did you know newsletter n°2 2014
TRANSCRIPT

EUROPA UOMO / Did You Know? 02/2014 1
Europa Uomo Board
Ken Mastris Ekke Büchler Tor Tausvik Max Lippuner Christian Arnold Malcolm Duncan
Chairman Vice-Chairman Vice-Chairman Secretary Treasurer Member
__________________________________________________________________________________________________________
Contents
p.1 Editorial p.2 The launching of the European Clinical
Trials Register on PCa p.3 What counts as a successful outcome in
cancer care? p.5 An end to Second Class Citizenship
(continued) p.7 Review of Project Committee Perfor-
mance – status of achievements p.8 The psycho-oncological nightmare of PCa p.9 Member Reminiscences p.12 Selbsthilfe Prostatakrebs, Austria p.12 US TOO Belgium p.13 Europa Uomo CZ, Czech Republic p.13 The Danish PCa Association – PROPA p.14 Finnish PCa Association – PROPO p.15 Anamacap, France p.16 The Bundesverband Prostatakrebs
Selbsthilfe e.V., Germany p.17 Men Against Cancer – PCa Support
Group, Ireland p.18 The Polish Gladiator PCa Association p.18 The Portuguese Prostate Patients
Association p.19 Europa Uomo Slovakia p.20 FEFOC, Spain p.21 Tackle Prostate Cancer, UK p.22 The Hippocratic Corner
Editorial Malcolm G. Duncan - Newsletter Coordinator
The enthusiasm already shown by our member associations has been further confirmed. While the first issue covered 14 pages we have now reached 27. Our associations, colleagues and friends have fully realized the benefit which can be achieved by contributing to this periodical by exchanging news on activities and problems and efforts to resolve the latter. In fact we received up-to-date accounts from 10 countries. It was interesting to note how several national associations have successfully managed to develop local groups spread over the country. Germany tops the list with 250, followed by the UK and Denmark. The number of members for Denmark is most surprising (3,400), bearing in mind the modest dimensions of its population. In the table dedicated to established national screening arrangements, we saw how appropriate was the title of the article “An End to Second Class Citizenship” in the previous issue, as prostate cancer established screening tests are limited to Lithuania and Poland. In several countries you may also have to pay for it even if you acquire a prescription from your family doctor (Belgium, Denmark, Norway and Switzerland), whereas the genteel sex is well cared for in practically every country. This should be a Europa Uomo’s top priority.
Newsletter of the 23 European member Forums dedicated to improving knowledge of cancer of the prostate
Did You Know? N°2 - 2014

EUROPA UOMO / Did You Know? 02/2014 2
One of the most common complaints of several national associations was the lack of finance in order to be able to be more active. For that reason it is of paramount importance that Europa Uomo does not take an initial “no” by the European Parliament to their plea for financial aid entitled “A Call for Action”. Another initiative, proposed by the Italian association, called “Europa Uomo: A New Approach” has similar ambitious objectives. However it still awaits Board approval.
The efforts and success of the Project Committee, working in co-operation with several other European and North American research bodies, has been finally disclosed in the Newsletter. One important project which they have co-operated on now gives up-to-date information on trials and new cures in the prostate cancer sector and can be simply obtained by linking up with the email address of the European Clinic Trials Register. In future this will surely reduce the feeling of panic on being informed that you have contracted prostate cancer. The problem of psycho-oncological nightmares on hearing such dreadful news is discussed in detail by Dr. Tania Estapé from Spain.
The Hippocratic Corner, written by Prof. Louis Denis, evaluates the much discussed PSA (Prostate Specific Antigen) which was first introduced in 1960 and has been the object of more than 22,000 articles since its inauguration. The problem of the PSA test is its correct interpretation and the danger of subsequent overtreatment as in many cases the patient is more in danger of dying from other causes. In fact there is an increasing recourse to “active surveillance” as opposed to invasive procedures as surgery or/and radiation.
We sincerely hope to finally have news from our Bulgarian and Romanian colleagues in time for the next issue of the Newsletter, as we feel sure that, like in the cases of Poland and Hungary, Europa Uomo may be able to help them to achieve their most ambitious goals.
The Launching of the European Clinic Trials Register on Prostate Cancer Günter Feick, BPS, Germany
In future the immediate panic which frequently overwhelms many men, their wives or life companions and offspring when they receive the much dreaded news that they have contracted prostate cancer may now in part be avoided, thanks to the recent publication of the above Register, part of the strive to help men deal with this deadly disease. In Europe some 417,000 men are so diagnosed every year.
Günter Feick
It is the positive outcome of an All Clinical Trials Register Petition to which Gunter Feick, past Board member and at present ex-officio Board member, joined on behalf of Europa Uomo and which has led to the EU law of 3rd April 2014. In future prostate cancer patients can count on up-to-date information about clinical trials, their progress and results, simply by referring to European Medicines Agency European Clinical Trials Database (EudraCT), website: https://eudract.ema.europa.eu/. These trials include dealing with metastatic castrate-resistant prostate cancer, investigational immunotherapy PROSTVAC-VF+/- in men with asymptomatic or minimal symptomatic metastatic castrate-resistant prostate cancer seeking to improve overall survival. The Affinity trial is also evaluating whether custirsen (experimental treatment), when

EUROPA UOMO / Did You Know? 02/2014 3
combined with second-line chemotherapy, can improve survival rates and delay disease progression.
Patients who wish to participate in all such trials must meet a prescribed set of criteria to be eligible. The Newsletter will try to keep you posted on important improvements. In the meantime patients may resort to the official home page of the Europe Clinical Trials Register (see above).
What counts as a successful outcome in cancer care? Hannu Tavio, PROPO, Finland
Discussion about the topic mentioned in the heading has been raised in a LinkedIn group called Beat Prostate Cancer. Simon Crompton, English health journalist, has also handled the same topic widely and to his credit including patient stories in an article in May-June issue of Cancer World.
In the beginning of his article he summarizes: “Every patient wants to be cured. But a culture that defines success as a “cure” condemns many patients and doctors to failure. Should the cancer community be looking to broaden the concept of success to better reflect how well care plans deliver the best possible outcome tailored to each patient’s personal priorities?”
Are the organizations seeing the topic from a patient’s perspective often left out from open discussion? Or is it seen as a medical question that is purely a professional matter for doctors and researchers to speculate on? It is natural that treatments are thoroughly discussed between patient and doctor when planning and deciding about the treatment. The question however is whether the “silent thought” of cure being the only successful outcome in cancer care living in community gives justice to the patient. Or does it even compare to general treatment knowledge of
today? From a broader perspective I think it is relevant to question if the persistent thought of relating cancer and death to each other is based on this same definition of successful outcome – cure.
My personal experience is that still, 15 years after getting a cancer diagnosis, people generally think that treatments must have cured me, that I’m completely free from cancer cells in my body.
Simon Crompton: “What does treatment ‘success’ mean in cancer? Does it only mean curing the cancer? Or controlling it? Extending life? Or providing a good quality of life, even for a short time?
How we define success and failure is important because it has a profound impact on the goals that patients and their doctors set themselves and the experience of the cancer journey. Developing a shared under-standing of what success means is also essential for informed public debate about the value of different interventions in different settings and how to get the best outcomes from the resources we have.”
Active surveillance and basic medical treatment New situations and answers related to the topic of this article have appeared at least in Finland when talking about prostate cancer today. When a man with newly diagnosed prostate cancer gets a briefing and makes an agreement of moving into active surveillance, actual curative treatments aren’t necessarily even “looked for”. It may be very simply said, but for most of these men it is true that if and when active surveillance is enough for the rest of their life it means that this treatment is a success without curative elements.
It is also a fact that specified diagnoses based on better knowledge of the disease itself offer a possibility to treat with blocking hormones or other basic medicines without curative aim not only prostate cancer in an early phase but

EUROPA UOMO / Did You Know? 02/2014 4
also when the disease is advanced. The main objective is to stop or slow down the advancement of the disease. It wouldn’t be fair to patients and attending doctors if it were claimed that this third kind of treatment doesn’t include elements of success for the majority of patients.
Chronic cancer It is all more often that prostate cancer is said to be chronic for many patients. Either, as said above, it is not seen as necessary to start curative treatments or radical treatment with curative aims which haven’t reached the objective. The disease becoming chronic after radical treatment means that the disease can’t be cured with current methods, but it can be controlled and by that way it is possible to give the patient more years, even decades to his life. Not to forget the factor of the quality of life. Here is one big group of cases, where we can talk about different levels of successful treatments and once again, without a definite cure. These treatments offer patients and their close ones hope and tell them that the future is not depending only on the cure. Treatment has been planned carefully and it has succeeded in many sectors. However, it is realistic to understand that many medical treatments still have limited time efficacy but finally the effect is very individual.
Change of treatment approach The question of cure is not necessarily the most important aspect from the patient’s point of view, not even when the man has an advanced, metastatic prostate cancer. This is seen in many patient stories.
Negotiation is challenging when patients, especially aged ones, experience that best success, often in the form of a radical treatment, is not necessary. This is often related to situations where latest, approved cytotoxic or other drugs are not used or where active treatment is stopped. These events are commonly associated directly but
incorrectly to increasing and tightening cost awareness. You can hear prostate cancer patients and their close ones say that they are forbidden to get a beneficial “drug cocktail” which would offer them some more valuable weeks or months to their life. Not because they have unrealistic expectations but because they feel that they are seen as less valuable to society.
It may feel all wrong that stopping an active cancer treatment could in any way be a successful care. It is however a fact that this kind of solution works for the best for a patient who would get severe adverse events or side-effects from treatments which wouldn’t even help in the fight against the cancer anymore. It is of course essential for the patients and their close ones that all needed information is given and that they understand why the treatment approach has changed. From the patient’s point of view the basis for a successful treatment is that the patient in all different stages of his sickness knows, what the aim of each treatment is. In that way there will not be doubts about being left alone but instead it creates hope that palliative, symptom based and pain relieving treatment gives the patient an active life as the situation allows. It is important that the patient is helped to understand that the doctor can do something for him even if a cure is not possible. Sometimes you hear relatives and friends say that it is not just buying time for the patient. Instead one month can be worth as much as one year for the close ones as well as for the patient if it has become obvious that life expectance has become limited.
Treatment in the end At the moment terminal treatment is widely discussed and it is justifiable to say that terminal care is one form of successful treatment. Nowadays experts openly describe how well organized terminal or hospice care means dignified, painless death when it’s successful. It also serves relatives and friends
EUROPA UOMO / Did You Know? 02/2014 5
in their deep sorrow. It is extremely tough for the close ones if their family member has died because of unsuccessful late stage treatment even if there had been long and successful treatment periods before that. By discussing and getting appropriate information from doctors and other professionals this kind of unfortunate situations can be prevented.
What becomes of Finnish prostate cancer we can say the following as an answer to the question in the heading: a successful outcome in prostate cancer care is a chain of treat-ments based in high know-how. It starts from the diagnoses, continues to different carefully considered treatments and ends in follow-up or, if the situation requires, high quality terminal care.
Sources: Hannu Tavio, PROPO Magazine 1/2014 Simon Crompton, Cancer World Magazine, May/June 2014
Louis Denis & Hannu Tavio
An End to Second Class Citizen-ship (continued) Malcolm Duncan, Europa Uomo Italy
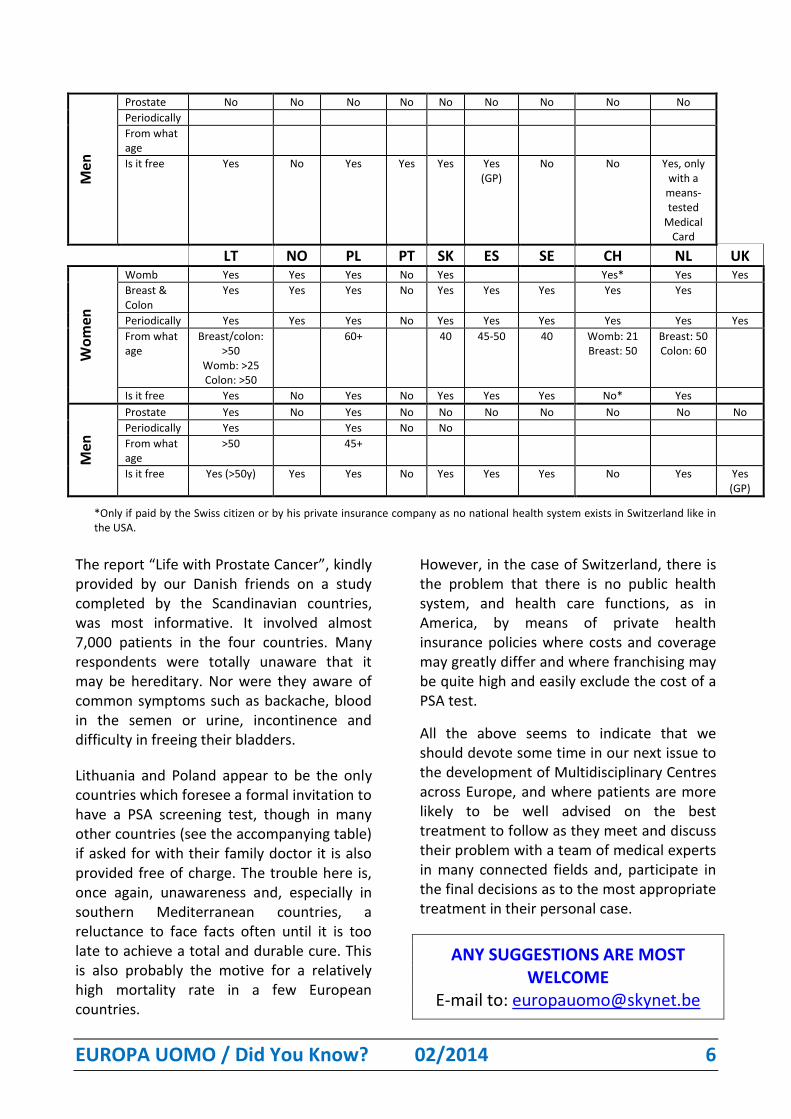
The present article is based on the replies kindly supplied on time by 19 member associations whom we most sincerely thank, and is a follow up on the article which appeared in the previous number of the Newsletter. That means that 4 replies are still missing. The answers received unfortunately confirmed my personal fears, expressed in the previous edition. This can be clearly discerned by the accompanying table.
The principal shortcoming in the treatment of prostate cancer is the common unawareness of the male population of the risk of getting a prostate cancer and also of many GPs (General Practitioners or family doctors), who frequently limit the request of a PSA screening to a desire communicated by their male patients or, very often, by their wives or companions for life.
Something needs to be done urgently to address this important health issue, also in view of the fact that it is expected that, due to increasing longevity, prostate cancer incidence will double in the course of the next twenty years and the mortality rate to even treble. That is notwithstanding medical advance. See the attached table for details, country by country, provided by the national associations of 19 Europa Uomo associations.
Table: Male and female screening testing for cancers
AT BE CZ DK FI FR DE HU IE
Wo
men
Womb Yes Yes Yes Yes Yes
Breast & Colon
Yes Yes Yes Yes Yes Yes Yes (breast)
Yes Yes
Periodically Yes Yes Yes Yes Yes Yes Yes
From what age
40 50 45/45/55 50 50 50-69 45-65 55
Is it free Yes Yes Yes Yes Yes Yes Yes Yes
EUROPA UOMO / Did You Know? 02/2014 6
Men
Prostate No No No No No No No No No
Periodically
From what age
Is it free Yes No Yes Yes Yes Yes (GP)
No No Yes, only with a
means-tested
Medical Card
LT NO PL PT SK ES SE CH NL UK
Wo
men
Womb Yes Yes Yes No Yes Yes* Yes Yes
Breast & Colon
Yes Yes Yes No Yes Yes Yes Yes Yes
Periodically Yes Yes Yes No Yes Yes Yes Yes Yes Yes
From what age
Breast/colon: >50
Womb: >25 Colon: >50
60+ 40 45-50 40 Womb: 21 Breast: 50
Breast: 50 Colon: 60
Is it free Yes No Yes No Yes Yes Yes No* Yes
Men
Prostate Yes No Yes No No No No No No No
Periodically Yes Yes No No
From what age
>50 45+
Is it free Yes (>50y) Yes Yes No Yes Yes Yes No Yes Yes (GP)
*Only if paid by the Swiss citizen or by his private insurance company as no national health system exists in Switzerland like in the USA.
The report “Life with Prostate Cancer”, kindly provided by our Danish friends on a study completed by the Scandinavian countries, was most informative. It involved almost 7,000 patients in the four countries. Many respondents were totally unaware that it may be hereditary. Nor were they aware of common symptoms such as backache, blood in the semen or urine, incontinence and difficulty in freeing their bladders.
Lithuania and Poland appear to be the only countries which foresee a formal invitation to have a PSA screening test, though in many other countries (see the accompanying table) if asked for with their family doctor it is also provided free of charge. The trouble here is, once again, unawareness and, especially in southern Mediterranean countries, a reluctance to face facts often until it is too late to achieve a total and durable cure. This is also probably the motive for a relatively high mortality rate in a few European countries.
However, in the case of Switzerland, there is the problem that there is no public health system, and health care functions, as in America, by means of private health insurance policies where costs and coverage may greatly differ and where franchising may be quite high and easily exclude the cost of a PSA test.
All the above seems to indicate that we should devote some time in our next issue to the development of Multidisciplinary Centres across Europe, and where patients are more likely to be well advised on the best treatment to follow as they meet and discuss their problem with a team of medical experts in many connected fields and, participate in the final decisions as to the most appropriate treatment in their personal case.
ANY SUGGESTIONS ARE MOST WELCOME
E-mail to: [email protected]
EUROPA UOMO / Did You Know? 02/2014 7
Review of Project Committee Performance Status of achievements Gunter Feick, Project Committee Chairman GOAL 1: COORDINATED EUROPEAN RESEARCH PROGRAM WITH PATIENT ADVOCATE REPRESENTATION
Achieved: - EUomo representative accredited to EMA for participating in clinical trials´ reviews. - Over 400 MEPs signed DECLARATION 80/2010 COORDINATED CANCER RESEARCH. - EAU secretary general, Prof. Abrahamson agreed on EAU becoming the hub for coordinated prostate cancer research and work with EUomo. - EUomo and member organizations signed ALL CLINICAL TRIALS REGISTERED/RESULTS REPORTED petition. - 3 April 2014 petition turned into EU law. Information on clinical trials/results is now publicly available in new European Medicines Agency European Clinical Trials Database (EudraCT): https://eudract.ema.europa.eu/
GOAL 2: THERAPY GUIDELINES IN ALL EUROPEAN STATES BASED UPON THE LATEST EVIDENCE
Achieved: EAU guideline for treatment of prostate cancer updated with EUomo input. Continued EUomo input for updates assured.
GOAL 3: CENTERS OF EXCELLENCE IN ALL EUROPEAN STATES
Achieved: - EUomo initiated and contributed to the preparation of a concept paper, delineating requirements for prostate centers, published in the European Journal of Cancer. - EAU joined prostate centers work group (PCWG) - EUomo is member in PCWG
- Prostate center accreditation and design requirements consented by PCWG.
GOAL 4: QUALITY OF TREATMENT AT WORLD TOP LEVEL IN ALL EUROPEAN STATES
Achieved: - International Consortium of Health Outcome Measurement (ICHOM) consented Patient Related Outcomes (PROs) for localized low and medium risk prostate cancer: http://www.ichom.org/wp-content/uploads/2014/04/DCUM_LPC_KL_040914_website.pdf - Report on health outcome measurement by ICHOM work group and patient statement published in medical journals this year. Work financed by Movember. - ICHOM PROs added to prostate cancer treatment guidelines and reporting requirements for certified prostate cancer centers, Germany. - ICHOM PROs for advanced prostate cancer are in progress. Prof. Denis will be patient representative for Europe.
GOAL 5: NEW SUPPORT GROUPS IN NEW EU STATES
Achieved: Poland based regional office established.
Group picture GA EUomo, London, June 2014

EUROPA UOMO / Did You Know? 02/2014 8
The psycho-oncological nightmare of prostate cancer Dr. Tania Estapé, psycho-oncologist, FEFOC/ Europa Uomo Spain
A cancer diagnosis is a stressful event in the life of any person associated with various difficulties such as
anxiety, depression, fear (of
recurrence, uncertainty about the future etc.) as well as physical problems involving the effects of treatment. In the case of prostate cancer there is a high probability that treatment significantly impacts the quality of life of patients. We mainly refer to the chances of urinary incontinence and/or dysfunction erectile, but also others, such as loss of libido, gastrointestinal effects and mood disorders.
The psychological impact due to prostate cancer adds, then, two aspects: those associated with cancer in general, and those specifically related to site and treatment.
- As for the psychological impact of cancer, these are due to the usual attitude of people that attribute a meaning of death, stigma and uncertainty, its causes and possible cure. Disorders more frequent in mood are anxiety and depression. There may also be periods of insomnia, anorexia and interruption of daily activities as well as persistent fear about the possibility of relapse.
- Prostate cancer means, for the purposes of treatment, a threat due to the perception of damage to men’s self-image and masculinity. This can seriously affect relationships and self-esteem. Possible problems such as incontinence and sexual impotence may harm a patient’s self conception as a man. He may be filled with shame and discomfort. If he is still an active worker, he may have
functional difficulties at work, for example, having to urinate often, with all that this implies, added to the fear that workmates realize about it. If no longer employed, he may have an emotional disturbance and wish to retire (with all that implies in our society for a man). Physical losses due to prostate cancer may have a high repercussion especially on men who feel old and useless as he has stopped working. Moreover, we should add important aspects related to the medical situation but that may increase anxiety in patients:
- The choice between different treatment alternatives: the possibility of more than one potential therapeutic strategies (medical decision-making), with different side effects which have a double impact on the welfare of the patient. On the one hand, it certainly adds anxiety on whether he has chosen the best option. Moreover, if the patient is well informed by the physician, it may help to increase the feeling of control, which is very important, especially in males. In some cases, in which information has not been reported or has not been done properly, patients experience an increase in the level of distress. It is very important that the patient has the feeling that there is a high degree of communication between him and the doctor.
- Knowledge regarding tumour markers: Increasingly, patients with cancer receive information regarding numbers, and control when the numbers indicate that something is wrong. The prostate cancer patient is usually informed about the PSA and when waiting results or if they increase, even if it is a minimum increment, he may be distressed. This is called the "PSA anxiety" and can become a real psychological problem. There are patients who do graphics with their PSA and others go to different analysts to corroborate results. In English, with some kind of humour, to indicate the source of distress that can generate this analysis which is called the Patient Stress and Anxiety

EUROPA UOMO / Did You Know? 02/2014 9
(Stress and anxiety of the patient) or the analysis that Promotes Stress and Anxiety. It is so important that there is a questionnaire to assess specific anxiety due to PSA.
Prostate cancer can be a major challenge in the life of the affected male. It may impair many aspects of the patient’s life, both personal and relative to social activities. Thus it may be important to receive psychological support, individual or with a couple, when resources common in the patient's life, are not sufficient. One way to try to prevent a high degree of discomfort and distress of the patient is to maximize the level of information about the disease, treatment and side effects. A good communication with the doctor is one of the keys to achieving peace and a sense of control by the patient.
The establishment of therapeutic goals is complicated by problems presented by the patient. Regardless of the specific demand expressed they affect, in general, and their most frequent reasons for consultation are related to sexual issues, couple relationships and adaption to a new physical situation. PSA anxiety is something recognized but usually there are no specific demands about it. The patients with prostate cancer convey their fears and problems and very specific psychological aspects of health and more often physical ones too.
An example of this is the great interest of these patients for all the information regarding healthy lifestyles. In this sense, the work of the psychologist should include psycho-educational intervention as a therapeutic strategy. The group modality is usually the most used by the special connotations of men and prostate cancer. Support groups in prostate cancer have been most recently formed within the oncology field. However, once treated, it must be said that their constancy and interest to remain in the group becomes very high.
Definitely prostate cancer is a major goal for its increasing number of cases, and by the side effects of treatment thereof and in the quality of life of the patient and his partner.
FEFOC, which is the Spanish representative of Europa Uomo, has a sound area of work in prostate cancer. Our group of patients’ activities began in 2000, and since 2008 we have a specific web devoted to prostate cancer (www.cancerdeprostata.org) available in both the Spanish and the English languages. We have an individual psycho-therapy program for patients and /or their couples or relatives. Our last contribution to prostate cancer has been our 16 recommendations code to patients and men in general.
Member Reminiscences Malcolm Duncan
Thirteen member associations have already kindly provided details on historical information and events. The main purpose of this new column is to share experiences and initiatives which help us to improve awareness and visibility as well as funding and maybe glean interesting events which we could also do independently or in co-operation with others. We have already discovered that mutual co-operation is already common among Poland, Slovakia and
EUROPA UOMO / Did You Know? 02/2014 10
Austria. Compliments to them. Let’s hope others will take the hint and follow suit. The Irish, Finnish and Spanish (FEFOC) appear to be among the first pioneers in this battle for life, respectively founded in 1993, 1997 and 1998 which is clearly expressed in FEFOC’s Code on Prostate Cancer which has been distributed to about 500 public and private hospitals. The Portuguese association had a most original beginning in 2004. Initially membership was almost completely composed of ex military (mostly from the army). The German BPS (Bundsverband ProstataKrebs Selbsthilfe) appears to be the most developed national association with over 9,000 members and covers the entire territory. It has a network for research and treatment of advanced prostate cancer. Another group named Castration Resistance Prostate Cancer was founded in 2011 and consists of 12 university clinics for urology. The UK association is a little sensitive to the term “castration resistant” which they interpret as offensive to men who are on a long term androgen deprivation therapy. BPS is member of the national prostate cancer guidelines commission insuring which 96 Prostate Cancer Centers in Germany are committed to applying the guideline while treating patients in a multidisciplinary fashion and report their health outcomes by use of identical quality indicators for transparency and bench marking. These institutes are still lacking or of limited number in most of the 23 national association members of Europa Uomo, but the situation should improve in the near future. Other indicators for international use have also been devised in co-operation with ICHOM and used in the case of low risk prostate cancer. As previously affirmed general awareness of this deadly disease is still scarce in many
countries, which tends to aggravate mortality rates. Visibility is another closely related problem. This calls for action by Europa Uomo but together with local national associations and not independently, without any involvement or knowledge by the local association, as was reported by one member country, which led to some embarrassment on the part of the interested association. This shyness defect is most common in Mediterranean countries where men are reluctant to consider let alone talk about the danger of getting prostate cancer. However Ireland also denounces a similar problem. Though the number of diagnosed as suffering from prostate cancer is thought to have increased, recourse to the HelpLine phone service has surprisingly declined and the question is at present being discussed on how to overcome this setback. One of the most dynamic national associations on the question of promoting awareness appears to be Slovakia. Apart from their co-operation with Gladiator in Poland, to which Austria is also active, they edit a website which includes hundreds of educational and scientific articles and they also dispose of hotline phone networks and internet for those who prefer to communicate their questions and doubts via email. They have also co-operated with various TV channels and the ONKO magazine to favour a better public knowledge of prostate cancer. Lastly they have established contacts with European MEPs in the hope to reduce the cost of health care drugs for prostate patients. It is a pity through the lack of a Newsletter at that time, they were not involved early on in the very worthwhile “Call for Action” venture. Their latest initiative has involved the media and promotion even in hospital ambulances.

EUROPA UOMO / Did You Know? 02/2014 11
Finland, with 1,800 odd members, a remarkable achievement for such a small population, is very active with regard to the problem of awareness. It organizes regular open lecture and provides further information on request. Its success is also partly thanks to its close co-operation with the Finnish Cancer Society. It publishes 4 annual magazines as well as Newsletters, organises public meetings and road shows country wise. They have established a very good slogan to help their awareness “Less cancer – more Life!”. With the same intention, the Austrian association has recently presented a book named “Everyday life is precious”.
Both Anamacap in France and the Slovakian association have achieved official recognition. In France by means of the label “Institute of Public Interest” and in the Slovakian Republic by the Ministry for the Interior (2012) but, unfortunately, at least until now, they have achieved no State financial aid.
The Czech Republic recently achieved increased awareness by an original Billboard campaign on the main roads near their capital Prague and Brno.
Another way of attracting and maintaining interest and contacts is by organizing regular member meetings. This was started in Belgium by 3 monthly meetings named “Café Santé”, where patients and doctors can discuss common problems. One possibly disappointing factor is that no excellent quality Belgian beer is served. They also produce a magazine called “PROSTAATinfo” with a circulation of 4,000 copies mainly distributed in Belgian hospitals and managed by its Scientific Committee headed by Prof. Van Poppel. France has a similar initiative in mind for the near future. The Slovakian Republic association has established a series of clubs and is now considering the use of internet in
combination with their Helpline phone service. Previously the internet and email alternative was thought as of little use due to the age of most patients and their limited predisposition to Internet. Now however they realize that the situation has radically changed and many men are often reluctant to discuss their prostate problems over the phone to an unknown spokesman or spokeswoman.
The Irish association, MAC, is located in Dublin and was established in 1993, mainly thanks to the effort of Tom Hudson, later EU chairman, and is managed by a 10 member Steering Committee, which in view of a limited membership of about 250 due to the size of its population, appears a more democratic way to conduct such an important association, as opposed to a mere 7 member board for Europa Uomo which has 23 country association members. However that is a personal opinion based on previous professional experience in an international sphere. It regularly organizes hospital visits on the invitation of nurses.
One of the chief problems is developing regional centres with local activities. This is an ongoing problem in Italy. The most successful cases appear to be Germany (250), followed by the United Kingdom which at present has some 50 local groups of patients and their families representing some 15,000 national members. This was surely helped by the decision, after much thought, of merging 4 national groups to form a Prostate Cancer Support Federation.
Thanks to Prostate UK and their activities, the Imperial College of London has assured them financial support since 2011, giving them £60,000 in annual grants. In 2011 they also agreed to a pay for a CEO for the next 5 years. In 2011 they changed their name to Tackle Prostate Cancer UK” which was thought would acquire a more positive public reaction and support. One very original event

EUROPA UOMO / Did You Know? 02/2014 12
promoted by EU UK.
Together with other Cancer associations there is a walk called “A Shining Night Walk” already in its fourth annual edition held in the historical centre of London beginning near Tower Bridge. Participants can choose between doing the full walk (26.2 miles) and the more modest walk of only 13.1 miles). Since it beginning in 2010 this initiative has raised £13.5 million to help cancer research in the UK and this year is expected to raise a further £4.7 million. Worth considering?
Austria has a similar initiative but at present I have no information on its achievements.
PLEASE VISIT OUR WEBSITE www.europa-uomo.org
AUSTRIA
„Selbsthilfe Prostatakrebs“ Austria: 2011 Reorganising of the Board of SHP. Reduction of members from 9 to 6. Chairman, Secretary and Cashier plus one deputy each
2011 Reorganising of website “www.prostatakrebse.at” and official co-operation with the “Austrian Assoziation of Urologists” (bvU Berufsverband der Österreichischen Urologen).
2014 Presentation of the book „Everyday Life is precious” from Astellas in June 2014. Beginning of cooperation with the “Academy for Sexual Health”, press conference in June 2014.
Preliminary studies of our project of the book “Prostate Cancer” (Prostatakrebs) in German. In cooperation with the Urological Department of the Medical University in Vienna, the Austrian Association of Urologists.
Re-establishing of the Upper Austrian SHP prostate cancer patients society.
Selbsthilfe Prostatakrebs www.prostatakrebse.at
BELGIUM
The Belgian EUomo member, is now called US TOO Belgium (official) – Wij Ook (for the Flemish) – Nous Aussi (for the French speaking population) and Wir Auch (for the German speaking part).
Started in 2002 by Jack Pais as an international member of US TOO USA. The goals included awareness of the prostate diseases, patient information and education, and access to specialized and cost-effective care.
Over the years expansion primarily in the Flemish region led to subgroups Wij Ook in Antwerp, East and West Flanders, and Mechelen.
For patient information we started our “Café Santé” programs. A scientific, social meeting for the members. However no beer is served on these 3 monthly meetings. Out of these meetings came a traditional European prostate cancer patient day on the 3rd Saturday of September followed by a Walk for Cancer on the following Sunday.
We edit a patient members magazine “PROSTAATinfo”, mainly composed of contributions from professionals especially our Scientific Committee headed by Prof. H. Van Poppel and our members. The 4,000 distribution goes to all urological departments in the Flemish hospitals and personal, that is providers of prostate management in the health care.

EUROPA UOMO / Did You Know? 02/2014 13
Our latest project involved awareness of exercise as a major contribution to health for prostate cancer patients. The program was developed with the support of UCL (Prof. B. Tombal) and went from MyCoach to a European program “Feel+”.
We hope to continue this ambitious program with our Board, different committees and especially the response of each member. Each one of us feels the need and the obligation.
Activities in Urology Week:
1. Symposium “Prostate Cancer: actual insights” (September 13) 2. European Patient Day symposium (September 20) with the support of the Belgian Society Urology, university hospitals and Wij Ook. 3. 60+ walk against cancer (September 21). Foot rally, lunch and prizes organized by the Oncology Centre Antwerp – Wij Ook.
Us Too/Wij Ook Belgium www.wijook.be
CZECH REPUBLIC
Europa Uomo CZ increased public awareness about prostate cancer significantly by means of its website with a lot of educational info, online advisory office, Billboard campaigns, press conferences every year on the occasion of Urology week, as well as lay awareness brochures.
Activities Urology Week:
Europa Uomo CZ
www.europauomo.cz
DENMARK
The Danish Prostate Cancer Association PROPA
PROPA was founded in 2000 and reached a membership of approx. 50 members in the first year. The association developed over the subsequent years and has now reached a membership of 3,400. PROPA is divided into six regions and has a total of 18 local groups distributed over the country. The association is governed by a national board consisting of 10 persons – 6 of these are the chairmen of the regions, one is the representative of the relations of the members and the remaining 3 are chosen from the total membership at the annual national meeting, which is the top governing body of the association. There are each year

EUROPA UOMO / Did You Know? 02/2014 14
approx. 100 meetings for the members of PROPA around Denmark for example with talks by leading medical specialists, dieticians, physiotherapists etc.
In 2014 PROPA has chosen patient involvement as a general theme. It was used at the Citizens’ Meeting on the island of Bornholm (as covered in Newsletter No. 1), at the national meeting of the association and now in the Prostate Cancer Month September as a part subject in the five theme meetings held in PROPAs regions.
During the autumn six family runs are arranged at golf courses and other pleasant landscape sites around the country with a view to create attention about prostate cancer and the association and to collect money for the activities of PROPA.
PROPA also arranges a Master Class for the extended management of the association, where the top professional specialists provide contributions.
In November PROPA cooperates with MOVEMBER in order to visualise the prostate cancer disease for the Danish population.
PROPA’s vision – the goals PROPA would like to reach are:
That the treatment of prostate cancer is characterised by a correct and safe diagnosis understood by the patient, and the best possible individual treatment ensuring optimum quality of life for him and his family.
That PROPA has general recognition, support and success in its work.
PROPA’s mission – the overall subjects PROPA will deal with:
PROPA works as a patient association for the best treatment and support of prostate cancer patients. PROPA does this by:
- Influencing the health political agenda towards the best possible treatment of prostate cancer.
- Disseminating general knowledge about prostate cancer and its treatment and thus removing the taboo about the disease.
- Working for improved quality of life for patients and their relatives.
- Working to ensure that diagnosis, treatment and rehabilitation – regardless of address – fulfils the highest inter-national standards.
- Working to achieve that at least 25% of prostate cancer patients are members of PROPA.
- Working to achieve that practicing doctors are seriously aware of the danger signals of prostate cancer.
PROPA’s value basis – what PROPA wishes to be known for:
PROPA wishes to be widely recognized for its informative and serious work by members, health authorities and society in general.
Prostatakreftforeningen - PROPA
www.propa.dk
FINLAND
Finnish Prostate Cancer Association - PROPO
Founded: 10.10.1997 Organisation: President: chairman of board, Matti RJ Niemi
Board: 3 patient members, 2 physicians, 1 nurse and their personal assistants.
Executive Director, Irma Lehtimaja

EUROPA UOMO / Did You Know? 02/2014 15
Address: Finnish Prostate Cancer Association, PROPO Saukonpaadenranta 2
FIN-00180 Helsinki E-mail: [email protected]
Members: Currently 1,800 all over Finland
Prostate cancer patients and relatives Physicians and nurses related to prostate
cancer Supporters, persons, institutions, etc.
Mission: Link advocacy organisation for prostate cancer patients
Distribute data, produce information and increase common awareness of prostate cancer
Means: Information, education, support services Organize meetings for prostate cancer patients and their relatives Follow and promote research and information related to prostate cancer Make initiatives to improve the situation of prostate cancer patients Increase common awareness of prostate cancer disease with open lectures Give statements when needed
Collaborating with: Member organization of the Cancer Society of Finland as well as other member organizations of Cancer Society of Finland State and local authorities and other health organizations are also involved. Active Member of EUROPA UOMO and ECPC (+ WWPCC) Taking part in regularly organised Nordic groups
Permanent actions: Publishes yearly 4 magazines and newsletters for members
Yearly large meetings and road shows with Supporters. Small groups are also organized.
Key issues today: Strengthen finance, campaigns and public support Develop organisation and work of the board and its efficiency Analyse and take benefit of 4 different covering members’ inquiries and studies Publishing of latest made in 2014
Suomen eturauhassyöpäyhdistys ry Finlands prostatacancerförening rf Finnish Prostate Cancer Association PROPO Membership growth 1997-2013
Slogan: “Less cancer – more life”
Finnish Prostate Cancer Association - PROPO www.propo.fi
FRANCE
Anamacap was set up in 2002 with the support of 3 Urology and Oncology University Professors. Anamacap and got the label of public interest from the French authorities as from April 2010 (highest level for an association).
Anamacap has 2 branches: a Scientific Advisory Board including high level urologists, oncologists and radiotherapists on

EUROPA UOMO / Did You Know? 02/2014 16
one side and a Board including 12 volunteers acting and managing the association. In 2014, Anamacap has more than 1,200 members.
Revenues are coming from members' fees and subsidies by laboratories and private persons; anamacap does not receive for the time being any subsidy from public authorities.
Anamacap General Assembly is held every year on the third Saturday of the month of September. In addition, some information meetings are held in France main cities (3 or 4 per year).
Anamacap makes available an information line by phone every morning (except weekend) and provides a forum and a Q and A service through its website (only for members). A newsletter should be launched very soon now.
Anamacap had several meetings with the highest Health Authorities in France (including French Health Minister) on important issues (the approval of new drugs, screening, etc...). Anamacap is the leading association in France as regards Prostate Cancer Issues and Patients Advise. We are eager to attract more volunteers in order to develop additional actions all over French Territory.
Activities Urology Week:
1. Participation on 15/09, a Prostate Cancer Awareness Day at the Bichat Hospital in Paris ° a booth was set up ° a brochure and information were distributed to passers-by ° Projections of small video films (anatomical sheets, treatment of prostate disease, expert advice, micro sidewalk ...) ° Press interview with Prof. Ravery (Head of the Service) ° Musical entertainment by a group led by a physician, a game with questions and
answers on prostate issues to win a lot of gifts
2. The organisation of a scientific conference for the members of Anamacap on 20/09 ° Update on focal treatments and their indication (45’), by Prof. Olivier Cussenot, Urologist/Oncologist at TENON Hospital, Paris (AP-HP) ° A speech on “The Management of prostate cancer for older men” (45’), by Prof. Pierre-Mongiat Artus, Urologist at Saint-Louis Hospital, Paris (AP-HP) ° Therapeutic education and oral chemo-therapy for prostate cancer (45'), by Dr. Gilles Galula, Oncologist at TENON Hospital, Paris (AP-HP) ° Introducing the web-platform for decision support and patient education on prevention and prostate cancer treatments” (10’), by Prof. Olivier Cussenot ° Nutritional and medicinal supplements in addition to hormonal treatment or chemotherapy to reduce their side effects (10'), by Prof. Olivier Cussenot
3. Giving a public lecture on 22/09 in Rennes ° Active Surveillance and the presentation of the web-platform for decision support” ° Support of prostatic hypertrophy and avoiding dysfunction before curative treatment of prostate cancer ° New treatment for localized prostate cancer
Anamacap www.anamacap.fr
GERMANY
The Bundesverband Prostatakrebs Selbst-hilfe e. V. (BPS) has subscribed to goals and reports achievements as follows:

EUROPA UOMO / Did You Know? 02/2014 17
Goal 1: A medical network of competence for treatment and research of advanced prostate cancer.
Achievement: The German Working Group on Castration Resistant Prostate Cancer (GWG-CRPC) was founded 2011 consisting of 12 university clinics for urology. Specialized treatment for patients with advanced prostate cancer is available with research performed simultaneously and coordinated within the GWG-CRPC.
Goal 2: National diagnosis and therapy guideline updated regularly in accordance with latest evidence base medical knowledge.
Achievement: Third guideline update since 2011 completed with of 3 BPS members in a guideline commission. Patient guideline/ information based on the medical/scientific guideline completed with BPS contribution.
Goal 3: Quality indicators for measurement and comparison of prostate cancer treatment
Achievement: a. Indicators have been defined and are
applied in 95 certified prostate cancer centers.
b. Identical indicators have been defined for worldwide use by the international consortium for health care measurement (ICHOM) for the low risk prostate cancer
Goal 4: Treatment in certified, specialized prostate cancer centers.
Achievement: Since 2010 95 concept development centres have been accredited and treat patients according to the guidelines, measurements and quality report treatment using identical indicators.
Bundesverband Prostatakrebs Selbsthilfe e.V. www.prostatakrebs-bps.de
IRELAND
Men Against Cancer (MAC) Prostate Cancer Support Group
Organisation The group is based in Dublin with members in a number of other large towns and cities. It is, as far as we know, the only group dedicated solely to supporting men diagnosed and treated for Prostate Cancer, in the Republic of Ireland, although there are at least 60 general Cancer Support groups. The group is run by a Steering Committee of ten members elected at the Annual General Meeting in May each year. The Committee elects the Chairman, Treasurer, and Secretary. Currently there are approximately 36 members with about half living in the Dublin area. Overall approximately half have been trained in Peer to Peer support.
Work This consists of Peer to Peer telephone support for men who are referred to the Irish Cancer Society (ICS) Helpline Nurses. Visits to the ICS ”Drop In” Daffodil Centres located in the main Public and Private Hospitals on request from Nurses. Participation in Public Awareness meetings, and attendance at the ICS Annual Conference for Cancer Survivors. Limited Fund raising as required, usually by means of sponsored 5 km Walks. Members also provide speakers on request from ICS for interview on National and Local Radio and by National and Local papers. All MAC members who deal with survivors have been trained by ICS professionals.
History MAC was founded in 1993 in St Vincent’s Hospital in Dublin, by a small group of Men who had been treated for Prostate Cancer. The group was affiliated in 1996 to the Irish Cancer Society through the efforts of the Founder members and by Tom Hudson who

EUROPA UOMO / Did You Know? 02/2014 18
was CEO of the Society at that time. From that time the Society provided meeting accommodation, limited expenses, literature, and training, and continues to do so. The group became an independent support group in 2012, but continues its close relationship with the Irish Cancer Society.
Future Although the number of men being diagnosed is increasing, the number contacting the Helpline has decreased, and the group is currently engaged in a role review process to decide how to best help men diagnosed in the future. This review will be the subject of a special meeting in October 2014, using the services of an outside facilitator.
Men Against Cancer www.menagainstcancer.net
POLAND
The Polish Gladiator Prostate Cancer Association
Our association actually has 738 patients. Our activities aim to unify our patient – members and educate them of the basic medicine rules to assure early detection and correct diagnosis and prevention of cancer diseases and also the necessity of prevention testing.
Educational meetings take place in the Institute of Oncology named after “Maria Sklodowska – Curie” in Warsaw every month from January to December 2014 (with Holiday break from July to August).
In addition to educational meetings in Warsaw we organize similar meetings in different places in Poland(Lodz, Poznan, Gdansk, Wroclaw, Krakow).
In the year 2014 on 10th June we organized an extra educational meeting. The lecturers at the meeting are the best specialists (professors from the Medical Academy and Oncology Institute). A similar educational meeting will be organized by us on the occasion of European Urologic Week. The meeting is fixed for 14th October at 12.00 AM in “Maria Sklodowska – Curie” Institute of Oncology in Warsaw.
On our website: www.gladiator-prostata.pl we presented professional information about prostate and urinary tract cancer diseases – diagnosis and prevention testing.
Our phone helpline 48 502 438 648 works daily from 8.00 AM to 20.00 PM and arouses much interest of patients and their family members.
We have no financial support from our government.
We prepare materials, the edition and distribution of our bulletin “Gladiator” (an edition every 3 months) and also the publication of booklets, leaflets and posters.
We inform that in Poland there are 9,000/positive diagnoses per year of cases of prostate cancer. Mortality c. 4,000 Men/per year.
„GLADIATOR” The Association of Patients with Prostate and Urinary Tract Diseases www.gladiator-prostata.pl
PORTUGAL
Progress in the last 10 years: - The Portuguese Prostate Patients Association (APDP) started in 2004, and during its first 2 years was mainly composed of retired members from the Portuguese

EUROPA UOMO / Did You Know? 02/2014 19
Armed Forces (mainly the Army), in a number fewer than 100. During these two first years external activities were very limited and the Association had time to organize and start to plan external events. After 2006, APDP was then able to start an external activity mainly based on public sessions to transmit information about the prostate and its diseases. We were able to cover the whole country and we performed more than 30 sessions from North to South, with an average of 70 to 80 patients per session. These sessions were possible to organize with external funds (mainly Pharma industry) and lasted until 2009.
- In the meantime we built and published our website and started to prepare a free SOS telephone number, that started to be available by the end of 2009.
- With the decline of the Pharma industry contributions to our external activities started to lose frequency and in the subsequent years we were forced to limit our public sessions to 2 or 3 per year.
- In the meantime we were able to more than duplicate the number of Associates and we are now close to 250.
- Due to the success of the SOS phone line we started a second one and now we operate one during week days from 3:00 to 6:00 PM and a new one every day from 6:00 to 11:00 PM.
- Knowing that some people do not like to call a public phone number, we just started a "written" box in the main page of the website were people may receive also writing answers to their personal e-mail addresses.
- Due to the economic crisis, we have no new objectives, as we are afraid of being incapable to maintain the existing activities. Visibility and general awareness is still a big issue that we face every day. We were able to obtain the membership of one public
figure (one ex-minister and ex-UN General Assembly President), but the gentleman is now retired and now has a very low public profile. We see our future with preoccupation.
Activities Urology Week:
- participation in two or three TV programs - organisation of a public session on September 25th (in the Auditorium of the British Hospital in Lisbon): a round table with the participation of 5 urologists (some very famous locally) and public. The Portuguese Patients Association (APDP) sat at the table representing patients. The public session ended with a questions/answers period with free participation of the audience.
Associação Portuguesa dos Doentes da Próstata (APD Prostata) www.apdprostata.com
SLOVAKIA
Europa Uomo Slovakia is a civic organization which was registered at the Ministry of Interior of the Slovak Republic on 17 February 2006. Association is funded primarily through donations and contributions from individuals and legal entities. The activities of the organization are based primarily on voluntary activities of members of the civic association.
As a part of a pan-European organization Europa Uomo organizes various meetings of experts and laymen. These lectures are focused on medical topics, but also on practical matters. For example, the establishment of clubs, their work, how to find resources for their activities, and what

EUROPA UOMO / Did You Know? 02/2014 20
kind of activities have to be developed. They motivate members and candidates to take care of themselves and their health more actively. We are realizing further education and advocacy according to the patients´ interests. We encounter patients with the same disease and raise awareness of the diagnosis in a language which is for ill people short and understandable which is very important.
The scope of our Slovak organization is focusing on activities for which we are able to find the resources and which we consider as an effective communication. For example, whereas prostate cancer mainly affects men in older age, we must also consider other forms of communication such as the internet, which is not very used among older people. Therefore, members try to send at least occasionally printed materials about the disease. We also invite them to the meeting. We are trying to create good conditions for dialogue and they can also share their experience. As you know, for many men it is not always easy to talk about their problems, especially when it comes to problems with the prostate. Such meetings may therefore be a good start to feel that a man is not alone with his problem, but we are here to help them.
Our EUS has established three regional centres and added into their ranks leading urologists – oncologists during its existence. These doctors do awareness actions for people, lead professional website about prostate cancer and its treatment, provide personalized advice, and they are available on unpaid telephone line or the email address. We also work with the Slovak Association of Urology. Its chairman Prof. Kliment is a member of our EUS. We jointly issued several leaflets about prostate cancer and we published a book, which is available for our members but also serves to urological clinics and also medical students.
We actively promoted through the media, ambulances of urologists and by post EPAD 2012, and 13. We took part in urological days or days of the fight against prostate cancer. Excellent cooperation and mutual support has EUS with Gladiator Poland and also Prostatakrebs Austria. Personally, we meet every year in every state. We distribute Gladiator magazine from Poland for our members in Slovakia; we exploit proximity of our national languages.
Our main effort is directed towards meeting Manifesto EUomo.
Europa Uomo Slovensko www.europauomo.sk
SPAIN
In 1998 we started our activities as FEFOC. To do this our first priority was the construction, development, diffusion and continuous activities on the online page: www.cancerdeprostata.org. The page is written both in Spanish and English. We have good penetration in South America and of course in Spain. Many consultants are relatives of the patients themselves. One relevant task is to give psychological support and research. We had a lot of public presentations on prostate cancer. And, very difficult, we maintain a very active support group. The production and diffusion of educative material is good. Our last Code on prostate cancer has reached some 500 Spanish hospitals. Our free helpline also works well. Right now we are in the process of reconstructing and radically changing our online page in order to modernize it widening our contacts and diffusion through the social networks. Another important and difficult task we are dealing with is to have good contacts with representatives of the 15
EUROPA UOMO / Did You Know? 02/2014 21
Autonomous Communities and the two Autonomous Cities. The big problem is of course to find financial support to sustain and extend our activities. We have not until now obtained a public figure willing to help us. This is very important of course. Nevertheless we know that Spanish men are very reluctant to speak up if affected by prostate cancer. For instance, we know three very relevant professors of Medicine, all them prostate cancer patients, absolutely negative when we repeatedly asked them to openly share our public presentations.
What's more the ambiguous relation with the industry. We have written to Erik Briers about this matter. As some labs told us they are already cooperating with Europa Uomo (central) and for this reason are not ready to help also the National group. This is a very important question to be solved.
FEFOC www.cancerdeprostata.org
UNITED KINGDOM
In 2008, the UK’s four largest patient-led prostate cancer support groups, representing over 2,000 members and patients, formed the Prostate Cancer Support Federations. These organisations are: PCaSO Prostate Cancer Network, PCSA Central England, Prostate Cancer Support (formerly PSA North West) and the Prostate Cancer Support Association (PSA).
The idea of such a federation was first mooted in 2001 when the establishment of an umbrella organisation was proposed, that would focus the work of the many independent local patient-led support groups across the country, and, through synergy,
allow small groups to harness the totality of their resources.
Initial progress was slow, for a variety of reasons, chief of which was the difficulty of framing a constitution that was sufficiently robust whilst recognising the fierce independence of some patient groups. However, under the wise guidance of Prof John Dwyer, harmony was achieved and the Federation was formally established as a charity in 2008. Since then we have made great strides. In particular we have developed a modus operandi that reflects well the aspirations of the original founders, whilst maintaining the essential independence of member organisations.
The existence, and subsequent development of the Federation is very much due to the generosity of Prostate UK (later renamed as Prostate Action, and in 2012 absorbed into Prostate Cancer UK). Thanks to them we have held two conferences or workshops every year since our Launch including an event at Imperial College London in 2008. They have supported us with hard cash ever since, in particular enabling us to make grants of nearly £60,000 to member groups. In 2011 they agreed to funding the employment of a Chief Executive for five years, to lead the Charity and transform it into the independent Voice of Patients.
In 2013, we adopted the working name of the “Tackle prostate cancer” which was felt to have more impact on the general public (although to our members we are still affectionately known as “The Fed”). We now have over 50 member groups, who, in total, represent some 15,000 prostate cancer patients and their families. We have campaigned on a number of issues with success – a small example being that we persuaded the National Health Service to avoid the term “castration resistant”, which we see as an insult to men on long term androgen deprivation therapy. Of much more

EUROPA UOMO / Did You Know? 02/2014 22
significance is our current main thrust, the Early Detection Campaign, which aims to promote more widespread but also more intelligent use of PSA as the only currently available indication of early stage, i.e. curable, prostate cancer.
Tackle Prostate Cancer www.tackleprostate.org
“Strength and growth come only through continuous effort and
struggle” Napoleon Hill
The Hippocratic Corner Louis Denis
I was invited by our editor to contribute to our Europa Uomo Newsletter in the tradition of Hippocrates from Kos, father of modern western medicine. He lived from 460 BC to 370 BC and became famous by his success to replace the cult of Asklepios, the Greek god of healing, practised by priests/physicians in temples called Asklepiera by observation and talking/listening to his patients. A note of modesty. This type of medicine was already practised in China and India long before Hippocrates and after more than 2,000 years patients still value a doctor with a listening ear and some time. Nihil novi sub sole. Nothing is new under the sun. His heritage is recorded in the oath of Hippocrates still pledged by new doctors in medicine and a series of aphorisms assembled in the Corpus Hippocraticum. Next to the ethical obligations he was also a practical man. The oath states that he will not operate, even not on those suffering from bladder stones, and leaves this responsibility to experts. An advice that should be remembered today where learned scientists, expert in their own field, have no problem to express their contempt for urology not bothered by their obvious lack of knowledge on the complexity of the treated subject. Let there be no misunderstanding. The practice and art of urology especially on diseases of the prostate experienced an unprecedented improvement since the last few decades but the ideal is not reached yet. Referring back to our Hippocrates his most popular quote is “Do no harm”. It sounds nice but in reality it is quite impossible to go for any surgery or cancer treatment without harming the patient. We translate this for the 21st century as the patient comes first before the treatment of his cancer. A prime example of a misunderstanding is without doubt the rise and fall of the famous
EUROPA UOMO / Did You Know? 02/2014 23
PSA test. Is it Prostate Specific Antigen saving the lives of thousands of prostate cancer patients or is it the Patient Scaring Antigen causing thousands of biopsies and subsequent overtreatment leading to serious side-effects as impotence and incontinence? A recent publication of Richard J. Ablin, with the help of a professional writer Roland Rana, is called the “Great Prostate Hoax”. The subtitle is revealing “How big medicine hijacked the PSA test and caused a public health disaster” (Palgrave Macmillan, New York, 2014, ISBN 978-1-137-27874-6). The book is addressed to the countless millions of men and their families who have suffered needlessly because of the misuse of the PSA test. The key word here is of course the word misuse. Indeed the authors state that this book concerns the MISUSE of the PSA test for screening healthy men.
The message of this contribution is that the PSA test, of use in prostate diseases and not only for prostate cancer, is an excellent biomarker of these diseases but its interpretation requires knowledge of the natural (treated) history of the same diseases.
The story of the PSA molecule is fascinating. It concerns the journey of how a misunderstood molecule achieved stardom in oncology, heralded as the best cancer diagnostic marker ever and now treated as a danger to men’s health by leading medical authorities supported by epidemiologists, public health specialists and yes even associations of family physicians. As the rise and fall of the PSA test is related to its “value” as a tumour marker we provide a short review of some landmarks in cancer research, in tumour markers and finally the PSA test. Already Socrates made a distinction between cancer as a benign growth and carcinoma as
a malignancy. The period of speculation finished with observation and description by Morgagni, Pott (chimney sweeps cancer of the scrotum) and the great Virchow with many others laying the foundation of pathology and the cellular origin of malignant diseases. The 20th century brought us laboratory investigations and the start of health technology with highlights as X-rays, tissue culture, the PAP test in 1928 as well as the reported effect of castration in prostate cancer by Huggins in 1941. After describing the effect of castration on benign hyperplasia of the prostate, a common affection in men over 60 years, he demonstrated with Hodges in 1940 that castration or estrogens reduced acid phosphatase of serum in metastatic prostate cancer. This tumour marker, first described by Kutscher in 1935, was further studied by the Gutman brothers and linked to the prostate, prostate cancer and osteoplastic metastatic disease. The Huggins paper stated that with acid phosphatase present in activity greater than 10 units (King & Armstrong) in 100 cc. disseminated prostate cancer is present. The clinical improvement of the prostate cancer patients improved in general by both castration or estrogens and worsened with the injection of androgens. The era of androgen depletion treatment for prostate cancer was launched and clinical research on this subject is still ongoing in line with our increased understanding of biology and the natural (treated) history of prostate cancer. The consequence was that after World War II, when global medical communication was re-established, the castration of all men suffering from prostate cancer became routine. By the time that I took my first steps in prostate cancer research, in 1958, treatment included after the relapse of prostate cancer in castrated patients bilateral surrenalectomies and even hypo-physectomies. These surgical interventions
EUROPA UOMO / Did You Know? 02/2014 24
are now replaced by specific medication as abiraterone and LHRH agonists and antagonists. The PSA story started around 1960. A number of investigators studied prostate proteins, their enzymatic activities and its metabolism. Using electrophoresis to separate proteins in an electric field a number of proteins were described in semen and prostate fluid. We described the isozymes of lactate dehydrogenase in 1961, awarded by the AUA and the James Ewing Cancer society, showing a shift to anaerobic metabolism in cancer of potential use in the diagnosis. However it was Ruben Flocks and his team who were the first to describe a number of antigens in benign and cancerous prostatic tissue. Others followed and these efforts resulted in a number of specific proteins to the prostate found in abundance in the semen. Forensic specialists thought to use the presence of these antigens to confirm cases of rape but the characterized bands later identified as acid phosphatase, prostate specific antigen and much later prostate specific membranous antigen (PSA & PSMA) were studied as markers in clinical prostate diseases including prostatitis, benign hyperplasia and cancer. A decade of confusion followed by a diversity of names for the PSA molecule as seminoproteine, E1, p30, PA which were all identical. Ablin claims the discovery of PSA in 1970 but a later patent fight with Wang before the courts of justice gave the patent rights to Wang of Roswell Park in Buffalo, New York for his discovery and purification of PSA. This court case and the subsequent rise of the PSA test as the best tumour marker in oncology lies at the basis of the frustration of Ablin. Indeed the PSA test, based on the immunologic properties of the protein took off, after this first decade of confusion, as the rising star in cancer of the prostate evaluation and diagnosis. In the first decade
we could identify 58 papers in English, in the second decade from 1990 to 2000 some 2,262 articles and from 2000 till now more than 20,000 articles. This enthusiasm is fuelled by the simple observation that it is more sensitive than prostatic acid phosphatase (PAP) in diagnosing early prostate cancer which remains the chance for cure where symptoms are lacking, digital rectal examination (DRE) disappointing and imaging by transrectal ultrasound (TRUS) ineffective. Recently Magnetic Resonance Imaging (MRI) are studied for this purpose. Still there are weaknesses in this grand hope. After a radio-immunological test came an enzymatic immunochemical test based on two monoclonal antibodies against PSA. The Hybritech-Tandem E test was first, is still leading the field but has to compete with a number of concurrent tests on the market that may provide different results. The WHO decision in 1999 provided PSA calibrations which are now used by most companies. Equimolarity, measuring both free and complexed PSA in the serum with the identified 83 PSA antibodies finally resulted in a more or less exact measurement for clinical use. This is the reason that any follow-up or clinical use should be measured with the same methodology.
PSA test results depend on the measuring methodology and biological variations in relation to our daily activities.
The most important weakness is that PSA is not specific for cancer but specific for prostate diseases. This lack of specificity for cancer has the advantage that the PSA test is useful in prostatitis and benign hyperplasia where elevated levels correlate with the infectious process or the volume of the functional gland. There is no question in our clinical work that a diagnosis of prostate disease should be examined by a DRE and a

EUROPA UOMO / Did You Know? 02/2014 25
PSA test. Unfortunately an elevated PSA test is frequently wrongly believed to be cancer, causing anxiety in the patient and the general practitioner, leading to unnecessary biopsies and overtreatment. To remember all trauma to the prostate (digital examination, biopsy, bicycling and even sex) may result in elevated levels. This is NO diagnosis of cancer and any PSA test needs the interpretation as a possible risk of having prostate cancer. We advise to control an elevated PSA test after six weeks and compare the controls after an antibiotic treatment for infection or the congestion of the prostate when lower urinary tract symptoms are present or after a few days without bicycle racing or sex. The human prostate is not made out of plastic and can be congested just as any other organ. For a high risk of cancer we expect elevations to 10 or 20 µg/cc and for a risk of metastatic disease one expects levels of above 40 to 50 µg/cc. The actual status of the PSA test as a tumour marker is evident after removing the prostate (radical prostatectomy). Here one expects 0 or < 0,2 µg/cc. A decline is also noted after successful radiotherapy and PSA testing is useful in the follow-up of cancer treatment and/or relapse after treatment. The use of the PSA test as a risk of cancer in asymptomatic men is disputed especially when it is proposed as a tool in population screening. Here are serious limitations to any test and certainly in prostate cancer screening. Most pilot studies were performed in symptomatic patients with significant positivity in prostate cancer testing to define the level of risk. This is very different in patients with early stage disease and no symptoms. The cut off value used to define sensitivity and specificity are set empirically (the common cut off level of 4 µg/cc was casted in a huge retrospective study). Any screening
test will result in false positive (75% for PSA) or false negative (15% for PSA) depending on the results of the subsequent biopsy. Another problem may be the prevalence of the disease under a certain age. So a tumour marker of value in monitoring recurrence or relapse may be devoid of use in screening. A third problem is the frequent presence of indolent prostate cancers, already described in the 1930’s in Vienna, that may never develop into a clinical cancer. Cited figures in the literature are from 50% at the age of 60 to 80% at the age of 80. The assessment of a test consists of its ability to diagnose the disease (called sensitivity measured by the true positive cases divided by the true positive + false negative) or predict the absence of disease (called specificity measured by the true negative divided by the true negative and false negative). Important to note if you raise the cut off you will obtain fewer false positives and increase specificity. However you will miss cancers and sensitivity will be reduced. Therefore in the clinic we rely on positive or negative predictive value.
The problem in the use of the PSA test is not the test result itself but the interpretation in a clinical situation where it is used as an excuse for repeated, excessive blind biopsies and subsequent overtreatment.
To summarize the clinical usefulness of the PSA test:
1. PSA is a good tumour marker but not ideal due to limitations in sensitivity and specificity.
2. The clinical value is clear in prostatic diseases but weak in population screening for prostate cancer.
3. Improvements are possible by combining free and complexed PSA (PSA is a protease destroying proteins and neutralized by anti-chymotrypsine in the serum).

EUROPA UOMO / Did You Know? 02/2014 26
4. The laboratory results are variable as well as the biological variation (the latter up to 20%).
5. Part of the PSA is occult in the serum gobbled up by macroglobulines. 6. All derivations or measurements carry the same lack of sensitivity for cancer.
So together with Ablin we can conclude that the PSA test is useful in our clinical work if correctly interpreted in a particular situation. Among particular situations we note:
1. The PSA test increases in the aging process due to the development of hyperplasia.
2. A cut off of < 1.0 µg/ml at the age of 45 years seems to guarantee a decade without cancer.
3. There is a correlation with prognosis of cancer (very high values carry poor prognosis). There is no relation to the grading of cancer tissue but to the volume of the cancer.
4. The generalist physician sees usually one patient with prostate cancer diagnosed in any year of practice. It is impossible to demand from him a clear view of the complexity and paradoxes in the natural history of prostate cancer.
5. Hereditary prostate cancer is rare but disease present in father and brothers and breast cancer in mothers should guide to early diagnostic action.
The case for screening following evidence-based studies for our male population has been published in European Urology titled “Early Detection Prostate Cancer: EAU recommendations”. This article was communicated to the membership. If you missed it, please check A. Heidenreich et al. European Urology 64 (2013): 347-354 or available from the secretariat.
The everlasting quote from Whitmore remains the mantra of the urologist (1994).
“Appropriate treatment implies that therapy be applied neither to those patients for whom it is unnecessary nor to those for whom it will prove ineffective. Furthermore, the therapy should be that which will most assuredly permit the individual a qualitatively and quantitatively normal life. It need not necessarily involve an effort at cancer cure!”
On prostate cancer we can conclude with the published results of a 13 year follow-up on 260,000 participants in the European Randomised Screening Study for Prostate Cancer (ERSPC). Launched in Antwerp in 1991 with a number of pilot studies on DRE, TRUS and PSA > 10 µg/ml the official start of the study in Rotterdam in 1994 was quickly followed by centres in 8 countries. This mega study, not a meta-analysis of different studies, showed a decrease of mortality of 20 to 40% (40% in Sweden) and decrease of morbidity with a clear shift in the diagnosis to localised disease in registration of early cancer. Unfortunately we were also the first to note the overtreatment of small, early cancers that can be evaluated over time and only treated if the risk of progression becomes intermediate or high. These low risk cancers, about 50% in a screening setting, show small volume < 0,5 ml, low Gleason score (Gleason score 6 = 3+3 grade almost never metastasize) and a serum PSA < 10 µg/ml. Based on the ERSPC results the gain in mortality reduction is overshadowed by a 40% overtreatment with common side-effects as impotence and incontinence. Population screening should aim for high risk potentially lethal prostate cancer and avoid overtreatment of the “benign” forms of this disease by careful monitoring. This advice in treatment, called active surveillance, is different from watchful waiting. This form of treatment decision is based on the slow growth of prostate cancer whose natural history to death takes usually 15 years. So any patient with a life

EUROPA UOMO / Did You Know? 02/2014 27
expectancy of less than 10 years without any complaints of lower urinary tract symptoms should be left in peace without any PSA test. The final advice is that we shall not allow any further studies on prostate cancer diagnosis or treatment with only mortality as an endpoint. Quality of life in patients’ outcome results and cost-efficacy must be included in all end results of any study or trial. The pendulum has swung towards a negative, nihilistic conception on the value of the PSA test especially in population screening. This is as bad as the preceding exaltation of the test. The problem of prostate cancer mortality is real and each year about 70,000 men die of the disease in Europe and a multiplicity are lucky as most patients with advanced cancer of the prostate still die with the disease and not by the disease. Urologists are determined and emotional on early diagnosis as the only stage of cancer limited to the gland is curable. Unfortunately the effective, invasive treatments as surgery or radiation carry serious side-effects as incontinence and
impotence and should be used by experienced physicians in prostate cancer centres. The book of Ablin is interesting but he lacks in depth knowledge of all aspects of prostate cancer leading to negative conclusions on still open questions. It is not only the PSA test that requires interpretation but the inept stage listing of prostate cancer in T1 a, b and c is confusing, adequate indications for a correct biopsy procedure, lack of diagnostic accuracy of TRUS, new imaging as MRI and Pet, measuring co-morbidity of patients and last but not least informing them adequately to share a decision in diagnosis and treatment remain an enormous challenge. We need more than awareness and empathy to solve this problem to the benefit of patients and science. All these points will be handled in the next article. We look forward to heated discussion and ad-rem dialogues. ”Du choc des idées jaillit la lumière”.
EUROPA UOMO Secretariat Lange Gasthuisstraat 35-37, 2000 Antwerp – Belgium
Tel: +32 3 338 91 51, Fax: +32 3 338 91 52 E-mail: [email protected] - Website: www.europa-uomo.org
Publication co-sponsored by
“Did You Know?” European Newsletter contacts and email
Austria: Ekkehard Büchler, [email protected]; Belgium: Henk Van daele, [email protected]; Bulgaria: Alexander Marinov, [email protected]; Cyprus: Andreas Moyseos, [email protected]; Czech Republic: Dalibor Pacík, [email protected]; Denmark: K.B. Madsen, [email protected]; Finland: Hannu Tavio, [email protected]; France: Roland Muntz, [email protected].; Germany: Günter Feick, [email protected]; Hungary: Dr. Tamás Simon MD. Ph.D., [email protected]; Ireland: John Dowling; [email protected]; Italy: Malcolm Galloway Duncan, [email protected] - [email protected]; Lithuania: Zygimantas Kardelis, [email protected]; Norway: Tor Tausvik, [email protected]; Poland: Tadeusz Rudzinski, [email protected]; Portugal: Joaquim da Cruz Domingos, [email protected]; Romania: Toma Catalin Marinescu, [email protected]; Slovak Republic: Josef Blazek, [email protected] – [email protected]; Spain: Jordi Estapé, [email protected]; Sweden: Calle Waller, [email protected]; Switzerland: Max Lippuner, [email protected]; The Netherlands: Kees van den Berg, [email protected]; United Kingdom: Ken Mastris, [email protected].