disability head injury: the use glasgow scale286 with their eyes, showreflex responses in their...
TRANSCRIPT

Journal of Neurology, Neurosurgery, and Psychiatry, 1981, 44, 285-293
Disability after severe head injury: observationson the use of the Glasgow Outcome ScaleB JENNETT, J SNOEK*, M R BOND, AND N BROOKS
From the Departments ofNeurosurgery and Psychological Medicine, University of Glasgow, and theInstitute ofNeurological Sciences, Glasgow
SUMMARY The nature of the neurological and mental disabilities resulting from severe head injuriesare analysed in 150 patients. Mental handicap contributed more significantly to overall social dis-ability than did neurological deficits. This social handicap is readily described by the Glasgow Out-come Scale, an extended version of which is described and compared with alternatives. Commentsare made about the quality oflife in disabled survivors.
Some of the patients who now survive severe headinjury due to intensive therapy in the acute stage makea satisfactory recovery. Others are left with sequelaewhich range from the inconvenient to those whichrender the patient totally dependent. Many of thesesurvivors are young and they face many years ofdisability, which commonly affects both mental andphysical function. Although the separate componentsof handicap after brain damage have frequently beendescribed, particularly those which can be measuredby psychometric tests, what matters to the patient isthe net effect of all his separate disabilities on hisfunctioning as a person, which includes the extent ofhis dependency on others. This may be termed theoverall social outcome, and it is often described inpoorly defined terms such as: "good," "fair,""6poor,..".acceptable,"' "practical," "worthwhile,"'or "tolerable"-the last two involving value judge-ments about the quality of life.Some years ago we devised a simple scale for
describing overall social outcome,1 mainly in orderto facilitate two multicentre studies on outcomefrom coma due to structural brain damage. One ofthese dealt with severe head injury,2 the other withcoma due to non-traumatic conditions;3 the purposeof both was to evolve a system of predicting outcomesix months after the ictus. The need was for a limitedset of outcomes which had to be sufficiently clearlydefined to be used reliably by observers in severalcentres, some of whom were in different countries.
*Visiting neurologist from the Department of Neurology, AcademischZiekenhuis Groningen, Oostersingel 59, Groningen, Netherlands.Address for reprint requests: Professor B Jennett, Institute ofNeurological Sciences, Glasgow G5 1 4TF, Scotland.Accepted 20 November 1980
Subsequently, a leading American neurosurgeonsuggested that the Glasgow Outcome Scale should beadopted world-wide for reporting series of severelyhead injured patients, at least for a period of fiveyears, in order to facilitate comparison betweendifferent studies.4 In the event most recent publica-tions reporting recovery after head injury from NorthAmerica and Europe have used this scale, and themulticentre studies of severe head injury and ofruptured aneurysm recently initiated in the USA bythe NINCDS require participants to classify sur-vivors on the Glasgow scale.
It is timely therefore to review the practicalapplication of the scale, to compare it with alternativesystems of assessing outcome, and to describe thecomponents of physical and mental disability inpatients who reach the various points on the scale.This paper discusses these matters by reference to aseries of severely head injured patients who wereprospectively studied during their recovery. It alsoproposes sub-division of the original scale to allowmore sensitive measures of recovery in patients whoregain consciousness.
THE ORIGINAL GLASGOW OUTCOME SCALEThe scale proposed four outcome categories forsurviving patients as follows:(a) Vegetative state: This was defined by Jennett andPlum5 in rigorous terms which limited it to patientswho showed no evidence of meaningful responsive-ness. Patients who obey even simple commands, orwho utter any words, are assigned to the bettercategory of severe disability. Vegetative patientsbreathe spontaneously, have periods of spontaneouseye-opening when they may follow moving objects
285
Protected by copyright.
on March 17, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.4.285 on 1 April 1981. D
ownloaded from

286
with their eyes, show reflex responses in their limbs(to postural or painful stimuli), and they mayswallow food placed in their mouths. This non-sentient state must be distinguished from otherconditions of wakeful, reduced responsiveness-such as the locked-in syndrome, akinetic mutismand total global aphasia. Although the vegetativestate indicates lack of function in the cerebral cortex,this may be structurally intact; for this reason Jennettand Plum argued that the term "apallic syndrome"was inappropriate.(b) Severe disability: This indicates that a patient isconscious but needs the assistance of another personfor some activities of daily living every day. This mayrange from continuous total dependency (for feedingand washing) to the need for assistance with onlyone activity-such as dressing, getting out of bed ormoving about the house, or going outside to a shop.More often dependency is due to a combination ofphysical and mental disability-because whenphysical disability is severe after head injury there isalmost always considerable mental deficit. But a fewpatients who have little or no physical deficit areunable to organise their day-to-day lives effectively,and must be classified as severely disabled. The worstof these requires the care and protection which onlya mental hospital can provide, while others cope athome with the support of attentive relatives, but couldnot be left overnight because they would be unableto plan their meals or to deal with callers, or anydomestic crisis which might arise. The severelydisabled are described by the phrase "conscious butdependent."(c) Moderate disability: These patients may besummarised as "independent but disabled," but it isperhaps the least easily described categery of sur-vivor. Such a patient is able to look after himself athome, to get out and about to the shops and to travelby public transport. However, some previousactivities, either at work or in social life, are now nolonger possible by reason of either physical or mentaldeficit. Some patients in this category are able toreturn to certain kinds of work, even to their own job,if this happens not to involve a high level of per-formance in the area of their major deficit.(d) Good recovery: This indicates the capacity toresume normal occupational and social activities,although there may be minor physical or mentaldeficits. However, for various reasons, the patientmay not have resumed all his previous activities, andin particular may not be working.
Patients and methods
Characteristics of the patientsA data bank of over 1000 severely head injured patientsfrom three countries has been accumulated prospectively
B Jennett, J Snoek, M R Bond, and N Brooks
in Glasgow over the last ten years. The minimum severityof injury was a period of coma of at least six hours (comais defined as not opening the eyes, not obeying commands,not uttering understandable words). Post-traumaticamnesia (PTA) in survivors was at least two days, andin 94% exceeded a week. Many initial features of thepatients in each of the three countries were similar, aswere the mortality rates (about 50%) and the distributionof outcomes on the Glasgow scale six months after injury(2:6).For a more detailed analysis of disability a series of 150
conscious adult survivors in Glasgow were called to aspecial clinic for the purpose of this study, at least oneyear after injury (range 1-14 years, mean 5-2, SD 2 6),where they were assessed by a neurologist (JS). Thesepatients had a similar distribution of outcome categoriessix months after injury as the remaining Glasgow cases,and as the cases from other centres (table 1). Their meanage was 28 years, 44% being under 20 years and 5% over60 years; males predominated (5:1). PTA was over 28days in 61 %, 15-28 days in 9% and 2-14 days in 30%. Anacute intracranial haematoma had been evacuated in 52%of these patients.
Table I Conscious survivors 6 months after injury
Other A 11 Glasgow,data bank Glasgow detailedcentres cases follow-up191 314 150
Severe disability 21% 19% 20%Moderate disability 35 % 34% 40%Good recovery 44% 47% 40%
Results
1 RELIABILITY OF THE SCALEThe outcome category at six months and at twelvemonths was assigned by JS for the 150 patientswhom he saw in the clinic. These assessments werecompared with those already made by BJ, as part ofthe ongoing data bank study. For both times therewas agreement between these two observers in morethan 95% of patients; each observer scored a fewpatients higher and a few lower than the other.
2 HOW MANY CATEGORIES?Several sizeable reports in recent years have recog-nised only two categories of survivor after severehead injury,7"-1 and one made no distinction betweenthe disabled and the recovered.'2 The categories inthese classifications are seldom clearly defined buttheir probable equivalence to the practical scaleunder discussion is set out in table 2. Consideringthe range of disability which occurs, it does seemimportant to recognise at least the difference betweendisabled patients who are dependent and those whoare not. Even the three-category Glasgow scale isconsidered by some to be over-compressed, and
Protected by copyright.
on March 17, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.4.285 on 1 April 1981. D
ownloaded from

Table 2 Classification ofdisability ofhead injury survivors who became conscious.
Jennett and Bond Carlsson Pazzaglia et al Heiskanen and Vigoroux et al Overgaard et al Vapalhati and Troupp(1975) (1968) (1975) Sipponen (1979) (1973) (1971)
(1970)
Severe disability Persisting Partially Permanent Serious SevereDementia Re-integrated invalid sequelae deficit
Moderate disabilityRecovery
Good Mental Recovered Recovery Nil/slight Goodrecovery restitution sequelae recovery
40 therefore to be insensitive to degrees of improvement1nyear (122 patients)
which occur within one of its categories. For this301 reason we divided each of the 150 conscious sur-
vivors in this study into a better and worse level0/0 20- _ within each of the original categories to which they
had been assigned. The proportional distribution
10 along the six-point scale for conscious survivors at_IIIL six and twelve months after injury showed only small
0 r J numbers of patients at the extreme ends of this scaleo 1 2 3 4 5 (figure). Including dead and vegetative this makes
40 eight outcome categories. For some purposes,6months (150 patients) however, it may be more appropriate to contract the
30t original five point scale to two or three outcomes(table 3); for example, for statistical calculations of
/* 20 ] probable outcome at six months-on the basis of datacollected in the first week after injury.
10 A number of outcome scales have been published_III-~ with more categories than the original Glasgow
0 [ _ ] _ J scale15-'9 but none of these scales has its categories0 1 2 3 4 5 as evenly spread across the range of disability as theGood Moderate Severe extended Glasgow scale (table 4). More than half of
Figure Distribution ofdisability ofconscious survivors the aggregate of categories from five publishedon the 6-point Glasgow scale (from Management of scales refer to patients whom we would classify asHead Injuries-Jennett B and Teasdale G. F A Davis: severely disabled and who make up less than a fifth ofPhiladelphia 1981). survivors six months after severe head injury.
Table 3 Outcome after severe brain damage (variations on Glasgow Scale)
Dead Dead/ Vegetative Deadl Vegetative Dead Dead Dead
Dependent Vegetative Vegetative
Severely Disability:Disabled Severely
Disabled 4
Survivors Conscious
Moderately 3Disabled 2
Independent IndependentGood
I
Recovery O
No.ofcategories 2 3 5 8
Disability after severe head injury 287
Protected by copyright.
on March 17, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.4.285 on 1 April 1981. D
ownloaded from
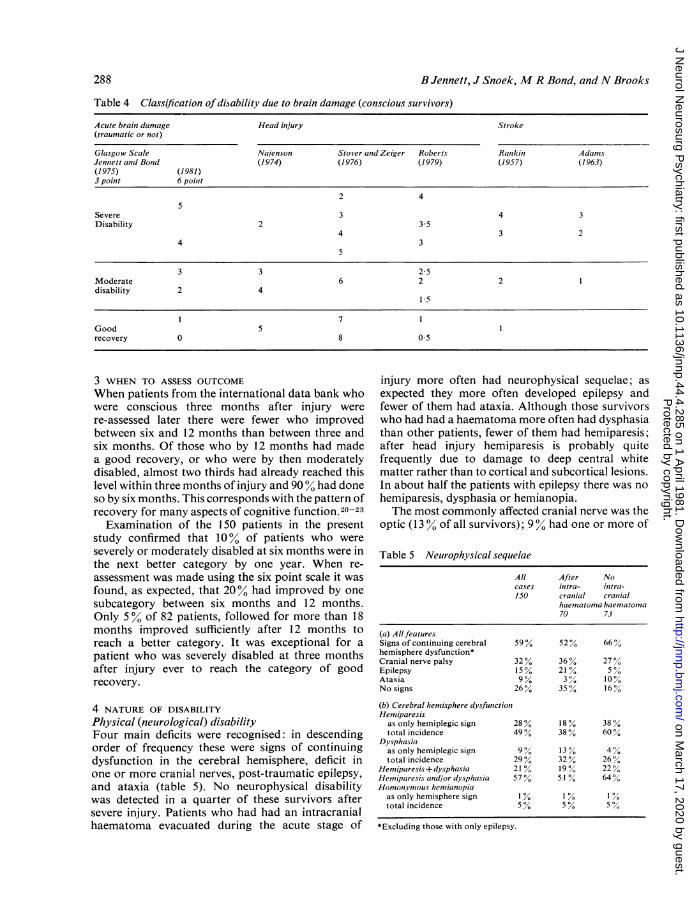
Table 4 Classification ofdisability due to brain damage (conscious survivors)
Acute brain damage Head injury Stroke(traumatic or not)
Glasgow Scale Najenson Stover and Zeiger Roberts Ratikin AdamsJennett and Bond (1974) (1976) (1979) (1957) (1963)(1975) (1981)3 point 6 poinit
2 45
Severe 3 4 3Disability 2 3 5
4 3 24 3
5
3 3 25Moderate 6 2 2 1disability 2 4
15
1 7 1Good 5 1recovery 0 8 0 5
3 WHEN TO ASSESS OUTCOME
When patients from the international data bank whowere conscious three months after injury were
re-assessed later there were fewer who improvedbetween six and 12 months than between three andsix months. Of those who by 12 months had madea good recovery, or who were by then moderatelydisabled, almost two thirds had already reached thislevel within three months of injury and 90% had doneso by six months. This corresponds with the pattern ofrecovery for many aspects of cognitive function.20-23Examination of the 150 patients in the present
study confirmed that 10% of patients who were
severely or moderately disabled at six months were inthe next better category by one year. When re-
assessment was made using the six point scale it wasfound, as expected, that 20% had improved by one
subcategory between six months and 12 months.Only 5% of 82 patients, followed for more than 18months improved sufficiently after 12 months toreach a better category. It was exceptional for a
patient who was severely disabled at three monthsafter injury ever to reach the category of goodrecovery.
4 NATURE OF DISABILITY
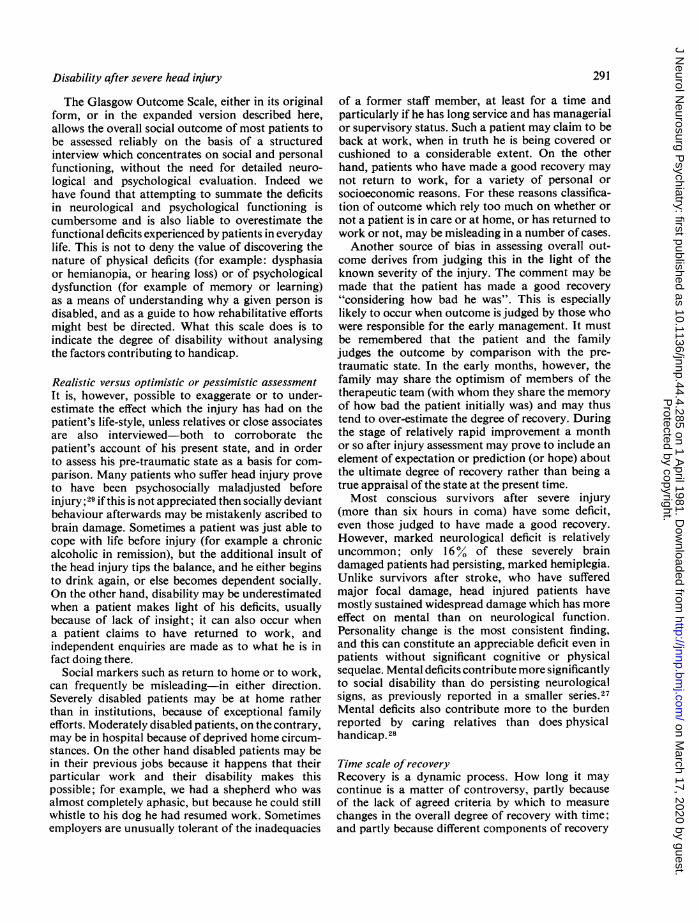
Physical (neutrological) disabilityFour main deficits were recognised: in descendingorder of frequency these were signs of continuingdysfunction in the cerebral hemisphere, deficit inone or more cranial nerves, post-traumatic epilepsy,and ataxia (table 5). No neurophysical disabilitywas detected in a quarter of these survivors aftersevere injury. Patients who had had an intracranialhaematoma evacuated during the acute stage of
injury more often had neurophysical sequelae; asexpected they more often developed epilepsy andfewer of them had ataxia. Although those survivorswho had had a haematoma more often had dysphasiathan other patients, fewer of them had hemiparesis;after head injury hemiparesis is probably quitefrequently due to damage to deep central whitematter rather than to cortical and subcortical lesions.In about half the patients with epilepsy there was nohemiparesis, dysphasia or hemianopia.The most commonly affected cranial nerve was the
optic (13 % of all survivors); 9% had one or more of
Table 5 Neurophysical sequelae
All After Nocases intra- initra-150 cranial craniial
haematoma haematoma70 73
(a) AllfeaturesSigns of continuing cerebral 597% 52% 66%hemisphere dysfunction*Cranial nerve palsy 32 % 36 % 27%Epilepsy 15% 21% 5 %Ataxia 9 % 3 , 10%No signs 26% 35 % 16%
(b) Cerebral hemisphere dvsfunctionHemiparesis
as only hemiplegic sign 28 % 18 % 38 %total incidence 49% 38 % 60%
Dysphasiaas only hemiplegic sign 9 % 13 % 4%total incidence 29% 32% 26%
Hemiparesis+ dysphasia 21% 19% 22%Hemiparesis and/or dysphasia 57 % 51% 64%Homonymous hemianopia
as only hemisphere sign % I% 1 /total incidence 5 % 5 % 5 %
*Excluding those with only epilepsy.
288 B Jennett, J Snoek, M R Bond, andN Brooks
Protected by copyright.
on March 17, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.4.285 on 1 April 1981. D
ownloaded from

Disability after severe head injury
Table 6 Frequency ofphysical sequelae in each outcomecategory
Good Moderate Severerecovery disability disability60 60 30
f Mild 25% 40% 37%Hemiparesis ) Severe 0 20% 40%
f Mild 10% 32% 17%Dysphasia Q Severe 0 12% 30%o
Both Hemiparesis f Either severe 0 27 % 60%and Dysphasia Both severe 0 2% 17%
Cranial nerveMild 20% 32% 23 %Cranialnerve Severe 0 15%Y 30%Y
Only CN (± epilepsy) 20% 15% 7%Epilepsy 17% 10% 30%Ataxia 2% 13% 17%
the nerves to ocular muscles affected and 80% hadsensorineural deafness. Anosmia was noted in only5%- possibly an underestimate because assessmentin severely damaged patients can be difficult. Dys-arthria was present in 4% and facial weakness in 2 %.Deficits in patients judged to have made a goodrecovery most often consisted of mild hemiparesis,cranial nerve palsies, or epilepsy (table 6). Theseverely disabled had a higher incidence of severehemiparesis or severe dysphasia, one or other ofwhich affected a third of these patients; half of thesepatients were both severely paralysed and severelydysphasic. Epilepsy was also more frequent in theseverely disabled.
Psychological and social disabilityThe nature and time course of the cognitive deficitsand disorders of personality found in severely braindamaged patients (as defined here) has been describedin several previous reports from this Institute.20-26In the present series the neurologist made a clinicalassessment of the degree of personality change fromquestioning of the patient and a close relative.Formal tests of cognitive function were carried outindependently on as many patients as possible bya psychologist who did not know the neurologist'srating of outcome category for the patient. The testbattery comprised verbal and non-verbal learningand memory, verbal and performance intelligence,and measures of perceptual/constructional function.In these severely injured patients it was oftenimpractical to carry out full cognitive testing; forthis reason the totals vary for different tests inthe tables.The overall severity of the cognitive deficit was
graded (in 3 categories) by the neurologist, who hadaccess later to the psychologist's reports, and therelationship to the outcome category was explored
289
(table 7). None of the nine patients with severecognitive deficit was judged to have made a good re-covery, and only two were in the moderate disabilitycategory. Of the 45 patients with good cognitiverecovery, none had an outcome category of severedisability, while of the seven patients with a moderatecognitive disability, four were in the outcomecategory of moderate disability. The picture forpersonality change was very similar, with no patientswith moderate or severe personality change beingplaced in the good recovery category, and only 13%of those with a mild degree of personality changebeing severely disabled.
Table 7 Frequency ofdeficits in each outcome category
Good Moderate Severerecovery disability disability29 23 9
fMild 29 23 6Physical (as a whole) {Severe 0 0 2
f Mild 12 15 1Personality ) Severe 0 3 7
Cognitive f Mild 29 21 2(as a whole) Severe 0 2 7
VerbalIQfMild 3 9 2
Verbal IQ (Severe 0 0 4
Performance IQ Mild 13 13 8Seee 0 1 8
C Mild 1 1 12 1Verbal memory gjsSevere 1 5 8
f Mild 16 11 2Non-verbal memory :Severe 0 5 7
Combination ofmental andphysical deficitsSome deficit was detected, albeit sometimes mild, in970% of these 150 patients. Two thirds had person-ality change which in almost 30%, was the onlydeficit. It was found to a marked degree in over60% of patients whose physical deficit was nil ormild, and in the same proportion of those with nilor minimal cognitive deficit. By contrast, mostpatients with marked cognitive or physical deficitsalso had definite deficits in either of the other twocomponents of disability.The relative severity of physical, cognitive and
personality disorder in patients in each outcomecategory was assessed for the 61 patients who hadcompleted the full psychological test battery (table 7).The table shows the number of cases judged by thepsychologist to have deficits in each cognitive area.Disorders of verbal intellect were found to be rela-tively infrequent, while disorders of learning andmemory, and of performance intelligence were foundto be severe and persistent; these findings are in
Protected by copyright.
on March 17, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.4.285 on 1 April 1981. D
ownloaded from

290
accord with several psychological studies of severehead injury. 20-26Although some neurophysical deficit (including
epilepsy) occurred in three-quarters of the patients,mental handicap was judged by the examiningneurologist to be more significant than physicalsequelae in contributing to the overall disability inover half the cases; physical features were moresignificant in less than 30% (table 8). This dominance
Table 8 Contribution ofmental andphysicalfeatures tooverall disability in each outcome category
Balance ofdisability Good Moderate Severerecovery disability disability Total55 60 30 145
Mental worse 56% 48% 63% 54%Physical worse 27% 30% 23 % 28%Equal 17% 22% 13 % 18%
Mental > physical 73% 70% 76% 72%
of mental sequelae, which was similar in each of thethree categories of outcome, confirms an earlyobservation on the interaction between componentsof the disability after head injury.27 A more detailedstudy of psychosocial disability has shown that whenrelatives were questioned about the frequency of awide variety of deficits, physical deficits were felt tobe infrequent during the first year after injury.28However, emotional personality and memory dis-ability were all rated as frequent, and disorders ofemotional control and affect were still very common12 months after injury.
Relationship ofPTA to disabilityAlmost all the patients with severe disability hadmore than four weeks ofPTA; but so did the majorityof those with moderate disability and more than athird ofthose who had made a good recovery (table 9).Less than a third ofpatients with more than a month'sPTA were left severely disabled, whilst over 80%with less than two weeks PTA made a good recovery(table 9b). This relationship between PTA and out-come also holds for the six point scale, although thenumbers in some categories are small (table 10). Itfollows from this that if a patient has emerged fromPTA in less than four weeks he is almost certain tobecome independent, although he may be leftmoderately disabled.
Discussion
Classifying the outcome after severe head injurycommands much less attention than does character-terisation of the initial damage and early complica-tions. Yet there is a need for a simple, reliable means
B Jennett, J Snoek, M R Bond, andN Brooks
Table 9 PTA and outcome (486 data bank cases on3 point scale)
(a) PTA duration for each outcome categoryGood Moderate Severe
PTA n 226 170 90
<7days 12% 2%8-14 days 25% 8 %15-28 days 28% 18% 3%>28 days 35% 72% 97%
(b) Outcome categoriesfor different PTA durations< 7 days 8-14 days 15-28 days >28 days
n 30 71 96 289
Good 90% 80% 66% 27%Moderate 10% 20% 31% 43%Severe 0 0 3% 30%
Table 10 PTA and outcome (148 Glavgow cases on6 point scale)
(a) PTA duration for each outcome categoryGood Moderate Sever-e
0 1 2 3 4 5n 5 54 34 24 21 9
<7 days 2 9 1 0 0 08-14 days 1 21 7 2 0 015-28 days 0 9 6 2 0 0>28 days 7 15 20 20 21 9
(b) Outcome categories for different PTA durations< 7 days 7-14 days 15-28 days >28 days
n 12 31 17 88
0 3 1 0 2Good 1 9 21 9 15
2 0 7 6 21Moderate 3 0 2 2 20
Severe 4 0 0 0 21Seee 5 6 0 6 9
of describing the degree of recovery. Assessing therelative efficacy of alternative therapeutic measuresdepends on valid comparison of the outcomes inpatients differently treated. Prediction of outcome,on which both management decisions and advice tothe patient and his family depend, requires therelationship between early features and ultimateoutcome to be established; that is possible only ifwell-defined outcome categories are recognised. Inthe later stages of recovery the rate of improvementin individual patients may be important in assessingthe need for, and the effectiveness of, rehabilitation;this calls for a scale by which to measure change.When disability is prolonged or permanent, appropri-ate arrangements for continuing care demand thatthe degree and nature of the disability be readilycategorised.
Protected by copyright.
on March 17, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.4.285 on 1 April 1981. D
ownloaded from
Disability after severe head injury
The Glasgow Outcome Scale, either in its originalform, or in the expanded version described here,allows the overall social outcome of most patients tobe assessed reliably on the basis of a structuredinterview which concentrates on social and personalfunctioning, without the need for detailed neuro-logical and psychological evaluation. Indeed wehave found that attempting to summate the deficitsin neurological and psychological functioning iscumbersome and is also liable to overestimate thefunctional deficits experienced by patients in everydaylife. This is not to deny the value of discovering thenature of physical deficits (for example: dysphasiaor hemianopia, or hearing loss) or of psychologicaldysfunction (for example of memory or learning)as a means of understanding why a given person isdisabled, and as a guide to how rehabilitative effortsmight best be directed. What this scale does is toindicate the degree of disability without analysingthe factors contributing to handicap.
Realistic versus optimistic or pessimistic assessmentIt is, however, possible to exaggerate or to under-estimate the effect which the injury has had on thepatient's life-style, unless relatives or close associatesare also interviewed-both to corroborate thepatient's account of his present state, and in orderto assess his pre-traumatic state as a basis for com-parison. Many patients who suffer head injury proveto have been psychosocially maladjusted beforeinjury ;29 if this is not appreciated then socially deviantbehaviour afterwards may be mistakenly ascribed tobrain damage. Sometimes a patient was just able tocope with life before injury (for example a chronicalcoholic in remission), but the additional insult ofthe head injury tips the balance, and he either beginsto drink again, or else becomes dependent socially.On the other hand, disability may be underestimatedwhen a patient makes light of his deficits, usuallybecause of lack of insight; it can also occur whena patient claims to have returned to work, andindependent enquiries are made as to what he is infact doing there.
Social markers such as return to home or to work,can frequently be misleading-in either direction.Severely disabled patients may be at home ratherthan in institutions, because of exceptional familyefforts. Moderately disabled patients, on the contrary,may be in hospital because of deprived home circum-stances. On the other hand disabled patients may bein their previous jobs because it happens that theirparticular work and their disability makes thispossible; for example, we had a shepherd who wasalmost completely aphasic, but because he could stillwhistle to his dog he had resumed work. Sometimesemployers are unusually tolerant of the inadequacies
291
of a former staff member, at least for a time andparticularly if he has long service and has managerialor supervisory status. Such a patient may claim to beback at work, when in truth he is being covered orcushioned to a considerable extent. On the otherhand, patients who have made a good recovery maynot return to work, for a variety of personal orsocioeconomic reasons. For these reasons classifica-tion of outcome which rely too much on whether ornot a patient is in care or at home, or has returned towork or not, may be misleading in a number of cases.Another source of bias in assessing overall out-
come derives from judging this in the light of theknown severity of the injury. The comment may bemade that the patient has made a good recovery"considering how bad he was". This is especiallylikely to occur when outcome is judged by those whowere responsible for the early management. It mustbe remembered that the patient and the familyjudges the outcome by comparison with the pre-traumatic state. In the early months, however, thefamily may share the optimism of members of thetherapeutic team (with whom they share the memoryof how bad the patient initially was) and may thustend to over-estimate the degree of recovery. Duringthe stage of relatively rapid improvement a monthor so after injury assessment may prove to include anelement of expectation or prediction (or hope) aboutthe ultimate degree of recovery rather than being atrue appraisal of the state at the present time.Most conscious survivors after severe injury
(more than six hours in coma) have some deficit,even those judged to have made a good recovery.However, marked neurological deficit is relativelyuncommon; only 16% of these severely braindamaged patients had persisting, marked hemiplegia.Unlike survivors after stroke, who have sufferedmajor focal damage, head injured patients havemostly sustained widespread damage which has moreeffect on mental than on neurological function.Personality change is the most consistent finding,and this can constitute an appreciable deficit even inpatients without significant cognitive or physicalsequelae. Mental deficits contribute more significantlyto social disability than do persisting neurologicalsigns, as previously reported in a smaller series.27Mental deficits also contribute more to the burdenreported by caring relatives than does physicalhandicap. 28
Time scale ofrecoveryRecovery is a dynamic process. How long it maycontinue is a matter of controversy, partly becauseof the lack of agreed criteria by which to measurechanges in the overall degree of recovery with time;and partly because different components of recovery
Protected by copyright.
on March 17, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.4.285 on 1 April 1981. D
ownloaded from

292
may plateau at different periods after injury.21-23 27Isolated reports of continued improvement over
years, and ofoccasional cases ofdelayed late recovery,have led to the generalisation that assessment ofultimate outcome should be postponed for years inthose who are disabled; moreover, clinicians may
therefore remain optimistic about further substantialimprovement for longer than is realistic. It is our
experience that maintaining unrealistic expectationsfor further substantial recovery may impede theacceptance of disability by the patient and his family;this in turn will postpone the time when practicalsteps are taken to adjust to the new circumstances ofplanning the future in the light of the disability.Another aspect of the persistence of disability inmany severely injured patients is that the prevalenceof patients in the community who are suffering fromhead injury is considerable. Even severely disabledyounger patients have only five years reduction inexpectancy of life over the next 20 years, accordingto Roberts;'7 thus many disabled patients live for20-40 years after head injury.Our studies emphasise that the proportional
distribution ofpatients among the outcome categoriesof the Glasgow Scale does change considerably astime passes during the first year after injury. Validcomparisons between the results of treatment inseries of severely head injured patients thereforerequires adequate information about when outcomewas assessed. But our studies also show that themajority of patients have reached their final outcomecategory (on this scale) within six months of injury,and that very few change category after a year. Thisis not to deny that there may be considerable im-provement without this being sufficient to justifyreclassification. This later improvement in overallsocial functioning may not be associated with anymeasurable change in neurological deficit or inmental performance on tests. Instead it may reflecta passing of the phase of denial of disability throughwhich many patients pass and that hinders theirmaking appropriate adjustments in their mode oflife. What is subsequently recorded as improvementmay therefore represent adaptation or acceptance ofa disability which is in fact fixed and will not becomeany less.
Quality of lifeMuch is heard nowadays about the importance ofquality of life in patients rescued from life-threateningsituations; when it is judged that the life saved seemsto be hardly worth living then doubts are sometimesraised about the wisdom of having expended suchefforts to achieve survival. Such doubts are particuu-larly likely to arise in regard to head injured youthspreviously fully normal and with so many years
B Jennett, J Snoek, MR Bond, andN Brooks
ahead of them. But discussion about the quality of lifetends to remain unfocused; it may therefore behelpful to consider six aspects of living as a basis forreviewing a given patient's disability.
(1) Activities of daily living (ADL) are widely usedby geriatricians when analysing the degree of de-pendence of victims of stroke. Scores are evolved toindicate whether the patient can feed, dress and toilethimself, or requires varying degrees of aid fromothers; mobility-from bed to chair, or around theroom, is another vital activity. An elderly patient mayregard a degree of partial independence for some ofthese activities as a reasonable achievement; a manin his twenties may take a different view.
(2) Mobility beyond the sick room-about thehouse and outside of it-is essential if the patient isto have the possibility of organising his life himself,either hour to hour or day to day. It may be thatmental handicap prevents this, the patient requiringsomeone else to plan every part of the day lest heforgets to start, or fails to finish, even simple tasks,like preparing a meal.
(3) Social relationships depend on initiative andresponse-the patient who must wait to be visitedor is limited entirely to the company of his ownfamily may feel limited and frustrated.
(4) Work or leisure activities represent the nextstage in the hierarchy of returning to normal life,and are important for most people's sense of purpose-once the struggle for survival, and then to achievethe activities of daily life, is over.
(5) Present satisfaction and future prospects aredifficult to measure, and depend to some extent onpre-traumatic personality. Some patients seem tohave such blunted insight that they may not seemto suffer; others are only too well aware of theirplight and are frustrated by their limitations. It isunfeeling to pretend that the initial satisfaction atachieving certain milestones of recovery will belasting, if the recovery is arrested far short of thatpatient's previous performance. Doctors need toguard against glib judgements such as "practical orworthwhile recovery," which often prove to beeuphemisms for severe disability. Similarly it isdoubtful whether outcome scales that have manysubdivisions within the category that we have termedsevere disability, are helpful in reflecting the truedegree of disability. Thus the eleven point scale ofRoberts'7 recognised severe and profound disabilityas well as total dependence, and then subdivided thelatter into four more categories. This may be of someuse in indicating the amount of physical supportrequired on an hour to hour basis, but in terms ofsurvival over many years it does not seem to ususeful to have as many subdivisions.More important is to recognise the burden borne
Protected by copyright.
on March 17, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.4.285 on 1 April 1981. D
ownloaded from

Disability after severe head injury
by the families of patients who do becomeindependent, but who have serious mental deficits,particularly of personality. Such patients may seemto be functioning at a satisfactory level when com-pared with the population in general, even on formalpsychological tests-but their relatives and closefriends know that they are changed persons. Pre-viously quiet and kind, they may now be talkativeand tactless, liable to outbursts of temper, forgetfuland irritable. This is much harder for relatives tobear than hemiplegia or even paraplegia-and it isunfair to draw comparisons with severe physicaldisability and the courage and resourcefulness withwhich it is dealt with by patients and their families.After brain damage the ability to cope and to adaptis affected, as part of the disability, whilst the natureof the mental disability is more likely to causeexasperation than to provoke pity or to elicitsympathy.
These studies formed part of a programme ofresearch into head injury supported by the MedicalResearch Council.
References
I Jennett B, Bond M. Assessment of outcome aftersevere brain damage. Lancet 1975; i:480-4.
2 Jennett B, Teasdale G, Galbraith S, et al. Severe headinjuries in three countries. J Neurol NeurosurgPsychiatry 1977; 40:291-8.
3 Bates D, Caronna JJ, Cartlidge NEF, et al. Aprospective study of non-traumatic coma: methodsand results in 310 patients. Ann Neurol 1977; 2:211-20
4 Langfitt TW. Measuring the outcome from headinjuries. JNeurosurg 1978; 48:673-8.
5 Jennett B, Plum F. Persistent vegetative state afterbrain damage. Lancet 1972; i:734-7.
6 Jennett B, Teasdale G, Braakman R, et al. Prognosisin series of patients with severe head injury. Neuro-surgery 1979; 4:283-9.
7 Carlsson CA, Essen C von, Lofgren J. Factorsaffecting the clinical course of patients with severehead injuries. J Neurosurg 1968; 29:242-51.
8 Pazzaglia P, Frank G, Frank F, Gaist G. Clinicalcourse and prognosis of acute post-traumatic coma.J Neurol Neurosurg Psychiatry 1975; 38: 149-54.
9 Heiskanen 0, Sipponen P. Prognosis of severe braininjury. Acta Neurol Scand 1970; 46:343-8.
10 Vigoroux RP. Rehabilitation. Neurochirurgica 18;suppl 2: 1972.
11 Overgaard J, Christensen S, Hvid-Hansen 0, et al.Prognosis after head injury based on early clinicalexamination. Lancet 1973; ii:631-5.
293
12 Vapalahti M, Troupp H. Prognosis for patients withsevere brain injuries. BritMedJ 1971 ; 3:404-7.
13 Jennett B, Teasdale G, Braakman R, Minderhoud J,Knill-Jones R. Predicting outcome in individualpatients after severe head injury. Lancet 1976;i:1031-4.
14 Titterington DM, Murray GD, Parker LS, et al.Comparison of discrimination techniques applied toa complex data set of head injured patients. J RoyStat Soc 1980. In press.
15 Najenson T, Mendelson L, Schechter I, David C,Mintz N, Groswasser Z. Rehabilitation after severehead injury. ScandJ Rehab 1974; 6:5-14.
16 Stover SL, Zeiger HE. Head injury in children andteenagers: functional recovery correlated with theduration of coma. Arch Phys Med Rehab 1976;57:201-5.
17 Roberts AH. Severe Accidental Head Injury. AnAssessment of Long-Term Prognosis. London:MacMillan Press, 1979.
18 Rankin J. Cerebral vascular accidents in patientsover the age of 60. Scot MedJ 1957; 2:127,200-55.
19 Adams, GF. Prospects for patients with strokes. BrMedJ 1963; 2:253-9.
20 Bond MR, Brooks DN. Understanding the process ofrecovery as a basis for the investigation of rehabili-tation for the brain injured. Scand J Rehab 1976;8:127-33.
21 Brooks DN, Aughton ME. Cognitive recoverythrough the first year after severe blunt head injury.Int Rehab Med 1979; 1 :166-72.
22 Mandleberg IA, Brooks DN. Cognitive recoveryafter severe head injury. 1 Serial testing on theWechsler Adult Intelligence Scale. JNeurolNeurosurgPsychiatry 1975; 38:1121-6.
23 Mandleberg IA. Cognitive recovery after severe headinjury. 3 WAIS verbal and Performance IQs as afunction of post-traumatic amnesia duration andtime from injury. J Neurol Neurosurg Psychiatry1976;39:1001-7.
24 Bond MR Stages of recovery from severe headinjury with special reference to late outcome. IntRehab Med 1979; 1 :155-9.
25 Brooks DN, Aughton ME. Cognitive consequencesof blunt head injury. Int Rehab Med 1979; 1:1 60-5.
26 Brooks DN, Aughton ME, Bond MR, Jones eRizvi S. Cognitive sequelae in relationship to thearly indices of severity of brain damage after severeblunt head injury. J Neurol Neurosurg Psychiatry1980; 43:529-34.
27 Bond MR. Assessment of the psychosocial outcomeof severe head injury. Acta Neurochir 1976; 34:57-70.
28 McKinlay WW, Brooks DN, Bond MR, Martinage,D, Marshall MM. Outcome of severe blunt headinjury as reported by relatives of the injured person.Submitted to J Neurol Neurosurg Psychiatry 1980.
29 Jamieson KG. Prevention of head injury. In: HeadInjuries. Edinburgh: Churchill Livingstone 1971.12-15.
Protected by copyright.
on March 17, 2020 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.44.4.285 on 1 April 1981. D
ownloaded from