diagnosis & management of resistant hypertension -...
TRANSCRIPT

Diagnosis & Management of
Resistant Hypertension
Dr.Vinod Sharma
National Heart Institute
New Delhi

“As we enter the third millennium,
we are on the verge of the
biggest epidemic of cardiovascular
disease in human history,
most of it blood pressure related”

Hypertension in India
PREVALENCE
Urban Adults 25%
Rural Adults 10-15%
JAPI Feb 2013

Hypertension – Rule of Halves
Only ½ have been diagnosed.
Only ½ of those diagnosed have been treated.
Only ½ of those treated are adequately
controlled.
Thus only 12.5% overall are adequately
controlled.
1999 WHO – ISH Guidelines
• Blood pressure remaining above goal in spite
of concurrent use of 3 antihypertensive agents of
different classes.
• Ideally, 1 of the 3 agents should be a diuretic &
all agents should be prescribed at optimal dose
amounts.
Resistant Hypertension

Definition Highlights
• Use of diuretic recommended but not required before
diagnosing resistant hypertension.
• Doses should be optimal but not necessarily maximal
before diagnosing resistant hypertension.
• Controlled resistant hypertension: high blood pressure
controlled but with use of 4 of more agents should be
considered resistant.

Resistant HT: Introduction
This definition does not apply to patients who have been
recently diagnosed with HT
Resistant HT is not synonymous with uncontrolled HT
Uncontrolled HT includes all hypertensive patients who lack
BP control under treatment, namely,
- those receiving an inadequate treatment regimen,
- those with poor adherence, and
- those with undetected secondary HT, as well as
- those with true treatment resistance
J Am Coll Cardiol 2008;52:1749–57


Prevalence (contd)
• ACCOMPLISH (Avoiding Cardiovascular events through
Combination therapy in Patients Living with Systolic
Hypertension) Study – 25 to 28% of subjects remained
uncontrolled in spite of intensification of treatment.
Circulation 2012: 125: 1594-96

Resistant hypertension is primarily a
systolic and age related problem
• Diastolic BP goal achieved ≥ 90% in the
major trials
• Systolic BP goal achieved 60-65% in the
major trials
• True resistance occurs in about 15%

Drug-related causes
58%
Nonadherence 16%
Unknown 6%
Office resistance
6%
Psychological causes
9%
Secondary HTN 5%
Interfering substances
1%
Am J Hypertens 2003;16:925-930
Cause of resistance
found in 133/141 –
94% (83/91 – 91%)
cases
Resistant HT: Primary Cause
Pseudo-resistance
Lack of BP control with
appropriate treatment in a
patient who does not have
resistant hypertension
J Am Coll Cardiol 2008;52:1749–57

Pseudo-resistance (Contd)
J Am Coll Cardiol 2008;52:1749–57
Causes of Pseudo-Resistant Hypertension

Resistant HT
Factors Contributing to
Resistant HT
J Am Coll Cardiol 2008;52:1749–57

Common
• Obstructive sleep apnea
• Renal parenchymal disease
• Primary aldosteronism
• Renal artery stenosis
Secondary Causes of Resistant
Hypertension
Secondary Causes of Resistant Hypertension
Uncommon
Pheochromocytoma
Cushing’s disease
Hyperparathyroidism
Aortic coarctation
Intracranial tumor

RHTN & Obstructive Sleep Apnoea
Prevalence – Men 24%; Women 9% (Wisconsin Sleep
Cohort Study)
High prevalence of RHTN in OSA (n = 41); 96% men,
65% women (apnea – hyperapnoea Index > 10)
Mechanism
- Increased sympathetic activity
- Increased Aldosterone levels
- Increase in reactive oxygen species with
concomitant reductions in nitric oxide bioavailability.

RHTN & Obstructive Sleep Apnoea
A BP increase during progressive stages of sleep.
Significant correlation between Aldosterone level &
severity of OSA.
Chronic parapharyngeal fluid retention mediated by
aldosterone excess and nocturnal rostral fluid shift from
lower extremities contributes to the worsening airways
resistance in OSA.

RHTN & Obstructive Sleep Apnoea
“The hypothesis of Aldosterone excess worsening
severity of OSA is supported by a prospective study
showing a reduction in severity after 8 weeks of treatment
with spironolactone in patient with RHTN & Obstructive
Sleep apnea”.
J Hum Hypertens 2010

RHTN & Aldosterone
Prevalence of primary hyperaldosteronism in patients
with RHTN 11 – 20% Lancet 2008: 371
Compared to Conn’s syndrome, picture of biochemically
confirmed primary hyperaldosteronism remains diverse:
- shows negative imaging
- remains Idiopathic
- hypokalemia is usually a late manifestation
- normokalemia is quite common among these
patients
J. Clin Endocrinol Metab 2009

RHTN & Renal Artery Stenosis
Renovascular disease ( >70% stenosis) found in more
than 20% cases undergoing CAG.
Role of such lesion in causation of hypertension is
unknown.
> 90% RAs are atherosclerotic (elderly male), < 10% are
due to FMD (F, <50 yrs of age).
Large experience with both surgical and endovascular
revascularization indicates that some patients with
renovascular hypertension experienced improved BP
control although RCT in general have not shown
convincing benefit in regard to improvement in renal
function or BP control.

Renal Artery Stenosis: Investigation
Screening
Ultrasound, Doppler
Renogram /scintigraphy
Peripheral PRA
Definitive
CT angio, MRA, DSA
Conventional angio
Renal vein renin ratio

Resistant HT (Contd)
How to evaluate & manage
with Patients Appearing to
Have Resistant HT?
J Am Coll Cardiol 2008;52:1749–57

Exclude Pseudoresistance
•Is patient adherent with prescribed regimen?
•Obtain home, work, or ambulatory blood pressure
readings to exclude white coat effect
Identify and Reverse Contributing Lifestyle Factors
•Obesity
•Physical inactivity
•Excessive alcohol ingestion
•High salt, low-fiber diet

Modification Approximate SBP
Reduction
Weight Reduction 5-10 mmHg/10kg
Adopt DASH eating plan 8-14 mmHg
Dietary sodium reduction 2-8 mmHg
Physical activity 4-9 mmHg
Moderation of alcohol intake 2–4 mmHg
Lifestyle Modifications….. help

•Non-steroidal anti-inflammatory agents
•Sympathomimetics
- Diet pills
- Decongestants
•Stimulants
•Oral contraceptives
•Licorice
•Ephedra
Discontinue or Minimize Interfering Substances

Screen for Secondary Causes of Hypertension
• Obstructive sleep apnea (snoring, witnessed apnea, excessive daytime
sleepiness)
• Primary aldosteronism (elevated aldosterone/renin ratio)
• Chronic kidney disease (creatinine clearance <30 mL/min)
• Renal artery stenosis (young female, known atherosclerotic disease,
worsening renal function)
• Pheochromocytoma (episodic hypertension, palpitations, diaphoresis,
headache)
• Cushing’s disease (moon facies, central obesity, abdominal striae,
inter-scapular fat deposition)
• Aortic coarctation (differential in brachial or femoral pulses, systolic
bruit)

Resistant Hypertension
Constructing a potent Antihypertensive
Regimen

Resistant Hypertension
Do not accept blood pressure that are not at
target: there are still things that can be done.
Revisit the initial regimen and ensure optimal
dosed drug & combination.

Resistant Hypertension
Do not keep Adding medications
- appropriate & optimally dosed 3 drug regimen
should suffice for BP control.
- adding multiple additional drug has potential for
serious side effects.
- attempt to find an underlying cause & tailoring
treatment for that cause is necessary.
RHTN – Constructing an effective
antihypertensive regimen
Are dose titrations appropriate?
E.g. Carvedilol should be maximized to
25-50 mg twice a day.
Low dose diuretics 12.5 mg HCTZ will not
work in chronic renal disease and may
have a substandard effect in others.

Resistant Hypertension – Constructing a
potent antihypertensive regimen
Adding a complementary agent from another class of
antihypertensives may be superior to “maxing out” single agent
first.
Doubling the dose of one drug (or monotherapy) had
approximately one-fifth of the equivalent incremental blood
pressure lowering effect of adding another drug class before trying
to max-out.
CAVEATS: 50 mg HCTZ or combination Diuretics.
Wald DS et al: Combination treatment Vs Monotherapy in
reducing blood pressure: a meta-analysis on 11,000 participants in
42 trials. Am J Med 2009: 122: 290

Resistant Hypertension
Perform a “Diuretic Review”.
Diuretics is the mainstay of the resistant
hypertension patient medication regimen &
should be optimized to see full therapeutic
benefit.

Diuretics
Studies indicate that patients with
resistant HT
Frequently have inappropriate volume
expansion contributing to their treatment
resistance such that a diuretic is essential to
maximize BP control
In most patients, use of a long-acting
thiazide diuretic will be most effective
Circulation. 2008;117:e510-e526

Resistant Hypertension – Diuretic Review
Chlorthalidone may give more “bang for the buck” than HCTZ.
- Chlorthalidone is more patent than HCTZ (50mg HTCZ = 25 –
37 mg CHTD).
- It has longer duration of action (16 – 24 hrs Vs 48-72 hrs)
- Gives better lowering of BP
- 1 month of chlorthalidone use translates into 1 day of additional
life.
- 23 year follow up of Cohort – Chlorthalidone can be a “gift that
keeps on giving”.

Resistant Hypertension – Diuretic Review
Thiazide Diuretic may lack effect at lower GFR (Stage 3
Kidney disease).
Frusemide may a better option than thiazide for BP
control.
Because of shorter half life, Frusemide may be dosed
twice.
Resistant Hypertension
Is Patient taking Betablockers?

Resistant Hypertension - Betablockers
Betablockers are no longer acceptable first line
therapies, unless there are compelling indications like
CAD, CHF etc. &
One agent specifically Atenolol may increase central
aortic pressure Central Study, J Clin Hypert 2011
Switch to a optimal dose of dual acting Beta blocker
(Carvedilol or Labetalol).
- additional lowering of BP due to ∞ blockade.
- better LV / Vascular coupling
- carvedilol does not increase Insulin resistance.

RHTN – Constructing a antihypertensive
regimen
Antihypertensives at night
“When you snooze you lose”
Controlling BP in chronic renal disease
“Night time is the right time”
Rutecki GW. Consultant Live 2011
Use a long half life agent at night rather
than in the morning.

α1-Adrenergic Receptor Blockers
Not to be used for monotherapy:
ALLHAT (class effect)
May be used as an add-on for resistant
hypertension
May cause urinary incontinence,
especially in females, due to bladder outlet
relaxation

RHTN – Constructing an effective
antihypertensive regimen
The Use of last line agents viz. Clonidine
lacks outcome data and may add adverse
drug reaction & decreased adherence
because of dosing frequency.

RHTN – Constructing a potent
antihypertensive regimen
Question the value of Hydralazine
Hydralazine does not have much
evidence of efficacy for prevention of
cardiovascular benefit when used for
essential hypertension.
Cochrane Database Syst Rev 2011

RHTN – Constructing a potent
antihypertensive regimen
MINOXIDIL Should be a last Resort
Potent vasodilator and should be used with betablocker
& diuretics.
Difficult to use & fraught with many serious side effects
(Edema, anasarca, pericardial effusion & hirsutism).
Can be used for select patients by physicians who are
comfortable with dosing & side effects
J Hyperten 2007

Mineralocorticoid Receptor Antagonists
Consistent with reports of a high prevalence
of primary aldosteronism in patients with
resistant HT have been studies
demonstrating that
Mineralocorticoid receptor antagonists
provide significant antihypertensive benefit
when added to existing multidrug regimens
Circulation. 2008;117:e510-e526

RHTN – Constructing an optimal
antihypertensive regimen
Switch to a regimen relying on a
spironolactone backbone.
Multiple studies attested efficacy of
spironolactone in patients with RHTN, especially
those with OSA.
Dose of spironolactone may be titrated
upwards, needs serial K+ monitoring especially
in CKD.
J Hum Hypertens 2012

Mineralocorticoid Receptor Antagonists (Contd)
Spironolactone
Used for resistant HT with normal
aldosterone levels, 12.5-50mg/daily
Additional benefits: antiproteinuric,
improves heart failure survival (RALES)
10% gynecomastia
Not when creatinine > 2.5, K > 5.0

Drug Combinations
• Chlorthalidone 25mg + spironolactone 12.5-50 mg Excellent diuretic maximization, also vs hypokalemia
Chlorthalidone, can
↓ s. K+ enough to cause cardiac arrest
Aldosterone blockers spironolactone eplerenone can
Protect vulnerable patients and
Significantly reduce BP resistant to ≥ 3 drugs,
A logical way to provide maximal anti-HT efficacy and
to prevent hypokalemia might be a
Combination of chlorthalidone and spironolactone
12.5/25.0 mg/d
Hypertension 2009;54;951-953

RHTN – Optimal Antihypertensive Regimen
Preferred Antihypertensive Combinations
A RAAS inhibitor & a Calcium Channel Blocker
A RAAS inhibitor & a Diuretics (especially a
thiazide)
A RAAS inhibitor & a Calcium Channel Blocker
plus a Diuretic
Eur Heart J: 2011: 32

RHTN – Optimal Antihypertensive Regimen
Acceptable Combinations
Betablockers & Diuretics
Calcium Channel Blockers & Diuretics
Dual Calcium Channel Blockade (DHP & NDHP agent)
Unacceptable Combinations
Dual RAAS blockade
RAAS inhibitors plus betablockade
Betablockers plus antiadrenergic drugs
Eur Heart J 2011

Diagrammatic representation of L/N-dual action
of cilnidipine
Efferent arterioles Afferent arterioles

Newer therapeutic agent
Endothellin antagonist: Darusentan
ACEI/ ARB + naprilysin inhibitor : LCZ 696
Aldosternone synthase inhibitors: Fadrozole, LCI 1699

Endothelial receptor antagonist
Class of agents that may prove useful for resistant HT
is endothelin-receptor antagonists (ERAs)
In patients with mild-to-moderate essential HT, both
nonselective and selective (type A receptor) ERAs
Produce BP reductions comparable to those of common
antihypertensive agents, but
Concerns about adverse events precluded their use as a
treatment option for uncomplicated hypertension
Darusentan (Contd)
Lancet 2009
Randomised, double-blind study was
undertaken in 117 sites in North and South
America, Europe, New Zealand, and Australia
Lancet 2009; 374:1423-1431
Darusentan (Contd)
Results
The mean reductions in clinic systolic and
diastolic blood pressures were
9/5 mm Hg (SD 14/8) with placebo,
17/10 mm Hg (15/9) with darusentan 50 mg,
18/10 mm Hg (16/9) with darusentan 100 mg,
18/11 mm Hg (18/10) with darusentan 300 mg
(p<0·0001 for all effects)
Lancet 2009; 374:1423-1431

Darusentan (Contd)
Results (Contd)
The main adverse effects were related to fluid
accumulation
Oedema or fluid retention occurred in 67 (27%) patients
given darusentan compared with 19 (14%) given placebo
One patient in the placebo group died (sudden cardiac
death), and five patients in the three darusentan dose
groups combined had cardiac-related serious adverse
events
Lancet 2009; 374:1423-1431

Darusentan (Contd)
Interpretation
Darusentan provides additional reduction
in blood pressure in patients who have not
attained their treatment goals with three or
more antihypertensive drugs. As with other
vasodilatory drugs, fluid management with
effective diuretic therapy might be needed
Lancet 2009; 374:1423-1431

Interventional Management of
Resistant Hypertension

CORAL (Cardiovascular Outcomes in
Renal Atherosclerotic Lesions) TRIAL 2013
STENTS NO BENEFIT IN RENAL ARTERY
STENOSIS
“Effective Medical Therapy should be the first line of
treatment in patients with presumed Renovascular
Hypertension”. For patients who fail medical therapy or
are unable to tolerate medical therapy, stenting remains
a reasonable option.
NEJM 2013

RHTN – Renal Denervation Therapy (RDN)
RDN is a use of low energy radiofrequency
delivered via a percutaneously inserted catheter
for the bilateral disruption of afferent & efferent
sympathetic nerves in the adventitia of renal
arteries.
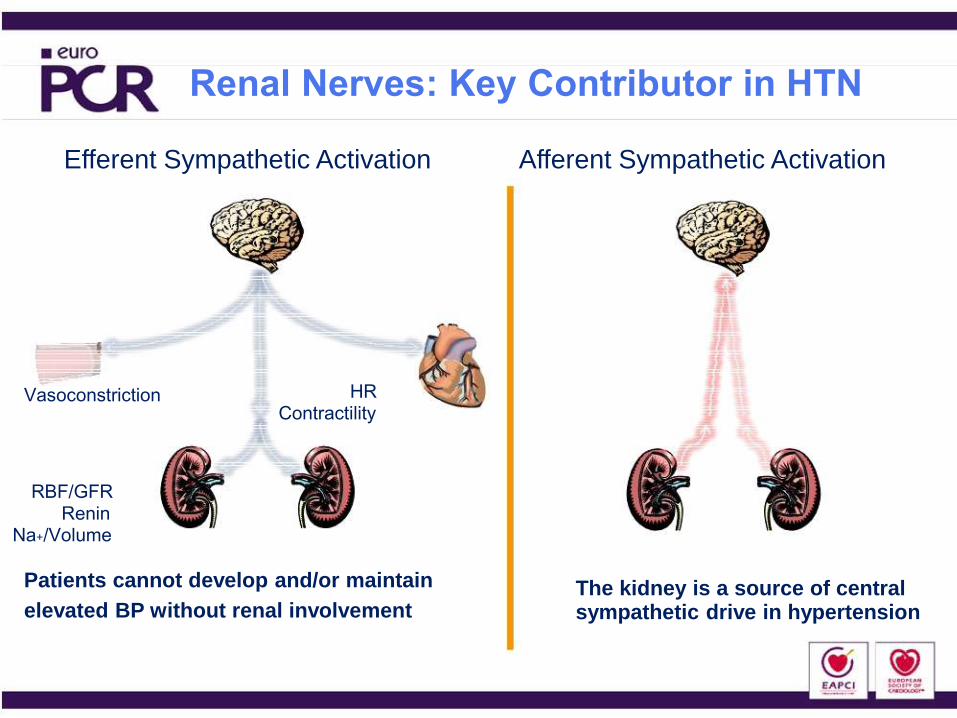
Renal Nerves: Key Contributor in HTN
Efferent Sympathetic Activation Afferent Sympathetic Activation
HR Vasoconstriction Contractility
RBF/GFR Renin
Na+/Volume
Patients cannot develop and/or maintain The kidney is a source of central elevated BP without renal involvement sympathetic drive in hypertension

Anatomical Location of Renal
Sympathetic Nerves
• Arise from T10-L1
• Follow the renal artery to the kidney
• Primarily lie within the adventitia
Vessel
Lumen
Media
Adventitia
Renal
Nerves

RHTN – Renal Denervation Therapy Simplicity HTN – 1
Multi-centre, proof-of-principle study to demonstrate feasibility,
efficacy & safety of RDN in patients with RHTN.
N = 45, Mean BP 177 / 101 mm Hg; Mean of 4.7 Antihypertensive
drugs.
BP reduction – 21/11 mm Hg at 6 months
27/17 mm Hg at 12 months
32/14 mm Hg at 24 months
Decrease in LV mass of 9%
----------------------------------------------------------------------------------------------
Encouraging result
Did not include a control group & was not a blinded study.
Placebo effect could not be excluded.
NEJM 2009

RHTN – Renal Denervation Therapy
Simplicity HTN - 2
Multicentre, Randomized Control, trial in 106 patients
BP reduction – 32 / 12 – 6 months
Similar at 12 months
------------------------------------------------------------------------------
Non-blinded Study
SIMPLICITY HTN – 3 ONGOING
LANCET 2010

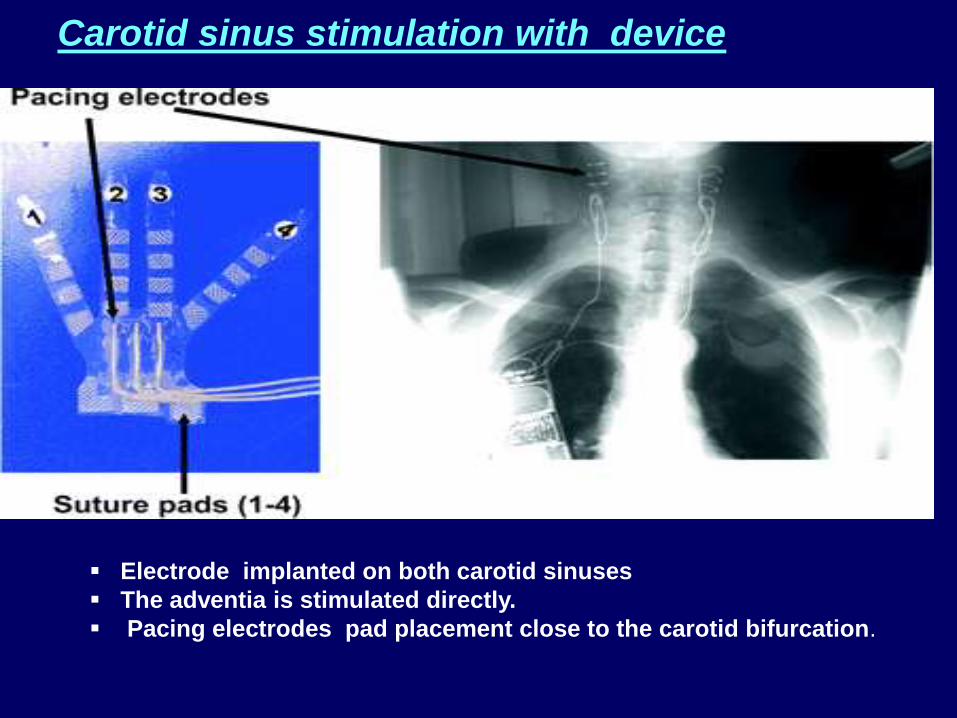
Carotid sinus stimulation with device
Electrode implanted on both carotid sinuses
The adventia is stimulated directly.
Pacing electrodes pad placement close to the carotid bifurcation.
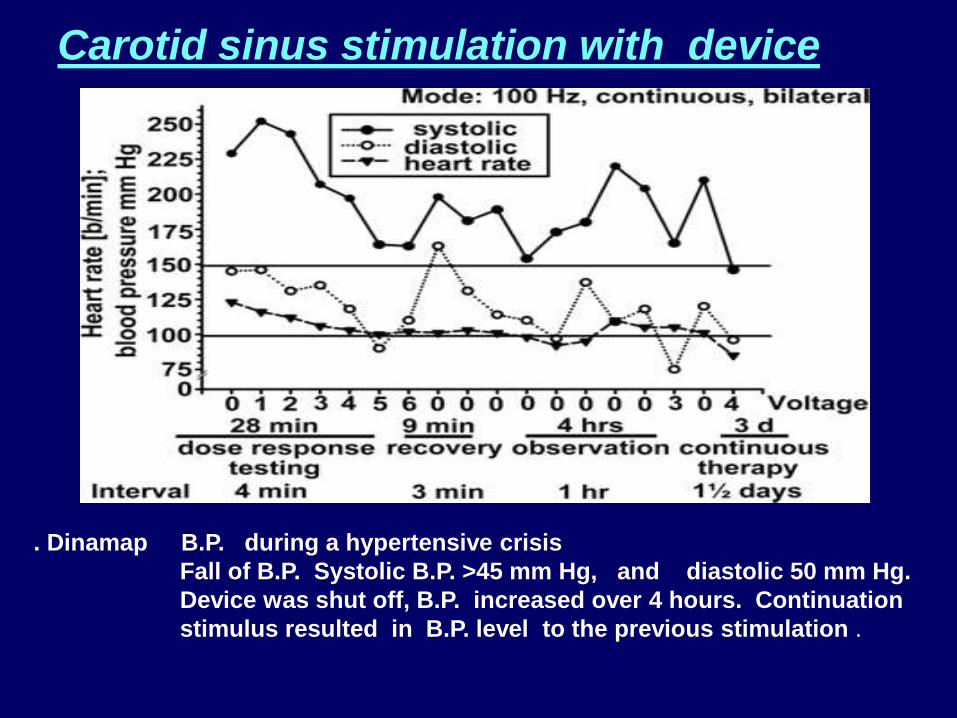
Carotid sinus stimulation with device
. Dinamap B.P. during a hypertensive crisis
Fall of B.P. Systolic B.P. >45 mm Hg, and diastolic 50 mm Hg.
Device was shut off, B.P. increased over 4 hours. Continuation
stimulus resulted in B.P. level to the previous stimulation .

Rheos Device
Promising new technology
May help those difficult to control
patients in combination with drug
therapy
May be useful in non compliant patients
May be useful in patients intolerant to
medication

RHTN – Diagnosis & Management CONCLUSION
RHTN, a common problem, in a subset of patients.
Pseudo resistance needs to be rules out.
ABPM a very helpful tool.
Secondary causes must be rules out & treated appropriately.
Judicious up-titration of single / or appropriate combination of
drugs overcomes this problem.
Diuretics, cornerstone of therapy of RHTN.
Stenting Renal artery in RAS, does not help much.
Newer drugs & interventions holds promise for the future.

THANK YOU