diabetes effec on wound healing
TRANSCRIPT

july 13 :: vol 25 no 45 :: 2011 41NURSING STANDARD
Boyko 2000). Nabuurs-Franssen et al (2005)showed that wound healing resulted in animprovement in patients’ quality of life.
Diabetes mellitus is a disease that affects aperson’s ability to control their blood glucoselevels, either because their body does not produce enough insulin or because their cells do not respond to insulin (insulin resistance)(Tortora and Derrickson 2007). Insulin is thehormone that regulates the uptake of glucosefrom the blood into most cells, but primarilymuscle and fat cells (Dunning 2009). High bloodsugar produces the classic symptoms of polyuria(frequent urination), polydipsia (excessive thirst),weight loss and lethargy.
In response to rising blood glucose levels, beta cells found in the islets of Langerhans in the pancreas release insulin into the blood. This process typically happens after eating (Shier et al 2010). Insulin enables other cells in the body to absorb glucose, which is thenmetabolised to produce energy and glycogen. If not enough insulin is released into thebloodstream, or if the cells do not respond to theinsulin being released, this results in a build-up of glucose in the bloodstream.
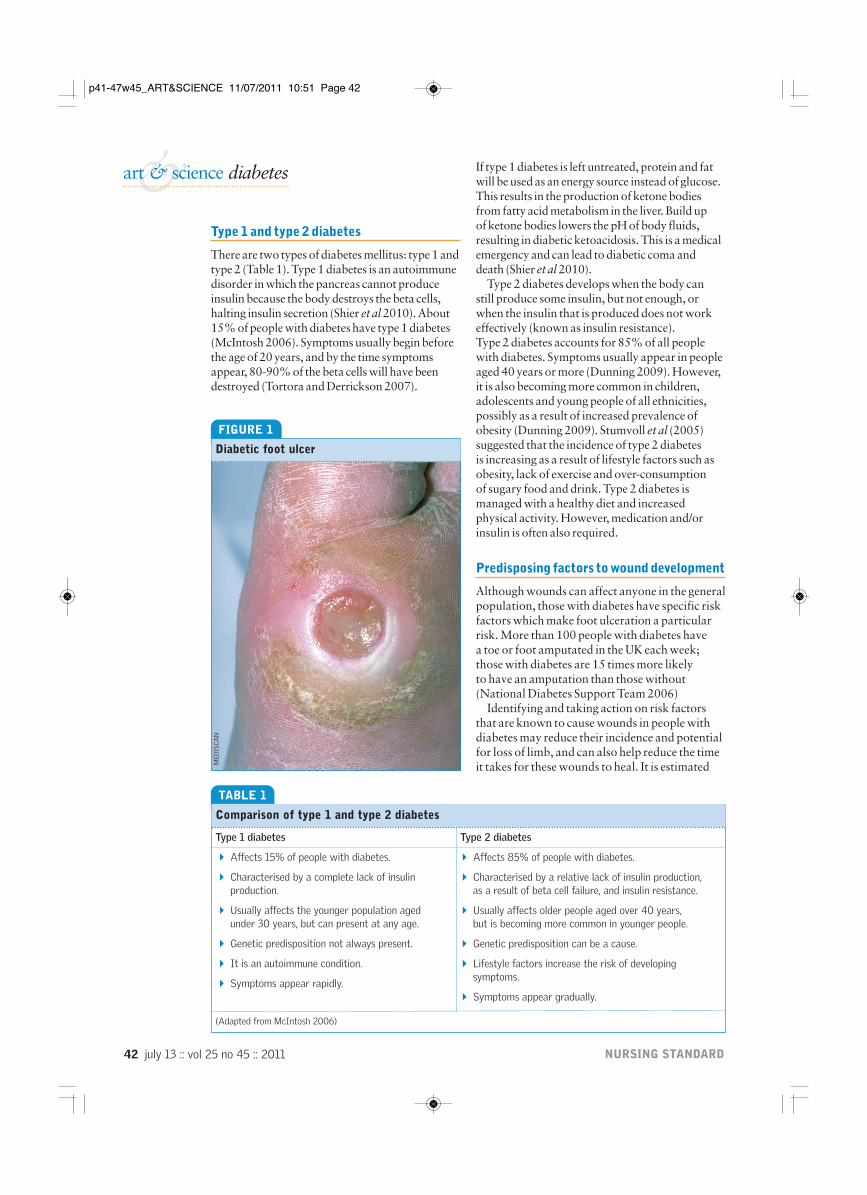
Diabetes mellitus predisposes patients tochronic complications affecting several organs of the body, including the eye, blood vessels,kidneys and the nervous system (Ahmed 2005). It can also have a significant effect on woundhealing. More than half of patients who have had a non-traumatic limb amputation havediabetes, and in a high number of cases theamputation was preceded by an ulcer or non-healing wound (Novak 2010). Intermittentclaudication (cramping pain in the calf and legmuscles caused by an inadequate blood supply to the affected muscles), absent pedal pulses and ischaemic gangrene are more prevalent in people with diabetes. Diabetic foot ulcers(Figure 1) affect up to one quarter of all peoplewith diabetes (Dunning 2009). This statisticshould make wound prevention and goodwound care in patients with diabetes a priorityin health care.
Diabetes and its effects on wound healing
Sharp A, Clark J (2011) Diabetes and its effects on wound healing. Nursing Standard. 25, 45, 41-47. Date of acceptance: October 1 2010.
&art & science diabetes
SummaryThis article discusses the reasons why wounds in people with diabetestake longer to heal and are more susceptible to complications. The physiology of the wound healing process, and how this is affected by diabetes, is outlined. The article also explains why wounds in patients with diabetes are more prone to infection anddiscusses preventive measures.
AuthorsAilsa Sharp, lecturer in adult nursing, Edinburgh Napier University,and Jane Clark, clinical support manager, Systagenix WoundManagement, Gatwick, Surrey. Email: [email protected]
KeywordsDiabetes, infection control, wound care, wound healingThese keywords are based on subject headings from the BritishNursing Index. All articles are subject to external double-blind peerreview and checked for plagiarism using automated software. Forauthor and research article guidelines visit the Nursing Standardhome page at www.nursing-standard.co.uk. For related articlesvisit our online archive and search using the keywords.
DIABETES UK estimate that 2.6 million people in the UK were known to have diabetes in 2009, with up to half a million beingundiagnosed (Diabetes UK 2010). By 2025 it is estimated that four million people in the UK will have been diagnosed with diabetes(Diabetes UK 2010).
Wounds can and do heal in patients withdiabetes, but healing may take longer because the process is impaired (Falanga 2005). A non-healing wound is prone to complications,such as infection and trauma, which can furtherdelay the healing process. This can have asignificant negative effect on patients and theirfamilies and carers (Armstrong et al 2008), withincreased patient morbidity and mortality and the economic consequences of being unable towork. One prospective study looking at quality oflife showed a reduction in general health, physicalfunctioning, physical role and vitality in patientswith active foot ulceration (Ahroni and
p41-47w45_ART&SCIENCE 11/07/2011 10:51 Page 41
42 july 13 :: vol 25 no 45 :: 2011 NURSING STANDARD
If type 1 diabetes is left untreated, protein and fatwill be used as an energy source instead of glucose.This results in the production of ketone bodiesfrom fatty acid metabolism in the liver. Build up of ketone bodies lowers the pH of body fluids,resulting in diabetic ketoacidosis. This is a medicalemergency and can lead to diabetic coma anddeath (Shier et al 2010).
Type 2 diabetes develops when the body can still produce some insulin, but not enough, orwhen the insulin that is produced does not workeffectively (known as insulin resistance). Type 2 diabetes accounts for 85% of all peoplewith diabetes. Symptoms usually appear in peopleaged 40 years or more (Dunning 2009). However,it is also becoming more common in children,adolescents and young people of all ethnicities,possibly as a result of increased prevalence ofobesity (Dunning 2009). Stumvoll et al (2005)suggested that the incidence of type 2 diabetes is increasing as a result of lifestyle factors such asobesity, lack of exercise and over-consumption of sugary food and drink. Type 2 diabetes ismanaged with a healthy diet and increasedphysical activity. However, medication and/orinsulin is often also required.
Predisposing factors to wound development
Although wounds can affect anyone in the generalpopulation, those with diabetes have specific riskfactors which make foot ulceration a particularrisk. More than 100 people with diabetes have a toe or foot amputated in the UK each week; those with diabetes are 15 times more likely to have an amputation than those without(National Diabetes Support Team 2006)
Identifying and taking action on risk factorsthat are known to cause wounds in people withdiabetes may reduce their incidence and potentialfor loss of limb, and can also help reduce the timeit takes for these wounds to heal. It is estimated
&art & science diabetes
Type 1 and type 2 diabetes
There are two types of diabetes mellitus: type 1 andtype 2 (Table 1). Type 1 diabetes is an autoimmunedisorder in which the pancreas cannot produceinsulin because the body destroys the beta cells,halting insulin secretion (Shier et al 2010). About15% of people with diabetes have type 1 diabetes(McIntosh 2006). Symptoms usually begin beforethe age of 20 years, and by the time symptomsappear, 80-90% of the beta cells will have beendestroyed (Tortora and Derrickson 2007).
TABLE 1
Comparison of type 1 and type 2 diabetes
Type 1 diabetes Type 2 diabetes
4 Affects 15% of people with diabetes.
4 Characterised by a complete lack of insulin production.
4 Usually affects the younger population aged under 30 years, but can present at any age.
4 Genetic predisposition not always present.
4 It is an autoimmune condition.
4 Symptoms appear rapidly.
(Adapted from McIntosh 2006)
4 Affects 85% of people with diabetes.
4 Characterised by a relative lack of insulin production, as a result of beta cell failure, and insulin resistance.
4 Usually affects older people aged over 40 years, but is becoming more common in younger people.
4 Genetic predisposition can be a cause.
4 Lifestyle factors increase the risk of developingsymptoms.
4 Symptoms appear gradually.
FIGURE 1
Diabetic foot ulcer
MED
ISCA
N
p41-47w45_ART&SCIENCE 11/07/2011 10:51 Page 42

july 13 :: vol 25 no 45 :: 2011 43NURSING STANDARD
that 34% of patients with diabetes who develop foot ulceration present each year with a recurrence of the ulcer (Dunning 2009).
The following factors contribute to theformation and impaired healing of foot ulcers in people with diabetes (International Working Group on the Diabetic Foot 1999,Reiber et al 1999):
4Neuropathy (leading to structural footproblems and Charcot’s joint).
4Peripheral vascular disease.
4Minor trauma.
4History of a previous ulcer.
4 Socioeconomic status.
Neuropathy Peripheral neuropathy is the cause of foot ulcers in 90% of cases (Driver et al 2007).In sensory neuropathy patients do not feel pain or discomfort to alert them to an injury. Sensoryneuropathy is thought to contribute to thedevelopment of Charcot’s joint – damaged,swollen and deformed joints resulting fromrepeated minor injuries of which the patient is unaware (Figure 2). The formation of Charcot’s joint can lead to motor neuropathy –arching of the foot and clawing of the toes – which alters the pressure points of the feet andcauses calluses, resulting in the formation of foot ulcers at the new pressure points (Shaw andBoulton 1995, Levin 2002, Falanga 2005).
Autonomic neuropathy can result in reducedsweating, which can cause the dry skin andfissures commonly seen in patients with diabetes(Meeking et al 2006). These cracks provide anentry point for bacterial and fungal infections.Fungal foot infection has been implicated as a risk factor for developing lower limb cellulitis(Bristow and Spruce 2009). Swabs are often taken
for bacterial culture and sensitivity in patientswith cellulitis, but checking for fungal infectionsshould also be considered.
Previous ulceration, notably when linked with poor glycaemic control, smoking, alcoholconsumption, self-neglect and peripheralneuropathy, increases the chance of recurrence(McIntosh 2006). Peripheral vascular disease Peripheral vasculardisease occurs twice as often in people withdiabetes compared with the non-diabeticpopulation (Falanga 2005), and can occur at a younger age and progress faster than in peoplewithout diabetes (Shaw and Boulton 1995, Shaw and Boulton 2001). It has been suggestedthat vascular disease alone is not a common cause of ulceration; however, in conjunction withother risk factors, any minor trauma can lead toulceration (Boulton 2006).
Red blood cells consist of haemoglobinsolution contained in a flexible membrane (Shin and Ku 2005), which allows red blood cellsto pass through narrow capillaries. However,
TABLE 2
Risk factors for foot ulcer formation
Risk factor Outcome
Neuropathy:
4 Sensory Reduced or absent sensation signalling damage to the tissues.
4 Motor Altered gait, claw toes or high arch, resulting in change in pressure points,callus development and Charcot’s joint (also a result of sensory neuropathy).
4 Autonomic Reduced sweating, causing cracks and fissures in the tissue, which increasespotential for infection.
Peripheral vascular disease:
4 Atherosclerosis Narrowed lumen with reduced blood supply.
4 Higher blood viscosity Stasis of blood in small vessels.
4 Glycoslyated haemoglobin Less oxygen released to tissues.
4 Thickened basement membrane Reduced diffusion of nutrients and oxygen.
FIGURE 2
Charcot’s foot
WEL
LCO
ME
IMA
GES
p41-47w45_ART&SCIENCE 11/07/2011 10:51 Page 43
44 july 13 :: vol 25 no 45 :: 2011 NURSING STANDARD
in diabetes these red blood cells are lessdeformable, causing vascular complications(Brown et al 1995). A higher blood viscositycaused by increased blood glucose levels results in blood becoming stagnant in the small bloodvessels (Morain and Colen 1990). Glycosylatedhaemoglobin has a higher affinity for oxygen,which reduces the availability of oxygen for thetissues (Stadelmann et al 1998).
Peripheral arterial disease is caused by thepresence of atherosclerosis, in which fattydeposits accumulate and form plaques within the arteries that occlude the lumen over time.Calcification of the peripheral arteries,particularly the distal tibial vessels, is alsocommon in patients with diabetes (McIntosh2006). This can lead to stroke and cardiovasculardisease, which in turn causes reduced mobility,and hence a greater risk of ulceration.
An additional observation in people withdiabetes is a thickening of the basement membraneof capillaries, known as diabetic microangiopathy.This is thought to be more prevalent in the feetbecause of high capillary pressures (Falanga 2005)and is linked to poor delivery of oxygen andnutrients to the tissues (Table 2).Minor trauma Traumatic damage to the tissues is often the cause of a wound. A minor traumamay cause a wound in anyone, but in those withdiabetes the healing process may be compromisedresulting in an ongoing chronic wound. Theprotective elements of sensation may be absent so the damage is unnoticed or not caught as early as it could have been. When the gait is alteredpressure points build up leading to callus formationthat can obscure an ulcer, increasing the risk ofdeveloping ulceration (Foster and Edmonds 2001).Recurrence of ulceration Recurrence ofulceration has been identified as an issue with40% of those with either a new ulcer or arecurrent ulcer appearing within four months of the initial ulcer healing (Pound et al 2005).Studies suggest this is related to poor self-care and control, smoking, high alcohol consumptionand peripheral neuropathy (McIntosh 2006).Socio-economic status Socio-economic status or deprivation is linked to high levels of obesity,inactivity, smoking, a poor diet and high bloodpressure (Diabetes UK 2010). These factors arelinked to both developing diabetes and thepotential to develop complications of diabetesfor those already diagnosed.
Compromised wound healing
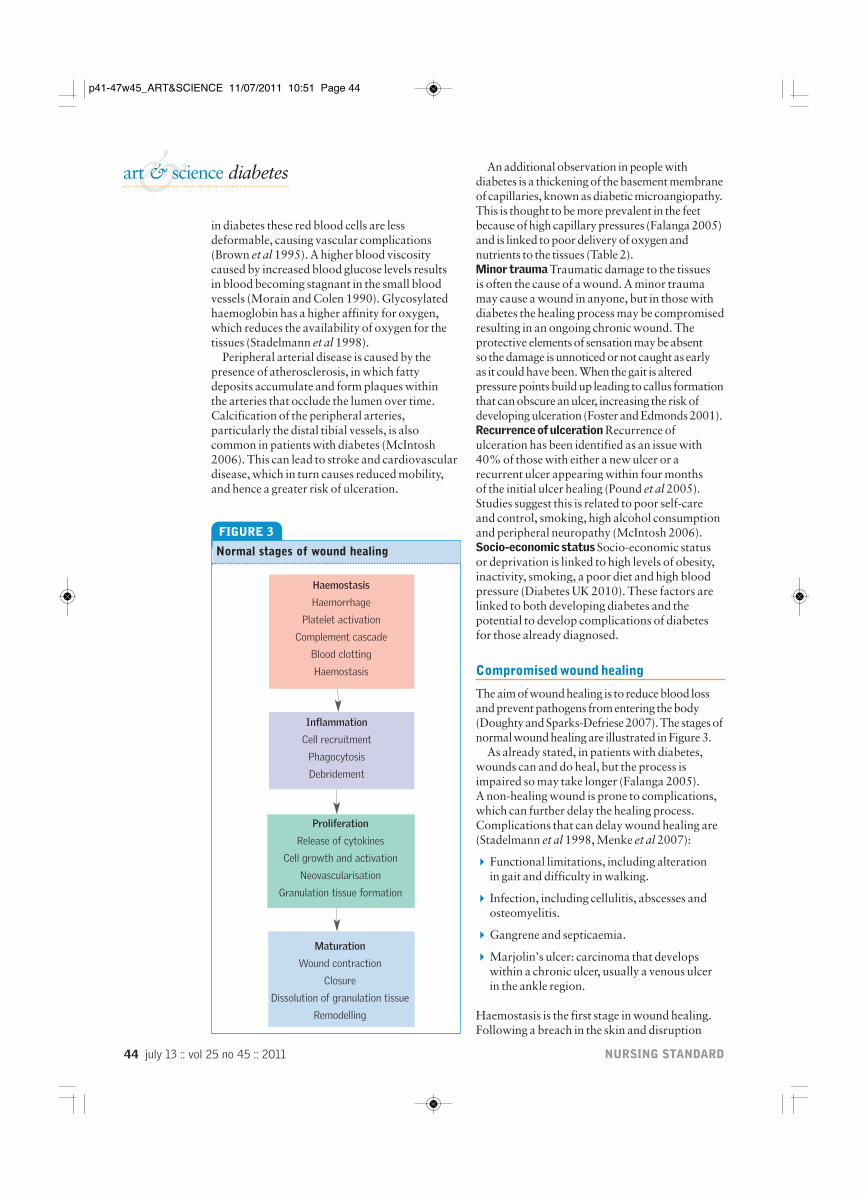
The aim of wound healing is to reduce blood lossand prevent pathogens from entering the body(Doughty and Sparks-Defriese 2007). The stages ofnormal wound healing are illustrated in Figure 3.
As already stated, in patients with diabetes,wounds can and do heal, but the process isimpaired so may take longer (Falanga 2005). A non-healing wound is prone to complications,which can further delay the healing process.Complications that can delay wound healing are(Stadelmann et al 1998, Menke et al 2007):
4Functional limitations, including alteration in gait and difficulty in walking.
4 Infection, including cellulitis, abscesses andosteomyelitis.
4Gangrene and septicaemia.
4Marjolin’s ulcer: carcinoma that developswithin a chronic ulcer, usually a venous ulcer in the ankle region.
Haemostasis is the first stage in wound healing.Following a breach in the skin and disruption
&art & science diabetes
FIGURE 3
Normal stages of wound healing
Haemostasis
Haemorrhage
Platelet activation
Complement cascade
Blood clotting
Haemostasis
Inflammation
Cell recruitment
Phagocytosis
Debridement
Proliferation
Release of cytokines
Cell growth and activation
Neovascularisation
Granulation tissue formation
Maturation
Wound contraction
Closure
Dissolution of granulation tissue
Remodelling
p41-47w45_ART&SCIENCE 11/07/2011 10:51 Page 44

july 13 :: vol 25 no 45 :: 2011 45NURSING STANDARD
of local blood vessels, vasoconstriction andcoagulation with a platelet plug take place(Falanga 2005). However, if the area is poorlysupplied with blood this process can be delayed,potentially allowing invading organisms to enterthe body. The platelets release a wide range ofgrowth factors that recruit cells to the damagedarea and start the wound healing process.
Reduced oxygen supply to the tissues accountsfor some of the problems associated with woundhealing in diabetes. Hypoxia occurs as a result of vascular changes. Hypoxia also has a role in wound infection as it affects the ability of neutrophils and macrophages to function and so allows infection to spread quickly in thediabetic wound (Falanga 2005). In someinstances, hypoxia can be the cause of the woundin the first place, for example in acute arterialocclusion. Hypoxia plays a part in stimulatingangiogenesis – the development of new bloodvessels – and fibroblast proliferation in the early stages of the healing process (Stadelmann et al 1998). However, if oxygen levels do notimprove with new blood vessels supplyingoxygenated blood to the wound bed, thenfibroblasts cannot produce collagen, resulting in impaired healing (Hunt and Pai 1972).
The inflammatory phase of wound healing is impaired in people with diabetes because thereis a reduced number of leucocytes at the woundsite as a result of a narrowing of the blood vessels(Lioupis 2005, Kidman 2008). It has also beensuggested that the phagocytic ability ofleucocytes is impaired (Lioupis 2005). Kidman(2008) suggested that inflammatory cytokinesremain in the diabetic wound much longer thannormal to compensate for the reduced leucocyteactivity, thereby perpetuating and prolongingthe inflammatory phase, resulting in suppressionof granulation tissue formation.
During the early stages of inflammation,neutrophils in the wound site prevent microbial
contamination that could result in infection(Adamson 2009). Proteases and proteins arereleased into the wound bed (Davis 2008), whichis normally a therapeutic process as proteases areneeded to remove damaged components of tissuedestruction and allow cell migration. Theinflammatory phase is usually short lived;however, if the inflammatory phase is prolongedby poor control of proteases, the effect onwound healing can be considerable. Over timethese proteases can cause oedema and localdamage by destroying the new extracellularmatrix (Falanga 2005).
During the proliferative stage in normal wound healing, angiogenesis produces newvascular tissue to support the fibroblastsproducing collagen for the extracellular matrix.However, in the patient with diabetes, thisproliferation of tissue can be compromised.Proliferation follows the inflammatory phase,and can be compromised because the cytokine (or chemical messenger) profile of the wound bed is altered in diabetes. Because of the highnumbers of inflammatory components, including tumour necrosis factor alpha, there is a reduction in the factors that promoteproliferation (for example, platelet-derivedgrowth factor) with pro-inflammatory cytokines dominating the proliferative cytokines. There is also a suggestion thatfibroblasts are less responsive to growth factors in ulcers in people with diabetes (Loot et al 2002) and the tensile strength ofcollagen is poorer, with a tendency to break(Lioupis 2005).
The result is slower production of matrix in the wound bed as proliferative activity issuppressed (Lobmann et al 2002). Essentially the inflammatory processes are poorly regulatedin patients with diabetes, promoting continuedinflammation and delay of the proliferative stageof healing (Table 3).
TABLE 3
Impaired wound healing in patients with diabetes
Normal wound healing Impairment in diabetes
Haemostasis Increased risk of infection. Poor vascular supply.
Inflammation Slow recruitment of neutrophils. Persistent inflammation.
Infection Hyperglycaemia encourages bacterial growth. Slow and ineffective neutrophil and macrophage activity.
Proliferation Reduced tensile strength of collagen. Reduced collagen deposition. Reduced fibroblast activity.
Maturation Reduced tensile strength of collagen. Risk of ulcer recurrence as a result of weakened area of scar tissue.
p41-47w45_ART&SCIENCE 11/07/2011 10:51 Page 45

46 july 13 :: vol 25 no 45 :: 2011 NURSING STANDARD
&art & science diabetes
Adamson R (2009) Role of themacrophages in normal wound healing: an overview. Journal of Wound Care. 18, 8, 349-351.
Ahmed N (2005) Advanced glycationendproducts: role in pathology of diabeticcomplications. Diabetes Research andClinical Practice. 67, 1, 3-21.
Ahroni JH, Boyko EJ (2000)Responsiveness of the SF-36 amongveterans with diabetes mellitus. Journal of Diabetes and its Complications. 14, 1, 31-39.
Armstrong D, Lavery A, Wrobel J,Vileikyte L (2008) Quality of life inhealing diabetic wounds: does the endjustify the means? Journal of Foot andAnkle Surgery. 47, 4, 278-282.
Boulton AJM (2006) The pathway toulceration: aetiopathogenesis. In Boulton AJM, Cavanagh PR, Rayman G(Eds) The Foot in Diabetes. Fourth edition.John Wiley & Sons, Chichester. 51-67.
Boyko EJ, Lipsky BA, Sandoval R et al(1989) NIDDM and the prevalence ofnasal staphylococcus aureus colonization.San Luis Valley Diabetes Study. DiabetesCare. 12, 189-192.
Bristow IR, Spruce MC (2009) Fungal foot infection, cellulitis anddiabetes: a review. Diabetes Medicine.26, 5, 548-551.
Brown CD, Ghali HS, Zhao Z, Thomas LL,Friedman EA (2005) Association of
reduced red blood cell deformability and diabetic nephropathy. KidneyInternational. 67, 1, 295-300
Davis P (2008) The immunology ofwound healing: the body as a battlefield.Wound Healing Science. 4, 4, 54-69.
Diabetes UK (2010) Diabetes in the UK2010: Key Statistics on Diabetes.www.diabetes.org.uk/Documents/Reports/Diabetes_in_the_UK_2010.pdf (Lastaccessed: June 23 2011.)
Doughty DB, Sparks-Defriese B (2007)Wound healing physiology. In Bryant RA,Nix DP (Eds) Acute and Chronic Wounds:Current Management Concepts. Mosby, St Louis MO. 56-81.
Driver VR, Landowski MA, Madsen JL(2007) Neuropathic wounds: the diabeticwound. In Bryant RA, Nix DP (Eds) Acute and Chronic Wounds: CurrentManagement Concepts. Mosby, St Louis MO. 307-336.
Dunning T (2009) Care of People withDiabetes: A Manual of Nursing Practice.Third edition. Wiley-Blackwell, Chichester.
Edmonds ME, Foster AV (2006) ABC of wound healing. Diabetic footulcers. British Medical Journal. 332, 7538, 407-410.
Falanga V (2005) Wound healing and its impairment in the diabetic foot. TheLancet. 366, 9498, 1736-1743.
Hunt TK, Pai MP (1972) The effect of variant ambient oxygen tensions on
wound metabolism and collagensynthesis. Surgery Gynaecology andObstetrics. 135, 4, 561-567.
International Working Group on theDiabetic Foot (1999) InternationalConsensus on the Diabetic Foot.International Working Group on theDiabetic Foot, Amsterdam.
Kidman K (2008) Tissue repair andregeneration: the effects of diabetes onwound healing. Diabetic Foot Journal.11, 2, 73-79.
König M, Vanscheidt W, Augustin M,Kapp H (2005) Enzymatic versusautolytic debridement of chronic legulcers: a prospective randomised trial.Journal of Wound Care. 14, 7, 320-323.
Levin ME (2002) Management of thediabetic foot: preventing amputation.Southern Medical Journal. 95, 1, 10-20.
Lioupis C (2005) Effects of diabetesmellitus on wound healing: an update.Journal of Wound Care. 14, 2, 84-86.
Lipsky BA, Berendt AR (2006)Infection of the foot in persons withdiabetes: epidemiology, pathophysiology,microbiology, clinical presentation andapproach to therapy. In The Foot inDiabetes. Fourth edition. Wiley & Sons,Chichester. 159-168.
Lobmann R, Ambrosch A, Schultz G et al (2002) Expression of matrix-metalloproteinases and theirinhibitors in the wounds of diabetic and
References
with diabetes with an increased risk of infectionand associated complication rates compared withnon-diabetic patients (Zerr et al 1997, Talbot2005). Talbot (2005) proposed that it is notsimply glycaemic control that increases the risk of surgical site infection in cardiothoracicpatients; obesity is a known surgical site infectionrisk and 90% of all patients newly diagnosed with type 2 diabetes are overweight. Carriage of Staphylococcus aureus has also been shown to increase the risk of staphylococcal surgical site
FIGURE 4
Wound infection
Hyperglycaemia is responsible for the developmentof wound infections in people with diabetes.McIntosh (2009) and Lipsky and Berendt (2006)suggested that bacteria thrive on the increasedglucose available in the bloodstream, and that at thesame time the high glucose concentration inhibitsneutrophil action, leading to a proliferation ofbacteria and infection. Cellulitis, abscesses andosteomyelitis ensue. Classic signs of infection –pain, heat, redness and swelling – are often absentor diminished. This is attributed to neuropathy andischaemia, which impair the normal inflammatoryresponse (Edmonds and Foster 2006).
Necrosis and sloughy tissue are oftenproblematic in the diabetic wound (McIntosh2006), with frequent manual debridementnecessary in all diabetic wounds (Figure 4). Thepresence of this debris in the wound bed can be a reservoir for bacteria and toxins, increasing therisk of wound infection (König et al 2005). Acutesurgical wounds are also problematic in patients
Infected foot ulcer
SCIE
NC
E PH
OTO
LIB
RAR
Y
p41-47w45_ART&SCIENCE 11/07/2011 10:51 Page 46

july 13 :: vol 25 no 45 :: 2011 47NURSING STANDARD
infections. S. aureus, considered one of the moreimportant pathogens (Lipsky and Berendt 2006),is frequently found in the nose of diabetic patients(Boyko et al 1989, Stanaway et al 2007) andtherefore increases the likelihood of surgical siteinfection (Talbot 2005). Pre-operative skinpreparation may have a role in reducing post-operative infection in these patients.
Management of diabetic wounds
People with diabetes should be encouraged tomanage their blood glucose to minimise thepotential damage that can result from raisedblood glucose levels. Providing advice on whatconstitutes a healthy diet and encouragingphysical activity are advocated to help patientscontrol blood glucose levels and minimisecomplications (Nair 2007). Smoking cessation is recommended to reduce the risk of vasculardisease, as is weight loss in people who are obese(Stumvoll et al 2005).
Management of wounds in the patient withdiabetes is frequently the responsibility of a multidisciplinary team. Patients with footulceration, because of the recognised risk ofamputation, should be referred to the specialist
non-diabetic patients. Diabetologia. 45, 7, 1011-1016.
Loot MA, Kenter SB, Au FL et al(2002) Fibroblasts derived from chronic diabetic ulcers differ in theirresponse to stimulation with ECF, IGF-I,bFGF and PDVGF-AB compared tocontrols. European Journal of Cell Biology. 81, 3, 153-60.
McIntosh C (2006) Diabetic Foot Ulcers:An Educational Booklet. Wounds UKPublishing, Aberdeen.
McIntosh C (2009) Managing diabeticfoot ulceration: review of best practice.Wound Essentials. 4, 102-111 .
Meeking D, Holland E, Land D (2006)Diabetes and foot disease. In Shaw KM,Cummings MH (Eds) Diabetes: ChronicComplications. Wiley, Chichester. 47-78.
Menke NB, Ward KR, Witten TM,Bonchev DG, Diegelmann RF (2007)Impaired wound healing. Clinics inDermatology. 25, 1, 19-25.
Morain WD, Colen LB (1990) Woundhealing in diabetes mellitus. Clinics inPlastic Surgery. 17, 3, 493-501.
Nabuurs-Franssen MH, Huijberts MS,Nieuwenhuijzen Kruseman AC,Willems J, Schaper NC (2005) Health-related quality of life of diabeticfoot ulcer patients and their caregivers.Diabetologia. 48, 9, 1906-1910.
Nair M (2007) Nursing management ofthe person with diabetes mellitus. Part 2.British Journal of Nursing. 16, 4, 232-235.
National Diabetes Support Team (2006)Diabetic Foot Guide. www.diabetes.nhs.uk/document.php?o=196 (Last accessed: June 23 2011.)
Novak M (2010) Diabetes mellitus. InNettina SM (Ed) Manual of NursingPractice. Lippincott Williams & Wilkins,Wolters Kluwer, London. 944-969.
Pound N, Chipchase S, Treece K, Game F, Jeffcoate W (2005) Ulcer freesurvival following management of footulcers in diabetes. Diabetic Medicine. 22,10, 1306-1309.
Reiber GE, Vileikyte L, Boyko EJ et al(1999) Causal pathways for incidentlower-extremity ulcers in patients withdiabetes from two settings. DiabetesCare. 22, 1, 157-162.
Shaw JE, Boulton AJM (1995) TheCharcot foot. Foot. 5, 65-70.
Shaw JE, Boulton AJM (2001) Thediabetic foot. In Beard JD, Gaines PA(eds) Vascular and Endovascular Surgery.Second edition. WB Saunders, London.105-126.
Shier D, Butler J, Lewis R (2010) Hole’sAnatomy and Physiology. Twelfth edition.McGraw-Hill, Boston MA.
Shin S, Ku Y (2005) Hemorheology andclinical application: association of
impairment of red blood cell deformabilityand diabetic nephropathy. Korea-AustraliaRheology Journal. 17, 3, 117-123.
Stadelmann WK, Digenis AG, Tobin GR(1998) Impediments to wound healing.American Journal of Surgery. 176, Suppl 2a, 39s-47s.
Stanaway S et al (2007) Methicillin-resistant Staphylococcusaureus (MRSA) isolation from diabeticfoot ulcers correlates with nasal MRSAcarriage. Diabetes Research and ClinicalPractice. 75, 1, 47-50.
Stumvoll M, Goldstein BJ, van Haeften TW (2005) Type 2diabetes: principles of pathogenesis and therapy. The Lancet. 365, 9467, 1333-1346.
Talbot TR (2005) Diabetes mellitus andcardiothoracic surgical site infections.American Journal of Infection Control. 33, 6, 353-359.
Tortora GJ, Derrickson B (2007)Introduction to the Human Body: TheEssentials of Anatomy and Physiology.Seventh edition. Wiley, New York NY.
Watret L (2005) Wound bed preparationand the diabetic foot. Diabetic Foot. 8, 1, 18-26.
Zerr KJ, Furnary AP, Grunkemeier GLet al (1997) Glucose control lowers therisk of wound infection in diabetics afteropen heart operations. Annals of ThoracicSurgery. 63, 2, 356-361.
foot team, a multidisciplinary team focusing onthe foot in diabetes (McIntosh 2006). However,any wound can potentially be a problem if thepatient has diabetes. Effective wound care is vitaland this starts with thorough assessment.
There are several wound assessment toolsavailable and they should assist the practitioner in choosing the most appropriate wound carepractices. The concept of wound bed preparation– preparing the wound bed to be in the bestpossible condition to support healing – is the basisof most modern wound care (Watret 2005).Debridement is a fundamental aspect of woundmanagement: removal of necrotic material isessential to allow healing to take place and reducethe risk of infection. Managing moisture levels in a wound can be difficult, especially if the woundis in the inflammatory stage of healing when thereis likely to be increased levels of exudate.
Conclusion
Wound healing is usually a well organised andcomplex series of events which can be impaired in the presence of a chronic illness such as diabetes.An understanding of the wound healing processand the effects of diabetes on this process areessential to promote effective wound healing NS
p41-47w45_ART&SCIENCE 11/07/2011 10:51 Page 47

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.