diagnosis and management of adrenal...
TRANSCRIPT

R
U
D
RC
C
R
2
Document downloa
adiología. 2011;53(6):516---530
www.elsevier.es/rx
PDATE IN RADIOLOGY
iagnosis and management of adrenal incidentaloma�
. Oliveira Caiafa ∗, R. Salvador Izquierdo, L. Bunesch Villalba, M.C. Sebastià Cerqueda,
. Nicolau Molina
entro de Diagnóstico por la Imagen, Hospital Clínic, Barcelona, Spain
eceived 27 October 2010; accepted 15 June 2011
KEYWORDSAdrenalincidentaloma;Computedtomography;Magnetic resonanceimaging;Positron emissiontomography/computedtomography;Algorithm
Abstract The growing demand for imaging tests and the progressive aging of the populationhave led to a progressive increase in the detection of indeterminate adrenal lesions. Oncean adrenal incidentaloma is detected, clinical and hormone tests together with a battery ofimaging techniques (CT, MRI, PET/CT. . .) make it possible to determine the cause in most cases.In this article, we discuss the advantages and limitations of each technique. We show the imagingcharacteristics of the most common adrenal lesions and propose a diagnostic algorithm to enabletheir diagnosis.© 2010 SERAM. Published by Elsevier España, S.L. All rights reserved.
PALABRAS CLAVEIncidentalomasuprarrenal;Tomografíacomputarizada;Resonancia
Manejo y diagnóstico del incidentaloma suprarrenal
Resumen La creciente demanda de pruebas radiológicas y el envejecimiento progresivo de lapoblación ha llevado al aumento progresivo en la detección de lesiones suprarrenales indeter-minadas. Una vez detectado el incidentaloma suprarrenal, disponemos actualmente de pruebasclínicas y hormonales y de una batería de técnicas de imagen (TC, RM, PET/TC. . .) que hacen
ded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
magnética;Tomografíapor emisión depositrones/tomografía
posible el diagnóstico etiológico de la mayoría de estos incidentalomas. En este artículo pre-sentamos las ventajas y limitaciones de cada técnica, las características por imagen de laslesiones suprarrenales más frecuentes y proponemos un algoritmo diagnóstico que permita eldiagnóstico de las mismas.© 2010 SERAM. Publicado por Elsevier España, S.L. Todos los derechos reservados.
computarizada;Algoritmo
� Please cite this article as: Oliveira Caiafa R, et al. Manejo y diagnóst∗ Corresponding author.
E-mail address: [email protected] (R. Oliveira Caiafa).
173-5107/$ – see front matter © 2010 SERAM. Published by Elsevier Esp
ico del incidentaloma suprarrenal. Radiología. 2011;53:516---30.
aña, S.L. All rights reserved.

si
I
C
Agmattwp
n(e1ai2t
utml
aitms
e
a(
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Diagnosis and management of adrenal incidentaloma
Introduction
Adrenal incidentalomas are clinically silent adrenal massesthat are discovered during the study, treatment or follow-up of unrelated clinical conditions. This definition excludespatients imaged for cancer staging or follow-up.1,2
In autopsy studies, the mean prevalence of adrenalincidentalomas is approximately 2.3%, with no significantdifferences between men and women, and higher rates inolder patients.3 In the current setting of increasing demandand use of high-resolution diagnostic imaging techniques,there has been a significant increase in the detection ofthese lesions. Adrenal lesions are found in 4---5% of com-puted tomography (CT) studies performed for unrelatedreasons.3---7
Seventy per cent of all adrenal incidentalomas arenon-functioning adenomas; 5---16% are functioning adeno-mas; 6% are pheochromocytomas; 5% are adrenocorticalcarcinomas; 2% are metastatic carcinomas, and the rest,other types of lesions (myelolipomas, hematomas, cysts orlymphoma).3,8,9
When an adrenal incidentaloma is discovered during animaging examination, the major issues are whether thelesion is hormonally functional and whether the lesion islikely to be benign or malignant. The results from thesetests will determine whether lesion resection or conserva-tive management is indicated.
Although the majority of adrenal incidentalomas are non-functioning, a fair number of these patients present with asubclinical form of hormonal dysfunction and may representa population at higher risk of metabolic disorders and car-diovascular disease. For this reason, when an incidentalomais found, a complete medical history and physical examina-tion, a hormonal evaluation and, in some cases, additionalradiologic studies are required. Screening for pheochromo-cytoma, primary hypercortisolism and hyperaldosteronismis routinely recommended for hypertensive patients, unlessthere are unequivocal features of myelolipoma, hemorrhageor adrenal cyst.1,10,11
Radiologists have at their disposal a variety of imag-ing techniques for characterizing adrenal incidentalomas,from CT and magnetic resonance (MR), which allow for thediagnosis of most adrenal lesions, to more sophisticatedtechniques such as positron emission tomography/computedtomography (PET/CT) and MR-spectroscopy, the latter stillat an experimental stage. However, a small proportion ofadrenal lesions remain undetermined and often represent amajor diagnostic and therapeutic challenge given that thereis no consensus in the literature as to when fine needle aspi-ration (FNA), surgery or follow-up (clinical, biochemical, andradiologic) is indicated.
This article examines the advantages and limitationsof the different imaging techniques used in the characteriza-tion of incidentalomas and proposes a diagnostic algorithmthat includes clinical, biochemical and, especially, imag-ing parameters.Although the definition of incidentalomaexcludes patients undergoing imaging procedures as a partof staging or follow-up for cancer,1,2 we have included infor-
mation on the diagnosis and management of adrenal lesionsin oncologic patients, given that 50% of adrenal lesions inthese patients are metastatic.12 Additionally, the character-ization of these lesions is important for noninvasive tumorstr
517
taging and for formulating a therapeutic plan and predict-ng the prognosis.8
maging techniques
omputed tomography
t CT, parameters such as a size larger than 6 cm, rapidrowth, irregular or nodular margins and heterogeneityay be suggestive of a malignant adrenal incidentaloma,
lthough these features are not very specific.13,14 However,he unenhanced CT attenuation measurements, the his-ogram analysis and the values of contrast-enhancementashout allow for adrenal lesion characterization in a highercentage of cases.6,15,16
The appropriate technique for the evaluation of adrenalodules involves a study without intravenous (IV) contrastbaseline) in all patients, followed if necessary by a contrast-nhanced CT (portal phase at 60 s and delayed phase at5 min). A thin slice thickness (2---3 mm) is required, as wells attenuation measurements obtained through regions ofnterest covering a significant portion of the lesion (1/2 to/3 of the lesion area), but avoiding the peripheral edges ofhe mass to prevent partial volume artifacts.14,17
The quantification of the mean attenuation values onnenhanced (baseline) CT is a simple and highly sensitiveask to detect fat within the tumor, which makes it theost useful parameter in the initial assessment of adrenal
esions.18,19
Other tool that may be useful in the characterization ofdrenal lesions is the histogram analysis, that is, a graph-cal representation that displays the individual analysis ofhe attenuation values for each pixel in a given area. Thisethod is highly sensitive for the detection of fat, repre-
ented as pixels with negative attenuation values.8,17,20,21
The most commonly used parameters in contrast-nhanced CT are:
Absolute washout: quantifies the delayed washout com-pared to portal-phase enhancement.
Absolute washout = Portal AC − Delayed ACPortal AC − Baseline AC
× 100
where AC is the attenuation coefficient (HU).Relative washout: is an estimated calculation of the abso-lute washout when an adrenal lesion is discovered onenhanced CT (portal and delayed phase) and no previousbaseline study is available.
Relative washout = Portal AC − Delayed ACPortal AC
× 100
Washout values are of little use in the characterization ofdrenal masses with heterogeneous areas of low attenuationnecrosis or cystic areas).
The recent emergence of dual energy CT allows us toubtract, using a postprocessing algorithm, the iodine con-rast agent from the abdominal images obtained after cont-ast administration and generate a virtual unenhanced study

518
Figure 1 Adrenal adenoma. Abdominal CT scan in a72-year-old patient investigated for infrarenal abdominal aor-tl-
to
M
Co
ogomsoml
qio
A
P
wo
famp
Fuaa
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
ic aneurysm. Unenhanced CT scan shows a hypodense nodularesion in the left adrenal gland, with attenuation values of-- 13 HU, compatible with an adenoma.
hat can be used to estimate the baseline attenuation valuesf an adrenal lesion.22
agnetic resonance
hemical shift imaging is the mainstay of MR evaluationf solid adrenal lesions and is based on the detection
tai
Fusion V
igure 2 Adrenal adenoma. Abdominal dual energy CT scan in a
nenhanced study was performed. The portal-phase enhanced CT scdrenal gland of 39 HU. With the dual energy technique, a virtual uttenuation of the lesion was 3 HU, compatible with an adenoma.
R. Oliveira Caiafa et al.
f cytoplasmic lipid using in-phase and opposed-phaseradient-echo T1-weighted Images.23---26 This method reliesn the differences in resonance frequency of lipid and waterolecules. On opposed-phase images, the phase of the lipid
ignal is opposite to that of the water, resulting in a dropf signal in those voxels containing both elements, whichicroscopically correlates with the presence of intracellular
ipid.27
The chemical shift phenomenon can be assessed eitherualitatively, by visual comparison of the adrenal lesionntensity with that of the spleen, or quantitatively, throughne of the following formulas28,29:
drenal/spleen ratio
= Adrenal SI OP/Spleen SI OPAdrenal SI IP/Spleen SI IP
× 100
ercentage of SI loss
= Adrenal SI IP − Adrenal SI OPAdrenal SI IP
× 100
here SI is the signal intensity; IP the in-phase; and OP thepposed-phase.
Additionally, the protocols may include T1-, T2- andat-suppressed T1-weighted sequences obtained beforend after contrast administration, providing data on theorphology and behavior of the adrenal lesions com-arable to those provided by CT.
Gadolinium-enhanced dynamic MR imaging involveshe IV administration of gadolinium contrast media and thecquisition of consecutive fast sequences at variable timentervals, depending on the protocol of each institution, in
irtual baseline
63-year-old patient with a history of colorectal carcinoma; noan (fusion 140 kVp + 100 kVp) shows a nodular lesion in the leftnenhanced study could be obtained and this showed that the

Diagnosis and management of adrenal incidentaloma 519
Baseline Portal‐phase Delayed phase
23 HU 88 HU 43 HU
dentathe a
fpm
aotaSa
iiap
rp
F
Itg
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Figure 3 Adrenal adenoma. A 72-year-old patient with an incian attenuation of 23 HU on the unenhanced CT study; however,
order to obtain a curve representing the absolute or relativevariation in signal within a specific time frame.30,31
MR-spectroscopy has proved potentially useful in the dif-ferential diagnosis of adrenal lesions based on metaboliteratios, and has proved particularly useful in the character-ization of pheochromocytomas32 and in the differentiationof adenomas and pheochromocytomas from carcinomas andmetastases.33,34
Thus far, diffusion MR imaging has not proved useful todifferentiate benign from malignant lesions.31
Ultrasonography
Ultrasonography does not allow for the characterization ofmost adrenal incidentalomas. It has been recently reportedthat the use of contrast-enhanced ultrasonography mayimprove the diagnostic accuracy since malignant lesionsare usually hypervascular. This would translate into earlycontrast enhancement in the arterial phase and rapidwashout.35
Nonetheless, its systematic use is limited by the difficultvisualization of the adrenal glands with this technique.
Positron emission tomography/computed
tomography18F-fluorodeoxyglucose PET/CT (18F-FDG PET/CT) protocolsvary among institutions. This technique is highly sensitive
dmaa
lly discovered adrenal nodule in the left adrenal gland that hasbsolute washout is 69%, which is compatible with an adenoma.
or differentiating benign from malignant lesions,28,36 beingarticularly useful in the identification of metastatic adrenalasses in the workup of oncologic patients.37
The metabolic activity can be evaluated by qualitativenalysis, that is, visual comparison between the uptakef the adrenal lesion and that of the liver, or by quan-itative analysis based on the determination of the meannd maximum SUVs (Standardized Uptake Values) andURs (Standardized Uptake Ratios), obtained through thedrenal/liver ratio.
The usefulness of 11C-metomidate (MET) PET/CT imagingn the detection of non-necrotic primary adrenal tumors38
s being validated, as well as that of 11C-hydroxyephedrinend of 18F-dihydroxyphenylalanine in the detection ofheochromocytomas.8
MIBG (a radiotracer taken up by chromaffin cells) scintig-aphy allows pheochromocytoma detection in a significantercentage of cases.28,36
ine needle aspiration
n the algorithms for the management of adrenal inciden-alomas, FNA is indicated for the characterization of activelyrowing lesions, in cases of equivocal radiologic findings
epending on the clinical setting and of high suspicion ofetastasis27 (in patients with a known primary cancer),nd only if the definitive diagnosis changes the treatmentpproach.
520
R. O
liveira Caiafa
et al.
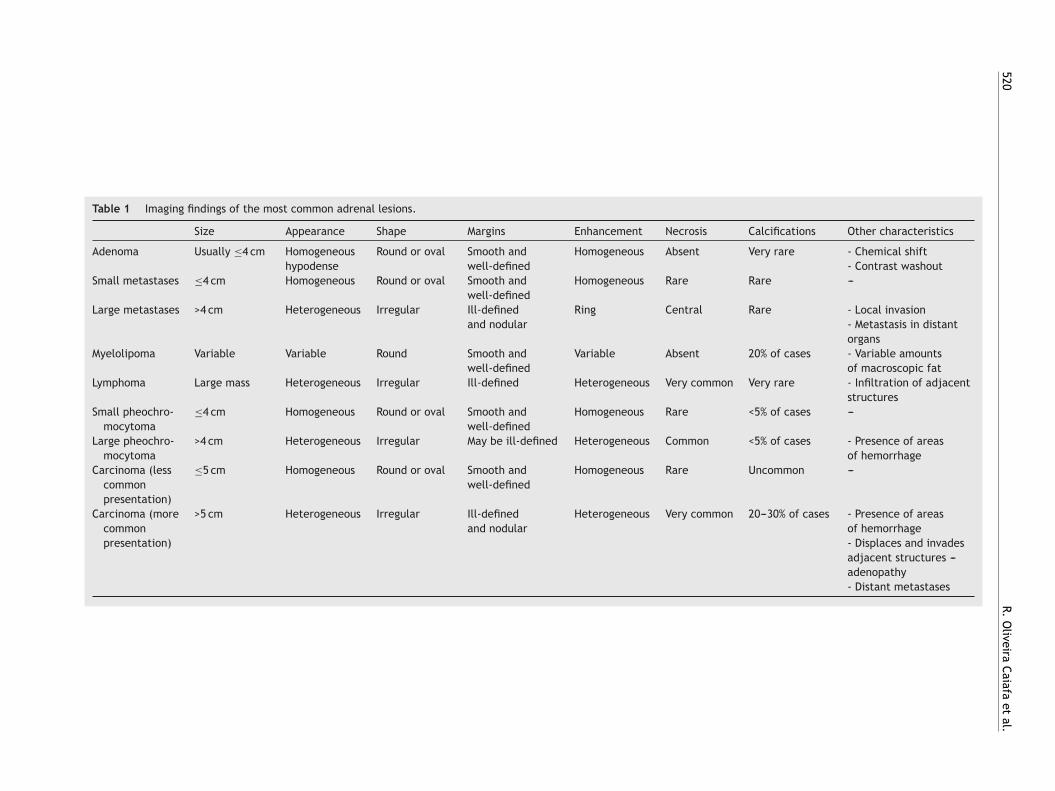
Table 1 Imaging findings of the most common adrenal lesions.
Size Appearance Shape Margins Enhancement Necrosis Calcifications Other characteristics
Adenoma Usually ≤4 cm Homogeneoushypodense
Round or oval Smooth andwell-defined
Homogeneous Absent Very rare - Chemical shift- Contrast washout
Small metastases ≤4 cm Homogeneous Round or oval Smooth andwell-defined
Homogeneous Rare Rare ---
Large metastases >4 cm Heterogeneous Irregular Ill-definedand nodular
Ring Central Rare - Local invasion- Metastasis in distantorgans
Myelolipoma Variable Variable Round Smooth andwell-defined
Variable Absent 20% of cases - Variable amountsof macroscopic fat
Lymphoma Large mass Heterogeneous Irregular Ill-defined Heterogeneous Very common Very rare - Infiltration of adjacentstructures
Small pheochro-mocytoma
≤4 cm Homogeneous Round or oval Smooth andwell-defined
Homogeneous Rare <5% of cases ---
Large pheochro-mocytoma
>4 cm Heterogeneous Irregular May be ill-defined Heterogeneous Common <5% of cases - Presence of areasof hemorrhage
Carcinoma (lesscommonpresentation)
≤5 cm Homogeneous Round or oval Smooth andwell-defined
Homogeneous Rare Uncommon ---
Carcinoma (morecommonpresentation)
>5 cm Heterogeneous Irregular Ill-definedand nodular
Heterogeneous Very common 20---30% of cases - Presence of areasof hemorrhage- Displaces and invadesadjacent structures ---adenopathy- Distant metastases
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

Diagnosis and management of adrenal incidentaloma 521
Portal-phase
15 HU 0 HU
Delayed phase
Area: 0.44 cm2
Mean: 15.54Standard deviation: 14.79
Area: 0.47 cm2
Mean: 1.04Standard deviation: 15.15
Figure 4 Adrenal adenoma. A 56-year-old patient investigated for a left renal mass. Intravenous contrast-enhanced abdominalCT scans, portal phase at 60 s and delayed phase at 15 min, show a nodular lesion in the left adrenal gland. No unenhanced scanis available and, therefore, the absolute washout cannot be estimated. Nonetheless, the relative washout of 96% is suggestive of
ctihnoans2roww
iao
3o
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
adenoma.
FNA is particularly useful in the differentiation betweenadrenal and non-adrenal tissue (metastasis or infection).Nonetheless, FNA cytology has low or no diagnostic yield inthe differentiation of adenomas from adrenal carcinomas.FNA can be performed under CT, MR or ultrasound guidanceand its diagnostic accuracy varies from 83% to 93%, witha complication rate of approximately 3% (most commonlypain, hemorrhage and pneumothorax).39,40 Hormonal evalu-ation must be done before FNA is undertaken in order to ruleout the possibility of pheochromocytoma, as the puncturemay precipitate a hypertensive crisis.
Most common adrenal incidentalomas
Adenomas
One of the key points in the diagnosis of adenomas isthe presence of a variable proportion of intracellular lipid,whose detection allows a highly accurate diagnosis. A max-imum threshold of 10 HU at unenhanced CT for adenoma
characterization (Figs. 1 and 2) yields a sensitivity of 71%and a specificity of 98%. These parameters are close to100% when size, growth and shape are also taken intoaccount.16,18,19cAofi
Most adenomas, even lipid-poor adenomas, supposedlyontain enough amounts of cytoplasmic lipid to allow forheir characterization.20 Histogram analysis may be usefuln the characterization of lipid-poor adenomas. At unen-anced CT, the histogram analysis with a cutoff of 10%egative pixels yields a specificity of 100% and a sensitivityf 46---91%.17,20,21,41 When using an unenhanced CT attenu-tion threshold of 10---20 HU, the finding of more than 10%egative pixels yields a sensitivity of 92% for the diagno-is of adenoma. For unenhanced CT attenuation values of0---30 HU and >30 HU, the sensitivity drops to 10% and 0%,espectively.21 The combination of values ≤10 HU or >10%f negative pixels yields a sensitivity of up to 91% comparedith 68% sensitivity when attenuation values are used alone,hile the specificity remains at 100%.20
Therefore, the histogram analysis of unenhanced CTmproves the overall sensitivity for the characterization ofdenomas, particularly in lesions with attenuation valuesf 10---20 HU on unenhanced CT.
Approximately 70% of adenomas are lipid-rich42---44 and0% are lipid-poor. Both types show a more rapid washoutf contrast medium than malignant tumors, therefore the
alculation of the washout may be useful.6,15,16,42,43,45,46bsolute washout ≥60% (88% sensitivity and 96% specificity)r relative washout ≥40% (96% sensitivity and 100% speci-city) are suggestive of adenoma16,42,43,45---47 (Figs. 3 and 4).

522 R. Oliveira Caiafa et al.
Phase Opposed ‐phase
Area: 0.36 cm2
Mean: 166.76Standard deviation: 8.81
Area: 0.64 cm2
Mean: 119.17Standard deviation: 4.25
Area: 0.42 cm2
Mean: 31.00Standard deviation: 5.42
Area: 0.80 cm2
Mean: 120.65Standard deviation: 5.18
Figure 5 Adrenal adenoma. Abdominal MRI in a 52-year-old patient investigated for an incidentally discovered adrenal noduleon CT in the left adrenal gland. Opposed-phase gradient echo sequence shows a significant signal loss of the nodule in comparisonw al ad
IieltuLult
sacaarbsmb
watli
bae
nmeoeea
M
Lswq
aCs
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
ith the in-phase sequence, which is highly suggestive of adren
t should be noted that these values are set for delayedmages obtained 15 min after contrast administration. Parkt al.48 analyzed the relative washout values of adrenalesions at 3 min after contrast administration and reportedhat values >25% were diagnostic for adenoma, and val-es ≤5% were compatible with non-adenomatous lesions.esions with values between 5% and 25% were considerednspecific. However, the study had some methodologicalimitations and further research is thus required to validatehese results.
At MRI, on gradient-echo in- and opposed-phaseequences, the signal loss on opposed phase (knowns chemical shift) is indicative of cytoplasmic lipidontent,24---26 which yields a sensitivity of 81---100% and
specificity of 94---100% for the characterization ofdenomas.24,26,49 In quantitative terms, an adrenal/spleenatio ≤70%50,51 or a signal intensity loss >16.5 is compati-le with adenoma.52 However, visual analysis of chemicalhift imaging compared with splenic intensity is an easierethod of adrenal lesion analysis and has been reported toe comparable to quantitative assessments28,29 (Fig. 5).
Chemical shift imaging is not effective in adenomasith unenhanced CT attenuation >30 HU and is as effective
s unenhanced CT in adenomas ≤10 HU.23,25,50,52 Althoughhe sensitivity for adenomas with attenuation 10---30 HU isower than the calculation of contrast washout on CT, chem-cal shift imaging is indicated for these attenuation valuess
Fa
enoma.
ecause it yields a higher sensitivity than unenhanced CTnd avoids the radiation associated with the three contrast-nhanced CT sequences.
After administration of gadolinium contrast media, ade-omas show mild enhancement and rapid washout, whilealignant lesions and pheochromocytomas show marked
nhancement with slower washout.53 There is no consensusn the usefulness of the quantitative assessment of contrastnhancement curves30,53; nonetheless, significant differ-nces in the time-to-peak have been described betweendenomas and malignant lesions.31
etastasis
arge adrenal metastases are usually accompanied by datauggestive of malignancy on CT and MR imaging (Table 1),hile the appearance of small lesions makes them fre-uently indistinguishable from adenomas.6,13,15
Metastases show low values of absolute washout (<0.6%)nd relative washout (<0.4%) on dynamic contrast-enhancedT studies (Fig. 6), and no signal loss on opposed-phaseequences in chemical shift MR imaging, but these are con-
idered non-specific findings.A recent meta-analysis37 has demonstrated that 18F-DG PET/CT has a sensitivity and specificity of 97%nd 91%, respectively, for differentiating between benign

Diagnosis and management of adrenal incidentaloma 523
Porta phase
98 HU 79 HU 69 HU 68 HU
Delayed phase
Area: 0.25 cm2
Mean: 97.95Standard deviation: 18.60
Area: 0.34 cm2
Mean: 69.48Standard deviation: 5.42
Area: 0.34 cm2
Mean: 88.27Standard deviation: 13.52
Area: 0.45 cm2
Mean: 78.82Standard deviation: 19.91
Figure 6 Adrenal metastasis. IV contrast-enhanced CT scan, portal phase at 60 s and delayed phase at 15 min, in a patient witha history of breast cancer shows round/oval homogeneous nodules with smooth, well-defined margins in both adrenal glands.
d 12%
ngcrmcIb
ad
M
Mm
(t
c
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
The lesions show unspecific relative washout of 28% (right) anof the lesions, which confirmed the diagnosis of metastasis.
and malignant lesions, and that the qualitative analysis(visual comparison between adrenal and splenic uptake)is more accurate than quantitative analyses. The studysuggests that PET/CT provides high diagnostic accuracyin lesions >1 cm for distinguishing benign from malignantadrenal disease, particularly in the setting of oncologicpatients, making the use of additional imaging studiesunnecessary in this subgroup of patients.
However, PET/CT is not without limitations: false posi-tive results have been reported in 9%37 of benign lesions,54,55
and 3% of false negative findings37 may be seen inadrenal metastatic lesions with hemorrhage or necro-sis, small-sized (<10 mm) lesions or hypometabolic tumors(bronchioloalveolar carcinoma or carcinoid tumors).54 Addi-tionally, PET/CT is a costly technique with limitedavailability.28,54
MET PET/CT, still not in widespread use, can dif-ferentiate adrenal lesions (adenomas, carcinomas) fromnon-adrenal lesions (adrenal metastases, pheochromocy-tomas, lymphomas) with a sensitivity of 89% and specificityof 96%.38
Growth of an adrenal lesion over a period of less than
3---6 months or the presence of new lesions is suggestive ofmalignancy.When dealing with an incidentaloma in a patientthat presents without an identifiable primary tumor and
e
nt
(left). CT follow-up at 4 months demonstrated enlargement
on-conclusive imaging findings, FNA is rarely indicatediven the low frequency of metastases, the risk ofomplications and the significant rate of false negativeesults. Surgical treatment or CT follow-up are thus recom-ended based on the characteristics of the mass and other
linical characteristics (patient’s age, comorbidity).1,10,28,56
f the mass enlarges during the follow-up period, FNA cane performed before surgical planning.27
The primary indication for FNA is a known primary tumornd high suspicion of metastasis, provided that the definitiveiagnosis changes the therapeutic approach.27
yelolipoma
yelolipomas are tumors composed of varying amounts ofature adipose tissue and hematopoietic cells.The key CT finding is the identification of macroscopic fat
<−20 HU), a characteristic finding that makes unnecessaryhe use of additional techniques6,57,58 (Fig. 7).
FNA is rarely indicated and it is only used in doubtfulases for the characterization of malignant fatty tumors,
specially liposarcomas.The malignant transformation of myelolipomas hasot been reported, and therefore follow-up or surgicalreatment is not required. However, large myelolipomas
524
Figure 7 Myelolipoma. IV contrast-enhanced portal-phaseabdominal CT examination in a 61-year-old-patient investigatedfor evaluation of complications after radical prostatectomy. Thescan shows bilateral lesions with a predominance of fat density,compatible with myelolipomas.
(h
L
Pons
fi
tsmid
P
Og(oit
Baseline
Portal phase
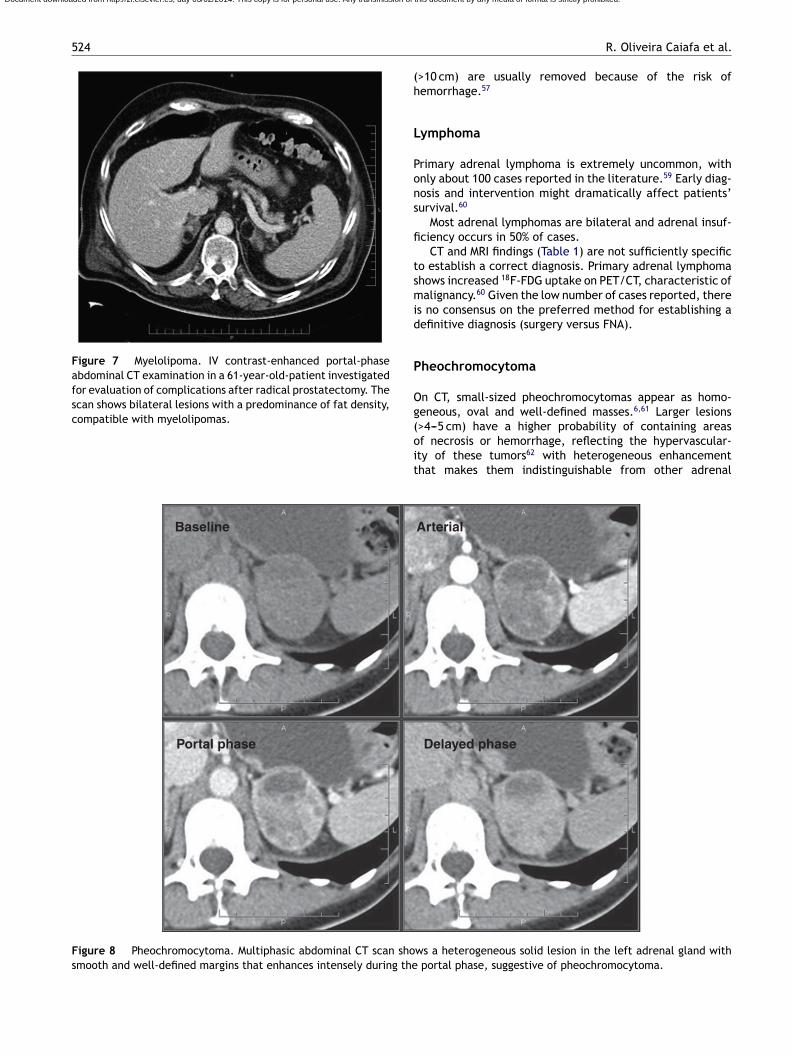
Figure 8 Pheochromocytoma. Multiphasic abdominal CT scan shosmooth and well-defined margins that enhances intensely during the
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
R. Oliveira Caiafa et al.
>10 cm) are usually removed because of the risk ofemorrhage.57
ymphoma
rimary adrenal lymphoma is extremely uncommon, withnly about 100 cases reported in the literature.59 Early diag-osis and intervention might dramatically affect patients’urvival.60
Most adrenal lymphomas are bilateral and adrenal insuf-ciency occurs in 50% of cases.
CT and MRI findings (Table 1) are not sufficiently specifico establish a correct diagnosis. Primary adrenal lymphomahows increased 18F-FDG uptake on PET/CT, characteristic ofalignancy.60 Given the low number of cases reported, there
s no consensus on the preferred method for establishing aefinitive diagnosis (surgery versus FNA).
heochromocytoma
n CT, small-sized pheochromocytomas appear as homo-eneous, oval and well-defined masses.6,61 Larger lesions
>4---5 cm) have a higher probability of containing areasf necrosis or hemorrhage, reflecting the hypervascular-ty of these tumors62 with heterogeneous enhancementhat makes them indistinguishable from other adrenalArterial
Delayed phase
ws a heterogeneous solid lesion in the left adrenal gland with portal phase, suggestive of pheochromocytoma.

Diagnosis and management of adrenal incidentaloma 525
Figure 9 Pheochromocytoma (same patient as Fig. 8). MRI with intravenous contrast material shows a heterogeneous massous
saerf
ipmPmw
C
Tt4hs
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
with hypersignal areas on T2-weighted images, and heterogenesuggestive of pheochromocytoma.
neoplasms; biochemical correlation is thus required for diag-nosis (Fig. 8).
Most pheochromocytomas do not contain lipid; however,a small fraction of cases may contain sufficient intracellularlipid to have attenuation values <10 HU, making them indis-tinguishable from adenomas.44,62---64 Absolute and relativecontrast washout are <60% and <40%, respectively, in 84---89%of cases,43,45,64,65 and pheochromocytomas have attenuationcoefficients on portal-phase CT usually higher than those ofadenomas (up to 110---120 HU), but there is overlap.45
Traditionally, the administration of iodinated contrastmaterial to a patient with pheochromocytoma has beenreported to precipitate a hypertensive crisis, if alpha-receptor blockade has not been instituted.66 However,Mukherjee67 suggests that non-ionic iodinate contrast agentswith low osmolality are safe in these patients, even withoutalpha blockade. Current clinical practice would generallyavoid the use of iodinated contrast material in a patientwith suspected pheochromocytoma.62
T2-weighted imaging is more specific than CT forthe diagnosis of pheochromocytoma62 because of thehyperintensity secondary to the cystic component.68,69
Pheochromocytomas do not lose signal on opposed-phase
T1-weighted sequences,44,62---64 with the exception of thefew cases that contain microscopic fat. Intense and per-sistent enhancement appears after IV administration ofgadolinium70 (Fig. 9).Mmes
areas of hyperintensity on arterial-phase T1-weighted images,
At MR spectroscopy, pheochromocytomas show a uniquepectral signature with a 6.8 ppm peak that may bettributed to the presence of catecholamines and cat-cholamine metabolites.32 However, further research isequired to validate MR spectroscopy as a diagnostic toolor the characterization of pheochromocytoma.
MIBG scintigraphy and 18F-FDG PET/CT are usedn the localization of biochemically suspectedheochromocytomas,28,36 but their use in incidentalo-as is limited as lesions are already localized. Since METET/CT can differentiate adrenal metastases and pheochro-ocytomas from adrenocortical lesions,38 it could be usefulhen dealing with a suspected pheochromocytoma.
arcinoma
he prevalence of adrenal carcinoma is clearly related tohe size of the tumor (2% of tumors ≤4 cm; 6% of tumors.1---6 cm; and 25% of tumors >6 cm), with larger tumorsaving a worse prognosis. Most studies report <50% 5-yearurvival, and many even report <50% at 2 years.2
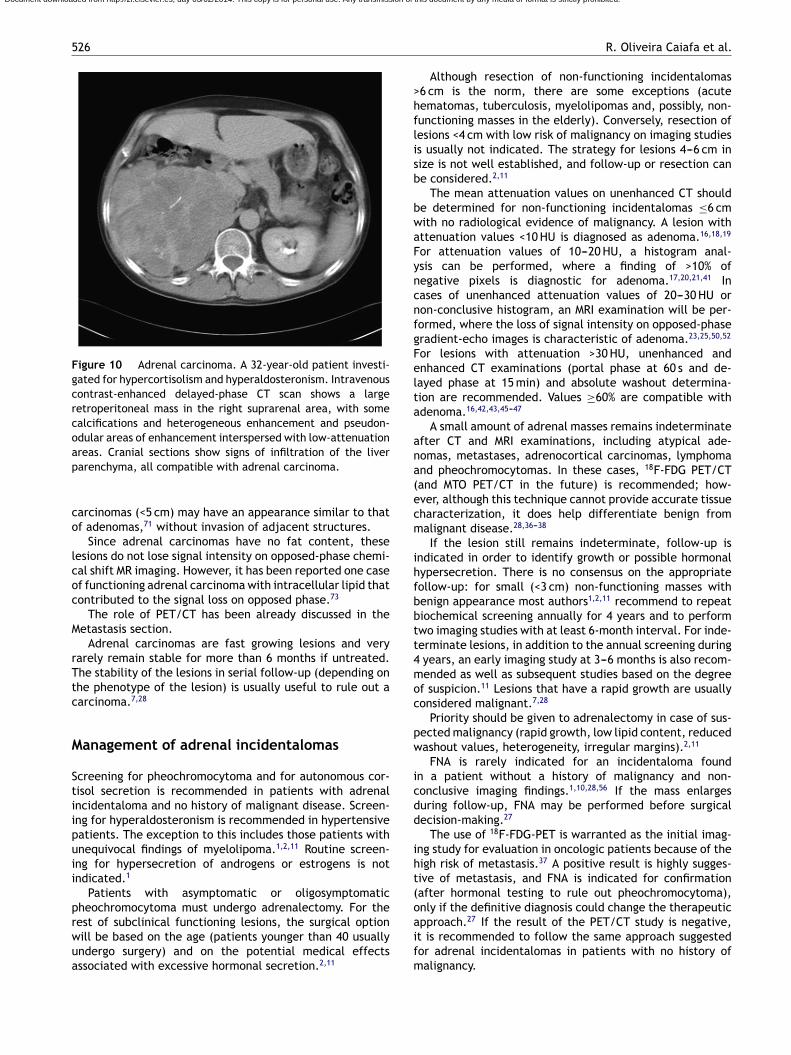
Carcinomas usually appear as large masses on CT and
R imaging (Fig. 10) accompanied by findings suggestive ofalignancy (Table 1). Adrenocortical carcinomas may alsoxtend directly into the vena cava and identification ofuch invasion is essential for surgical planning.71,72 Small
526
Figure 10 Adrenal carcinoma. A 32-year-old patient investi-gated for hypercortisolism and hyperaldosteronism. Intravenouscontrast-enhanced delayed-phase CT scan shows a largeretroperitoneal mass in the right suprarenal area, with somecalcifications and heterogeneous enhancement and pseudon-odular areas of enhancement interspersed with low-attenuationap
co
lcoc
M
rTtc
M
Stiipuii
prwua
>hflisb
bwaFyncnfgFelta
ana(ecm
ihfbbtt4moc
pw
icdd
iht(oapproach.27 If the result of the PET/CT study is negative,
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
reas. Cranial sections show signs of infiltration of the liverarenchyma, all compatible with adrenal carcinoma.
arcinomas (<5 cm) may have an appearance similar to thatf adenomas,71 without invasion of adjacent structures.
Since adrenal carcinomas have no fat content, theseesions do not lose signal intensity on opposed-phase chemi-al shift MR imaging. However, it has been reported one casef functioning adrenal carcinoma with intracellular lipid thatontributed to the signal loss on opposed phase.73
The role of PET/CT has been already discussed in theetastasis section.
Adrenal carcinomas are fast growing lesions and veryarely remain stable for more than 6 months if untreated.he stability of the lesions in serial follow-up (depending onhe phenotype of the lesion) is usually useful to rule out aarcinoma.7,28
anagement of adrenal incidentalomas
creening for pheochromocytoma and for autonomous cor-isol secretion is recommended in patients with adrenalncidentaloma and no history of malignant disease. Screen-ng for hyperaldosteronism is recommended in hypertensiveatients. The exception to this includes those patients withnequivocal findings of myelolipoma.1,2,11 Routine screen-ng for hypersecretion of androgens or estrogens is notndicated.1
Patients with asymptomatic or oligosymptomaticheochromocytoma must undergo adrenalectomy. For theest of subclinical functioning lesions, the surgical option
ill be based on the age (patients younger than 40 usuallyndergo surgery) and on the potential medical effectsssociated with excessive hormonal secretion.2,11ifm
R. Oliveira Caiafa et al.
Although resection of non-functioning incidentalomas6 cm is the norm, there are some exceptions (acuteematomas, tuberculosis, myelolipomas and, possibly, non-unctioning masses in the elderly). Conversely, resection ofesions <4 cm with low risk of malignancy on imaging studiess usually not indicated. The strategy for lesions 4---6 cm inize is not well established, and follow-up or resection cane considered.2,11
The mean attenuation values on unenhanced CT shoulde determined for non-functioning incidentalomas ≤6 cmith no radiological evidence of malignancy. A lesion withttenuation values <10 HU is diagnosed as adenoma.16,18,19
or attenuation values of 10---20 HU, a histogram anal-sis can be performed, where a finding of >10% ofegative pixels is diagnostic for adenoma.17,20,21,41 Inases of unenhanced attenuation values of 20---30 HU oron-conclusive histogram, an MRI examination will be per-ormed, where the loss of signal intensity on opposed-phaseradient-echo images is characteristic of adenoma.23,25,50,52
or lesions with attenuation >30 HU, unenhanced andnhanced CT examinations (portal phase at 60 s and de-ayed phase at 15 min) and absolute washout determina-ion are recommended. Values ≥60% are compatible withdenoma.16,42,43,45---47
A small amount of adrenal masses remains indeterminatefter CT and MRI examinations, including atypical ade-omas, metastases, adrenocortical carcinomas, lymphomand pheochromocytomas. In these cases, 18F-FDG PET/CTand MTO PET/CT in the future) is recommended; how-ver, although this technique cannot provide accurate tissueharacterization, it does help differentiate benign fromalignant disease.28,36---38
If the lesion still remains indeterminate, follow-up isndicated in order to identify growth or possible hormonalypersecretion. There is no consensus on the appropriateollow-up: for small (<3 cm) non-functioning masses withenign appearance most authors1,2,11 recommend to repeatiochemical screening annually for 4 years and to performwo imaging studies with at least 6-month interval. For inde-erminate lesions, in addition to the annual screening during
years, an early imaging study at 3---6 months is also recom-ended as well as subsequent studies based on the degree
f suspicion.11 Lesions that have a rapid growth are usuallyonsidered malignant.7,28
Priority should be given to adrenalectomy in case of sus-ected malignancy (rapid growth, low lipid content, reducedashout values, heterogeneity, irregular margins).2,11
FNA is rarely indicated for an incidentaloma foundn a patient without a history of malignancy and non-onclusive imaging findings.1,10,28,56 If the mass enlargesuring follow-up, FNA may be performed before surgicalecision-making.27
The use of 18F-FDG-PET is warranted as the initial imag-ng study for evaluation in oncologic patients because of theigh risk of metastasis.37 A positive result is highly sugges-ive of metastasis, and FNA is indicated for confirmationafter hormonal testing to rule out pheochromocytoma),nly if the definitive diagnosis could change the therapeutic
t is recommended to follow the same approach suggestedor adrenal incidentalomas in patients with no history ofalignancy.

Diagnosis and management of adrenal incidentaloma 527
ADRENAL INCIDENTALOMA a
History of cancer?
Yes
PET/CT b
Positive
Suspected metastasis/Consider FNA if
appropriate c
Negative
Hormonal testing
Unenhanced CT
Adenoma
Hormonalscreeningannually
Consider FNA
Surgery
Indeterminate lesion/suspected malignancy
Low suspicionof malignancy
Hormonal screening for 4 years+
2 imaging studies at intervalsof at least 6 months
PET/CT b
OEnlargement
Hormonal screening for 4 years +
Imaging studies over shorter intervals dependingon the degree of suspicion of malignancy
Indeterminate adrenal lesion
≥10% negativepixels
<10% negative pixels
Signal loss onopposed phase
No signal loss onopposed phase
Histogram analysis Chemical shift MRIWashout CT (unenhanced
phase, portal phase at60 sec and delayed at 15 min)
Hormonal testingand surgery d
Absence of excessivehormonal secretion
Subclinical hormonalsecretion
Surgery or medicaltreatment e
≤6 cm
≤10 HU >10 HU and ≤20 HU >20 HU and ≤30 HU >30 HU
>6 cm
≥60 % >60%
Lesion size
No
Figure 11 Algorithm for the management of adrenal incidentalomas. aNo additional examination is required in case of unequivocalcharacteristics of myelolipoma; bAdrenal uptake values greater than those of the liver on 18F-FDG PET/CT (visual analysis) aresuggestive of malignant disease. cPrior to FNA, hormonal testing is recommended to rule out pheochromocytoma. dSome authorsrecommend resection of lesions 4---6 cm in size, especially those with characteristics suggestive of malignancy (heterogeneity andirregular margins). ePatients with pheochromocytomas should undergo resection. For the rest of lesions, surgical decision-makingwill be based on the patient’s age and on the potential medical effects associated with excessive hormonal secretion.
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.

5
i
C
Rinbgafag
A
1
C
T
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
28
The algorithm for diagnosis and management of adrenalncidentaloma is shown in Fig. 11.
onclusions
adiologists should participate actively in the diagnosis ofndeterminate lesions by using the appropriate imaging tech-iques. They have to be able to reach a conclusive diagnosisased on the behavior of the lesions, but also, they shouldive advice on the subsequent steps that a non-conclusivedrenal lesion requires based on the experience in the dif-erent techniques available at their institutions. Having anlgorithm is essential as this allows for an appropriate mana-ement of adrenal incidentalomas.
uthorship
1. Responsible for the integrity of the study: ROC, RSI,CNM.
2. Conception of the study: ROC, RSI, LBV, MCSC, CNM.3. Design: ROC, RSI, LBV, MCSC, CNM.4. Acquisition of data: ROC, RSI, LBV, MCSC, CNM.5. Analysis and interpretation of data: ROC, RSI, LBV,
MCSC, CNM.6. Statistical analysis: ROC, RSI, CNM.7. Bibliographic search: ROC, RSI, CNM.8. Drafting of the manuscript: ROC, RSI, CNM.9. Critical review of the manuscript with intellectually rel-
evant contributions: ROC, RSI, LBV, MCSC, CNM.0. Approval of the final version: ROC, RSI, LBV, MCSC, CNM.
onflict of interest
he authors declare not having any conflict of interests.
eferences
1. Young WF. Clinical practice. The incidentally discovered adrenalmass. N Engl J Med. 2007;356:601---10.
2. State-of-the-Science NIH. Statement on management of theclinically inapparent adrenal mass (incidentaloma). NIH ConsensState Sci Statements. 2002;19:1---23.
3. Barzon L, Sonino N, Fallo F, Palu G, Boscaro M. Prevalence andnatural history of adrenal incidentalomas. Eur J Endocrinol.2003;149:273---85.
4. Song JH, Chaudhry FS, May-Smith WW. The incidental adrenalmass on CT: prevalence of adrenal disease in 1,049 consecutiveadrenal masses in patients with no known malignancy. AJR AmJ Roentgenol. 2008;190:1163---8.
5. Song JH, Chaudhry FS, Mayo-Smith WW. The incidental inde-terminate adrenal mass on CT (>10 HU) in patients withoutcancer: is further imaging necessary? Follow-up of 321 con-secutive indeterminate adrenal masses. AJR Am J Roentgenol.2007;189:1119---23.
6. Dunnick NR, Korobkin M. Imaging of adrenal incidentalomas:current status. AJR Am J Roentgenol. 2002;179:559---68.
7. Mayo-Smith WW, Boland GW, Noto RB, Lee MJ. State-of-the-artadrenal imaging. Radiographics. 2001;21:995---1012.
8. Boland GW, Blake MA, Hahn PF, Mayo-Smith WW. Inciden-
tal adrenal lesions: principles, techniques, and algorithms forimaging characterization. Radiology. 2008;249:756---75.9. Mantero F, Terzolo M, Arnaldi G, Osella G, Masini AM, Alì A,et al. A survey on adrenal incidentaloma in Italy. Study Group
3
R. Oliveira Caiafa et al.
on Adrenal Tumors of the Italian Society of Endocrinology. J ClinEndocrinol Metab. 2000;85:637---44.
0. Korobkin M. CT characterization of adrenal masses: the timehas come. Radiology. 2000;217:629---32.
1. Nieman LK. Approach to the patient with an adrenal inciden-taloma. J Clin Endocrinol Metab. 2010;95:4106---13.
2. Lenert JT, Barnett Jr CC, Kudelka AP, Sellin RV, Gagel RF, PrietoVG, et al. Evaluation and surgical resection of adrenal massesin patients with a history of extra-adrenal malignancy. Surgery.2001;130:1060---7.
3. Zagoria RJ. Imaging of the adrenal glands. In: Zagoria RJ, editor.Genitourinary Radiology: The Requisites. Philadelphia: MosbyInc; 2004. p. 352---80.
4. Lee MJ, Hahn PF, Papanicolaou N, Egglin TK, Saini S, Mueller PR,et al. Benign and malignant adrenal masses: CT distinction withattenuation coefficients, size, and observer analysis. Radiology.1991;179:415---8.
5. Dunnick NR, Korobkin M, Francis I. Adrenal radiology: distin-guishing benign from malignant adrenal masses. AJR Am JRoentgenol. 1996;167:861---7.
6. Korobkin M, Brodeur FJ, Francis IR, Quint LE, Dunnick NR, LondyF. CT time-attenuation washout curves of adrenal adenomas andnonadenomas. AJR Am J Roentgenol. 1998;170:747---52.
7. Bae KT, Fuangtharnthip P, Prasad SR, Joe BN, Heiken JP. Adrenalmasses: CT characterization with histogram analysis Method.Radiology. 2003;228:735---42.
8. Korobkin M, Brodeur FJ, Yutzy GG, Francis IR, Quint LE, DunnickNR, et al. Differentiation of adrenal adenomas from nonade-nomas using CT attenuation values. AJR Am J Roentgenol.1996;166:531---6.
9. Boland GW, Lee MJ, Gazelle GS, Halpern EF, McNicholas MM,Mueller PR. Characterization of adrenal masses using unen-hanced CT: an analysis of the CT literature. AJR Am JRoentgenol. 1998;171:201---4.
0. Ho LM, Paulson EK, Brady JM, Wong TZ, Schindera ST. Lipid-pooradenomas on unenhanced CT: does histogram analysis increasesensitivity compared with a mean attenuation threshold? AJRAm J Roentgenol. 2008;191:234---8.
1. Jhaveri KS, Wong F, Ghai S, Haider MA. Comparison of CThistogram analysis and chemical shift MRI in the characteriza-tion of indeterminate adrenal nodules. AJR Am J Roentgenol.2006;187:1303---8.
2. Graser A, Johnson TR, Chandarana H, Macari M. Dual energy CT:preliminary observations and potential clinical applications inthe abdomen. Eur Radiol. 2009;19:13---23.
3. Outwater EK, Siegelman ES, Radecki PD, Piccoli CW,Mitchell DG. Distinction between benign and malignant adrenalmasses: value of T1-weighted chemical-shift MR imaging. AJRAm J Roentgenol. 1995;165:579---83.
4. Savci G, Zeynep Y, Sahin N, Akgöz S, Tuncel E. Value of chemicalshift subtraction MRI in characterization of adrenal masses. AJRAm J Roentgenol. 2006;186:130---5.
5. Haider MA, Ghai S, Jhaveri K, Lockwood G. Chemical shift MRimaging of hyperattenuating (>10 HU) adrenal masses: does itstill have a role? Radiology. 2004;231:711---6.
6. Park BY, Kim CK, Kim B, Lee JH. Comparison of delayedenhanced CT and chemical shift MR for evaluating hyperatten-uating incidental adrenal masses. Radiology. 2007;243:760---5.
7. Song JH, Mayo-Smith WW. Incidentally discovered adrenal mass.Radiol Clin North Am. 2011;49:361---8.
8. Blake MA, Cronin CG, Boland GW. Adrenal imaging. AJR Am JRoentgenol. 2010;194:1450---60.
9. Mayo-Smith WW, Lee MJ, McNicholas MM, Hahn PF, Boland GW,Saini S. Characterization of adrenal masses (< 5 cm) by use of
chemical shift MR imaging: observer performance versus quan-titative measures. AJR Am J Roentgenol. 1995;165:91---5.0. Slapa RZ, Jakubowski W, Januszewicz A, Kasperlik-Zaluska AA,Dabrowska E, Fijuth J, et al. Discriminatory power of MRI for
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
Diagnosis and management of adrenal incidentaloma
differentiation of adrenal non-adenomas vs adenomas evalu-ated by means of ROC analysis: can biopsy be obviated? EurRadiol. 2000;10:95---104.
31. Inan N, Arslan A, Akansel G, Anik Y, Balci NC, Demirci A.Dynamic contrast enhanced MRI in the differential diagnosis ofadrenal adenomas and malignant adrenal masses. Eur J Radiol.2008;65:154---62.
32. Kim S, Salibi N, Hardie AD, Xu J, Lim RP, Lee VS,et al. Characterization of adrenal pheochromocytoma usingrespiratory-triggered proton MR spectroscopy: initial experi-ence. AJR Am J Roentgenol. 2009;192:450---4.
33. Miller FH, Wang Y, McCarthy RJ, Yaghmai V, Merrick L, LarsonA, et al. Utility of diffusion-weighted MRI in characterization ofadrenal lesions. AJR Am J Roentgenol. 2010;194:W179---85.
34. Faria JF, Goldman SM, Szejnfeld J, Melo H, Kater C, Kenney P,et al. Adrenal masses: characterization with in vivo proton MRspectroscopy----initial experience. Radiology. 2007;245:788---97.
35. Friedrich-Rust M, Schneider G, Bohle RM, Herrmann E, Sar-razin C, Zeuzem S, et al. Contrast-enhanced sonography ofadrenal masses: differentiation of adenomas and nonadenoma-tous lesions. AJR Am J Roentgenol. 2008;191:1852---60.
36. Blake MA, Prakash P, Cronin CG. PET/CT for adrenal assessment.AJR Am J Roentgenol. 2010;195:W91---5.
37. Boland GW, Dwamena BA, Sangwaiya MJ, Goehler AG, Blake MA,Hahn PF, et al. Characterization of adrenal masses by using FDGPET: a systematic review and meta-analysis of diagnostic testperformance. Radiology. 2011;259:117---26.
38. Hennings J, Lindhe O, Bergström M, Långström B, Sundin A,Hellman P. [11C]metomidate positron emission tomography ofadrenocortical tumors in correlation with histopathologicalfindings. J Clin Endocrinol Metab. 2006;91:1410---4.
39. Bernardino ME, Walther MM, Phillips VM, Graham Jr SD,Sewell CW, Gedgaudas-McClees K, et al. CT-guided adrenalbiopsy: accuracy, safety, and indications. AJR Am J Roentgenol.1985;144:67---9.
40. Welch TJ, Sheedy PF, Stephens DH, Johnson CM, Swensen SJ.Percutaneous adrenal biopsy: review of a 10-year experience.Radiology. 1994;193:341---4.
41. Halefoglu AM, Bas N, Yasar A, Basak M. Differentiation ofadrenal adenomas from nonadenomas using CT histogram anal-ysis method: a prospective study. Eur J Radiol. 2010;73:643---51.
42. Caoili EM, Korobkin M, Francis IR, Cohan RH, Dunnick NR.Delayed enhancement of lipid-poor adrenal adenomas. AJR AmJ Roentgenol. 2000;175:1411---5.
43. Caoili EM, Korobkin M, Francis IR, Cohan RH, Platt JF,Dunnick NR, et al. Adrenal masses: characterization withcombined unenhanced and delayed enhanced CT. Radiology.2002;222:629---33.
44. Johnson PT, Horton KM, Fishman EK. Adrenal mass imaging withmultidetector CT: pathologic conditions, pearls, and pitfalls.Radiographics. 2009;29:1333---51.
45. Szolar DH, Korobkin M, Reittner P, Berghold A, Bauernhofer T,Trummer H, et al. Adrenocortical carcinomas and adrenalpheochromocytomas: mass and enhancement loss evaluation atdelayed contrast-enhanced CT. Radiology. 2005;234:479---85.
46. Blake MA, Kalra MK, Sweeney AT, Lucey BC, Maher MM,Sahani DV, et al. Distinguishing benign from malignant adrenalmasses: multi-detector row CT protocol with 10-minute delay.Radiology. 2006;238:578---85.
47. Pena CS, Boland GW, Hahn PF, Lee MJ, Mueller PR. Charac-terization of indeterminate (lipid-poor) adrenal masses: useof washout characteristics at contrast-enhanced CT. Radiology.2000;217:798---802.
48. Park BK, Kim CK, Kim B. Adrenal incidentaloma detectedon triphasic helical CT: evaluation with modified relativepercentage of enhancement washout values. Br J Radiol.2008;81:526---30.
6
529
9. Korobkin M, Lombardi TJ, Aisen AM, Francis IR, Quint LE,Dunnick NR, et al. Characterization of adrenal masses withchemical shift and gadolinium-enhanced MR imaging. Radiology.1995;197:411---8.
0. Israel GM, Korobkin M, Wang C, Hecht EN, Krinsky GA.Comparison of unenhanced CT and chemical shift MRI in eval-uating lipid-rich adrenal adenomas. AJR Am J Roentgenol.2004;183:215---9.
1. Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR.The clinically inapparent adrenal mass: update in diagnosis andmanagement. Endocr Rev. 2004;25:309---40.
2. Fujiyoshi F, Nakajo M, Fukukura Y, Tsuchimochi S. Characteri-zation of adrenal tumors by chemical shift fast low-angle shotMR imaging: comparison of four methods of quantitative evalu-ation. AJR Am J Roentgenol. 2003;180:1649---57.
3. Krestin GP, Steinbrich W, Friedmann G. Adrenal masses: evalua-tion with fast gradient-echo MR imaging and Gd-DTPA-enhanceddynamic studies. Radiology. 1989;171:675---80.
4. Chong S, Lee KS, Kim HY, Kim YK, Kim BT, Chung MJ, et al. Inte-grated PET-CT for the characterization of adrenal gland lesionsin cancer patients: diagnostic efficacy and interpretation pit-falls. Radiographics. 2006;26:1811---24.
5. Bagheri B, Maurer AH, Cone L, Doss M, Adler L. Characterizationof the normal adrenal gland with 18F-FDG PET/CT. J Nucl Med.2004;45:1340---3.
6. Quayle FJ, Spitler JA, Pierce RA, Lairmore TC, Moley JF,Brunt LM. Needle biopsy of incidentally discovered adrenalmasses is rarely informative and potentially hazardous. Surgery.2007;142:497---502.
7. Kenney PJ, Wagner BJ, Rao P, Heffess CS. Myelolipoma: CT andpathologic features. Radiology. 1998;208:87---95.
8. Rao P, Kenney PJ, Wagner BJ, Davidson AJ. Imagingand pathologic features of myelolipoma. Radiographics.1997;17:1373---85.
9. Ho CH, Chueh SC, Pu YS, Chen SC, Yu HJ, Huang KH. Primaryadrenal lymphoma----a rare entity with grave prognosis. JTUA.2009;20:168---72.
0. Wang J, Sun NC, Renslo R, Chuang CC, Tabbarah HJ, Barajas L,et al. Clinically silent primary adrenal lymphoma: a case reportand review of the literature. Am J Hematol. 1998;58:130---6.
1. Miyake H, Maeda H, Tashiro M, Suzuki K, Nagatomo H, Aikawa H,et al. CT of adrenal tumors: frequency and clinical sig-nificance of low-attenuation lesions. AJR Am J Roentgenol.1989;152:1005---7.
2. Blake MA, Kalra MK, Maher MM, Sahani DV, Sweeney AT, MuellerPR, et al. Pheochromocytoma: an imaging chameleon. Radio-graphics. 2004;24:S87---99.
3. Motta-Ramirez GA, Remer EM, Herts BR, Gill IS, Hamrahian AH.Comparison of CT findings in symptomatic and inciden-tally discovered pheochromocytomas. AJR Am J Roentgenol.2005;185:684---8.
4. Blake MA, Krishnamoorthy SK, Boland GW, Sweeney AT,Pitman MB, Harisinghani M, et al. Low-density pheochromo-cytoma on CT: a mimicker of adrenal adenoma. AJR Am JRoentgenol. 2003;181:1663---8.
5. Yoon JK, Remer EM, Herts BR. Incidental pheochromocytomamimicking adrenal adenoma because of rapid contrast enhance-ment loss. AJR Am J Roentgenol. 2006;187:1309---11.
6. Raisanen J, Shapiro B, Glazer GM, Desai S, Sisson JC. Plasmacatecholamines in pheochromocytoma: effect of urographiccontrast media. AJR Am J Roentgenol. 1984;143:43---6.
7. Mukherjee JJ, Peppercorn PD, Reznek RH, Patel V, Kaltsas G,Besser M, et al. Pheochromocytoma: effect of nonionic contrastmedium in CT on circulating catecholamine levels. Radiology.
1997;202:227---31.8. Cirillo Jr RL, Bennett WF, Vitellas KM, Poulos AG, Bova JG.Pathology of the adrenal gland: imaging features. AJR Am JRoentgenol. 1998;170:429---35.

5
6
7
7
7
Document downloaded from http://zl.elsevier.es, day 03/02/2014. This copy is for personal use. Any transmission of this document by any media or format is strictly prohibited.
30
9. Krebs TL, Wagner BJ. MR imaging of the adrenalgland: radiologic---pathologic correlation. Radiographics.1998;18:1425---40.
0. van Gils AP, Falke TH, Van Erkel AR, Arndt JW, Sandler MP,Van der Mey AG, et al. MR imaging and MIBG scintigraphy
of pheochromocytomas and extra-adrenal functioning paragan-gliomas. Radiographics. 1991;11:37---57.1. Fishman EK, Deutch BM, Hartman DS, Goldman SM,Zerhouni EA, Siegelman SS. Primary adrenocortical carcinoma:
7
R. Oliveira Caiafa et al.
CT evaluation with clinical correlation. AJR Am J Roentgenol.1987;148:531---5.
2. Lee MJ, Mayo-Smith WW, Hahn PF, Goldberg MA, Boland GW,Saini S, et al. State-of-the-art MR imaging of the adrenal gland.Radiographics. 1994;14:1015---29.
3. Yamada T, Saito H, Moriya T, Tsuboi M, Ishibashi T, Sato A,et al. Adrenal carcinoma with a signal loss on chemical shiftmagnetic resonance imaging. J Comput Assist Tomogr. 2003;27:606---8.