diet – an emerging non- invasive, portable and low- cost approach to breast cancer screening prof...
TRANSCRIPT

DIET – An emerging non-invasive, portable and low-
cost approach to breast cancer screening
Prof J. Geoffrey Chase
Univ of Canterbury
Dept of Mechanical Engineering, Centre for Bio-Engineering
Christchurch, New Zealand

Overview
1. Background
2. DIET Technology
3. Clinical results
4. Summary

The Problem
Breast cancer was the most common cause of female cancer death in 1999
Over the period 1972 to 1997, the annual number of breast cancer deaths increased from 427 to 643[1]
Breast cancer is over represented among Maori (in NZ) and other ethnic groups worldwide
[1] NZ Ministry of Health, 2002

Breast Cancer Screening Reduces Mortality (Tabar et al, 2003)
• No real difference• Results due to improving care
• Screening = More early detection
+20%

Why? Low Compliance & Access
Source: NZ Ministry of Health, Trends and Projections 2002.
What you don’t see can kill you! [Breast Screen Aotearoa]
Goal is 70% every 2 years, but we get ~60% -- 40% missing!
• Predominant compliance rates in the US and EU range from 50-80% based on many factors
• Eligible populations (over 50 years) are growing demographically for next 10-20 years
• Certain sub-groups have very low screening rates and thus much higher mortality• Occurrence rates don’t seem to particularly favor any group

Screening
Screening has resulted is fewer deaths and earlier treatment
Concerns of screening Patient dose
When should women start screening
Costs
Resources
Impacts of false positives (in a gold-standard test that can only be done infrequently at older ages)
However, fundamentally, mammography is a scarce and increasingly costly resource … One thus cannot simply go get a repeat test to confirm, especially if you are
younger
Current Diagnostic Techniques
Palpation/Clinical Breast Examination (CBE) Very subjective Primary form of diagnosis Most mammograms occur after being
found this way first
Mammography only modality recommended for screening X-rays, breast compression (painful) Lower compliance due to pain, cost and access
Ultrasound High level of operator skills Significant (sensor) noise
MRI Very accurate, but expensive Very few can be served
No screening programs in most developing nations! Cost and X-Ray dose are major factors
Mammography
MRI
Problems with Existing Techniques
Currently, predominant breast cancer screening methods are:
Uncomfortable
Subject the patient to doses of radiation
Require expensive, location specific equipment and clinical staff.
They thus have relatively limited throughput (not enough capacity)
They are also low contrast as cancerous tissue density varies only ~5-10% from healthy tissue
Coupled with resulting low compliance rates the average tumour size detected is ~1cm = 10x larger than possible

What’s Needed?
An all new approach Must be clinically and commercially feasible Must address compliance (w/ screening) issues Must offer high throughput in terms of speed to test and access
An ideal design list would include: Low cost equipment with no need for specialist technician Portable No X-Ray dose Equal efficacy (1cm detection) compared to mammography Greater comfort (no compression)
Succinctly: less invasive, low cost screening system with more objective diagnosis (less ‘human error’)

The DIET Concept
DIET = Digital Imaging-based Elasto-Tomography
Can we meet all these needs?
Governors Bay, Christchurch Sunset over Southern Alps, Christchurch

The DIET System Concept

Advantages of the DIET Concept
Screening from a younger age (no radiation dose)
Possible to build a history (every year!)
Less painful alternative (equals higher compliance)
Accuracy (initial target 1cm)
Portability and ease of use (no specialised technician and no loss of compliance due to travel)
Scalability (will improve as silicon technology used improves)
Should be low cost (low-cost technologies used)

Prototype Development
Laboratory Hardware
1st Clinical prototype

DIET device at Canterbury BC

So, does it work??
If we could measure surface motions could we detect cancerous lesions, from surface data only?
Lake Mathieson, Mirror LakesWest Coast of S. Island
Lindis Pass and into WanakaCental Otago, S. Island

So, how does it work? And does it?
3 main steps: Vibration and image capture
Surface motion: (a) tracking and (b) characterisation
Diagnose based on surface motion
Proof of concept clinical trials as part of ergonomic and comfort trials shown Multiple volunteers, multiple frequencies of actuation
Test of technology and proof of clinical concept

Step 1: Vibration & Image Capture
Vibrate breast from underneath and capture digital image sequences from 5 cameras
Silicone gel with fiducial markers Simulation of human breast

Step 2a: Surface Motion Tracking
Markers tracked in 2D, then 3D correspondences
Optical flow skin tracking (better resolution)
Camera 1 Camera 2 Full 3D reconstruction
Fiducial tracking Skin tracking
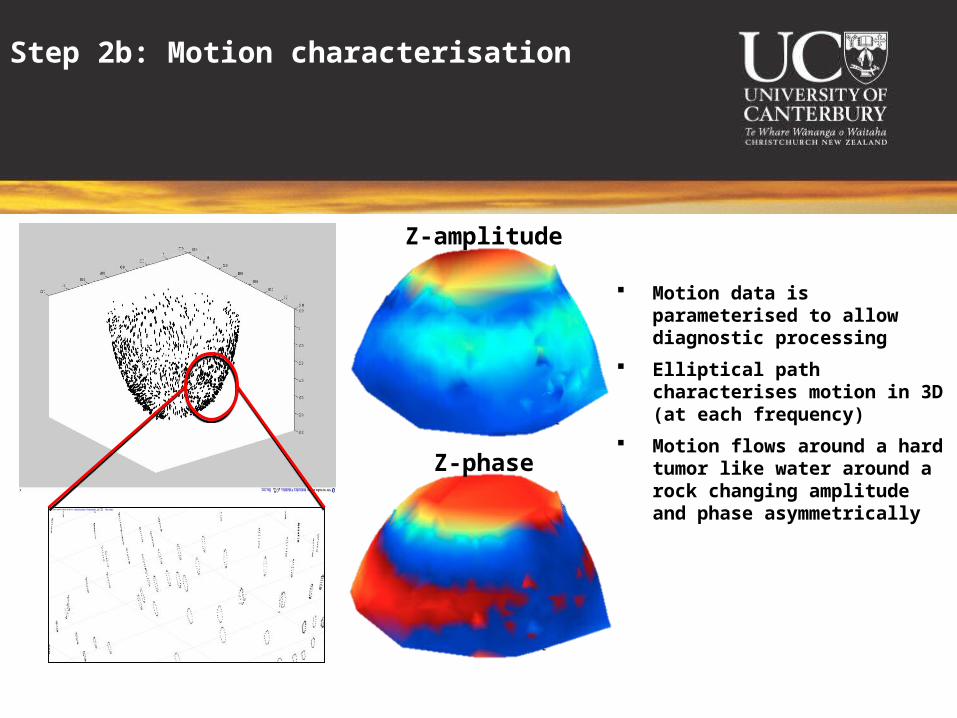
Step 2b: Motion characterisation
Motion data is parameterised to allow diagnostic processing
Elliptical path characterises motion in 3D (at each frequency)
Motion flows around a hard tumor like water around a rock changing amplitude and phase asymmetrically
Z-amplitude
Z-phase

Step 3: Diagnosis from tumour effect on motion
Silicone phantom with 20mm tumour at 6 o’clock Motion images alone can potentially give yes/no answer about
tumour inclusion Readily automated ... Entirely objective
Re Amplitude z-phase

In vivo results (preliminary)
Breast from ongoing trial
30mm tumour between 1-2 o’clock, left outer upper quadrant
Same effects as in phantoms are observed
TOP
BOTTOM
LEFTRIGHT
Z-phaseRez-amplitude

Some more visual outcomes
Both breasts of each subject shown at one frequency
120mm not shown, as it is almost entire breast
30mm @ 1:30 o’clock 20 + 8mm @ 2:30 o’clock
11mm @ 10:30 o’clock

DIET human trial summary
Ergonomics/Calibration trial
18 Subjects, age 49.3 (SD 8.5)
36 breasts imaged (both on each subject)
4 breasts with malignant tumors (11, 30, 20+8, 120mm)
2 breasts with benign cysts (clusters of 10-21mm, )
30 healthy breasts
Range of sizes and shapes see below.

First Uses: A 3 word case
Under-age
Under-served
Under-equipped
Plenty of “room” for a new modality like this

A Brief Summary
DIET is an all new approach to breast cancer screening that offers several potential advantages over current methods
Initial simulation and experimental proof of concept studies showed that it might be possible to achieve realistic screening (~1cm inclusion size detection)
The main imaging and reconstruction steps are technologically challenging
Initial proof of concept experiments on silicone phantoms have been successful in identifying inclusions both via reconstruction and from disturbances in surface motion
Acknowledgements
Prof Geoff Chase Dr Geoff Shaw Dr Thomas Desaive
Christina Starfinger
Dr. Chris Hann
Richard Brown
Rodney Elliot Crispen Berg
Dr. Richard Wien & Dr. Larry Ray
DIET Project Team 2004
Jerome Rouze Arnaud Milsant Ashton Peters
DIET Project Team 2005
Wili Berger
Ben Petit
Michael Wiertlewski Fabrice Jandet Edouard Ravni Anthony Hii Stefan Wortmann
Shig Kinoshita

Questions?