diabetes mellitus by arisha ibrahim
TRANSCRIPT


ARISHA IBRAHIM
ROLL NO. 105
2nd YEAR MBBS

“DIABETES MELLITUS”

LAY OUT Definition
Types
Etiology
Sign/symptoms
Complications
Ketoacidosis
Diagnosis
Treatment
References
Acknowledgements

DEFINITION “It is a metabolic syndrome of impaired Carbohydrate,Lipid & protein metabolism characterized by “Hyperglycemia” either due to insufficient insulin or defective insulin receptors leading to Polyuria, Polydipsia & Polyphagia.”


TYPES OF DM1) Type 1 DM
2) Type 2 DM
Type 2 is further classified as:
• Non-Obese Type 2 DM
• Obese Type 2 DM

TYPE 1 DM
Due to Insulin deficiency also called :
Insulin Dependent DM (IDDM)
Juvenile onset DM

TYPE 2 DM
Due to combined insulin resistance & decrease insulin secretions also known as :
Noninsulin Dependent DM (NIDDM)
Adult onset DM

SUB TYPES OF NIDDMNON-OBESE TYPE
2 DM
Do not show the early phase of insulin release in response to raised Plasma glucose but B cells do respond to other Insulinogenicstimuli.
OBESE TYPE 2 DM
Insulin Resistance cause Hyperplasia of B cells .Hyperinsulinemiacause Down Regulation of insulin receptors. Obesity is of Abdominal type (Apple Like ).


ETIOLOGYOF

TYPE 1DM TYPE2 DM
• Autoimmune Diseases
• Idiopathic
• Environmental Factors
Mumps
Rubella
Viruses
• Nutrients
Cow milk
• Mutation of insulin receptor Gene (19)
• Auto antibodies to insulin receptor
• Obesity
• Hemo-chromatosis


FACTORS CAUSING INSULIN RESISTANCE
Obesity
Excess Glucocorticoids
Excess Growth Hormone
Lipodystrophy
Ploycystic Ovary Disease
Mutation in Insulin Receptor
Contraceptive agents
B cell Adenoma
Other causes

16

17

SIGN/SYMPTOMS
o Glucosuria
o Polyuria
o Poydipsia
o Polyphagia
o Weight Loss
o Hyperlipedemia


COMPLICATIONS OF DM
EARLY
Ketoacidosis
Coma
Late Complications
Macrovascular
Microvascular

A. MACROVASCULAR
• Atherosclerosis of
Coronary Vessels
• Cerebral Accidents
(stroke)

B. MICROVASCULAR Diabetic Retinopathy

Diabetic Cataract

Diabetic Nephropathy
Proteinuria + Hypertension + Edema
( KIMMELSTEL-WILSON SYNDROME)

Diabetic Neuropathy

Diabetic Gangrene

EARLY Complications
• Diabetic Ketoacidosis
DKA
• Common
in Type 1
• Hyperosmolar
Hyperglycemic
Nonketotic
syndrome
HHNS
• Common
in Type 2

DKAInsulin + Glucagon
Hormone Sensitive Lipase
Lipolysis + Fatty acid oxidation
KETONE BODIES
(8-15mmol/l)
Ketonemia
Ketonuria
Ketoacdisis
Coma
HHNSBlood
glucose+Cellular
dehydration
Hyperosmolarity
(340mOsm/l)
Brain cells shrinkage
Coma

SIGN/SYMPTOMSDKA
1. Hyperglycemia
2. Nausea
3. Air Hunger
4. Fruity Breath Odor
5. Hypotension
6. Tachycardia
7. Abdominal Pain
8. Fatigue
HHNS
1. Altered Consciousness
2. Hyperthermia
3. Motor & sensory impairment
4. Seizures
5. Dry skin & Mucous Mem.
6. Hypotension
7. Extreme thirst
8. Hperglycemia

CLINICAL FEATURES OF DKA

DIAGNOSISDKA
• Metabolic Acidosis
• Blood Glucose is relatively low 350mg/dl
• Ketone bodies in Urine
• Low Bicarbonate & Blood ph
HHNS• No acidosis
• Blood glucose level is up to 800-1000 mg/dl
• Altered Level of Consciousness
• No fruity smell of Breath
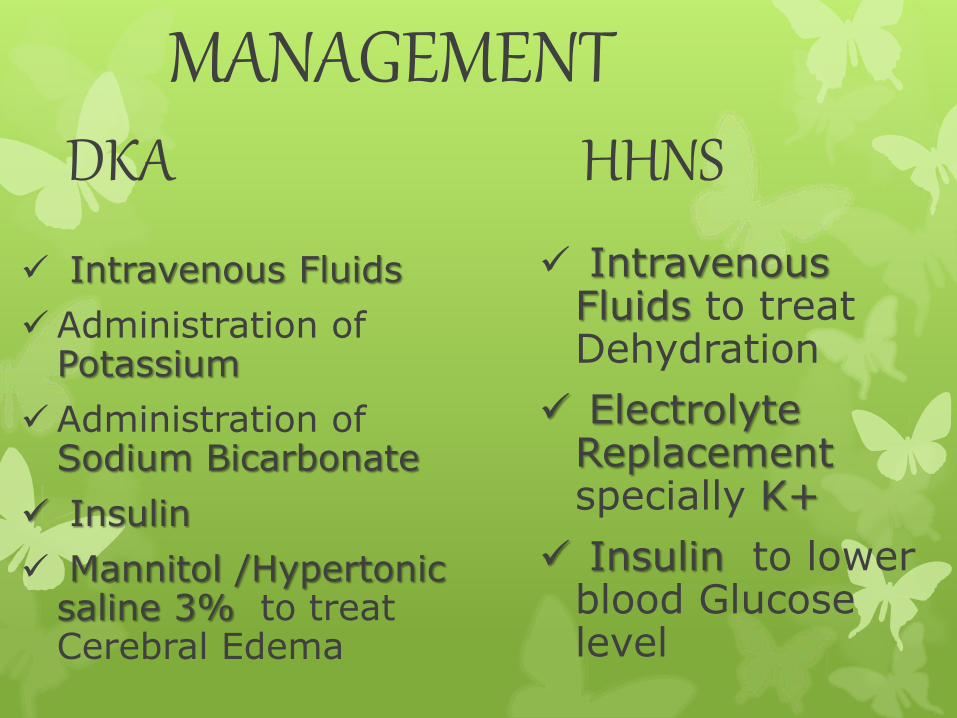
MANAGEMENTDKA
Intravenous Fluids
Administration of Potassium
Administration of Sodium Bicarbonate
Insulin
Mannitol /Hypertonic saline 3% to treat Cerebral Edema
HHNS
Intravenous Fluids to treat Dehydration
Electrolyte Replacementspecially K+
Insulin to lower blood Glucose level

INSULIN SHOCK & HYPOGLYCEMIA
Type 1 DM
Insulin therapy/Missing meals/ Excersise
Sign/symptoms
• Blood Glu (50-70mg/100ml) CNS excites
• Hallucinations
• Trembling/sweating
• Blood Glu (20-50mg/100ml)
• Clonic Seizures/Unconsciousnes
• Coma

DIAGNOSIS
• low blood Glucose level
• No rapid deep breathing
TREATMENT
• Iv Glucose
• Glucagon
• Epinephrine

DIAGNOSTIC TEST FOR DMo GLUCOSURIA
To detect Glucose in Urine
by a Paper Strip Method
o FASTING BLOOD GLUCOSE LEVEL
Normal : 60-110 mg/dl
Impaired: 110-126 mg/dl
Abnormal: >126 mg/dl

o RANDOM BLOOD GLUCOSE LEVEL
Normal : 110-140 mg/dl
Impaired : 140-200 mg/dl
Abnormal: >200 mg/dl

o GLUCOSE TOLERANCE TEST (GTT)
• Indicate Milder or Early DM
Standard Oral GTT
Intravenous GTT
FASTING
2Hrs
Normalmg/dl
100
<140
Impairedmg/dl
100-125
140-199
Diabetesmg/dl
>126
>200

o GLYCOSYLATED HAEMOGLOBIN HbA1c
• Normally it contains 4-6% of
total Hb
• In case of DM its is >7%

TREATMENT OF DM
Non pharmacological Therapy
Pharmacological Therapy

NON PHRAMACOLOGICAL THERAPY
DIET1. TYPE 1 DM :
Fat + Cholesterol+ Carbohydrate
2. TYPE 2 DM : (Cont’d)
“Caloric” Restriction
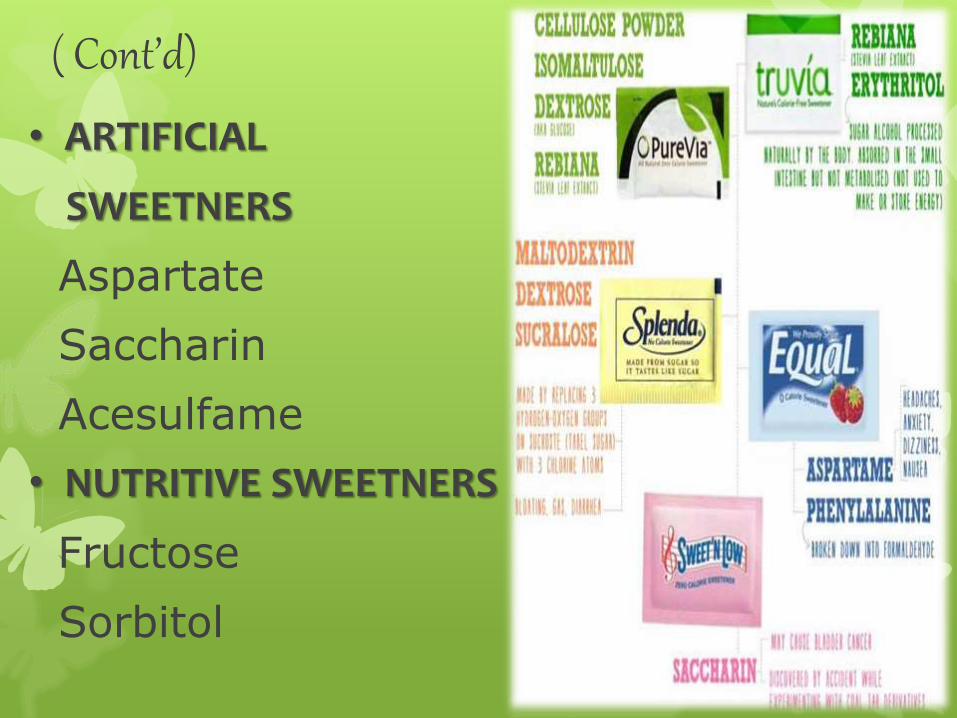
( Cont’d)
• ARTIFICIAL
SWEETNERS
Aspartate
Saccharin
Acesulfame
• NUTRITIVE SWEETNERS
Fructose
Sorbitol
ACTIVITYExercise should start slowly in patients to enhance Insulin sensitivity

PHARMACOLOGICAL THERAPY
o INSULIN both for DM Type 1 & 2
o Drugs Inc. Insulin sensitivity :
Thiazolidinedione
Metformin
Troglitazone
o Drugs Inc. Insulin Release :
Sulfonylureas
(Glyburide & Tolbutamide)
o α- Glucosidase Inhibitors

REFERENCESo Harrison’s Principles Of Internal
Medicine (17th Edition)
o William’s Book Of Endocrinology
(11th Edition)
o Guyton & Hall Physiology
(12th Edition)
o Medical Biochemistry By Mushtaq
Ahmad (7th Edition)
o Textbook Of Medical Biochemistry By MN.Chatterjea (8th Edition)
o Wikipedia

ACKNOWLEDGEMENTS• ALLAH ALMIGHTY
• Prophet (SAW)
• My Parents
• HOD of Biochemistry
“Dr. Khawaja Muhammad Fayyaz”
• My Sister
Dr. Sidra Zafar
• My Friends
