diabetes and its cardiovascular impact dr rashid iqbal consultant cardiologist surrey and sussex...
Post on 19-Dec-2015
223 views
TRANSCRIPT
Diabetes and its Cardiovascular Diabetes and its Cardiovascular ImpactImpact
Dr Rashid IqbalDr Rashid Iqbal
Consultant CardiologistConsultant Cardiologist
Surrey and Sussex Healthcare NHS TurstSurrey and Sussex Healthcare NHS Turst
St Georges Hospitals NHS TrustSt Georges Hospitals NHS Trust
AimsAims
Epidemiology of DM Epidemiology of DM
Coronary Artery Disease in DiabetesCoronary Artery Disease in Diabetes
How to protect Diabetic Heart?How to protect Diabetic Heart?
Diabetes Prevalence WorldwideDiabetes Prevalence Worldwide
In 2000 2.8% (171 million)In 2000 2.8% (171 million)
By 2030 4.4% (366 million)By 2030 4.4% (366 million)
A 36 % increase in 30 yearsA 36 % increase in 30 years
Wild S et al Diabetes Care 2004;27:1047-53
0
1995 2000 2005 2010 2015 2020 2025 2030
100
150
300
350
50
200
250
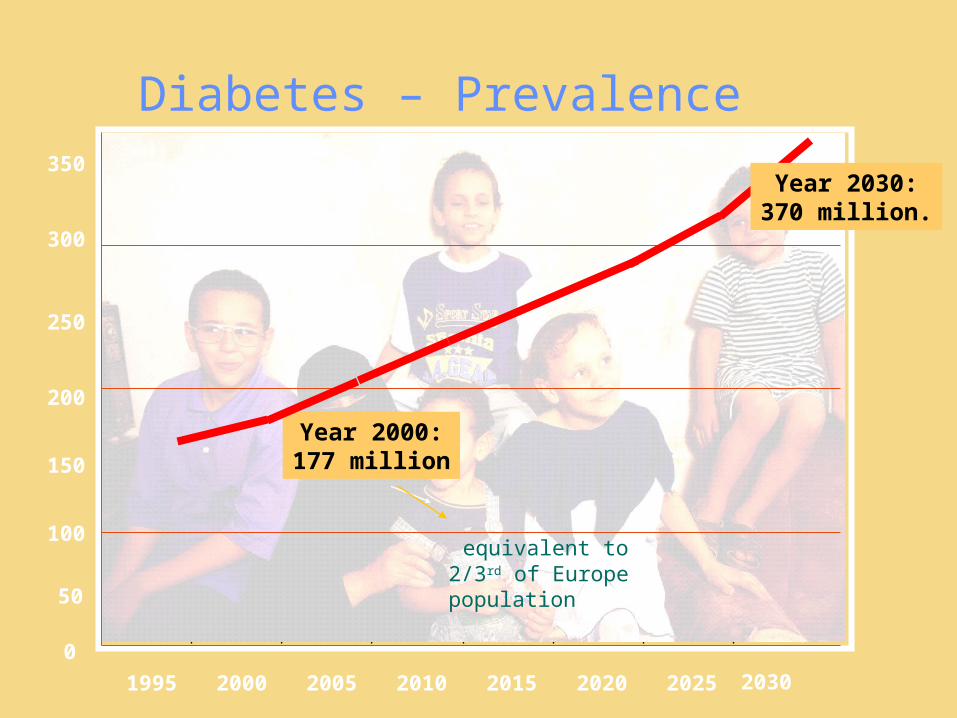
Diabetes – Prevalence
Year 2000:177 million
Year 2030:370 million.
equivalent to 2/3rd of Europe population
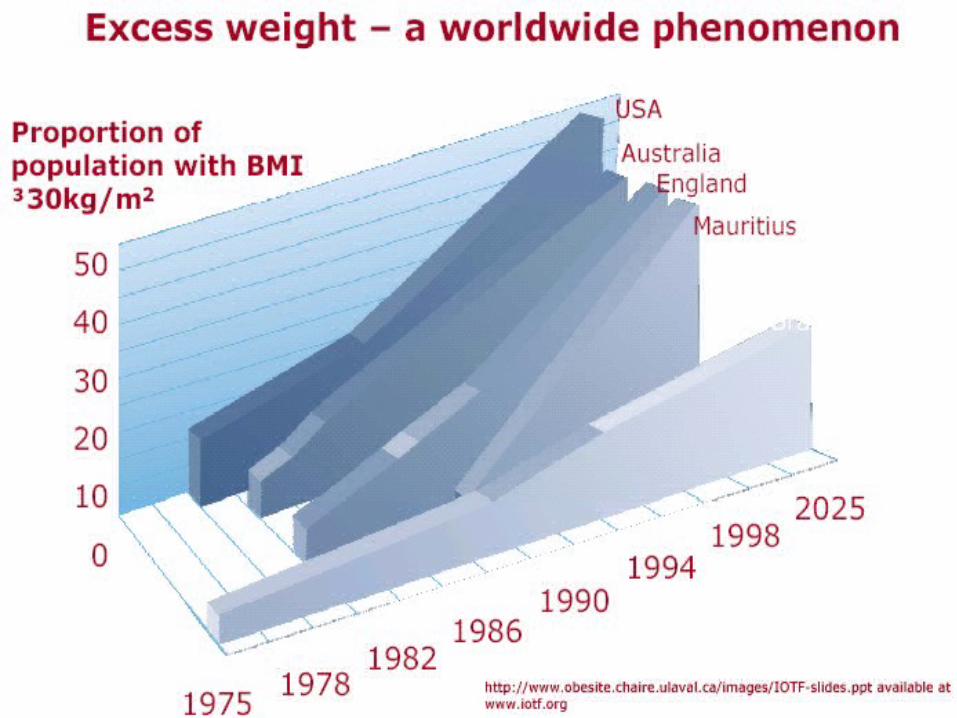
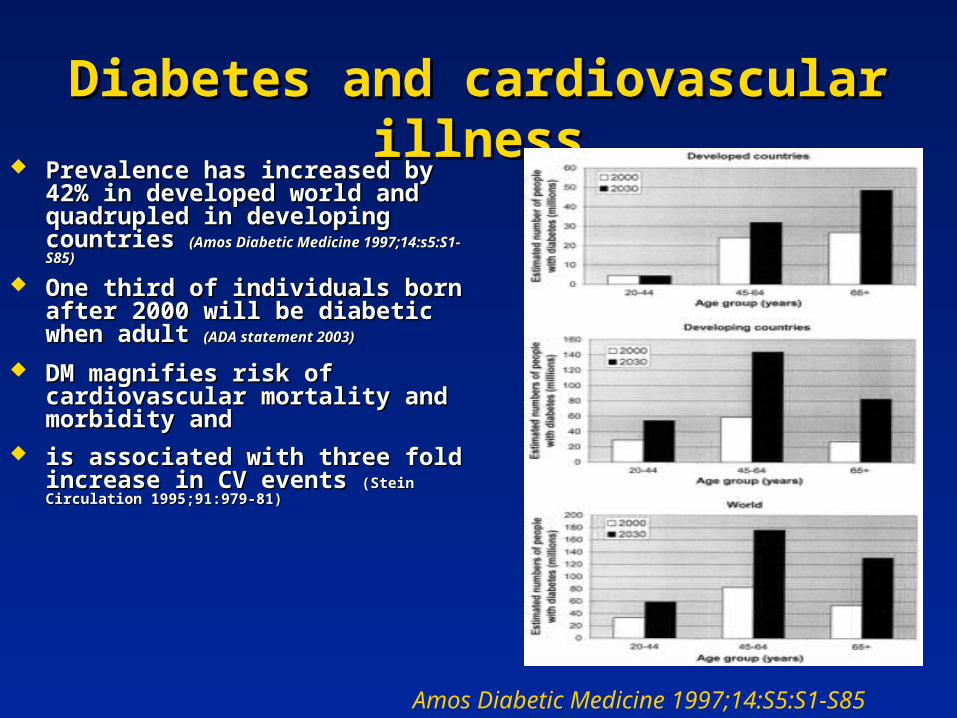
Diabetes and cardiovascular illnessDiabetes and cardiovascular illness Prevalence has increased by 42% in Prevalence has increased by 42% in
developed world and quadrupled in developed world and quadrupled in developing countries developing countries (Amos Diabetic Medicine (Amos Diabetic Medicine 1997;14:s5:S1-S85)1997;14:s5:S1-S85)
One third of individuals born after One third of individuals born after 2000 will be diabetic when adult 2000 will be diabetic when adult (ADA (ADA statement 2003)statement 2003)
DM magnifies risk of cardiovascular DM magnifies risk of cardiovascular mortality and morbidity andmortality and morbidity and
is associated with three fold increase is associated with three fold increase in CV events in CV events (Stein Circulation 1995;91:979-81)(Stein Circulation 1995;91:979-81)
Amos Diabetic Medicine 1997;14:S5:S1-S85

Obesity and type 2 diabetesObesity and type 2 diabetes
0
50
100
<22 23-23.9
25-26.9
29-30.9
>35
Body Mass Index
Age
adj
uste
d R
elat
ive
Ris
k of
D
iabe
tes
MenWomen
Chan et al (1994) and Colditz et al (1995)
Insulin Resistance and the Metabolic Insulin Resistance and the Metabolic SyndromeSyndrome
Insulin ResistanceInsulin Resistance
Resistance to the action of insulin occurring in the Resistance to the action of insulin occurring in the adipocyte, skeletal muscle and the liveradipocyte, skeletal muscle and the liver
Metabolic SyndromeMetabolic Syndrome
Insulin Resistance plus clustering of inflammatory Insulin Resistance plus clustering of inflammatory atherothrombotic cardiovascular riskatherothrombotic cardiovascular risk
Type 2 DiabetesType 2 Diabetes
Metabolic Syndrome plus dysglycaemiaMetabolic Syndrome plus dysglycaemia
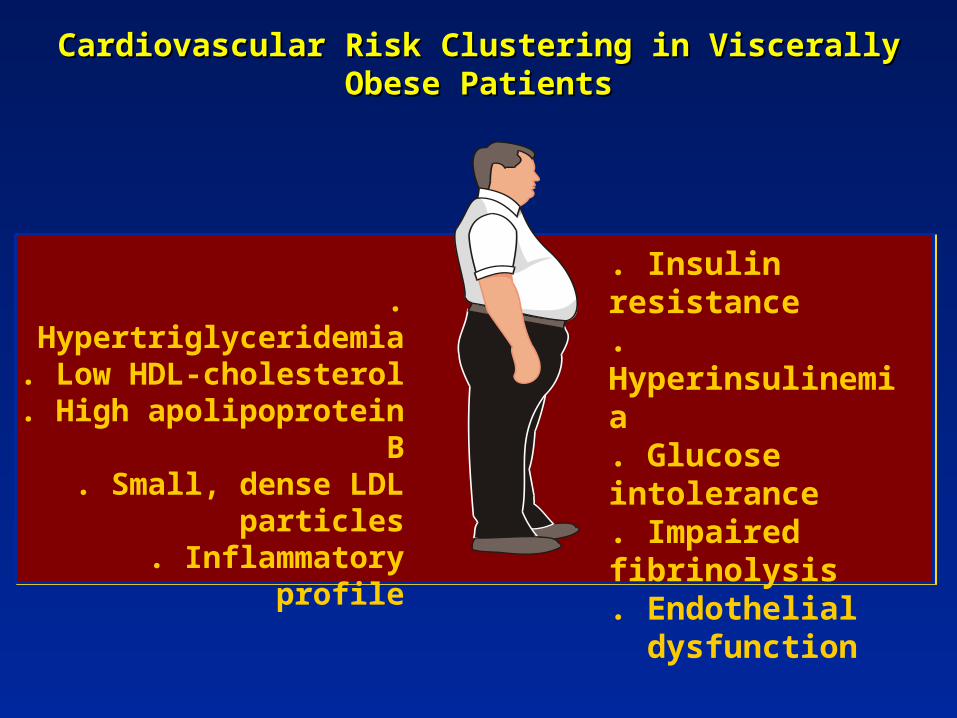
Cardiovascular Risk Clustering in Viscerally Obese PatientsCardiovascular Risk Clustering in Viscerally Obese Patients
. Hypertriglyceridemia
. Low HDL-cholesterol. High apolipoprotein B
. Small, dense LDL particles
. Inflammatory profile
. Insulin resistance
. Hyperinsulinemia
. Glucose intolerance. Impaired fibrinolysis. Endothelial dysfunction
Costs - Fact FileCosts - Fact File
Studies have shown that diabetes is a Studies have shown that diabetes is a costly disease costly disease
Type 2 diabetes accounted for between 3% Type 2 diabetes accounted for between 3% and 6% of total healthcare expenditure in and 6% of total healthcare expenditure in eight European countrieseight European countries
Hospital in-patient costs are the largest Hospital in-patient costs are the largest single contributor to direct healthcare costs single contributor to direct healthcare costs
Coronary heart disease and diabetesCoronary heart disease and diabetes
Studied using Studied using
– epidemiology
– post-mortem
– electrocardiography
– Angiography
High prevalence of subclinical atherosclerosisHigh prevalence of subclinical atherosclerosis
CAD more prevalent, more extensive, more diffuse, CAD more prevalent, more extensive, more diffuse, increased calcificationincreased calcification
High prevalence of Lt. Main disease, less collaterals High prevalence of Lt. Main disease, less collaterals
High prevalence of ‘silent ischemia’High prevalence of ‘silent ischemia’
Copyright © 2008 Society for Heart Attack Prevention and Eradication. All Rights Reserved.
12
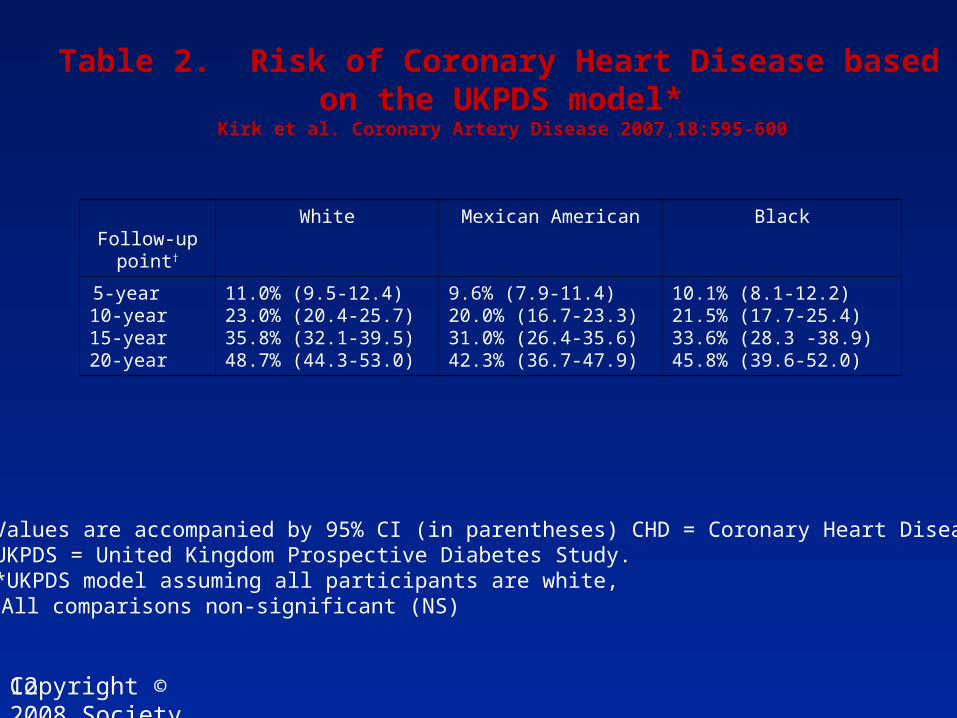
Table 2. Risk of Coronary Heart Disease based on the UKPDS model*
Kirk et al. Coronary Artery Disease 2007,18:595-600
Follow-up point†
White Mexican American Black
5-year10-year15-year20-year
11.0% (9.5-12.4)23.0% (20.4-25.7)35.8% (32.1-39.5)48.7% (44.3-53.0)
9.6% (7.9-11.4)20.0% (16.7-23.3)31.0% (26.4-35.6)42.3% (36.7-47.9)
10.1% (8.1-12.2)21.5% (17.7-25.4)33.6% (28.3 -38.9)45.8% (39.6-52.0)
Values are accompanied by 95% CI (in parentheses) CHD = Coronary Heart Disease, UKPDS = United Kingdom Prospective Diabetes Study.*UKPDS model assuming all participants are white, †All comparisons non-significant (NS)
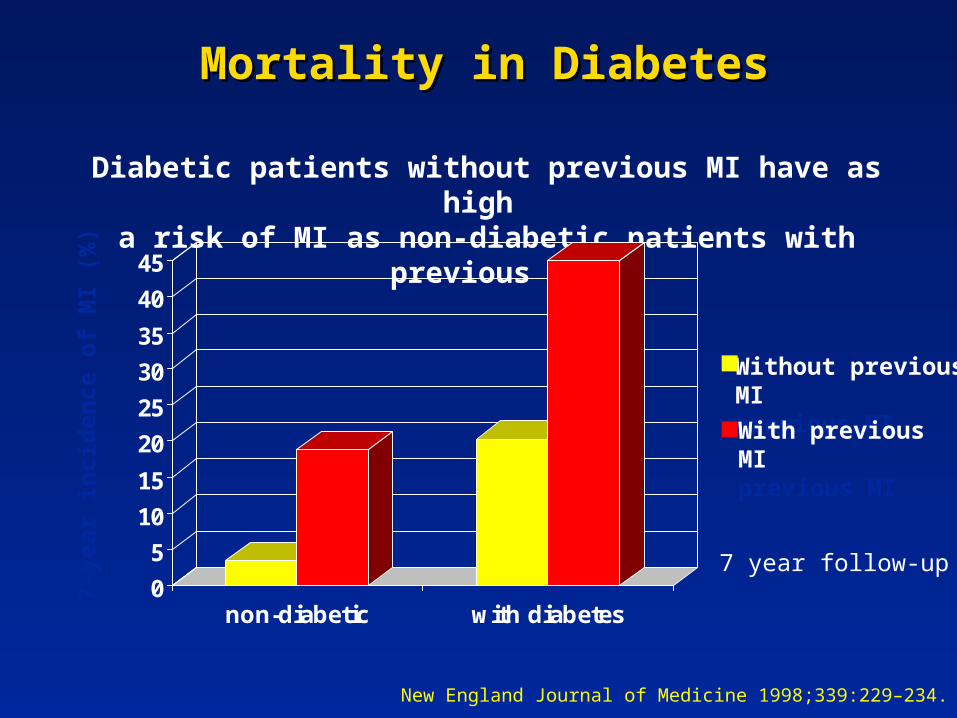
Mortality in DiabetesMortality in Diabetes
Diabetic patients without previous MI have as high a risk of MI as non-diabetic patients with previous MI
New England Journal of Medicine 1998;339:229–234.
Without previousMI previous MIWith previousMIprevious MI
7-ye
ar i
nci
den
ce o
f M
I (%
)
0
5
10
15
20
25
30
35
40
45
non-diabetic with diabetes
7 year follow-up
Diabetes-CVD Facts
More than 65% of all deaths in people with diabetes are caused by cardiovascular disease.
Heart attacks occur at an earlier age in people with diabetes and often result in premature death.
3
Diabetes-CVD Facts
Up to 60% of adults with diabetes have high blood pressure.
Nearly all adults with diabetes have one or more cholesterol problems, such as:
– high triglycerides
– low HDL (“good”) cholesterol
– high LDL (“bad”) cholesterol
4
The Good News…
By managing the ABCs of diabetes, people with diabetes can reduce their risk for heart disease and stroke.
A stands for A1C
B stands for Blood pressure
C stands for Cholesterol
5
Ask About Your A1C
A1C measures average blood glucose over the last three months.
Get your A1C checked at least twice a year.
A1C Goal = less than 7%
6
Treating Cardiovascular risk factors… Treating Cardiovascular risk factors…
Managing the ABCs of diabetes, people Managing the ABCs of diabetes, people with diabetes can reduce their risk for with diabetes can reduce their risk for heart disease and stroke.heart disease and stroke.
A stands for A1C
B stands for Blood pressure
C stands for Cholesterol
5
HbAHbA1c1c% 7.0% versus 7.9%% 7.0% versus 7.9%
Reduction in risk by:
25% for eye disease and early kidney disease
16% for Heart Attacks
24% for cataract surgery
Reduction in risk by:
25% for eye disease and early kidney disease
16% for Heart Attacks
24% for cataract surgery
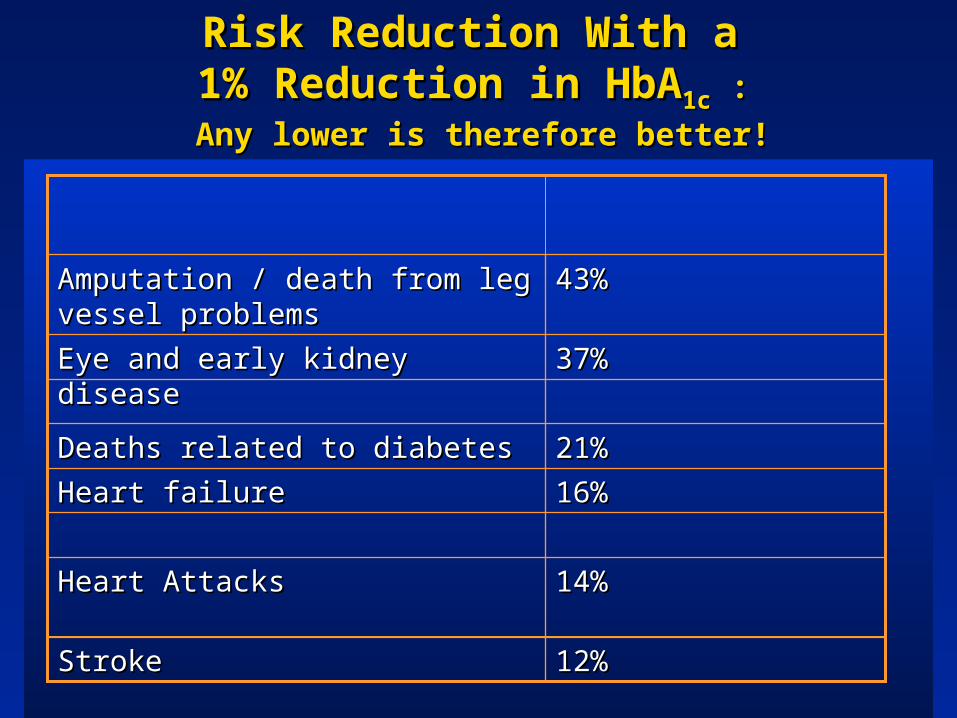
Risk Reduction With a Risk Reduction With a 1% Reduction in HbA1% Reduction in HbA1c1c : :
Any lower is therefore better!Any lower is therefore better!
16%16%Heart failureHeart failure
43%43%Amputation / death from leg vessel Amputation / death from leg vessel problemsproblems
37%37%Eye and early kidney diseaseEye and early kidney disease
12%12%StrokeStroke
14%14%Heart AttacksHeart Attacks
21%21%Deaths related to diabetesDeaths related to diabetes
Pharmacotherapy of HypertensionPharmacotherapy of Hypertension
Aim for 125/75-80Aim for 125/75-80
ACE inhibitors and ARBs have a favorable effectACE inhibitors and ARBs have a favorable effect
on renal and cardiovascular systems.on renal and cardiovascular systems.
ß-blockers along with ACE inhibitorsß-blockers along with ACE inhibitors help in help in reducingreducing myocardial infarction and heart failure.myocardial infarction and heart failure.
Calcium channel blockers in combination with ACE Calcium channel blockers in combination with ACE inhibitors, ß-blockers,inhibitors, ß-blockers, and diuretics help in and diuretics help in controlling blood pressure.controlling blood pressure.
Diuretics are recommended when BP control is Diuretics are recommended when BP control is still uncontrolled.still uncontrolled.
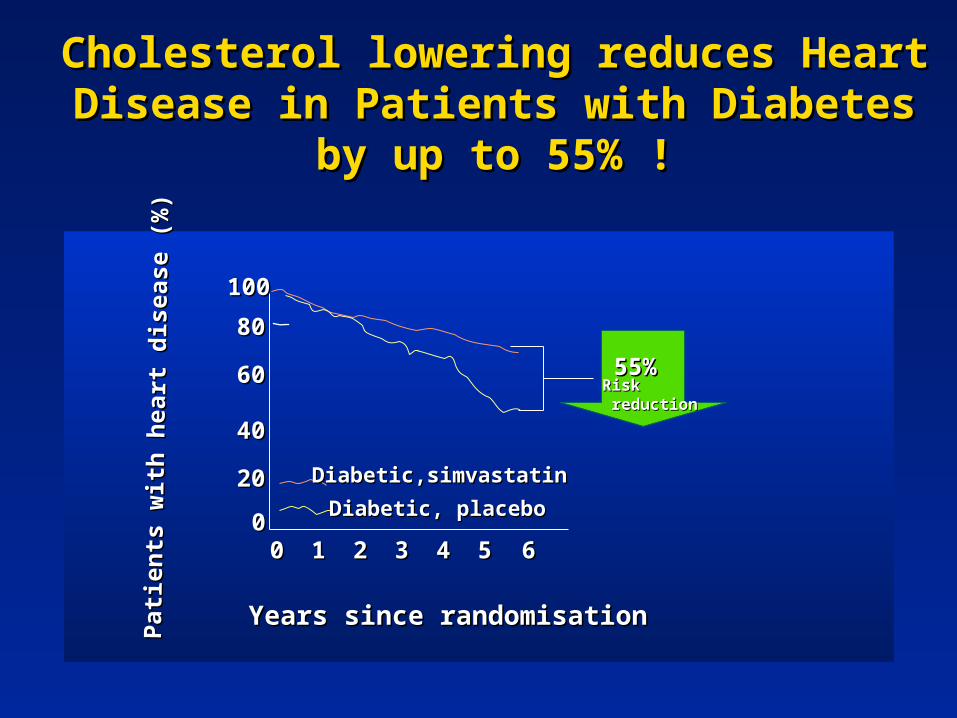
Cholesterol lowering reduces Heart Disease Cholesterol lowering reduces Heart Disease in Patients with Diabetes by up to 55% !in Patients with Diabetes by up to 55% !
11 22 33 44 55 660000
2020
4040
6060
8080
100100
RiskRisk reductionreduction
55%55%
Diabetic,simvastatin Diabetic,simvastatin
Diabetic, placebo Diabetic, placebo
Years since randomisationYears since randomisation
Pat
ien
ts w
ith
hea
rt d
isea
se (
%)
Pat
ien
ts w
ith
hea
rt d
isea
se (
%)
Multiple aetiology of atherosclerosis generationMultiple aetiology of atherosclerosis generation
increased inflammatory markersincreased inflammatory markers
hyperglycaemia induced endothelial dysfunctionhyperglycaemia induced endothelial dysfunction
increased vascular permeabilityincreased vascular permeability
adventitial inflammation (of vasa vasorum)adventitial inflammation (of vasa vasorum)
impaired fibrinolysisimpaired fibrinolysis
dysfunctional arterial remodellingdysfunctional arterial remodelling
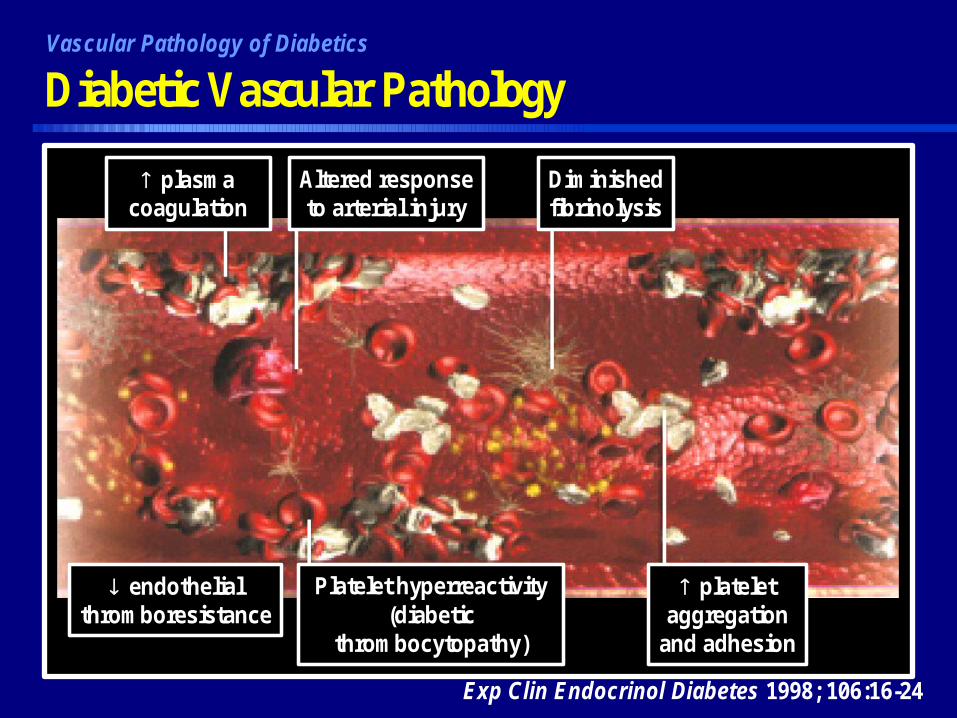
vDiabetic Vascular PathologyVascular Pathology of Diabetics
Exp Clin Endocrinol Diabetes 1998; 106:16-24
plasmacoagulation
Altered responseto arterial injury
Diminishedfibrinolysis
endothelialthromboresistance
Platelet hyperreactivity(diabetic
thrombocytopathy)
plateletaggregation
and adhesion
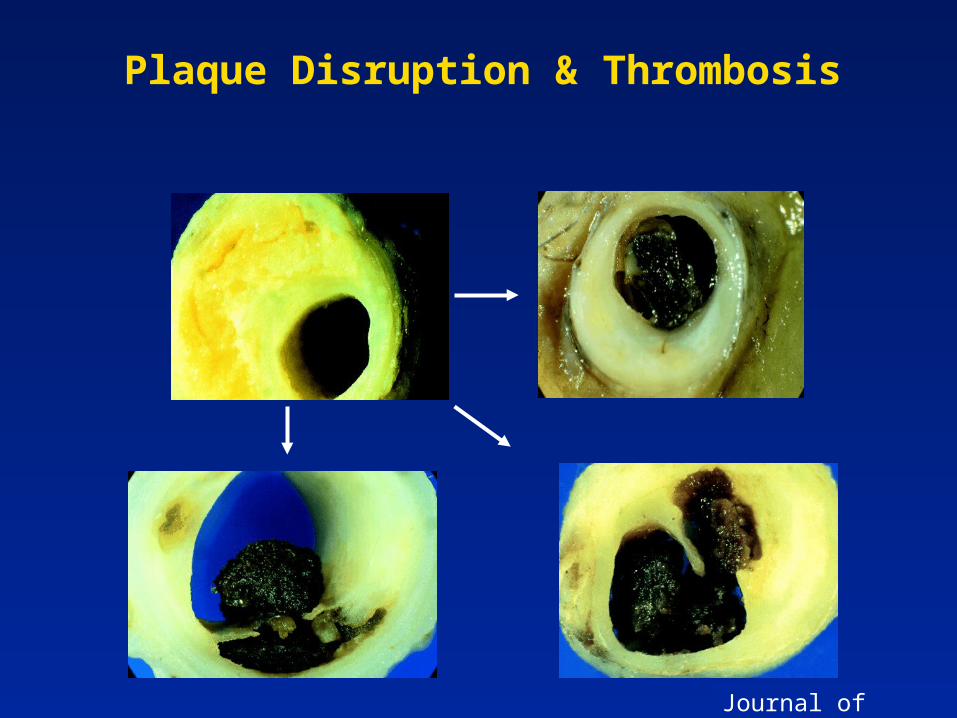
Plaque Disruption & Thrombosis
Journal of medicine
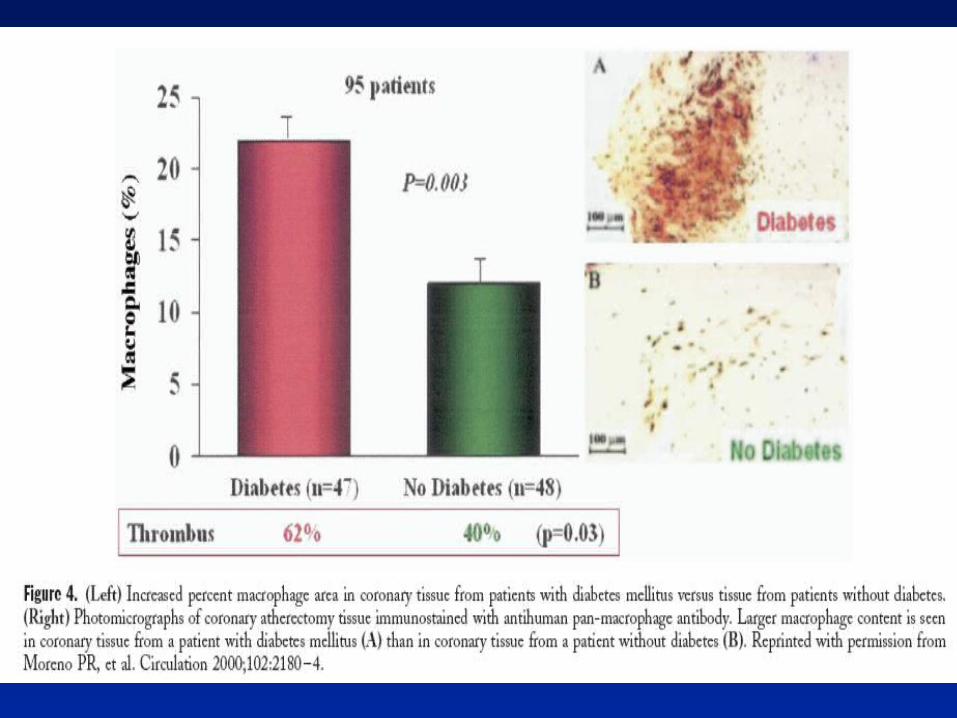
Atherothrombotic plaque in diabetic Atherothrombotic plaque in diabetic patientspatients
More in numberMore in number
More likely to ruptureMore likely to rupture
More likely to have existing surface thrombusMore likely to have existing surface thrombus
PCI Case
Optimising medical therapy
Metformin : reduced incidence of diabetes by 31% (Knowler NEJM 2002;346:393)
Ramipril : by 34% (HOPE JAMA 2001;286:1882)
Lipid lowering : by 22% (Collins Lancet 2003;361:2005)
Blood pressure control : SBP<140
Antiplatelets Antiplatelets
Aspirin 75mg once dailyAspirin 75mg once daily : :
Diabetes UK advises aspirin treatment in all patients with Diabetes UK advises aspirin treatment in all patients with diabetes over the age of 30 years with any of the following: diabetes over the age of 30 years with any of the following:
previous MI, angina, HT, diabetic eye disease, PVD, early kidney previous MI, angina, HT, diabetic eye disease, PVD, early kidney disease, raised cholesterol, family history of heart disease, disease, raised cholesterol, family history of heart disease, obesity, south Asians smokers, DM duration > 10 years.obesity, south Asians smokers, DM duration > 10 years.
Clopidogrel can be used as an alternative. Clopidogrel can be used as an alternative.
DES in Diabetes DES in Diabetes
Both Sirolimus- and Paclitaxel-eluting stents Both Sirolimus- and Paclitaxel-eluting stents substantially reduce angiographic and clinical substantially reduce angiographic and clinical restenosis compared with BMSrestenosis compared with BMS
DES have not eliminated the excess risk of DES have not eliminated the excess risk of restenosis in diabetics c/w non-diabeticsrestenosis in diabetics c/w non-diabetics
CABG: the “diabetic disadvantage”
Society of Thoracic Surgeons database of
1.37 million patients undergoing cardiac surgery
(1990-2000). Diabetic patients had higher rates of:
30 day mortality and
deep sternal wound infections
stroke
longer hospital stay
two-fold worse 10 year survival (36835 pts)
Brown et al Semin Thorac Cardiovasc Surg 2006;18:281
PCI v CABG( SYNTAX)
No mortality difference at 1 year
Higher incidence of CVA after CABG
More frequent angina after PCI
More frequent angiography and repeat revascularisation after PCI
Reducing risk in patients undergoing PCI – what can we do?
Tight glycaemic control (HbA1c ≤7) pre and post procedure (Corpus et al JACC 2004;43:8)
Thiazolidinediones – may reduce neointimal proliferation and restenosis in T2DM receiving BMS
Antithrhrombotic therapy
Drug eluting stents
ConclusionDiabetic patients are different
1. Epidemiology: increasing prevalence worldwide
2. Pathology: their vasculature is different - plaques more frequent and more prone to rupture .
3. Outcomes: for patients with type 2 diabetes sustaining an acute myocardial infarction is poor particularly if they have documented coronary artery disease.
4. Treatment: Modern therapies have a favourable effect but there remains a residual risk not addressed by these therapies.