differences in heart rate reserve of similar physical
TRANSCRIPT

University of Southern Denmark
Differences in heart rate reserve of similar physical activities during work and in leisure time –A study among Danish blue-collar workers
Coenen, Pieter; Korshøj, Mette; Hallman, David M.; Huysmans, Maaike A.; van der Beek,Allard J.; Straker, Leon M.; Holtermann, Andreas
Published in:Physiology and Behavior
DOI:10.1016/j.physbeh.2018.01.011
Publication date:2018
Document version:Accepted manuscript
Document license:CC BY-NC-ND
Citation for pulished version (APA):Coenen, P., Korshøj, M., Hallman, D. M., Huysmans, M. A., van der Beek, A. J., Straker, L. M., & Holtermann, A.(2018). Differences in heart rate reserve of similar physical activities during work and in leisure time – A studyamong Danish blue-collar workers. Physiology and Behavior, 186, 45-51.https://doi.org/10.1016/j.physbeh.2018.01.011
Go to publication entry in University of Southern Denmark's Research Portal
Terms of useThis work is brought to you by the University of Southern Denmark.Unless otherwise specified it has been shared according to the terms for self-archiving.If no other license is stated, these terms apply:
• You may download this work for personal use only. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying this open access versionIf you believe that this document breaches copyright please contact us providing details and we will investigate your claim.Please direct all enquiries to [email protected]
Download date: 05. Nov. 2021

Accepted Manuscript
Differences in heart rate reserve of similar physical activitiesduring work and in leisure time – A study among Danish blue-collar workers
Pieter Coenen, Mette Korshøj, David M. Hallman, Maaike A.Huysmans, Allard J. van der Beek, Leon M. Straker, AndreasHoltermann
PII: S0031-9384(18)30017-9DOI: doi:10.1016/j.physbeh.2018.01.011Reference: PHB 12042
To appear in: Physiology & Behavior
Received date: 3 October 2017Revised date: 27 December 2017Accepted date: 12 January 2018
Please cite this article as: Pieter Coenen, Mette Korshøj, David M. Hallman, Maaike A.Huysmans, Allard J. van der Beek, Leon M. Straker, Andreas Holtermann , Differencesin heart rate reserve of similar physical activities during work and in leisure time – Astudy among Danish blue-collar workers. The address for the corresponding author wascaptured as affiliation for all authors. Please check if appropriate. Phb(2018), doi:10.1016/j.physbeh.2018.01.011
This is a PDF file of an unedited manuscript that has been accepted for publication. Asa service to our customers we are providing this early version of the manuscript. Themanuscript will undergo copyediting, typesetting, and review of the resulting proof beforeit is published in its final form. Please note that during the production process errors maybe discovered which could affect the content, and all legal disclaimers that apply to thejournal pertain.

ACC
EPTE
D M
ANU
SCR
IPT
Differences in heart rate reserve of similar physical activities during work and in leisure time – A study among Danish blue-collar workers
Pieter Coenen1,2, Mette Korshøj3, David M Hallman4, Maaike A Huysmans2, Allard J van der Beek2, Leon M Straker1, Andreas Holtermann3,5
1 School of Physiotherapy and Exercise Science, Curtin University, Perth Australia 2 Department of Public and Occupational Health, Amsterdam Public Health research
institute, VU University Medical Center, Amsterdam, The Netherlands 3 National Research Centre for the Working Environment, Copenhagen, Denmark
4 Department of Occupational and Public Health Sciences, Centre for Musculoskeletal Research, University of Gävle, Gävle, Sweden
5 Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark
Corresponding author Dr Pieter Coenen Department of Public and Occupational Health Amsterdam Public Health research institute, VU University Medical Center (VUmc) van der Boechorststraat 7, 1081 BT, Amsterdam, The Netherlands Phone: +31 20 444 5511 Fax: +31 20 444 8387 Email: [email protected]
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Abstract Recent studies suggest that while leisure-time physical activity (LTPA) promotes general health, engaging in occupational physical activity (OPA) may have negative health consequences. It has been hypothesized that the different health effects from OPA and LTPA can be explained by differences in physical activity (PA) intensity in these two domains. To assess the intensity of OPA and LTPA, we aimed to study the percentage heart rate reserve (%HRR) during similar types of OPA and LTPA during workdays Data from the NOMAD study on Danish blue-collar workers (n=124) with objective measurements of PA (using accelerometers) and heart rate (using heart rate monitors) for 4 workdays were analysed. Activities of sitting, standing, moving, walking, and stair climbing were identified and %HRR in each of these activities was determined for work and leisure. %HRR was significantly higher during OPA than LTPA. These differences were more pronounced in men than in women. Although not statistically significant in the fully adjusted model, we found indications that these differences were more pronounced in those with low compared to high fitness. To our knowledge, this is the first study with objective measurements showing that %HRR is higher during the same gross-body postural activities when performed at work compared to leisure-time during workdays. This elevated intensity may help explaining the negative health consequences of engagement in high levels of OPA. Future guidelines should distinguish OPA from LTPA, possibly by advising workers to remain active during their leisure time, in particular when they are highly active at work. Keywords: Physical activity – Heart rate reserve – Blue-collar workers – Accelerometry – Occupational physical activity – Leisure-time physical activity
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
1. Introduction Physical activity (PA) is considered to play an important role in the prevention of various adverse health outcomes, including cardio-vascular diseases, type-2 diabetes and cancer (Lee et al., 2012). However, recent studies have shown that while leisure-time PA (LTPA) promotes health, occupational PA (OPA) may have negative health consequences (Krause, 2010). Workers engaged in high levels of OPA are shown to have a higher risk of long-term sickness absence (Holtermann et al., 2012), cardio-vascular disorders (Li et al., 2013) and early mortality (Harari et al., 2015; Richard et al., 2015). Hence, there appears to be a PA health paradox. It has been shown that this paradox is more prominent in men than in women (Hu et al., 2014), and in those with low fitness compared to high fitness (Holtermann et al., 2016).
An explanation for the PA health paradox may be differences in the intensity of similar activities in OPA and LTPA (Hallman et al., 2015). LTPA, on the one hand, typically takes place in short high-intensity bouts of sufficient intensity to improve cardiorespiratory fitness and dispersed across the week to allow for recovery. OPA, on the other hand, often consists of different tasks, such as repetitive work and prolonged static postures, executed over long durations (e.g., 40 hours per week) to meet job demands. If such tasks are performed at a high aerobic intensity for many hours, it is presumed this will lead to chronic elevated heart rate and blood pressure (Korshøj et al., 2016), causing increased arterial wall stress (Krause et al., 2009) that may ultimately result in cardio-vascular disorders (He and Whelton, 1999; Krause et al., 2007). Accordingly, the International Labour Organization has recommended the average intensity of OPA over an 8-hour workday to be less than one-third of the maximal intensity (Bonjer and Parmeggiana, 1971). Additionally, activities which are apparently the same during work and leisure time, such as sitting, standing or walking, may be performed at a different intensity in the occupational compared with the leisure context.
However, differences in relative intensity of OPA and LTPA from objective measurements have not been described yet. Although absolute values of PA intensity have been used to compare whole day intensity levels of OPA and LTPA (Gram et al., 2016), a way to assess relative intensity of PA is by measuring the percentage heart rate reserve (%HRR). %HRR is expressed as a percentage of a person’s range in heart rate (Karvonen and Vuorimaa, 1988), considering their maximal heart rate (which is dependent on age (Tanaka et al., 2001)) and resting heart rate (dependent on cardiorespiratory fitness (Mackinnon et al., 2003)). As there is a linear relationship between %HRR and oxygen consumption (Karvonen and Vuorimaa, 1988), %HRR is closely related to PA intensity (Wu and Wang, 2002). As compared to oxygen consumption, HRR is relatively feasible to measure in a field-based situation without putting a burden on participants. %HRR is an established and valid physiological metric, depicting a balance between a person’s demand and capacity (Ilmarinen, 1992), which allows for a good comparisons between participants and has previously been used in the occupational context (Korshøj et al., 2013).
We aimed to 1) examine the difference in %HRR between the same activities performed during occupational time and leisure time on workdays and 2) assess whether possible differences in %HRR between OPA and LTPA depend on sex and level of cardiorespiratory fitness. We will address these issues by analysing objectively measured PA and heart rate from a sample of Danish blue-collar workers.
2. Material and methods 2.1 Study population and design In this study, we analysed data from the Danish cross-sectional ‘New method for Objective Measurements of physical Activity in Daily living’ (NOMAD) study, which has been described in more detail before (Gupta et al., 2015). In short, workers were recruited from seven
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
workplaces that were selected based on their variation in PA representing different types of blue-collar workers, thereby maintaining homogeneity in socioeconomic status. Invited workers completed a screening questionnaire, after which workers were included if they
wished to participate, worked 20 hours per week, were between 18 and 65 years of age, and provided a signed informed consent. White-collar workers, pregnant women and those with fever and/or skin allergy to adhesive tape used for mounting objective measurement devices were excluded. Out of 391 workers invited to participate in the NOMAD study, 259 (66%) blue-collar workers agreed to participate. These workers completed a detailed computer-based questionnaire and took part in anthropometric and cardiorespiratory fitness measurements. These workers were also asked to participate in a protocol of objective measurements (with accelerometry and heart rate monitoring) that took place over the course of four workdays in which a total of 188 (48%) workers participated.
The NOMAD study was approved by the Ethics Committee for the Capital Region of Denmark (journal number H-2–2011–047) and conducted in accordance with the Helsinki declaration. Informed consent was obtained from all participants included in the study. 2.2 Measurements 2.2.1 Objective measurement protocol On the first day of the objective measurement protocol, workers were mounted with ambulatory PA and heart rate monitors and were asked to wear these devices continuously (day and night) for four consecutive days. These periods were to cover at least two full workdays, including occupational and leisure-time periods. Workers were instructed to take off the devices if they caused any kind of discomfort (e.g., itching or sleep disturbance) and were asked to keep a diary regarding their working, leisure, sleep and non-wear hours. In PA research, also the domain of transport has frequently been addressed (Owen et al., 2011). However to consider the burden on the participants of filling out diaries, this domain has not been assessed in this study. We thus only focus on work and non-work (from this point onwards: leisure time) awake time. Here, work was defined as the self-reported hours spent at the primary occupation and leisure-time as the remaining waking hours. 2.2.2 Physical activity PA was assessed using two accelerometers (Actigraph GT3X+, Actigraph LLC, Pensacola, USA) that were worn at the level of the thigh (at the front of the right thigh, midway between the illiac crest and patella) and trunk (at processus spinosus at the level of T1– T2) (Skotte et al., 2014). Accelerometers were secured to the skin using tape (3M, Hair-Set, double-sided adhesive tape, and Fixomull, BSN medical). The accelerometers measure tri-axial acceleration with a frequency of 30 Hz, a dynamic range of ±6G (with 1G being 9.81m/s2) and a precision of 12 bit. According to the manufacturer no recalibration of the devices is required. In order to test this, we developed an apparatus in which the accelerometers could continually be turned 360° so they were exposed to gravitational forces ranging from -1G to +1G. A test, using 200 Actigraph units showed an average (SD) of 1.8(1.5)% deviation from ±1G, for all three axes. Initialization of the devices and downloading of the data was done using the manufacturer’s software (Actilife Software version 5.5, ActiGraph LLC, Pensacola) while further analyses were conducted using custom-made MATLAB based software, Acti4 (The National Research Centre for the Working Environment, Copenhagen, Denmark and Federal Institute for Occupational Safety and Health, Berlin, Germany). This program allowed for estimation of different types of PA with high sensitivity and specificity (Skotte et al., 2014). In this procedure, the trunk accelerometer was used to assess trunk inclination which allows for more accurate distinction between the various activities (Korshøj et al., 2014). To do so, reference measurements (i.e., daily standing in an upright position for 15 seconds) were used to obtain the coordinate transformation between the
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
axis of the accelerometers and the orientation of the thigh and trunk. Data processing was performed according to an established protocol, which has
been shown to have excellent sensitivity and specificity for identifying activities from accelerometer-based data (Skotte et al., 2014). All non-workdays, sleep or bedtime periods, and non-wear periods were discarded. Besides non-wear periods reported by the workers, all periods >90 minutes in which the accelerometer entered the standby status because of no movements, were marked as non-wear periods by the Acti4 software. Here, standby status was detected by the mean of the standard deviation for the three axes <0.01G. Periods 10-90 minutes without accelerometer movements were also marked as non-wear periods if the position of the accelerometer matched a horizontal orientation (indicating that the accelerometer was lying flat on a table) and SDx+SDy+SDz<0.5G for any second during a 5-second interval immediately before the period without movement (using raw, unfiltered data).
Visual inspection completed the quality checking of the recordings. For the remaining measurement periods, the exact beginning and end of the following activities (depicting common activities occurring both during work and leisure-time) at work and during leisure-time were identified: sitting, standing, moving (being the transition phase between standing and walking), walking and stair climbing (Skotte et al., 2014). Other activities such as lying, running, cycling and rowing were also outputted using this software (see Supplementary Material 1), however those activities were chosen not to be used for further analyses due to their limited occurrence in either domain (i.e., work or leisure time). Identification of all activities was solely based on readings of the thigh- and trunk-worn accelerometer (Skotte et al., 2014), which includes only gross-body postures without considering any other (e.g., upper limb) movement. 2.2.3 Heart rate reserve Actiheart (CamNtech Ltd., Cambridge, UK) worn on the chest, consisting of two electrodes connected by a short lead, attached to the skin by two standard electrocardiography (ECG) pads (Ambu©, Blue sensor VL-00-S/25), was used to determine heart rate by measuring inter-beat intervals. After preparation of the skin (i.e., cleaning with ethanol solution), the ECG electrodes were placed on the chest at one of the two standardized positions (Brage et al., 2006). The Actiheart devices were set to record in the short term mode, capable to record inter-beat intervals for up to 440,000 heartbeats. After data collection, the inter-beat intervals were downloaded by the Actiheart software and read into the aforementioned custom-made Acti4 software for error checking and processing, according to an earlier described protocol (Kristiansen et al., 2011). Inter-beat intervals were considered erroneous and were discarded from further analysis if they corresponded to a heart rate <36 or >200 beats per minute, or if they deviated >15% compared to the neighbouring inter-beat intervals. Moreover, measurement periods with a resulting error rate >50% were discarded. For the rest of the measurements periods, the inter-beat series were resampled with a frequency of 4 Hz using a linear interpolation scheme. The resampled and interpolated series were then used for calculation of heart rate values. Heart rate reserve (%HRR) was defined according to the earlier described equation (Karvonen et al., 1957):
%HRR = (HRHRwork/leisure-time−HRHRmin) / (HRHRmax−HRHRmin) × 100
for which HRmin is the minimum heart rate of an average of ten heart beats throughout all measurement periods (including sleep time) and maximal heart rate (HRmax) was estimated according to an equation by Tanaka and colleagues (2001):
HRmax = 208 − 0.7 × age
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
2.2.4 Covariates Workers self-reported their sex while the worker’s age was determined from the Danish civil registration records. Smoking behaviour was obtained from the question: “Do you smoke?” with response categories summarized into: yes (yes, daily; yes, sometimes) and no (used to smoke; I have never smoked). Alcohol use was determined by asking workers about their weekly consumption of alcoholic beverages (expressed in number of consumptions – which due to the differences in alcohol percentage of various consumptions may have an inferior between- and within-participant comparability than the number of alcoholic units consumed).
Worker’s influence at work (decision latitude) was assessed using a 4-item scale from the Copenhagen Psychosocial Questionnaire (Pejtersen et al., 2010). Responses were scored on a 5-point Likert scale, while compositional scores (normalized to a scale ranging from 0 to 100) were calculated, with higher scores representing a higher degree of influence at work. Time spent carrying and lifting at work was self-reported with outcome categories summarized into: high (almost all the time, approximately 3/4 of the time and 1/2 of the time), moderate (1/4 of the time) and low (rarely/very little and never). Moreover, heart and/or lung medication use (yes/no) was self-reported.
Anthropometric measurements of worker’s body height and weight were performed with standardised methods and their body mass index (BMI, kg/m2) was calculated. Workers’ cardiorespiratory fitness was estimated using a one point Åstrand sub-maximal bicycle ergometer test (Åstrand, 1956), which is generally shown to be a valid (Cink and Thomas, 1981) and feasible test to be performed among blue-collar workers at the work site (Gram et al., 2012). After two minutes of warm-up cycling, the resistance was increased to elicit a steady heart rate of ≥60% of HRmax (Tanaka et al., 2001) based on age and self-reported fitness. Workers were instructed to maintain a 60 cycles/minute cadence throughout. Heart rate was recorded continuously and the age- and sex-corrected cardiorespiratory fitness (in mlO2/min/kg) was estimated by the Åstrand nomogram, based on heart rate and corresponding workload. Cardiorespiratory fitness was subsequently dichotomised (into low and high) using established threshold values (Shvartz and Reibold, 1990). 2.3 Data analysis For the current analysis, workers with at least one valid day of PA and heart rate measurement were included. For the PA measurements, a valid workday consisted of either ≥4 measured hours of work time or ≥75% of the individual’s average reported work time. A valid leisure-time day was defined as ≥4 measured hours of leisure-time or ≥75% of the individual’s average reported leisure-time. For heart rate measurements, a valid day was defined as ≥4 hours/day of work time and a total of ≥7 hours during all recorded working periods (work and leisure-time activities combined). The reason for choosing these criteria was to prevent bias due to inclusion of extreme unrepresentative data and to reflect optimal daily wear time . Sleep time was not considered in the present analysis.
For each of the activities (i.e., sitting, standing, moving, walking and stair climbing; at work and during leisure-time) average %HRR was calculated and were tabulated. Average %HRR (averaged over all activities) and weighted average %HRR (averaged over all activities and weighted by the measurement duration in each of the activities) at work and during leisure-time were estimated. Differences in %HRR between activities at work and during leisure-time were tested using linear mixed-models with random intercepts for individual participants, using domain (occupational vs. leisure-time, within-participants) as a categorical independent variable and %HRR as continuous dependent variable. Two additional regression models were applied to test whether potential differences in %HRR
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
between OPA and LTPA depended on sex or fitness, respectively. In these regression models, the interaction effect of domain*sex and domain*cardiorespiratory fitness were tested, respectively. In these analyses, interaction as well as main effect of the respective variables were modelled.
Differences between domains (occupational vs leisure-time) as well as the interaction effect were expressed by regression coefficients (beta) with 95% confidence interval (95% CI). P-values <0.05 were considered statistically significant (2-sided) and all statistical procedures were performed using Stata (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, USA). For each of the aforementioned models, unadjusted and fully adjusted models (adjusting for the continuous variables age, BMI, alcohol consumption and influence at work and categorical variables sex, carrying/lifting at work, smoking and heart/lung medication use) were estimated. As the total measurement duration of each of the activities may impact the outcomes of the studied models, sensitivity analyses were performed in which models were additionally adjusted for measurement duration.
3. Results Of the 188 eligible workers that took part in the protocol with objectively measurements of PA and heart rate, 124 workers had sufficient valid data on PA and %HRR. This group of workers was on average (mean (standard deviation)) 46.6(9.12) years of age and 61(49%) of them were female (Table 1). Total time of PA and %HRR measurements was 33.3(11.6) hours, measured over 2.0(0.7) workdays on average; 16.5(2.1) hours/workday, of which 8.6(2.0) hours/day were at work and 7.9(2.3) hours/day were during leisure-time.
%HRR in each of the activities during work and leisure during workdays are presented in Figure 1 and Table 2, showing a generally higher %HRR during gross-body postural activities at work than during the same activities in leisure-time (unadjusted beta with 95% CI: -2.0 [-2.5 -1.5], p<0.001). This reflects a difference in %HRR during OPA (33.4(7.3)) compared to during LTPA (31.4(5.7)). Differences between %HRR during OPA and LTPA were somewhat larger when weighted averages were taken (30.2 and 25.9 %HRR, respectively) and did not change substantially when those weighted averages included other activities that were excluded from the statistical analysis (30.1 and 25.3 %HRR, respectively; Supplementary Material 1). A significant between domain difference remained when adjusting for age, sex, BMI, alcohol consumption, smoking, heart/lung medication use, influence at work and carrying/lifting at work (beta with 95% CI: -1.9 [-2.4 -1.4], p<0.001).
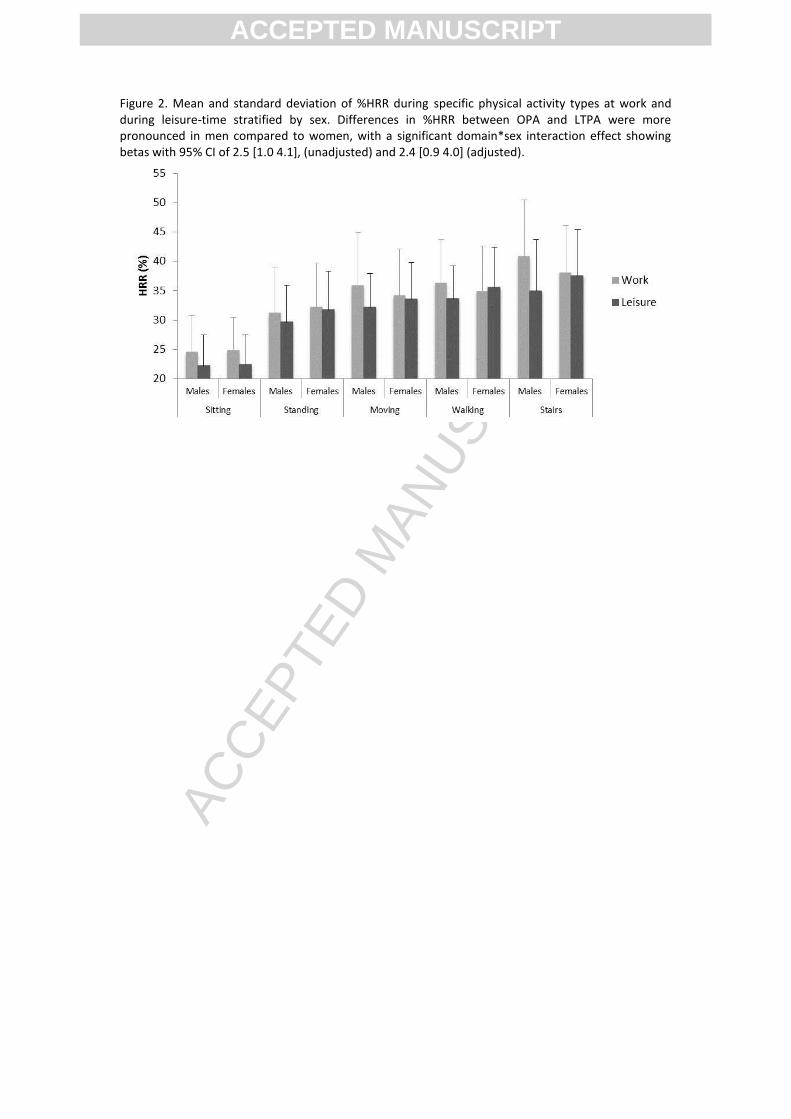
Differences in %HRR between OPA and LTPA were more pronounced in men compared to women (Figure 2), with a significant domain*sex interaction effect (2.5 [1.0 4.1], p=0.001), that remained when adjusting for aforementioned confounders (2.4 [0.9 4.0], p<0.002). Differences in %HRR between OPA and LTPA also depended on the cardiorespiratory fitness of workers. While %HRR appears to be lower in workers with a higher cardiorespiratory fitness, more pronounced differences between OPA and LTPA were observed in those with low compared to those with high cardiorespiratory fitness. This was expressed with a (non-significant) unadjusted domain*fitness interaction effect (1.43 [-0.50 3.36], p=0.147; Figure 3), and a somewhat stronger and statistically significant interaction effect when adjusting for aforementioned relevant confounders 1.91 [0.33 3.48], 0.018). Sensitivity analyses additionally adjusted for total measurement duration did not lead to substantially different outcomes, both for main and interaction effects (data not reported).
4. Discussion This study was the first to use objective measurements to assess differences in %HRR of similar physical activities at work and during leisure-time on workdays. Our results showed that in Danish blue-collar workers, %HRR was higher in activities at work compared to when
ACCEPTED MANUSCRIPT
ACC
EPTE
D M
ANU
SCR
IPT
performing the same gross-body postural activities during leisure-time, suggesting that on workdays OPA is performed with a higher intensity compared to LTPA. Workers operating on high OPA intensities are known to have elevated resting blood pressure (Clays et al., 2012) and heart rate (Jakobsen et al., 2014), that may ultimately lead to cardio-vascular disorders (Krause et al., 2007) and early mortality (Harari et al., 2015; Richard et al., 2015). This potentially straining higher intensity of OPA suggests interventions aiming for a healthy active lifestyle, modification of work tasks so that they promote health and capacity (Straker et al., 2017), as well as PA guidelines ought to distinguish between OPA and LTPA. Since we only assessed workdays in our study, these findings can not necessarily be extrapolated to non-workdays, and thus to total LTPA. Apart from developing guidelines and interventions, another possibility is the development of employment standards, stipulating the necessary attributes to work in a particular job (Tipton et al., 2013).
An explanation for the elevated intensity of OPA compared to LTPA may be that activities at work require a certain productivity level with tasks executed at an elevated pace. This may be associated with additional occupational demands that have not been fully captured by our adjustment for self-reported carrying/lifting and influence at work. For example, compared to gross-body postures of activities during leisure time, similar activities at work can be accompanied with certain movement or postures of other (e.g., upper limb) body parts increasing the intensity of OPA. For instance, occupational lifting and manual handling can put additional stress on the cardiovascular system (van der Molen et al., 2008). Apart from physical demands at work, mental stressors can additionally increase heart rate (Johnston et al., 2016; Taelman et al., 2011) as well as blood pressure (Hjortskov et al., 2004). Such mental stressors can, for example, be a results of high mental demands in combination with limited rewards or control over these demands (Karasek, 1979; Siegrist, 1996). It can thus be concluded that OPA may be associated with additional physical and/or mental demands, which could (partly) explain the higher intensity levels during OPA. A limitation of the current study is that no such physical and/or mental demands were measured. To gain a better understanding of the current findings, future research can focus on such measurements, for example by additionally measuring trunk and/or upper extremity movement (using accelerometers or other motion capturing systems), while also measuring mental work demands.
It remains to be determined to what extent the elevated intensity of OPA, shown in our study, may have negative health consequences. Recommended thresholds for OPA intensity (including those from the International Labour Organisation) during a 8-hour workday vary from 30% (Bonjer and Parmeggiana, 1971) to 33% (Ilmarinen, 1992) and 30-35% (Jørgensen, 1985). Although intensity of LTPA is also relatively high in our study, with an average %HHR at work above 30%, it is expected that OPA may lead to negative health consequences, as intensity reaches levels well beyond this threshold. Moreover, our conclusion is strengthened by the fact that activities of standing, moving, walking and stair climbing are performed for longer duration of time at work than during leisure-time (Table 2). This means that the exposure is sustained for longer duration, resulting in even higher cumulative exposure differences between OPA and LTPA. The latter can be seen in the weighted (by measurement duration) %HRR values presented in Table 2. Moreover, averages were not affected by the intensity of those activities that were not considered in the statistical analysis of this study (i.e., lying, running, cycling and rowing). However, duration of time spent in certain activities may differ when also considering non-workdays, as it is for example known that workers may spend more time on LTPA during non-workdays compared to workdays (Thorp et al., 2012).
Future work should elaborate on temporal patterns of OPA and LTPA intensity, for example studying the amount of time above a certain intensity level or the bout duration of activities, in order to get a better understanding of the differences between OPA and LTPA.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Earlier work has shown that OPA and LTPA differ in their temporal patterns. For example, OPA is, compared to LTPA, characterised by a higher occurrence of short bouts of standing and walking (Hallman et al., 2015). Such differences in characteristics of OPA and LTPA can at least partly explain the intensity differences found in this study and can provide more insight into the health consequences of both activities, in particular the possible negative health consequences of OPA. It should however be acknowledged that the health consequences of high intensity OPA may depend on several factors such as duration, activity types performed, time-pattern and individual characteristics. Thus, high intensity OPA is not necessarily harmful, but could also be beneficial for health, depending on these factors. For example, sitting is known to be an independent risk factor for ill-health (Straker et al., 2016). As such, increasing workers’ activity intensity during occupational sitting (which is substantially lower than the 30% threshold) may have positive health effects among sedentary workers or may protect workers from the negative health consequences of strenuous OPA. Similarly, worksite activities have been shown to be beneficial for certain other adverse health outcomes, such as musculoskeletal symptoms (Moreira-Silva et al., 2016).
Differences in %HRR between PA at work and leisure-time were more pronounced in men than in women. As can be seen in Figure 2, women’s leisure-time activities are higher in intensity than those of men. Moreover, our findings suggest that men are more prone than women to higher PA intensity at work. An explanation for the latter can be the apparent differences in work content between male and female workers (Hallman et al., 2015), with men being employed in different (more physically demanding) occupations. However, males and females are not evenly distributed among occupations (which is also the case in our study), making a direct comparison between males and females difficult. Nevertheless, our findings are in line with earlier research showing men to have a higher risk for high levels of OPA than women (Hu et al., 2014).
Differences in %HRR between PA at work and leisure-time seemed to be more pronounced in workers with low fitness compared to those with high cardiorespiratory fitness (although not statistically significant in the unadjusted model). As can be seen in Figure 3, PA is relatively high for workers with low cardiorespiratory fitness, both at work and during leisure-time. This suggests that workers with a relatively low fitness operate their daily activities (both work and leisure) at a higher capacity than those who are fitter (Karlqvist et al., 2003). The larger differences in intensity of OPA and LTPA in those with low compared to those with high levels of fitness are in line with earlier research indicating the PA health paradox to be more prominent in workers with low fitness (Holtermann et al., 2016). It should however be noted that, although our calculation of HRR (which comprises of the age-adjusted HRmax) takes the age of participants into consideration, fitness was lower in the older age groups. Mean (SD) fitness was 28.2(6.0) mlO2/min/kg in those >44 years old compared to 36.7(9.7) and 39.3(5.9) mlO2/min/kg for those 30-44 and <30 years of age, respectively. It can therefore not be excluded that fitness, to some extent, is affected by age. Nevertheless, these findings underline the importance of a good cardiorespiratory fitness among blue-collar workers. A good level of fitness could possibly be achieved by advising workers to remain active during their leisure time, in particular those who are highly active at work. This advice, remains, however controversial, since a recent study showed that LTPA did not protect worker with high OPA from all-cause mortality (Krause et al., 2017), while another study showed an increased risk of coronary heart disease among those who were highly active during leisure-time while also being active at work (Clays et al., 2013). When knowledge is further developed, guidelines, interventions and employment standards can be developed to create healthy and sustainable systems of work for all. Our research suggests that such initiatives should take inter-individual factors including sex, age and fitness into consideration.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
4.1 Methodological considerations As far as we are aware, this is the first study to objectively measure differences in intensity (through %HRR) of OPA and LTPA. Such objective measurements are more reliable and valid than those from self-reports (Gupta et al., 2016; Kwak et al., 2011), as a result of which our study provides an accurate overview of intensity of OPA and LTPA. Objective measures furthermore allow for even more detailed assessments of PA (e.g., measuring bout duration or variation in intensity), which can be the focus of further research. Despite the use of objective measurements for PA, HRR and cardiorespiratory fitness, HRmax was estimated based on participant’s age. These estimates were used in further calculations of %HRR and cardiorespiratory fitness, which may reduce their accuracy. This assessment may, due to their relatively low cardiorespiratory fitness, overestimate the HRmax of a sample of blue collar workers.
A limitation of the current study is that only workdays were considered. Although this allowed us to make a good comparison of similar activities in LTPA and OPA during workdays, it is yet unknown to what extent these differences vary from those of non-workdays. Comparisons of PA in work and non-workdays have been performed before in workers from various occupations (Parry and Straker, 2013; Thorp et al., 2012), showing substantial differences between workdays and non-workdays. For example, it was shown that some workers tend to be more physically active during leisure-time on non-workdays compared to workdays. Secondly, in the current study, PA during leisure time (including transportation) and at work was considered. Therefore, the domain of transportation (as often described in literature) has not been individually addressed. Another limitation of the present study is that objective measurements were conducted for up to four days only. This could hamper the reliability of the estimation of PA and HRR, since it has been shown that variation in activities between days may occur (Svendsen et al., 2005). Finally, as our study fails to provide information on temporal patterns of OPA and LTPA intensity, such patterns (e.g., by assessing the amount of time above a certain intensity level or the bout duration of activities) should be studied in future research.
Apart from the aforementioned physiological implications of our study findings, the current results also bear methodological implications. The fact that intensity of comparable activities differs by domain (work vs leisure-time), sex and cardiorespiratory fitness suggests that only relying on accelerometer measurements for the assessment of PA may provide only limited information on the nature of PA. Future studies should therefore consider combining measurement of accelerometry with those of physiological outcomes (e.g., heart rate), to get more detailed PA information.
We only included blue-collar workers, as a result of which our findings cannot be generalised to other populations, including those from white-collar occupations. However, the advantage of this methodology is that the relatively homogeneous population that was studied reduces the risk of potential socio-economic biases to the presented findings. Moreover, the findings presented in this study are based on a relatively small sample, in particular for the analysis for cardiorespiratory fitness sample size is low, for which it is known that those who did not take the fitness tests were mainly participants with musculoskeletal symptoms and/or elevated blood pressure. Nevertheless, for most of the studied associations, strong and significant effect sizes were found while results appear to be robust when adjusting for confounders.
5. Conclusions This study is the first to use objective measurements to study differences in %HRR for OPA and LTPA during workdays, showing higher intensity of similar activities at work compared to during leisure-time. This higher intensity of OPA suggests that there may indeed be
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
negative health consequences for engagement in high levels of OPA. Although this phenomenon should be better understood, our findings suggest that interventions for a healthy active working lifestyle as well as PA guidelines ought to distinguish between OPA and LTPA and particularly target male populations (with high levels of OPA) and those with low cardiorespiratory fitness. Possibly, such guidelines can advise workers to remain active during their leisure time, in particular when they are highly active at work. Acknowledgements This study was conducted with the financial support from Federal Institute for Occupational Safety and Health (BAuA), Berlin, Germany and The National Research Centre for the Working Environment (NRCWE), Copenhagen, Denmark. We would also like to thank our colleagues from The National Research Centre for the Working Environment (NRCWE), Copenhagen, Denmark for contribution to data collection, data analyses and management. Declaration of interests There were no conflicts of interest reported by the authors Compliance with ethical standards There were no conflicts of interest reported by the authors. This research involves human participants, who provided their written informed consent to participate in the study. References Åstrand, P.O., 1956. Human physical fitness with special reference to sex and age. Physiol
Rev 36, 307–335. Bonjer, F.H., Parmeggiana, L., 1971. Encyclopedia of Occupational Health and Safety.
International Labour Organisation, Geneva, Switzerland. Brage, S., Brage, N., Ekelund, U., Luan, J., Franks, P.W., Froberg, K., Wareham, N.J., 2006.
Effect of combined movement and heart rate monitor placement on physical activity estimates during treadmill locomotion and free-living. Eur J Appl Physiol 96, 517-524.
Cink, R.E., Thomas, T.R., 1981. Validity of the Astrand-Ryhming nomogram for predicting maximal oxygen intake. Br J Sports Med 15, 182-185.
Clays, E., De Bacquer, D., Janssens, H., De Clercq, B., Casini, A., Braeckman, L., Kittel, F., De Backer, G., Holtermann, A., 2013. The association between leisure time physical activity and coronary heart disease among men with different physical work demands: a prospective cohort study. Eur J Epidemiol 28, 241-247.
Clays, E., De Bacquer, D., Van Herck, K., De Backer, G., Kittel, F., Holtermann, A., 2012. Occupational and leisure time physical activity in contrasting relation to ambulatory blood pressure. BMC Public Health 12, 1002.
Gram, B., Holtermann, A., Bultmann, U., Sjøgaard, G., Søgaard, K., 2012. Does an exercise intervention improving aerobic capacity among construction workers also improve musculoskeletal pain, work ability, productivity, perceived physical exertion, and sick leave? A randomized controlled trial. J Occup Environ Med 54, 1520-1526.
Gram, B., Westgate, K., Karstad, K., Holtermann, A., Søgaard, K., Brage, S., Sjøgaard, G., 2016. Occupational and leisure-time physical activity and workload among construction workers - a randomized control study. Int J Occup Environ Health 22, 36-44.
Gupta, N., Christiansen, C.S., Hallman, D.M., Korshøj, M., Carneiro, I.G., Holtermann, A., 2015. Is objectively measured sitting time associated with low back pain? A cross-sectional investigation in the NOMAD study. PLoS One 10, e0121159.
Gupta, N., Heiden, M., Mathiassen, S.E., Holtermann, A., 2016. Prediction of objectively measured physical activity and sedentariness among blue-collar workers using survey questionnaires. Scand J Work Environ Health 42, 237-245.
ACCEPTED MANUSCRIPT
ACC
EPTE
D M
ANU
SCR
IPT
Hallman, D.M., Mathiassen, S.E., Gupta, N., Korshøj, M., Holtermann, A., 2015. Differences between work and leisure in temporal patterns of objectively measured physical activity among blue-collar workers. BMC Public Health 15, 976.
Harari, G., Green, M.S., Zelber-Sagi, S., 2015. Combined association of occupational and leisure-time physical activity with all-cause and coronary heart disease mortality among a cohort of men followed-up for 22 years. Occup Environ Med 72, 617-624.
He, J., Whelton, P.K., 1999. Elevated systolic blood pressure and risk of cardiovascular and renal disease: overview of evidence from observational epidemiologic studies and randomized controlled trials. Am Heart J 138, 211-219.
Hjortskov, N., Rissen, D., Blangsted, A.K., Fallentin, N., Lundberg, U., Søgaard, K., 2004. The effect of mental stress on heart rate variability and blood pressure during computer work. Eur J Appl Physiol 92, 84-89.
Holtermann, A., Hansen, J.V., Burr, H., Søgaard, K., Sjøgaard, G., 2012. The health paradox of occupational and leisure-time physical activity. Br J Sports Med 46, 291-295.
Holtermann, A., Marott, J.L., Gyntelberg, F., Søgaard, K., Mortensen, O.S., Prescott, E., Schnohr, P., 2016. Self-reported occupational physical activity and cardiorespiratory fitness: Importance for cardiovascular disease and all-cause mortality. Scand J Work Environ Health 42, 291-298.
Hu, G.C., Chien, K.L., Hsieh, S.F., Chen, C.Y., Tsai, W.H., Su, T.C., 2014. Occupational versus leisure-time physical activity in reducing cardiovascular risks and mortality among ethnic Chinese adults in Taiwan. Asia Pac J Public Health 26, 604-613.
Ilmarinen, J., 1992. Job design for the aged with regard to decline in their maximal aerobic capacity: Part I - Guidelines for the practitioner. Int J Ind Ergonom 10, 53-63.
Jakobsen, M.D., Sundstrup, E., Persson, R., Andersen, C.H., Andersen, L.L., 2014. Is Borg's perceived exertion scale a useful indicator of muscular and cardiovascular load in blue-collar workers with lifting tasks? A cross-sectional workplace study. Eur J Appl Physiol 114, 425-434.
Johnston, D., Bell, C., Jones, M., Farquharson, B., Allan, J., Schofield, P., Ricketts, I., Johnston, M., 2016. Stressors, Appraisal of Stressors, Experienced Stress and Cardiac Response: A Real-Time, Real-Life Investigation of Work Stress in Nurses. Ann Behav Med 50, 187-197.
Jørgensen, K., 1985. Permissible loads based on energy expenditure measurements. Ergonomics 28, 365-369.
Karasek, R.A., 1979. Job demands, job decision latitude, and mental strain: implications for job redesign. Admin Sci Q 24, 285-308.
Karlqvist, L., Leijon, O., Harenstam, A., 2003. Physical demands in working life and individual physical capacity. Eur J Appl Physiol 89, 536-547.
Karvonen, J., Vuorimaa, T., 1988. Heart rate and exercise intensity during sports activities. Practical application. Sports Med 5, 303-311.
Karvonen, M.J., Kentala, E., Mustala, O., 1957. The effects of training on heart rate; a longitudinal study. Ann Med Exp Biol Fenn 35, 307–315.
Korshøj, M., Clays, E., Lidegaard, M., Skotte, J.H., Holtermann, A., Krustrup, P., Søgaard, K., 2016. Is aerobic workload positively related to ambulatory blood pressure? A cross-sectional field study among cleaners. Eur J Appl Physiol 116, 145-152.
Korshøj, M., Krustrup, P., Jespersen, T., Søgaard, K., Skotte, J.H., Holtermann, A., 2013. A 24-h assessment of physical activity and cardio-respiratory fitness among female hospital cleaners: a pilot study. Ergonomics 56, 935-943.
Korshøj, M., Skotte, J.H., Christiansen, C.S., Mortensen, P., Kristiansen, J., Hanisch, C., Ingebrigtsen, J., Holtermann, A., 2014. Validity of the Acti4 software using ActiGraph GT3X+accelerometer for recording of arm and upper body inclination in simulated work tasks. Ergonomics 57, 247-253.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Krause, N., 2010. Physical activity and cardiovascular mortality--disentangling the roles of work, fitness, and leisure. Scand J Work Environ Health 36, 349-355.
Krause, N., Arah, O.A., Kauhanen, J., 2017. Physical activity and 22-year all-cause and coronary heart disease mortality. Am J Ind Med 60, 976-990.
Krause, N., Brand, R.J., Kaplan, G.A., Kauhanen, J., Malla, S., Tuomainen, T.P., Salonen, J.T., 2007. Occupational physical activity, energy expenditure and 11-year progression of carotid atherosclerosis. Scand J Work Environ Health 33, 405-424.
Krause, N., Brand, R.J., Kauhanen, J., Kaplan, G.A., Syme, S.L., Wong, C.C., Salonen, J.T., 2009. Work time and 11-year progression of carotid atherosclerosis in middle-aged Finnish men. Prev Chronic Dis 6, A13.
Kristiansen, J., Korshøj, M., Skotte, J.H., Jespersen, T., Søgaard, K., Mortensen, O.S., Holtermann, A., 2011. Comparison of two systems for long-term heart rate variability monitoring in free-living conditions--a pilot study. Biomed Eng Online 10, 27.
Kwak, L., Proper, K.I., Hagströmer, M., Sjöström, M., 2011. The repeatability and validity of questionnaires assessing occupational physical activity--a systematic review. Scand J Work Environ Health 37, 6-29.
Lee, I.M., Shiroma, E.J., Lobelo, F., Puska, P., Blair, S.N., Katzmarzyk, P.T., Lancet Physical Activity Series Working Group, 2012. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 380, 219-229.
Li, J., Loerbroks, A., Angerer, P., 2013. Physical activity and risk of cardiovascular disease: what does the new epidemiological evidence show? Curr Opin Cardiol 28, 575-583.
Mackinnon, L.T., Ritchie, C.B., Hooper, S., Abernethy, P., 2003. Exercise Management: Concepts and Professional Practice. Human Kinetics Champaign, USA.
Moreira-Silva, I., Teixeira, P.M., Santos, R., Abreu, S., Moreira, C., Mota, J., 2016. The effects of workplace physical activity programs on musculoskeletal pain: a systematic review and meta-analysis. Workplace Health Saf 64, 210-222.
Owen, N., Sugiyama, T., Eakin, E.E., Gardiner, P.A., Tremblay, M.S., Sallis, J.F., 2011. Adults' sedentary behavior determinants and interventions. Am J Prev Med 41, 189-196.
Parry, S., Straker, L., 2013. The contribution of office work to sedentary behaviour associated risk. BMC Public Health 13, 296.
Pejtersen, J.H., Kristensen, T.S., Borg, V., Bjorner, J.B., 2010. The second version of the Copenhagen Psychosocial Questionnaire. Scand J Public Health 38, S8-S24.
Richard, A., Martin, B., Wanner, M., Eichholzer, M., Rohrmann, S., 2015. Effects of leisure-time and occupational physical activity on total mortality risk in NHANES III according to sex, ethnicity, central obesity, and age. J Phys Act Health 12, 184-192.
Shvartz, E., Reibold, R.C., 1990. Aerobic fitness norms for males and females aged 6 to 75 years: a review. Aviat Space Environ Med 61, 3-11.
Siegrist, J., 1996. Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol 1, 27-41.
Skotte, J., Korshøj, M., Kristiansen, J., Hanisch, C., Holtermann, A., 2014. Detection of physical activity types using triaxial accelerometers. J Phys Act Health 11, 76-84.
Straker, L., Coenen, P., Dunstan, D.W., Gilson, N., Healy, G.N., 2016. Sedentary work - Evidence on an emergent work health and safety issue. Safe Work Australia, Canberra, Australia.
Straker, L., Mathiassen, S.E., Holtermann, A., 2017. The 'Goldilocks Principle': designing physical activity at work to be 'just right' for promoting health. Br J Sports Med 10.1136/bjsports-2017-097765.
Svendsen, S.W., Mathiassen, S.E., Bonde, J.P., 2005. Task based exposure assessment in ergonomic epidemiology: a study of upper arm elevation in the jobs of machinists, car mechanics, and house painters. Occup Environ Med 62, 18-27.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Taelman, J., Vandeput, S., Vlemincx, E., Spaepen, A., Van Huffel, S., 2011. Instantaneous changes in heart rate regulation due to mental load in simulated office work. Eur J Appl Physiol 111, 1497-1505.
Tanaka, H., Monahan, K.D., Seals, D.R., 2001. Age-predicted maximal heart rate revisited. J Am Coll Cardiol 37, 153-156.
Thorp, A.A., Healy, G.N., Winkler, E., Clark, B.K., Gardiner, P.A., Owen, N., Dunstan, D.W., 2012. Prolonged sedentary time and physical activity in workplace and non-work contexts: a cross-sectional study of office, customer service and call centre employees. Int J Behav Nutr Phys Act 9, 128.
Tipton, M.J., Milligan, G.S., Reilly, T.J., 2013. Physiological employment standards I. Occupational fitness standards: objectively subjective? Eur J Appl Physiol 113, 2435-2446.
van der Molen, H.F., Kuijer, P.P., Hopmans, P.P., Houweling, A.G., Faber, G.S., Hoozemans, M.J., Frings-Dresen, M.H., 2008. Effect of block weight on work demands and physical workload during masonry work. Ergonomics 51, 355-366.
Wu, H.C., Wang, M.J., 2002. Relationship between maximum acceptable work time and physical workload. Ergonomics 45, 280-289.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Figure 1. Mean and standard deviation of %HRR during specific physical activity types at work and during leisure-time. A generally higher %HRR during OPA than during the same activities in LTPA was found with betas with 95% CI of -2.0 [-2.5 -1.5] (unadjusted) and -1.9 [-2.4 -1.4] (adjusted).
ACCEPTED MANUSCRIPT
ACC
EPTE
D M
ANU
SCR
IPT
Figure 2. Mean and standard deviation of %HRR during specific physical activity types at work and during leisure-time stratified by sex. Differences in %HRR between OPA and LTPA were more pronounced in men compared to women, with a significant domain*sex interaction effect showing betas with 95% CI of 2.5 [1.0 4.1], (unadjusted) and 2.4 [0.9 4.0] (adjusted).
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Figure 3. Mean and standard deviation of %HRR during specific physical activity types at work and during leisure-time stratified by physical fitness. Differences in %HRR between OPA and LTPA depended on the cardiorespiratory fitness of workers, with a domain*fitness interaction effects
showing betas with 95% CI of 1.43 [-0.50 3.36] (unadjusted) and 1.91 [0.33 3.48] (adjusted). The
figure represents only those 92 workers who took part in the cardiorespiratory fitness cycling test, that were classified into a group with low fitness (70%) and a group with high fitness (30%).
20
25
30
35
40
45
50
55
Lowfitness
Highfitness
Lowfitness
Highfitness
Lowfitness
Highfitness
Lowfitness
Highfitness
Lowfitness
Highfitness
Sitting Standing Moving Walking Stairs
HR
R (
%)
Work
Leisure
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Table 1. Characteristics of the study sample. Mean values with standard deviation or number of participants with prevalence are presented. Variables Mean (SD) n (%)
Number of participants 124 Number of females 61 (49%) Smoking, number of smokers 75 (62%) Heavy lifting, number of participants who lift >1/4 of the work time 76 (61%) Ingest heart/lung medication on a daily basis, number of participants 18 (14%) Age (years) 46.6 (9.1) Influence at work
1 47.3 (22.4)
Alcohol consumption (beverages per week) 2.6 (5.1) BMI (kg/m
2) 26.0 (4.6)
Cardiorespiratory fitness (mlO2/min/kg)2 32.3 (8.8)
1Ranging from 0 to 100, with high scores representing a higher degree of influence at work
2Based on n=92 participants who participated in the cycle test.
ACCEPTED MANUSCRIPT

ACC
EPTE
D M
ANU
SCR
IPT
Table 2. Mean (and standard deviation) of percentage heart rate reserve (%HRR) during each of the specific physical activity types at work and during leisure-time combined (left columns), at work (middle columns) and during leisure-time (right columns). Also the number of participants and mean (and standard deviation) of measurement duration are shown. Data during sleeping intervals are not shown. Total Work Leisure
n
Measurement
duration (hours/day)
%HRR n
Measurement
duration (hours/day)
%HRR n
Measurement
duration (hours/day)
%HRR
Sitting 124
7.9 (2.4) 23.4 (5.8)
123
3.4 (1.6) 24.7 (6.0)
123
4.5 (1.7) 22.2 (5.3)
Standing 124
3.7 (1.2) 31.2 (7.1)
123
2.3 (1.2) 31.7 (7.6)
123
1.4 (0.7) 30.6 (6.5)
Moving 124
1.9 (0.9) 33.9 (7.4)
123
1.3 (0.9) 35.1 (8.5)
123
0.6 (0.3) 32.8 (6.0)
Walking 124
2.1 (0.9) 35.1 (7.0)
122
1.4 (0.9) 35.6 (7.6)
123
0.7 (0.4) 34.5 (6.3)
Stair climbing
124
0.1 (0.1) 37.9 (8.8)
122
0.1 (0.1) 39.5 (8.9)
120
0.0 (0.0) 36.2 (8.4)
Total 124
15.7 (2.3) 32.5
(5.7)1
124
8.5 (2.0) 33.4
(7.3)1
124
7.2 (2.3) 31.4
(5.7)1
Weighted total
124
28.22
124
30.22
124
25.92
1Average %HRR over all activities
2Weighted average %HRR over all activities (weighted by measurement duration)
ACCEPTED MANUSCRIPT
ACC
EPTE
D M
ANU
SCR
IPT
Highlights Recent evidence suggests contrasting health effects from occupational and
leisure-time physical activity As the nature of physical activity in these two domains may explain these
health differences, we assessed the intensity of occupational and leisure-time physical activity
We analysed objectively measured physical activity and % heart rate reserve (%HRR) from blue collar workers
%HRR was significantly higher during occupational physical activity than during leisure-time physical activity
This elevated intensity may help explaining negative health consequences of engagement in high levels of occupational physical activity
Future work should focus more on the difference between occupational and leisure-time physical activity
ACCEPTED MANUSCRIPT