diagnostics and disease monitoring in ibd: state of the...
TRANSCRIPT
David T. Rubin, MD 2011 1
Diagnostics and disease monitoring in IBD:
State of the art 2011
D id T R bi MDDavid T. Rubin, MDAssociate Professor of Medicine
Co-Director, Inflammatory Bowel Disease CenterUniversity of Chicago Medical Center
The First Goal of Management in IBD: Obtain a Clear and Accurate Diagnosis
A clear diagnosis should provide information that:– Explains the patient’s current symptoms and problemsy– Is accurate now and withstands the test of time– Provides prognostic information– Makes a distinction in the management decisions such
that therapy chosen now impacts both short- and long-term outcomes.
– May have implications for the care of others (ie family y p ( ymembers).
In 2011, should include disease extent and current severity and some element of longitudinal prognosis.

David T. Rubin, MD 2011 2
What is Disease Monitoring in IBD?
Assessment of the status of disease activity over time.
Performed in order to control disease and prevent Performed in order to control disease and prevent symptomatic relapses or disability.
Monitoring requires:– Understanding of the disease process– Acceptable methods of assessment– Interventions that are effective and tolerable (by the patient and by
the MD))
Examples:– Clinical follow-up– Routine laboratory testing for drug efficacy or safety– Measures of mucosal integrity or immune activity
Clinical Features of UC and CD
Ulcerative ColitisUlcerative Colitis– Continuous inflammation– Colon only
Crohn’s DiseaseCrohn’s Disease– Patchy inflammation– Mouth to anus involvementy
– Superficial inflammation– Variable extent– Risk of cancer– Extraintestinal
manifestations
– Full-thickness inflammation– Fistulas and strictures– Risk of cancer– Extraintestinal
manifestations
Greatest Least
Frequency of Involvement

David T. Rubin, MD 2011 3
Montreal ClassificationCrohn’s disease
Location (L)
L1 Terminal ileum
L2 Colon
L3 Ileocolon
L4 Upper GI
Behavior (B)
B1 Non-stricturing, non-penetrating
B2 Stricturing
B3 Penetrating
(p) modifier Perianal
Montreal Classificationulcerative colitis
Classification by Extent
Ulcerative proctitis (E1)
Left-sided ulcerative colitis (E2)
Extensive ulcerative colitis (E3)

David T. Rubin, MD 2011 4
The Challenges to Diagnosis in IBD
Lack of knowledge about the disease and its various manifestations (primary care?)
Lag time of pre-symptomatic disease before presentation
Inaccurate classification system– Overlap of phenotypes between UC and Crohn’s
disease– Variations of existing disease presentations
The Spectrum of Utility in IBD
Predicting Behavior Rx Response
Need for
Surgery & Outcome
Monitoring
activity, response

David T. Rubin, MD 2011 5
Diagnosis in IBD
Primary Dx of IBD Rule out imposters
Clarification of IBD Dx Ileocolonoscopy with
biopsy Obvious GI symptoms/signs and classic presentation
Extra-intestinal symptoms/signs and findings
biopsy Distinction between IBS
and active inflammation Reliable expert pathology Evaluation of small bowel
– WCE– CTE/MRE
E d h i Re-evaluation over time Exam under anesthesia, exploratory lap
Use of other clues– family history– serologies– Non-GI specialists
Historical Features that Help to Confirm a Diagnosis of IBD
Appendectomy protects Early Appendectomy Early Appendectomy Protects Against UCProtects Against UCpp y p
against UC
Ex-smokers may develop UC
Smokers have CD
Family history usually concordant
Andersson RE, et al. N Engl J Med. 2001;344:808–814.
David T. Rubin, MD 2011 6
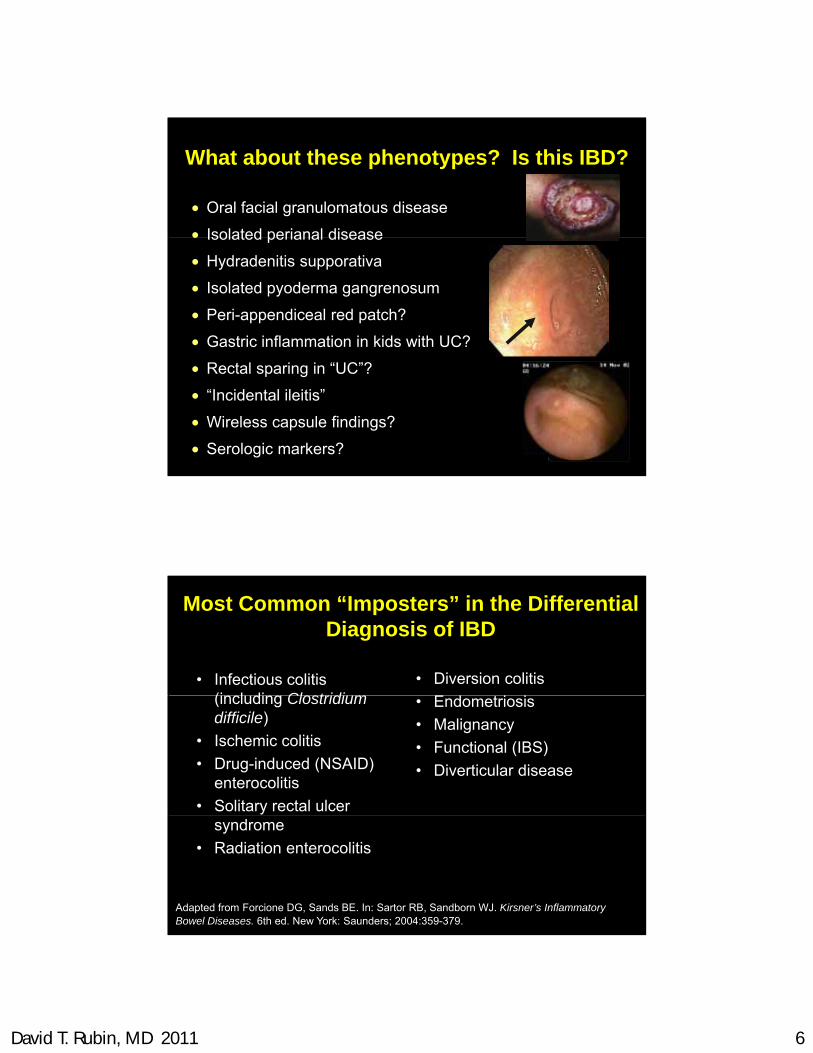
What about these phenotypes? Is this IBD?
Oral facial granulomatous disease
Isolated perianal disease Isolated perianal disease
Hydradenitis supporativa
Isolated pyoderma gangrenosum
Peri-appendiceal red patch?
Gastric inflammation in kids with UC?
Rectal sparing in “UC”?
“Incidental ileitis”
Wireless capsule findings?
Serologic markers?
• Infectious colitis (i l di Cl t idi
• Diversion colitis
E d i i
Most Common “Imposters” in the Differential Diagnosis of IBD
(including Clostridium difficile)
• Ischemic colitis
• Drug-induced (NSAID) enterocolitis
• Solitary rectal ulcer
• Endometriosis
• Malignancy
• Functional (IBS)
• Diverticular disease
syndrome
• Radiation enterocolitis
Adapted from Forcione DG, Sands BE. In: Sartor RB, Sandborn WJ. Kirsner’s Inflammatory Bowel Diseases. 6th ed. New York: Saunders; 2004:359-379.
David T. Rubin, MD 2011 7
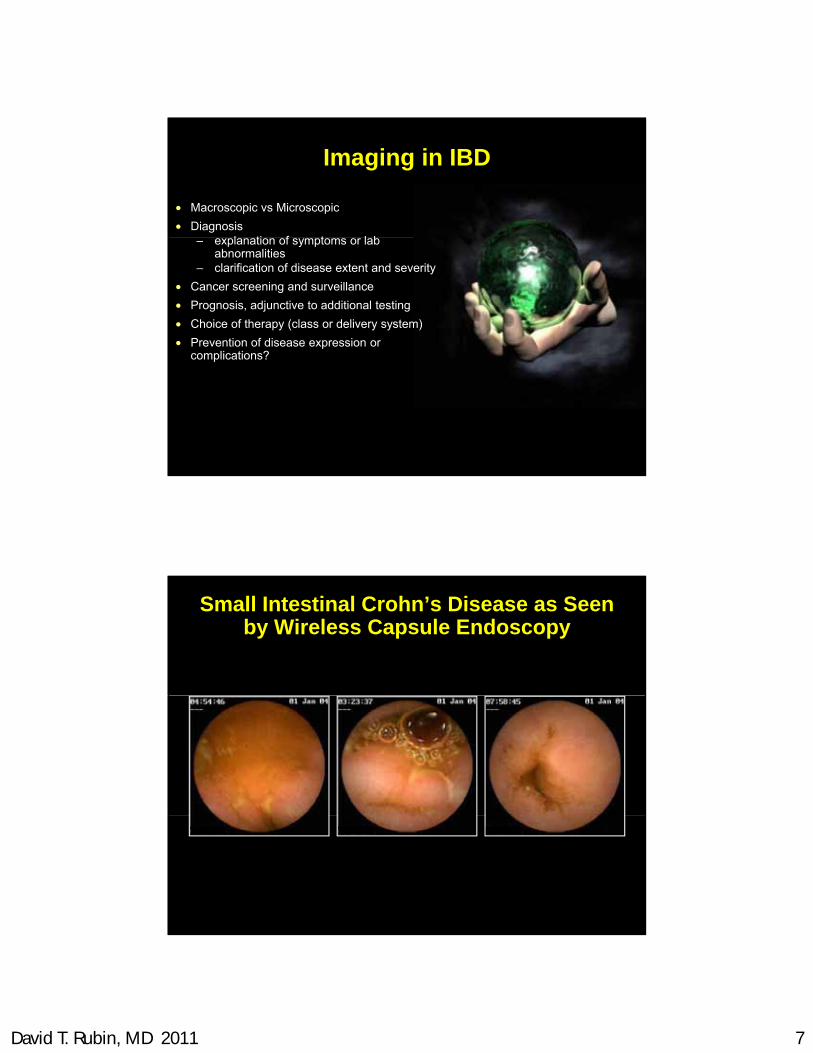
Imaging in IBD
Macroscopic vs Microscopic
Diagnosisl ti f t l b– explanation of symptoms or lab
abnormalities– clarification of disease extent and severity
Cancer screening and surveillance
Prognosis, adjunctive to additional testing
Choice of therapy (class or delivery system)
Prevention of disease expression or complications?complications?
Small Intestinal Crohn’s Disease as Seenby Wireless Capsule Endoscopy

David T. Rubin, MD 2011 8
Promise and Problems of CE in IBD
PROMISE Exquisite imaging of small bowel
mucosa
PROBLEMS Observer-dependent interpretation
training required Less invasive diagnostics (?)
Emerging information about significance of findings, etc
Recent FDA indication for monitoring of CD
– training required– inter/intra observer variability
Uncertain significance of many findings- what’s “normal”?– Short-term– Long-term– Need blinded comparator
studies
Heterogeneous data quality of Heterogeneous data quality of studies
Capsule retention
Are All Small Bowel Lesions CD?
David T. Rubin, MD 2011 9
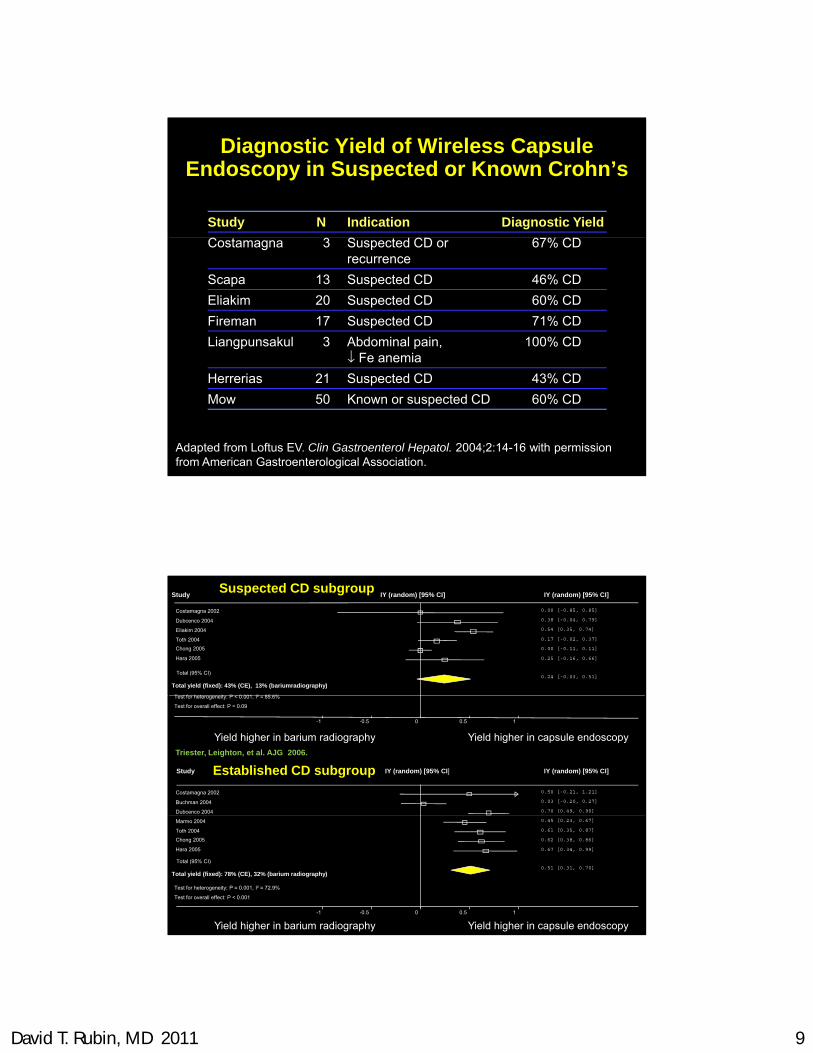
Diagnostic Yield of Wireless Capsule Endoscopy in Suspected or Known Crohn’s
Study N Indication Diagnostic Yield
Costamagna 3 Suspected CD or recurrence
67% CD
Scapa 13 Suspected CD 46% CD
Eliakim 20 Suspected CD 60% CD
Fireman 17 Suspected CD 71% CD
Liangpunsakul 3 Abdominal pain, Fe anemia
100% CD
Adapted from Loftus EV. Clin Gastroenterol Hepatol. 2004;2:14-16 with permission from American Gastroenterological Association.
Fe anemia
Herrerias 21 Suspected CD 43% CD
Mow 50 Known or suspected CD 60% CD
Suspected CD subgroupStudy IY (random) [95% CI] IY (random) [95% CI]
Costamagna 2002 0.00 [-0.85, 0.85]
Dubcenco 2004 0.38 [-0.04, 0.79]
Eliakim 2004 0.54 [0.35, 0.74]
Toth 2004 0.17 [-0.02, 0.37]
Chong 2005 0.00 [-0.11, 0.11]
Hara 2005 0.25 [-0.16, 0.66]
Total (95% CI)0.24 [-0.03, 0.51]
Total yield (fixed): 43% (CE), 13% (bariumradiography)
T t f h t it P < 0 001 I² 85 6%Test for heterogeneity: P < 0.001, I² = 85.6%
Test for overall effect: P = 0.09
-1 -0.5 0 0.5 1
Yield higher in barium radiography Yield higher in capsule endoscopy
Study IY (random) [95% CI] IY (random) [95% CI]
Costamagna 2002 0.50 [-0.21, 1.21]
Buchman 2004 0.03 [-0.20, 0.27]
Dubcenco 2004 0.70 [0.49, 0.90]
Established CD subgroup
Triester, Leighton, et al. AJG 2006.
22
Marmo 2004 0.45 [0.23, 0.67]
Toth 2004 0.61 [0.35, 0.87]
Chong 2005 0.62 [0.38, 0.86]
Hara 2005 0.67 [0.34, 0.99]
Total (95% CI)0.51 [0.31, 0.70]
Total yield (fixed): 78% (CE), 32% (barium radiography)
Test for heterogeneity: P = 0.001, I² = 72.9%
Test for overall effect: P < 0.001
-1 -0.5 0 0.5 1
Yield higher in barium radiography Yield higher in capsule endoscopy

David T. Rubin, MD 2011 10
How Often do Lesions Occur in Normal Volunteers?
Findings from a study of COX-2 selective NSAIDs and SB injury in normal volunteersNSAIDs, and SB injury in normal volunteers– 14% on no NSAIDS had “mucosal breaks” at
baseline
CE studies in osteoarthritis patients without GI symptoms and on no NSAIDSsymptoms and on no NSAIDS
– 17% on acetaminophen and no NSAIDS, had SB lesions at baseline
Goldstein et al. CGH 2005 Graham, et al CGH 2005
The Problem of Strictures

David T. Rubin, MD 2011 11
Capsule Retention
Capsule Retention Rate in CD Depends on Clinical Scenario
Author Patients Capsule CD?
(n) retention (%)(n) retention (%)
Herrerias 21 0 Suspected
Fireman 17 0 Suspected
Eliakim 20 0 Suspected
Sant’Anna 20 5 Susp (hi prob)
M 50 4 KMow 50 4 Known
Buchman 30 6 Known
Cheifetz 38 13 Known
Cheifetz 64 10 Suspected strictures

David T. Rubin, MD 2011 12
Small bowel radiographs:radiographs:
is it time to retire?
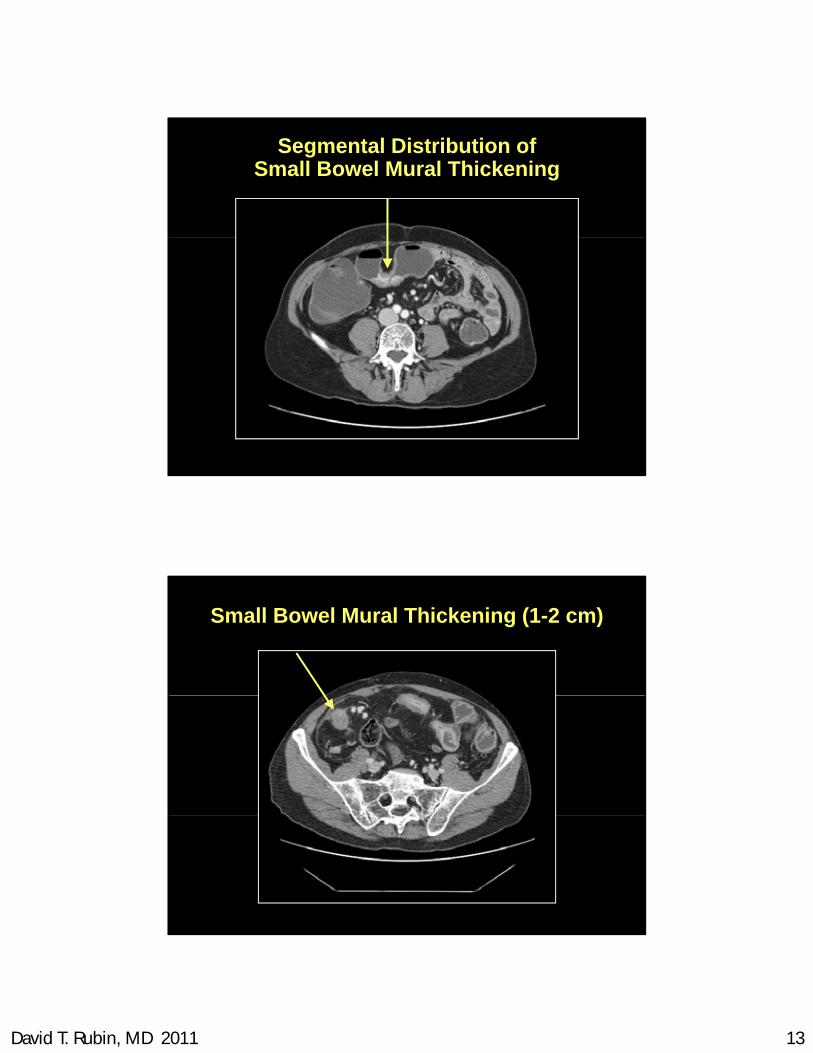
CT Enterography
Combines high-resolution CT scanning with some of the concepts of barium radiography
Ingestion of large volume of a negative contrast agent (either PO or via NJT) to distend loops– Water or diluted PEG
Intravenous contrast, scan after 70 seconds (venous phase)
Thin slices on helical CT
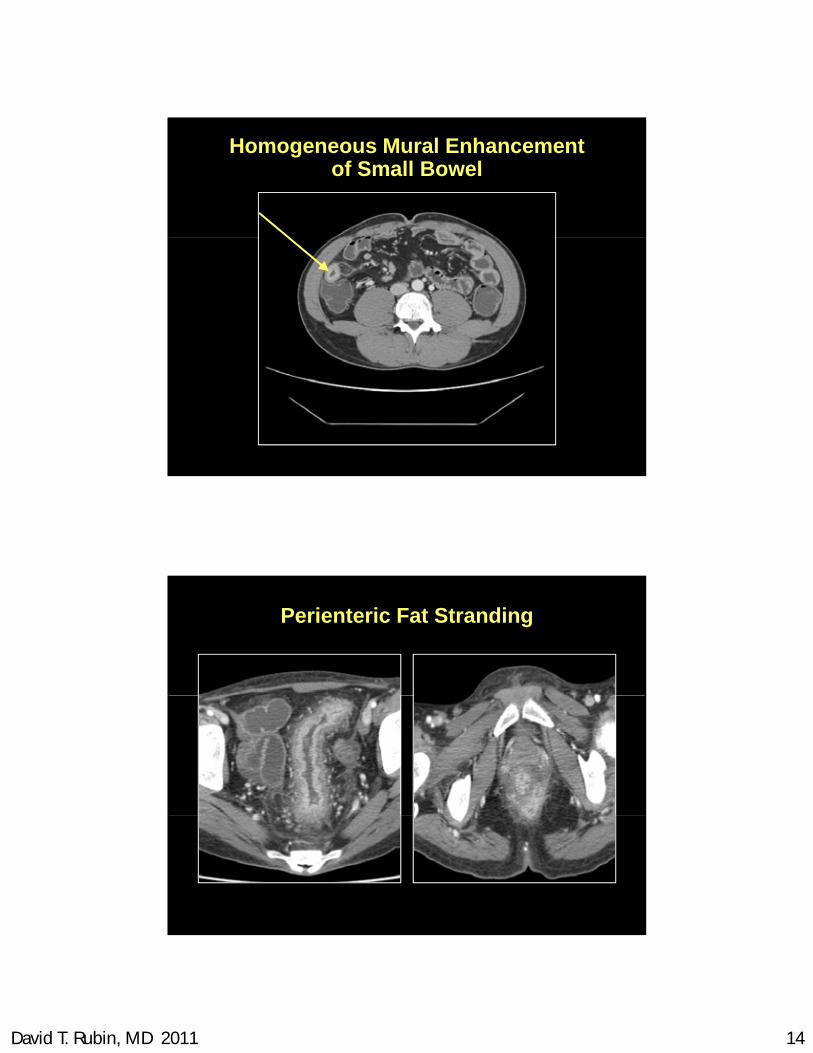
Signs of inflammation Signs of inflammation
David T. Rubin, MD 2011 13
Segmental Distribution of Small Bowel Mural Thickening
Small Bowel Mural Thickening (1-2 cm)
David T. Rubin, MD 2011 14
Homogeneous Mural Enhancementof Small Bowel
Perienteric Fat Stranding

David T. Rubin, MD 2011 15
Fistulas
Tracts
Usually enhancing (unless perianal)
+/- fluid/air/ fluid/air
Effective Doses of Radiation
CXR: 0.1 mSv
Round trip airflight NYC-London 0 1 mSv
CXR: 0.1 mSv
Round trip airflight NYC-London 0 1 mSv Round trip airflight, NYC-London, 0.1 mSv
Mammogram: 0.7 mSv
SBFT: 2-6 mSv
Average annual background radiation, 2.4 mSv
Standard CTE (single phase): 8-12 mSv
Radiation orker e pos re ann al limit 20 mSV
Round trip airflight, NYC-London, 0.1 mSv
Mammogram: 0.7 mSv
SBFT: 2-6 mSv
Average annual background radiation, 2.4 mSv
Standard CTE (single phase): 8-12 mSv
Radiation orker e pos re ann al limit 20 mSV Radiation worker exposure annual limit: 20 mSV
Bleed protocol CTE (triple phase): 30-40 mSv
International Space Station, annual: 170 mSv
Radiation worker exposure annual limit: 20 mSV
Bleed protocol CTE (triple phase): 30-40 mSv
International Space Station, annual: 170 mSv

David T. Rubin, MD 2011 16
MR Enterography
Ileal Inflammation
A. Enteroclysis
B. MRI Enterography
Schreyer AG, et al. Clin Gastroenterol Hepatol. 2004;2:491.

David T. Rubin, MD 2011 17
Accuracy of MRE versus Ileocolonoscopy (IC)
• 22 pediatric subjects underwent MRE and IC for newly diagnosed Crohn’s disease• 98 subjects with established Crohn’s disease
d t MRE d IC
• 4/10 false negative MRE’s were due to radiologic interpretation errors
Sensitivity(95% CI)
Specificity(95% CI)
TI/Anastomosis 72% (53% - 86%) 85% (74 – 92%)
Colorectum 59% (42% - 74%) 90% (80% - 96%)
underwent MRE and IC
• MRE has modest sensitivity for terminal ileal Crohn’s disease, utility in the colon is lower
• Radiologists interpretingMRE should be well-trained
Veereman et al. DDW 2011; abstract no. Su 1921Bruining et al. DDW 2011; abstract no. Su1189
• MRE had good sensitivity for ileal lesions, but sensitivity for colonic lesions was limited
Ability of MRI to Evaluate Therapeutic Response in Crohn’s Disease
• Magnetic resonance enterography (MRE) to evaluate response to Crohn’s therapy
• MR enteroclysis to evaluate effects of infliximab on transmural Crohn’s
• MR enteroclysis score of severity in ilealp py
• 27 subjects received adalimumab or corticosteroids for induction of remission
• Novel index (MaRIA) quantified severity of MR findings
• MaRIA correlated with CDEIS (r=0.70 at week 12)
• MaRIA score <40 predicted endoscopic remission (sensitivity 0.82, specificity
MR enteroclysis score of severity in ileal Crohn’s disease (MICD) calculated
• Primary endpoint: proportion of subjects with >2 points and >50% decrease in MICD at 26 weeks
• 15 subjects in final analyses
• 32% met primary endpoint
• Results were not compared with endoscopic or histological findings
0.85)
• MRE can accurately evaluate response to Crohn’s therapy
endoscopic or histological findings
• MR enteroclysis can monitor effects of infliximab in Crohn’s disease
• What should be done for patients who have evidence of active disease on MRI but are in clinical remission?
Van Assche et al. DDW 2011; abstract no. 344Ordás et al. DDW 2011; abstract no. 343
David T. Rubin, MD 2011 18
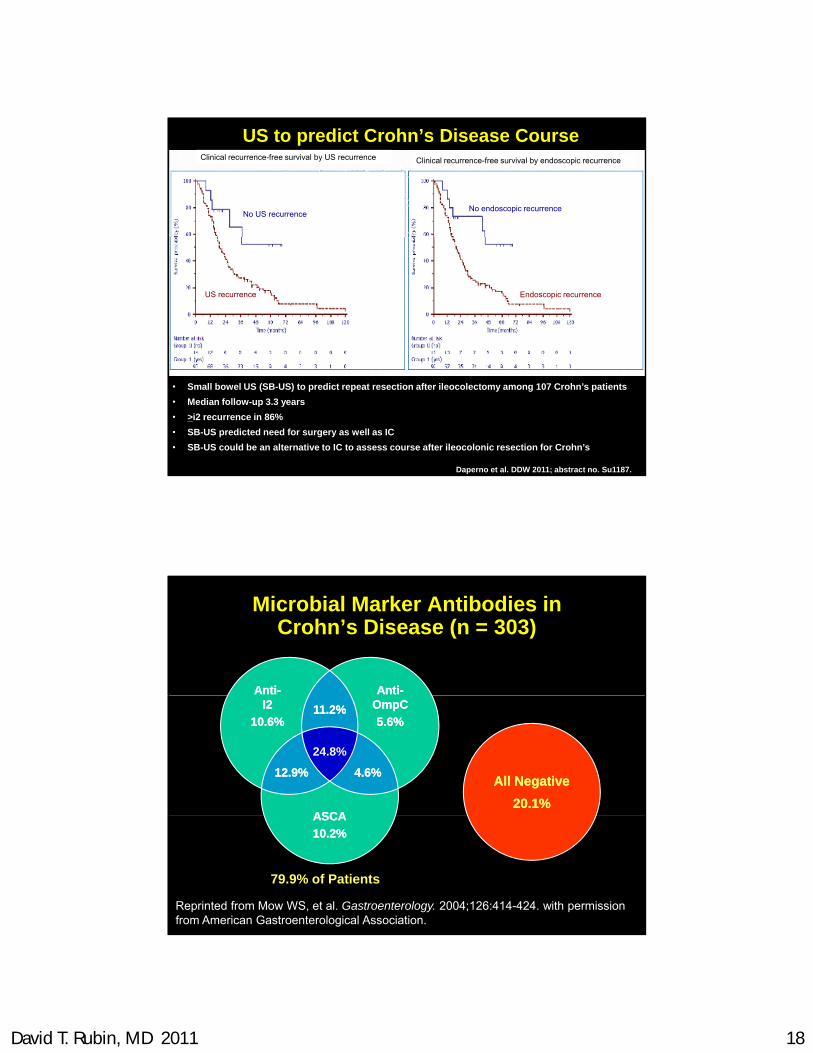
US to predict Crohn’s Disease Course
No US recurrenceNo endoscopic recurrence
Clinical recurrence-free survival by US recurrence Clinical recurrence-free survival by endoscopic recurrence
US recurrence Endoscopic recurrence
Daperno et al. DDW 2011; abstract no. Su1187.
• Small bowel US (SB-US) to predict repeat resection after ileocolectomy among 107 Crohn’s patients
• Median follow-up 3.3 years
• >i2 recurrence in 86%
• SB-US predicted need for surgery as well as IC
• SB-US could be an alternative to IC to assess course after ileocolonic resection for Crohn’s
Microbial Marker Antibodies in Crohn’s Disease (n = 303)
AntiAnti--AntiAnti--
All NegativeAll Negative
20.1%20.1%ASCAASCA
24.8%
11.2%11.2% OmpCOmpC
5.6%5.6%
I2I2
10.6%10.6%
12.9%12.9% 4.6%4.6%
79.9% of Patients
ASCAASCA
10.2%10.2%
Reprinted from Mow WS, et al. Gastroenterology. 2004;126:414-424. with permission from American Gastroenterological Association.

David T. Rubin, MD 2011 19
Serology as Initial Test?
• No prospectively supported datap p y pp
• Diagnostic algorithms not published
• ↓ prevalence: ↑ false positives
• ↑ in autoimmune disorders– ASCA: celiac, Behcet's, PBC, hepatitis
ANCA i hili & ll liti– ANCA: eosinophilic & collagenous colitis
– OMP-C & I2: infection, diverticulitis
• Cost
Austin et al. Clin Gastr Hep 2007;5:545–547Damoiseaux et al. J Clin Immunol 2002; 2(5):281-8
Serologies in IBD: What is State of the Art in 2011?
Diagnosis vs. Prognosis
The accurate integration of serology testing is a The accurate integration of serology testing is a function of the pre-test probability of IBD– i.e. If pre-test probability is low, positive serologies are
likely to be false positives– i.e. If pre-test probability is high, negative serologies
are likely to be false negatives
Serologies therefore are of diagnostic value in patients with intermediate likelihood of IBD

David T. Rubin, MD 2011 20
5-year clinical course after diagnosis
Age at onset40 40 0 0004
Predictors of Disabling Disease:
– <40 years vs ≥40 years; p=0.0004
Location of disease– small bowel + colon vs small bowel only; p=0.002
Smoking status– smoker vs ex- or non-smoker; p=0.09
Perianal lesion at diagnosis– yes vs no; p=0.01
Required steroids for first flare– yes vs no; p=0.0001
Beaugerie et al, Gastroenterology 2006; 130: 650
Serum Immune Responses Predict Rapid Disease Progression in Children with CD
n=70
p=0.03
n=97
Serologic markers: ASCA, anti-OmpC, anti-I2, anti-CBir1
Dubinsky M et al. Am J Gastroenterol 101:2006.

David T. Rubin, MD 2011 21
The Risk of Chronic Pouchitis is Significantly Increased With Pre-Op High Level pANCA
100f
25
50
75
100
ativ
e In
cid
ence
of
ic P
ou
chit
is (
%)
High level
M di l l
P = 0.03
0
25
0 6 12 24 36 48 60
Months After IPAA
Cu
mu
laC
hro
ni
Low levelMedium level
pANCA-neg
Fleshner, P et al. Gut 2001
Should we be treating to achieve mucosal healing?
YES!!Th i fl d d i j d
WAIT- NOT YET!W ’t t th i t• The inflamed and injured
bowel is the hallmark of active disease
• A healed bowel is the sign of disease control or resolution
M f th i
• We can’t get there in most patients with existing therapies.
• How is this defined???– Partial?– Complete?– Histology?• Many of our therapies can
achieve it.
• Existing strategies are not effective at longer term management control.
– Histology? – Endoscopy?– Radiographic??
• Cost
• Convenience

David T. Rubin, MD 2011 22
10 000
20 000 * * p< 0.0001*
Fecal Calprotectin Levels in IBD Patients with Active Disease and “Mucosal Healing”
100
1000lp
rote
ctin
mg/
LLo
g sc
ale
��
10
1
Ca
Crohn’s diseaseactive / remission
Ulcerative colitisactive / remission
Roseth Scand J Gastro 2004
Mucosal healing
IBD Diagnosis and Management: The Near Future
First Visit:
IBD Panel
Phenotype: Location, EIM, Behavior
Serology Genetics Proteomics
IBD Subtype
Disease Prognosis
Patient-specific treatment plan
Targeted-specific therapyDisease Monitoring for Efficacy and Safety