diabetes and periodontal disease ,at two way relationship
TRANSCRIPT

Diabetes and Periodontal disease A two way relationship
Contentsbull Diabetes overview
bull Periodontal disease overview
bull Relation between Diabetes and
Periodontal disease
bull effect of diabetes on periodontal disease
and its mechanism
bull Effect of periodontal disease on diabetes
and its mechanism
bull references
Introduction
bull Its widely thought that any diseases associated with each other
then one caused the other
bull But many of these diseases interrelationship mechanisms is
obscure
bull A better understanding of this relationship provides more
appropriate treatment for these patients
bull So in this seminar we will figure out the relation between
diabetes and periodontal disease and its bidirectional
mechanisms
DiabetesAmong many systemic diseases diabetes have been a nightmare
to researches doctors and patients due to its difficult control and
diverse complications
Classification
according to
its patho-
physiology
DM
Type I
IDDM
due to destruction of beta cells of
pancreas
Type II
NIDDM
due to insulin
resistance
Gestational
temporary condition
occurs during
pregnancy
others
Drug- or chemical-
induced
Diseases of the
exocrine pancreas
Genetic defects in
β-cell function insulin action
bull Actually to understand diabetes its as simple as just
increase in glucose in blood whether its due to insulin
deficiency or resistance
bull But what will result from this increase
Why is it dangerous then
bull Deficiency of insulin secretion or insulin resistance results in
Inability to transport
glucose into cells
Glucose retained in the blood stream
Hyperglycemia Complications
bull microangiopathy
bull nephropathy
bull neuropathy
bull macro vascular disease
bull delayed wound healing
- All the forms of DM are associated with hyperglycemia
hyperlipidemia and associated complications
bull The five classic major complications of diabetes
include
bull Periodontitis has been recognized as the sixth
complication associated with diabetes-Diabetes-related complications can be very serious
and even life-threatening
-So medical management is necessary to
Prevent initiation or progression of
complications
Medical management if
diabetic patients
Pharmacological
Insulin therapyOral
hypoglycemic agents
Non pharmacological
Exercise dietary control weight
loss
The best method to evaluate the glycemic control of patients is HBA1cWhere the ADA recommends a target of lt7 for individual with DM
Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Contentsbull Diabetes overview
bull Periodontal disease overview
bull Relation between Diabetes and
Periodontal disease
bull effect of diabetes on periodontal disease
and its mechanism
bull Effect of periodontal disease on diabetes
and its mechanism
bull references
Introduction
bull Its widely thought that any diseases associated with each other
then one caused the other
bull But many of these diseases interrelationship mechanisms is
obscure
bull A better understanding of this relationship provides more
appropriate treatment for these patients
bull So in this seminar we will figure out the relation between
diabetes and periodontal disease and its bidirectional
mechanisms
DiabetesAmong many systemic diseases diabetes have been a nightmare
to researches doctors and patients due to its difficult control and
diverse complications
Classification
according to
its patho-
physiology
DM
Type I
IDDM
due to destruction of beta cells of
pancreas
Type II
NIDDM
due to insulin
resistance
Gestational
temporary condition
occurs during
pregnancy
others
Drug- or chemical-
induced
Diseases of the
exocrine pancreas
Genetic defects in
β-cell function insulin action
bull Actually to understand diabetes its as simple as just
increase in glucose in blood whether its due to insulin
deficiency or resistance
bull But what will result from this increase
Why is it dangerous then
bull Deficiency of insulin secretion or insulin resistance results in
Inability to transport
glucose into cells
Glucose retained in the blood stream
Hyperglycemia Complications
bull microangiopathy
bull nephropathy
bull neuropathy
bull macro vascular disease
bull delayed wound healing
- All the forms of DM are associated with hyperglycemia
hyperlipidemia and associated complications
bull The five classic major complications of diabetes
include
bull Periodontitis has been recognized as the sixth
complication associated with diabetes-Diabetes-related complications can be very serious
and even life-threatening
-So medical management is necessary to
Prevent initiation or progression of
complications
Medical management if
diabetic patients
Pharmacological
Insulin therapyOral
hypoglycemic agents
Non pharmacological
Exercise dietary control weight
loss
The best method to evaluate the glycemic control of patients is HBA1cWhere the ADA recommends a target of lt7 for individual with DM
Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en
Introduction
bull Its widely thought that any diseases associated with each other
then one caused the other
bull But many of these diseases interrelationship mechanisms is
obscure
bull A better understanding of this relationship provides more
appropriate treatment for these patients
bull So in this seminar we will figure out the relation between
diabetes and periodontal disease and its bidirectional
mechanisms
DiabetesAmong many systemic diseases diabetes have been a nightmare
to researches doctors and patients due to its difficult control and
diverse complications
Classification
according to
its patho-
physiology
DM
Type I
IDDM
due to destruction of beta cells of
pancreas
Type II
NIDDM
due to insulin
resistance
Gestational
temporary condition
occurs during
pregnancy
others
Drug- or chemical-
induced
Diseases of the
exocrine pancreas
Genetic defects in
β-cell function insulin action
bull Actually to understand diabetes its as simple as just
increase in glucose in blood whether its due to insulin
deficiency or resistance
bull But what will result from this increase
Why is it dangerous then
bull Deficiency of insulin secretion or insulin resistance results in
Inability to transport
glucose into cells
Glucose retained in the blood stream
Hyperglycemia Complications
bull microangiopathy
bull nephropathy
bull neuropathy
bull macro vascular disease
bull delayed wound healing
- All the forms of DM are associated with hyperglycemia
hyperlipidemia and associated complications
bull The five classic major complications of diabetes
include
bull Periodontitis has been recognized as the sixth
complication associated with diabetes-Diabetes-related complications can be very serious
and even life-threatening
-So medical management is necessary to
Prevent initiation or progression of
complications
Medical management if
diabetic patients
Pharmacological
Insulin therapyOral
hypoglycemic agents
Non pharmacological
Exercise dietary control weight
loss
The best method to evaluate the glycemic control of patients is HBA1cWhere the ADA recommends a target of lt7 for individual with DM
Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

DiabetesAmong many systemic diseases diabetes have been a nightmare
to researches doctors and patients due to its difficult control and
diverse complications
Classification
according to
its patho-
physiology
DM
Type I
IDDM
due to destruction of beta cells of
pancreas
Type II
NIDDM
due to insulin
resistance
Gestational
temporary condition
occurs during
pregnancy
others
Drug- or chemical-
induced
Diseases of the
exocrine pancreas
Genetic defects in
β-cell function insulin action
bull Actually to understand diabetes its as simple as just
increase in glucose in blood whether its due to insulin
deficiency or resistance
bull But what will result from this increase
Why is it dangerous then
bull Deficiency of insulin secretion or insulin resistance results in
Inability to transport
glucose into cells
Glucose retained in the blood stream
Hyperglycemia Complications
bull microangiopathy
bull nephropathy
bull neuropathy
bull macro vascular disease
bull delayed wound healing
- All the forms of DM are associated with hyperglycemia
hyperlipidemia and associated complications
bull The five classic major complications of diabetes
include
bull Periodontitis has been recognized as the sixth
complication associated with diabetes-Diabetes-related complications can be very serious
and even life-threatening
-So medical management is necessary to
Prevent initiation or progression of
complications
Medical management if
diabetic patients
Pharmacological
Insulin therapyOral
hypoglycemic agents
Non pharmacological
Exercise dietary control weight
loss
The best method to evaluate the glycemic control of patients is HBA1cWhere the ADA recommends a target of lt7 for individual with DM
Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Classification
according to
its patho-
physiology
DM
Type I
IDDM
due to destruction of beta cells of
pancreas
Type II
NIDDM
due to insulin
resistance
Gestational
temporary condition
occurs during
pregnancy
others
Drug- or chemical-
induced
Diseases of the
exocrine pancreas
Genetic defects in
β-cell function insulin action
bull Actually to understand diabetes its as simple as just
increase in glucose in blood whether its due to insulin
deficiency or resistance
bull But what will result from this increase
Why is it dangerous then
bull Deficiency of insulin secretion or insulin resistance results in
Inability to transport
glucose into cells
Glucose retained in the blood stream
Hyperglycemia Complications
bull microangiopathy
bull nephropathy
bull neuropathy
bull macro vascular disease
bull delayed wound healing
- All the forms of DM are associated with hyperglycemia
hyperlipidemia and associated complications
bull The five classic major complications of diabetes
include
bull Periodontitis has been recognized as the sixth
complication associated with diabetes-Diabetes-related complications can be very serious
and even life-threatening
-So medical management is necessary to
Prevent initiation or progression of
complications
Medical management if
diabetic patients
Pharmacological
Insulin therapyOral
hypoglycemic agents
Non pharmacological
Exercise dietary control weight
loss
The best method to evaluate the glycemic control of patients is HBA1cWhere the ADA recommends a target of lt7 for individual with DM
Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

bull Actually to understand diabetes its as simple as just
increase in glucose in blood whether its due to insulin
deficiency or resistance
bull But what will result from this increase
Why is it dangerous then
bull Deficiency of insulin secretion or insulin resistance results in
Inability to transport
glucose into cells
Glucose retained in the blood stream
Hyperglycemia Complications
bull microangiopathy
bull nephropathy
bull neuropathy
bull macro vascular disease
bull delayed wound healing
- All the forms of DM are associated with hyperglycemia
hyperlipidemia and associated complications
bull The five classic major complications of diabetes
include
bull Periodontitis has been recognized as the sixth
complication associated with diabetes-Diabetes-related complications can be very serious
and even life-threatening
-So medical management is necessary to
Prevent initiation or progression of
complications
Medical management if
diabetic patients
Pharmacological
Insulin therapyOral
hypoglycemic agents
Non pharmacological
Exercise dietary control weight
loss
The best method to evaluate the glycemic control of patients is HBA1cWhere the ADA recommends a target of lt7 for individual with DM
Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

bull Deficiency of insulin secretion or insulin resistance results in
Inability to transport
glucose into cells
Glucose retained in the blood stream
Hyperglycemia Complications
bull microangiopathy
bull nephropathy
bull neuropathy
bull macro vascular disease
bull delayed wound healing
- All the forms of DM are associated with hyperglycemia
hyperlipidemia and associated complications
bull The five classic major complications of diabetes
include
bull Periodontitis has been recognized as the sixth
complication associated with diabetes-Diabetes-related complications can be very serious
and even life-threatening
-So medical management is necessary to
Prevent initiation or progression of
complications
Medical management if
diabetic patients
Pharmacological
Insulin therapyOral
hypoglycemic agents
Non pharmacological
Exercise dietary control weight
loss
The best method to evaluate the glycemic control of patients is HBA1cWhere the ADA recommends a target of lt7 for individual with DM
Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

bull microangiopathy
bull nephropathy
bull neuropathy
bull macro vascular disease
bull delayed wound healing
- All the forms of DM are associated with hyperglycemia
hyperlipidemia and associated complications
bull The five classic major complications of diabetes
include
bull Periodontitis has been recognized as the sixth
complication associated with diabetes-Diabetes-related complications can be very serious
and even life-threatening
-So medical management is necessary to
Prevent initiation or progression of
complications
Medical management if
diabetic patients
Pharmacological
Insulin therapyOral
hypoglycemic agents
Non pharmacological
Exercise dietary control weight
loss
The best method to evaluate the glycemic control of patients is HBA1cWhere the ADA recommends a target of lt7 for individual with DM
Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Medical management if
diabetic patients
Pharmacological
Insulin therapyOral
hypoglycemic agents
Non pharmacological
Exercise dietary control weight
loss
The best method to evaluate the glycemic control of patients is HBA1cWhere the ADA recommends a target of lt7 for individual with DM
Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Oral complications of DM
XEROSTOMIA
Candidiasis
Burning mouth
syndrome
Dental caries
Periodontal disease
Oral mucosal diseases
Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Periodontal disease
bull Definition
PD is a chronic bacterial
infection that affects both the
gingiva and the bone that
supports the teeth and is
caused by anaerobic Gram-
negative microorganisms that
are present in the bacterial
plaque that adheres to the
teeth
bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

bull Periodontal diseases include
- gingivitis (in which the inflammation is confined to
the gingiva and is reversible with good oral hygiene)
- periodontitis (in which the inflammation extends and
results in tissue destruction and alveolar bone
resorption)
bull As a whole periodontal diseases can be found in over
90 of people
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en
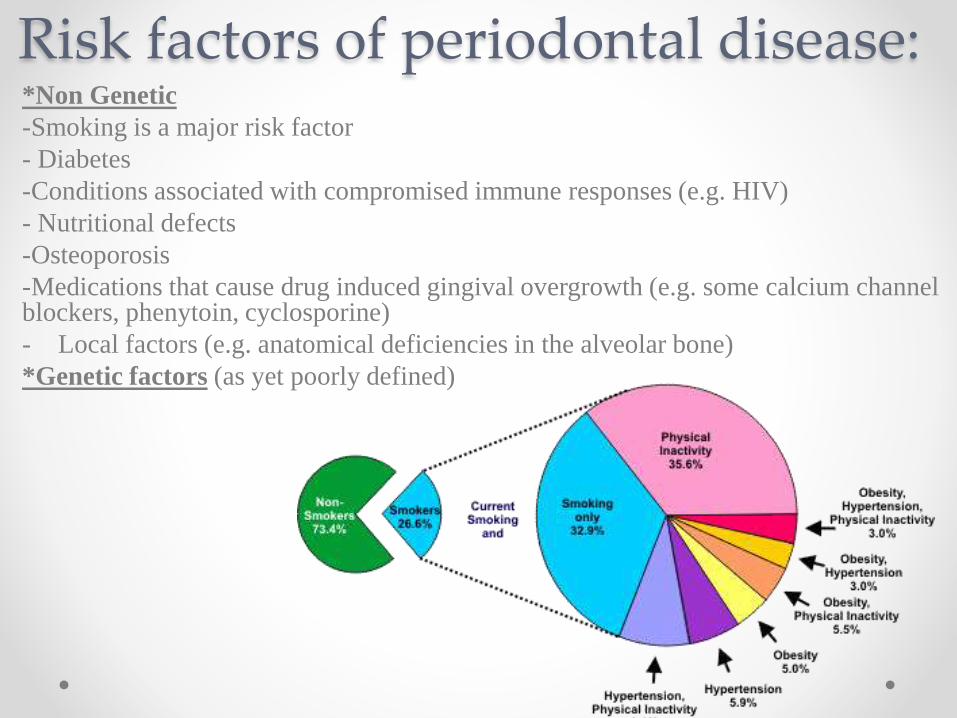
Risk factors of periodontal diseaseNon Genetic
-Smoking is a major risk factor
- Diabetes
-Conditions associated with compromised immune responses (eg HIV)
- Nutritional defects
-Osteoporosis
-Medications that cause drug induced gingival overgrowth (eg some calcium channel blockers phenytoin cyclosporine)
- Local factors (eg anatomical deficiencies in the alveolar bone)
Genetic factors (as yet poorly defined)
Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Epidemiologybull severe periodontitis that threatens tooth retention affecting 10ndash
15 of adults
bull Moderate periodontitis is even more common affecting 40ndash
60 of adults
bull Periodontitis is therefore a highly prevalent but largely hidden
chronic inflammatory disease Furthermore it has negative and
profound impacts on many aspects of daily living and quality of
life affecting confidence social interactions and food choices
PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

PathogenesisMicrobial plaque
Microbial enzymes waste products bacterial antigens
Release of pro-inflammatory cytokines and other chemical mediators by epithelial and dendritic cells
Inflammatory response in gingival tissue
Gingival edema due to fluid accumulation and cell infiltration
Production of degrading enzymes (MMP-8) by inflammatory cells causing CT destruction
Breakdown of junctional epithelium contact tooth is lost pocket is formed
Pocket favors more colonization of facultative and anaerobic micro-organisms
More immune response tissue destruction bone resorption
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en
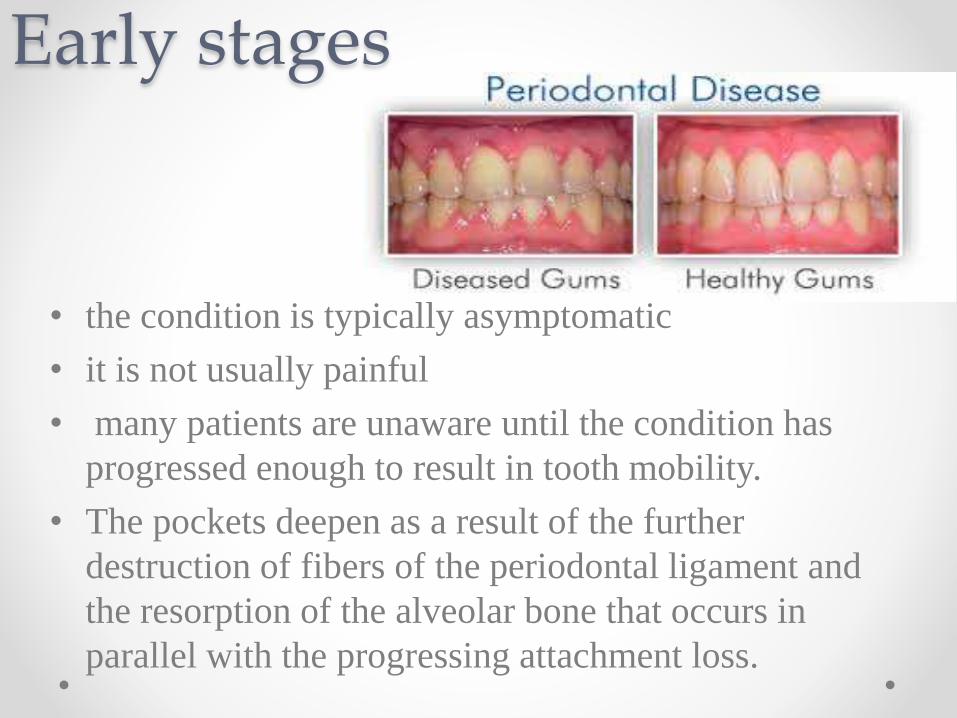
Early stages
bull the condition is typically asymptomatic
bull it is not usually painful
bull many patients are unaware until the condition has
progressed enough to result in tooth mobility
bull The pockets deepen as a result of the further
destruction of fibers of the periodontal ligament and
the resorption of the alveolar bone that occurs in
parallel with the progressing attachment loss
Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Advanced periodontitis
bull Characterized by
- gingival erythema and edema
- gingival bleeding
- gingival recession
- tooth mobility drifting of teeth
- suppuration from periodontal pockets
- tooth loss
bull The pocket is the space between the root surface and the gingiva
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en
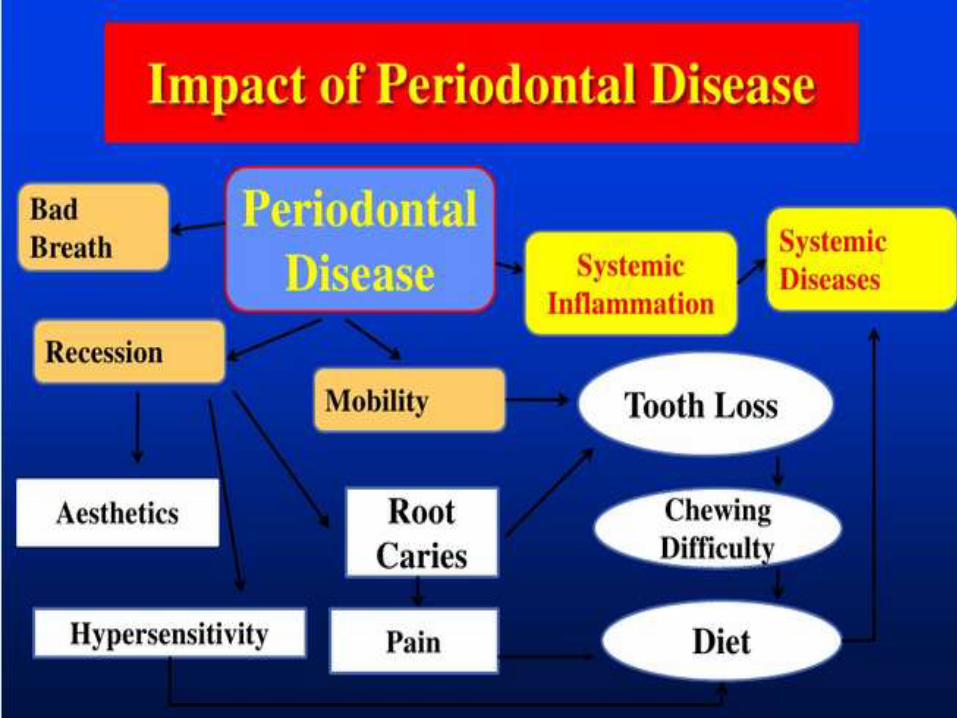
Relation to Diabetesbull Its Considered the sixth complication of
diabetes
bull More likely to occur in diabetic patients
bull Poorly controlled diabetics are more likely to develop periodontal disease than well-controlled diabetics
bull bull Poorly controlled diabetics had three foldincreases in risk of having periodontitis compared to non-diabetics
bull The duration of having diabetes is an important factor to evaluate the risk for development of periodontal disease
Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Effect of diabetes on periodontium
bull The fact that poor periodontal outcomes result from hyperglycemia in diabetes has been recognized for a long time
bull This is due to change in
Micro-organisms
Host response
Blood vessels
Wound healing
1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

1-Change in oral Microorganisms
So increase the susceptibility of diabetics to periodontal disease
2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

2-Change in Host Response differences in the immunoinflammatory response to bacteria
between people with diabetes and those without diabetes
1 The function of cells including neutrophils monocytes and
macrophages is altered in many people with diabetes
The adherence chemotaxis and phagocytosis of neutrophils are often impaired so it prevents destruction of
bacteria in the periodontal pocket thereby increasing periodontal
destruction
2-Other immune inflammatory responses are up regulated in people with diabetes
For example macrophages and monocytes often exhibit elevated production of pro -inflammatory cytokines and mediators
such as (TNF-α) in the blood and gingival crevicular fluid in response to PDL
pathogens which may increase host tissue destruction suggesting both a local and
systemic hyper responsiveness of this immune cell line
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en
a)The primary reparative cell in the periodontium the fibroblast does not function properly in high-glucose environments
b)Furthermore the collagen that is produced by these fibroblasts is susceptible to rapid degradation by matrix metalloproteinase enzymes which are elevated in diabetes
Thus periodontal wound healing responses to chronic microbial insult may be altered in those with sustained hyperglycemia resulting in increased bone loss and attachment loss
3-Altered wound healing
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en
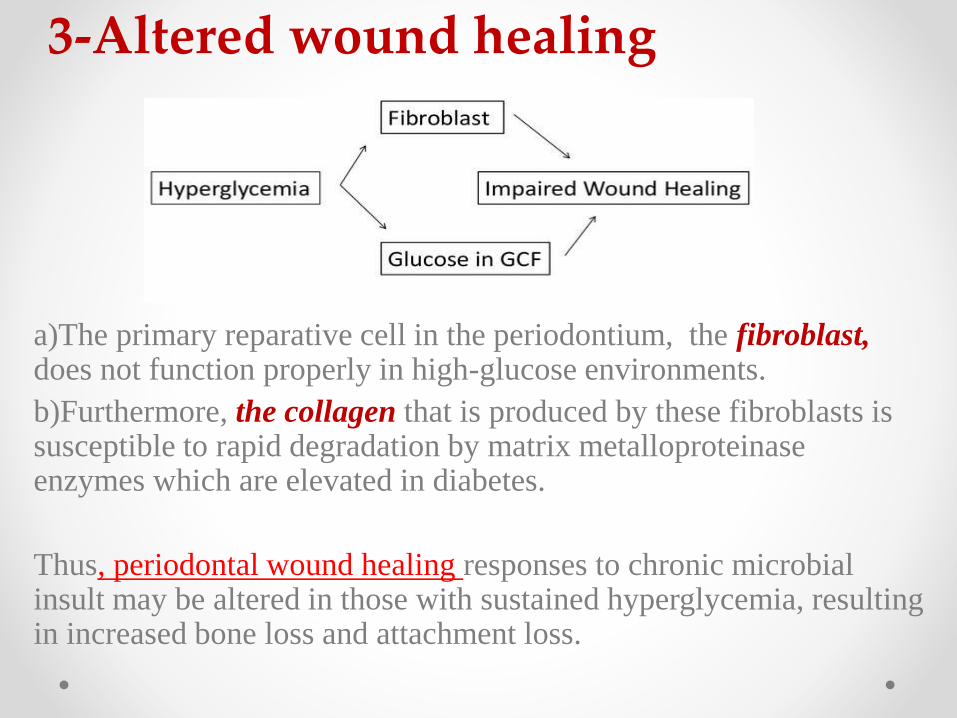
Diabetics with poor glycemic control have accumulated high levels of
irreversibly glycated proteins called advanced glycation end products
(AGEs) in the tissues including the periodontium
AGEs are a primary link between numerous diabetic complications because
a) they induce marked changes in cells and extracellular matrix
components including abnormal endothelial cell function capillary
growth and vessel proliferation also occur in the periodontium of some
people with diabetes
b) Interactions between AGEs and their receptors on inflammatory cells
result in the increased production of pro-inflammatory cytokines such as IL-
1 α and TNF- α seen in subjects with diabetes compared with those without
diabetes and it may contribute to the increased prevalence and severity of
periodontal diseases found in numerous studies of populations of people with
diabetes
4Change in microvascular integrity
HyperglycemiaNon enzymatic
glucose metabolism
Advance glycation end
products
(AGE`s)
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en
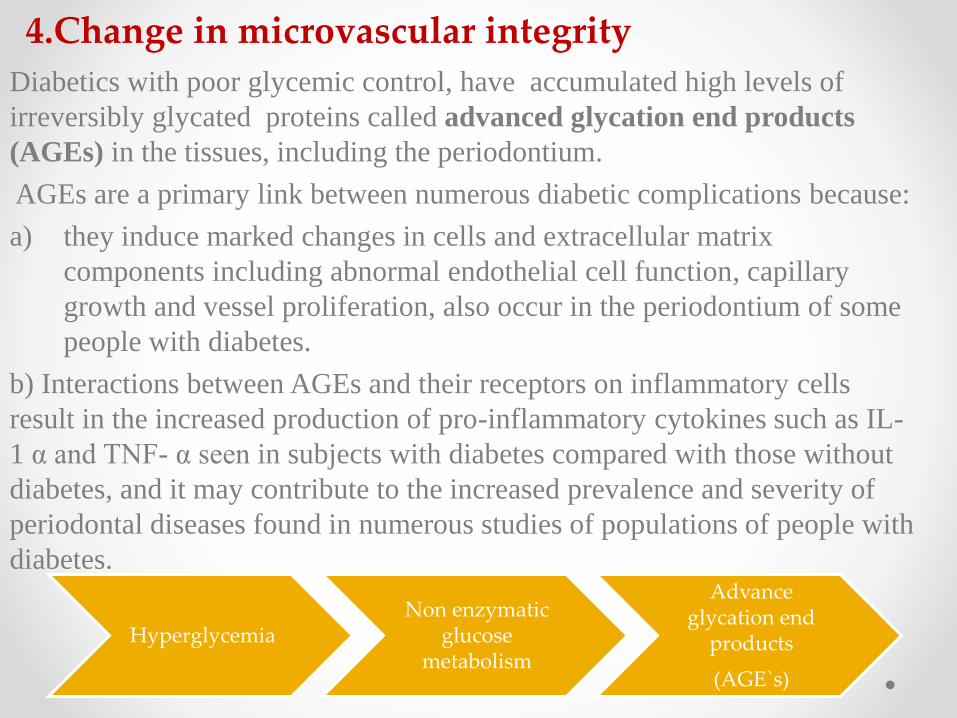
Effect of periodontitis on diabetes bull Inflammation is a common link between periodontal diseases and
diabetes
bull In patients with diabetes hyper inflammatory immune cells can
exacerbate the elevated production of proinflammatory cytokines This
has the potential to increase insulin resistance and make it more difficult
for the patient to control his or her diabetes
bull periodontal treatment that decreases inflammation may help diminish
insulin resistance
bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

bull In a recent study of subjects with type 2 diabetes and periodontitis it
was found that periodontal treatment resulted in a significant reduction
in serum levels of TNF-α that was accompanied by a significant
reduction in mean HbA1c values (from 80 to 71 percent)
bull The improvement in HbA1c values was correlated strongly with the
reduction in serum TNF-α levels across the patient population This
suggests that a reduction in periodontal inflammation may help
decrease inflammatory mediators in the serum that are associated with
insulin resistance thereby improving glycemic control
CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

CONCLUSION
The relationship between diabetes and periodontitis
bull The severity of periodontitis was significantly higher in
diabetic patients compared to non- diabetic patients
bull this bidirectional relationship between periodontal disease and
diabetes mellitus makes diabetes a disorder of importance to
dentists and dental hygienists and to patients seen in the dental
office
bull Diabetes is associated with an increased risk of developing
inflammatory periodontal diseases and glycemic control is
an important determinant in this relationship
Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Any Questions
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en
Made by Lobna Muhammad Ihab Ghada AbdelMohsen Karma NabeelFatma Mahmoud Mayan Sayed
Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en

Resources-Paper on PubMed1ldquoTreating periodontal disease may improve metabolic control in diabeticsrdquo(2010)Vergnes JN11Department of Dentistry Toulouse University Hospital (CHU de Toulouse) and Toulouse Dental School Paul Sabatier University Toulouse FrancePaper link httpwwwncbinlmnihgovpubmed20938470
2- The effects of periodontal treatment on diabetes(Oct 2003)Taylor GW11Department of Cariology Restorative Sciences and Endodontics The University of Michigan School of Dentistry Ann Arbor 48109-1078 USA gwtumicheduPaper link httpwwwncbinlmnihgovpubmed18196672
3-Treatment of periodontal disease for glycemic control in people with diabetes( may 2010)Simpson TC1 Needleman I Wild SH Moles DR Mills EJ
1Edinburgh Dental Institute University of Edinburgh Lauriston Place Edinburgh Scotland UK EH3 8HAPaper link httpwwwncbinlmnihgovpubmed20464734
4- Oral DiseasesVolume 14 Issue 3 pages 191ndash203 April 2008by Taylor GW1 Borgnakke WS
1School of Dentistry University of Michigan Ann Arbor MI 48109 USA gwtumichedu
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en
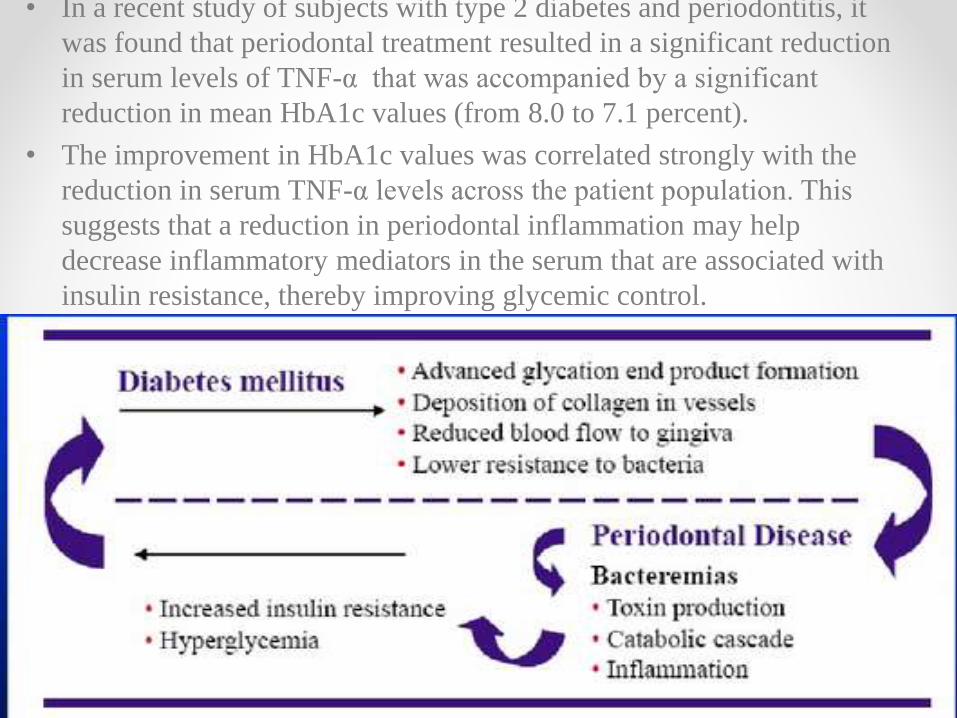
5 -Periodontal disease and diabetesA two-way streetBrian L Mealey DDS MSLink httpwwwadaorg~mediaADAMember20CenterFIlesPerio_diabetesashx
6 -Periodontitis and Diabetes Mellitus (Nov 2012)Michal Straka1 and Michaela Straka-Trapezanlidis2
1] Slovak Medical University Bratislava Slovakia[2] Private Practice Krizna 44 Bratislava SlovakiaLink httpwwwintechopencombookspathophysiology-and-complications-of-diabetes-mellitusperiodontitis-and-diabetes-mellitus
7 -Periodontal disease and systemic complications (2012)
Rui Vicente OppermannI Patricia WeidlichI Marta Liliana MusskopfII
department of Periodontology School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Brazil IIGraduate Program in Dentistry School of Dentistry Univ Federal do Rio Grande do Sul - UFRGS Porto Alegre RS Link httpwwwscielobrscielophpscript=sci_arttextamppid=S1806-83242012000700007amplng=enampnrm=isoamptlng=en