diseases of face
TRANSCRIPT
The Face
Prof. Dr.
Mohammed Ali Nasr

Congenital anomalies (Cleft lip-palate).√√√√ Trauma) Maxillo-Facial Fracture). Inflammatory ( Infection --- › Dangerous
area). Tumors (skin tumors).
0

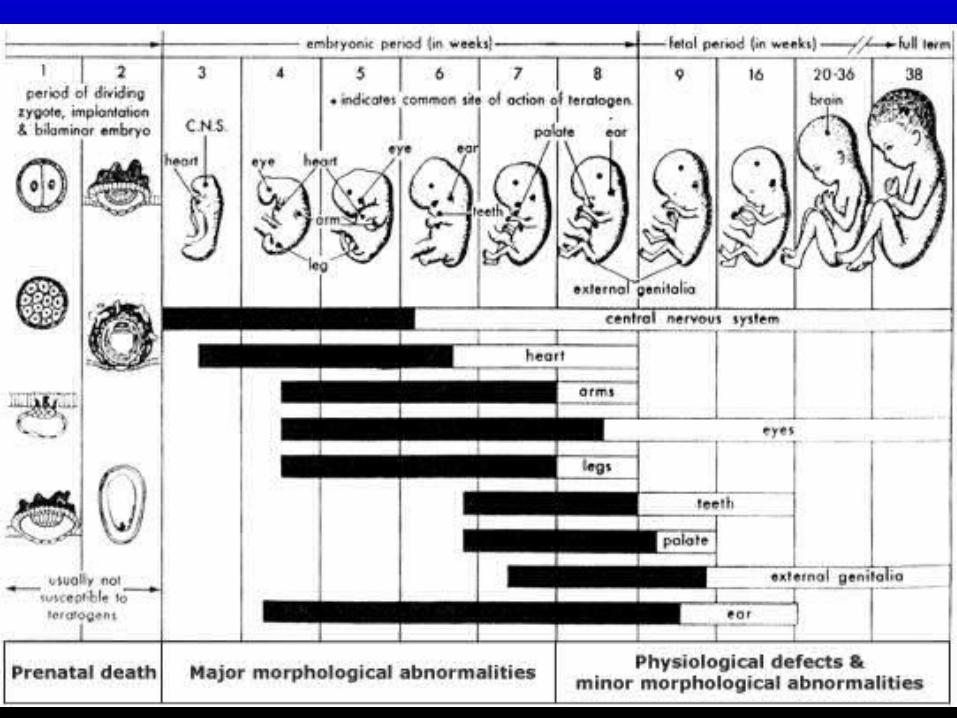
Embryonic Period From fertilization to the end of 8th week of gestation :
-by 6 days age, as implantation of a spherical mass of cells with a central cavity called Blastocyst.
-by 2 weeks: -uteroplacental circulation has begun-2 distinct layers, ectoderm and endoderm
-by 3 weeks: -mesoderm has appeared along with primitive neural
tube and blood vessels.

-4-8 weeks:-lateral folding of the neural plate followed by growth
at the cranial and caudal ends.-budding of arms and legs produces a human like
shape-precursors of skeletal muscles,, vertebrae, along with
the branchial arches that will form the mandible, maxilla, palate, external ear and other head and neck structures start to develop.

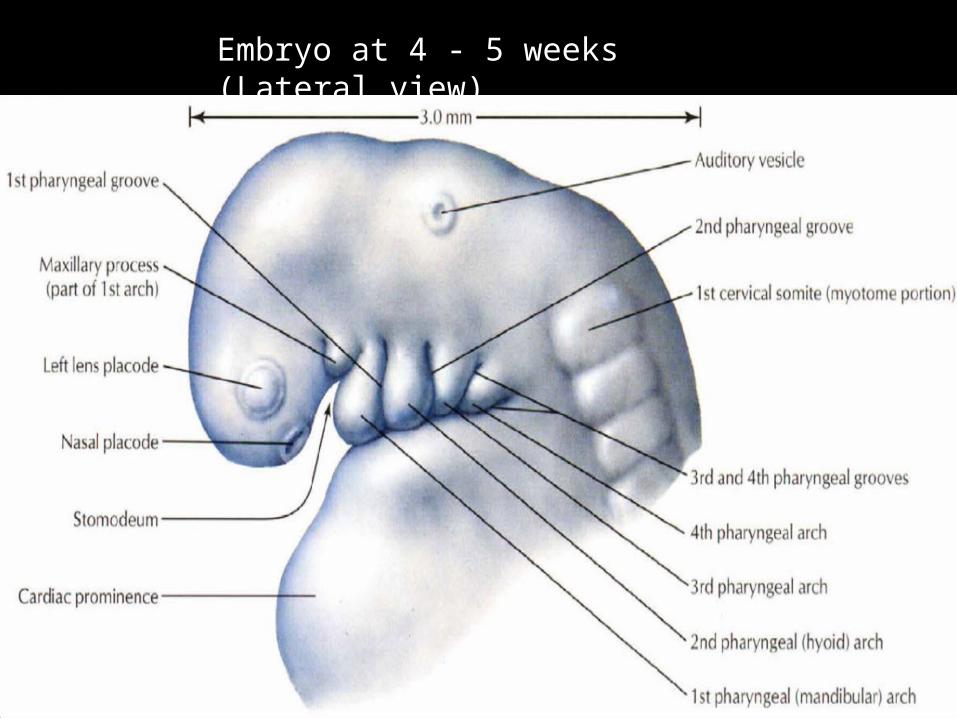
Embryo at 4 - 5 weeks (Lateral view)
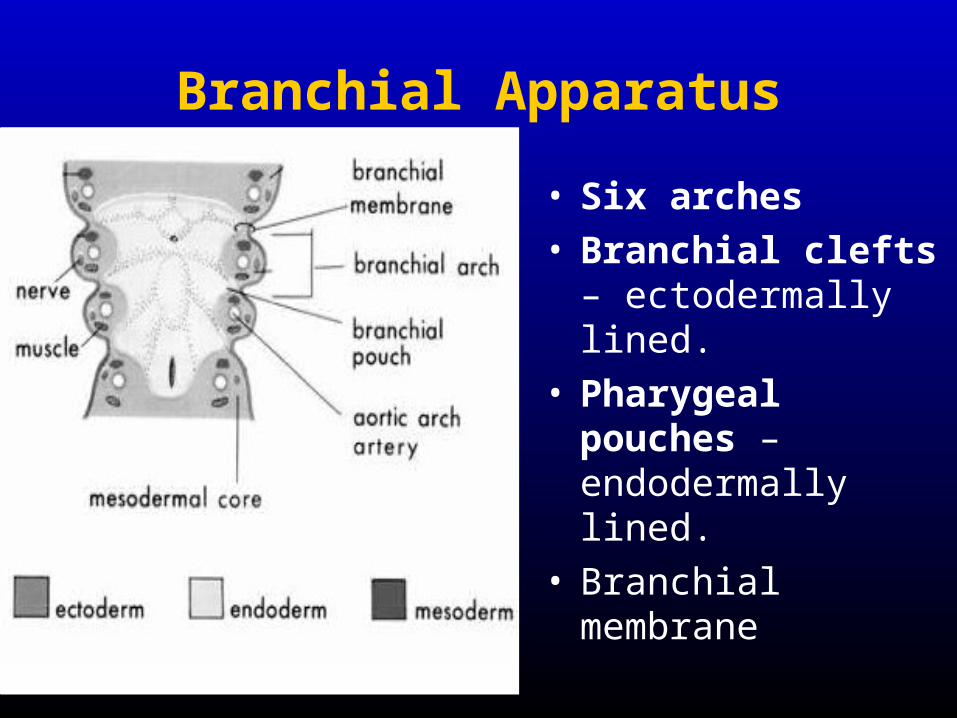
Branchial Apparatus
• Six arches• Branchial clefts –
ectodermally lined.• Pharygeal pouches –
endodermally lined.• Branchial membrane

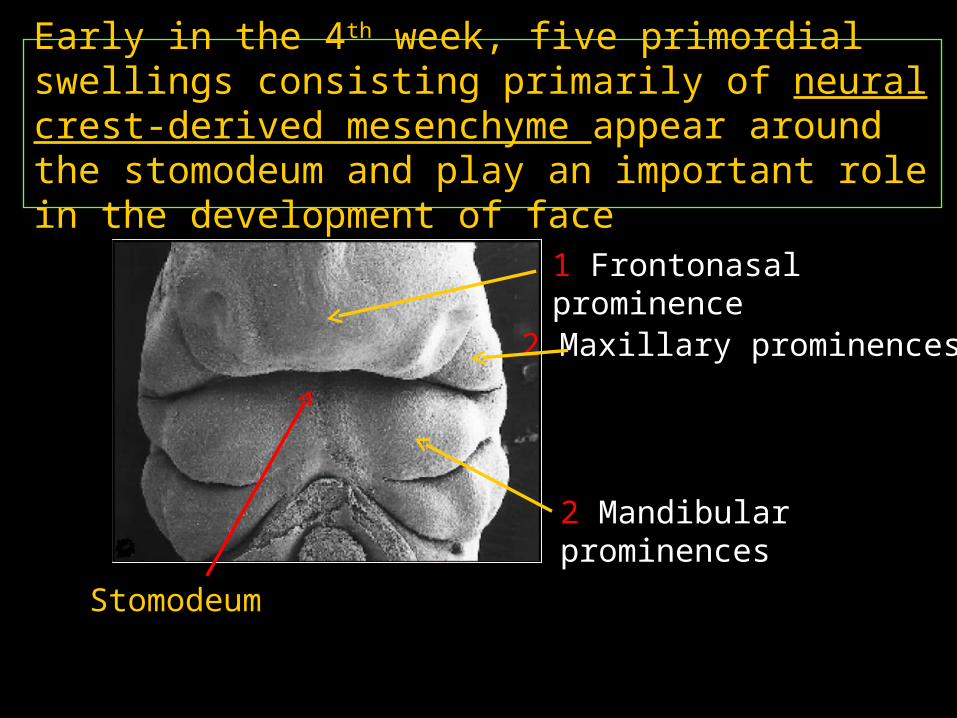
Early in the 4th week, five primordial swellings consisting primarily of neural crest-derived mesenchyme appear around the stomodeum and play an important role in the development of face
Stomodeum
1 Frontonasal prominence2 Maxillary prominences
2 Mandibular prominences
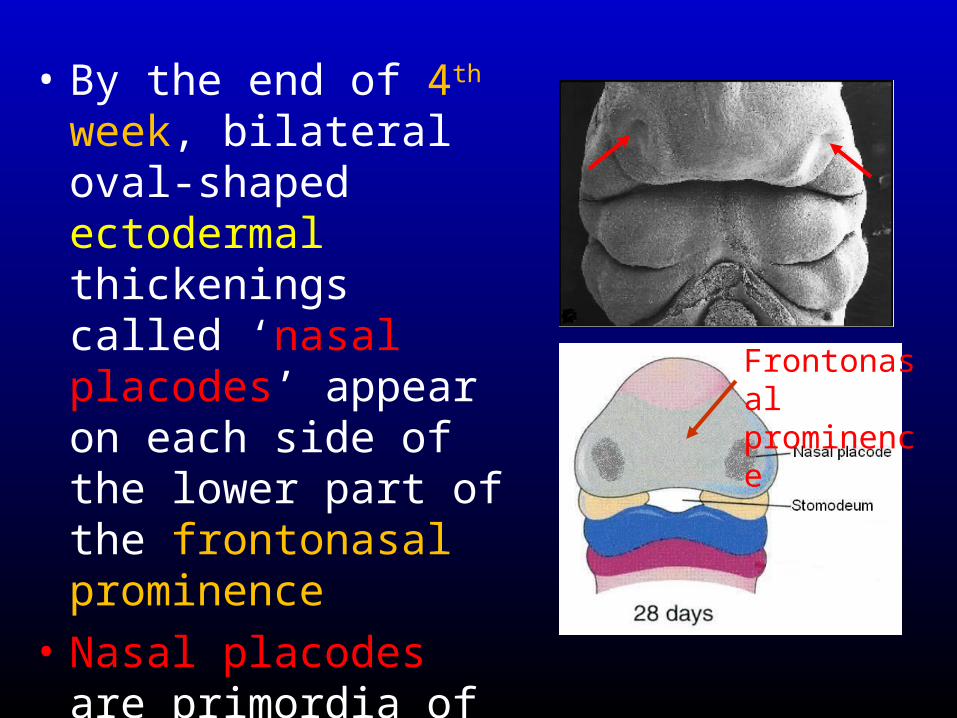
• By the end of 4th week, bilateral oval-shaped ectodermal thickenings called ‘nasal placodes’ appear on each side of the lower part of the frontonasal prominence
• Nasal placodes are primordia of the nose and nasal cavities.
Frontonasal prominence

Mouse embryo: 6 weeks

ANATOMY• Hard Palate
Maxilla( Palatine Processes) +
Palatine Bones(Horizontal Lamina)
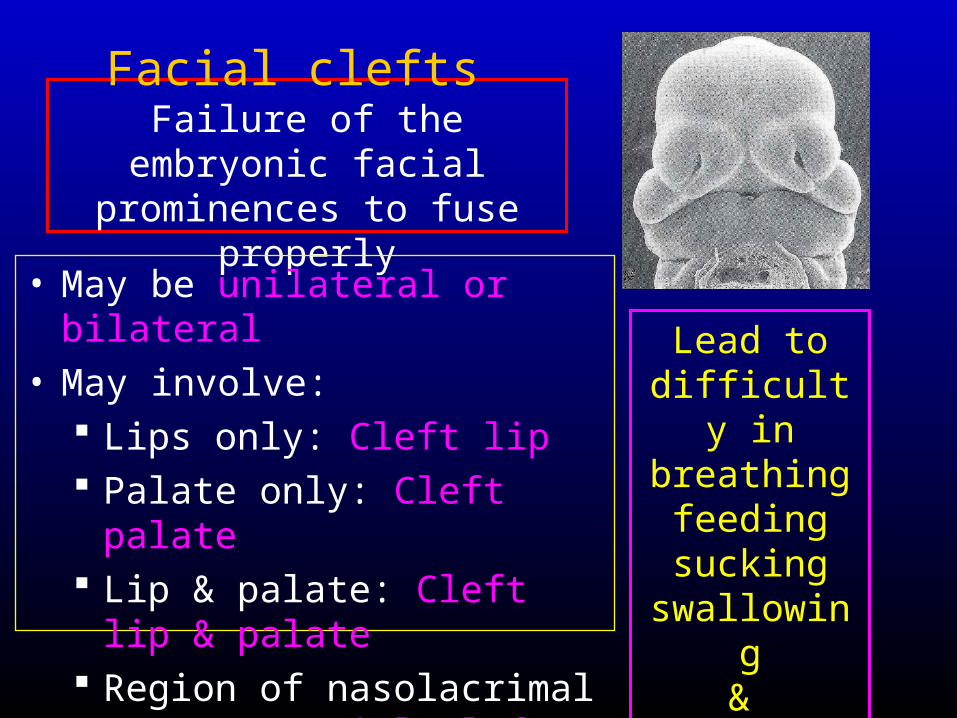
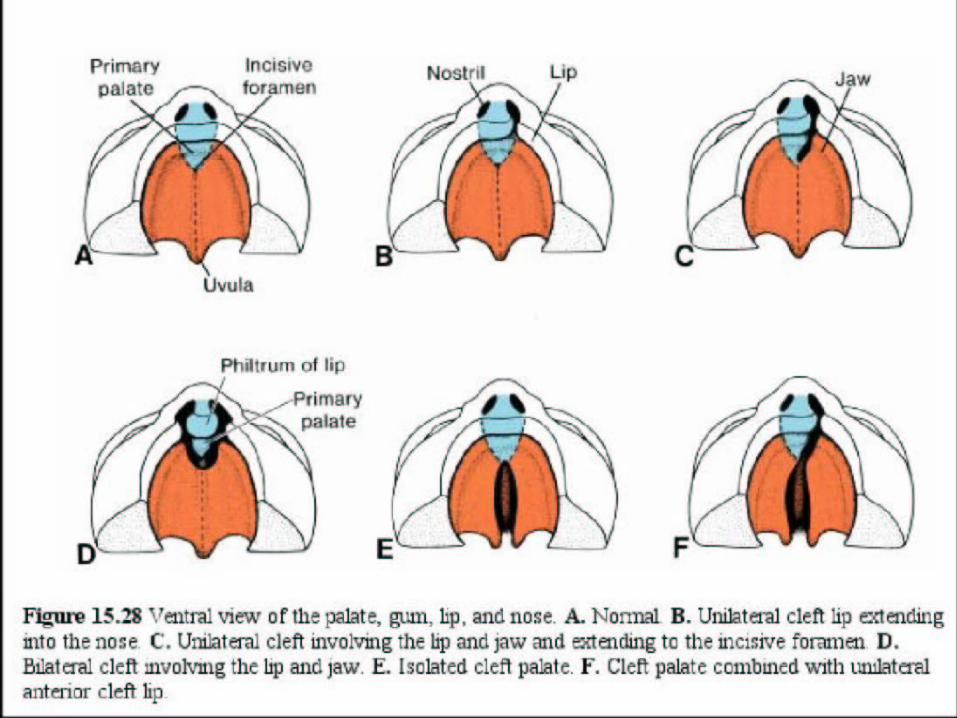
Facial clefts Failure of the embryonic
facial prominences to fuse properly
• May be unilateral or bilateral• May involve:
Lips only: Cleft lip Palate only: Cleft palate Lip & palate: Cleft lip &
palate Region of nasolacrimal
groove: Facial clefts
Lead to difficulty in breathing feeding sucking
swallowing&
speech
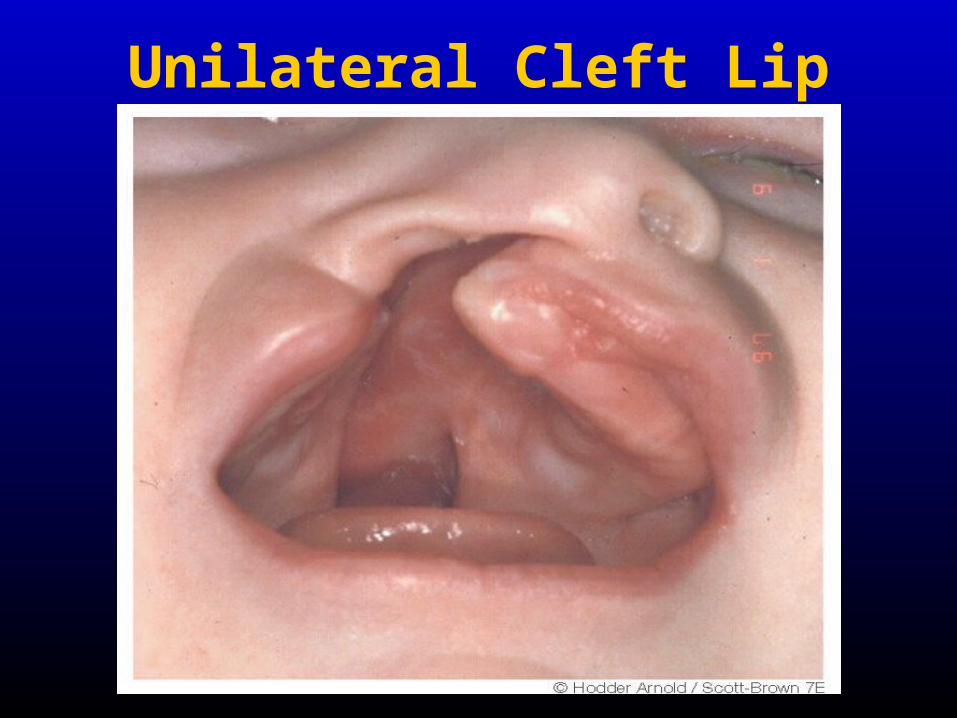
Unilateral Cleft Lip

Bilateral Cleft Lip

• Median cleft lip: results from failure of the medial nasal prominences to merge and form the intermaxillary segments
• Unilateral cleft lip: result from failure of the maxillary prominence to merge with the medial nasal prominence on the affected side
• Bilateral cleft lip: results due to failure of maxillary prominences to meet and unite with the medial nasal prominences on both sides
Median Cleft lip
Unilateral cleft lip
Bilateral cleft lip

2. Oblique facial cleft: results from failure of the maxillary prominence to fuse with the lateral nasal prominence
3. Cleft palate leaves the nasal and oral cavities connected & results in nursing problem for the new born
May be: Anterior/posterior to incisive
foramen Unilateral/bilateral
Cleft lip, cleft jaw & cleft palate
Oblique facial cleft


EtiologyEtiologyGenesGenes
• 2 to 20 genes are thought to interact to result in facial clefting2 to 20 genes are thought to interact to result in facial clefting• Chromosomal abnormalitiesChromosomal abnormalities
• Trisomy 13
• Environmental agentsEnvironmental agents• MedicationsMedications :phenytoin valproate :phenytoin valproate
– With corticosteroids : With corticosteroids : Possible association could not be excludedPossible association could not be excluded..• Cigarette smokingCigarette smoking • AlcoholAlcohol • Folate deficiencyFolate deficiency
• Mechanical Mechanical √√√√• Cleft of lip increases likelihood of cleft of palate because tongue gets
trapped.

INCIDENCE Facial clefting is one of most common congenital
deformity (1:750 live births). 1:Clefts lip only (Pre-alveolar) 25%, more in male,
unilateral in75% ,bilateral in25% rarely median2:Clefts palate only (Post-alveolar) 25%, more in
females (Fusion precedes from before backward)3:Cleft lip and palate (Alveolar) 50% uni/bi
Problems are cosmetic, dental, speech, swallowing, hearing, facial growth, emotional

Unilateral incomplete
Unilateral complete
Bilateral complete
Incomplete cleft palate
Unilateral complete lip and palate
Bilateral complete

Prenatal DiagnosisPrenatal Diagnosis
Obstetrical Obstetrical ManagementManagement
• As of January 2002, "in utero" correction As of January 2002, "in utero" correction had been attempted only once in Mexico had been attempted only once in Mexico – The child delivered prematurely and died at two The child delivered prematurely and died at two
months of life months of life

MANAGEMENT
• Team Approach• Surgical Repair• Speech Disorders• Orthodontics

ManagementManagement• The Care will entail attention, not only to The Care will entail attention, not only to
surgical repair, but also more immediate surgical repair, but also more immediate needs such as feeding. needs such as feeding.
• Primary lip repairs can often be undertaken Primary lip repairs can often be undertaken at three months of age with palatal repairs at three months of age with palatal repairs around six months till 1.5year.around six months till 1.5year.
• Additional surgeries as well as speech and Additional surgeries as well as speech and orthodontic therapies are often needed. orthodontic therapies are often needed.
Surgical Techniques
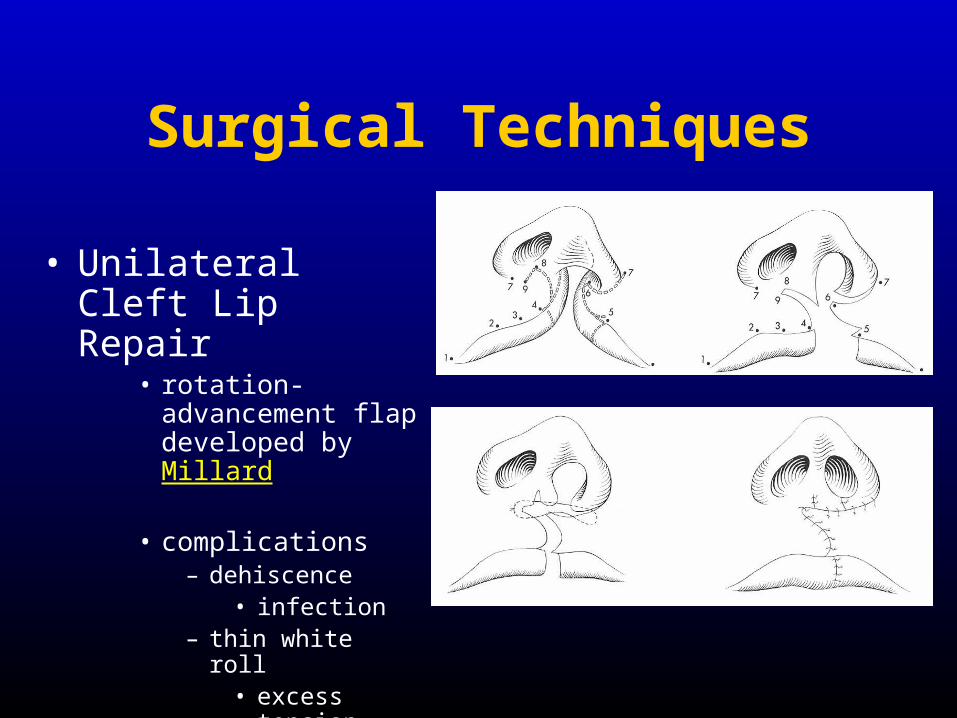
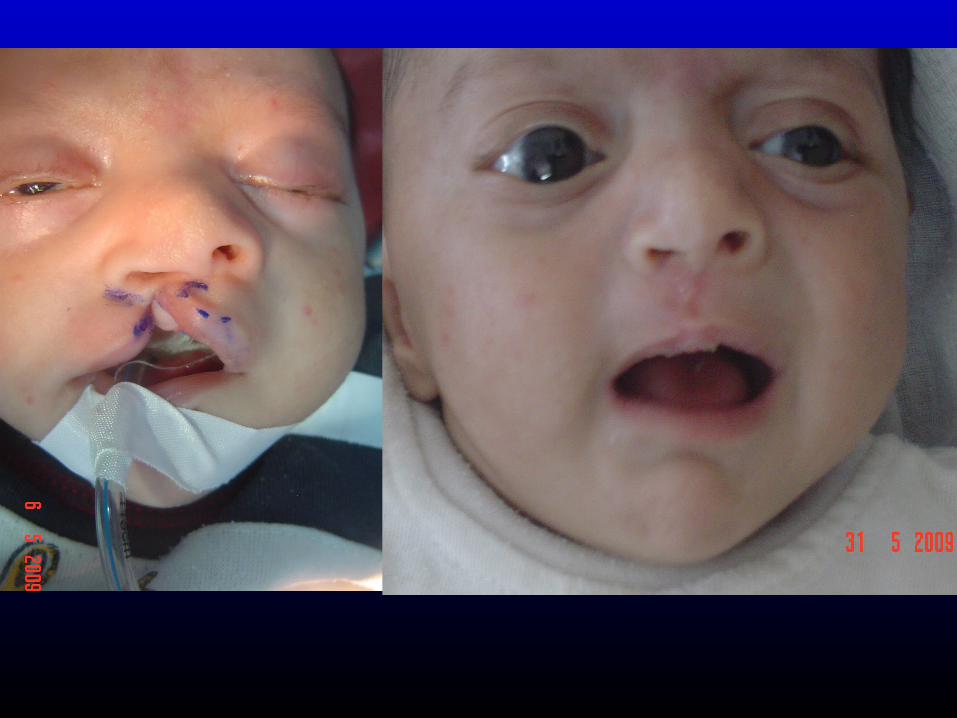
• Unilateral Cleft Lip Repair
• rotation-advancement flap developed by Millard
• complications– dehiscence
• infection– thin white roll
• excess tension
Surgical Techniques
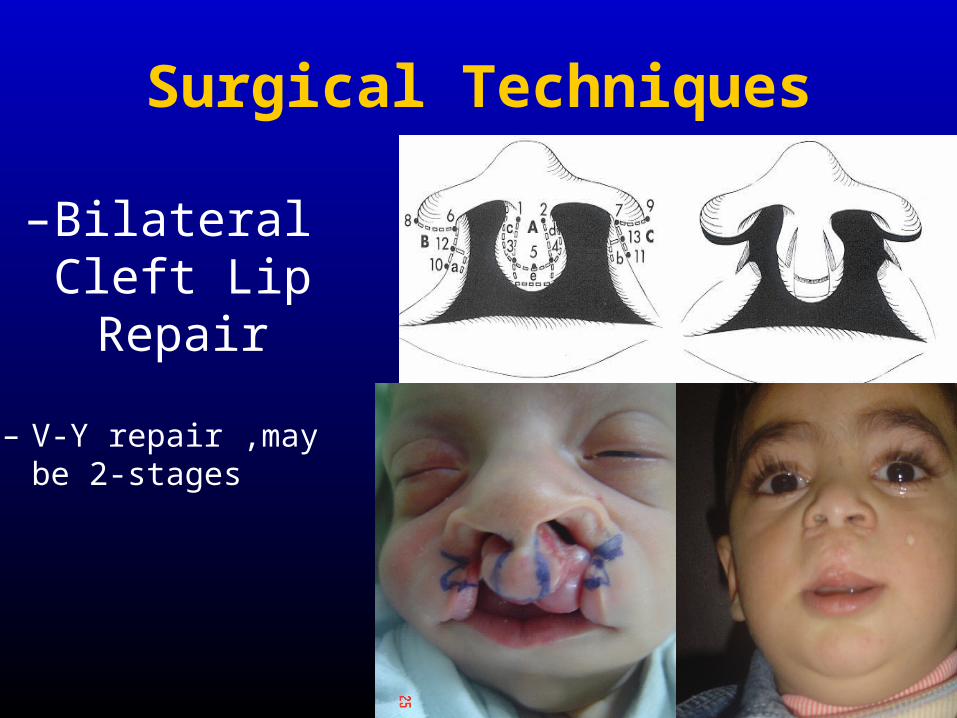
–Bilateral Cleft Lip Repair
– V-Y repair ,may be 2-stages

Surgical Repair- Cleft Palate
• Scarring of palate may cause impaired mid-facial growth (alveolar arch collapse, midface retraction, malocclusion)
• Facial growth may be less affected if surgery is delayed until 18-24 months, but feeding, speech, socialization may suffer.

Waldill (push-back)
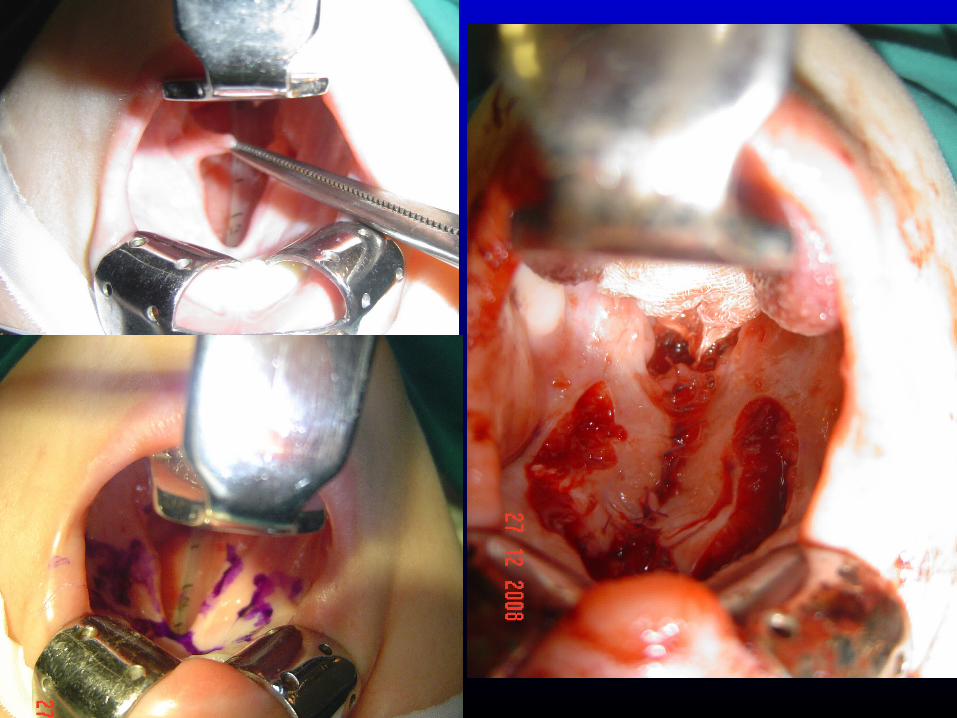
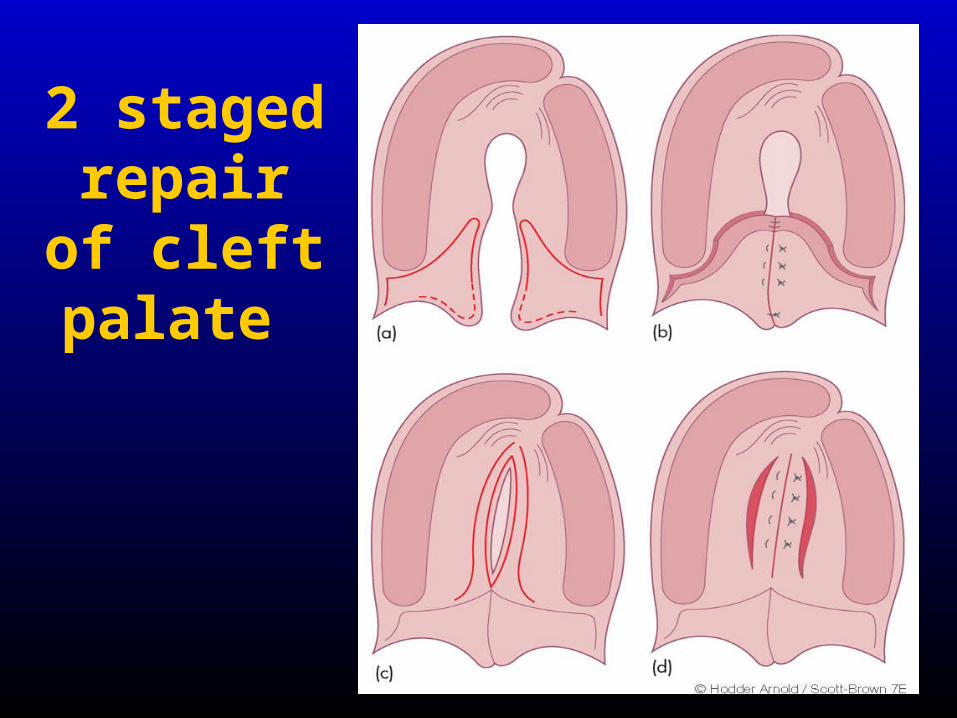
2 staged repair of
cleft palate

• THANK YOU