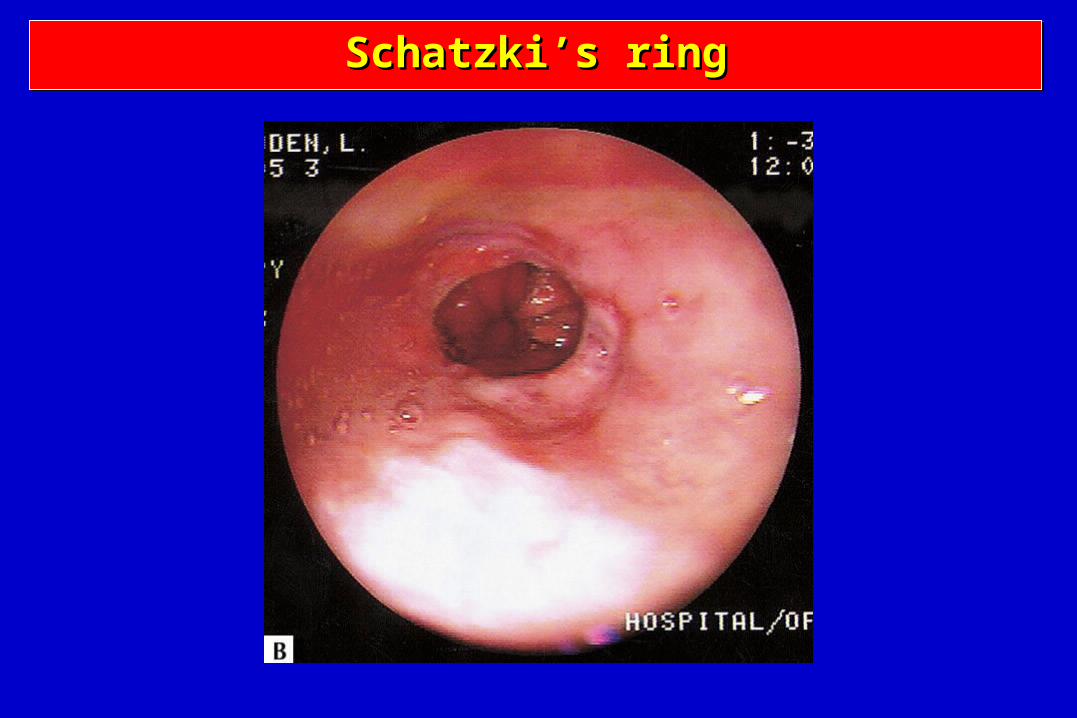
Schatzki’s ringSchatzki’s ringSchatzki’s ringSchatzki’s ring

Endoscopic image of the narrow Endoscopic image of the narrow area in mid-esophagusarea in mid-esophagus

Post-mortem specimen from a similar case of esophageal Post-mortem specimen from a similar case of esophageal narrowing in a young boxer.narrowing in a young boxer.

Map of lymph nodes near the oesophagus

Radiographic evaluation in suspected esophageal cancer

Gastroesophageal junction Gastroesophageal junction type II tumorstype II tumors

Esophageal cancer


AJCC Staging of Esophagus: TNM Staging
Regional lymph nodes (N)Nx Regional lymph nodes cannot be assassedN0 No regional lymph node metastasisN1 Regional lymph node metastasis
Distant metastasis (M)Mx Distant metastasis cannot be assassedM0 No distant metastasisM1 Distant metastasis
Tumors of lower or upper esophagusM1a Metastasis in nonregional lymph nodeM1b Distant metastasis (eg: liver, bone, brain)
Tumors of middle esophagusM1a Not applicableM1b Metastasis in nonregional lymph node or distant metastasis (eg: liver, bone, brain)

AJCC Staging of Esophagus: TNM Staging
Stage Tumor Node Metastasis
Stage 0 Tis N0 M0Stage I T1 N0 M0
T2 N0 M0Stage IIA T3 N0 M0
T1 N1 M0Stage IIB T2 N1 M0
T3 N1 M0Stage III T4 Any N M0Stage IV Any T Any N M1Stage IV A Any T Any N M1aStage IV B Any T Any N M1b

Resected esophageal specimen

Other esophageal disorders
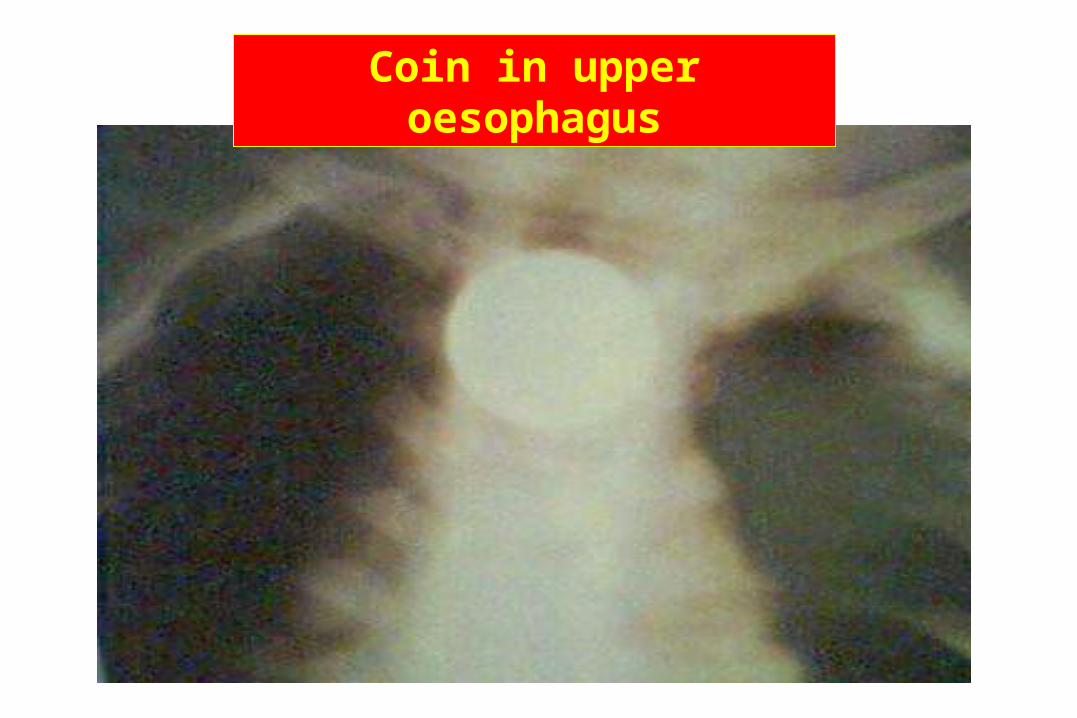
Coin in upper oesophagus

INFECTIONS OF THE OESOPHAGUSINFECTIONS OF THE OESOPHAGUSINFECTIONS OF THE OESOPHAGUSINFECTIONS OF THE OESOPHAGUS
Viral herpes, CMVFungal Candida
Most common in immuncompromized patients:AIDSImmunosuppressive treatmentImmune defectsAntibiotic os steroid treatment

Candida oesophagitisCandida oesophagitisCandida oesophagitisCandida oesophagitis
Acid-related Acid-related diseases of the diseases of the
oesophagus oesophagus GERD / GORDGERD / GORD

Talley et al., BMJ 2001; 323: 1294–7.de Caestecker, BMJ 2001; 323: 736–9.
Nathoo, Int J Clin Pract 2001; 55: 465–9.Quigley, Eur J Gastroenterol Hepatol 2001; 13(Suppl 1): S13–18.
Heartburn:Heartburn: • Burning retrosternal pain radiating upward due to
exposure of the oesophagus to acid
Oesophagitis:Oesophagitis: • Endoscopically demonstrated damage to the
oesophageal mucosa
Gastro-oesophageal reflux disease (GORD):Gastro-oesophageal reflux disease (GORD):• Pathological reflux ranges from simple to erosive to
Barrett’s
Non-erosive reflux disease (NERD):Non-erosive reflux disease (NERD):• Reflux disease in which erosion does not occur
DefinitionsDefinitionsDefinitionsDefinitions

Impaired mucosal defence
de Caestecker, BMJ 2001; 323:736–9.Johanson, Am J Med 2000; 108(Suppl 4A): S99–103.
salivary HCO3
Hiatus herniaImpaired LOS (smoking, fat, alcohol)
– transient LOS relaxations
– basal toneH+
PepsinBile and
pancreatic enzymes
oesophageal clearance of acid (lying flat, alcohol, coffee)
acid output (smoking, coffee)
intragastric pressure (obesity, lying flat)
bile reflux gastric emptying (fat)
Pathophysiology of GORDPathophysiology of GORDPathophysiology of GORDPathophysiology of GORD

Diagnosis of GORDDiagnosis of GORDDiagnosis of GORDDiagnosis of GORD• History
1. Does reflux exist? 2. Is acid R responsible for symptoms? 3. Has R led to esophagus damage?
• Barium swallow• Radionuclide scintigraphy (99mTc sulfur colloid)
• E. manometry• Bernstein test• pH monitoring• Endoscopy

Bernstein testBernstein testBernstein testBernstein test
Retrosternal pain for 0.1 N HCl
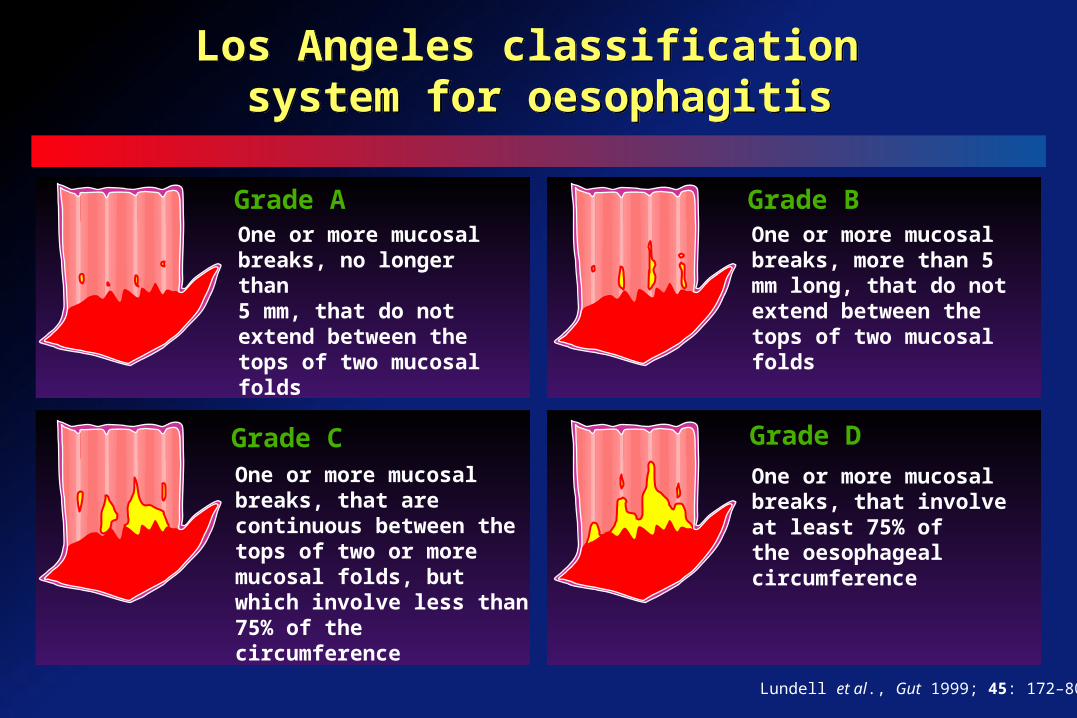
One or more mucosal breaks, no longer than 5 mm, that do not extend between the tops of two mucosal folds
Grade AOne or more mucosal breaks, more than 5 mm long, that do not extend between the tops of two mucosal folds
Grade B
One or more mucosal breaks, that are continuous between the tops of two or more mucosal folds, but which involve less than 75% of the circumference
Grade COne or more mucosal breaks, that involve at least 75% ofthe oesophageal circumference
Grade D
Lundell et al., Gut 1999; 45: 172–80.
Los Angeles classification system for oesophagitis
Los Angeles classification system for oesophagitis

Savary & Miller. The Esophagus. In: Handbook & Atlas of Endoscopy. Solothurn, Switzerland: Verlag Gassman AG, 1978: 119–205.
Savary-Miller classification of oesophagitis
Savary-Miller classification of oesophagitis
Grade I One or several erosions in one mucosal fold
Grade II Several erosions in several mucosal folds,
the erosions can merge
Grade III Erosions surrounding the oesophageal circumference
Grade IV Ulcer(s), strictures, shortening of the oesophagus
Grade V Barrett’s epithelium
Grade I - V

Quigley, Eur J Gastroenterol Hepatol 2001; 13(Suppl 1): S13–18.
Nathoo, Int J Clin Pract 2001; 55: 465–9.www.gastrolab.net
Savary-Miller classification
One or several erosions in one mucosal fold
Grade I oesophagitisGrade I oesophagitis

www.gastrolab.net
Savary-Miller classification
Several erosions in several mucosal folds, the erosions
can merge
Grade II oesophagitisGrade II oesophagitis

Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Savary-Miller classification
Erosions surrounding the oesophageal circumference
Grade III oesophagitisGrade III oesophagitis

Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Savary-Miller classification
Ulcer(s), shortening of the oesophagus
Grade IV oesophagitisGrade IV oesophagitis

Nadel, UCHC
Savary-Miller classification
Stricture
Grade IV oesophagitisGrade IV oesophagitis

Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Savary-Miller classification
Moderate Barrett’s oesophagus
Grade V oesophagitisGrade V oesophagitis

Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Savary-Miller classification
Moderate Barrett’s oesophagus
Grade V oesophagitisGrade V oesophagitis
Chromoendoscopic picture

Barrett’s dysplasiaBarrett’s dysplasiaBarrett’s dysplasiaBarrett’s dysplasia
Columnar cells instead of squamous cells

Freytag et al., Atlas of gastrointestinal endoscopy. www.home.t-online.de/home/afreytag/indexe.htm
Savary-Miller classification
Severe Barrett’s oesophagus
Grade V oesophagitisGrade V oesophagitis

Nadel/Saint Francis Hospital. In: Gastrointestinal Pathology. Fenoglio-Preiser, New York: Raven Press, 1989: 96–100.
Adenocarcinoma of the oesophagus
Adenocarcinoma of the oesophagus
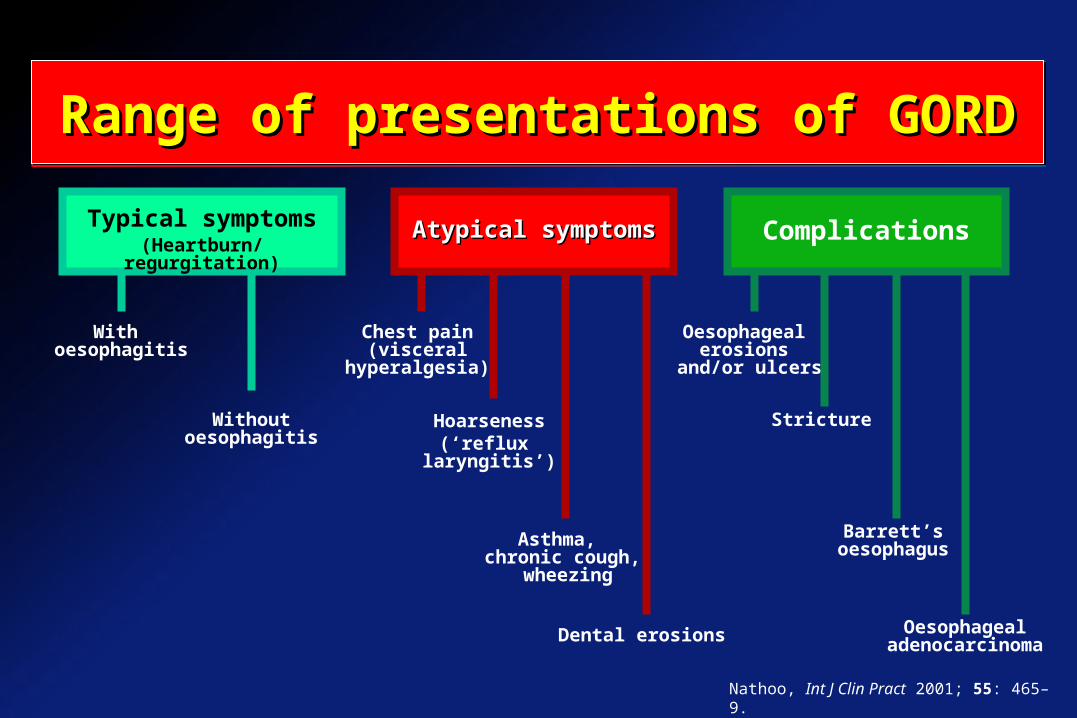
Typical symptoms(Heartburn/regurgitation)
Atypical symptomsAtypical symptoms Complications
With oesophagitis
Without oesophagitis
Chest pain(visceral
hyperalgesia)
Asthma, chronic cough,
wheezing
Hoarseness(‘reflux
laryngitis’)
Oesophageal erosions
and/or ulcers
Stricture
Barrett’s oesophagus
Oesophageal adenocarcinomaDental erosions
Nathoo, Int J Clin Pract 2001; 55: 465–9.
Range of presentations of GORDRange of presentations of GORDRange of presentations of GORDRange of presentations of GORD

Locke et al., Gastroenterology 1997; 112: 1448–56.
Pre
vale
nce
(%
)
25–34 35–44 45–54 55–64 65–74
Age (years)
40
0
Women: at least weekly episodes
Men: at least weekly episodes
Prevalence of heartburn or acid regurgitation
Prevalence of heartburn or acid regurgitation
%

Ast
hm
a p
atie
nts
exp
erie
nci
ng
GO
RD
sy
mp
tom
s (%
)
Perrin-Fayolle et al. (n=150)
O’Connell et al.(n=189)
Field et al. (n=109)
Harding & Sontag, Am J Gastroenterol 2000; 95(Suppl): S23–32.
100
80
60
40
20
0
6572
77
GORD can be a trigger for asthma
GORD can be a trigger for asthma

Wheezing or shortness of breath
Cough
Chest pain
Heartburn
Regurgitation
Nausea
Asthmatic patients with GORD (n=118)
Harding et al., Chest 1999; 115: 654–9.
Respiratory and oesophageal symptoms associated with oesophageal acid events (%)
Correlation of respiratory and oesophageal Correlation of respiratory and oesophageal symptoms with oesophageal acid eventssymptoms with oesophageal acid events
Correlation of respiratory and oesophageal Correlation of respiratory and oesophageal symptoms with oesophageal acid eventssymptoms with oesophageal acid events
65
98
60
83
87
91
0 20 40 60 80 100

Oesophageal acid-induced bronchoconstriction:
vagally mediated oesophageal bronchial reflex
heightened bronchial reactivity microaspiration
Evidence of airway inflammation: Substance P and tachykinin release
Increase: minute ventilation respiratory rate
Harding & Sontag, Am J Gastroenterol 2000; 95(Suppl): S23–32.
Mechanism of asthma symptoms on exposure to oesophageal acid
Mechanism of asthma symptoms on exposure to oesophageal acid
Asthma symptoms plus oesophageal acid

Receptors Cough centreVN Vagus nerveN Cortical input
Irwin & Madison, Am J Med 2000; 108(Suppl 4A): S126–30.
Chronic cough and GORD
Chronic cough and GORD

Kiljander et al., Chest 1999; 16: 1257–64.
Sym
pto
m
sco
re
Effect of PPI on pulmonary and GI symptoms in asthma patients
Effect of PPI on pulmonary and GI symptoms in asthma patients
14
12
10
8
6
4
2
0
Pulmonary symptoms score
Gastric symptom score
Placebo
Weeks PPI
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18

Oesophageal stricture
Barrett’s oesophagus
Oesophageal adenocarcinoma
Anaemia
Savary-Miller Grade IV and above
Nathoo, Int J Clin Pract 2001; 55: 465–9.
Consequences of severe and Consequences of severe and prolonged GORDprolonged GORD
Consequences of severe and Consequences of severe and prolonged GORDprolonged GORD
• Oesophageal stricture
• Barrett’s OE
• OE Adenocarcinoma
• Anemia
Oesophageal cancerOesophageal spasmGORDGlobus hystericusEpiglottitisIngestion of caustic substancesPharyngitisPeritonsillar abscessForeign bodyOesophageal candidiasis
Differential diagnosis of oesophageal stricture
Differential diagnosis of oesophageal stricture

1. Jankowski et al., The Lancet 2000; 356: 2079–85.2. Gore et al., Aliment Pharmacol Ther 1993; 7: 623–8.
3. Spechler. Digestion 1992; 51(Suppl 1): 24–9.4. Peters et al., Gut 1999; 45: 489–94.
Barrett’s found at endoscopy: 0.5–2%1
Barrett’s found while investigating GORD: 10–15%2,3
Barrett’s is common in white males4
Prevalence of adult heartburn: 20–40%3
Barrett’s increases the risk of oesophageal cancer 50–100-fold4
Prevalence and risks of Barrett’s oesophagus in Europe/USA
Prevalence and risks of Barrett’s oesophagus in Europe/USA

0
500
1000
1500
2000
2500
3000
3500
4000
79 84 89 94 97
Mo
rtal
ity
Year
Office of National Statistics, 1999.
Mortality due to oesophageal adenocarcinoma in England and Wales
Mortality due to oesophageal adenocarcinoma in England and Wales

Lagergren et al., N Engl J Med 1999; 340: 825–31.
Od
ds
rat
io
20
0None 1 2–3 >3 0 <12 12–20 >20
Frequency
Chronicity
1
5.1
6.3
16.7
1
5.2
16.4
7.5
Heartburn episodes/week Duration of symptoms (years)
Frequency and duration of symptoms
Heartburn as a risk factor for oesophageal adenocarcinomaHeartburn as a risk factor for oesophageal adenocarcinoma

Management of upper GI symptoms Management of upper GI symptoms in primary carein primary care
Management of upper GI symptoms Management of upper GI symptoms in primary carein primary care
Appropriate treatment
Age >45
Test-and-treat for H. pylori
Treat empirically
Clinical history
Heartburn (GORD)
Manage with antisecretory
agents
Upper abdominal pain/dyspepsia
Early endoscopy
Alarm features

Odynophagia
Dysphagia
Vomiting
Bleeding
Weight loss
Alarm Alarm featuresfeatures
Nathoo, Int J Clin Pract 2001; 55: 465–9.
Alarm features for GORDAlarm features for GORDAlarm features for GORDAlarm features for GORD

Careful analysis of symptoms and history is key to diagnosis
Diagnosis based on symptoms can be aided by a trial of treatment
Clear endoscopic abnormalities are found in <50% of patients
Treatment should start with a proton pump inhibitor (PPI)
Most patients will require long-term treatment; anti-reflux surgery may be as effective as PPIs, but is less predictable
Summary of conclusions from a multidisciplinary workshop held in Genval, Belgium in 1999.Dent et al., BMJ 2001; 322: 344–7.
European practice guidelines: European practice guidelines: GORDGORD
European practice guidelines: European practice guidelines: GORDGORD

Alarm symptoms (e.g. dysphagia, weight loss, bleeding, abdominal mass)
Diagnostic problems (e.g. atypical symptoms)
Heartburn for 5 years or longer
Failure to respond to initial treatment
Pre-operative assessment
Dent et al., BMJ 2001; 322: 344–7.
When should endoscopy be considered in patients with GORD?
When should endoscopy be considered in patients with GORD?

Hiatus hernia
Oesophageal stricture
Oesophageal cancer
Chest pain of cardiac origin
Functional dyspepsia
Nathoo, Int J Clin Pract 2001; 55: 465–9.
Differential diagnosis of GORDDifferential diagnosis of GORDDifferential diagnosis of GORDDifferential diagnosis of GORD

Treatment options in GORDTreatment options in GORD• Simple (lifestyle) measures• Medical treatment
antacidsacid secretion suppressors -
PPI, H2RAs, H.p. erad. prokinetics
• Surgery (laparascopic)

Reduce weight
Stop smoking
Avoid reflux-promoting agents (e.g. alcohol, coffee, some foods) (not evidence based)
Elevate headof bed
Consider alternatives to
reflux-promoting drugs (e.g. theophylline, anticholinergics)
ModificationsModifications
Eat small meals,no late meals, reduce
fat
Lifestyle modificationsLifestyle modifications for the management of GORDfor the management of GORD
Lifestyle modificationsLifestyle modifications for the management of GORDfor the management of GORD

Increase the pH of gastric refluxate Reduce the erosive effect and hence reduce symptoms
Suitable for quick relief of mild symptoms
Most antacids are not suitable therapies for established GORD or oesophagitis
Less effective than H2RAs or PPIs for treatment of GORD
Adverse effects include: Accumulation in patients with renal impairment Milk-alkali syndrome with high doses Constipation Diarrhoea
Sonnenberg A, Pharmacoeconomics 2000; 17: 391–401.de Caestecker, BMJ 2001; 323: 736–9.
Hatlebakk & Berstad, Clin Pharmacokinet 1996; 31: 386–406.Scott & Gelhot, Am Fam Physic 1999; 59: 1161–9.
AntacidsAntacids
AntacidsAntacids

Inhibit histamine stimulation of gastric parietal cell, resulting in reduced gastric acid secretion
Slower onset but longer duration of action than antacids
Cimetidine is associated with more drug interactions than other H2RAs, such as ranitidine
H2RAs are generally not as effective as PPIs for symptom relief or healing
de Caestecker, BMJ 2001; 323: 736–9.Sonnenberg, Pharmacoeconomics 2000; 17: 391–401.
H2-receptor antagonists (H2RAs)H2-receptor antagonists (H2RAs)HH22-receptor antagonists (H-receptor antagonists (H22RAs)RAs)

Omeprazole
Lansoprazole
Pantoprazole
Rabeprazole
Esomeprazole
But are they all the same?
Available PPIs in Europe in 2002Available PPIs in Europe in 2002
Available Available PPIsPPIs in Europe in 2002 in Europe in 2002

Bio
avai
lab
ilit
y (%
)
Tolman et al, J Clin Gastroenterol 1997; 24: 65–70.Fitton & Wiseman, Drugs 1996; 51: 460–82.
Hassan-Alin et al, Gastroenterology 2000; 118: A16.Swan et al., Aliment Pharmacol Ther 1999; 13(Suppl 3): 11–7.
Howden, Clin Pharmacokinet 1991; 20: 38–49.
PPI bioavailability after the first dosePPI bioavailability after the first dose
8090
80
70
60
50
40
30
20
10
0
Lansoprazole Pantoprazole Esomeprazole Rabeprazole Omeprazole
77
64
52
40

LANSOPRAZOLE
CYP2C19
Hydroxy lansoprazole
CYP3A4
Lansoprazole sulphone
Liver Liver enzymes enzymes
unaffectedunaffected
LAN LAN
Tolman et al., J Clin Gastroenterol 1997; 24: 65–70.Welage & Berardi, J Am Pharm Assoc 2000; 40: 52–62.
Lansoprazole metabolism is unaltered with repeated dosingLansoprazole metabolism is
unaltered with repeated dosing
LAN

L = lansoprazole P = pantoprazole O = omeprazole R = rabeprazole
Healing rates for various PPIs in GORD
Healing rates for various PPIs in GORD
Thomson, Curr Gastroenterol Rep 2000; 2: 482–93.
Petite et al. L30/O20
Castell et al. L30/O20
Mee et al. L30/O20
Mulder et al. L30/O40
Mossneret al. P40/O20
Corinaldesi et al. P40/O20
Hotz et al. P40/O20
Vicari et al. P40/O20
Thjodleifsson et al. R20/O20
Dekkers et al. R20/O20
Patients healed at 8 weeks (%)
30 = 30 mg/day, 20 = 20 mg/day, 40 = 40 mg/day
0 20 40 60 80 100

Nissen’s fundoplication for GORDNissen’s fundoplication for GORDNissen’s fundoplication for GORDNissen’s fundoplication for GORD
Acid suppression therapy with PPIs1
Surveillance endoscopy with biopsies
Mucosal ablation (electrocautery, laser or photodynamic therapy) combined with high-dose acid suppression
Oesophageal resection
1. de Caestecker, BMJ 2001; 323: 736–9.
Clinical management of Barrett’s oesophagus
Clinical management of Barrett’s oesophagus

Reflux symptoms are frequent throughout lifeReflux symptoms are frequent throughout life
Incidence of oesophageal adenocarcinoma Incidence of oesophageal adenocarcinoma
is rising:is rising: Associated with increasing incidence of reflux
and decreasing incidence of H. pylori
Heartburn is a risk factor for oesophageal Heartburn is a risk factor for oesophageal adenocarcinoma:adenocarcinoma:
Frequency Duration Severity
Hennessy, Postgrad Med J 1996; 72: 458–63.Malfertheiner & Gerards, Baillière’s Clin Gastroenterol 2000; 14: 731–41.
ConclusionsConclusions

Long-term GORD can result in serious complications, which may prove fatal
Early treatment of GORD is associated with excellent outcomes
Late treatment is associated with an increased risk of complications and potentially poor outcomes
Early intervention relieves symptoms and helps prevent serious complications
Key pointsKey pointsKey pointsKey points

Mallory-Weiss syndromeMallory-Weiss syndromeMallory-Weiss syndromeMallory-Weiss syndrome
Bleeding from rupture of esophageal mucosa

Pill induced esophageal mucosal lesionPill induced esophageal mucosal lesionPill induced esophageal mucosal lesionPill induced esophageal mucosal lesion

Portal hypertension – Esophageal varicesPortal hypertension – Esophageal varicesPortal hypertension – Esophageal varicesPortal hypertension – Esophageal varices

Esophageal varicesEsophageal varicesEsophageal varicesEsophageal varices