diagnosis and management of pergolide-induced fibrosis
TRANSCRIPT

12. Bucher SF, Seelos KC, Oertel WH, Reiser M, Trenkwalder C.Cerebral generators involved in the pathogenesis of restless legssyndrome. Ann Neurol 1997;41:639–645.
13. Lee MS, Choi YC, Lee SH, Lee SB. Sleep-related periodic legmovements associated with spinal cord lesions. Mov Disord 1996;11:719–722.
14. Hartmann M, Pfister R, Pfadenhauer K. Restless legs syndromeassociated with spinal cord lesions. J Neurol Neurosurg Psychiatry1999;66:688–689.
15. Brown LK, Heffner JE, Obbens EA. Transverse myelitis associ-ated with restless legs syndrome and periodic movements of sleepresponsive to an oral dopaminergic agent but not to intrathecalbaclofen. Sleep 2000;23:591–594.
16. Trenkwalder C, Bucher SF, Oertel WH. Electrophysiological pat-tern of involuntary limb movements in the restless legs syndrome.Muscle Nerve 1996;19:155–162.
17. Connor JR, Boyer PJ, Menzies SL, et al. Neuropathological ex-amination suggests impaired brain iron acquisition in restless legssyndrome. Neurology 2003;61:304–309.
18. Grol CJ. Chemistry of dopamine. In: Horn AS, Korf J, WesterinkBHC, editors. The neurobiology of dopamine. London: AcademicPress; 1979. p 7–27.
19. Campbell NR, Hasinoff B. Ferrous sulfate reduces levodopa bio-availability: chelation as a possible mechanism. Clin PharmacolTher 1989;45:220–225.
20. Youdim MB, Gassen M, Gross A, Mandel S, Grunblatt E. Ironchelating, antioxidant and cytoprotective properties of dopamine re-ceptor agonist; apomorphine. J Neural Transm Suppl 2000;58:83–96.
Diagnosis and Management ofPergolide-Induced Fibrosis
Pinky Agarwal, MD, Stanley Fahn, MD,and Steven J. Frucht, MD*
Department of Neurology, Columbia-Presbyterian MedicalCenter, Division of Movement Disorders, New York,
New York, USA
Abstract: We report on 2 patients treated with pergolide, 1of whom developed pleural fibrosis and the other retroper-itoneal fibrosis. In both cases, an extensive diagnostic eval-uation and surgical intervention were required to reach adiagnosis. Based on our experience with these patients anda review of cases of pergolide-induced fibrosis in the En-glish-language literature, we propose guidelines for the di-agnosis and management of this rare complication. © 2004Movement Disorder Society
Key words: pergolide; pleural fibrosis; retroperitoneal fibro-sis; surgery
The ergot dopamine agonist pergolide mesylate ismost commonly prescribed to treat Parkinson’s disease(PD) and restless leg syndrome (RLS). Pergolide is usedas monotherapy in patients with mild symptoms andsigns of PD and also as an adjunct to levodopa in patientswho develop motor fluctuations and dyskinesias. Likeother ergot agonists, pergolide may rarely induce fibrosisaffecting the pleural, retroperitoneal, or cardiac valvularstructures.1–14 Our experience with 2 patients who devel-oped fibrosis during treatment with pergolide promptedus to review the English-language literature to look forcommon features that could assist in the diagnosis andmanagement of this rare complication.
MATERIALS AND METHODS
We performed a Medline search using the key words“pergolide” and “fibrosis.” Only articles published inEnglish were reviewed, and publications referenced in thesearticles were also reviewed. We identified 12 studies1–7,11–15
describing 24 patients who developed symptomatic fibrosisduring the course of treatment with pergolide.
CASE SUMMARIES
Case 1
A 65-year-old man presented at age 54 with 1 year oftremor and pain in the right hand. He was diagnosed withPD and treated with pergolide, with good symptomaticbenefit. To obtain adequate relief of symptoms, the doseof pergolide was gradually increased to 7.5 mg/day.Levodopa (L-dopa) was added 5 years later because ofmotor deterioration. Eight years after the introduction ofpergolide, he developed a cough and shortness of breath.A magnetic resonance imaging scan of the chest revealeda possible mass in the left lung. A diagnostic work-upwas performed at another medical center, including anevaluation of pleural fluid (no evidence of tuberculosis ormalignancy), a bronchial biopsy (unrevealing), and aneedle biopsy consistent with pulmonary fibrosis.
Despite discontinuation of pergolide, a computed to-mography (CT) scan of the chest 1 year later showedpersistence of pleural and parenchymal fibrosis. One yearafter discontinuing pergolide, he developed severe bilat-eral leg edema and dysuria. His erythrocyte sedimenta-tion rate (ESR) was 100 mm/hr. A CT scan of theabdomen revealed thickening of the retroperitoneum,which was highly suggestive in appearance of retroper-itoneal fibrosis. The retroperitoneal mass was not acces-sible to biopsy, because it encased the abdominal aorta.An echocardiogram showed no evidence of cardiac val-vular fibrosis. A retrograde pyelogram showed stricturesof both ureters, requiring ureteral stents.
*Correspondence to: Dr. Steven J. Frucht, The Neurological Insti-tute, 710 West 168th Street, New York, NY 10032.E-mail: [email protected]
Received 25 November 2003; Accepted 14 February 2004Published online 19 May 2004 in Wiley InterScience (www.
interscience.wiley.com). DOI: 10.1002/mds.20200
PERGOLIDE-INDUCED FIBROSIS 699
Movement Disorders, Vol. 19, No. 6, 2004
TA
BL
E1.
Cli
nica
lco
urse
ofpa
tien
tsw
hode
velo
ped
fibro
sis
onpe
rgol
ide
Patie
ntno
.(R
ef.)
Age
(yr)
Gen
der
Dx
mg/
day
Rx
(yr)
tto
Dx
(mo.
)Sy
mpt
oms
ESR
Imag
ing
Path
olog
yC
ours
e
1(1
)63
MPD
12.
514
Che
stpa
in,
dysp
nea,
coug
h,an
emia
,w
eigh
tlo
ss40
–55
CX
Ran
dC
Tch
est:
pleu
ral
thic
keni
ngE
cho:
peri
card
ial
thic
keni
ng
Thi
ck,
calc
ified
peri
card
ium
Tig
htba
nds
arou
ndsu
peri
oran
din
feri
orve
naca
va
Tot
alpe
rica
rdec
tom
yw
ithre
solu
tion
ofsy
mpt
oms
2(1
)61
MPD
32
0E
dem
aof
leg,
urin
ary
freq
uenc
y,gr
oin
pain
57C
Tab
d:se
vere
left
hydr
onep
hros
is,
retr
oper
itone
alfib
rosi
sR
etro
grad
eur
eter
ogra
phy:
stri
ctur
ein
mid
-ure
ter
NA
Impr
ovem
ent
ingr
oin
pain
,re
duct
ion
inE
SR,
with
pred
niso
ne20
mg/
day
3(1
)70
MPD
3.75
1.5
6Sh
ould
eran
dch
est
wal
lpa
in;
Mild
dysp
nea
onex
ertio
nN
AC
XR
and
CT
ches
t:ri
ght
pleu
ral
thic
keni
ngPl
eura
lbi
opsy
:de
nse,
calc
ified
fibro
ustis
sue
No
clin
ical
orra
diog
raph
icim
prov
emen
t4
(2)
67M
PDN
A1
6D
yspn
ea,
mild
cong
estiv
ehe
art
failu
reN
AC
Tch
est:
calc
ifica
tion
ofpe
rica
rdiu
mC
XR
:bi
late
ral
pleu
ral
effu
sion
sE
cho:
righ
tat
rial
enla
rgem
ent,
thic
kene
dpe
rica
rdiu
m
NA
Impr
ovem
ent
afte
rpe
rica
rdec
tom
y
5(3
)65
MR
LS
3.5
330
Wei
ght
loss
,dy
spne
a,fa
tigue
NA
CX
R:
hydr
opne
umot
hora
xT
hora
scop
y:pl
aque
-lik
ele
sion
son
ches
tw
all
Bro
ncho
alve
olar
lava
ge:
reac
tive
epith
elia
lce
llsL
ung
biop
sy:
chro
nic
infla
mm
atio
n
Impr
ovem
ent
indy
spne
a,C
XR
and
pulm
onar
yfu
nctio
nte
sts
with
2w
kof
ster
oids
6(4
)68
FPD
22
0L
eged
ema,
wei
ght
gain
,ab
dom
inal
pain
,an
emia
NA
CT
abd:
soft
tissu
esu
rrou
ndin
gur
eter
sR
enal
ultr
asou
nd:
bila
tera
lhy
dron
ephr
osis
Ret
rogr
ade
uret
erog
raph
y:bi
late
ral
uret
eric
stri
ctur
es
NA
Res
olut
ion
ofsy
mpt
oms
afte
rst
oppi
ngpe
rgol
ide
7(5
)63
FPD
4.5
112
Dys
pnea
,le
ged
ema,
wei
ght
gain
,an
emia
NA
CT
abd:
retr
oper
itone
alfib
rosi
sA
bdul
tras
ound
:bi
late
ral
hydr
onep
hros
is
NA
Res
olut
ion
ofhy
dron
ephr
osis
with
sten
ting
8(6
)68
FPD
12.
53
Lef
tle
ged
ema,
anem
ia,
diur
esis
127
CT
abd:
retr
oper
itone
alfib
rosi
ssu
rrou
ndin
gle
ftur
eter
and
kidn
eyA
bdul
tras
ound
:m
oder
ate
dila
tatio
nof
rena
lpe
lvis
and
uret
er
Ret
rope
rito
neal
fibro
sis
Res
olut
ion
ofsy
mpt
oms
with
surg
ical
rem
oval
ofm
ass;
ESR
retu
rned
tono
rmal
9(7
)72
FPD
34
7L
eged
ema,
wei
ght
gain
NA
Abd
and
pelv
icC
T:
norm
alE
cho:
seve
reth
icke
ning
and
retr
actio
nof
tric
uspi
dva
lve;
mod
erat
eca
rdia
cdi
latio
n
Exc
ised
tric
uspi
dva
lve:
diff
use
fibro
sis
NA
10(7
)74
FPD
1.5
124
Exe
rtio
nal
dysp
nea,
orth
opne
a,le
ged
ema
NA
CT
ches
t/abd
/pel
vis:
norm
alE
cho:
thic
keni
ngof
tric
uspi
dm
itral
and
aort
icva
lves
,se
vere
regu
rgita
tion
Exc
ised
valv
es:
endo
card
ial
fibro
sis
NA
11(7
)61
FPD
3.75
736
Hea
rtm
urm
urN
AA
bdul
tras
ound
:no
rmal
Ech
o:ao
rtic
,m
itral
and
tric
uspi
dva
lve
thic
keni
ngan
dre
gurg
itatio
n
NA
No
chan
geat
3-m
o.fo
llow
-up
12(8
)83
FPD
32
1L
eged
ema
NA
CT
abd:
mas
sen
velo
ping
both
uret
ers
Abd
ultr
asou
nd:
bila
tera
lhy
dron
ephr
osis
Bio
psy:
retr
oper
itone
alfib
rosi
sU
rete
ral
sten
ting
13(1
1 )52
FPD
4.5
418
Cou
ghN
AC
SR:
Nor
mal
CT
ches
t:D
iffu
segr
ound
glas
ssh
adow
ing
Bro
ncho
scop
yan
dtr
ansb
ronc
hial
biop
sy:
norm
alIm
prov
emen
t3
mo.
afte
rst
oppi
ngpe
rgol
ide;
pred
niso
ne1
mg/
kgan
dcy
clop
hosp
ham
ide
100
mg/
day
700 P. AGARWAL ET AL.
Movement Disorders, Vol. 19, No. 6, 2004
TA
BL
E1.
(Con
tinu
ed)
Patie
ntno
.(R
ef.)
Age
(yr)
Gen
der
Dx
mg/
day
Rx
(yr)
tto
Dx
(mo.
)Sy
mpt
oms
ESR
Imag
ing
Path
olog
yC
ours
e
14(1
1 )64
MPD
1.5
40.
25L
etha
rgy,
coug
h89
CX
R:
card
iom
egal
y,bi
late
ral
inte
rstit
ial
shad
own
and
pleu
ral
effu
sion
sE
cho:
peri
card
ial
effu
sion
CT
ches
t:pa
tchy
grou
ndgl
ass
opac
ifica
tion
Pleu
ral
aspi
rate
:m
ixed
infla
mm
ator
yce
lls,
lym
phoc
ytos
isIm
prov
emen
t2
wk
afte
rst
oppi
ngpe
rgol
ide
15(1
2 )61
MPD
81.
512
Hea
rtfa
ilure
NA
Ech
o:m
itral
,tr
icus
pid,
aort
icre
gurg
itatio
nN
ASu
dden
deat
h
16(1
2 )73
FPD
73
NA
New
holo
syst
olic
mur
mur
NA
Ech
o:se
vere
mitr
alan
dao
rtic
regu
rgita
tion
Val
ve:
foca
len
doca
rdia
lth
icke
ning
Val
vere
plac
emen
t
17(1
3 )64
MPD
NA
13
Dys
pnea
,co
ugh
NA
CX
R:
pleu
ral
effu
sion
NA
Res
olut
ion
ofsy
mpt
oms
2m
oaf
ter
stop
ping
perg
olid
e18
(13 )
63M
PD5
5N
AD
yspn
ea,
coug
h,at
ypic
alch
est
pain
NA
NA
Pleu
ral
biop
sy:
fibro
usgr
anul
omat
ous
infla
mm
atio
nR
esol
utio
nof
sym
ptom
s
19(1
3 )65
MPD
1.5
37
Dys
pnea
NA
CX
Ran
dC
Tch
est:
bila
tera
lpl
eura
lth
icke
ning
Pleu
ral
biop
sy:
reac
tive
fibro
uspl
euri
tisN
oim
prov
emen
tsi
nce
stop
ping
perg
olid
e20
(13 )
63M
PD4.
53.
51
Dys
pnea
,co
ugh
96C
Tch
est:
fibro
sis,
pleu
ral
thic
keni
ngan
def
fusi
onPl
eura
lbi
opsy
:no
nspe
cific
fibro
usin
flam
mat
ion
Impr
ovem
ent
afte
rst
oppi
ngpe
rgol
ide
21(1
4 )73
MPD
1.75
31
Dys
pnea
,le
ged
ema
C-r
eact
ive
prot
ein
35m
g/dl
6E
cho:
mild
righ
tve
ntri
cle
hypo
kine
sia
CT
ches
t:sm
all
bila
tera
lpl
eura
lef
fusi
ons
NA
Impr
ovem
ent
1m
oaf
ter
stop
ping
perg
olid
e
22(C
ase
1)C
urre
ntpa
per
65M
PD7.
58
24C
ough
,dy
spne
a,ed
ema
100
MR
Ich
est:
left
lung
mas
sC
Tab
d:re
trop
erito
neal
fibro
sis
Ret
rogr
ade
pyel
ogra
m:
narr
owin
gof
both
uret
ers
NA
Dra
mat
icim
prov
emen
ton
pred
niso
ne60
mg/
day
23(C
ase
2)C
urre
ntpa
per
73M
RL
S5
21
Dys
pnea
NA
CX
R:
left
pleu
ral
effu
sion
,m
ass
Bro
ncho
scop
y:ho
mog
eneo
usth
icke
ning
ofpl
eura
NA
Gra
dual
relie
fof
dysp
nea
afte
rst
oppi
ngpe
rgol
ide
24(1
5 )56
FPD
4.5
30.
1E
dem
aN
AE
cho:
seve
retr
icus
pid
regu
rgita
tion,
mod
erat
eao
rtic
and
mitr
alre
gurg
itatio
n
NA
No
prog
ress
ion
sinc
est
oppi
ngpe
rgol
ide
25(1
5 )74
MPD
44
0.1
Ede
ma,
sync
ope
NA
Ech
o:se
vere
tric
uspi
dan
dm
ildm
itral
regu
rgita
tion
Val
ve:
noni
nflam
mat
ory
fibro
ticde
gene
ratio
nN
opr
ogre
ssio
nsi
nce
stop
ping
perg
olid
e26
(15 )
67F
PD4.
51.
31.
6D
yspn
ea,
edem
aN
AE
cho:
seve
retr
icus
pid,
mod
erat
em
itral
and
aort
icre
gurg
itatio
n
NA
Dra
mat
icim
prov
emen
taf
ter
stop
ping
perg
olid
e
Rpn
,rop
inir
ole;
Ppx,
pram
ipex
ole;
CX
R,c
hest
radi
ogra
ph;
ESR
,ery
thro
cyte
sedi
men
tatio
nra
te;
PFT
,pul
mon
ary
func
tion
test
;E
cho,
echo
card
iogr
am;
Dx,
diag
nosi
s;R
x,tim
etr
eate
d;C
T,
com
pute
dto
mog
raph
y;PD
,Pa
rkin
son’
sdi
seas
e;R
LS,
rest
less
legs
synd
rom
e;N
A,
not
avai
labl
e.
PERGOLIDE-INDUCED FIBROSIS 701
Movement Disorders, Vol. 19, No. 6, 2004

He was initially treated with tamoxifen 40 mg/day for4 weeks with no benefit. Subsequently, he was treatedwith prednisone 60 mg/day for 6 weeks with dramaticradiographic improvement of abdominal fibrosis. He wasthen treated with pramipexole without recurrence of fi-brosis and has since undergone implantation of bilateralsubthalamic nucleus stimulators.
Case 2
A 71-year-old man presented with symptoms of severeidiopathic RLS. Initial treatment with L-dopa producedno symptomatic benefit. Treatment with pergolide dra-matically improved his symptoms, although he requiredgradually increasing doses over a period of 1 year (up to5 mg/day). Two years after pergolide was introduced, hedeveloped shortness of breath. A chest radiograph re-vealed a left pleural effusion and a wedge-shaped massin the left upper lobe. Analysis of pleural fluid showed noevidence of malignancy. A fluorodeoxyglucose positronemission tomographic scan of the chest revealed lowactivity in the left chest wall, consistent with a reactiveprocess. Thorascopic examination showed homogenouswhite thickening of the pleura, and biopsy of the lungmass revealed evidence of chronic inflammation andinterstitial fibrosis with no evidence of malignancy.
Pergolide was stopped, and his dyspnea graduallyresolved. OxyContin was ineffective at relieving hissymptoms of disabling restlessness. He is currentlytreated with pramipexole, with excellent benefit and nosymptomatic or radiologic recurrence of fibrosis.
PUBLISHED LITERATURE
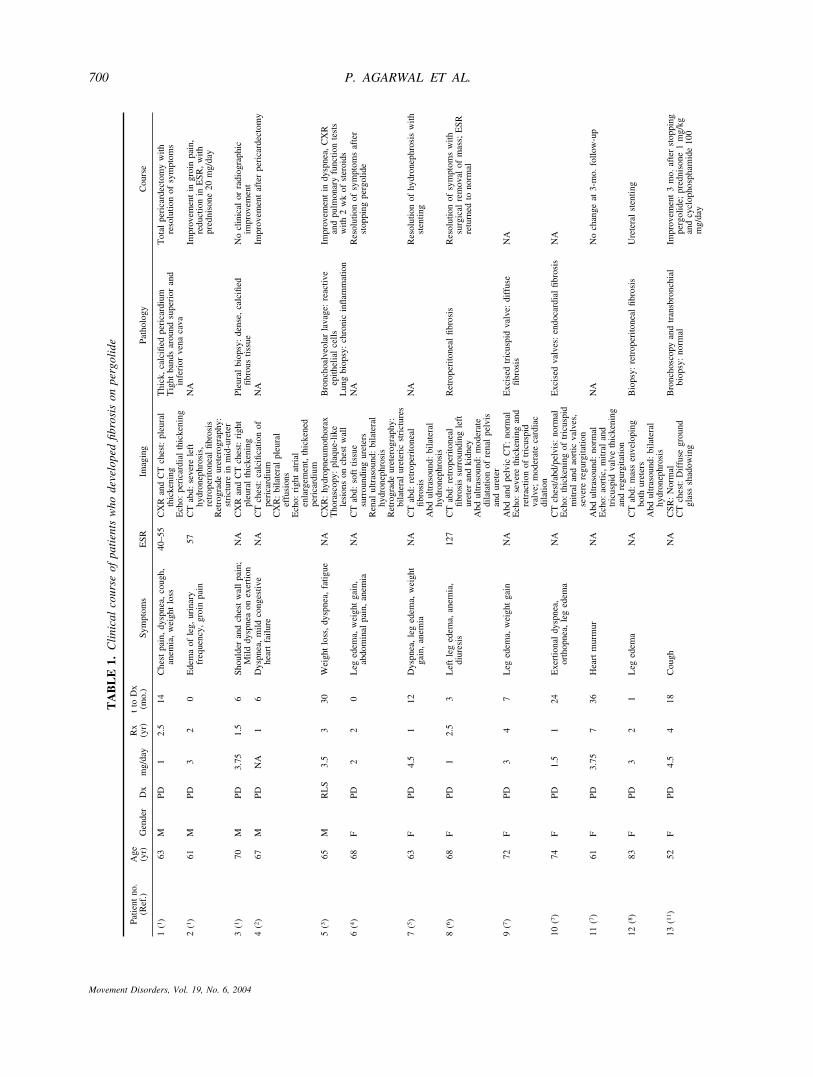
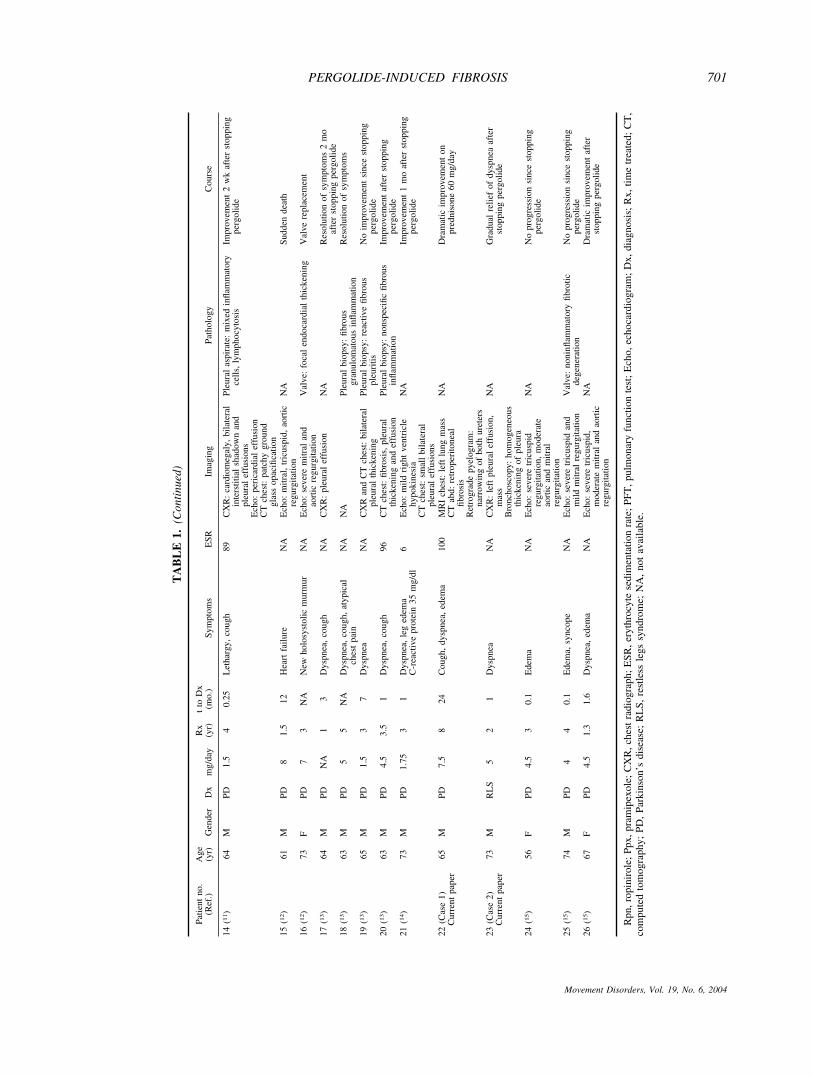
Clinical information on patients (including the 2 re-ported in this study) who developed serosal fibrosis dur-ing treatment with pergolide is summarized in Table 1.Patients ranged in age from 42 to 83 years, with a malepreponderance (63%). A total of 24 patients receivedpergolide as treatment for PD and 2 for RLS. The totaldaily dosage of pergolide ranged from 1 mg/day to 7.5mg/day. Patients received the drug for 11 months to 8years before symptoms began. In at least 6 patients, theESR rate was elevated, from 40 to 127 mm/hour; in theother patients the ESR was either not measured or notreported. In 1 patient (Patient 21), the ESR was normalbut C-reactive protein was elevated.
In those patients who developed pulmonary fibrosis,chest radiographs were abnormal with the exception ofPatient 13. Abdominal CT scan was abnormal in patientswho developed retroperitoneal fibrosis. Twenty-one pa-tients required an invasive procedure to secure the diag-nosis. Pergolide was discontinued in all cases, and 4patients were treated with steroids, experiencing dra-
matic benefit within several weeks of treatment. Peri-cardectomy, valve replacement and ureteral stentingwere necessary in some cases. Three patients (Patients 3,11 and 19) did not improve, despite discontinuation ofthe drug. One patient (Patient 15) died suddenly whileawaiting surgery. Further details regarding clinical fea-tures and management are summarized in Table 1.
DISCUSSION
Like its cousins bromocriptine, lisuride, and cabergoline,and related ergots methysergide, lysergic acid, and diethyl-amide ergotamine, pergolide is known to rarely triggerserosal fibrosis affecting pleural or retroperitoneal struc-tures.1–15 Recent reports of patients with fibrotic valvularheart disease7,12,15 and additional possible cases of cardiacand pulmonary fibrosis attributed to the drug10 have gener-ated concern in the minds of patients and physicians. Wechose to present our experience with 2 such patients, andreview the published literature to attempt to answer severalquestions: How do patients present with fibrotic complica-tions from pergolide?; Is fibrosis related to the dose orduration of treatment?; What happens to these patients oncethe drug is stopped?; and finally, What other treatmentoptions are available?
The most common presenting symptom was dyspnea(54%). Leg edema could also occur either in one leg orboth, and cough and chest pain were not infrequent. Mostpatients gained weight (probably due to fluid accumula-tion), although 3 patients lost weight. Time from firstsymptom to diagnosis ranged from 1 to 36 months. Thetotal daily dosage of pergolide in published cases rangedfrom 1 mg/day to 8 mg/day, and duration of exposureranged from 11 months to 8 years. Thus, it would appearthat fibrosis can occur in patients treated with a low doseof pergolide for a short time, and that there may not be acompletely risk-free dose or duration of exposure.Rather, fibrosis may be an idiosyncratic event, occurringin patients who are somehow predisposed to develop it.It has also been suggested that increased serotonin levelsmay activate fibroblasts, leading to scarring.16 In patientswith pleural interstitial lung injury, an idiosyncratic im-mune reaction has also been postulated.1
In at least 6 patients, the inflammatory marker ESRwas elevated, ranging from 40 to 127 mm; the ESR wasnot reported in other cases except one in which it wasnormal. Anemia was reported in 4 patients. In thosepatients who developed pulmonary fibrosis, abnormali-ties were clearly visible on plain chest radiographs ex-cept for 1 patient (Patient 13). Abdominal CT and trans-thoracic echocardiography were very useful in definingthe extent of pathology in patients with fibrosis affectingthe retroperitoneum or cardiac valves. The time from
702 P. AGARWAL ET AL.
Movement Disorders, Vol. 19, No. 6, 2004

symptom onset to definitive diagnosis varied from 1 to36 months, suggesting that lack of awareness of thediagnosis may have contributed to the delay.
In all cases, pergolide was discontinued as soon as thediagnosis was secured. Invasive surgical procedures (peri-cardectomy, valve replacement, abdominal resection) werefrequently necessary, and most patients underwent an ex-tensive work-up to exclude malignancy. We used tamox-ifen in our first patient because of reports suggesting that itinhibits human mast cell proliferation, possibly through ionchannel modulation. It has been hypothesized that tamox-ifen might be useful in the treatment of mast cell-mediateddiseases, including mastocytosis, asthma, and pulmonaryfibrosis.17 Unfortunately, it was not effective in our patient.Prednisone acts as an anti-inflammatory agent and reducesphagocytic activity, collagen deposition, fibroblast activity,and ultimately scar formation. Response to treatment withprednisone was dramatic in 3 patients, suggesting the pos-sibility that early diagnosis and initiation of steroid treat-ment might alter the course of the illness. In most patients,the fibrotic process remits when the drug is stopped; how-ever, in some patients it does not. In our first case, despitediscontinuation of the drug, retroperitoneal fibrosis devel-oped 1 year later, which was, fortunately, extremely respon-sive to steroids. Five patients were subsequently exposed tononergot agonists without recurrence of fibrosis at lastfollow-up.
Given these facts, how should neurologists managethis rare but potentially serious complication? We rec-ommend the following strategies. All patients should becounseled about the rare possibility of fibrosis beforestarting pergolide, and all patients already taking thedrug should be informed of the possibility of this seriousadverse event. We recommend documenting this conver-sation in the medical record. It would seem prudent toavoid pergolide in any patient with a known elevatedESR, abnormal renal function, congestive heart failure,or valvular heart disease. Although the data are verylimited, it would appear that patients who develop fibro-sis from pergolide can be safely treated with nonergotdopamine agonists.
The nonergot dopamine agonists pramipexole andropinirole may be better choices than pergolide for initialfirst-line therapy in patients with PD or RLS. Given ourconcerns about pergolide-induced fibrotic complications,at our center, we no longer routinely use pergolide asfirst-line treatment in PD or RLS, instead reserving it forsituations where nonergot dopamine agonists have failedor are not tolerated. We are uncertain whether or not therare risk of pergolide-induced fibrosis is sufficient towarrant removing this valuable drug from the PD arma-
mentarium; however, this is a possibility given the avail-ability of other dopamine agonists and L-dopa.
We believe that, because the incidence of pergolide-induced fibrosis is not high, it is impractical to screenevery patient taking pergolide for fibrotic complications.However, patients who develop new dyspnea, chest pain,weight gain, or symptoms of urinary outflow obstructionshould be imaged. An elevated ESR may be an earlyindicator, although this marker is very nonspecific. Echo-cardiography and CT scan of the chest, abdomen, andpelvis are more valuable tests. Given the dramatic benefitfrom treatment with prednisone, it seems reasonable toattempt a trial of steroids in all patients who developfibrosis, especially before embarking on invasive surgi-cal procedures.
A more difficult question facing neurologists is howto manage patients who develop swelling of one orboth legs while taking pergolide. Like all dopamineagonists, pergolide can induce leg swelling, and thevast majority of these patients do not have retroperi-toneal fibrosis. Our approach in patients with signifi-cant leg swelling is to switch to another agonist or toconsider using L-dopa instead. Patients are followedweekly by telephone call or office visit, and if addi-tional symptoms such as dysuria and dyspnea developor leg swelling does not decrease, we initiate awork-up for serosal fibrosis, including CT of the chest,abdomen, and pelvis.
REFERENCES
1. Shaunak S, Wilkins A, Pilling JB, et al. Pericardial, pleural andretroperitoneal fibrosis induced by pergolide. J Neurol NeurosurgPsychiatry 1999;66:79–81.
2. Balachandran KP, Stewart D, Berg GA, Oldroyd KG. Chronicpericardial constriction linked to the antiparkinsonian dopamineagonist pergolide. Postgrad Med J 2002;78:49–50.
3. Danoff SK, Grasso ME, Terry PB, Flynn JA. Pleuropulmonarydisease due to pergolide use for restless legs syndrome. Chest2001;120:313–316.
4. Kunkler RB, Osborn DE, Abbott RJ. Retroperitoneal fibrosiscaused by treatment with pergolide in a patient with Parkinson’sdisease. Br J Urol 1998;82:147.
5. Mondal BK, Suri S. Pergolide induced retroperitoneal fibrosis. IntJ Clin Pract 2000;54:403.
6. Jimenez-Jimenez FJ, Lopez-Alvarez J, Sanchez-Chapado M, et al.Retroperitoneal fibrosis in a patient with Parkinson’s diseasetreated with pergolide. Clin Neuropharmacol 1995;18:277–279.
7. Pritchett AM, Morrsion JF, William ED, Schaff HV, ConnollyHM, Espinosa RE. Valvular heart disease in patients taking Per-golide. Mayo Clinic Proc 2002;77:1280–1286.
8. Lund BC, Neiman RF, Perry PJ. Treatment of Parkinson’s diseasewith ropinirole after pergolide-induced retroperitoneal fibrosis.Pharmacotherapy 1999;19:1437–1438.
9. Bhatt MH, Keenan SP, Fleetham JA, Calne DB. Pleuropulmonarydisease associated with dopamine agonist therapy. Ann Neurol1991;30:613–616.
PERGOLIDE-INDUCED FIBROSIS 703
Movement Disorders, Vol. 19, No. 6, 2004

10. Flowers CM, Racoosin JA, Lu SL, Beitz JL. The US food and drugadministration’s registry of patients with pergolide-associated val-vular heart disease. Mayo Clin Proc 2003;78:730–731.
11. Kastelik JA, Aziz I, Greenstone MA, Thomopson R, Morice AH.Pergolide-induced lung disease in patients with Parkinson’s dis-ease. Respir Med 2002;96:548–550.
12. Camp GV, Flamez A, Cosyns B, Goldstein J, Perdaens C, Schoors D.Heart valvular disease in patients with Parkinson’s disease treatedwith high-dose pergolide. Neurology 2003;61:859–861.
13. Bleumink GS, van der Molen-Eijgenraam M, Strijbos JH, SanwikarjaS, van Puijenbroek EP, Stricker BHC. Pergolide-induced pleuropul-monary fibrosis. Clin Neuropharmacol 2002;25:290–293.
14. Varsano S, Gershman M, Hamaoui E. Pergolide-induced dyspnea,bilateral pleural effusion and peripheral edema. Respiration 2000;67:580–582.
15. Horvath J, Fross RD, Kleiner-Fisman G, et al. Severe multivalvularheart disease: a new complication of the ergot derivative dopamineagonists. Mov Disord (in press).
16. Morelock SY, Sahn SA. Drugs and the pleura. Chest 1999;116:212–221.
17. Duffy SM, Lawley WJ, Kaur D, Yang W, Bradding P. Inhibitionof human mast cell proliferation and survival by tamoxifen inassociation with ion channel modulation. J Allergy Clin Immunol2003;112:965–972.
704 P. AGARWAL ET AL.
Movement Disorders, Vol. 19, No. 6, 2004