diabetes care: can qof miss the point? unexpected
TRANSCRIPT
82 PRACTICAL DIABETES VOL. 30 NO. 2 COPYRIGHT © 2013 JOHN WILEY & SONS
IntroductionIn 2004, the Quality and OutcomesFramework (QOF) for diabetes mel-litus introduced a points system forattainment of target HbA1c values forpatients in primary care.1 Thesepoints contribute to practice remu-neration for provision of diabetescare, and diabetes management hasimproved as a result.2 However, whilepatients with poor glycaemic controlwill be identified and offered treat-ment advice, those with unantici-pated reduction in HbA1c may not bebrought to the attention of healthcare professionals as they appear to‘meet’ QOF targets.
We present a patient with poorlycontrolled type 2 diabetes in whomAddison’s disease caused recurrenthypoglycaemia and a fall in HbA1cinto the non-diabetic range over a year. Suggestive symptoms werepresent some months prior to heremergency presentation, but a causefor the low HbA1c and hypogly-caemia had not been sought.
This case illustrates the need tobeware the patient in whom a fallingHbA1c is unexplained, and seek anunderlying cause.
Case reportA 71-year-old woman presented tothe medical assessment unit with anepisode of hypoglycaemia (capillaryblood glucose 2.6mmol/L). Shegave a two-week history of poor
appetite, vomiting and generalmalaise. On direct questioning, thepatient disclosed significant weightloss of 20kg plus recurrent hypogly-caemic episodes over the preceding12 months, despite a reduction inher gliclazide dose by her GP. Shehad attended the surgery regardingbrown discolouration of the skin onher elbows, for which no explana-tion was found. She denied recentsteroid therapy. Her past historyincluded a nine-year history of type2 diabetes, hyperlipidaemia, glau-coma and hypothyroidism. She hadrecently been referred to haematol-ogy regarding persistent lymphocy-tosis but had failed to attend.
Her treatment consisted of met-formin 850mg twice daily, gliclazide80mg once daily, levothyroxine 50µgonce daily, and dorzolamide eyedrops. She was a non-smoker anddrank little alcohol.
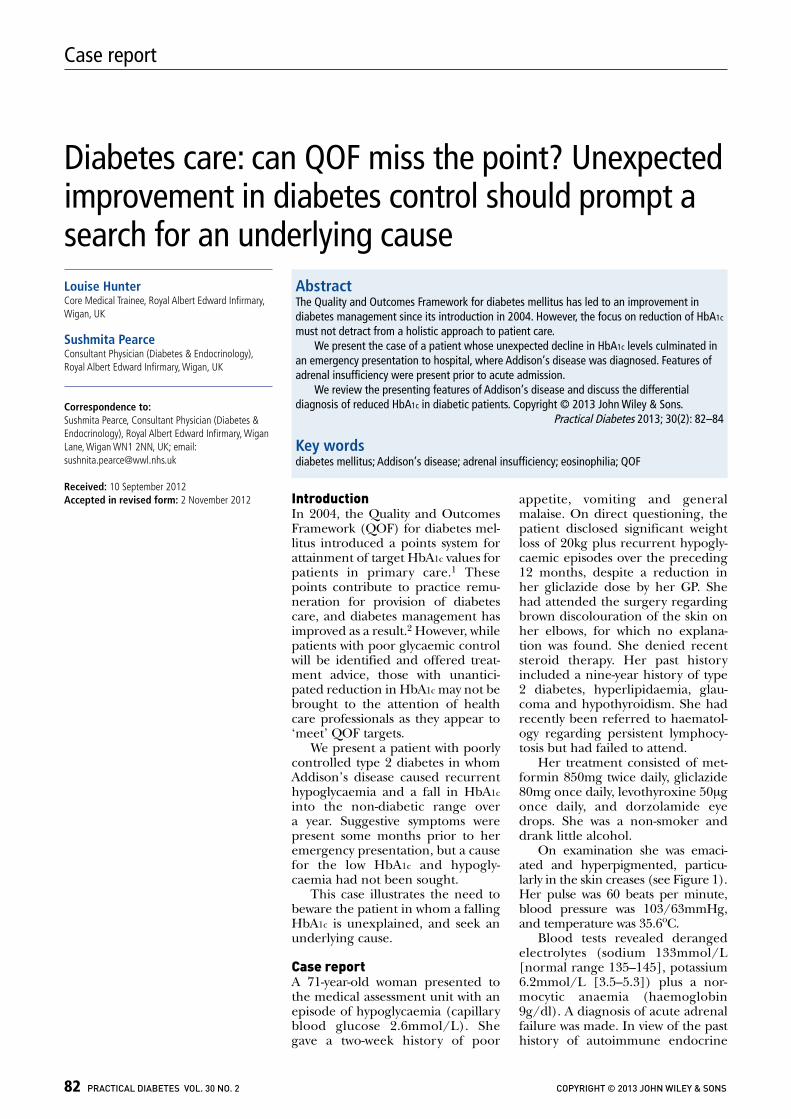
On examination she was emaci-ated and hyperpigmented, particu-larly in the skin creases (see Figure 1).Her pulse was 60 beats per minute,blood pressure was 103/63mmHg,and temperature was 35.6oC.
Blood tests revealed derangedelectrolytes (sodium 133mmol/L[normal range 135–145], potassium6.2mmol/L [3.5–5.3]) plus a nor-mocytic anaemia (haemoglobin9g/dl). A diagnosis of acute adrenalfailure was made. In view of the pasthistory of autoimmune endocrine
Case report
Diabetes care: can QOF miss the point? Unexpectedimprovement in diabetes control should prompt asearch for an underlying cause
AbstractThe Quality and Outcomes Framework for diabetes mellitus has led to an improvement indiabetes management since its introduction in 2004. However, the focus on reduction of HbA1c
must not detract from a holistic approach to patient care. We present the case of a patient whose unexpected decline in HbA1c levels culminated in
an emergency presentation to hospital, where Addison’s disease was diagnosed. Features ofadrenal insufficiency were present prior to acute admission.
We review the presenting features of Addison’s disease and discuss the differentialdiagnosis of reduced HbA1c in diabetic patients. Copyright © 2013 John Wiley & Sons.
Practical Diabetes 2013; 30(2): 82–84
Key wordsdiabetes mellitus; Addison’s disease; adrenal insufficiency; eosinophilia; QOF
Louise Hunter Core Medical Trainee, Royal Albert Edward Infirmary,Wigan, UK
Sushmita PearceConsultant Physician (Diabetes & Endocrinology),Royal Albert Edward Infirmary, Wigan, UK
Correspondence to: Sushmita Pearce, Consultant Physician (Diabetes &Endocrinology), Royal Albert Edward Infirmary, WiganLane, Wigan WN1 2NN, UK; email:[email protected]
Received: 10 September 2012Accepted in revised form: 2 November 2012
disease, Addison’s disease (primaryadrenal insufficiency) was thoughtto be the likeliest cause. Blood was taken for cortisol, adrenocorti-cotrophic hormone, and HbA1clevels followed by immediate treat-ment with intravenous saline, dex-trose, and hydrocortisone. The random cortisol level was 12nmol/L(normal range 250–650nmol/L for morning samples); ACTH was >1250ng/L (normal range<46ng/L); and HbA1c 26mmol/mol(DCCT 4.5%) – normal IFCC rangefor our hospital 20–42mmol/mol(DCCT 4–6%). CT adrenals showedbilateral small glands with no otherabnormal morphology.
The patient made excellentprogress and was duly switched tooral hydrocortisone 10mg threetimes daily, plus fludrocortisone100µg once daily. Her diabetes control deteriorated and she eventu-ally required insulin and metforminto control her diabetes. Her weightimproved by 11kg over the subse-quent five months.
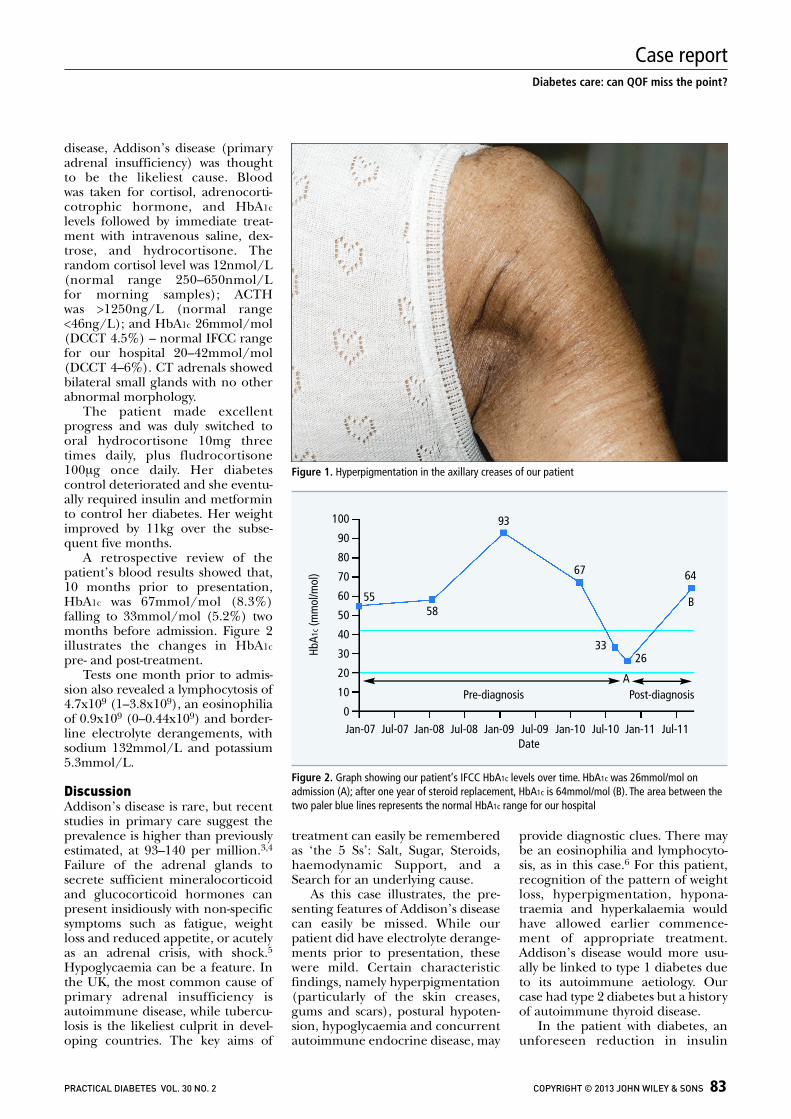
A retrospective review of thepatient’s blood results showed that,10 months prior to presentation,HbA1c was 67mmol/mol (8.3%)falling to 33mmol/mol (5.2%) twomonths before admission. Figure 2illustrates the changes in HbA1cpre- and post-treatment.
Tests one month prior to admis-sion also revealed a lymphocytosis of4.7x109 (1–3.8x109), an eosinophiliaof 0.9x109 (0–0.44x109) and border-line electrolyte derangements, withsodium 132mmol/L and potassium5.3mmol/L.
DiscussionAddison’s disease is rare, but recentstudies in primary care suggest theprevalence is higher than previouslyestimated, at 93–140 per million.3,4
Failure of the adrenal glands tosecrete sufficient mineralocorticoidand glucocorticoid hormones canpresent insidiously with non-specificsymptoms such as fatigue, weightloss and reduced appetite, or acutelyas an adrenal crisis, with shock.5Hypoglycaemia can be a feature. Inthe UK, the most common cause ofprimary adrenal insufficiency isautoimmune disease, while tubercu-losis is the likeliest culprit in devel-oping countries. The key aims of
treatment can easily be rememberedas ‘the 5 Ss’: Salt, Sugar, Steroids,haemodynamic Support, and aSearch for an underlying cause.
As this case illustrates, the pre-senting features of Addison’s diseasecan easily be missed. While ourpatient did have electrolyte derange-ments prior to presentation, thesewere mild. Certain characteristicfindings, namely hyperpigmentation(particularly of the skin creases,gums and scars), postural hypoten-sion, hypoglycaemia and concurrentautoimmune endocrine disease, may
provide diagnostic clues. There maybe an eosinophilia and lymphocyto-sis, as in this case.6 For this patient,recognition of the pattern of weightloss, hyperpigmentation, hypona-traemia and hyperkalaemia wouldhave allowed earlier commence-ment of appropriate treatment.Addison’s disease would more usu-ally be linked to type 1 diabetes dueto its autoimmune aetiology. Ourcase had type 2 diabetes but a historyof autoimmune thyroid disease.
In the patient with diabetes, anunforeseen reduction in insulin
PRACTICAL DIABETES VOL. 30 NO. 2 COPYRIGHT © 2013 JOHN WILEY & SONS 83
Diabetes care: can QOF miss the point?
Case report
Figure 1. Hyperpigmentation in the axillary creases of our patient
Figure 2. Graph showing our patient’s IFCC HbA1c levels over time. HbA1c was 26mmol/mol onadmission (A); after one year of steroid replacement, HbA1c is 64mmol/mol (B). The area between thetwo paler blue lines represents the normal HbA1c range for our hospital
HbA1
c(m
mol
/mol
)
100
90
80
70
60
50
40
30
20
10
0Pre-diagnosis Post-diagnosis
Jan-07 Jul-07 Jan-08 Jul-08 Jan-09 Jul-09 Jan-10 Jul-10 Jan-11 Jul-11Date
5558
93
67
3326
64
A
B

84 PRACTICAL DIABETES VOL. 30 NO. 2 COPYRIGHT © 2013 JOHN WILEY & SONS
Diabetes care: can QOF miss the point?
Case report
requirement or HbA1c warrantsinvestigation. Causes which shouldbe considered are listed in Table 1.While weight loss is generally recom-mended in the treatment of type 2diabetes, it is crucial to ensure thatany sudden change in weight isintentional rather than pathological.
While the QOF has undoubt-edly had a significant positive effecton diabetes care,2 a focus on reduc-ing HbA1c levels must not distract
clinicians from identifying patientsin whom unprecedented normali-sation of HbA1c belies seriouspathology. We believe that this caseserves as a reminder that assess-ment of the diabetic patientrequires a holistic approach, ofwhich biochemical parametersform only a part.
AcknowledgementSushmita Pearce is the guarantor.The patient has kindly given herwritten consent for her photographand a description of her case toappear in this work.
Declaration of interestsThere are no conflicts of interestdeclared.
References1. Quality and Outcomes Framework guidance for
GMS contract 2011/12. Delivering investment ingeneral practice. BMA, NHS Employers, April 2011.
2. Oluwatowoju I, et al. Improvements in glycaemiccontrol and cholesterol concentrations associatedwith the Quality and Outcomes Framework: aregional 2-year audit of diabetes care in the UK.Diabet Med 2010;27:354–9.
3. Willis AC, Vince FP. The prevalence of Addison’s disease in Coventry, UK. Postgrad Med J1997;73:286–8.
4. Løvås K, Husebye ES. High prevalence and increasing incidence of Addison’s disease inWestern Norway. Clin Endocrinol (Oxf)2002;56:787–91.
5. Vaidya B, et al. Addison's disease. BMJ 2009;339:b2385.
6. Burke CW. Adrenocortical insufficiency. ClinEndocrinol Metab 1985;14:947–76.
l Unintentional improvement indiabetes control or unexplainedhypoglycaemia are red-flag findingsnecessitating medical review of thepatient
l Beware the patient with type 2diabetes in whom weight loss isactually unintentional
l Addison’s disease is rare, easily missed,and can present with hypoglycaemia
l Diabetes control can be affected by amyriad of factors from social topsychological to medical, requiring abroad approach on the part of allhealth professionals
Key points• Unintentional weight loss• Medication issues (e.g. compliance, side
effect)• Adrenal insufficiency• Pituitary insufficiency• Coeliac disease, or other causes of
malabsorption• Renal failure• Liver failure• Underlying malignancy • Insulinoma (very rare)• Haemolysis/spurious
Table 1. Causes which should be considered inthe investigation of reduced HbA1c
www.practicaldiabetes.com
Online resourcePractical Diabetes has its own dedicatedwebsite www.practicaldiabetes.comwhere visitors can access articles from current and archived issues.
The website also carries additionalinformation and CPD resources. This includes:
● Specialty Certificate Examination revision exercises
● ABCD position statements
● All previously published drug notes
● Up-to-date news items
● Related articles from other journals
● Diabetes in special circumstances
● Useful links to other specialist websites