direction-modulated brachytherapy for high-dose-rate treatment of cervical cancer. i: theoretical...
TRANSCRIPT
International Journal of
Radiation Oncologybiology physics
www.redjournal.org
Physics Contribution
Direction-Modulated Brachytherapy for High-Dose-RateTreatment of Cervical Cancer. I: Theoretical DesignDae Yup Han, MSc,*,y Matthew J. Webster, MSc,*,z Daniel J. Scanderbeg, PhD,*Catheryn Yashar, MD,* Dongju Choi, PhD,* Bongyong Song, PhD,*Slobodan Devic, PhD,x,k Ananth Ravi, PhD,{ and William Y. Song, PhD*,{
Departments of *Radiation Medicine and Applied Sciences, yElectrical and Computer Engineering, and zPhysics, Universityof California San Diego, La Jolla, California; xMedical Physics Unit, McGill University, Montreal, Quebec, Canada;kDepartment of Radiation Oncology, Jewish General Hospital, Montreal, Quebec, Canada; and {Department of MedicalPhysics, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada
Received Oct 1, 2013, and in revised form Feb 11, 2014. Accepted for publication Feb 26, 2014.
Summary
A novel, DMBT-concept,HDR tandem applicator thatallows for improved doseconformality in cervicalcancer treatment is proposed.The design consists of 6grooved channels in an MRI-compatible tungsten rod,encased in polyoxy-methylene plastic tubing,with a 6.4-mm total thick-ness. After replanning 15patient cases treated with aconventional tandem andovoids applicator, the DMBTapplicator consistently pro-duced better-quality plans,with better OAR sparing,thus fittingly complementingthe latest 3D imagingebased
Reprint requests to: William Y. Song, PhD
Physics, Sunnybrook Health Sciences Centre
Toronto, ON M4N 3M5, Canada. Tel: (416) 4
This project has been supported by a Un
Diego R01 Bridge Grant and the Collaborativ
Int J Radiation Oncol Biol Phys, Vol. -, No.
0360-3016/$ - see front matter � 2014 Elsevie
http://dx.doi.org/10.1016/j.ijrobp.2014.02.039
Purpose: To demonstrate that utilization of the direction-modulated brachytherapy(DMBT) concept can significantly improve treatment plan quality in the setting ofhigh-dose-rate (HDR) brachytherapy for cervical cancer.Methods and Materials: The new, MRI-compatible, tandem design has 6 peripheralholes of 1.3-mm diameter, grooved along a nonmagnetic tungsten-alloy rod(r Z 18.0 g/cm3), enclosed in Delrin tubing (polyoxymethylene, r Z 1.41 g/cm3),with a total thickness of 6.4 mm. The Monte Carlo N-Particle code was used to calcu-late the anisotropic 192Ir dose distributions. An in-house-developed inverse planningplatform, geared with simulated annealing and constrained-gradient optimization algo-rithms, was used to replan 15 patient cases (total 75 plans) treated with a conventionaltandem and ovoids (T&O) applicator. Prescription dose was 6 Gy. For replanning, wereplaced the conventional tandem with that of the new DMBT tandem for optimizationbut left the ovoids in place and kept the dwell positions as originally planned. AllDMBT plans were normalized to match the high-risk clinical target volume V100coverage of the T&O plans.Results: In general there were marked improvements in plan quality for the DMBTplans. On average, D2cc for the bladder, rectum, and sigmoid were reduced by0.59 � 0.87 Gy (8.5% � 28.7%), 0.48 � 0.55 Gy (21.1% � 27.2%), and0.10 � 0.38 Gy (40.6% � 214.9%) among the 75 plans, with best single-plan reduc-tions of 3.20 Gy (40.8%), 2.38 Gy (40.07%), and 1.26 Gy (27.5%), respectively. Thehigh-risk clinical target volume D90 was similar, with 6.55 � 0.96 Gy and6.59 � 1.06 Gy for T&O and DMBT, respectively.
, Department of Medical
, University of Toronto,
80-5000 x87181; E-mail:
iversity of California San
e Research Opportunities
(CRO) Program at the San Diego Supercomputer Center (Award Number
CRO04). S.D. is a research scientist supported by the Fonds de Recherche
en Sante du Quebec (FRSQ).
Conflict of interest: none.
AcknowledgmentdThe authors thank Mr. Harry Easton of Sunnybrook
Engineering Services for manufacturing the prototype applicator.
-, pp. 1e8, 2014r Inc. All rights reserved.

Han et al. International Journal of Radiation Oncology � Biology � Physics2
brachytherapy planning
trend.Conclusions: Application of the DMBT concept to cervical cancer allowed forimproved organ at risk sparing while achieving similar target coverage on a sizeablepatient population, as intended, by maximally utilizing the anatomic information con-tained in 3-dimensional imaging. A series of mechanical and clinical validations are tobe followed. � 2014 Elsevier Inc.
Introduction
At present, external beam radiation therapy (EBRT) fol-lowed by brachytherapy (with or without concurrentchemotherapy) is the standard treatment for cervical cancer(1). With EBRT alone it has been shown to be difficult todeliver prescription dose to tumors without significant sideeffects, such as inflammation, fibrosis, necrosis, and fis-tulas, because of the anatomic location of the normal pelvicorgans surrounding the cervix (2). For this reason, high-dose-rate (HDR) intracavitary brachytherapy plays amajor role in the therapeutic management of patients withcervical cancer (2-6). Traditionally, many systems of ap-plicators (eg, Manchester, Fletcher, Stockholm) have beenproposed for cervical cancer treatment, typically localizedwith 2-dimensional (2D) x-ray imaging (1, 2, 7). Two-dimensional x-ray images, however, are not adequate toidentify anatomic organs, thus potentially increasing therisk of complications (7-9). Furthermore, this system as-sumes that all tumors are the same size and shape. If thetumor happens to extend to the pelvic sidewall, forexample, then this would increase relapse rates (10, 11).
Modern 3-dimensional (3D) imaging technologies, suchas CT and MRI, give more valid and reliable informationabout individual tumor extension and organ configurations(2-6). Compared with traditional treatment approachesusing 2D imaging, image-guided adaptive brachytherapy(IGABT) using 3D imaging leads to better tumor coverageand organ-at-risk (OAR) sparing, thus providing superioroutcomes (7, 12-15). To help ease the 2D-to-3D transitionto clinic, the Groupe Europeen de Curietherapie and Eu-ropean Society for Radiotherapy and Oncology formed agynecologic working group to publish a series of guidelinesfor acceptable treatment practices (2-5). According to theguidelines, the high-risk clinical target volume (HRCTV)for brachytherapy is at least the entire cervix for any stageand treatment protocol plus the palpable disease. In addi-tion, depending on the residual tumor extent, some partsof the corpus uteri, vagina, or parametrium should beincluded (1, 2). However, the frequent abutment of theOARs, such as bladder, rectum, and sigmoid, to theHRCTV makes adherence to the desired dose volume ob-jectives challenging. Ideally, because of the geometricpositioning of the HRCTV and the surrounding OARs, thedose distribution should generally be compressed in theanterioreposterior direction for maximal OAR sparing.With conventional intracavitary applicators, such as tan-dem, ovoids, and rings, this is very challenging to achieve
(ie, anterior-posteriorecompressed isodose lines). This iswhy combined intracavitaryeinterstitial applicators arefinding more frequent utilization in IGABT (15). Althoughthe interstitial needles are useful, the adequate training ofphysicians and the dependence of the treatment plan qualityon skill and experience of the physician inserting the nee-dles into the appropriate positions are some of the chal-lenges. Obviously, intracavitary-alone applicators are lessprone to these issues.
There are broadly 2 types of growth patterns for cervicalcancer: exophytic and endophytic (1). For the exophyticgrowth pattern the cervical cancer tends to grow outward(favorable for Papanicolaou tests), whereas for the endo-phytic growth pattern the cervical cancer tends to growinward toward the uterus along the cervical canal. Thelength of the canal is typically 2-5 cm. For intracavitaryapplicators, if the gross disease does not regress by the timebrachytherapy is administered (eg, extended disease), thecancer can be too far in the superior direction to be reachedby the dose from the ovoids (or rings). Therefore, virtuallythe entire dose must come from the tandem, which has anextremely limiting fluence modulation capability becausethe 192Ir source is isotropic and the tandem is single-channeled. Therefore, limiting dose to OARs, especiallythe bladder and sigmoid, becomes quite challenging inthese cases. Innovations such as the Fletcher-Williamsonapplicator, (balloon) spacers, and rectal retractors (16)can help reduce the dose to OARs, but these technologiestypically assist in dose limitations from the vagina, thusmostly benefiting the rectal dose at and below the cervixonly. Thus, to date, the best treatment option for extendeddisease remains use of combined intracavitaryeinterstitialapplicators (15).
To address the seemingly apparent lag in intracavitaryapplicator technology development, and to complement therecent trend of 3D imaging-based IGABT, we propose anovel intrauterine tandem design that is capable of creatinganisotropic 192Ir radiation profiles that can generate highlyconformal dose distributions to nonsymmetrical targetvolumes. The design allows modulation of directional ra-diation profiles (process called anisotropic modulation), incombination with inverse planning and algorithmic opti-mizations, to achieve superior levels of dose conformality.The concept is called direction-modulated brachytherapy(DMBT) and recently has been applied successfully forrectal and breast cancer applications (17-19). This articlewill discuss the concept, design, and performance analysiswith 15 patient cases (total 75 plans) clinically treated with

Volume - � Number - � 2014 DMBT for HDR brachytherapy of cervical cancer 3
conventional tandem and ovoids (Conv. T&O) applicators.The study aims to demonstrate that utilization of the DMBTconcept can significantly improve treatment plan quality inthe setting of cervical cancer HDR brachytherapy.
Methods and Materials
Applicators and designs
The titanium Fletcher-Suit-Delclosestyle T&O applicatorset (Varian Medical Systems, Palo Alto, CA) was used forall HDR treatments. The tandem is hollow and is composedof titanium (r Z 4.5 g/cm3) (20) with a 3-mm diameter,and each ovoid is wrapped by Delrin (polyoxymethylene,r Z 1.41 g/cm3) around the titanium channel.
In this study the intrauterine tandem was redesigned toconform to the DMBT concept (17-19). The ovoids wereleft unchanged and are compatible with the new tandemdesign. Figure 1 illustrates our proposed design. As can beseen, the DMBT tandem design has 6 peripheral holes of1.3-mm diameter, grooved along a nonmagnetic tungsten-alloy rod (r Z 18.0 g/cm3), enclosed in Delrin tubing,with the tungsten rod and total thickness of 5.4 and 6.4 mm,respectively. Materials were chosen carefully to be MRIcompatible with the tungsten-alloy rod composition of 95%tungsten, 3.5% nickel, and 1.5% copper. Because of thegun-revolver-type design with 60� angular channel spacing(Fig. 1d), it allows for anisotropic modulation of radiationprofiles as opposed to the conventional isotropic radiationprofile of the 192Ir source (Fig. 1f).
Patient data
The patient planning dataset comprised 75 individual plans(15 patients with 5 fractions per patient), nonsurgical andnoninterstitial candidates, treated with the Varian T&Oapplicator (described above). The clinical cases were wideranging, with age of 49.1 � 11.3 (range, 24-62) years,HRCTV volume of 24.3 � 10.4 (range, 5.0-55.0) cm3, andInternational Federation of Gynecology and Obstetricsstage IB1-IIIB. The prescription dose was 6 Gy. All patientsreceived EBRT of 1.8 Gy � 25 fractions to the whole pelvisbefore brachytherapy, which were initiated near the end ofEBRT. The total course of treatment was completed within56 days. All plans were CT based, with at least 1 MRI scantaken during/before the brachytherapy course, and plannedon BrachyVision (Varian Medical Systems). Every plan hadat least the HRCTV, bladder, rectum, and sigmoidcontoured.
Monte Carlo simulations
The Monte Carlo N-Particle version 2.6.0 simulationspackage was used to calculate the dose distributionsresulting from the VariSource iX 192Ir source (VarianMedical Systems). It has 2 identical adjoining iridium cores
0.34 mm in diameter and 2.5 mm in length each, and isencapsulated by a 0.59-mm diameter nitinol wire of density6.45 g/cm3. For each decay event simulated, an average of2.363 g emissions were generated (21). To achieve bettersimulation efficiency, a lower energy cutoff of 10 keV forelectron transport simulations was enforced (17-19). Allspace outside of the applicator was treated as water. Allsimulations were run through the San Diego SupercomputerCenter, using 512 central processing unit (CPU) cores, eachsimulating 100,000 particles, for a total of 51 million decayevents. A uniform cubic voxel size of 2.5 mm3 was usedand subsequently interpolated (using exponential interpo-lation) down to a 1.0-mm3 dose grid. Because of the rota-tional symmetry of the applicator, it was only necessary tosimulate dwell positions along a single channel.
DMBT plan optimization
Both the T&O and DMBT plans were reoptimized toreceive the exact same V100 coverage as achieved in theclinically treated T&O plans, using the in-house-codedgradient projection convex optimization algorithm (17-19).A quadratic objective function, with variable weights thatare kept constant between the 2 applicator plans, was usedto minimize the dose to the OARs while matching the V100coverage. Except for a nonnegativity condition on the dwelltimes, no additional dose constraints were enforced.Weights and optimization conditions were kept constantduring the generation of the T&O and DMBT plans. Arigorous explanation of the optimization process used ispresented in the first DMBT work (17-19). No manualadjustments by an expert physician followed after theoptimization. This was done to maintain the integrity ofcomparing the capability to generate conformal, asym-metric plans by the T&O and DMBT applicators, withoutintroducing external bias. Thus the plans can deviate fromthe classic “pear-shape” (and are not of clinically treatablequality). This was acceptable because the main objective ofthis planning exercise was to demonstrate the flexibility inthe DMBT applicator to achieve conformal dose distribu-tions to nonsymmetric target volumes, driven by theanisotropic modulation.
The clinically relevant parameters (22), such as D0.1 ccand D2cc for OARs, and V100, V150, V200, and D90 forHRCTV, were calculated thereafter.
Results
Monte Carlo N-Particle dose calculations
The variance of energy deposition calculations was <1%for most regions of clinical interest. Typically the variancewithin 20 mm from the source was <0.5%. The opensource simulation was compared with Task Group (TG)-43standards (23, 24), and the agreement was within 2%.

Fig. 1. (a) A conventional tandem and ovoid applicator. (b) The direction-modulated brachytherapy (DMBT) tandemdesign with 6 peripheral holes in a multi-groove design. (c) A conventional tandem cross-section. (d) The DMBT tandemcross-section. (e) A Monte Carlo simulated dose distribution of an isotropic 192Ir source in a conventional tandem. (f) AMonte Carlo simulated dose distribution of a directional 192Ir radiation profile emitted in the DMBT tandem.
Han et al. International Journal of Radiation Oncology � Biology � Physics4
Figure 1e and f show the resulting dose distributionscorresponding to the open source, from the Monte Carlosimulations, in the conventional tandem and DMBT tan-dem, respectively. Compared with the isotropic dose dis-tribution typical of an open source for the conventionaltandem (Fig. 1e), the DMBT tandem is characterized by amarked directionality (Fig. 1f) due to the tungsten shielddesign with 14.7% backside leakage, measured at 10 mmfrom the center. Because of the off-center position of the192Ir source (ie, 2.05 mm from the center), doses aregenerally hotter on the open side of the DMBT applicator
compared with the same corresponding positions in theconventional tandem.
Plan data and design
Table 1 lists the HRCTV D90 values, averaged over 5 plansper patient, and the population average of all 75 plans, forthe Conv. T&O and DMBT plans. In terms of targetcoverage, the D90 was similar between the 2 plans, with6.55 � 0.96 Gy and 6.59 � 1.06 Gy for T&O and DMBT,respectively.
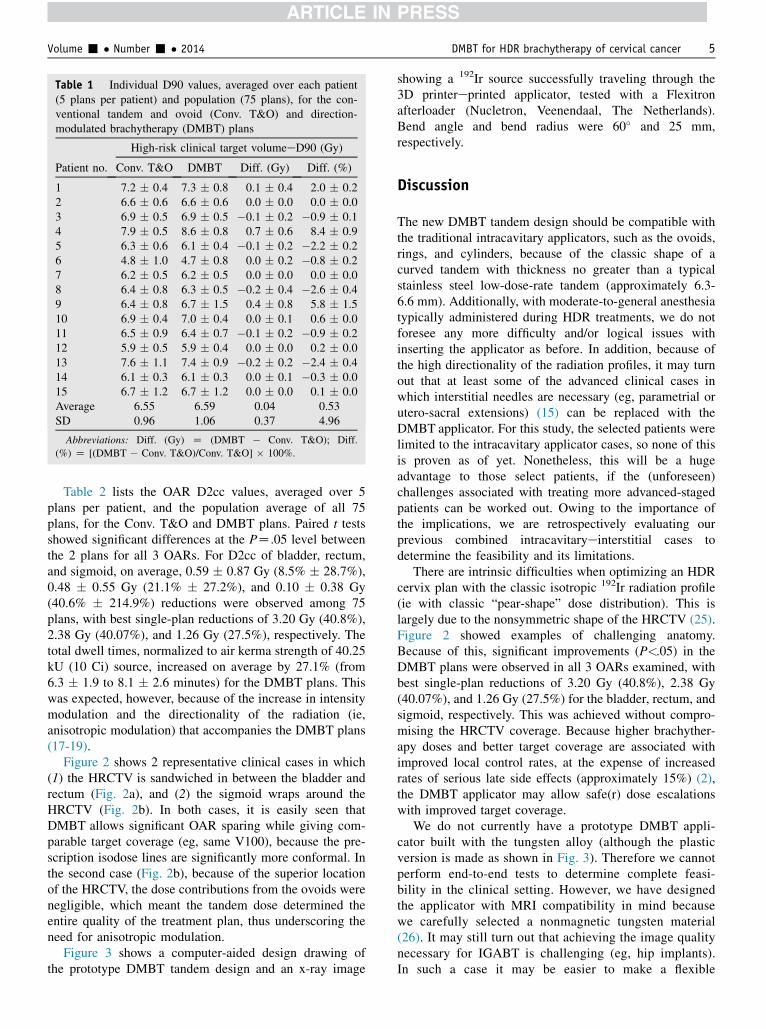
Table 1 Individual D90 values, averaged over each patient(5 plans per patient) and population (75 plans), for the con-ventional tandem and ovoid (Conv. T&O) and direction-modulated brachytherapy (DMBT) plans
Patient no.
High-risk clinical target volumeeD90 (Gy)
Conv. T&O DMBT Diff. (Gy) Diff. (%)
1 7.2 � 0.4 7.3 � 0.8 0.1 � 0.4 2.0 � 0.22 6.6 � 0.6 6.6 � 0.6 0.0 � 0.0 0.0 � 0.03 6.9 � 0.5 6.9 � 0.5 �0.1 � 0.2 �0.9 � 0.14 7.9 � 0.5 8.6 � 0.8 0.7 � 0.6 8.4 � 0.95 6.3 � 0.6 6.1 � 0.4 �0.1 � 0.2 �2.2 � 0.26 4.8 � 1.0 4.7 � 0.8 0.0 � 0.2 �0.8 � 0.27 6.2 � 0.5 6.2 � 0.5 0.0 � 0.0 0.0 � 0.08 6.4 � 0.8 6.3 � 0.5 �0.2 � 0.4 �2.6 � 0.49 6.4 � 0.8 6.7 � 1.5 0.4 � 0.8 5.8 � 1.510 6.9 � 0.4 7.0 � 0.4 0.0 � 0.1 0.6 � 0.011 6.5 � 0.9 6.4 � 0.7 �0.1 � 0.2 �0.9 � 0.212 5.9 � 0.5 5.9 � 0.4 0.0 � 0.0 0.2 � 0.013 7.6 � 1.1 7.4 � 0.9 �0.2 � 0.2 �2.4 � 0.414 6.1 � 0.3 6.1 � 0.3 0.0 � 0.1 �0.3 � 0.015 6.7 � 1.2 6.7 � 1.2 0.0 � 0.0 0.1 � 0.0Average 6.55 6.59 0.04 0.53SD 0.96 1.06 0.37 4.96
Abbreviations: Diff. (Gy) Z (DMBT � Conv. T&O); Diff.
(%) Z [(DMBT � Conv. T&O)/Conv. T&O] � 100%.
Volume - � Number - � 2014 DMBT for HDR brachytherapy of cervical cancer 5
Table 2 lists the OAR D2cc values, averaged over 5plans per patient, and the population average of all 75plans, for the Conv. T&O and DMBT plans. Paired t testsshowed significant differences at the PZ.05 level betweenthe 2 plans for all 3 OARs. For D2cc of bladder, rectum,and sigmoid, on average, 0.59 � 0.87 Gy (8.5% � 28.7%),0.48 � 0.55 Gy (21.1% � 27.2%), and 0.10 � 0.38 Gy(40.6% � 214.9%) reductions were observed among 75plans, with best single-plan reductions of 3.20 Gy (40.8%),2.38 Gy (40.07%), and 1.26 Gy (27.5%), respectively. Thetotal dwell times, normalized to air kerma strength of 40.25kU (10 Ci) source, increased on average by 27.1% (from6.3 � 1.9 to 8.1 � 2.6 minutes) for the DMBT plans. Thiswas expected, however, because of the increase in intensitymodulation and the directionality of the radiation (ie,anisotropic modulation) that accompanies the DMBT plans(17-19).
Figure 2 shows 2 representative clinical cases in which(1) the HRCTV is sandwiched in between the bladder andrectum (Fig. 2a), and (2) the sigmoid wraps around theHRCTV (Fig. 2b). In both cases, it is easily seen thatDMBT allows significant OAR sparing while giving com-parable target coverage (eg, same V100), because the pre-scription isodose lines are significantly more conformal. Inthe second case (Fig. 2b), because of the superior locationof the HRCTV, the dose contributions from the ovoids werenegligible, which meant the tandem dose determined theentire quality of the treatment plan, thus underscoring theneed for anisotropic modulation.
Figure 3 shows a computer-aided design drawing ofthe prototype DMBT tandem design and an x-ray image
showing a 192Ir source successfully traveling through the3D printereprinted applicator, tested with a Flexitronafterloader (Nucletron, Veenendaal, The Netherlands).Bend angle and bend radius were 60� and 25 mm,respectively.
Discussion
The new DMBT tandem design should be compatible withthe traditional intracavitary applicators, such as the ovoids,rings, and cylinders, because of the classic shape of acurved tandem with thickness no greater than a typicalstainless steel low-dose-rate tandem (approximately 6.3-6.6 mm). Additionally, with moderate-to-general anesthesiatypically administered during HDR treatments, we do notforesee any more difficulty and/or logical issues withinserting the applicator as before. In addition, because ofthe high directionality of the radiation profiles, it may turnout that at least some of the advanced clinical cases inwhich interstitial needles are necessary (eg, parametrial orutero-sacral extensions) (15) can be replaced with theDMBT applicator. For this study, the selected patients werelimited to the intracavitary applicator cases, so none of thisis proven as of yet. Nonetheless, this will be a hugeadvantage to those select patients, if the (unforeseen)challenges associated with treating more advanced-stagedpatients can be worked out. Owing to the importance ofthe implications, we are retrospectively evaluating ourprevious combined intracavitaryeinterstitial cases todetermine the feasibility and its limitations.
There are intrinsic difficulties when optimizing an HDRcervix plan with the classic isotropic 192Ir radiation profile(ie with classic “pear-shape” dose distribution). This islargely due to the nonsymmetric shape of the HRCTV (25).Figure 2 showed examples of challenging anatomy.Because of this, significant improvements (P<.05) in theDMBT plans were observed in all 3 OARs examined, withbest single-plan reductions of 3.20 Gy (40.8%), 2.38 Gy(40.07%), and 1.26 Gy (27.5%) for the bladder, rectum, andsigmoid, respectively. This was achieved without compro-mising the HRCTV coverage. Because higher brachyther-apy doses and better target coverage are associated withimproved local control rates, at the expense of increasedrates of serious late side effects (approximately 15%) (2),the DMBT applicator may allow safe(r) dose escalationswith improved target coverage.
We do not currently have a prototype DMBT appli-cator built with the tungsten alloy (although the plasticversion is made as shown in Fig. 3). Therefore we cannotperform end-to-end tests to determine complete feasi-bility in the clinical setting. However, we have designedthe applicator with MRI compatibility in mind becausewe carefully selected a nonmagnetic tungsten material(26). It may still turn out that achieving the image qualitynecessary for IGABT is challenging (eg, hip implants).In such a case it may be easier to make a flexible

Table 2 Individual D2cc values, averaged over each patient (5 plans per patient) and population (75 plans), for the conventionaltandem and ovoid (Conv. T&O) and direction-modulated brachytherapy (DMBT) plans
Patient
no.
BladdereD2cc (Gy) RectumeD2cc (Gy) SigmoideD2cc (Gy)
Conv.
T&O DMBT
Diff.
(Gy)
Diff.
(%)
Conv.
T&O DMBT
Diff.
(Gy)
Diff.
(%)
Conv.
T&O DMBT
Diff.
(Gy)
Diff.
(%)
1 4.3 � 1.1 4.3 � 0.8 �0.0 � 0.4 �0.9 � 0.3 3.8 � 0.9 3.4 � 0.7 �0.4 � 0.5 �10.3 � 3.3 0.7 � 0.8 0.7 � 0.7 0.0 � 0.2 1.4 � 2.0
2 2.4 � 2.0 2.1 � 1.7 �0.2 � 0.4 �8.9 � 10.5 1.0 � 0.9 0.7 � 0.7 �0.3 � 0.4 �33.7 � 46.8 1.4 � 1.3 1.3 � 1.2 0.0 � 0.1 �1.5 � 2.0
3 2.4 � 1.2 2.2 � 1.4 �0.2 � 0.3 �8.4 � 6.8 2.0 � 0.3 1.7 � 0.2 �0.3 � 0.2 �13.3 � 2.8 3.5 � 1.2 3.2 � 1.1 �0.3 � 0.3 �7.2 � 3.6
4 5.2 � 2.7 4.1 � 1.7 �1.1 � 1.4 �20.9 � 14.0 2.2 � 1.8 1.9 � 1.8 �0.3 � 0.2 �13.8 � 17.1 2.5 � 1.5 2.7 � 1.5 0.2 � 0.7 8.5 � 7.1
5 6.4 � 2.0 4.8 � 1.4 �1.6 � 1.0 �25.0 � 10.8 3.4 � 1.7 2.3 � 1.1 �1.0 � 0.9 �30.8 � 21.4 0.9 � 1.2 1.0 � 1.6 0.2 � 0.5 18.6 � 38.9
6 3.2 � 1.2 3.3 � 1.2 0.0 � 0.5 1.5 � 0.8 4.3 � 1.3 3.9 � 1.4 �0.4 � 0.3 �10.2 � 4.9 1.6 � 1.1 1.6 � 1.1 0.1 � 0.2 3.8 � 3.6
7 1.3 � 1.5 1.1 � 1.3 �0.2 � 0.3 �16.5 � 27.9 1.2 � 1.2 1.0 � 0.8 �0.3 � 0.4 �21.8 � 27.6 4.1 � 0.5 3.4 � 0.2 �0.6 � 0.6 �15.8 � 2.2
8 3.8 � 2.2 3.4 � 1.9 �0.4 � 0.4 �10.8 � 8.7 1.2 � 1.5 0.9 � 1.0 �0.3 � 0.5 �27.1 � 46.3 1.5 � 1.6 1.3 � 1.3 �0.2 � 0.5 �16.1 � 23.8
9 5.0 � 0.3 3.9 � 0.8 �1.1 � 0.6 �22.7 � 4.9 1.9 � 0.7 0.8 � 0.6 �1.1 � 0.7 �56.6 � 45.7 0.1 � 0.1 0.1 � 0.1 0.1 � 0.1 116.7 � 179.3
10 2.7 � 2.5 2.4 � 2.3 �0.3 � 0.3 �10.6 � 14.2 0.8 � 0.4 0.7 � 0.2 �0.1 � 0.3 �13.4 � 6.8 1.4 � 2.0 1.3 � 1.9 �0.1 � 0.1 �5.0 � 9.7
11 6.8 � 0.7 4.3 � 0.4 �2.5 � 0.4 �36.2 � 5.2 2.0 � 0.9 0.6 � 0.5 �1.4 � 0.6 �70.7 � 73.9 0.0 � 0.0 0.0 � 0.0 0.0 � 0.0 0.0 � 0.0
12 3.7 � 0.9 3.6 � 1.1 �0.1 � 0.2 �2.4 � 0.9 2.0 � 0.9 1.7 � 0.8 �0.3 � 0.1 �12.7 � 8.2 3.4 � 1.4 3.0 � 1.3 �0.4 � 0.4 �11.0 � 6.6
13 4.8 � 1.3 4.5 � 1.1 �0.3 � 0.5 �5.7 � 2.1 2.0 � 1.1 1.9 � 1.0 �0.1 � 0.2 �4.0 � 3.1 1.0 � 1.8 1.0 � 1.4 �0.1 � 0.4 �8.7 � 19.8
14 4.9 � 0.5 4.3 � 1.0 �0.6 � 0.8 �11.7 � 3.0 3.7 � 2.0 3.0 � 2.0 �0.6 � 0.5 �16.9 � 14.4 0.5 � 0.9 0.3 � 0.6 �0.2 � 0.3 �38.9 � 95.1
15 2.6 � 0.6 2.3 � 0.7 �0.3 � 0.3 �12.1 � 4.9 3.2 � 1.0 2.8 � 1.1 �0.4 � 0.2 �12.0 � 6.0 1.3 � 1.1 1.2 � 1.0 �0.1 � 0.2 �6.2 � 7.3
Average 3.95 3.37 �0.59* �8.47 2.30 1.82 �0.48* �21.13 1.58 1.48 �0.10* 40.63
SD 2.08 1.62 0.87 28.69 1.52 1.42 0.55 27.24 1.62 1.48 0.38 214.93
Abbreviations as in Table 1.
For all 3 organs at risk, the D2cc doses were significantly different at the level of PZ.05, using paired t tests.
* Statistically significantly different (paired t test).
Han et al. International Journal of Radiation Oncology � Biology � Physics6
place-holder applicator, insert it during the MRI, and usethe DMBT applicator for CT and coregister. A series ofclinical validation studies would need to be followed,
Fig. 2. Two representative anatomies of cervix cancer. (a) Atween a horseshoe-shaped bladder and an abutting rectum, and (sigmoid volume, representing a typical endophytic growth pattescription dose for the conventional tandem and ovoid and direct
however. In terms of CT compatibility, it may causemetal-induced artifacts that potentially obstruct contour-ing/planning. This needs to be fully addressed in the
high-risk clinical target volume (HRCTV) sandwiched be-b) a high-risk clinical target volume surrounded by a largern. Dotted and solid isodose lines represent the 6-Gy pre-ion-modulated brachytherapy (DMBT) plans, respectively.
Fig. 3. A computer-aided design drawing of the prototype direction-modulated brachytherapy (DMBT) tandem design(left) with an x-ray image showing the Nucletron 192Ir source successfully traveling through the 3-dimensional printeregenerated applicator using plastic (right). Bend angle and bend radius were 60� and 25 mm, respectively.
Volume - � Number - � 2014 DMBT for HDR brachytherapy of cervical cancer 7
future because there are hardware solutions (eg,increasing the x-ray energy [27]) and software solutions(eg, metal artifact reduction techniques [28]) that canenhance the compatibility. Dose calculation with a high-density metal presence was another potential concern tous because TG-43 formalism assumes a homogeneouswater medium (23, 24), thus requiring a significantmodification to the existing planning systems. However,with the recent introduction of model-based dose calcu-lation algorithms (29), heterogeneity corrections thatused to be ignored are now starting to be accounted for.This new trend could not have come at a better time: theDMBT concept is entirely based on the anisotropicity ofthe 192Ir radiation profile. Next-generation afterloaderdesigns, which may have a third drive (or more), couldalso aid in the adoption of the DMBT treatment paradigmbecause the third drive (or more) may have an intelli-gently designed shielding attached that can move incombination with an 192Ir source, for example, thuscreating anisotropic modulation tailored for individualpatient anatomy. Such a concept not only complementsthe up-and-coming trend of 3D imagingebased brachy-therapy planning (2-5, 13, 22), and with dose-volumeedriven objectives (4, 22), but is an intuitively naturalprogression that was already observed in the EBRT world(ie, transition from 3D conformal radiation therapy tointensity modulated radiation therapy for improved doseconformality in 3D target volumes (30).
Conclusions
Application of the DMBT concept (ie, anisotropic modu-lation) to cervical cancer allowed for improved OARsparing while achieving similar target coverage on a size-able patient population. The technology is intuitive anddesigned to maximally utilize the abundant anatomic in-formation contained in 3D imaging, in IGABT, fittinglyaligned with the latest dose-volumeedriven brachytherapyplanning trend. However, because the technology is still a
theoretical concept, a series of mechanical and clinicalvalidations are to be followed.
References
1. Berek JS. Berek and Novak’s Gynecology. 15th ed. Philadelphia:
Lippincott Williams & Wilkins; 2011.
2. Gerbaulet A, Potter R, Haie-Meder C. Cervix cancer. In: Gerbaulet A,
Potter R, Mazeron JJ, et al. editors. The GEC ESTRO Handbook of
Brachytherapy. Brussels: European Society of Therapeutic Radiology
and Oncology; 2002. p. 301-363.
3. Haie-Meder C, Potter R, Van Limbergen E, et al. Recommendations
from Gynaecological (GYN) GEC-ESTRO Working Group (I): Con-
cepts and terms in 3D image based 3D treatment planning in cervix
cancer brachytherapy with emphasis on MRI assessment of GTV and
CTV. Radiother Oncol 2005;74:235-245.
4. Potter R, Haie-Meder C, Limbergen EV, et al. Recommendations from
Gynaecological (GYN) GEC ESTRO Working Group (II): Concepts
and terms in 3D image-based treatment planning in cervix cancer
brachytherapyd3D dose volume parameters and aspects of 3D image-
based anatomy, radiation physics, radiobiology. Radiother Oncol
2006;78:67-77.
5. Dimopoulos JC, Petrow P, Tanderup K, et al. Recommendations from
Gynaecological (GYN) GEC-ESTRO Working Group (IV): Basic
principles and parameters for MR imaging within the frame of image
based adaptive cervix cancer brachytherapy. Radiother Oncol 2012;
103:113-122.
6. Lang S, Nulens A, Briot E, et al. Intercomparison of treatment con-
cepts for MR image assisted brachytherapy of cervical carcinoma
based on GYN GEC-ESTRO recommendations. Radiother Oncol
2006;78:185-193.
7. Sadozye A, Reed N. A review of recent developments in image-guided
radiation therapy in cervix cancer. Curr Oncol Rep 2012;14:519-526.
8. Perez CA, Grigsby PW, Lockett MA, et al. Radiation therapy
morbidity in carcinoma of the uterine cervix: Dosimetric and clinical
correlation. Int J Radiat Oncol Biol Phys 1999;44:855-866.
9. Barnes EA, Thomas G, Ackerman I, et al. Prospective comparison of
clinical and computed tomography assessment in detecting uterine
perforation with intracavitary brachytherapy for carcinoma of the
cervix. Int J Gynecol Cancer 2007;17:821-826.
10. Perez CA, Grigsby PW, Nene SM, et al. Effect of tumor size on the
prognosis of carcinoma of the uterine cervix treated with irradiation
alone. Cancer 1992;69:2796-2806.
11. Stehman FB, Bundy BN, Disaia PJ, et al. Carcinoma of the cervix
treated with radiation therapy I. A multi-variate analysis of prognostic

Han et al. International Journal of Radiation Oncology � Biology � Physics8
variables in the gynecologic oncology group. Cancer 1991;67:2776-
2785.
12. Kang HC, Shin KH, Park SY, et al. 3D CT-based high-dose-rate
brachytherapy for cervical cancer: Clinical impact on late rectal
bleeding and local control. Radiother Oncol 2010;97:507-513.
13. Potter R, Dimopoulos J, Georg P, et al. Clinical impact of MRI
assisted dose volume adaptation and dose escalation in brachytherapy
of locally advanced cervix cancer. Radiother Oncol 2007;83:148-155.
14. Tanderup K, Nielsen SK, Nyvang GB, et al. From point A to the
sculpted pear: MR image guidance significantly improves tumour dose
and sparing of organs at risk in brachytherapy of cervical cancer.
Radiother Oncol 2010;94:173-180.
15. Kirisits C, Lang S, Dimopoulos J, et al. The Vienna applicator for
combined intracavitary and interstitial brachytherapy of cervical
cancer: Design, application, treatment planning, and dosimetric re-
sults. Int J Radiat Oncol Biol Phys 2006;65:624-630.
16. Rai B, Patel FD, Chakraborty S, et al. Bladder-rectum spacer balloon
in high-dose-rate brachytherapy in cervix carcinoma. Int J Radiat
Oncol Biol Phys 2013;85:e217-e222.
17. Webster MJ, Devic S, Vuong T, et al. Dynamic modulated brachy-
therapy (DMBT) for rectal cancer. Med Phys 2013;40:011718.
18. Webster MJ, Devic S, Vuong T, et al. HDR brachytherapy of rectal
cancer using a novel grooved-shielding applicator design. Med Phys
2013;40:091704.
19. Webster MJ, Scanderbeg D, Yashar C, et al. Dynamic modulated
brachytherapy for accelerated partial breast irradiation. Med Phys
2013;40:466.
20. Haynes WM. CRC Handbook of Chemistry and Physics. 93th ed.
Oxford: Taylor & Francis; 2012.
21. Borg J, Rogers DWO. Monte Carlo Calculations of Photo Spectra in
Air from 192-Ir Sources, NRC Report No. PIRS-629r. Canada: Na-
tional Research Council; 1999.
22. Potter R, Fidarova E, Kirisits C, et al. Image-guided adaptive
brachytherapy for cervix carcinoma. Clin Oncol 2008;20:426-432.
23. Nath R, Anderson LL, Luxton G, et al. Dosimetry of interstitial
brachytherapy sources: Recommendations of the AAPM Radiation
Therapy Committee Task Group No. 43. Med Phys 1995;22:209-234.
24. Rivard MJ, Coursey BM, DeWerd LA, et al. Update of AAPM Task
Goup No. 43 report: A revised AAPM protocol for brachytherapy dose
calculations. Med Phys 2004;31:633-674.
25. Landoni F, Bocciolone L, Perego P, et al. Cancer of the cervix, FIGO
stages IB and IIA: Patterns of local growth and paracervical extension.
Int J Gynecol Canc 1995;5:329-334.
26. Price MJ, Jackson EF, Gifford KA, et al. Development of prototype
shielded cervical intracavitary brachytherapy applicators compatible
with CT and MRI imaging. Med Phys 2009;36:5515-5524.
27. Paudel MR, Mackenzie M, Fallone BG, et al. Evaluation of normal-
ized metal artifact reduction (NMAR) in kVCT using MVCT prior
images for radiotherapy treatment planning. Med Phys 2013;40:
081701.
28. Zhang X, Xing L. Sequentially reweighted TV minimization for CT
metal artifact reduction. Med Phys 2013;40:071907.
29. Beaulieu L, Tedgren AC, Carrier JF, et al. Report of the Task Group
186 on model-based dose calculation methods in brachytherapy
beyond the TG-43 formalism: Current status and recommendations for
clinical implementation. Med Phys 2012;39:6208-6236.
30. Bortfeld T. IMRT: A review and preview. Phys Med Biol 2006;51:
R363-R379.