diagnosis and key points in the management of systemic ... · lupus: the essential clinicians...
TRANSCRIPT

Diagnosis and Key Points in the Management of Systemic Lupus
Erythematosus
Amish J. Dave, MD, MPH
Virginia Mason Medical Center
© 2014 Virginia Mason Medical Center
Disclosures
No faculty, provider or planning committee member in a position to influence or control the
content of this presentation has any relevant financial relationships to disclose.
2

© 2014 Virginia Mason Medical Center
Learning Objectives
3
1. Understand common manifestations of SLE and differences between
SLE, cutaneous lupus, and drug-induced lupus
2. Describe initial work-up of SLE
3. Consider initial management approaches and recent updates in
therapy
4. Learn where to find rheumatology patient and provider education
materials
© 2014 Virginia Mason Medical Center
Clinical Case
4
26 year old woman with depression, new onset joint pain in the hands and
feet, fatigue, and hair loss. She notes fingers turning colors in the cold since
age 13
Meds: fluoxetine, oral contraceptive pill
Labs: CBC: 3.1 / 12.5 / 129
CMP notable for albumin 3.0,creatinine 0.8
AST 20, ALT 20, and AP 90
ESR: 43 CRP <3.0
TSH: 3.95
ANA: 1:160 (homogenous)

© 2014 Virginia Mason Medical Center
Does this woman have SLE?
5

© 2014 Virginia Mason Medical Center
Does this woman have SLE?
6
- Young woman
- Positive ANA?
- ESR elevation with normal CRP
- Hypoalbuminemia
- Leukopenia and thrombocytopenia
- Raynaud’s?

© 2014 Virginia Mason Medical Center
Review of Systems for SLE
7
Alopecia
Oral/nasal ulcers (painless)
New headaches
Hx of migraines
Hx of uveitis/scleritis
Hx of pleuritis or pericarditis
Blood in the stool or urine
Joint pain or swelling
Morning stiffness
Fevers
Muscle pain
Focal weakness
Numbness/tingling
Rashes (malar)
Photosensitivity
Dry eyes/mouth
Hx of miscarriages
Hx of blood clots
Hx of seizures
Hx of Raynaud’s

© 2014 Virginia Mason Medical Center
Further history provided…
8
• Fatigue despite adequate sleep.
• Pain and swelling of the wrists, knees, ankles (worse in mornings and
improved with NSAIDs)
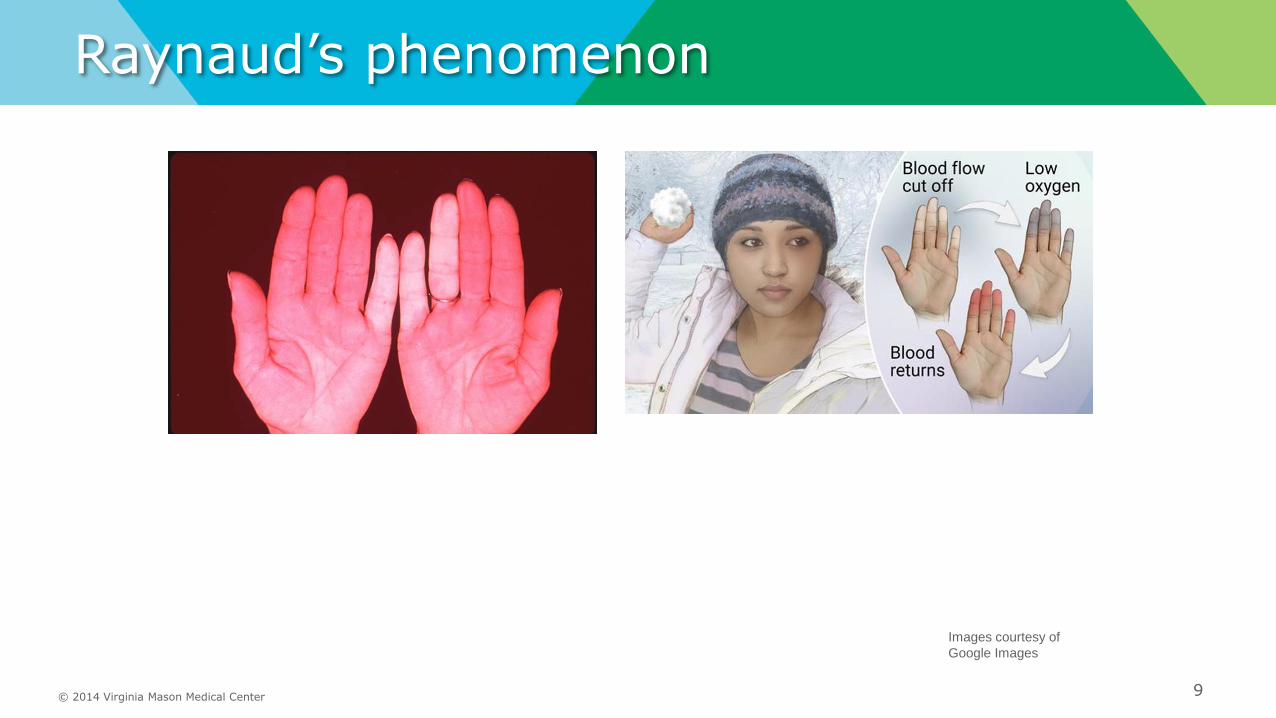
• Patchy hair loss without scarring, fingers have white/blue/red color changes
© 2014 Virginia Mason Medical Center
Raynaud’s phenomenon
9
Images courtesy of
Google Images

What Is Systemic Lupus Erythematosus?
• Systemic lupus erythematosus (SLE) is a progressive chronic autoimmune disease that results in inflammation and tissue damage
• Characterized by flares, spontaneous remission, and relapses
• SLE can affect any part of the body but often results in damage to the skin, joints, heart, kidneys, lungs, and nervous system
Wallace DJ. Lupus: The Essential Clinicians Guide. New York, NY: Oxford University Press; 2009.
Slide courtesy of Dr.
Daniel J. Wallace, MD
(UCLA): Disorders
that overlap with
scleroderma
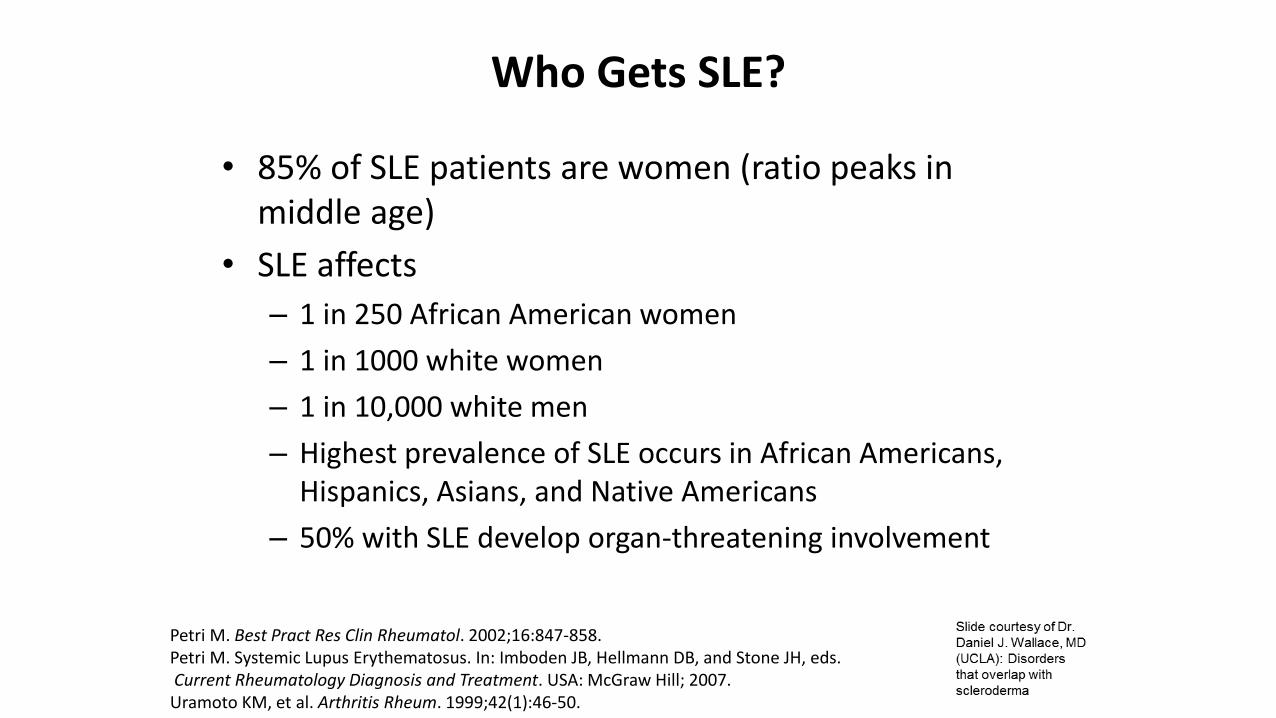
Who Gets SLE?
• 85% of SLE patients are women (ratio peaks in middle age)
• SLE affects
– 1 in 250 African American women
– 1 in 1000 white women
– 1 in 10,000 white men
– Highest prevalence of SLE occurs in African Americans, Hispanics, Asians, and Native Americans
– 50% with SLE develop organ-threatening involvement
Petri M. Best Pract Res Clin Rheumatol. 2002;16:847-858.Petri M. Systemic Lupus Erythematosus. In: Imboden JB, Hellmann DB, and Stone JH, eds.Current Rheumatology Diagnosis and Treatment. USA: McGraw Hill; 2007.Uramoto KM, et al. Arthritis Rheum. 1999;42(1):46-50.

Types of Lupus Erythematosus
• Cutaneous (discoid) lupus erythematosus (40%)
• Systemic lupus erythematosus (50%)
– Nonorgan-threatening disease (25%)
– Organ-threatening disease (25%)
• Drug-induced lupus erythematosus (<1%)
• Crossover or overlap syndrome and/or mixed connective tissue disease (MCTD) (10%)
• Neonatal lupus (<1%)
Wallace DJ. The Lupus Book. New York, NY: Oxford University Press; 2013.

Epidemiology of Lupus Erythematosus (LE) (cont)
• Only 1 in 3 diagnosed with lupus fulfills ACR criteria,1 suggesting prevalence in US between 500,000 and 1,000,000; many have undifferentiated connective tissue disease (UCTD)
• UCTD: presence of autoantibodies with either evidence for inflammatory arthritis or Raynaud’s that does not fulfill criteria for systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), or scleroderma
• Highest prevalence of SLE in US is among African-American women in San Francisco (1/250); lowest is among white men (1/5000)
1. Hochberg MC. Lupus. 1996.

© 2014 Virginia Mason Medical Center
Diagnostic versus Classification Criteria
Diagnostic criteria
Diagnosis may be defined as the determination of the cause or nature of an illness by evaluation of the signs, symptoms and supportive tests in an individual patient.
Diagnostic criteria are a set of signs, symptoms, and tests for use in routine clinical care to guide the care of individual patients.
Diagnostic criteria are generally broad and must reflect the different features of a disease (heterogeneity), with a view to accurately identify as many people with
the condition as possible. Given this complexity, the development and validation of diagnostic criteria can be quite challenging. The Diagnostic and Statistical Manual of
Mental Disorders (DSM) is likely the best-known example of diagnostic criteria. Its initial development was prompted by the observation of extremely poor agreement among
providers regarding patients’ psychiatric diagnoses. There are only a few validated diagnostic criteria in rheumatology, and clinicians commonly establish a diagnosis
based on subjective combination of clinical signs/symptoms, available clinical tests, and knowledge about the epidemiology of their geographical area.
Classification criteria
Classification criteria are standardized definitions that are primarily intended to create well-defined, relatively homogenous cohorts for clinical research; they are
not intended to capture the entire universe of possible patients, but rather to capture the majority of patients with key shared features of the condition. Hence the
goal of classification differs from the intent of diagnostic criteria. Validated classification criteria are considered critical to the interpretation of study findings and comparisons of
results between studies. Despite facilitating the comparison of study results, classification criteria have the potential to restrict the external validity of studies, as interventions
may perform differently in the study participants who fulfill classification criteria for a disease than in the broader group of persons having been diagnosed with the same
disease, i.e., those that share only some but not other disease manifestations considered in classification criteria.
14
Aggarwal R, et al. Arthritis Care Res
(Hoboken). 2015 Jul; 67(7): 891–897.

2019 ACR/EULAR Classification criteria
for systemic lupus erythematosus
Martin Aringer et al. Ann Rheum Dis 2019;78:1151-1159
©2019 by BMJ Publishing Group Ltd and European League Against Rheumatism

SLICC CRITERIA FOR SLE: 2012
• CLINICAL– SKIN
• Acute cutaneous LE
• Chronic cutaneous LE
– ORAL ULCERS
– ALOPECIA
– SYNOVITIS
– SEROSITIS
– RENAL• Prot/Cr ≥0.5
• RBC casts
• BIOPSY*******
– NEUROLOGIC• Sz, psychosis, mononeuritis,
myelitis, p or c neuropathy, acute confusional state
– HEMOLYTIC ANEMIA
– LEUKOPENIA (<4000) or LYMPHOPENIA (<1000)
– THROMBOCYTOPENIA(100k)
• IMMUNOLOGIC
– ANA > normal value
– ANTI-dsDNA
– ANTI-Sm
– ANTI-PHOSPHOLIPID
– LOW COMPLEMENT
– DIRECT COOMB’S POS
93% specificity; 92% sensitivity
Petri M et al for SLICC, Arthritis Rheum 2012
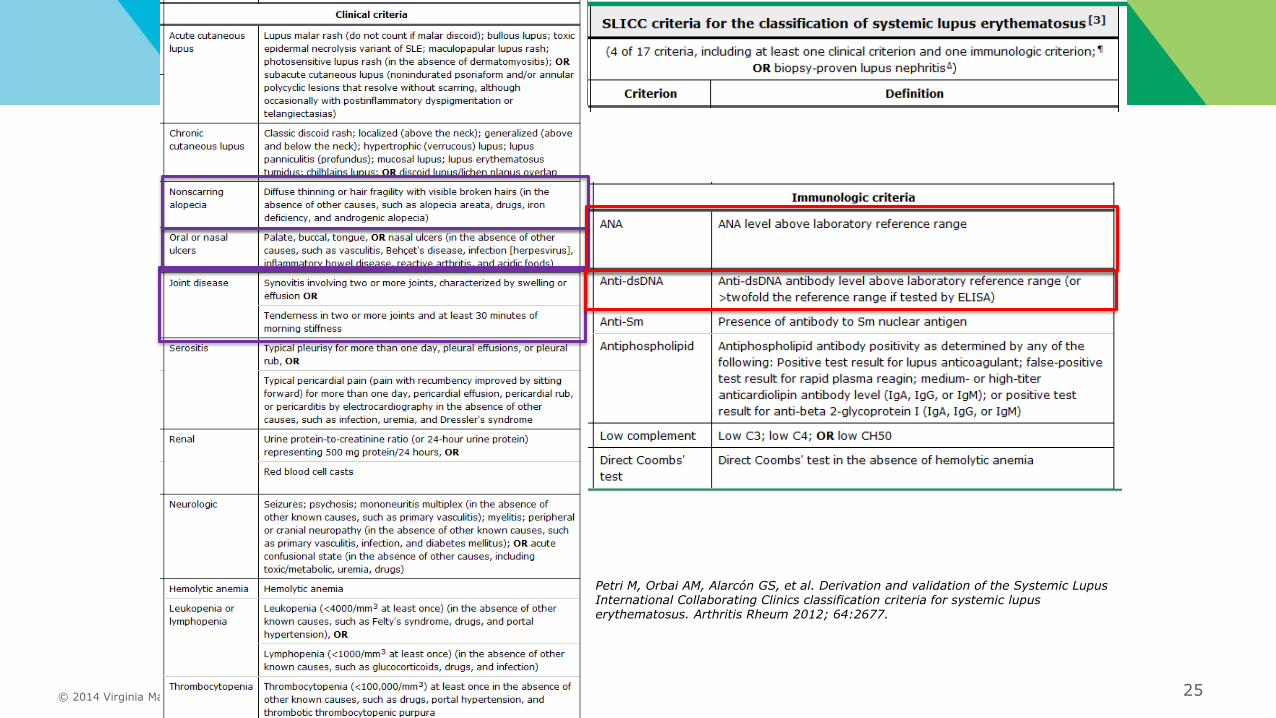
≥4 out of 17 criteria (≥1 clinical and ≥ 1 immunologic) = classify as SLE

© 2014 Virginia Mason Medical Center 17
Petri M, Orbai AM, Alarcón GS, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum 2012; 64:2677.

© 2014 Virginia Mason Medical Center
SLICC Clinical Criteria

© 2014 Virginia Mason Medical Center 19

© 2014 Virginia Mason Medical Center
SLICC Clinical Criteria
20

© 2014 Virginia Mason Medical Center
SLICC Immunologic criteria
21
ANA: >1:160
The majority of individuals with ANA detected at
a dilution of 1:40 (approx. 30% of normal
population) have a false positive result
Ds-DNA- specific for SLE (by ELISA ~70%)
- fluctuate with SLE disease activity
- association w/ active glomerulonephritis
Anti-Smith (Sm)- presents in10 to 50% SLE patients
- specificity: 55 to 100 percent
- does not mirror disease activity
Antiphospholipid antibodies- lupus anticoagulant
*screening tests: dilute Russell viper
venom time (dRVVT) and activated partial
thromboplastin time (aPTT)
* can’t check on anti-coagulation
- anticardiolipin antibody
>40 GPL or MPL, or > the 99th %ile
Venereal Disease Research
Laboratory (VDRL) and rapid plasma
reagin (RPR) tests contains cardiolipin
- anti-beta-2 glycoprotein-I antibody
in titer >the 99th percentile
* association of the IgA isotypes with clinical
thrombosis remains controversial

© 2014 Virginia Mason Medical Center
Further work-up
22
CBC (with differential), CMP
ANA (with titer) including ds-DNA (quantitated), Smith, RNP, SSA/SSB
Anti-TPO, thyroglobulin
ESR, CRP
C3/C4 levels
UA (urine protein and creatinine)
APS (anti-cardiolipin, B2-glycoprotein, lupus anticoagulant), Coombs
HIV, Quantiferon, hepatitis B and C serologies, RPR

© 2014 Virginia Mason Medical Center
Clinical Case
23
26 yo F with hx of hypothyroidism presents with joint pain, fatigue, and hair loss. Meds: fluoxetine, OCP
Exam: swelling of wrist and ankle joints, non-scarring alopecia, ulceration on oral palate
Labs: CBC: 3.1 / 12.5 / 129
CMP notable for albumin 3.0
ESR: 43 CRP: <3
TSH: 3.95
ANA: 1:160 (homogenous), ds-DNA: 300, + SSA
APS negative, Coombs negative
UA wnl, low C3 with normal C4 level

2019 ACR/EULAR Classification criteria
for systemic lupus erythematosus
Martin Aringer et al. Ann Rheum Dis 2019;78:1151-1159
©2019 by BMJ Publishing Group Ltd and European League Against Rheumatism
© 2014 Virginia Mason Medical Center 25
Petri M, Orbai AM, Alarcón GS, et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum 2012; 64:2677.

© 2014 Virginia Mason Medical Center
SLE Management
26
Initial Management:
• Rheumatology referral!
• Start hydroxychloroquine
Up to 6.5 mg/kg* if tolerating
Baseline eye exam
Caution if G6PD deficient
• NSAIDs if no renal involvement
• +/- low dose prednisone (10-15 mg) for arthritis

© 2014 Virginia Mason Medical Center
DMARD Use in SLE
• Hydroxychloroquine (Plaquenil)
• Azathioprine (Imuran)
• Belimumab (Benlysta)
• Mycophenolate (CellCept)
• Cyclophosphomide (Cytoxan)
• Rituximab (Rituxan)*
• Avoid Sulfa Medications (especially
Bactrim!!!)
27

Mechanisms of Benefit of
Hydroxychloroquine• Reduce cytokine secretion: IFNalpha, IL1, IL6, TNFa
• Inhibit lysosomal activity by altering acidic state : reduction
of Ag processing/presentation by DC and M/M
• Inhibit autophagy
• Inhibit signaling through TLR7 and TLR9
• Reduce phospholipase A2 activation
• Reduce synthesis of cholesterol
• Reduce platelet adhesiveness
• Clinical Effects in SLE: Reduce disease flares (?), reduce
damage, reduce thrombosis, reduce cholesterol levels, reduce
HgA1c levels
Fessler BJ et al 2005; Costedoat-Chalumeau N et al
2013: PubMed Search Oct 2015
Slide courtesy of Dr.
Bevra Hahn, MD
(UCLA): SLE 2015 –
Arthritis and Joint
Pain
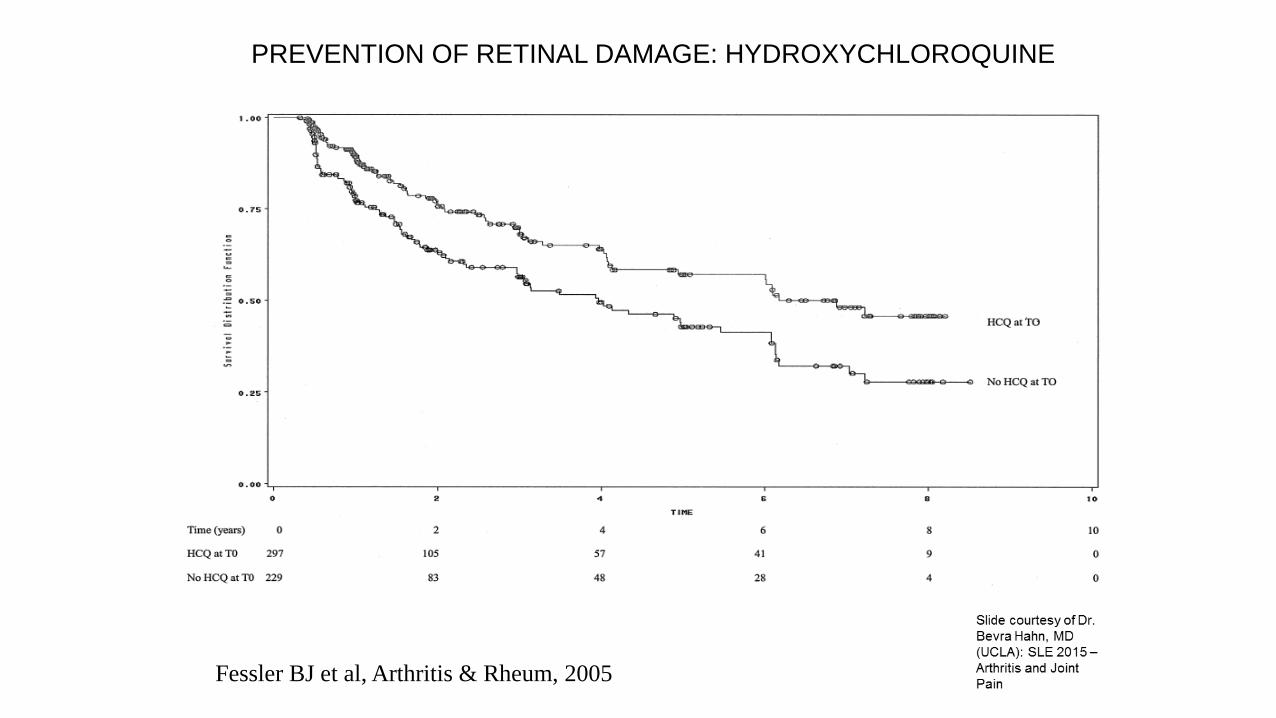
Fessler BJ et al, Arthritis & Rheum, 2005
PREVENTION OF RETINAL DAMAGE: HYDROXYCHLOROQUINE

Hydroxychloroquine and Retinal Toxicity
• Am Association Ophthalmology recommends
– Do not exceed 6.5 mg/kg/day dose.
– Eye exams every 5 years for low risk patients.
– Eye exams every 6-12 months for high risk or retinal
findings.
• High Risk: >8 yrs of Rx, age >60, obesity, renal dz, hepatic dz,
cumulative dose >1000 g
• Expect in Ophth exam: one test of visual field (subjective) and
at least one objective test: spectral domain optical coherence
tomography(OCT), ERG, autofluorescence.
Browning D 2013; Dubois book 2013: Marmor et al 2011

Ophthalmologists Tools for Antimalarial Toxicity
Visual field
Optical Coherence
Tomography
AutofluorescenceERG
Marmor et al 2011

Rates and predictors of hydroxychloroquine retinal toxicity in patients with rheumatoid
arthritis and systemic lupus erythematosus
Arthritis Care & Research Wolfe F et al 2010
Volume 62, Issue 6, pages 775-784, 12 FEB 2010 DOI: 10.1002/acr.20133
http://onlinelibrary.wiley.com/doi/10.1002/acr.20133/full#fig2
Toxicity increases at 8 yrs.
Increase is 5-fold.
Cumulative dose is 1000 g

MP/DC
HLA
TCR
Inosinic acidInosinic acid purines
IMPDH
purines
IMPDH
CD28 B7 B CellT Cell
CD20
CD22
BCMA
TACI
BAFF-R
Y
DNA-
binding
BCR
By BH Hahn
Targeted Therapies in SLE
IMPDH= inosine monophosphate dehydrogenase
CD40L CD 40
Anti-CD40L
LJP394
Treg
Edratide, Lupuzor
BLyS
aBLySTACI Ig
MP/DC
CTLA4 Ig
ICOS B7RP1
Hydroxychloroquine (Laquinimod, OGN for TLR, anti-IFNa)
Cyclophosphamide
Azathioprine
FcγR
Syki
Mycophenolate Mycophenolate
IL6R
Anti-IL6
Rituximab
Ocrelizumab
Epratuzumab
IC C’
Anti-C5a
Syk
CaMK4
NFAT
mTOR
Inhibitors
Tacrolimus
Rapamycin
GLUCOCORTICOIDS
Anti-TWEAK
Proteosome inh

Annual Costs of SLE-related Medications (2015)
• HCQ $ 1,080
• Prednisone $ 156
• Methotrexate $ 408
• Azathioprine $ 1,560
• Mycophenolate $ 5,668
• Belimumab $41,760 (w/o infusion costs)
Hahn BH, data from Epocrates Oct 2015, based on www.goodrx.com
Neuropsychiatric SLE
• SLICC Criteria
– Seizures
– Psychosis
– Mononeuritis
– Myelitis
– Peripheral neuropathy
– Cranial neuropathy
– Acute Confusional State
– ?Depression?Petri et al, Arthritis Rheum 2012

Key Questions in Neuro Lupus
• Is the problem due to lupus or something else (e.g.
infection, meds, atherosclerosis)
– 50/50
• If lupus, is it vascular or non-vascular?
• If lupus, is it inflammatory or non-inflammatory?

CNS SLE
• Evidence that it is INFLAMMATORY
– SLE is active in other systems
– CSF contains elevated protein, cells,
oligoclonal bands, high Ig synthesis (anti-
neuronal, anti-ribosomal P Abs)
– MRI shows enhancing lesions
– Labs show evidence of inflammation; CRP,
ESR, hypocomplementemia, anemia
West, Sterling, in Dubois’ LE 2013

Sibbitt WL Jr, et al, Semin A&R, 2010
VASCULOPATHIC CNS SLE: AUTOPSY OF 14/22 PTS DIED
WITH ACTIVE CNS/SLE OUT OF 200 FOLLOWED 10y w MRI

Trevisani VFM et al, Cochrane
Review, 2009, based on Barileo –
Fabrica et al 2005
Cyclophosphamide in CNS Lupus: ? Better than Steroids
All induced with steroid pulse and maintained on 1 mg/kg/d: Cy = 750 mg/m2 quarterly
For 2 yrs, vs IV steroids monthly, then q 2 mos, then q6 mos. F/u 2 yrs. N = 32 total
3 deaths in Cy; 1 in steroids.

EULAR Guidelines
• 1A Recommendation:
– MRI analysis should include T1 T2-weighted, contrast, DWI
– GLUCOCORTICOID and IMMUNOSUPPRESSIVE THERAPY are indicated for NP manifestations reflecting an immune/inflammatory process with other causes excluded
• Acute confusional state
• Aseptic meningitis
• Myelitis
• Cranial or peripheral neuropathy
• Psychosis
• Optic neuritis (may consider steroids alone)
Bertsias et al ARD 2010

© 2014 Virginia Mason Medical Center
Non-pharmacologic management
• Sun protection
- Exposure to ultraviolet (UV) light may flare SLE
- Sunscreens that block both UV-A and UV-B, SPF ≥55
- Avoid medications that can cause photosensitivity
• Vitamin D (goal 30-60)*
• Herbal remedies are of unproven benefit and may cause harm
?Avoid garlic, melatonin, echinacea, alfalfa sprouts
• Immunizations
Influenza and pneumococcal vaccines are safe
Resultant antibody titers are somewhat less in patients with SLE than in controls Quadrivalent human papilloma virus (HPV) vaccine
No live vaccines:
Glucocorticoids ≥20 mg/day (for more than two weeks)
Azathioprine ≥ 3 mg/kg per day
Belimumab
• Treating comorbid conditions
Accelerated atherosclerosis
Pulmonary hypertension
Antiphospholipid syndrome
Osteopenia or osteoporosis
41
© 2014 Virginia Mason Medical Center
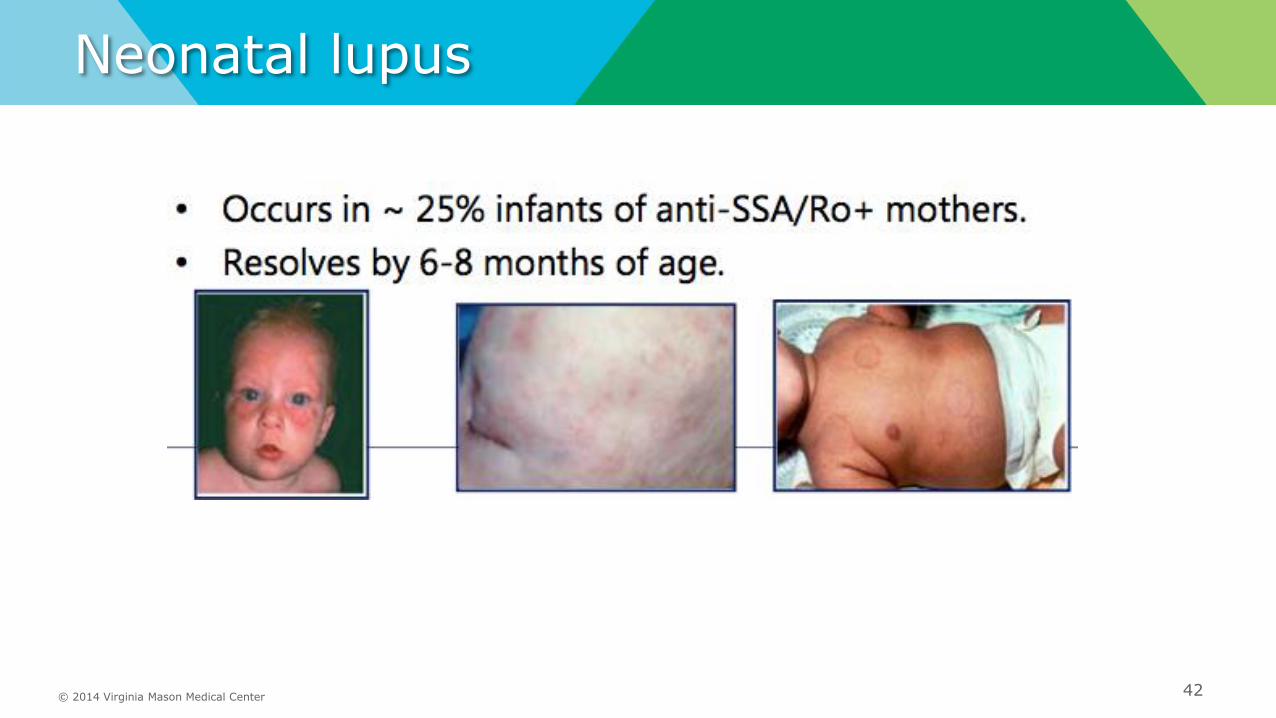
Neonatal lupus
42

© 2014 Virginia Mason Medical Center 43

© 2014 Virginia Mason Medical Center
Prior to Rheumatology Referral
44
Labs:
Recent CBC/CMP
ANA (with IFA)
TSH, TPO-ab, thyroglobulin
UA with urine Protein/Cr if indicated
ESR/CRP
PT/PTT
Hepatitis panel, HIV/Quant gold
XRs hands/feet if joint pain
Dermatology evaluation if concerning rash

Differential Diagnosis of SLE• Autoimmune (RA, scleroderma, myositis, vasculitis, spondyloarthropathies,
inflammatory bowed disorders, Behcet’s, sarcoidosis, Sjogren’s syndrome, thyroiditis, polymyalgia rheumatica, undifferentiated connective tissue disease)
• Infections (TB, HIV, Lyme, CMV, bacterial endocarditis, EBV)
• Fibromyalgia
• Allergies
• Neurologic disorders (esp. myasthenia gravis, MS)
• Malignancy (esp. lymphoproliferative disorders)
• Drug-induced lupus (chlorpromazine, methyldopa, hydralazine,
procainamide, isoniazid, quinidine)
• Psychiatric disorders (eg, bipolar illness, malnutrition, substance abuse)
Wallace DJ. The Lupus Book. New York, NY: Oxford University Press; 2012.Manson JJ, et al. Orphanet Journal of Rare Diseases.2006, 1:6http://bestpractice.bmj.com/best-practice/monograph/103/diagnosis/differential.html. http://emedicine.medscape.com/article/332244-differential. Both accessed July 2013.

© 2014 Virginia Mason Medical Center
Drug induced SLE
46

© 2014 Virginia Mason Medical Center
Patient Education
47
American College of Rheumatology:
http://www.rheumatology.org/I-Am-A/Patient-Caregiver
Lupus Foundation: http://www.lupus.org/

© 2014 Virginia Mason Medical Center
Questions?
Phone: (206) 223-6824
Fax: (206) 625-7288
48
