digital transformation & the anywhere clinical desktop · “gate” your project 1....
TRANSCRIPT
Digital Transformation &
The Anywhere Clinical Desktop

DIGITAL CHANGE IS COMING

eHealth records coming to
emergency departments in NSW

BETTER INFORMED=
BETTER OUTCOMES

AGENDA
• Welcome and introductions
• Perspectives from the Health Sector
• Pain points and challenges
• Developing the business case for change
• How to get there
• A Day in the Life… What does “Good” look like?
• What next?
• Q&A
6

JOINING US TODAY…
• Andrew Fox – Director End User Computing and Mobility for ANZ, VMware
• David Lennon – Managing Partner Business Aspect
• Janet Brimson – Partner Data & Analytics, Business Aspect
• Nathan Wittke - Manager, Strategic Partners, End User Computing, VMware

PERSPECTIVES ON THE HEALTH SECTOR
• BA and VMware real life stories
From our experiences in the industry

WHY ARE WE HERE
• Extend on these perspectives
• Identify the areas of real pain in Health business and ICT
• Discuss the areas of highest priority
• Discuss a solution that meets many needs
9
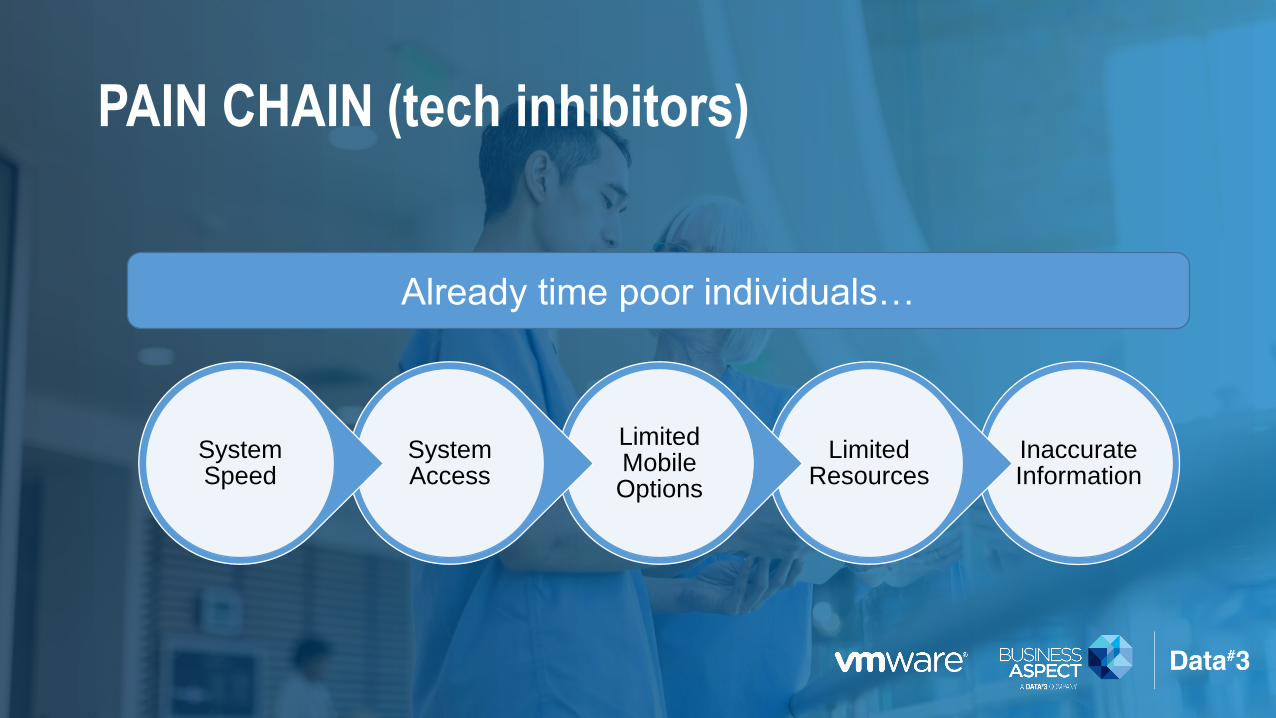
PAIN CHAIN (tech inhibitors)
Inaccurate Information
Limited Resources
Limited Mobile Options
System Access
System Speed
Already time poor individuals…

CHALLENGES YOU SEE EVERY DAY
• Fragmented poorly coordinated care
• Clinicians & Care teams over worked
• Need for Robust access to information
• Need for agile access to that information
• Limited resources
of healthcare IT operating budget is
spent on infrastructure
81%

THE VALUE OF DIGITAL CHANGE…
12
IMPROVEDDIAGNOSTICS
CLINICALWORKFLOW
SECURELY SHAREINFORMATION
PATIENTOUTCOMES
SYSTEMACCESS
ENABLINGTECHNOLOGIES

BETTER CLINICAL, PATIENT & BUSINESS OUTCOMES
13

What are your priority areas of pain with Health ICT?
Lets have a discussion….
14

THE ANYWHERE CLINICALDESKTOP
Imagine a desktop that moves with you:
• Logged in and working as soon as you are in the room
• Sharing results with patients on their own device without
craning over your shoulder
• User access & security, desktops & mobile devices all
coming together in one seamless eco-system
The Reality is Here:
• The Digital Clinical Workspace that moves with care
providers throughout their day

SO WHAT IS THE BUSINESS CASE
• Find clinical efficiencies
• Improve speed to treat
• Provide better patient service
• Increase systems usability
• Reduce infrastructure costs
• Improve identity management
• Streamline security
• Minimise infrastructure complexity
Domains
(eg. Emergency)
Roles
(eg. Clinicians)
Mobility
(eg. Smart watches
& smart phones
managing Clinical
scheduling)
Infrastructure Management
Security
Domains
(eg. general wards)
Domains
(eg. people s
bedside and homes
Domains
(eg. different
hospitals &
specialist services)
Roles
(eg. Admintrators)
Roles
(eg. Patients &
Carers)
Roles
(eg. Community
Health Workers,
Emergency
Workers)
Mobility
(eg. Moving from
Desktop to mobile
online forms on
admission)
Mobility
(eg. iPads & tablets
on the wards and
for home support)
Mobility
(eg. Patient records
updated anywhere,
anytime on any
device)
Virtual Devices
Access to the right information & systems at the right time
Anywhere, anytime on any device - supplied or BYOD

OUTCOMES
CARE TEAMS
• More time caring for patients
• Quicker access to clinical information
• Just in time access to information & relevant systems
PATIENT
• Better service
• Better understanding of care & medications
• Connected to the information experience
BUSINESS
• Effective resource use
• Simplify systems complexity
• Greater risk & security management
• Revenue savings

So where do things go wrong inHealthcare ICT projects?
Lets have a discussion….
18
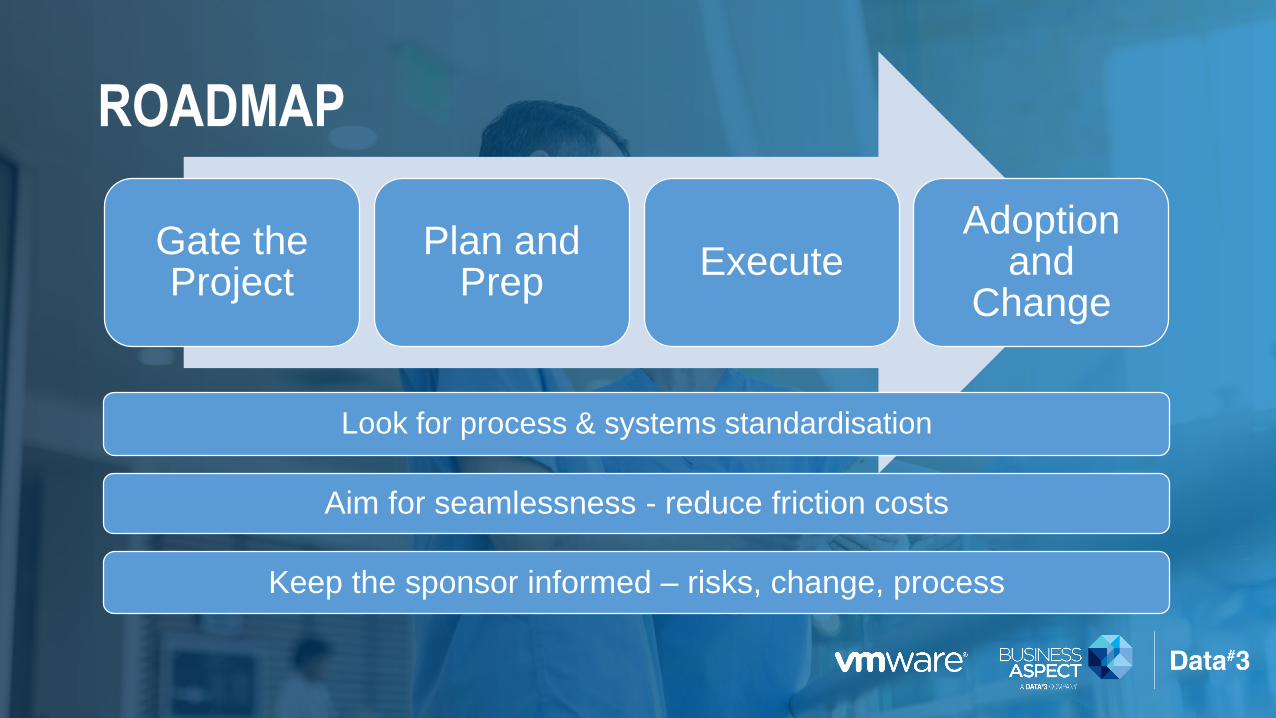
ROADMAP
Gate the Project
Plan and Prep
ExecuteAdoption
and Change
Aim for seamlessness - reduce friction costs
Keep the sponsor informed – risks, change, process
Look for process & systems standardisation
“GATE” YOUR PROJECT
1. Sponsorship – must have interest
2. Money – sponsor must have budget
3. User Readiness – users must be ready for change
4. IT Resources – resources need to be available, be made available or be procured
Kumar Chatani, Executive Vice
President and Chief Information
Officer, Mount Sinai Health
System, New York

PLAN AND PREPARATION
1. Audiences: Who are you enabling?
2. What devices do they like to use in these places?
3. Environment: Where are you enabling them?
4. Process & Context: What they need to do when they get there?
5. What systems do they access now/what’s missing - any pain points?
6. Security requirements per staff, patient and carer roles

PROJECT EXECUTION
1. Coordinated delivery and rollout
2. Device alignment to context
3. Centralised deployment
4. Training and handover for support staff

ADOPTION & CHANGE: BENEFITS REALISATION
1. The software they use is not changing
2. Communicating the benefits of change
3. Providing strong support on rollout and hypercare
4. Measuring the difference

OUTCOME: SIMPLE, SECURE & TAILORED TO CLINICIAN AND PATIENT OUTCOMES
• Improving health care outcomes
• Access to the right information quickly
• Supporting time poor people
• Getting tech out the way to get on with it
• Governance and Security assured
24

A Day in the Life…
What does “Good” Look Like?

THE DIGITALLY ENABLED CLINICIAN
11:30PM
Dr. Hoskin gets a call patient slipped
and injured himself. Using his
MacBook he accesses the digital
image and consults online with
orthopedic surgeon - decides bone is
not broken. Avoid trip to hospital.
7:00AM
Dr. Hoskin logs into his MacBook to check
his patient list for day accessing the hospitals
EMR system.
8:30AM
At the hospital, Dr. Hoskin taps his ID
badge on the integrated card reader at his
office workstation and immediately resumes
his EMR session and prepares for rounds.
10:30AM
Dr. Hoskin grabs an iPad and logs in
with his credentials. He is able to
engage a patient in their treatment
plan at bedside showing them their
latest lab result.
1:30PM
Dr. Hoskin uses his ID badge to log into a
shared clinical workstation in his recently
admitted patients room and immediately
shares the lab results. From there Dr
Hoskin starts his afternoon rounds.
1:15PM
Dr. Hoskin is at lunch at a local Café
when he receives an email on his
BYO Phone that the lab results he
was waiting on are now available. He
heads back to begin his rounds.

THE DIGITALLY ENABLED CLINICIAN7:00AM
Dr. Hoskin logs into his
MacBook to check his
patient list for day
accessing the hospitals
EMR system.

8:30AM
At the hospital, Dr. Hoskin taps
his ID badge on the integrated
card reader at his office
workstation and immediately
resumes his EMR session and
prepares for rounds.
THE DIGITALLY ENABLED CLINICIAN
THE DIGITALLY ENABLED CLINICIAN
10:30AM
Dr. Hoskin grabs an iPad and
logs in with his credentials.
He is able to engage a
patient in their treatment
plan at bedside showing
them their latest lab result.

THE DIGITALLY ENABLED CLINICIAN
1:15PM
Dr. Hoskin is at lunch at a local
Café when he receives an
email on his BYO Phone that
the lab results he was waiting
on are now available. He heads
back to begin his rounds.

THE DIGITALLY ENABLED CLINICIAN
1:30PM
Dr. Hoskin uses his ID badge
to log into a shared clinical
workstation in his recently
admitted patients room and
immediately shares the lab
results. From there Dr Hoskin
starts his afternoon rounds.
THE DIGITALLY ENABLED CLINICIAN
11:30PM
Dr. Hoskin gets a call
patient slipped and injured
himself. Using his MacBook
he accesses the digital
image and consults online
with orthopedic surgeon -
decides bone is not broken.
Avoids a trip to hospital.
WE ARE HERE TO HELP
• Design a POC to demonstrate the
value of the Anywhere Clinical Desktop
• Develop your:
• Deployment strategy
• Mobility strategy
• Security strategy
• Plan your Anywhere Clinical Desktop
Experience
We are making a difference with:
NSW eHealth
SA Health
WA Health
National Disability Insurance Agency
Metro Health South & North
Sunshine Coast PHN
Metropolitan Fire & Emergency
Services Board

QUESTIONS?

CONCLUSION
• See a live demonstration of The Anywhere Clinical Desktop at the Data#3 stand - Stand 1
• Next Steps1:1 meetings with David Lennon – Tuesday @ HIC from 1:00pm
• Prize draw winner announced
Thank you