dichotomizing children’s behavior problems: carving nature at its joints sandy braver, jenessa...
TRANSCRIPT

Dichotomizing Children’s Behavior Problems:
Carving Nature at Its Joints
Sandy Braver, Jenessa Shapiro & Amy Weimer
SPRI and Quant Seminar Presentation

2
Statisticians Have Strongly Argued Against Dichotomizing Inherently
Continuous Variables (MacCallum et al., 2002)
• Very Common Practice• Derives from a “Group” ANOVA Mentality• Medical Model:Categories of Disease, Not Continua• Can Handle Through Regression Instead, But Not All
Researchers Know This• A Number of Statistical and Inferential Problems
Result

3
Statistical Problems
• “Dichotomization is rarely defensible and often will yield misleading results.”
• Lower Statistical Power• Cutpoints Are Typically Arbitrary• Other Cutpoints Might Not Replicate Result• Cutpoint Itself (e.g. median) Won’t Replicate• Forces one into nonsensical positions:
1 and 62 (both below cutpoint) are the SAME, but 62 and 63 (one below and one above cutpoint) are
DIFFERENT

4
But Real World Often Demands Dichotomization
• Selection Problems• Screening• At Risk• Insurance• DSMIV • (But see Fall 2005 Special Issue of Journal of
Abnormal Psychology, which argues for replacing categorical approach of DSMIV with a DIMENSIONAL Approach in Forthcoming DSMV)

5
Dichotomization Natural and Appropriate for Some Medical
Problems • Cancer
For Other Problematic Conditions, Dichotomization More Arbitrary•High Blood Pressure•Diabetes•Depression and Most Mental Health Conditions
• Pregnancy• Death

6
NIMH: “Congress is Interested in Us Preventing or Treating Serious Mental
Health Problems”
“I Need to Show Them We Can Prevent Schizophrenia”
Our Primary Dependent Variable at PRC: Child Well-Being or Mental Health
“Caseness” Desired By Policy-Makers; Detecting Children Who Are
Seriously Mentally ill

7
Current Standard:Child Behavior Checklist (CBCL)
Achenbach• E.g., The 2001 Annual Report to Congress on
the Evaluation of the Comprehensive Community Mental Health Services for Children and Their Families Program says:
“The CBCL (Achenbach, 1991a) has been identified as the most reliable and valid parent report measure currently available for assessing children's emotional and behavioral problems (Reitman, Hummel, Franz, & Gross, 1998).”

8
Characteristics of the CBCL• 133 items: “Argues A Lot”; “Depressed, Withdrawn”• not true=0, somewhat or sometimes true =1, very true or often
true=2• Parent Report, Youth Self-Report, Teacher Report• Total Problems Score; Broad Band (Internalizing,
Externalizing); Narrow Band (e.g., Attention Problems/Hyperactivity, Oppositional Defiant, and Somatization)
• Raw Score, T-Score• Clinical Cutoff: “Internalizing, Externalizing, and Total
Problems scale T-scores are considered in the clinical range if they are above 63, while scores from 60 to 63 are borderline. Scores in the clinical range indicate a need for clinical care.”
• High Reliability (Alpha and Test-Retest)• Excellent National Norms• Lots of Validation Studies• Thousands of studies use the CBCL and report the percent of
their study group in the clinical (and borderline clinical) range, reifying the arbitrary clinical range cutoff

9
Alternatives to the CBCL
• Rutter• DISC (Takes several hours to administer,
many hours to train and certify testors, matches Psychiatrists’ DSM Diagnosis)
• Short Form of CBCL, the Behavior Problem Index (BPI) 32 items
• Not Copyrighted—Free• We Use BPI

10
Validation Studies Need a Criterion
• CBCL’s Criterion is referred to as “Referral Status”
• That is, A Clinic Sample vs A “Matched” Non-Clinic Sample Were Assessed
• Lots of differences are found between the two “status groups” on various CBCL variables, which establishes validity of scale

11
Cutoff Determination ALSO requires a criterion variable
• Choice of Cutoff Value for Caseness Determination can and should use the same criterion variable as for Validity studies
• This is a very common problem in medical settings (e.g., high blood pressure, diabetes) and human resources settings (e.g., hire, no hire)
• a technology (ROC) for distinguishing “normal” from “case” has developed and received acceptance

12
Brief Primer on Cutoff Determination:ROC (Receiver Operating Characteristic,
Signal Detection) Analysis
Diagnosis
- +
Tests’ Value Relative to Proposed Cutoff
Below False
Negative(FN)
At or Above
False Positive(PN)

13
ROC Analysis Uses Constructs of Sensitivity & Specificity
• SE: {Sensitivity}: Is the proposed cutoff value sensitive? Does it detect most of the Positive Cases?
• SP: {Specificity}: Is the proposed cutoff value specific to the positive cases? Does it correctly indicate the cases that are NOT POSITIVE
• For a good test, with a well selected cutoff, both should be very high.

14
Sensitivity & Specificity ExampleDiagnosis
- +Test’s Value Relative to Proposed Cutoff
Below A=500 B=200 A+B=700
At or Above
C=100 D=200 C+D=300
A+C=600 B+D=400 T=1000
=A+B+C+D50.
400DB
200D
SE=Sensitivity=Prob of pos test given pos diag=
833.600CA
500A
SP=Specificity= Prob of neg test given neg diag=
1-Specificity= Prob of POS test given neg diag=.167
1-Specificity Should be LOW

15
Ideal pointCoordinates of the Curve
Test Result Variable(s): educ Educational Level (years)
7.00 1.000 1.000
10.00 .911 .861
13.00 .671 .269
14.50 .647 .269
15.50 .326 .116
16.50 .190 .005
17.50 .151 .000
18.50 .116 .000
19.50 .012 .000
20.50 .004 .000
22.00 .000 .000
Positive ifGreater Thanor Equal To
aSensitivity 1 - Specificity
The test result variable(s): educ Educational Level (years)has at least one tie between the positive actual state groupand the negative actual state group.
The smallest cutoff value is the minimumobserved test value minus 1, and the largest cutoffvalue is the maximum observed test value plus 1.All the other cutoff values are the averages of twoconsecutive ordered observed test values.
a.
Best Cutoff
1-SP too high
SE too low
ROC Graph (SPSS):Sensitivity & 1-Specificity Are Calculated
Repeatedly, for Each Potential Cutoff Value
A CONVINCING Cutoff Should Be Noticeably Better Than Its Neighbors
Potential Cutoffs
15

16
A CONVINCING Cutoff Should Be Noticeably Better Than Its Neighbors• Otherwise, Cutoff Is Arbitrary
• Flat ROC Curves Provide No Compelling Rationale For Choosing One Cutoff Value vs Another For This Important Real World Choice
• Depends on Emphasis on SE or SP

Alternatives to Sensitivity & Specificity (Helena Kraemer)
Diagnosis
- +
Test’s Value Relative to Proposed Cutoff
Below A=500 B=200 A+B=700
At or Above
C=100 D=200 C+D=300
A+C=600 B+D=400 T=1000=A+B+C+D
PVP=predictive value of a positive test =(D=200)/((C+D=300) =.67PVN=predictive value of a negative test =(A=500)/((A+B=700)=.71
Quality PVP=κ(0,0)=(PVP-P)/(1-P)=(.67-.4)/(1-.4)=.44, weights avoiding False PositivesP=Prevalence (of a Pos Diag) =(B+D=400)/(T=1000)=.40
Quality PVN=κ(1,0)=(PNP-(1-P))/P=(.71-.6)/.4=.29,weights avoiding False NegativesCohen’s Kappa [κ(.5,0)]=.35, weights FN & FP equally
Weighted Kappa [κ(r,0)] [e.g. κ(.8,0)]=.31, weights FN & FP relatively, by r
Efficiency=EFF=Overall Prob of Correct Class=(A+D=500+200=700)/(T=1000)=.70
PHI coefficient (Φ)
r =WFN/(WFN+WFP), W is weight; r of .8 means that FN are 4 times worse than FP 4/(4+1)
17

http://www.erlbaum.com/Documents/JPA/3_04/2%20x%202%20Stat%20Calculator.xls
Diagnosis Present Diagnosis AbsentTest Positive 118 52 170
Test Negative 69 761 830187 813 1000
Prevalence 0.187 Prevalence* Enter #(*Enter prevalence as a value between 0 and 1)
Sensitivity 0.631 SensitivitySpecificity 0.936 Specificity
Odds ratio (OR) 25.027 Odds ratio (OR)Likelihood Ratio+ (LR+) 9.866 Likelihood Ratio+ (LR+)
Likelihood Ratio- (LR-) 2.537 Likelihood Ratio- (LR-)
Positive Predictive Power (PPP) 0.694 Positive Predictive Power (PPP)Negative Predictive Power (NPP) 0.917 Negative Predictive Power (NPP)
Overall Correct Classification (OCC) 0.879 Overall Correct Classification (OCC)Incremental PPP 0.507 Incremental PPPIncremental NPP 0.104 Incremental NPP
Quality PPP 0.624 Quality PPPQuality NPP 0.555 Quality NPP
Kappa 0.588 KappaKraemer's Kappa 0.594 Kraemer's Kappa
Phi coefficient 0.589 Phi coefficientPretest Odds+ 0.230 Pretest Odds+
Posttest Odds+ 2.269 Posttest Odds+Pretest Odds- 4.348 Pretest Odds-
Posttest Odds- 11.029 Posttest Odds-
Dx Present Dx AbsentTest Positive
Test Negative
**Program created by Jared DeFife, Adelphi University, 2004.
*Formulas and calculations based on Streiner, D.L. (2003). Diagnosing tests: Using and misusing diagnostic and screening tests. Journal of Personality Assessment, 81(3), 209-219.
DIAGNOSTIC EFFICIENCY STATISTICS CALCULATOR*
For statistics based upon the observed prevalence rate from your SAMPLE, use the results below:
To customize a prevalence rate that is based on a POPULATION (I.e. not from your sample),
enter a prevalence rate below then calculate by
click ing on the YELLOW BOX :
**ALWAYS CLICK HERE TO CALCULATE FINAL RESULTS**
Enter raw data into RED cells then click the YELLOW box to calculate:
Population Prevalence Adjusted Table:
18

19
Example 1
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
k(0,0) Qual PVP
k(1,
0) Q
ual
PV
N
3
4
2
sens & spec
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
1 - spec
sen
s
6
5
4
3
2
Raw Data Example 1
0
0.2
0.4
0.6
0.8
1
1 2 3 4 5 6 7 8
scoreP
rob
of
crit
weighted kappas and phi
0
0.1
0.2
0.3
0.4
0.5
1 2 3 4 5 6 7
score
κ(.2,0) κ(.4,0) κ(.5,0)=Cohen's κ(.6,0) κ(.8,0) phi
rpbi Note that it’s>Φ
20
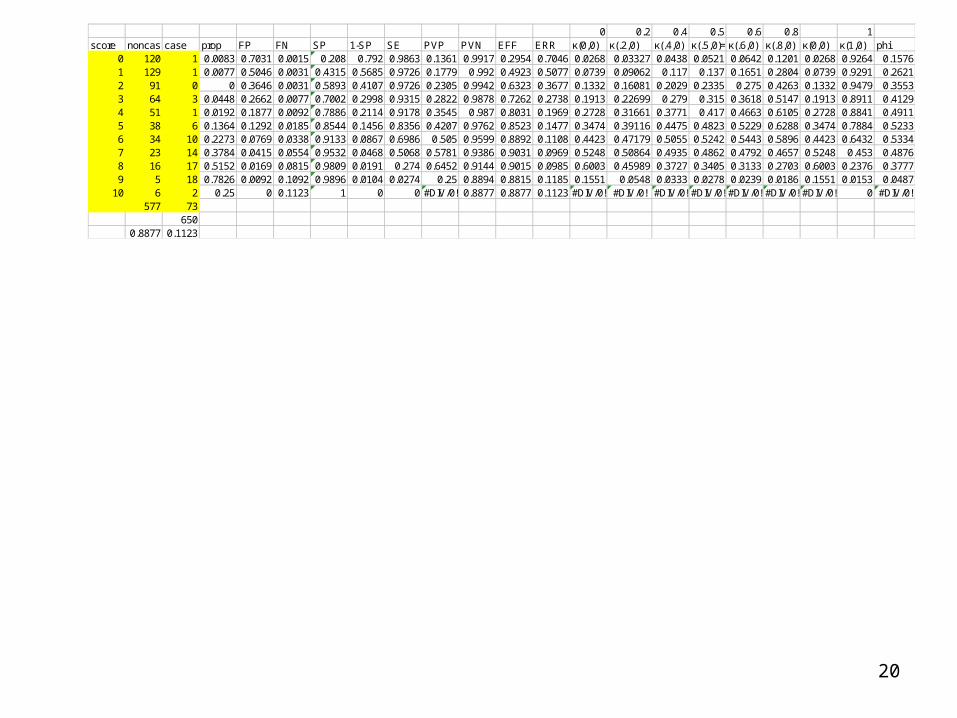
0 0.2 0.4 0.5 0.6 0.8 1score noncasecase prop FP FN SP 1-SP SE PVP PVN EFF ERR κ(0,0) κ(.2,0) κ(.4,0) κ(.5,0)=Cohen'sκ(.6,0) κ(.8,0) κ(0,0) κ(1,0) phi
0 120 1 0.0083 0.7031 0.0015 0.208 0.792 0.9863 0.1361 0.9917 0.2954 0.7046 0.0268 0.03327 0.0438 0.0521 0.0642 0.1201 0.0268 0.9264 0.15761 129 1 0.0077 0.5046 0.0031 0.4315 0.5685 0.9726 0.1779 0.992 0.4923 0.5077 0.0739 0.09062 0.117 0.137 0.1651 0.2804 0.0739 0.9291 0.26212 91 0 0 0.3646 0.0031 0.5893 0.4107 0.9726 0.2305 0.9942 0.6323 0.3677 0.1332 0.16081 0.2029 0.2335 0.275 0.4263 0.1332 0.9479 0.35533 64 3 0.0448 0.2662 0.0077 0.7002 0.2998 0.9315 0.2822 0.9878 0.7262 0.2738 0.1913 0.22699 0.279 0.315 0.3618 0.5147 0.1913 0.8911 0.41294 51 1 0.0192 0.1877 0.0092 0.7886 0.2114 0.9178 0.3545 0.987 0.8031 0.1969 0.2728 0.31661 0.3771 0.417 0.4663 0.6105 0.2728 0.8841 0.49115 38 6 0.1364 0.1292 0.0185 0.8544 0.1456 0.8356 0.4207 0.9762 0.8523 0.1477 0.3474 0.39116 0.4475 0.4823 0.5229 0.6288 0.3474 0.7884 0.52336 34 10 0.2273 0.0769 0.0338 0.9133 0.0867 0.6986 0.505 0.9599 0.8892 0.1108 0.4423 0.47179 0.5055 0.5242 0.5443 0.5896 0.4423 0.6432 0.53347 23 14 0.3784 0.0415 0.0554 0.9532 0.0468 0.5068 0.5781 0.9386 0.9031 0.0969 0.5248 0.50864 0.4935 0.4862 0.4792 0.4657 0.5248 0.453 0.48768 16 17 0.5152 0.0169 0.0815 0.9809 0.0191 0.274 0.6452 0.9144 0.9015 0.0985 0.6003 0.45989 0.3727 0.3405 0.3133 0.2703 0.6003 0.2376 0.37779 5 18 0.7826 0.0092 0.1092 0.9896 0.0104 0.0274 0.25 0.8894 0.8815 0.1185 0.1551 0.0548 0.0333 0.0278 0.0239 0.0186 0.1551 0.0153 0.0487
10 6 2 0.25 0 0.1123 1 0 0 #DIV/0! 0.8877 0.8877 0.1123 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! 0 #DIV/0!577 73
6500.8877 0.1123

21
Example 2
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6
k(0,0) Qual PVP
k(1,
0) Q
ual
PV
N
3
4
2
sens & spec
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
1 - spec
sen
s
6
5
4
3
2
Raw Data Example 1
0
0.2
0.4
0.6
0.8
1 2 3 4 5 6 7 8
score
Pro
b o
f cr
it
weighted kappas and phi
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
1 2 3 4 5 6 7
score
κ(.2,0) κ(.4,0) κ(.5,0)=Cohen's κ(.6,0) κ(.8,0) phi
rpbi
Φ>rpbi

22
Example 3
0
0.2
0.4
0.6
0.8
1
0 0.05 0.1 0.15 0.2 0.25 0.3 0.35 0.4 0.45
k(0,0) Qual PVP
k(1,
0) Q
ual
PV
N
3 42
sens & spec
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
1 - spec
sen
s
6
5
4
3
2
weighted kappas and phi
0
0.1
0.2
0.3
0.4
0.5
1 2 3 4 5 6 7
score
κ(.2,0) κ(.4,0) κ(.5,0)=Cohen's κ(.6,0) κ(.8,0) phi
Raw Data Example 3
0
0.2
0.4
0.6
1 2 3 4 5 6 7 8
score
Pro
b o
f cr
it
rpbi
Φsubstantially>rpbi

23
Example 4
0
0.1
0.2
0.3
0 0.1 0.2 0.3 0.4 0.5
k(0,0) Qual PVP
k(1,
0) Q
ual
PV
N
3 42 5 6
sens & spec
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
1 - spec
sen
s
6
5
4
3
2
weighted kappas and phi
0
0.1
0.2
0.3
0.4
1 2 3 4 5 6 7
score
κ(.2,0) κ(.4,0) κ(.5,0)=Cohen's κ(.6,0) κ(.8,0) phi
rpbi
Φsubstantially>rpbi
Raw Data Example 4
0
0.2
0.4
0.6
1 2 3 4 5 6 7 8
score
Pro
b o
f cr
it

24
Only A Peaked ROC Curve Provides Strong Rationale for A Specific Value For
Cutoff, Whatever the Index Chosen• Chooses Same Cutoff By Any Criterion• No Need to Defend Choice of SE & SP, vs PVP
& PVN, vs Quality version, vs Kappas• No Need to Defend Weights for FN vs FP in
Kappas• No Need to Know Prevalence• A Peaked ROC curve will result only if the raw
data has a “Joint”, • Joint on all curves at same point• Want to “carve” (choose as cutoff) right at
Nature’s joint

25
Applying ROC Concepts to CBCL• Needs a True Dichotomous Criterion• i.e., the “Diagnosis”• Achenbach Uses Referral Status, the Same Variable Used as
Criterion in Validity Studies, As Recommended• Referred vs Not Referred • i.e., Clinic Cases vs Normal• The cutoff of 63 (Clinical Range) was chosen by Achenbach in order
to meet the following Criterion: Minimizing Error (=ERR=FN+FP=1-Efficiency)
• (i.e., Maximize EFF)• Difficulties with this Approach:
Doesn’t Provide ROC Curves, so Can’t Determine Whether ROC is Peaked, Whether that Cutoff Is Noticeably Better Than Neighbors
Is Equal Weighting of FN & FP Appropriate For Caseness?

26
Our Biggest Issue with the CBCL: The Validity Criterion Chosen
• They Say It’s “Referred vs Non-Referred”, But It’s Really Not
• It’s Really Clinic vs Non-Clinic• Not Known WHO Referred Or If “Referred” By Anyone At
All• This Leads to the Question of Which Kids Get to Clinic• Empirical Research on Parents Taking Kids to Clinic
Shows Many Factors Are Influential, Only One of Which is Kid’s Mental State (Lobitz and Johnson, 1975)Parents’ LabelingParent’s Belief in Efficacy of Clinical Therapy Insurance IssuesParent’s (Mother’s) Own Clinical Levels

27
Their Method Prevents Estimation of Prevalence, Needed For Some Indexes
• What Is prevalence of serious mental illness in Adolescents?
• Major Review Article of 52 Studies (Roberts,1998)• Lots Of Issues• What’s Criterion, What’s Population?• 3 to 54%• Median: About 15%• This “Feels About Right” to Diagnosticians• Matches Prevalence of Other Mental Health
Problems• CBCL Clinical Range T Score of 63 = About 15%

28
Is There Another Easy To Use True Dichotomous Criterion? Our Idea
• Teacher Report of Referral
• Actual Referral, Not Whether Being Seen
• Matches Notions About NEED For Services, Rather Than Use Of Services
• Teachers Are More Neutral Than Parents
• Teachers Have Better Frame Of Reference For Disturbed Behavior

29
Alternative: Peer Report of Psychopathology
• Data Suggests Peers of Adolescents Are Excellent Judges of Pathology
• Sociometrics Ratings of Peers Predict Better Than Any Other Variable Later Problem Behavior
• Sociometrics Cumbersome to Acquire
• Teachers Good Detectors of Sociometric Data
• Teacher Report on Peers Proxy for Peer Report

30
PAYS Data Set
• About 400 families• All with 7th Graders• Recruited from schools in AZ and
Riverside, CA• Will be 3 Waves• Mother, Father, Child Report on BPI
Internalizing and Externalizing• 2 Teacher Reports on our adapted version
of BPI

31
* p < .001
Correlations of Teacher 1, Teacher 2, Child, Mom and Dad on BPI
1 2 3 4 5
1. Teacher 1 .57* .33* .26* .32*
2. Teacher 2 .39* .30* .39*
3. Child's CBCL .35* .28*
4. BPI (Mom) .47*
5. BPI (Dad)
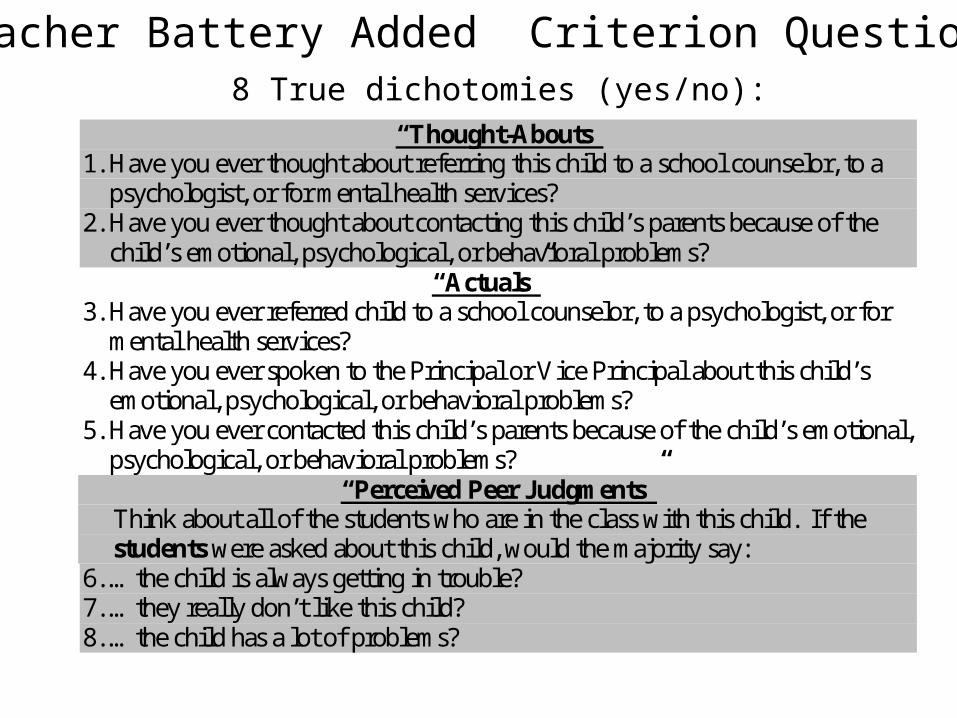
8 True dichotomies (yes/no):
Teacher Battery Added Criterion Questions
“Thought-Abouts” 1. Have you ever thought about referring this child to a school counselor, to a
psychologist, or for mental health services? 2. Have you ever thought about contacting this child’s parents because of the
child’s emotional, psychological, or behavioral problems? “Actuals”
3. Have you ever referred child to a school counselor, to a psychologist, or for mental health services?
4. Have you ever spoken to the Principal or Vice Principal about this child’s emotional, psychological, or behavioral problems?
5. Have you ever contacted this child’s parents because of the child’s emotional, psychological, or behavioral problems?
“Perceived Peer Judgments” Think about all of the students who are in the class with this child. If the students were asked about this child, would the majority say: 6. …the child is always getting in trouble? 7. …they really don’t like this child? 8. …the child has a lot of problems?

33
2 3 4 5 6 7 8 T1-T2 cor % yes
Has teacher ever thought about:1. Contacting this child's parents because of the child's emotional, psychological, or .52* .41* .77* .43* .51* .37* .49* .37* 17.9
2. Referring this child to a school counselor, to a psychologist, or for mental health services? .44* .47* .68* .46* .34* .56* .13* 9.5
Has teacher ever :3. Spoken to Principal or Vice Principal about this child's emotional, psychological, or behavior problems? .45* .46* .43* .33* .42* .19* 5.8
4. Contacted this child's parents because of the child's emotional, psychological, or behavior problems? .41* .51* .36* .48* .36* 13.9
5. Referred this child to a school counselor, to a psychologist, or for mental health services? .32* .28* .45* .14* 5.2
Would majority of kids in child's class say:
6. Child always is getting into trouble? .44* .55* .42* 8.4
7. They really don't like this child? .68* .04 4.0
8. This child has a lot of problems? .21* 5.2
Correlations of 8 dichotomous items; Percent of Teachers that said “Yes” for each item
* p<.05

34
Teacher BPI % yesHas teacher ever thought about:
1. Contacting this child's parents because of the child's emotional, psychological, or behavior problems? .56* 17.92. Referring this child to a school counselor, to a psychologist, or for mental health services? .42* 9.5Has teacher ever :3. Spoken to Principal or Vice Principal about this child's emotional, psychological, or behavior problems? .31* 5.84. Contacted this child's parents because of the child's emotional, psychological, or behavior problems? .49* 13.95. Referred this child to a school counselor, to a psychologist, or for mental health services? .33* 5.2Would majority of kids in child's class say:
6. Child always is getting into trouble? .49* 8.47. They really don't like this child? .29* 4.08. This child has a lot of problems? .37* 5.2
Correlations between individual dichotomies (N=700)with teacher BPI
* p<.001

35
Teacher Thought About Contacting Parentssens & spec
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
1 - spec
sen
s
6
5
43
2
7
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
k(0,0) Qual PVP
k(1,
0) Q
ual
PV
N
3
4
2
5
6
8
7
weighted kappas and phi
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0 1 2 3 4 5 6 7 8 9 10
score
κ(.2,0) κ(.4,0) κ(.5,0)=Cohen's κ(.6,0) κ(.8,0) phi
rpbi
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 2 3 4 5 6 7 8 9 10 11
score
pro
po
rtio
n c
ases

36
Teacher Actually Contacted Parentssens & spec
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
1 - spec
sen
s
6
5 4
32
7
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6
k(0,0) Qual PVP
k(1,
0) Q
ual
PV
N
3
4
2
5
6
8
7
weighted kappas and phi
0
0.1
0.2
0.3
0.4
0.5
0.6
0 1 2 3 4 5 6 7 8 9 10
score
κ(.2,0) κ(.4,0) κ(.5,0)=Cohen's κ(.6,0) κ(.8,0) phi
rpbi
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 2 3 4 5 6 7 8 9 10 11
score
pro
po
rtio
n c
ases
Better, but still no real joint

37
thought actual peerTeacher
BPI % Yesthought 1 0.77* 0.58* 0.58* 19.8
actual 1 0.57* 0.54* 16.1
peer 1 0.52* 10.8
Teacher BPI 1
Combine Dichotomies: 1 if ANY, 0 if NONE

38
Thought Aboutssens & spec
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
1 - spec
sen
s
6
5
4
3 2
7
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 2 3 4 5 6 7 8 9 10 11
score
pro
po
rtio
n c
ases
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
k(0,0) Qual PVP
k(1,
0) Q
ual
PV
N
3
4
2
5
6
8
7
weighted kappas and phi
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0 1 2 3 4 5 6 7 8 9 10
score
κ(.2,0) κ(.4,0) κ(.5,0)=Cohen's κ(.6,0) κ(.8,0) phi
rpbi

39
Actualssens & spec
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
1 - spec
sen
s
6
5
4 32
7
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8
k(0,0) Qual PVP
k(1,
0) Q
ual
PV
N
3
4
2
5
6
8
7
weighted kappas and phi
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0 1 2 3 4 5 6 7 8 9 10
score
κ(.2,0) κ(.4,0) κ(.5,0)=Cohen's κ(.6,0) κ(.8,0) phi
rpbi
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 2 3 4 5 6 7 8 9 10 11
score
pro
po
rtio
n c
ases

40
Peerssens & spec
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
1 - spec
sen
s
6 5 43 2
7
weighted kappas and phi
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0 1 2 3 4 5 6 7 8 9 10
score
κ(.2,0) κ(.4,0) κ(.5,0)=Cohen's κ(.6,0) κ(.8,0) phi
rpbi
0
0.2
0.4
0.6
0.8
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7
k(0,0) Qual PVP
k(1,
0) Q
ual
PV
N
34
2
5
6
8
7
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
1 2 3 4 5 6 7 8 9 10 11
score
pro
po
rtio
n c
ases
Nature at the Joint?

41
So, pick a score of 6 on BPI as Cutpoint with Peers as Criterion
SP .91
1-SP .09
SE .70
PVP .50
PVN .96
EFF .89
ERR .11
κ(0,0) .44
κ(.2,0) .47
κ(.4,0) .51
κ(.5,0)=Cohen's .52
κ(.6,0) .54
κ(.8,0) .59
κ(1,0) .64
phi .53
But why not just ask teacher the dichotomous
questions:
Forget the BPI