diagnosing and managing unstable angina -...
TRANSCRIPT

613
Diagnosing and Managing Unstable Angina
Eugene Braunwald, MD (Panel Chair); Robert H. Jones, MD; Daniel B. Mark, MD;Jay Brown, MD; Leslie Brown, MPH, JD; Melvin D. Cheitlin, MD; Craig A. Concannon, MD;Marie Cowan, PhD, RN; Conan Edwards, PhD; Valentin Fuster, MD, PhD; Lee Goldman, MD;
Lee A. Green, MD, MPH; Cindy L. Grines, MD; Bruce W. Lytle, MD;Kathleen M. McCauley, PhD, RN, CS; Alvin I. Mushlin, MD, ScM; Gregory C. Rose, MD;
Earl E. Smith III, MD; Julie A Swain, MD; Eric J. Topol, MD; and James T. Willerson, MD
Abstract This Quick Reference Guide for Clinicians containsrecommendations on the care of patients with unstable anginabased on a combination of evidence obtained through exten-sive literature reviews and consensus among members of anexpert panel. Principal conclusions include the following. (1)Many patients suspected of having unstable angina can bedischarged home after adequate initial evaluation. (2) Furtheroutpatient evaluation may be scheduled for up to 72 hoursafter initial presentation for patients with clinical symptoms ofunstable angina judged at initial evaluation to be at low risk forcomplications. (3) Patients with acute ischemic heart diseasejudged to be at intermediate or high risk of complicationsshould be hospitalized for careful monitoring of their clinicalcourse. (4) Intravenous thrombolytic therapy should not be
Purpose and ScopeUnstable angina is a transitory syndrome that causes
significant disability and death in the United States. In1991 alone, 570 000 hospitalizations for this principaldiagnosis resulted in 3.1 million hospital days. Unstableangina most often results from disruption of an athero-sclerotic plaque and the subsequent cascade of patho-logical processes that critically decrease coronary bloodflow. In most but not all patients presenting withunstable angina (Table 1), symptoms are caused bysignificant coronary artery disease (CAD).
This article provides recommendations and support-ing evidence for all aspects of the diagnosis and treat-ment of unstable angina in both the inpatient andoutpatient settings.Throughout this article, unstable angina is defined as
a clinical syndrome falling between stable angina andmyocardial infarction (MI) in the spectrum of patientswith CAD.
See Table 2 for a listing of information to be enteredinto the medical record during each phase of care.
Initial Evaluation and TreatmentInitial Evaluation
Diagnosis of unstable angina depends on a carefulclinical history, physical examination, and examinationof a resting 12-lead ECG. Therefore, the initial evalu-
administered to patients without evidence of ST segmentelevation and acute myocardial infarction. (5) Assessment ofprognosis by noninvasive testing often aids selection of appro-
priate therapy. (6) Coronary angiography is appropriate forpatients judged to be at high risk for cardiac complications or
death based on their clinical course or results of noninvasivetesting. (7) Coronary artery bypass surgery should be recom-
mended for almost all patients with left main disease and manypatients with three-vessel disease, especially those with leftventricular dysfunction. (8) The discharge care plan shouldinclude continued monitoring of symptoms; appropriate drugtherapy, including aspirin; risk-factor modification; and coun-
seling. (Circulation. 1994;90:613-622.)
ation of patients with symptoms consistent with isch-emic pain usually should take place in a medical facilityand not by telephone.The ECG provides crucial information in the diagno-
sis of unstable angina, and recordings taken both duringperiods of pain and after pain relief are useful.
In patients with symptoms suggesting unstable an-
gina, there are two complementary and equally impor-tant components to the initial assessment:
(1) assessment of the likelihood of CAD (Table 3;see Table 4 for Canadian Cardiovascular Society anginaclassifications) and
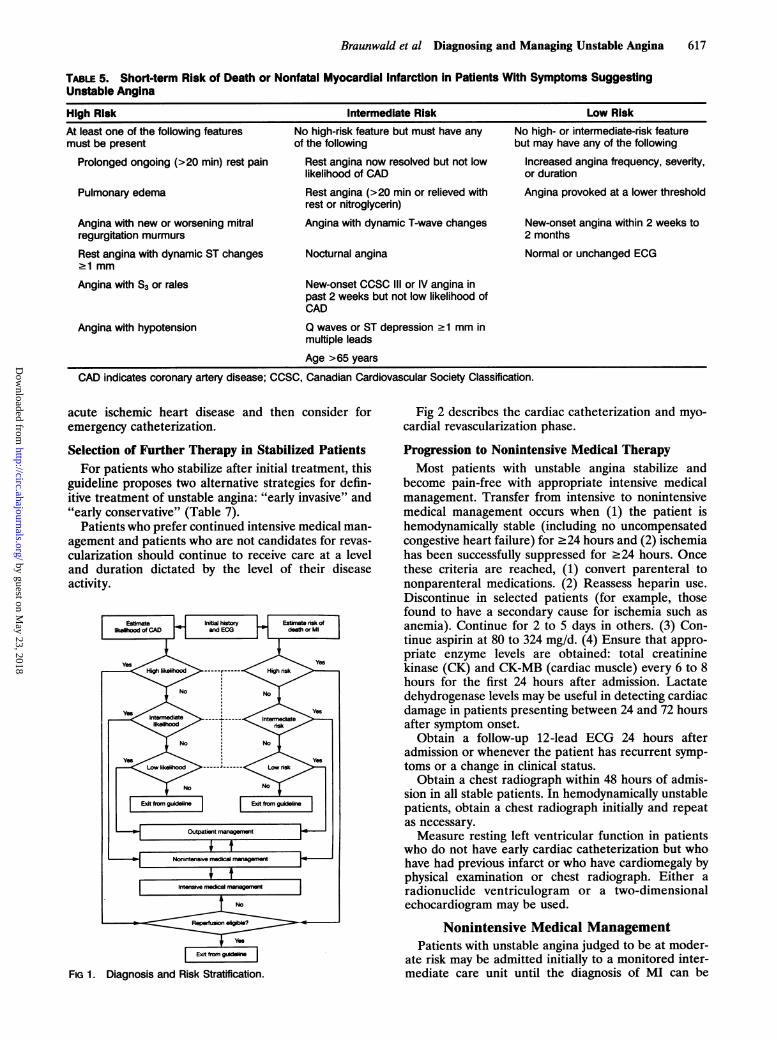
(2) assessment of the risk of adverse outcomes (Ta-ble 5).At the conclusion of this initial evaluation, the patient
can be assigned to one of four diagnostic categories: notcoronary artery disease, stable angina, acute MI, orunstable angina (Fig 1).
Initial Medical TreatmentThe certainty of diagnosis, severity of symptoms,
hemodynamic state, and medication history will deter-mine the choice and timing of drugs used in individualpatients. Drugs to be considered for use at the time ofinitial evaluation and treatment of patients with un-
stable angina include aspirin, heparin, nitrates, and13-blockers (Table 6).Drug treatment should be started in the emergency
department; it should not be delayed until hospitaladmission. The aggressiveness of drug dosage will de-pend on the severity of symptoms and, for many drugs,will require modification throughout the subsequenthospital course.
From the U.S. Department of Health and Human Services,Public Health Service, Agency for Health Care Policy and Re-search, National Heart, Lung, and Blood Institute.
Reprint requests to Dr E. Braunwald, Department of Medicine,Brigham and Women's Hospital, 75 Francis St, Boston, MA 02115.
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

614 Circulation Vol 90, No 1 July 1994
TABLE 1. Unstable Angina Presentations
Rest angina within 1 week of presentation
New onset angina of Canadian Cardiovascular SocietyClassification (CCSC) class Il1 or IV within 2 months ofpresentation (see Table 4)Angina increasing in CCSC class to at least CCSC Ill or IV
Variant angina
Non-O-wave myocardial infarctionPost-myocardial infarction angina (>24 hours)
Give supplemental oxygen to patients with cyanosis,respiratory distress, or high-risk features. Monitor foradequate arterial oxygenation with finger pulse oxime-try or blood gas determinations.
Place patients with intermediate- or high-risk unsta-ble angina on continuous ECG monitoring for ischemiaand arrhythmia detection.
Intravenous thrombolytic therapy is not indicated inpatients who do not have evidence of acute ST-segmentelevation or left bundle branch block on their 12-leadECG.
Outpatient CarePatients with unstable angina who are judged in the
initial evaluation and treatment phase to be at low riskfor adverse outcomes (Table 5) can, in many cases, besafely evaluated further as outpatients. Typically, theseare patients who have experienced new-onset or wors-ening symptoms that may be due to ischemia, but theyhave not had severe, prolonged, or rest episodes in thepreceding 2 weeks.
Schedule a follow-up evaluation as soon as possible,generally within 72 hours after the initial presentation.
Conduct a systematic search for precipitating noncar-diac causes that might explain the new development ofunstable angina symptoms or the conversion from a
stable to an unstable course. Thus, at the follow-upevaluation, each patient should have (1) a second ECGto look for asymptomatic ischemia or arrhythmias, (2)measurement of body temperature and blood pressure,(3) a hemoglobin or hematocrit determination, and (4)a physical examination for evidence of other cardiacdiseases (particularly aortic valve disease and hyper-trophic cardiomyopathy) or hyperthyroidism.Review the patient's history to determine additional
potential exacerbating factors, such as a recent increasein physical activity (especially in combination with en-vironmental temperature extremes), noncompliancewith medical therapy, or a recent increase in psycholog-ical stress levels.
Advise patients diagnosed with unstable angina totake aspirin, 80 to 324 mg/d, unless contraindicationsare present. For patients unable to take aspirin becauseof a history of true hypersensitivity or recent significantgastrointestinal bleeding, ticlopidine 250 mg twice a daymay be used as a substitute.Begin therapy for newly diagnosed patients, generally
with sublingual nitroglycerin as needed, followed by oral3-blockers and/or long-acting topical or oral nitrates.
Review the medical regimen of patients with unstableangina established coronary artery disease already on
medical therapy, and increase dosages as appropriatefor symptom management and as tolerated.
Consider prescribing long-acting forms of antianginaldrugs for enhanced patient compliance.
Intensive Medical ManagementIntensive medical treatment should begin immedi-
ately in the emergency department in patients at high orintermediate risk of death or nonfatal MI. For high-riskpatients, such as those with ongoing angina at restand/or those who appear unstable, simultaneous evalu-ation and treatment assume an urgency greater than forintermediate-risk patients, such as those with priordiscomfort who are asymptomatic during the initialevaluation.
Establish intravenous access while simultaneouslyobtaining a brief cardiovascular history, physical exam-ination, and ECG.
Institute daily aspirin and intravenous heparin plusnitrates and ,3-blockers, the latter to a heart rate of 50 to60 beats per minute (Table 6).
Consider adding calcium channel blockers in thesubset of patients who have significant hypertension(systolic blood pressure .150 mm Hg), in patients whohave refractory ischemia on 1-blockers, and in thosewith variant angina.
Recurrent symptoms after the initial hemodynamicgoals of therapy have been achieved may be regarded asa failure of medical therapy and should prompt consid-eration of urgent cardiac catheterization. Although it istheoretically desirable to have the maximal medicalregimen in place for >24 hours before declaring anypatient a failure of medical therapy, to do so in all casesmay be inappropriate or even dangerous.
Assign patients who have one or more recurrentsevere, prolonged (>20 minutes) ischemic episodes,particularly when accompanied by pulmonary edema, anew or worsening mitral regurgitation murmur, hypo-tension, or new ST- or T-wave changes, to the high-riskcategory regardless of the level of medical therapy andtriage them to early cardiac catheterization.
Assign patients with shorter, less severe ischemicepisodes without accompanying hemodynamic or ECGchanges to a substantially lower risk category andcontinue medical therapy.
Monitoring Medical TherapyDuring the period of intensive medical therapy, ap-
propriate monitoring includes the following.Heparin
Obtain an activated partial thromboplastin time(aPTT) 6 hours after initial therapy is started or anydosage change occurs and every 6 hours thereafter untila therapeutic level of 1.5 to 2.5 times control is obtainedon two consecutive aPTTs.
Obtain an aPTT every 24 hours, once a therapeuticrange is achieved.
Obtain an immediate aPTT if the patient's clinicalcondition changes significantly (eg, recurrent definiteischemia, bleeding, hypotension). Obtain an immediatehemoglobin/hematocrit and platelet determination ifany of the following occur: clinically significant bleeding,recurrent symptoms, or hemodynamic instability. A
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

Braunwald et al Diagnosing and Managing Unstable Angina 615
TABLE 2. Medical Record: Information to be Recorded in the Medical Record Summarizing Initial Evaluation andManagement for Each Patient Includes the Following
After initial evaluationAge and sexDuration and nature of symptoms before presentationPrevious history of coronary artery disease; if yes, prior noninvasive test result, prior cardiac catheterization result, priorrevascularization procedure (bypass or angioplasty)Medicatfon and drug useRisk factors (diabetes, smoking, hypercholesterolemia, hypertension)Systemic causes for precipitating or exacerbating ischemiaECG interpretationlnitial and final assignment of likelihood of coronary artery disease (high, intermediate, low) and basisInital and final risk assignment (high, intermediate, low) and basisSummary of other pertinent posHtive and negative findingsMajor or minor complications of diagnosis or treatmentPatient counseling, including assessment of patient responseDispositon for further careDeath classified as noncardiac or cardiacCardiac deaths classified as precipitated by arrhythmia, progressive ischemia, or progressive cardiac failure
After outpatent managementResults of ancillary clinical studiesFinal diagnosisFinal dispositionEffectiveness of antianginal medication used
After Intensive medical managementIntensity of pain (1-10) and duration (<20 min, <1 h, >1 h) of each episode of angina or equivalent ischemic symptomsDuration of longest anginal episode during the phaseSummary of pharmacological therapy usedDocumentation of the status of patient teaching, including evidence of what the patient appears to understandDocumentation of altemative treatment options discussed with the patientDocumented plan for further care as patient with stable coronary artery disease
After nonintensive medical managementMedications at the beginning and conclusion of this phaseNumber, severity, and duration of ischemic episodesComplications during this phaseEvaluation of patient's understanding of recommended lIestyle changes and assessment of the patient's willingness to adhere torecommendations
After noninvasive testingIndications for testType of test performedSummary of test results, including ECG changes, symptoms, hemodynamic changes, reason for termination (exercise tests)Test complicationsSummary of posttest prognosis (low, intermediate, high risk, or probability of adverse event calculation)
After cardiac catheterization and myocardial revascularizaonReasons for cardiac catheterizationCardiac catheterization findings summarized by number of major coronary arteries with 270% stenosis, presence or absence of a250% left main stenosis, left ventricular ejection fraction, presence and severity of valvular diseaseFor patients undergoing interventional therapy, the primary reason for the procedure, indicated as enhanced survival, pain relief, both,or otherComplications occurring during one procedure that led to another, different procedure (angioplasty failure leading to coronary arterybypass graft surgery), including assessment of severity at the beginning of the second procedure
After hospital dischargeIndicate discharge medical regimenMajor instructions about postdischarge activities and rehabilitation, and the patient's understanding and plan for adherence to therecommendations
At final outpatient visitSummarize cardiac eventsDocument current symptomsMedication changes since hospital discharge or last outpatient visit
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

616 Circulation Vol 90, No 1 July 1994
TABLE 3. Likelihood of Significant CAD in Patients With Symptoms Suggesting Unstable Angina
High Ukelihood Intermediate Ukelihood Low LikelihoodAny of the following features Absence of high likelihood features and Absence of high or intermediate
any of the following likelihood features but may haveKnown history of CAD Definite angina: mean <60 or Chest pain, probably not angina
women <70 years old
Definite angina: men .60 or women Probable angina: men >60 or One risk factor but not diabetes270 years old women >70 years old
Hemodynamic changes or ECG Probably not angina in diabetics or in T wave flat or inverted <1 mmchanges with pain nondiabetics with two or more other in leads with dominant R waves
risk factors*
Variant angina Extracardiac vascular disease Normal ECGST increase or decrease 21 mm ST depression 0.05 to 1 mm
Marked symmetrical T-wave T-wave inversion >1 mm in leadsInversion in multiple precordial leads with dominant R waves
*Coronary artery disease (CAD) risk factors include diabetes, smoking, hypertension, and elevated cholesterol.
drop in platelets necessitates close monitoring for hep-arin-induced thrombocytopenia.Monitor hemoglobin/hematocrit and platelets daily
for the first 3 days of heparin therapy.
3-BlockersMonitor heart rate and blood pressure (target heart
rate for ,3-blockade is 50 to 60 beats per minute).Monitor for congestive heart failure and bronchospasm.Use continuous ECG monitoring.
Discontinuation of Intravenous TherapyDiscontinue heparin after 3 to 5 days.Convert to an oral regimen of P-blockers after the
initial intravenous load in patients without limiting sideeffects. Selection of the oral agent should be based onthe clinician's familiarity with the agent as well as therisk of adverse effects.Change to oral or topical nitrate therapy when the
patient has been symptom-free for 24 hours. Toleranceto nitrates is dose- and duration-dependent and typi-cally becomes significant after only 24 hours of contin-uous therapy. Responsiveness can be enhanced by in-creasing the dose; switching the patient to a topical,oral, or buccal form of therapy; and using a nitrate-freeinterval of 6 to 8 hours.
Reassessing Persistent SymptomsMost patients stabilize and have improvement in their
chest pain after 30 minutes of aggressive medical man-agement and can be admitted to an intensive care unit
TABLE 4. Canadian Cardiovascular SocietyAngina Classification
Activity Umits toClass Evoking Angina Normal Activity
Prolonged exertion None11 Walking >2 blocks Slight
111 Walking <2 blocks MarkedIV Minimal or rest Severe
Adapted from: Campeau L. Grading of angina pectoris [letter].Circulation. 1976;54:522-523. Copyright 1976, American HeartAssociation, Inc. Used with permission.
or intermediate care unit. Failure to respond to initialtherapy should prompt reconsideration of other possi-ble serious causes of chest pain, including (1) ongoingacute MI, (2) aortic dissection, (3) pulmonary embo-lism, (4) pneumothorax, (5) esophageal rupture, and (6)rupture or ischemia of intra-abdominal organs.
Treatment of Severe Ischemia Refractory toAggressive Initial Therapy
Patients considered to have unstable angina afterfurther evaluation and who fail to respond within 30minutes to initial treatment are at increased risk for MIor cardiac death. The major ischemic complicationsseen in unstable angina are recurrent unstable angina,acute ischemic pulmonary edema, new or worseningmitral regurgitation, cardiogenic shock, malignant ven-tricular arrhythmias, and advanced atrioventricularblock. For these patients, in addition to maximizing themedical regimen described in the previous section andinstituting appropriate adjunctive therapy (eg, pulmo-nary artery pressure monitoring and inotropic therapyfor shock, antiarrhythmic therapy for malignant ventric-ular arrhythmias, pacemaker for symptomatic high-grade atrioventricular block), the clinician should con-sider insertion of an intra-aortic balloon pump andcardiac catheterization.
If emergency cardiac catheterization is not possible,an intra-aortic balloon pump should be placed in unsta-ble angina patients who have symptoms refractory tomedical management and those who have symptoms inconjunction with hemodynamic instability. An intra-aortic balloon pump can also serve as a bridge tostabilize the patient on the way to the catheterizationlaboratory or operating room. Exceptions to this recom-mendation include patients with severe peripheral vas-cular disease, significant aortic insufficiency, or knownsevere aortoiliac disease, including aortic aneurysm.
Refer for urgent diagnostic catheterization patientswho have received an intra-aortic balloon pump forstabilization. Transfer patients who have received anintra-aortic balloon pump for stabilization to a facilitycapable of providing diagnostic catheterization andrevascularization.
Reevaluate patients who have not stabilized afterplacement of the pump to reaffirm the diagnosis of
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from
Braunwald et al Diagnosing and Managing Unstable Angina 617
TABLE 5. Short-term Risk of Death or Nonfatal Myocardial Infarction in Patients With Symptoms SuggestingUnstable Angina
High Risk Intermediate Risk Low Risk
At least one of the following featuresmust be present
Prolonged ongoing (>20 min) rest pain
Pulmonary edema
Angina with new or worsening mitralregurgitation murmurs
Rest angina with dynamic ST changes21 mm
Angina with S3 or rales
Angina with hypotension
No high-risk feature but must have anyof the following
Rest angina now resolved but not lowlikelihood of CAD
Rest angina (>20 min or relieved withrest or nitroglycerin)
Angina with dynamic T-wave changes
Nocturnal angina
No high- or intermediate-risk featurebut may have any of the following
Increased angina frequency, severity,or duration
Angina provoked at a lower threshold
New-onset angina within 2 weeks to2 months
Normal or unchanged ECG
New-onset CCSC Ill or IV angina inpast 2 weeks but not low likelihood ofCAD
Q waves or ST depression 21 mm inmultiple leads
Age >65 years
CAD indicates coronary artery disease; CCSC, Canadian Cardiovascular Society Classification.
acute ischemic heart disease and then consider foremergency catheterization.
Selection of Further Therapy in Stabilized PatientsFor patients who stabilize after initial treatment, this
guideline proposes two alternative strategies for defin-itive treatment of unstable angina: "early invasive" and"early conservative" (Table 7).
Patients who prefer continued intensive medical man-agement and patients who are not candidates for revas-cularization should continue to receive care at a leveland duration dictated by the level of their diseaseactivity.
FIG 1. Diagnosis and Risk Stratification.
Fig 2 describes the cardiac catheterization and myo-cardial revascularization phase.
Progression to Nonintensive Medical TherapyMost patients with unstable angina stabilize and
become pain-free with appropriate intensive medicalmanagement. Transfer from intensive to nonintensivemedical management occurs when (1) the patient ishemodynamically stable (including no uncompensatedcongestive heart failure) for .24 hours and (2) ischemiahas been successfully suppressed for .24 hours. Oncethese criteria are reached, (1) convert parenteral tononparenteral medications. (2) Reassess heparin use.Discontinue in selected patients (for example, thosefound to have a secondary cause for ischemia such asanemia). Continue for 2 to 5 days in others. (3) Con-tinue aspirin at 80 to 324 mg/d. (4) Ensure that appro-priate enzyme levels are obtained: total creatininekinase (CK) and CK-MB (cardiac muscle) every 6 to 8hours for the first 24 hours after admission. Lactatedehydrogenase levels may be useful in detecting cardiacdamage in patients presenting between 24 and 72 hoursafter symptom onset.
Obtain a follow-up 12-lead ECG 24 hours afteradmission or whenever the patient has recurrent symp-toms or a change in clinical status.
Obtain a chest radiograph within 48 hours of admis-sion in all stable patients. In hemodynamically unstablepatients, obtain a chest radiograph initially and repeatas necessary.Measure resting left ventricular function in patients
who do not have early cardiac catheterization but whohave had previous infarct or who have cardiomegaly byphysical examination or chest radiograph. Either aradionuclide ventriculogram or a two-dimensionalechocardiogram may be used.
Nonintensive Medical ManagementPatients with unstable angina judged to be at moder-
ate risk may be admitted initially to a monitored inter-mediate care unit until the diagnosis of MI can be
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

618 Circulation Vol 90, No 1 July 1994
TABLE 6. Drugs Commonly Used in Intensive Medical Management of Patients With Unstable Angina
Drug Category Clinical Condition When to Avoid* DosageUnstable angina
Unstable angina inhigh-risk category
Symptoms are not fullyrelieved with threesublingual nitroglycerintablets and initiation of3-blocker therapy
Unstable angina
HypersensitivityActive bleedingSevere bleeding risk
Active bleedingHistory of heparin-inducedthrombocytopeniaSevere bleeding riskRecent stroke
Hypotension
PR ECG segment >0.24seconds20 or 30 atrioventricular blockHeart rate <60 beats perminuteBlood pressure <90 mm HgShockLeft ventricular failure withcongestive heart failureSevere reactive airway disease
324 mg (160-324) daily
80 units/kg IV bolus
Constant IV infusion at 18 U * kg-1 . h-'Titrated to maintain aPTT between 1.5 to 2.5times control
5 to 10 jLg/min by continuous infusion
Titrated up to 75 to 100 ,ug/min until relief ofsymptoms or limiting side effects (headacheor hypotension with a systolic bloodpressure <90 mm Hg or more than 30%below starting mean arterial pressure levelsif significant hypertension is present)
Topical, oral, or buccal nitrates areacceptable alternatives for patients withoutongoing or refractory symptoms
Metoprolol5-mg increments by slow (over 1 to 2minutes) IV administrationRepeated every 5 minutes for a total initialdose of 15 mgFollowed in 1 to 2 hours by 25 to 50 mgby mouth every 6 hoursIf a very conservative regimen is desired,initial doses can be reduced to 1 to 2 mg
Propranolol0.5 to 1.0 mg IV doseFollowed in 1 to 2 hours by 40 to 80 mgby mouth every 6 to 8 hours
EsmololStarting maintenance dose of 0.1mg* kg-'1 min IVTitration in increments of 0.05mg . kg-'1 min every 10 to 15 minutes astolerated by blood pressure until thedesired therapeutic response has beenobtained, limiting symptoms develop, or adose of 0.20 mg * kg-'1 min is reached
Optional loading dose of 0.5 mg/kg may begiven by slow IV administration (2 to 5minutes) for more rapid onset of action
Atenolol5-mg IV doseFollowed 5 minutes later by a second5-mg IV dose and then 50 to 100 mgorally every day initiated 1 to 2 hours afterthe IV dose
IV indicates intravenous; aPTT, activated partial thromboplastin time.*Allergy or prior intolerance contraindication for all categories of drugs listed in this chart.tPatients unable to take aspirin because of a history of hypersensitivity or major gastrointestinal intolerance should be started on
ticlopidine 250 mg twice a day as a substitute.*Choice of the specific agent is not as important as ensuring that appropriate candidates receive this therapy. If there are concerns
about patient intolerance due to existing pulmonary disease, especially asthma, left ventricular dysfunction, or risk of hypotension orsevere bradycardia, initial selection should favor a short-acting agent, such as propranolol or metoprolol or the ultra-short-acting agentesmolol. Mild wheezing or a history of chronic obstructive pulmonary disease should prompt a trial of a short-acting agent at a reduceddose (eg, 2.5 mg IV metoprolol, 12.5 mg oral metoprolol, or 25 g * kg-1 * min-1 esmolol as initial doses) rather than complete avoidanceof beta-blocker therapy.
Note: Some of the recommendations in this guide suggest the use of agents for purposes or in doses other than those specified bythe Food and Drug Administration. Such recommendations are made after consideration of concerns regarding nonapprovedindications. Where made, such recommendations are based on more recent clinical trials or expert consensus.
Aspirint
Heparin
Nitrates
,B-Blockerst
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

Braunwald et al Diagnosing and Managing Unstable Angina
TABLE 6. Continued
Drug Category Clinical Condition When to Avoid* Dosage
Calcium channel Patients whose symptoms Pulmonary edema Dependent on specific agentblockers are not relieved by Evidence of left ventricular
adequate doses of nitrates dysfunctionand (-blockers or inpatients unable to tolerateadequate doses of one orboth of these agents or inpatients with variantangina
Morphine sulate Patients whose Hypotension 2- to 5-mg IV dose
relieved after three serial Respiratory depression May be repeated every 5 to 30 minutes assublingual nitroglycerin Confusion needed to relieve symptoms and maintaintablets or whose Obtundation patient comfortsymptoms recur withadequate anti-ischemictherapy
excluded and it is clear that the patient's symptoms areadequately controlled on medical therapy. These patientsthen enter the nonintensive phase of management.Other moderate-risk and some low-risk patients
may be admitted directly to a regular hospital bedwith telemetry capabilities, thereby proceeding di-rectly to the nonintensive phase. High-risk unstableangina patients will be moved to the nonintensivephase after 1 or more days of intensive managementand stabilization.Once patients reach the nonintensive phase of man-
agement, reasons for continued hospitalization includeoptimization of medical therapy, evaluation of the pro-pensity for recurrent ischemia or ischemic complica-tions, and risk stratification to determine the need forcatheterization and revascularization.
Discontinue continuous monitoring of the ECG inthis phase for most patients.
Instruct all patients to notify nursing personnel im-mediately if chest discomfort recurs.
Recurrent ischemic episodes should prompt a briefnursing assessment and an emergent ECG and shouldbe brought to the attention of a physician.
Reevaluate the patient's medical regimen and adjustdoses of anti-ischemic agents as tolerated.Encourage the patient to progress gradually to a level
of activity, under the observation of the health care
TABLE 7. Alternative Early Strategies for Treatment ofUnstable Angina
Early invasive strategy
AJI hospitalized patients with unstable angina and withoutcontraindications receive cardiac catheterization within 48hours of presentation.
Early conservative strategy
Unless contraindicated, hospitalized patients with unstableangina receive a cardiac catheterization if they have one ormore of the following high-risk indicators: priorrevascularization; associated congestive heart failure ordepressed left ventricular function (ejection fraction <0.50)by noninvasive study; malignant ventricular arrhythmia;persistent or recurrent pain/ischemia; and/or a functionalstudy indicating high risk. All other patients receive medicalmanagement and undergo cardiac catheterization only whenmedical management fails.
team, commensurate with that required to performactivities of daily living.Advise the patient and his or her family regarding
risk-factor modification and have them work with thehealth care team to set appropriate goals.Many patients reaching this phase will be referred
within 1 to 2 days for either noninvasive functionaltesting or cardiac catheterization.
Recurrence of Pain and Return toIntensive Management
Transfer patients who have pain or ECG evidence ofischemia increasing in severity >20 minutes and unre-sponsive to nitroglycerin back to the intensive medicalmanagement phase protocol.
Patients who respond to sublingual nitroglycerin gen-erally do not need to return to intensive medical man-agement. However, a second recurrence of chest pain ofat least 20 minutes' duration in the setting of appropri-ate medical therapy should prompt return of the patientto a monitored environment and the management stepsoutlined in the intensive management phase.
Noninvasive TestingThe goals of noninvasive testing in a recently stabi-
lized patient with unstable angina are to estimate thesubsequent prognosis, especially for the next 3 to 6months, decide which additional tests and adjustmentsin therapy are required based on this prognosis, andprovide the patient with the information and reassur-ances necessary to return to a lifestyle as full andproductive as possible (Fig 3).Conduct exercise or pharmacological stress testing of
low-risk patients with unstable angina who are to bemanaged as outpatients, unless contraindicated.
Perform noninvasive testing within 72 hours of pres-entation (in most cases) in low-risk patients who are tobe managed as outpatients.
Perform noninvasive exercise or pharmacologicalstress testing in low- or intermediate-risk patients hos-pitalized with unstable angina who have been stabilizedand free of angina and congestive heart failure for aminimum of 48 hours, unless cardiac catheterization isindicated.
619
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

620 Circulation Vol 90, No 1 July 1994
FiG 2. Cardiac catheterization and myocardial revascularizaton.
Choice of TestBase the choice of the stress testing modality on an
evaluation of the patient's resting ECG, ability toperform exercise, and the local expertise and technolo-gies available.Use the exercise treadmill test as the standard mode
of stress testing in patients with a normal ECG who arenot taking digoxin.
Test patients with widespread resting ST depression(>1 mm), ST changes secondary to digoxin, left ventric-
ular hypertrophy, left bundle branch block/significantintraventricular conduction deficit, or preexcitation withan imaging modality.Use pharmacological stress testing in combination
with an imaging modality for patients unable to exer-cise because of physical limitations (eg, arthritis, am-putation, severe peripheral vascular disease, generaldebility).An exercise treadmill test is the most commonly used
stress test and has the largest reported experience foruse in patients with unstable angina. A nomogramuseful to convert results from this test into an assess-ment of risk has been derived on a large sample ofpatients with CAD exclusively (not in patients pres-enting with unstable angina) (see the Clinical PracticeGuideline, UnstableAngina: Diagnosis and Management).Use of this nomogram to quantify risk from results oftreadmill examinations provides more clinically usefulinformation than a simple normal/abnormal reading.
Interpreting Noninvasive Test ResultsImplications and appropriate follow-up for the exer-
cise treadmill tests are outlined in Table 8.
Cardiac Catheterization andMyocardial Revascularization
Indications for Cardiac CatheterizationThe goal of cardiac catheterization in patients with
unstable angina is to provide detailed structural informa-tion necessary to assess prognosis and select an appropri-ate long-term management strategy. The procedure isusually helpful in choosing between medical therapy,percutaneous transluminal coronary angioplasty, and cor-onary artery bypass graft surgery in patients at significantrisk for future cardiac events (Fig 2).
Patients undergoing cardiac catheterization includethose managed under either the "early invasive" or"early conservative" strategies defined in Table 7, pa-tients undergoing emergency catheterization directlyfrom the emergency room, and those who experiencedrecurrent ischemic episodes while being managed asoutpatients.
Patients with contraindications to revascularizationbecause of extensive comorbidity and patients who donot wish to consider interventional therapy should notundergo diagnostic catheterization.
Consider the possibility of noncoronary origin ofsymptoms in patients found at catheterization to havenormal coronary arteries or insignificant lesions.
Myocardial RevascularizationRefer patients found at catheterization to have sig-
nificant left main CAD (250%) or significant (>70%)three-vessel disease with depressed left ventricularfunction (ejection fraction <0.50) for coronary arterybypass graft surgery.
Refer patients with two-vessel disease with proximalsevere subtotal stenosis (.95%) of the left anteriordescending artery and depressed left ventricular func-tion for revascularization.
Consider for prompt revascularization (angioplastyor coronary artery bypass grafting) patients with signif-icant CAD if they have any of the following: failure tostabilize with medical treatment; recurrent angina/isch-FIG 3. Noninvasive testing.
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

Braunwald et al Diagnosing and Managing Unstable Angina
TABLE 8. Implications of Stress Test Results
Prognosis* Implications Treatment
Predicted average annual Low risk Manage medically, no need for referralcardiac mortality <1%O/yr to cardiac catheterization
Predicted average annual Intermediate riskt Refer for additional testing, eithercardiac mortality 2%-3%Iyr cardiac catheterization or an alternative
exercise imaging study
Predicted average annual High risk Refer for prompt cardiac catheterizationcardiac mortality .4%O/yr
*Predicted average annual cardiac mortality based on test results interpreted using exercise testing nomogramin Mark DB, Shaw L, Harrell FE et al., Prognostic value of a treadmill exercise score in outpatients with suspectedcoronary artery disease. N Engi J Med. 1991 ;325:849-853.tA stress test resuft of intermediate risk combined with evidence of left ventricular dysfunction should prompt
referral to cardiac catheterization.
emia at rest or with low-level activities; and/or ischemiaaccompanied by congestive heart failure symptoms, anS3 gallop, new or worsening mitral regurgitation, ordefinite ECG changes.For some patients without these high-risk features,
revascularization may still be an option, depending onrecurrent symptoms, test results, and patient preferences.The health care team should educate the patient and
his or her family or advocate about the expected risksand benefits of revascularization and determine individ-ual patient preferences and fears that may affect theselection of therapy.
Hospital Discharge and Postdischarge CareThe need for continued hospitalization of the patient
with unstable angina is determined by whether theobjectives of the hospital admission have been achieved.Patients who have undergone successful revasculariza-tion will usually have the remainder of their hospital-ization defined by the standard protocol for the givenprocedure (eg, 1 to 2 days for angioplasty, 5 to 7 days forcoronary artery bypass graft surgery).
Patients opting for medical treatment after a cardiaccatheterization or functional study include both a low-risk group that can be rapidly discharged (eg, 1 to 2 daysafter testing) and a high-risk group unsuitable for orunwilling to have coronary revascularization. Thesepatients may require a prolonged hospitalization toensure adequate (or as adequate as possible) symptomcontrol.The goal during the hospital discharge phase is to
prepare the patient for normal activities to the extentpossible.
Patient CounselingGive specific instructions on smoking cessation, daily
exercise, and diet.Consider referral, where possible and appropriate, to
a smoking-cessation program or clinic and/or an outpa-tient cardiac rehabilitation program.
Discuss resumption of sexual relations (eg, 2 weeksfor low-risk patients to 4 weeks for postsurgery coronaryartery bypass graft patients).
Give specific instructions, beyond "daily exercise," onactivities that are permissible and those that should beavoided (eg, heavy lifting, climbing stairs, yard work,household activities).
Discuss resumption of driving and return to work.
Discharge Medical RegimenContinue all patients on aspirin, 80 to 324 mg/d,
indefinitely after discharge unless contraindications arepresent.
Continue medications necessary to achieve adequatesymptom control.
Consider discontinuation of antianginal therapy inpatients with successful revascularization without recur-rent ischemia.
If patients have unsuccessful revascularization orrecurrent symptoms following revascularization, con-tinue the antianginal regimen required in hospital tocontrol their symptoms.
Instruct patients who are continuing on antianginaltherapy on the use of sublingual nitroglycerin.
Continue antihypertensive and antihyperlipidemicworkups and therapies started before admission orinitiated in the hospital.
Plan for follow-up medical care at the time of dis-charge whenever possible.
Following and Monitoring SymptomsSchedule follow-up of low-risk patients and patients
with successful coronary artery bypass grafting or an-gioplasty at 2 to 6 weeks and higher-risk patients at 1 to2 weeks.
Instruct the patient (and relevant family members oradvocate) in the purpose, dose, and major side effects ofeach medicine prescribed, using language the patientcan understand.
Give specific instructions for the proper use of sub-lingual nitroglycerin, especially since response of chestpain to this medication is useful in assessing the natureof recurrent symptoms.
Instruct the patient that recurrent symptoms lastingmore than 1 to 2 minutes should prompt him or her tostop all activities, sit down, and place a nitroglycerintablet under the tongue. This may be repeated twice at5-minute intervals for two additional tablets. If symp-toms persist after three nitroglycerin tablets have beentaken, the patient should promptly seek medicalattention.
Instruct the patient that if symptoms change in pat-tern (eg, asymptomatic to symptomatic, more frequentor more severe symptoms), he or she should contact hisor her primary care physician and discuss whetherchanges in the management plan are warranted.
621
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

622 Circulation Vol 90, No 1 July 1994
Instruct the patient to seek transportation to thenearest hospital emergency department, either by am-bulance or by the fastest available alternative, if he orshe cannot reach a physician and chest pain persists formore than 20 minutes or despite three nitroglycerintablets.The natural history of unstable angina is typically
characterized by either progression to nonfatal MI ordeath on the one hand or resumption of the morequiescent clinical course of chronic stable angina/CADon the other. The acute phase of unstable angina isusually over within 4 to 6 weeks. The goal of postdis-charge outpatient care is to make adjustments in thedischarge regimen that appear most appropriate afteran initial period away from direct patient care.The long-term management of unstable angina ends
as the patient reenters the stable phase of CAD.
AcknowledgmentThe guideline was prepared by the panel in collaboration
with a staff at Duke University Medical Center under the abledirection of Drs Robert H. Jones (Project Director) andDaniel B. Mark (Project Codirector). Funding was provided bythe Agency for Health Care Policy and Research and theNational Heart, Lung, and Blood Institute of the US Depart-ment of Health and Human Services (HHS). The constructivehelp of Drs B. Fleming and M. Horan of HHS is acknowl-edged, as is the expert participation of the Duke team,particularly N. Archibald, V. Moore, L.R. Smith, K. Kesler,R.M. Califf, D.B. Pryor, D.B. Matchar, R.H. Sprinkle, V.Hasselblad, and D.F. Fortin. Dr Douglas A. Morrison servedas a special consultant to the panel. Copies of the completeClinical Practice Guideline-Unstable Angina: Diagnosis andManagement (AHCPR publication No. 94-06 02) of this QuickReference Guide for Clinicians (AHCPR publication No. 94-0603) and the related Patient and Family Guide (AHCPR publi-cation No. 94-06 04) may be obtained from AHCPR Publica-tions Clearinghouse, PO Box 8547, Silver Spring, MD 20907 orby calling (800) 358-9295.
General References1. Cairns JA, Gent M, Singer J, et al. Aspirin, sulfinpyrazone, or both
in unstable angina: results of a Canadian multicenter trial. N EnglJ Med. 1985;313:1369-1375.
2. Held PH, Yusuf S, Furberg C. Calcium channel blockers in acutemyocardial infarction and unstable angina: an overview. Br Med J.1989;299:1187-1192.
3. Hirsh J. Heparin. N Engl J Med. 1991;324:565-574.4. ISIS-2 (Second International Study of Infarct Survival) Collabo-
rative Group. Randomized trial of intravenous streptokinase, oralaspirin, both, or neither among 17,187 cases of suspected acutemyocardial infarction: ISIS-2. Lancet. 1988;2:349-360.
5. Lee TH, Cook EF, Weisberg M, et al. Acute chest pain in theemergency room: identification and examination of low-riskpatients. Arch Intern Med. 1985;145:65-69.
6. Lewis HDJ, Davis JW, Archibald DG, et al. Protective effects ofaspirin against acute myocardial infarction and death in men withunstable angina: results of a Veterans Administration CooperativeStudy. N Engi J Med. 1983;309:396-403.
7. Lubsen J, Tijssen JG. Efficacy of nifedipine and metoprolol in theearly treatment of unstable angina in the coronary care unit:findings from the Holland Interuniversity Nifedipine/MetoprololTrial (HINT). Am J Cardiol. 1987;60:18A-25A.
8. Luchi RJ, Scott SM, Deupree RH. Comparison of medical andsurgical treatment for unstable angina pectoris: results of aVeterans Administration Cooperative Study. N Engl J Med. 1987;316:977-984.
9. Mark DB, Nelson CL, Califf RM, et al. The continuing evolution oftherapy for coronary artery disease: initial results from the era ofcoronary angioplasty. Circulation. In press.
10. Mark DB, Shaw L, Harrell FE, et al. Prognostic value of atreadmill exercise score in outpatients with suspected coronaryartery disease. N Engl J Med. 1991;325:849-853.
11. McCormick JR, Schick ECJ, McCabe CH, et al. Determinants ofoperative mortality and long-term survival in patients withunstable angina: the CASS experience. J Thorac Cardiovasc Surg.1985;89:683-688.
12. Muller JE, Turi ZG, Pearle DL, et al. Nifedipine and conventionaltherapy for unstable angina pectoris: a randomized double-blindcomparison. Circulation. 1984;69:728-739.
13. Parisi AF, Folland ED, Hartigan P, et al. A comparison of angio-plasty with medical therapy in the treatment of single-vesselcoronary artery disease. N Engi J Med. 1992;326:10-16.
14. Parisi AF, Khuri S, Deupree RH, et al. Medical compared withsurgical management of unstable angina: 5-year mortality andmorbidity in the Veterans Administration Study. Circulation. 1989;80:1176-1189.
15. Pryor DB, Shaw L, McCants CB, et al. Value of the history andphysical in identifying patients at increased risk for coronary arterydisease. Ann Intern Med. 1993;118:81-90.
16. RISC Group. Risk of myocardial infarction and death duringtreatment with low dose aspirin and intravenous heparin in menwith unstable coronary artery disease. Lancet. 1990;336:827-830.
17. RITA Trial Participants. Coronary angioplasty versus coronaryartery bypass surgery: the Randomized Intervention Treatment ofAngina (RITA) trial. Lancet. 1993;341:573-580.
18. Rouan GW, Lee TH, Cook EF, et al. Clinical characteristics andoutcome of acute myocardial infarction in patients with initiallynormal or nonspecific electrocardiograms (a report from the mul-ticenter chest pain study). Am J Cardiol. 1989;64:1087-1092.
19. Russell RO, Moraski RE, Kouchoukos N, et al. Unstable anginapectoris: national cooperative study group to compare surgical andmedical therapy. Am J Cardiol. 1978;42:839-848.
20. Scott SM, Luchi RJ, Deupree RH. Veterans Administration Coop-erative Study for treatment of patients with unstable angina: results inpatients with abnormal left ventricular function. Circulation. 1988;78(suppl I):I-113-I-121.
21. Selker HP, Griffith JL, D'Agostino RB. A tool for judging coronarycare unit admission appropriateness, valid for both real-time andretrospective use: a time-sensitive predictive instrument (TIPI) foracute cardiac ischemia: a multicenter study. Med Care. 1991;29:610-627.
22. Sharma GV, Deupree RH, Khuri SF, et al. Coronary bypass surgeryimproves survival in high-risk unstable angina: results of a VeteransAdministration cooperative study with an 8-year follow-up: VeteransAdministration Unstable Angina Cooperative Study Group.Circulation. 1991;84(suppl III):III-260-III-267.
23. Telford AM, Wilson C. Trial of heparin versus atenolol in preventionof myocardial infarction in intermediate coronary syndrome. Lancet.1981;1:1225-1228.
24. Theroux P, Ouimet H, McCans J, et al. Aspirin, heparin, or both totreat acute unstable angina. N Engi J Med. 1988;319:1105-1111.
25. Theroux P, Taeymans Y, Morissette D, et al. A randomized studycomparing propranolol and diltiazem in the treatment of unstableangina. JAm Coll Cardiol. 1985;5:717-722.
26. Theroux P, Waters D, Qiu S, et al. Aspirin versus heparin toprevent myocardial infarction during the acute phase of unstableangina. Circulation. 1993;88(pt 1):2045-2048.
27. TIMI IIIA Investigators. Early effects of tissue-type plasmogenactivator added to conventional therapy on the culprit coronarylesion in patients presenting with ischemic cardiac pain at rest.Circulation. 1993;87:38-52.
28. TIMI IIIB Investigators. Effects of tissue plasmogen activator anda comparison of early invasive and conservative strategies inunstable angina and non-Q-wave infarction: results of the TIMIIIIB trial. Circulation. 1994;89:1545-1556.
29. Wallentin LC. Aspirin (75 mg/day) after an episode of unstablecoronary artery disease: long-term effects on the risk for myo-cardial infarction, occurrence of severe angina and the need forrevascularization: Research Group on Instability in CoronaryArtery Disease in Southeast Sweden. JAm Coil Cardiol. 1991;18:1587-1593.
30. Williams DO, Kirby MG, McPherson K, et al. Anticoagulanttreatment of unstable angina. Br J Clin Prac. 1986;40:114-116.
31. Yusuf S, Wittes J, Friedman L. Overview of results of randomizedclinical trials in heart disease, II: unstable angina, heart failure,primary prevention with aspirin, and risk factor modification.JAMA. 1988;260:2259-2263.
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from

Cowan, C Edwards and V FusterE Braunwald, R H Jones, D B Mark, J Brown, L Brown, M D Cheitlin, C A Concannon, M
Diagnosing and managing unstable angina. Agency for Health Care Policy and Research.
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1994 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.90.1.613
1994;90:613-622Circulation.
http://circ.ahajournals.org/content/90/1/613World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 23, 2018
http://circ.ahajournals.org/D
ownloaded from