diet therapy for surgical conditions
DESCRIPTION
dietTRANSCRIPT
Diet Therapy for Surgical Conditions
Surgery is defined as a “planned anatomical alteration of the human organism designed to arrest, alleviate or eradicate some pathologic process”. Modern surgery underscores the significance of correct diagnosis of the illness and case of the patient prior to and after surgical procedure. While the success of the operation depends primarily on a qualified surgical team and the use of modern techniques, the severity of postoperative complication is linked to other important factors, including nutritional status. The roles of diet and nutrition support in the pre-operative and post-operative stages are emphasized.
The Surgical Process
There are three phases of surgical process: 1. pre-operative evaluation and preparation for surgery, 2. the surgery procedure itself and 3. the postoperative care. In all these phases, the patient undergoes physiologic and psychological stresses that require comprehensive care.
Based on the urgency of operation, surgery comes in two forms: emergency and elective operation. Emergency surgery Is performed when the nature of illness require an immediate intervention ( such as acute appendicitis ). Thus, there is limited time to prepare the patient especially when poor nutrition coexists. In contrast, elective surgery allows reasonable time to prepare the patient before surgery.
The crucial role of nutrition to overall care of surgical patient is well recognized and in fact, the overall importance of nutritional support to surgery is now considered of the same magnitude as antibiotics, blood transfusion, and critical care monitoring. Nutrition is a key factor to enable surgeons to produce and expect a better outcomes of the procedure.
Metabolic Response to Surgery
Surgery is accompanied by stress response. It is designed to produce sufficient calories to meet high metabolic demands from surgery and injury. The stress response involves an increase in the secretion of epinephrine, norepinephrine and corticosteroids resulting in breakdown of glycogen, fat stores and body proteins, especially skeletal muscles. The net effect in severe cases is increased urinary nitrogen loss, muscle wasting and weight loss.
The stress response is also intended to maintain the blood volume. Antidiuretic hormone (ADH) secretion increases during the stress response, with decreased urine output and retention of fluid. In hypovolemia, increased aldosterone secretion occurs and sodium and fluid are retained.
The catabolic responses to surgery or injury vary depending on the extent of tissue damaged. Minor surgery (such as a hernia repair) may evoke little systemic responses, whereas major surgery or accidental injuries (such as a cardiac bypass surgery or a 60% total body surface flame burn) induce maximal response.
Negative Nitrogen Balance
The loss of nitrogen from the body is primarily the result of increased excretion of urea and other nitrogenous products in the urine, loss of protein through the injured tissue in individuals with large open wounds. The pattern of protein breakdown is related to the degree of damage in a dose-response manner (i.e. the greater the injury, the larger the nitrogen loss). Nitrogen excretion is also dependent on nutritional state of the patient and the size of the lean body mass. Thus, a muscular, well nourished person will lose more nitrogen than a depleted individual will after similar, comparable operation .
Nitrogen excretion increases in the first few days after surgery and peaking for several days or week, and then gradually returning to equilibrium as the inflammation resolves and/ or the wound heals. This course, and the degree of the negative nitrogen balance, can be minimized, but not abolished, by food intake and exercise.
Hormonal and Inflammatory Response
Initially, insulin levels are low and then they gradually rise, although insulin resistance is present. The elaboration of the counter regulatory hormones cortisol, glucagon and cathecolamines is increased, and these factors play a central role in the response.
Inflammatory factors (such as cytokines, leukotrienes, etc.) contribute to the catabolic response, either directly or indirectly ( stimulating elaboration of catabolic hormones, causing anorexia through central nervous system mechanism and increasing body temperature ).
Translocation of the Amino Acids
The metabolic response to surgery is characterized by the breakdown of skeletal muscle protein and the translocation of the amino acids ( mainly alanine and glutamine ), to visceral organs and the wound. At these sites, the amino acids serve to enhance host defenses and support vital organ function and wound repair.
Pre-operative Diet
The pre-operative diet aims to improve the nutritional status of the patient, to prepare him for nutrient losses during surgery (e.g. protein, water, electrolytes, protein), to help hasten post-operative recovery, to build up glycogen reserves, and to strengthen bodily resistance to infections. Weight changes should be affected during the pre-operative stage. Patients whose weights are nearly within desirable levels are exposed to less surgical risks than obese or underweight patients. Diabetics should be especially attended to. Nutritional anemia and other deficiencies should be corrected prior to surgery.
Diet for elective surgery
In elective surgery, the surgery is planned and there is ample time to apply the prescribed pre-operative diets. Whenever possible, a high protein, high calories diet with vitamin and mineral supplementation is recommended. If patient is obese, use a low-calorie diet that includes carbohydrates adequate for glycogen stores. Intakes of zinc , vitamins C and K should be adequate.
Diet for Emergency Operations
For emergency cases, parenteral feeding is the fast method of nourishing the patient before surgery. “parenteral” means other than the oral route; i.e., subcutaneous, intramuscular or intravenous ( I.V ) feeding.
Diet immediately before surgery
Light evening meals is prescribed the day before the surgery. This is gradually restricted to clear liquids and then all foods are withheld for at least 8 hours to empty the stomach. Some clinicians prescribe a non-residue is clear liquid diet for several days especially when the surgical site involves the gastrointestinal tract. This eliminates the possibility of inhaling the vomitus during the anesthesia and reduces the feces in the colon.
In emergency cases, gastric lavage ( gastric suction) is administered to remove gastrointestinal contents. For gastrointestinal operations, a non-residue diet is given for several days. Clinically defined or elemental formulas can provide a complete diet in liquid form.

Post-Operative Diet
In general, nothing is given by mouth (NPO) immediately after the operation. When the patient has recovered from anesthesia effects or as soon as peristalsis is evident, a clear liquid diet is given. This is gradually changed to full liquid diet, a soft, and eventually to a regular diet. Depending on the patients tolerance for oral feeding, a high calorie, high protein diet is recommended.
The first rule of post-surgical care is to make the patient resume his normal diet food in the gastrointestinal tract hastens peristalsis and stimulates normal digestive function. While the best route for food is by mouth, there are cases when this is not possible. Intravenous or tube feeding are resorted to, ether totally or in part, to provide nutrients in a hurry. The rule of thumb is “when the gut works, use it”.
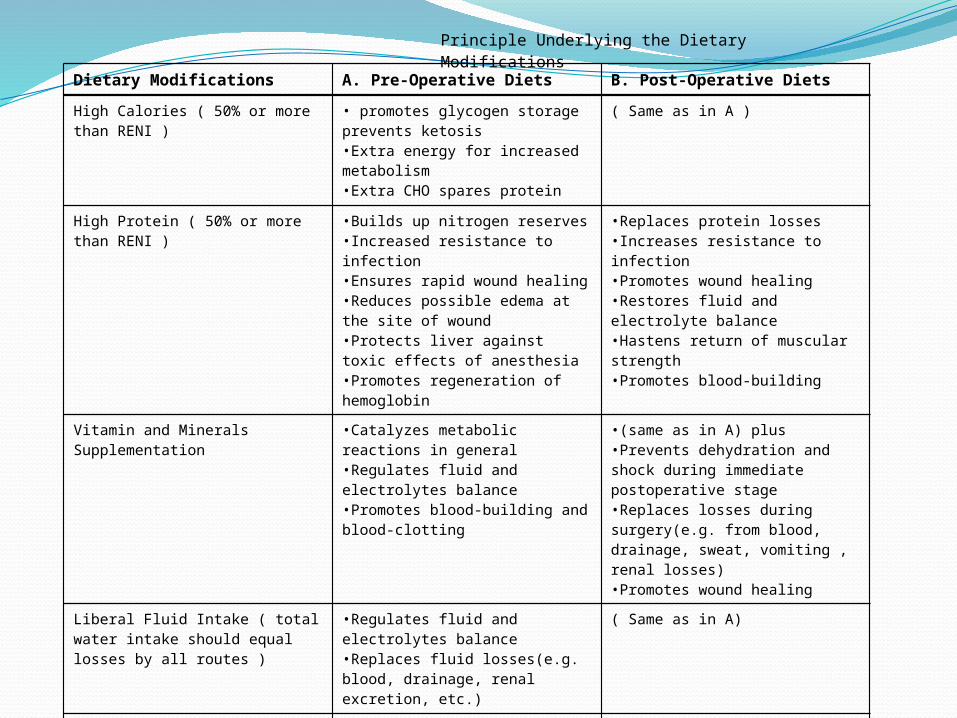
Dietary Modifications A. Pre-Operative Diets B. Post-Operative Diets
Principle Underlying the Dietary Modifications
High Calories ( 50% or more than RENI )
• promotes glycogen storage prevents ketosis•Extra energy for increased metabolism•Extra CHO spares protein
( Same as in A )
High Protein ( 50% or more than RENI )
•Builds up nitrogen reserves•Increased resistance to infection•Ensures rapid wound healing•Reduces possible edema at the site of wound•Protects liver against toxic effects of anesthesia•Promotes regeneration of hemoglobin
•Replaces protein losses•Increases resistance to infection•Promotes wound healing •Restores fluid and electrolyte balance•Hastens return of muscular strength•Promotes blood-building
Vitamin and Minerals Supplementation
•Catalyzes metabolic reactions in general•Regulates fluid and electrolytes balance•Promotes blood-building and blood-clotting
•(same as in A) plus•Prevents dehydration and shock during immediate postoperative stage•Replaces losses during surgery(e.g. from blood, drainage, sweat, vomiting , renal losses)•Promotes wound healing
Liberal Fluid Intake ( total water intake should equal losses by all routes )
•Regulates fluid and electrolytes balance•Replaces fluid losses(e.g. blood, drainage, renal excretion, etc.)
( Same as in A)
Intervals of feeding ( small, frequent feeding 6 times a day; more for liquid diets )
•Promotes assimilation and metabolism•Flexible to patient’s tolerance for food
( Same as in A)
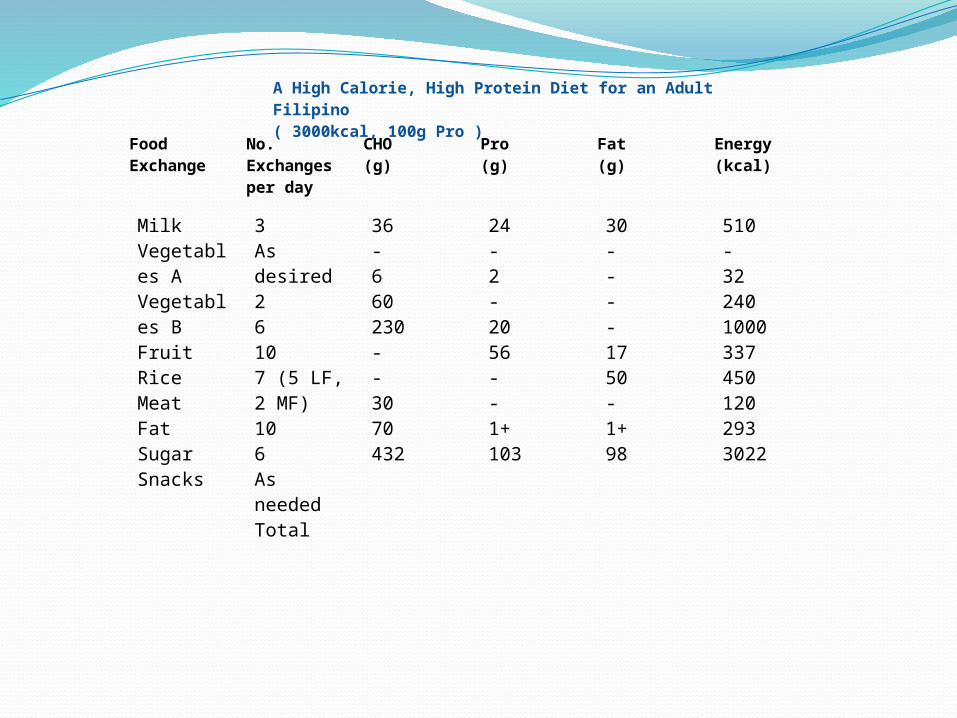
Food Exchange
No. Exchanges per day
CHO(g)
Pro(g)
Fat(g)
Energy(kcal)
A High Calorie, High Protein Diet for an Adult Filipino( 3000kcal, 100g Pro )
MilkVegetables AVegetables BFruit Rice MeatFatSugarSnacks
3As desired26107 (5 LF, 2 MF)106As neededTotal
36-660230--3070432
24-2-2056--1+103
30----1750-1+98
510-3224010003374501202933022

Meal pattern No. of exchange Sample menus
Breakfast:Fruit CerealProtein dishBreadButterBeverage(milk)Sugar 1 tbsp.Morning snack:Protein sourceBread-butterFruit juiceLunch:SoupMain dish w/ vegetables and cooking fatSaladRiceDessert(fruit)Afternoon snack:Milk sourceRice exchangeSupper:SoupMain dish w/ vegetables & cooking fatRiceDessert(milk containing)Bedtime snack:Milk beverage w/ sugarRice exchangeProtein source
2111213
122
2(meat)3(fat)
32
12
233
1-321
Orange juice, 1 tall glassChamporado w/ milk & sugarToasted dilisEnsaymada butter
Milk
Egg sandwish w/ mayonaise
Pineapple juice, 1 tall glass
Chicken tinola w/sili leaves brothThigh -1 large; sayote-1 cup
Fried fleshy fish-with sliced tomatoesRiceLacatan – 1 large
Milk shake and sponge cake
Almondigas soupBeef asado with carrots – one half cRiceCustard
Milo with milkCrackersCheese
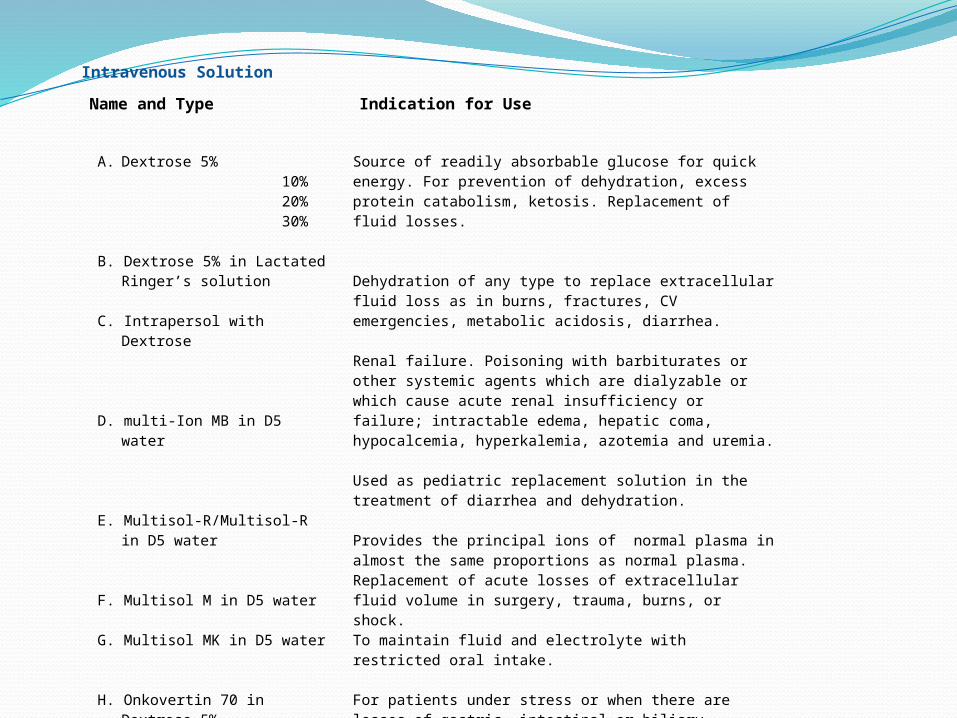
Intravenous Solution
Name and Type Indication for Use
A. Dextrose 5% 10% 20% 30%
B. Dextrose 5% in Lactated Ringer’s solution
C. Intrapersol with Dextrose
D. multi-Ion MB in D5 water
E. Multisol-R/Multisol-R in D5 water
F. Multisol M in D5 water
G. Multisol MK in D5 water
H. Onkovertin 70 in Dextrose 5%
Source of readily absorbable glucose for quick energy. For prevention of dehydration, excess protein catabolism, ketosis. Replacement of fluid losses.
Dehydration of any type to replace extracellular fluid loss as in burns, fractures, CV emergencies, metabolic acidosis, diarrhea.
Renal failure. Poisoning with barbiturates or other systemic agents which are dialyzable or which cause acute renal insufficiency or failure; intractable edema, hepatic coma, hypocalcemia, hyperkalemia, azotemia and uremia.
Used as pediatric replacement solution in the treatment of diarrhea and dehydration.
Provides the principal ions of normal plasma in almost the same proportions as normal plasma. Replacement of acute losses of extracellular fluid volume in surgery, trauma, burns, or shock.To maintain fluid and electrolyte with restricted oral intake.
For patients under stress or when there are losses of gastric, intestinal or biliary secretions or in potassium losing disease state.
Volume replacement for immediate treatment of shock, thrombo-prophylaxis; pre-operative hemo-dilution.
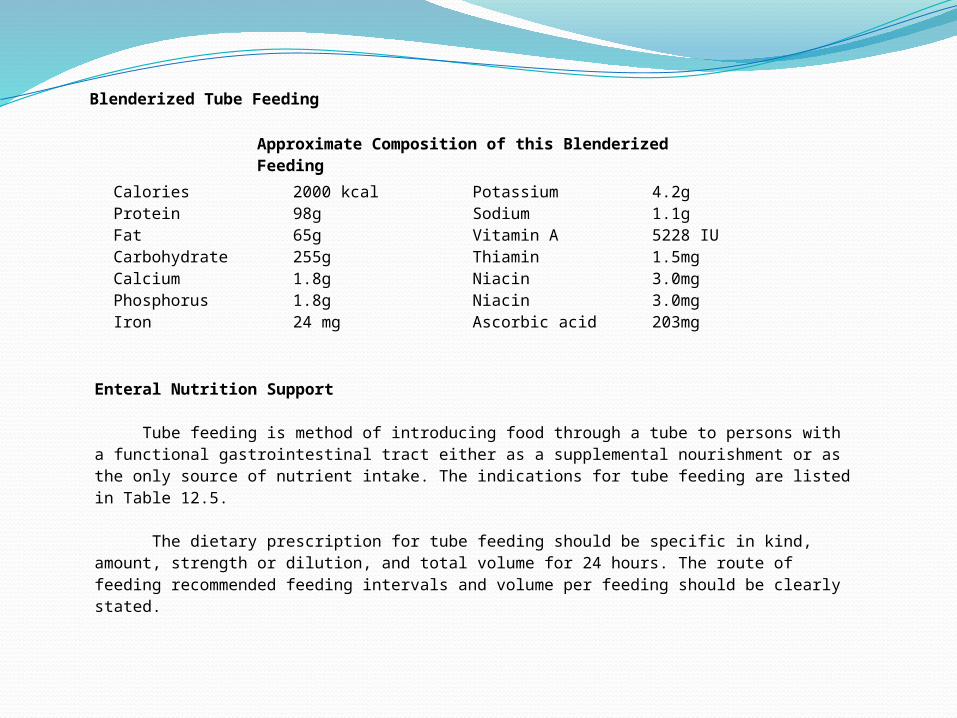
Blenderized Tube Feeding
Approximate Composition of this Blenderized Feeding
CaloriesProteinFatCarbohydrateCalciumPhosphorusIron
2000 kcal98g65g255g1.8g1.8g24 mg
PotassiumSodiumVitamin AThiaminNiacinNiacinAscorbic acid
4.2g1.1g5228 IU1.5mg3.0mg3.0mg203mg
Enteral Nutrition Support
Tube feeding is method of introducing food through a tube to persons with a functional gastrointestinal tract either as a supplemental nourishment or as the only source of nutrient intake. The indications for tube feeding are listed in Table 12.5.
The dietary prescription for tube feeding should be specific in kind, amount, strength or dilution, and total volume for 24 hours. The route of feeding recommended feeding intervals and volume per feeding should be clearly stated.

Table 12.5. Indication for Use of Tube feeding
Inability to ingest food normallyStupor, unconsciousness, coma, cerebrovascular accidentsInflammation in central nervous systemCerebral neoplasmFracture of mandibleOropharyngial neoplasmHead and neck surgeryDysphagiaRadiation to head or neckChemotherapyMultiple sclerosis
Physiologic deterrents to food intakeNausea or vomiting in pregnancy, drug reactions, radiation or chemotherapyDumping syndrome
Obstruction of gastrointestinal tract( if access is below obstruction )Esophageal stricture or neoplasmSpasm of pylorusNeoplasm, foreign body or other obstruction of stomach or intestine
Psychiatric illnessAnorexia nervosaDepressionDiversion of flow ( fistulas )
Impairment of digestion and or absorptionPancreatic insufficiency; carcinomaChronic pancreatitisBile salt insufficiencyBile acid-induced diarrhea; blind loop syndromeShort bowel syndromeGluten enteropathyCrohn’s diseaseDissacharidase deficiencyRadiation damageAbetalipoproteinemiaObstruction of lymph flow
Protein-calorie malnutritionHypermetabolic stateBurnsTraumaSurgeryFever
Intestinal surgeryPreparation for hemorrhoidectomyPreparation for instestinal surgery
Transition from total parenteral nutrition to conventional foods
Renal failureHepatic failure
Inborn errors of metabolism

Characteristic of tube feeding and preparation Tube feeding may be prepared from liquid foods using calculated formulas, from commercial preparations, or from regular or natural foods liquefied in a homogenizer or blender, and thus, called “blenderized feeding”. A satisfactory tube feeding must be nutritionally adequate, except for prescribed modifications for specific nutrients. It must be inexpensive, easily prepared, and stored. It should be well tolerated by the patient with no reaction in the gastrointestinal tract to cause flatulence, diarrhea, vomiting, etc. The mixture should pass the 2mm tube with relative ease. The prepared dilution is 1kcal/ml. the total volume should not exceed 2300 ml/day or 100ml/hr.
Choosing tube feeding preparation
physical properties – the physical properties to be considered in tubefeeding formulas are osmolality, renal solute load, residue and viscosity. The osmolality involves the concentration of solute per unit of solvent and is measured in terms of milliosmoles per kilogram of water (mOsm/kg). The osmolality is the measure of the ability of a solution to lose or draw water through a semi-permeable membrane. A formulas with high osmolality, administered quickly, will draw fluid in to intestine and may result in cramps, nausea, vomiting or diarrhea. Osmolality is a critical factor for individual who had gastric surgery, and those using jejunostomy feeding tubes. Osmolality may not be a problem if the formula is administered slowly or by a constant drip. Generally, the lower the osmolality of the formula, the more rapidly it can be infused. A well balanced diet of natural foodstuff has an osmolality of approximately 600 mOsm/kg of water compared woth serum which is approximately 300 mOsm/kg of water. The osmolality of tubefeedings is increased by the presence of free amino-acids, monosaccharides, disaccharides and electrolytes. Fats whole protein and starches are less osmotically active.
The renal solute load (RSL) refers to the amount of urea, sodium, potassium and chloride in the urine. If the renal solute load is especially high, a large quantity of water must be provided to excrete it. If this water is not given, the patient will become dehydrate. Patients receiving formulas with a high RSL must monitored carefully for signs of dehydration especially infants, those with impaired renal concentration ability and those with increased fluid losses from vomiting diarrhea, burns and fever.
The terms residue pertains to the amount of bulk remaining in the intestinal tract following digestion, especially the undigested and unabsorbed component if food. A reduction or absence of residue remaining in the intestine is desirable in some preoperative and postoperative patients, for patients with gastrointestinal disorders such as Crohn’s diseased or colitis, and for patients in transition between intravenous and tube feeding. These patients may be given low-residue or residue-free formulas. On the other hand, the low residue content of many formulas may cause constipation. For such patients, a family containing fiber may be used if not contraindicated by his condition.
Viscosity refers to be resistance of a fluid to flow. Formulas containing larger molecules, such as whole protein compared to amino acids, and formulas that have a higher caloric content per unit volume tent to be more viscous. The viscosity of the formula and the caliber of the tube must be compatible. More viscous formulas require a larger tube which is also generally less comfortable for patients. in tube feeding; both the quantity and type of ingredients must be considered in relation to patient’s specific needs.
Nutrient contribution. Caloric density considers the energy value of the food in relation to volume. Most tubfeeding yield 1 kcal/ml, but 1.5 and 2.0 kcal/ml formulas are available. These are useful for patients with high caloric needs and limited appetites or volume tolerance. The more calorically dense formulas also have high osmolarity and high RSL. Precautions must be taken to prevent dehydration and the patient must be monitored carefully.
Carbohydrates may come from many sources including, fruits, cereals, vegetables, corn syrup, glucose, sucrose, lactose, oligosaccharides and dextrins. Cornstarch , maltodextrins and oligosaccharides saccharides have been used to provide carbohydrate while minimizing formulas osmolality and sweetness. For patients who develop lactose intolerance, lactose free formulas are used.
Dietary fiber is present is formulas containing fruits, vegetables and cereals. Dietary fiber can be increased by adding banana flakes, applesauce, pureed fruits or tender leafy vegetables and are beneficial for patients with diarrhea and constipation.
Protein may be supplied in formulas as whole protein, hydrolyzed protein, or as free amino acids. A formulas low in protein is administered to individuals with renal or hepatic impairment. A high protein formula may be indicated for individuals who are manourished, for septic or pre and post-surgical cases or for those who have experienced trauma. Individuals receiving high-protein formulas, particularly those who are unconscious, who cannot communicate thirst, should be monitored for adequate water intake and fluid and electrolyte balance.
Fat adds calories to formulas. It is generally provided in the form of vegetables oils, which contain glycerol and long chain fatty acids and are called long chain triglycerides(LCT). If fat malabsorption is present, a formula low in fat, or one that contains medium chain triglycerides (MCT) in place of long chain fatty acids is indicated. LCT does not add to formula osmolality. Formulas containing MCT must contain some LCT to provide the required essential fatty acids.
Vitamins, Minerals and Trace Elements: these nutrients are generally provided in commercial formulas in amounts to meet recommended dietary allowances. Certain individuals with malabsorption or for those under stress may be getting inadequate amounts of these nutrients and should be monitored and supplemented when necessary. Modified commercial formulas or house blenderized formulas may be necessary when electrolyte or mineral intake must be controlled. The amount of sodium, potassium, and or phosphorus, may have to be altered for patients with renal, hepatic or cardiac failure.
Cost and Preparation Time House blenderized formulas prepared from regular foods permit flexibility in meeting needs, are relatively inexpensive, and are more psychologically acceptable since the formula can be perceived as regular food. In preparing tube feeding it is advisable to observe the following:1. Use enough liquid for better blending and liquefying (see recommended dilutions in Table 12.5)2. Plains pasteurized milk is not recommended because the butterfat tends to clump the blender. Use
homogenized milk instead.3. Avoid coarse, fibrous foods that tent to clog the blender. Use low-fiber fruits and vegetables, strain
after blending.4. For convenience, baby foods in bottles may be used.5. Keep prepared blended foods refrigerated until use. Discard formulas after 24 hours.
To prevent bacterial contamination during preparation, the following will be most useful:6. Use feeding containers that are closed to reduce the risk of airborne organism contamination.7. Never add new formulas to old ones.8. Extension tubing administration set and bag should be changed daily.9. Prepared formulas should be refrigerated if not used immediately.10.Feeding formulas should not be allowed to hang for longer than 8-hours.
Tube feeding should not be warmed before use. A chilled or cold formulas can be fed without problems if administered slowly. Heating the mixture may result in destruction of water-soluble vitamins, coagulation of protein, clogging of nasogastric tubes and coagulation of the formula.
Intervals of Feeding and Administration Tube feeding may be given as continuous drip or at intervals throughout the day. The feeding
regimen should be adjusted to the patients condition, nutritive and dietary prescription by the doctor. To initiate tube-feeding, use dilute mixture at first about half to concentration. Try 50 ml of the mixture at hourly intervals, then gradually increased the concentration and volume until the patients can tolerate 2000ml at 2-3 hours intervals. Do not exceed over 300ml of feeding of 3 to 4hour intervals. However, if pumps are used, formula need to be diluted.
For the continuous drip method, the flow of the tubefeeding should be very slow at first, then, increased gradually but kept in constant, steady rate. Total volume should not exceed 100 ml per hour. Additional water should be given as needed to meet fluid requirements. As patients condition improves and whether possible, food should be given orally. Again, small amount of liquid food is gradually introduced, increasing the volume and consistency, until part of the day’s feeding is by normal means.

Bolus feeding refers to rapid installation of feeding into the GI tract by syringe or funnel. The majority of patients seldom tolerated this method. Patients on enteral feeding may experience complication as a result of the formula, its administration or handling. Table 12.6 gives a list of potential complication and suggestion for resolving these complications.
Table 12.6. Enteral Feeding Complications and Suggestion for Solution
Complication Suggestion for Resolving Problem
Diarrhea
Aspiration
Clogged Tubes
Constipation
• Assess the administration of the enteral formula. Formula should be administered at room temperature. Assess the volume of the bolus feedings, drip rate of the drip feeding, and the number of cc’s per hour for pump administration.•Assess handling technique of the formula, tubing, addition of medications and fluids. Is there a possibility of contamination ? Could medication be the cause of the diarrhea ( antibiotics, stool softeners, laxatives or other medications that may cause diarrhea)?•Assess for fever, potential of flu or other illness. Consider a stool sample to assess for clostridium difficile toxin.•Assess for lactose intolerance•If diarrhea is severe, consider holding tube feeding for 12 hrs giving only clear liquids.•Assess osmolality of the feeding•Consider a fiber containing formula to increase bulk of the stool•If diarrhea continues, request an antidiarrheal medication and refer to physician•Head of bed should be elevated to 30-45 degrees to avoid aspiration•Gastric residuals should be checked prior to feeding•Enteral feedings should be held if gastric residuals are greater than 100-150cc, or per physician’s order.•Enteral tube replacement should be checked if aspiration is suspected•Consider post pyloric placement of tube if aspiration is a reoccuring problem•Flush tube with 50-1150cc of fluid before and after administration of formula or addition of medications•Avoid the use of juice, carbonated beverages or sugary fluids to flush the tube•Avoid use of crushed medications•Liquid medications may contain sorbital, which may clog tubes•Provide adequate fluids•Assess need for a fiber containing formula•Consider use of stool softener if laxatives if necessary.
Abdominal Distention
Nausea/Vomiting
Contamination of Formula
•Assess volume of formula administered for a short time•Assess possibility of lactose intolerance if client is receiving lactose containing formula•Assess for intolerance to fiber containing formula of appropriate•Consider holding feeding for 12 hours or until excessive vomiting passes•Check residual and tube placement•Assess volume of feeding administered for a short time•Consider anti-nauseant, or anti-emetic or anti-gas medication•A change in formula may be necessary. Assess for elemental formula. Refer to physician•Closed systems are ideal for avoiding potential contamination. They can hang for up to 24-48 hours (see manufacturer’s information for details)•Avoid addition of liquids, medications or new formula in a bag that has been hanging for a period of time•If open systems are used, formula should not hang more than 4-8 hrs or according to manufacturer. If enteral bags are filled by nursing staff do not allow nursing to add new formula to old formula (“topping off” the bag). Always clean tops of cans before opening•Clean poles and surrounding areas often•Discard unused formula•Use sanitary techniques for mixing and administering formula.

Parenteral Feeding
Pre-surgical and post-surgical feedings are given in a variety of ways that should be specific to each individual depending on the factors like the patient’s nutritional status, ability to swallow, level of digestion and absorption, presence of nausea, vomiting, anorexia and location of surgery, etc. The oral route is always preferred, but if the patients cannot tolerate normal eating, parenteral feeding is the alternative solutions. Parenteral feeding is a means of providing the nutrients by routes other than the mouth and digestive tract, such as subcutaneous, intramuscular or intravenous feeding. Parenteral feeding can used in addition to enteral feedings or used alone. If parenteral feeding is the main source if nutrition, other nutrients have to be given via the small veins, usually in the arm ( peripheral, parenteral nutrition of PPN), or centrally into the superior or inferior vena cava or the jugular vein. (central-parenteral nutrition or CPN) is also called total parenteral nutrition (TPN) or intravenous hyperalimentation (IVH). The decision to use PPN or CPN is based on the number of calories needed and the osmolality of the solution. TPN solutions are best prepared by the experts such as a pharmacist pr in industrial laboratories. A physician trained in this area prescribe and guides the use of TPN.
Diet Therapy for Specific Surgical Conditions
The main objective of dietary modification on specific surgical conditions ( such as tonsillectomy, colostomy, rectal surgery, gastric resection, etc. ) is to rest the organ involved and avoid irritation at the site of the resection. It also promotes rapid wound healing and replaces nutrient losses.

Tonsillectomy and Adenectomy The first day after the surgery, start with ice chips or sips of cold water progressing with plain gelatin, cold milk and non-irritating fruit juices. Avoid milk products only if patient cannot tolerate them. The second day, cold liquids, gelatin, ice creams and popsicles are added. Chocolate products and red colored beverages (including red gelatin) are not given because they may mask bleeding. On the third and the fourth day, strained warm cream soups, fruits and vegetable purees, strained warm cereals, milk, cheese, butter, rice porridge (lugao) and mashed potatoes are added to the cold liquid diet. This diet is inadequate in all nutrients and is usually ordered for only one or two days following surgery. It is low in iron, thiamin, ascorbic acid and folic acid. After the fourth day a soft to light diet is prescribed according to individual tolerance. The patients should be able to resume a normal diet after a week, some as early as the 6th day. Adequate daily fluid intake ( 3 L for adults and 2 L for children per day ) is important. Avoid hot, spicy foods, raw vegetables, toast and crackers, citrus fruits and other related foods until full recovery.
Surgery in the Mouth, Neck and Esophagus
After the surgery in the mouth, neck and esophagus, the patient has difficulty in chewing and or swallowing. Tube feeding is therefore required. Parenteral feedings may be indefinitely prolonged if surgery is extensive or major. As the patient’s condition improves, tube feedings become supplemental and oral feeding gradually initiated progressing from clear to full liquids, then soft to light and finally to regular diets.
Gastric Surgery as Gastrectomy
A partial gastric resection poses less dietary problems compared to a total gastrectomy. Removal of the stomach in part or as a whole reduces not only the reservoir of food but production of pepsin and HCL, resulting in reduced protein digestion. Intestinal motility is increased and there is defective mixing of food woth the intestinal juices. Fat digestion is also impaired due to reduced biliary and pancreatic juices, and insufficient mixing of enzymes with the food. Lack of HCL and the intrinsic factor found in the stomach leads to reduced utilization of iron and vitamin B12, 50% of patients often lose weight after gastric surgery.
After surgery, the diet will generally progress as follows:1. Ice help in mouth or small sips of water. Some patient tolerate warm water better than ice or cold
water.2. Increase in amounts of fluid given3. Bland foods/solid foods as tolerated
The guidelines must be tailored to each patient’s needs such as surgery, food tolerances and intolerances and nutritional problems and deficiencies:
1. Diet should be low in simple carbohydrate but should be high in complex carbohydrates, high in protein and moderate in fat.
2. Liquids should be given 30-60minutes after each meal.3. Small frequent feeding should be given , the number of which depends on the patient’s
tolerance to specific portions of food.4. Small amount of milk of milk maybe tolerated than large amounts . If there is milk
intolerance ,lactose free products maybe used. 5. Foods should be eaten slowly and chewed well.6. If there is steatorrhea, use of medium chain triglycerides and MCT oil may be indicated.7. If “dumping “ is a problem, it may help to lie down immediately after meals to retard transit
to the small bowel.8. The dietary fiber pectin, found in fruits and vegetables, may be helpful in the treatment of
dumping syndrome. Pectin delays gastric emptying time reduces the glycemic response and slows down carbohydrate absorption.
9. All food and drink should be moderate in temperature. Cold drinks tend to cause increased gastric activity.
Dumping Syndrome
Individuals who have had gastrectomy may experience the “dumping syndrome” characterized be nausea, weakness, syncope and diarrhea. This happens when the stomach contents are emptied into the jejunum at an abnormally fast rate. The guidelines of the post-gastrectomy diet for dumping syndrome ( especially in cases of total gastrectomy ) are follows:
10.Small frequent feeding 5-6 times per day11.Restricted liquid or a “dry” diet. Avoid fluid at least one hour before and after a meal.12.Low fiber low residue diet ( avoid milk, raw fruits and vegetables high in fiber)13.Low carbohydrates to prevent dumping of readily utilized carbohydrates in the jejunum. This
causes disruption in the water balance leading to the withdrawal of fluid from the blood to the intestine.
14.Multiple vitamin and mineral supplementation is prescribe.15.Learn to relax; rest before mealtime, eat slowly and chew food well.

Ostomies
An ostomy is the surgical procedure of creating an opening of the stomach wall of the abdomen. It is a procedure that brings movement of the GI tract usually intestinal to the skin surface. The main purpose is to evacuate stools or move the bowels when the normal route via the colon, rectum and anus is not medically allowed. Immediately after the surgery, IV feeding is given for 2 to 3 days until bowel sounds return. Start with clear liquid diet and progress gradually to one low in residue. Then give a soft or low fiber diet as tolerated. Gradually introduce fiber as tolerated. Avoid tough skin from fruits and vegetables and other foods that may cause stoma obstruction. Take plenty of fluids ( at least 8 to 10 cups per day ) especially of the ostomy output is excessive. When steatorrhea occurs, restrict fat and use MCT oil. A liberal supply of calories and protein ( at least 1.5 times the recommended nutrient intakes) will speed up recovery and prevent weight loss. In all cases, small frequent feedings are recommended. In ileostomy, MCT diet (medium chain triglycerides) is prescribe and fat soluble vitamins ADEK are supplemented. If there is increased fluid loss, both water intake and electrolytes are replenished.
Rectal Surgery
This condition refers to any operation done the rectum, as in rectal cancer or hemorrhoidectomy. A clear liquid diet is given within the first 24 hours after the operation, followed by a non-residue diet. In hemorrhoidectomy, diet is progressed from clear to full liquid omitting milk, then a low-residue diet until wound has healed and the patient can tolerate the regular diet. The use of mineral oil for a few days, helps, but should not be prolonged since mineral oils interfere with the utilization of fat soluble vitamins and some minerals. Some physician prescribe a low fiber diet to encourage normal defecation as soon as possible.

Fractures and other Mechanical Trauma
Current studies indicate that a unique metabolic reaction is triggered by trauma and stress. This condition is sometimes called a “hyper-metabolic state”. Shock, multiple fractures, major burns, anesthesia and major surgery are some of these cases when patients could be in hyper-metabolic states. Diet should be quite high in calories, proteins and fluids. Traumatic injury would need 35-40 kcal/kg body weight per day. An example of a diet prescription is 3000 kcal and 120 g protein. Vitamin and mineral supplementation is required, particularly calcium, phosphorus and magnesium (for calcification), vitamin D (for efficient utilization of the mineral) and vitamin C (for intercellular cementing substance.
Burns
Burns refer to tissue injury or destruction caused by excessive heat, caustics (acid or alkalis), friction, electricity or radiation. Treatment involves relief of pain and shock, prevention of infection, actual care for the thermal injuries and plastic surgery later as needed. In cases of serious burns, the loss of skin surface leads to enormous losses of fluid, electrolytes and proteins. Water moves from other tissues to the burn site in an effort to compensate for the loss, which only compound the problem. This fluid loss can reduce the blood volume and thus blood pressure, as well as urine output. Fluids and electrolytes are replaced by intravenous therapy immediately to prevent shock. Glucose is not included in these fluids for the first 2 or 3 days after the burn because it could cause hyperglycemia.
Wound healing
Wound is a physical injury to the body tissues disrupting the normal continuity of structure. Wound healing involves tissue synthesis and occurs in two phases. Initial wound healing occurs readily during a period of negative energy balance; subsequent healing occurs between the fifteenth day after surgery or trauma.
Diet therapy. Increased protein of 1.2-2.0 g/kg body weight is required to promote wound healing and preserve tissue integrity. Sufficient energy about 25-35 kcal/kg body weight is considered necessary to meet metabolic needs and to prevent protein from being utilized as fuel. Zinc, vitamin A and vitamin C are also necessary for continued wound healing. Other nutrients required in wound healing include arginine, magnesium, and selenium. In general, all nutrients related to immune function are needed to hasten wound healing. The provision of sufficient fluid is also necessary. Adjunctive enteral support may be necessary to facilitate wound healing, particularly when oral intake is suboptimal.